nurse/non-medical requested x-rays
TRANSCRIPT

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 1 of 40 Version 5.5
Nurse/Non-Medical Requested X-rays
This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the circumstances of the individual patient in
consultation with the patient and /or carer. Health care professionals must be prepared to
justify any deviation from this guidance.
INTRODUCTION The NHS Plan (DOH 2000) and Making a Difference (DOH 1999), the government’s strategy for nursing and midwifery, highlighted the need to introduce new roles and new ways of working for nurses, midwives and allied health professionals to help improve services and the quality of patient treatment and care. The aim of introducing a policy to support nurses and non-medical practitioners to request x-ray examination is to ensure prompt diagnosis and treatment and the delivery of patient focused high quality care.
THIS GUIDELINE IS FOR USE BY THE FOLLOWING STAFF GROUPS : Trained staff identified within this policy.
Lead Clinician(s) Philip Goode Specialist Nurse Practitioner
Approved by Trauma & Orthopaedics Countywide Directorate Meeting on:
12th January 2016
This guideline should not be used after end of: 12th January 2018

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 2 of 40 Version 5.5
Key amendments to this guideline
Date Amendment By:
14/09/2010 Appendix 6 – Add Specialist Practitioner – Medicine and Specialist Physiotherapist
Sharon Ellson
16/11/2010 Appendix 3 – Total Knee replacement – AP weight bearing knee and lateral knee
Sharon Ellson
27/07/2011 Appendix 13 – Add A&E nurses – Criteria change to chest X-Rays in preceding 48 hours
Sharon Ellson
01/05/2013 Guideline changes to reflect introduction of online requesting
Philip Goode
01/05/2013 Change heading from ‘Appendix’ to ‘Protocol’ Philip Goode 01/05/2013 Addition of CT/MRI to protocols 1,8,9,12,15 Philip Goode 01/05/2013 Restriction of protocol 6 to WRH practitioners and
Trustwide Specialist Physiotherapists Philip Goode
01/05/2013 Addition of protocol 7 for T&O Practitioners (ALX) Philip Goode 01/05/2013 Addition of protocol 19 for GI specialist nurses Philip Goode 01/05/2013 Change of protocol 9 from ‘Vascular Nurse Specialist’
to ‘Nurse Consultant’. Protocol changes to reflect post. Philip Goode
01/05/2013 Protocols 16 and 18 changes from Heaf to Mantoux test for screening in TB
Philip Goode
01/05/2013 Appendicular views added to protocol 1 Philip Goode 01/05/2013 Appendix A added – requesting on behalf of Philip Goode
23/08/2013 Incorporation of pre exisiting DEXA protocol into policy – Protocol 20
Philip Goode
14/08/2015 Document extended for 12 months as per TMC paper approved on 22nd July 2015
TMC
12/01/2016 Protocol 21 added – senior orthopaedic nurses in fracture clinic (ALX)
T&O Directorate

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 3 of 40 Version 5.5
Nurse/Non Medical Requested X-rays
Introduction The NHS Plan (DOH 2000) and Making a Difference (DOH 1999), the government’s strategy for nursing and midwifery, highlighted the need to introduce new roles and new ways of working for nurses, midwives and allied health professionals to help improve services and the quality of patient treatment and care. Within the NHS Plan (DOH 2000) the Chief Nursing Officer identified 10 key roles for nurses and as a result nurses are being empowered to undertake a wider range of clinical tasks including the right to make and receive referrals, admit and discharge patients, order diagnostic tests and prescribe drugs. The practice of nurses requesting x-rays has been pioneered the in the field of Accident & Emergency (A&E) and is now common practice in many departments. Research has shown that nurses are able to request x-rays appropriately (Lindley-Jones and Finlayson 2000) and has demonstrated other benefits including reduction in transit time (Allerton & Justham 2000), more efficient use of nursing time and skills, improvement in the overall quality of service and increased staff and patient satisfaction (Parris et al 1997, Ward 1999) The aim of introducing a policy to support nurses and non-medical practitioners to request x-ray examination is to ensure prompt diagnosis and treatment and the delivery of patient focused high quality care.
Competencies Required This role is restricted to the following staff groups:
Specialist practitioners and out of hours practitioners in Medicine, Surgery, Trauma and Orthopaedics, Theatres and Pre-assessment and non medical practitioners e.g. physiotherapists and podiatrists
Specialist Nurses
Critical Care Outreach Team
Qualified nurses, working in Accident & Emergency, Medical Assessment Unit, Coronary Care and Minor Injury Units across Worcestershire Acute Hospitals NHS Trust.
All staff requesting x-rays must have successfully completed an appropriate training programme either recognised by the Trust or supported by the Training and Development team and appropriate clinicians. All practitioners will be registered on the Trust list of referrers as per IR(ME)R rules. All staff completing the programme will be expected to demonstrate knowledge of:
Trust protocol for nursing and non-medical staff requesting x-rays
Implications and hazards of radiological examinations
Ionising Radiation (Medical Exposure) Regulations- IR(ME)R 2000
Locally agreed protocols for the individual referrer
Professional accountability and responsibility as outlined in the NMC Scope for Professional Practice and the individual professions’ Codes of Professional Conduct

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 4 of 40 Version 5.5
Specialist Practitioners/Specialist Nurses, Minor Injury Staff and Critical Care Outreach staff will also be expected to demonstrate knowledge of:
Patient assessment and management
How to interpret the X-rays they are requesting, in order to prioritise the need for clinical intervention
Staff will be expected to be familiar with the PACS system.
Patients Covered
Patients covered under this guideline will vary according the practitioner’s role or area of
work – see separate appendices. No patients under the age of 3 years will be included in this
protocol.
Special Points X-rays must only be requested when the results, either positive or negative may have the potential to alter patient management X-rays must not be requested on women of child – bearing age that are known to be or may be pregnant. Although any concerns regarding this can be discussed with the Radiographers for a final decision. If the Radiographer considers that the x-ray request is not clinically justified, he/she will address any queries to the referrer and if necessary the radiographer will seek advice from a radiologist. Where the individual practitioner is requesting a CXR, every effort must be made to ensure that the patient has not had a recent CXR within the last 6 weeks – Images can be transferred from most Trusts in the UK. Where this is the case the PACS team should be contacted via the web link on PACS to arrange transfer of the images (Mon-Fri 9-5). Exceptions to this are new onset symptoms or tube placement.
It is the responsibility of the person requesting the x-ray to ensure that a member of the medical team also sees the x-ray and that the results of the examination are recorded in the patient’s medical record. Nurse practitioners working in minor injury and accident & emergency departments are responsible for reviewing their own x-rays and recording the results in the patient’s medical record. The registered practitioner must have undergone the agreed training programme devised for this role as agreed by the Director of Nursing and Radiology Clinical Director and achieved the necessary competencies before commencing practice. The radiology department will hold a list of approved staff and specimen signatures. Where the protocols do not cover advancements in practice staff should refer Appendix A for “requesting on behalf of” application.
WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 5 of 40 Version 5.5
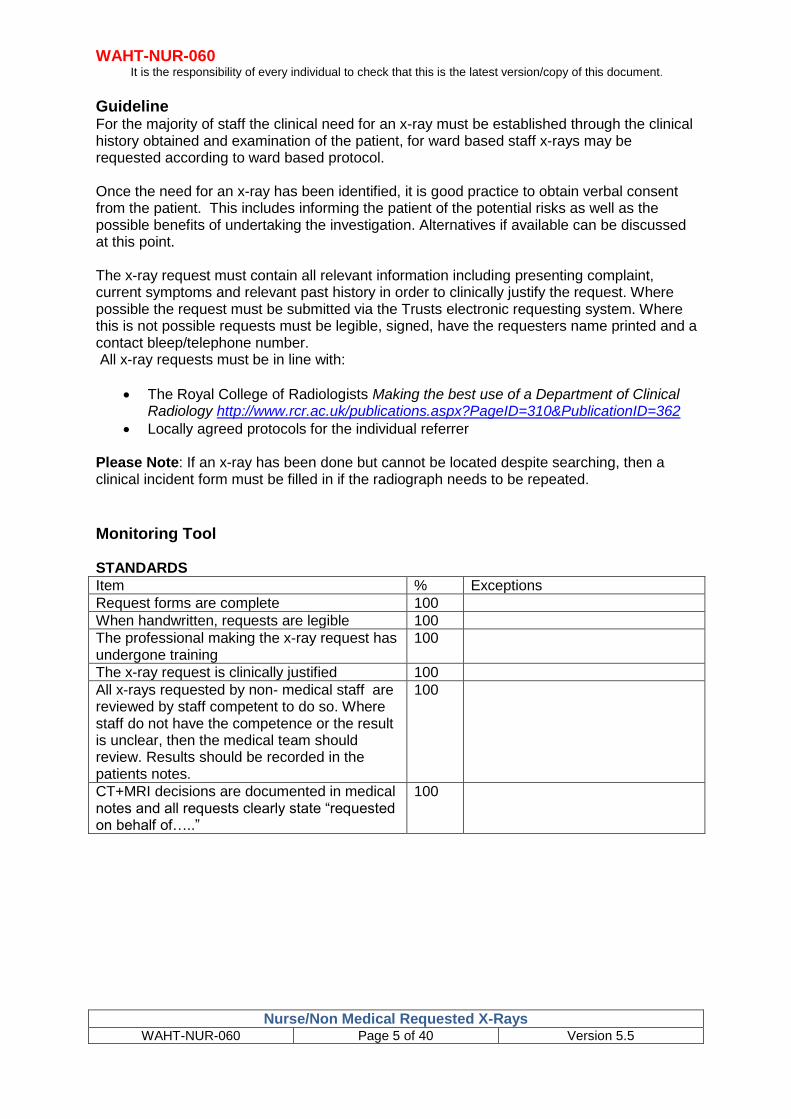
Guideline For the majority of staff the clinical need for an x-ray must be established through the clinical history obtained and examination of the patient, for ward based staff x-rays may be requested according to ward based protocol. Once the need for an x-ray has been identified, it is good practice to obtain verbal consent from the patient. This includes informing the patient of the potential risks as well as the possible benefits of undertaking the investigation. Alternatives if available can be discussed at this point. The x-ray request must contain all relevant information including presenting complaint, current symptoms and relevant past history in order to clinically justify the request. Where possible the request must be submitted via the Trusts electronic requesting system. Where this is not possible requests must be legible, signed, have the requesters name printed and a contact bleep/telephone number. All x-ray requests must be in line with:
The Royal College of Radiologists Making the best use of a Department of Clinical Radiology http://www.rcr.ac.uk/publications.aspx?PageID=310&PublicationID=362
Locally agreed protocols for the individual referrer Please Note: If an x-ray has been done but cannot be located despite searching, then a clinical incident form must be filled in if the radiograph needs to be repeated.
Monitoring Tool STANDARDS
Item % Exceptions
Request forms are complete 100
When handwritten, requests are legible 100
The professional making the x-ray request has undergone training
100
The x-ray request is clinically justified 100
All x-rays requested by non- medical staff are reviewed by staff competent to do so. Where staff do not have the competence or the result is unclear, then the medical team should review. Results should be recorded in the patients notes.
100
CT+MRI decisions are documented in medical notes and all requests clearly state “requested on behalf of…..”
100

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 6 of 40 Version 5.5
Need for x-ray identified
X-ray permitted under protocol
YES
NO
Await medical
assessment
Complete x-ray request (and send to x-ray department if
handwritten)
Radiographer to check name of referrer against approved staff list and protocol.
YES
NO
Request referred back
to department
manager
Radiographer to check that request can be clinically justified from information on request card.
YES
NO Discuss
with x-ray referrer
X-ray examination carried out Justified Refused
Referrer to ensure that a member of the medical team sees the x-ray and
that the results of the examination are recorded in the patient’s medical
records
Referrer qualified to interpret x-rays
Interpret x-ray and ensure that the results are recorded in the
patient’s records.
YES NO
NO
YES
Obtain patient’s verbal consent
X-ray requesting process for nurses and allied health professionals

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 7 of 40 Version 5.5
References
Allerton J, Justham D (2000) Nurse practitioners and the Ottawa Ankle Rules: Comparisons with medical staff in requesting x-rays for ankle injured patients. Accident & Emergency Nursing 8, 110-115
Department of Health (1999) Making a Difference, London, DOH
Department of Health (2000) The NHS Plan, London, DOH
Lee K M, Wong T W, Chan R, Lau C C, Fu Y K, Fung H (1996) Accuracy and efficiency of x-ray requests initiated by triage nurses in an Accident & Emergency department Accident & Emergency Nursing 4, 179-181
Lindley –Jones M, Finlayson B J (2000) Triage nurse requested x-rays – the results of a national survey Journal of Accident & Emergency Medicine 17: 108-110
Parris W, McCarthy S, Kelly A M, Richardson S (1997) Do triage nurse initiated x-
rays for limb injuries reduce transit time? Accident & Emergency Nursing 5, 14-15
Royal College of Radiologists Making the best use of a Department of Clinical
Radiology – Guidelines for Doctors
http://www.rcr.ac.uk/publications.aspx?PageID=310&PublicationID=362
Ward W (1999) Key issues in nurse requested x-rays Emergency Nurse Vol 6 No 9
19-23

WAHT-NUR-060 It is the responsibility of every individual to check that this is the latest version/copy of this document.
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 8 of 40 Version 5.5
CONTRIBUTION LIST
Key individuals involved in developing this document
Name Designation
Phil Goode Specialist Nurse Practitioner
Tracy Robson Superintendent radiographer
Circulated to the following individuals for comments
Name Designation
Dr Umesh Udeshi CD Radiology
David Hill Chief Radiographer
Pat Gowenlock Radiology WRH
Peter Holland Chair – Radiation Safety Committee
Specialist Nurses/AHP Trustwide
Chris Williams Superintendent Radiographer
Circulated to the following CD’s/Heads of dept for comments from their directorates / departments
Name Directorate / Department
Circulated to the chair of the following committee’s / groups for comments
Name Committee / group

Protocol 1
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 9 of 40 Version 5.5
Out of Hours Practitioners/Specialist Practitioners/Perioperative Practitioners X-ray Protocol
For adult patients aged 16 years or above
Following appropriate clinical examination and assessment the following investigations may be requested
Investigation Clinical problem/Criteria
Erect Chest X-ray PA (AP
view if unable to do PA)
Acute exacerbation of chronic obstructive airways disease
Erect Chest X-ray(AP view if
unable to do PA)
Pulmonary embolism
Erect Chest X-ray (AP view if
unable to do PA)
Pericarditis/pericardial effusion
Erect Chest X-ray(AP view if
unable to do PA)
Pneumonia
Erect Chest X-ray (AP view if
unable to do PA)
Pleural effusion
Erect Chest X-ray (AP view if
unable to do PA)
Haemoptysis
Erect Chest X-ray (AP view if
unable to do PA)
Acute exacerbation of asthma with either chest pain, clinical
signs of pneumothorax, pyrexia or raised WCC
Erect Chest X-ray (AP view if
unable to do PA)
Life threatening asthma- PEF < 33% predicted or best, or
SpO2 < 92% or PaO2 <8 Kpa.
Erect Chest X-ray (AP view if
unable to do PA)
Pneumothorax
Erect Chest X-ray (AP view if
unable to do PA)
Central chest pain? myocardial infarction.
Erect Chest X-ray (AP view if
unable to do PA)
Chest pain ?aortic dissection.
Erect Chest X-ray (AP view if
unable to do PA)
Post insertion of a fine bore nasogastric feeding tube with
guide wire or jejunostomy tube to confirm placement.
See Trust policy WHAT-NUR-065
Erect Chest x-ray, (AP view if
unable to do PA)
Supine abdominal x-ray
Acute abdominal pain? Perforation or obstruction.

Protocol 1
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 10 of 40 Version 5.5
Investigation Clinical problem/Criteria
Erect Chest x-ray Post insertion of central venous access devices (CVAD) to confirm position.
Erect Chest x-ray Post insertion of peripherally inserted central catheters (PICC) to confirm position.
Erect Chest x-ray Post insertion of a chest drain to confirm accurate tube placement.
Erect Chest x-ray Acute onset of shortness of breath? Left ventricular failure or worsening heart failure.
Erect Chest x-ray Post removal of a chest drain – provided competences associated with chest drain removal have been completed.
Erect Chest x-ray Post cardiac arrest and successful resuscitation to:-
- Confirm correct siting of tracheal tube, gastric tube,
central venous line.
- To exclude left ventricular failure
- To exclude pulmonary aspiration
- To exclude pneumothorax
- To establish size and shape of heart
Abdominal x-ray Acute exacerbation of inflammatory bowel disease of colon.
Forearm/wrist/hand/scaphoid Mechanism of Injury, Focal bony tenderness and Loss of function.
Elbow Mechanism of Injury, Focal bony tenderness and loss of function
Humerus Mechanism of Injury, Focal bony tenderness, loss of function
Shoulder Mechanism of Injury with restriction of shoulder movements/loss of function on movement
Clavicle Mechanism of injury, Focal bony tenderness, Obvious deformity.
X-ray pelvis with lateral x-ray
hip
Fall with inability to weight bear – patients over 65

Protocol 1
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 11 of 40 Version 5.5
Ankle Mechanism of Injury– refer to the Ottawa ankle rules and document on request
Knee Mechanism of Injury– refer to the Ottawa knee rules and document on request
Foot, Mechanism of Injury, Focal bony tenderness, loss of function
Tibia/Fibula Mechanism of Injury, Bony tenderness, non-weight bearing, bony deformity
CT/MRI Requests may only be initiated by a Consultant. Any request submitted following this request must have the following:
Documented decision in medical notes.
Documented in clinical history stating “Requested on behalf
of ……………..”

Protocol 2
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 12 of 40 Version 5.5
Critical Care Outreach X-ray Protocol
For adult patients aged 16 years or above
Following appropriate clinical examination and assessment the following investigations may be requested
Investigation Clinical problem/Criteria
Erect Chest X-ray PA (AP
view if unable to do PA)
Acute exacerbation of chronic obstructive airways disease
Erect Chest X-ray(AP view if
unable to do PA)
Pulmonary embolism
Erect Chest X-ray (AP view if
unable to do PA)
Pericarditis/pericardial effusion
Erect Chest X-ray(AP view if
unable to do PA)
Pneumonia
Erect Chest X-ray (AP view if
unable to do PA)
Pleural effusion
Erect Chest X-ray (AP view if
unable to do PA)
Haemoptysis
Erect Chest X-ray (AP view if
unable to do PA)
Acute exacerbation of asthma with either chest pain,
clinical signs of pneumothorax, pyrexia or raised WCC
Erect Chest X-ray (AP view if
unable to do PA)
Life threatening asthma- PEF < 33% predicted or best, or
SpO2 < 92% or PaO2 <8 Kpa.
Erect Chest X-ray (AP view if
unable to do PA)
Pneumothorax
Erect Chest X-ray (AP view if
unable to do PA)
Central chest pain ? myocardial infarction
Erect Chest X-ray (AP view if
unable to do PA)
Chest pain ?aortic dissection
Erect Chest X-ray (AP view if
unable to do PA)
Post insertion of a fine bore nasogastric feeding tube such
as a Flocare Pur tube with guide wire or jejunostomy tube
to confirm placement

Protocol 2
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 13 of 40 Version 5.5
Investigation Clinical problem/Criteria
Erect Chest x-ray Post insertion of central venous access devices (CVAD) to confirm position.
Erect Chest x-ray Post insertion of peripherally inserted central catheters (PICC) to confirm position.
Erect Chest x-ray Post insertion of a chest drain to confirm accurate tube placement.
Erect Chest x-ray Acute onset of shortness of breath? Left ventricular failure or worsening heart failure.
Erect Chest x-ray Post removal of a chest drain – provided competences associated with chest drain removal have been completed.
Erect Chest x-ray Post cardiac arrest and successful resuscitation to:
Confirm correct siting of tracheal tube, gastric tube, central venous line
To exclude left ventricular failure
To exclude pulmonary aspiration
To exclude pneumothorax
To establish size and shape of heart

Protocol 3
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 14 of 40 Version 5.5
Pre-operative/Perioperative Assessment Nurses X-ray Protocol
For adults aged 16 years or above
Orthopaedic X-ray Protocol
Procedure X-ray and reason
Total Hip replacement To have AP pelvis and lateral hip within 6 months of operation
Revision Hip replacement To have AP pelvis and lateral hip to include the whole prosthesis within 6 months of operation
Total knee replacement AP weight bearing knee and lateral knee
Other knee surgery AP weight bearing, lateral skyline views within 6 months of operation
Lumbar spinal decompression/fusion
AP and lateral lumbar spine – if not done in previous 3 years
Total shoulder replacement Shoulder AP within 6 months of operation
Rotator Cuff repair Shoulder AP within 6 months of operation
Impingement Shoulder AP within 6 months of operation
Shoulder instability Shoulder AP within 6 months of operation
Removal of metal work Up to date x-ray showing all metalwork
Cervical X- ray Protocol
Investigation Criteria
Cervical spine
Lateral and AP
In patients with rheumatoid arthritis or Downs Syndrome x-rays may be used to evaluate spinal instability. Cases must be discussed individually with the surgeon and anaesthetist.
Chest X-ray protocol
Investigation Criteria
Erect Chest X-ray Pre-operative chest x-ray should be taken for:
All patients with acute chest disease.
All immigrants (persons arriving in the country within the last 6 months) from areas with endemic TB, if no previous CXR available
Patients who following history, examination or pathology may have lung/heart disease
All patients with a known primary malignancy if no x-ray within last 6 months
All patients undergoing cardiac/chest surgery if no x-ray within last 6 months

Protocol 4
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 15 of 40 Version 5.5
Emergency Department Nurse X-ray Protocol
For adults and children age 5 or above
Qualified nurses in A&E, who have successfully completed the Trust training programme and
competency, may request x-rays on patients attending A&E with traumatic injuries when
there is clinically a very high suspicion of a fracture i.e. deformity, swelling, severe pain, bony
tenderness or loss of function. Special Points
Nurses will only request X-rays on children when there is parental consent.
Patients who require parenteral analgesia will be referred for medical advice
All radiographs must be reviewed by the doctor in A&E before the patient leaves the department.
Investigation Criteria
Finger/thumb Mechanism of Injury, Focal bony tenderness and Loss of function
Forearm/wrist/hand/scaphoid Mechanism of Injury, Focal bony tenderness and Loss of function.
Elbow Mechanism if Injury, Focal bony tenderness and loss of function
Humerus Mechanism of Injury, Focal bony tenderness, loss of function
Shoulder Mechanism of Injury with restriction of shoulder movements/loss of function on movement
Clavicle Mechanism of injury, Focal bony tenderness, Obvious deformity.
Ankle Mechanism of Injury– refer to the Ottawa ankle rules
Knee Mechanism of Injury– refer to the Ottawa knee rules
Foot Mechanism of Injury, Focal bony tenderness, loss of function
Pelvis and Hip Patients aged 65 or above with mechanism of injury eg. fall with suspected fractured neck of femur, non weight bearing and loss of function.
Foreign bodies To exclude foreign bodies when there is a clear history of penetration by a foreign body made of metal, stone or glass. X-rays to exclude foreign bodies are restricted to the areas in the ED Nurse protocol

Protocol 4
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 16 of 40 Version 5.5
Band 6 Nursing Staff and above trained and approved by ED Consultant
Erect Chest X-ray PA (AP
view if unable to do PA)
Chest Pain
Erect Chest X-ray (AP view
if unable to do PA)
Acute onset of breathlessness or worsening of pre-existing
breathlessness
Erect Chest X-ray (AP view
if unable to do PA)
Hypoxia (oxygen saturations below 94%)
Erect Chest X-ray(AP view
if unable to do PA)
Diagnosis of pneumothorax
Erect Chest X-ray (AP view
if unable to do PA)
Diagnosis recent aspiration
Erect Chest X-ray (AP view
if unable to do PA)
Haemoptysis
Erect Chest X-ray (AP view
if unable to do PA)
Diagnosis of myocardial infarction/cardiac
arrhythmia/angina/heart failure
Erect Chest X-ray (AP view
if unable to do PA)
Diagnosis of exacerbation of COPD/asthma
Erect Chest X-ray (AP view
if unable to do PA)
Elevated white cell count > 12 x 109 / L
Erect Chest X-ray (AP view
if unable to do PA)
Diagnosis of pneumonia/chest infection

Protocol 5
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 17 of 40 Version 5.5
Emergency Nurse Practitioner - Emergency Departments and Minor Injury Units
For adults and children aged 3 or above Special points
Other x-rays may be requested after prior discussion with the radiographer, following advice and instruction from a clinician. (This information must be documented on the x-ray request form).
X-rays requested by Emergency Nurse Practitioners may be reviewed independently.
Investigation Criteria
Finger/thumb Mechanism of Injury, Focal bony tenderness and Loss of function
Forearm/wrist/hand/scaphoid Mechanism of Injury, Focal bony tenderness and Loss of function.
Elbow Mechanism if Injury, Focal bony tenderness and loss of function
Shoulder Mechanism of injury with restriction of shoulder movements/loss of function on movement
Clavicle Mechanism of injury ,focal bony tenderness and obvious deformity
Foot including toes Mechanism of injury, bony tenderness and loss of function
Ankle History of trauma – refer to the Ottawa ankle rules
Knee History of trauma – refer to the Ottawa knee rules
Tibia/Fibula Mechanism of injury, bony tenderness, non weight bearing, bony deformity
Pelvis and Hip Patients aged 65 or above with mechanism of injury eg. fall with suspected fractured neck of femur, non weight bearing and loss of function.
Foreign bodies To exclude foreign bodies when there is a clear history of penetration by a foreign body made of metal, stone or glass. X-rays to exclude foreign bodies are restricted to the areas in the ENP protocol
CXR Age 3 – 16
To exclude metal FB
Metal detector activating above diaphragm
OR
Metal detector not activating with good history of swallowed metal FB

Protocol 6
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 18 of 40 Version 5.5
Nurse Practitioner in Trauma & Orthopaedics (WRH) and Specialist Physiotherapist.
For adults over 16 years
Special Points
For patients with orthopaedic and trauma conditions seen in pre-admission clinics, pre-operatively and postoperatively as an inpatient or in follow up clinics
X-rays requested by the specialist practitioner in trauma and orthopaedics may be reviewed independently (according to IRMER rules)
Where appropriately trained, Physiotherapists should request under the separate
Trust Guideline (WAHT-PHY-021)
Investigation Criteria
Knee – AP, Lateral views and skyline views
Feet - AP, Lateral and Medial views
Full leg -AP and lateral views
Forearm -AP and Lateral views
Wrist -AP and lateral views
Humerus and shoulder -AP, lateral, Oblique views
Pelvis- AP
Hip - Lateral
Lumbar spine - AP and lateral
Patients presenting with pain, deformity, unexpected swelling.
Patients following surgery
Inpatients and outpatients
Check of position
History of injury
Erect Chest X-ray Post insertion of a fine bore nasogastric feeding tube, (radio-opaque or with guide wires inserted), or jejunostomy tube to confirm placement
See Trust policy WHAT-NUR-065
Erect Chest X-ray(AP view if unable to do
PA)
Pulmonary embolism
Erect Chest X-ray(AP view if unable to do
PA)
Pneumonia

Protocol 6
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 19 of 40 Version 5.5
Investigation Criteria
Erect Chest X-ray
Pre-operative chest x-ray should be taken for :
All patients with acute chest disease.
All patients with chronic chest disease if no CXR for 6 months
All immigrants (persons arriving in the country within the last 6 months) from areas with endemic TB, if no previous CXR available
Patients who following history, examination or pathology may have lung/heart disease
All patients with a known primary malignancy

Protocol 7
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 20 of 40 Version 5.5
Orthopaedic Nurse Practitioners (ALX)
For Adults only
First line 1/7 post-op views only
Images will be reported by a radiologist or Reporting radiographer
Investigation Criteria
Knee - AP &Lateral Post-op total knee replacement
Post-op knee re-surfacing
Post-op partial knee replacement
Hip - AP pelvis & lateral Post-op total hip replacement
Post-op hip re-surfacing
Shoulder -AP &Lateral Post-op shoulder replacement
Elbow - AP &Lateral Post-op elbow replacement
Ankle - AP &Lateral Post-op ankle replacement
Wrist - AP &Lateral Post-op trapezium replacement
Hand - AP &Lateral Post-op MCPJ replacement

Protocol 8
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 21 of 40 Version 5.5
Respiratory Specialist Nurses
For adults aged 16 years or over
Investigation Criteria
Erect Chest X-ray PA & lateral if required (AP view if unable to do PA)
Post PICC line insertion to confirm position
Erect Chest X-ray PA & lateral if required (AP view if unable to do PA)
Acute exacerbation of bronchiectasis
Erect Chest X-ray PA & lateral if required
(AP view if unable to do PA)
Acute exacerbation of chronic obstructive
airways disease
Erect Chest X-ray PA & lateral if required
(AP view if unable to do PA)
Acute exacerbation of asthma with either
chest pain, clinical signs of pneumothorax,
pyrexia or raised WCC
Erect Chest X-ray (AP view if unable to do
PA)
Life threatening asthma- PEF < 33%
predicted or best, or SpO2 < 92% or PaO2
<8 Kpa.
Erect Chest X-ray PA & lateral if required
(AP view if unable to do PA)
Follow up for known malignancy - excluded if
recent x-ray (within 6 weeks) available,
unless request based on clinical presentation
of patient eg, exacerbation of symptoms
Erect Chest X-ray PA & lateral if required
(AP view if unable to do PA)
Follow up after thoracic surgery- if clinical
presentation indicates a need.
Erect Chest X-ray PA & lateral if required
(AP view if unable to do PA)
Screening for tuberculosis contacts
Erect Chest X-ray PA & lateral if required
(AP view if unable to do PA)
Outpatient follow –up COPD, Sarcoid,
Pulmonary fibrosis, Pneumonia, Asthma
CT/MRI Requests may only be initiated by a Consultant. Any request submitted following this request must have the following:
Documented decision in medical notes.
Documented in clinical history stating
“Requested on behalf of ……………..”

Protocol 9
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 22 of 40 Version 5.5
X-ray protocol for Vascular Nurse Consultant
For adult patients aged 16 or over
Investigation Criteria
Erect Chest X-ray Pre-operative chest x-ray should be taken for:
All patients with acute chest disease.
All patients with chronic chest disease if no CXR for 6 months
All immigrants (persons arriving in the country within the last 6 months) from areas with endemic TB, if no previous CXR available
Patients who following history, examination or pathology may have lung/heart disease
All patients with a known primary malignancy
Feet and or Calcaneum ? osteomyelitic changes
Ankle
Knee
Feet
Pelvis
Lumbar spine
Patients presenting with pain, deformity, unexpected swelling.to differentiate musculo-skeletal problem from vascular problem.
Patients following surgery
Inpatients and outpatients
History of injury
CT/MRI Any decision for CT/MRI should be made by
Consultant and discussion clearly
documented in the medical notes with the
request clearly stating, in the request text,
which Consultant made the decision.
“Following discussion with……………”

Protocol 10
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 23 of 40 Version 5.5
X-ray protocol for Rheumatology Nurse Practitioners
For adult patients aged 16 or over
Xray Criteria
Erect Chest X-ray Baseline investigation prior to commencing treatment with disease modifying agents where previous x-ray more than 6 months ago
Upper Limb Baseline investigation to determine progressive/degenerative changes where previous x-ray more than 6 months ago
Lower Limb Baseline investigation to determine progressive/degenerative changes where previous x-ray more than 6 months ago
Peripheral joints Baseline investigation to determine progressive/degenerative changes where previous x-ray more than 6 months ago.

Protocol 11
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 24 of 40 Version 5.5
X-ray protocol for Specialist Nurses for Heart Disease – Rapid Access Chest Pain
For adult patients aged 16 or over
Investigation Criteria
Erect Chest X-ray (AP view if unable to do
PA)
Unexplained ongoing chest pain
Erect Chest X-ray PA (AP view if unable to
do PA)
Pulmonary embolism
Erect Chest X-ray(AP view if unable to do
PA)
Pericarditis/pericardial effusion
Erect Chest X-ray (AP view if unable to do
PA)
Pneumonia
Erect Chest X-ray(AP view if unable to do
PA)
Pleural effusion
Erect Chest X-ray (AP view if unable to do
PA)
Haemoptysis
Erect Chest X-ray (AP view if unable to do
PA)
Pneumothorax
Erect Chest X-ray (AP view if unable to do
PA)
Acute onset of shortness of breath ?left
ventricular failure
Erect Chest X-ray (AP view if unable to do
PA)
Chest pain ?aortic dissection
Erect Chest X-ray (AP view if unable to do
PA)
All immigrants (persons arriving in the
country within the last 6 months) from areas
with endemic TB, if no previous CXR
available
Erect Chest X-ray (AP view if unable to do
PA)
Smokers with suspected malignancy
Protocol 12
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 25 of 40 Version 5.5
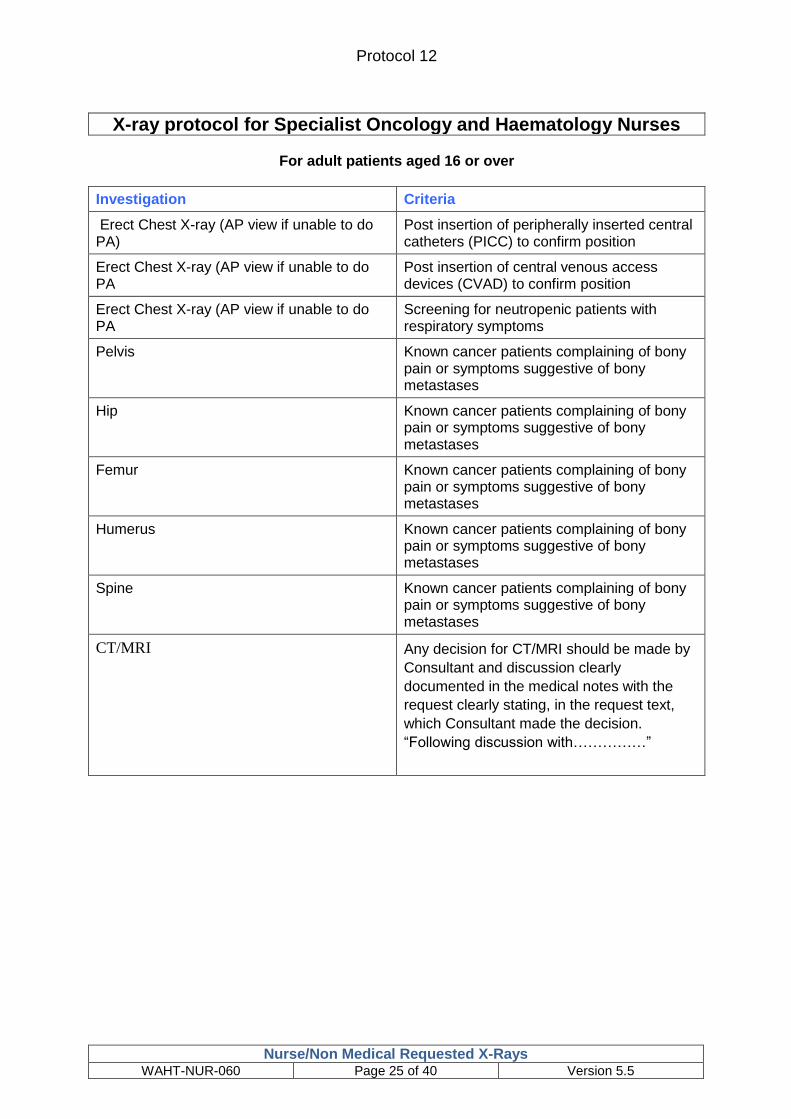
X-ray protocol for Specialist Oncology and Haematology Nurses
For adult patients aged 16 or over
Investigation Criteria
Erect Chest X-ray (AP view if unable to do PA)
Post insertion of peripherally inserted central catheters (PICC) to confirm position
Erect Chest X-ray (AP view if unable to do PA
Post insertion of central venous access devices (CVAD) to confirm position
Erect Chest X-ray (AP view if unable to do PA
Screening for neutropenic patients with respiratory symptoms
Pelvis Known cancer patients complaining of bony pain or symptoms suggestive of bony metastases
Hip Known cancer patients complaining of bony pain or symptoms suggestive of bony metastases
Femur Known cancer patients complaining of bony pain or symptoms suggestive of bony metastases
Humerus Known cancer patients complaining of bony pain or symptoms suggestive of bony metastases
Spine
Known cancer patients complaining of bony pain or symptoms suggestive of bony metastases
CT/MRI Any decision for CT/MRI should be made by
Consultant and discussion clearly
documented in the medical notes with the
request clearly stating, in the request text,
which Consultant made the decision.
“Following discussion with……………”

Protocol 13
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 26 of 40 Version 5.5
X-ray protocol for Diabetic Specialist Nurses /Podiatrists/Tissue Viability Nurse
For adult patients aged 16 or over
Investigation Criteria
Foot and calcaneum X-ray To exclude or monitor osteomyelitis, charcots
joints and foreign bodies.
Protocol 14
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 27 of 40 Version 5.5
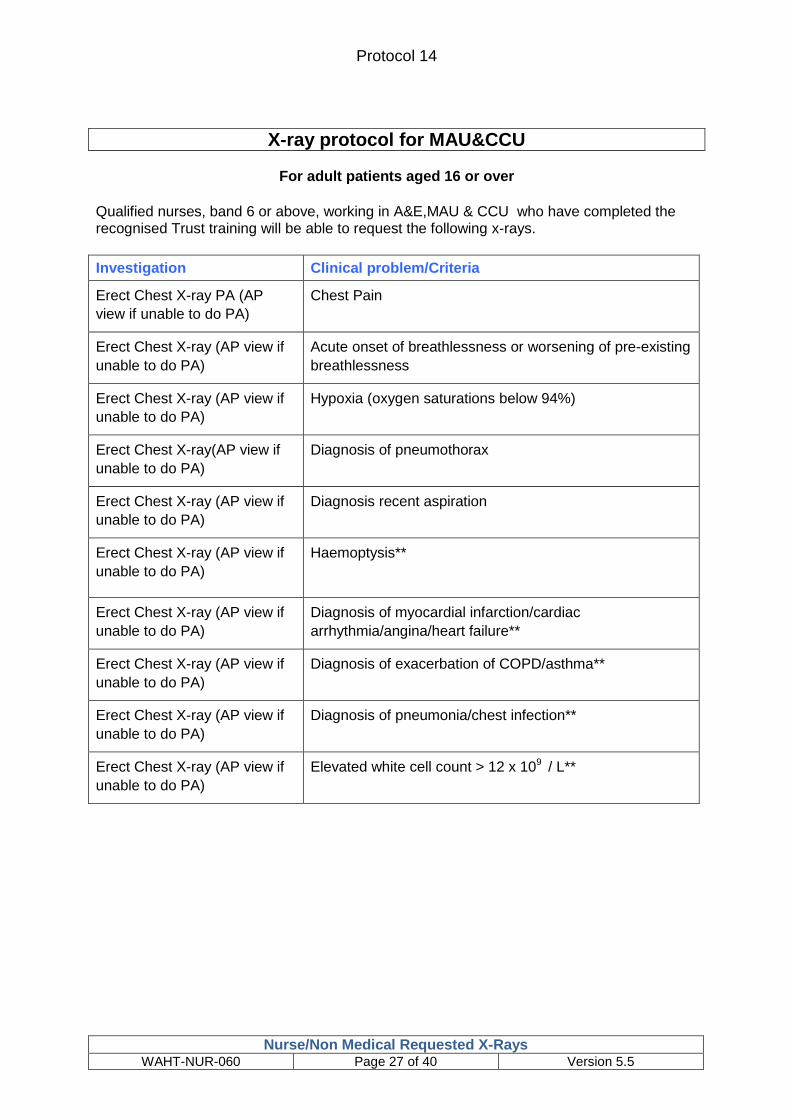
X-ray protocol for MAU&CCU
For adult patients aged 16 or over
Qualified nurses, band 6 or above, working in A&E,MAU & CCU who have completed the recognised Trust training will be able to request the following x-rays.
Investigation Clinical problem/Criteria
Erect Chest X-ray PA (AP
view if unable to do PA)
Chest Pain
Erect Chest X-ray (AP view if
unable to do PA)
Acute onset of breathlessness or worsening of pre-existing
breathlessness
Erect Chest X-ray (AP view if
unable to do PA)
Hypoxia (oxygen saturations below 94%)
Erect Chest X-ray(AP view if
unable to do PA)
Diagnosis of pneumothorax
Erect Chest X-ray (AP view if
unable to do PA)
Diagnosis recent aspiration
Erect Chest X-ray (AP view if
unable to do PA)
Haemoptysis**
Erect Chest X-ray (AP view if
unable to do PA)
Diagnosis of myocardial infarction/cardiac
arrhythmia/angina/heart failure**
Erect Chest X-ray (AP view if
unable to do PA)
Diagnosis of exacerbation of COPD/asthma**
Erect Chest X-ray (AP view if
unable to do PA)
Diagnosis of pneumonia/chest infection**
Erect Chest X-ray (AP view if
unable to do PA)
Elevated white cell count > 12 x 109 / L**

Protocol 15
Nurse/Non Medical Requested X-Rays WAHT-NUR-060 Page 28 of 40 Version 5.5
X-ray protocol for Specialist Urology Nurse/Rapid Access Urology Clinic Nurses- Trust Wide
Investigation Criteria
Plain abdominal X-ray (KUB) As part of the protocol for these clinics to
assess skeleton for sclerotic metastases,
and for renal tract calculi
Ultrasound KUB
Patients attending out patient clinic as a new
referral or proven malignancy
Plain x-rays of Chest, Pelvis, Spine (depending on bone scan report)
For patients with proven urological cancers
Plain x-ray of Chest
For diagnosis & staging of urological cancers
Trans rectal ultrasound guided biopsy of prostate gland
For diagnosis of prostate cancer
CT/MRI Any decision for CT/MRI should be made by
Consultant and discussion clearly
documented in the medical notes with the
request clearly stating, in the request text,
which Consultant made the decision.
“Following discussion with……………”

Protocol 16
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 29 of 40 Version 5.5
X-ray protocol for Occupational Health Nurse
For adult employees – aged over 16 years
Investigation Criteria
Erect Chest X-ray Pre employment of health care staff with
direct patient contact, who are from countries
with a high prevalence of TB (40
per100,000) who have not yet had a clear
chest x ray result on entry to the country-
screening for Tuberculosis
Mantoux result of 9mm or over with
respiratory symptoms indicative of TB-
screening for Tuberculosis
Respiratory Health surveillance as required
by Health and Safety Legislation, due to
exposure in the workplace of substances
hazardous to health. Eg Silica, Asbestos

Protocol 17
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 30 of 40 Version 5.5
X-ray protocol for Specialist Breast Care Nurse
Investigation Criteria
Mammogram Follow up annual screening for
women over 40 years of age
considered to be at moderate risk of
developing breast cancer as a result
of their family history – patients’ age
35-40 yrs - requests only after
discussion with consultant.
Annual post surgical follow up of
patients treated for breast cancer
Patients attending one-stop
mammography clinic after discussion
with consultant breast surgeon
Dexa scans Patient has been diagnosed with a
primary breast cancer.
Patient is post- menopausal.
The histopathology of the cancer has
been identified as oestrogen receptor
positive.
Patient has been commenced on an
aromatase inhibitor.
Protocol 18
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 31 of 40 Version 5.5
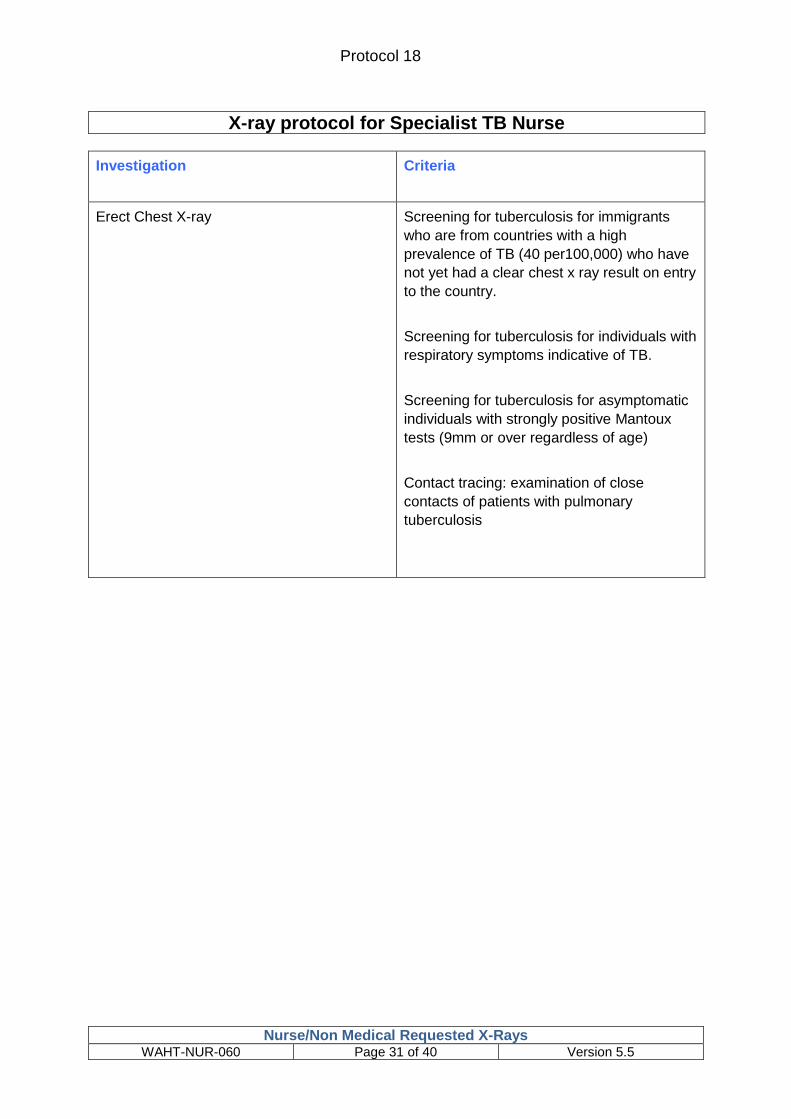
X-ray protocol for Specialist TB Nurse
Investigation Criteria
Erect Chest X-ray Screening for tuberculosis for immigrants
who are from countries with a high
prevalence of TB (40 per100,000) who have
not yet had a clear chest x ray result on entry
to the country.
Screening for tuberculosis for individuals with
respiratory symptoms indicative of TB.
Screening for tuberculosis for asymptomatic
individuals with strongly positive Mantoux
tests (9mm or over regardless of age)
Contact tracing: examination of close
contacts of patients with pulmonary
tuberculosis

Protocol 19
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 32 of 40 Version 5.5
X-ray protocol for Upper GI/Colorectal Specialist Nurse
For adult patients aged 16 or over
Investigation Criteria
CT/MRI Any decision for CT/MRI should be made by
Consultant and discussion clearly
documented in the medical notes with the
request clearly stating, in the request text,
which Consultant made the decision.
“Following discussion with……………”
Barium Swallow For patients presenting with history or
dysphagia and/or dysmotility
Barium meal with follow through For patients presenting with dysmotility or
symptoms suggestive of obstruction.
Erect Chest X-ray (AP view if unable to do
PA)
Acute onset of breathlessness or worsening
of pre-existing breathlessness
Abdominal x-ray Acute exacerbation of inflammatory bowel
disease of colon.
Erect Chest x-ray, (AP view if unable to do
PA)
Supine abdominal x-ray
Acute abdominal pain? Perforation or
obstruction.

Protocol 20
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 33 of 40 Version 5.5
X-ray protocol for Osteoporosis/Fracture Liaison Specialist Nurse
For adult patients aged 16 or over
Investigation Criteria
Dexa scan Investigation following NICE guidelines
(TA160 & TA161) and Worcestershire
guidelines for osteoporosis, where patient
has risk factors, in order to determine
treatment options

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 34 of 40 Version 5.5
Appendix A
“Requesting on behalf of” (ROBO)

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 35 of 40 Version 5.5
Directorate of Radiology
Radiology Requesting from ICE – Referrals input into ICE on behalf of a Clinician by Non-Medical Staff
Introduction: Robust methods need to be devised to ensure that electronically generated
requests for imaging procedures are authorised only by properly trained individuals. Guide to Justification for Clinical Radiologists Ref No: BFCR(00)5 The Royal College of Radiologists, August 2000 Ionising radiation (e.g. X-rays) can be harmful. Radiology and the Trust must operate under statute law IR(ME)R – Ionising Radiations (Medical Exposure) Regulations, Medical Exposure) when patients are referred for an examination which expose them to Ionising radiation. This ensures protection to the patient and that X-rays are only used if there is clear clinical justification and benefit to the patient. This helps to keep the dose of radiation that individual patients and the population of the country, receive from medical exposure as low as possible. IR(ME)R lays down stringent guidelines and regulations, which if the Trust or individuals ignore can lead to prosecution in a court of law.
Background: Requests historically are made using a handwritten request and only carried
out when signed by the referring clinician (usually a Doctor or other suitable trained, and IR(ME)R trained, health professional. The way requests are made is changing and most if not all requests will be made electronically using the ICE system. Using ICE is normally uncomplicated, as the clinician has been granted electronic password access to refer patients for radiological examinations. The clinician makes the request by entering this data into the ICE system. Radiology receive the information electronically as to who referred the patient but also who entered the data into ICE. Some clinicians, due to reasonable workflow practice, may ask radiology, that specific non medical staff i.e. specific nursing staff for certain clinics or midwives for antenatal ultrasound examinations are granted access to enter the request into ICE, following protocol or clinical assessment of the patient by the clinician.
Requirement: In order for clinicians to do this, and ensure proper compliance with
IR(ME)R and maintain proper clinical governance this will only be granted via a proper written procedure. The purpose of this form is to ensure that the individuals (the clinician and non medical staff) fully understand the issues and have both signed to enable their ICE access for radiology requesting, to be activated. Once signed please photocopy for you own records and send the original back to Tracy Scarborough, c/o General Management, Alexandra Hospital in hard copy format only. Radiology will then contact the ICE Team to amend your settings. You will be advised when this has been carried out.

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 36 of 40 Version 5.5
** Please print below your full name and role that this Form applies to: ……………………………………………………………………………………………………………………………….
I will only input radiological requests into ICE following clear instruction from the clinical staff (the consultant(s) who is the referrer, named on this form), who has made a clinical assessment of the patient and the radiological examination(s) required or this is done under protocol identified on this form.
I understand that I am inputting the request on behalf of the named Consultant(s) and I fully understand that I cannot make an electronic order for a radiological test on my own behalf or for anyone other than the named clinical staff included within this document.
I will only complete an ICE order if the patients demographic details, the examination being requested and the clinical history is absolutely clear and unambiguous. If it is not then I will refer this back to the consultant prior to the ICE request being submitted.
Failure to comply with this would be a breach of IR(ME)R regulations, if the request is for an examination involving X-rays e.g Chest X-ray, CT scan or Nuclear Medicine study. I understand that failure to comply could bring about prosecution in a Court of Law
For examinations not involving radiation e.g. MRI and Ultrasound then this would be breach of normal Trust guidelines and practice and could be a disciplinary offence.
Note: Form must be signed and returned in hard copy format only – email versions will not be accepted Signed:…………………………………………………(non medical staff member) Dated……………………………………………………………. Signed:…………………………………………………(Consultant 1) Print Name……………………….. Dated……………………………………………………………. Signed:…………………………………………………(Consultant 2) Print Name……………………….. Dated……………………………………………………………. List any other additional Consultants who you refer on behalf of: …………………………………………………………………………………………………………………………… This from may be modified or updated from time to time and may then require re submission.

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 37 of 40 Version 5.5
Protocol 21
Senior Orthopaedic Nurses in Fracture Clinic (ALX)
For Adults only
Follow up x-rays to assess alignment and healing in fracture clinic
X-rays may also be ordered if the clinic letter from the patient’s previous attendance
at # clinic states ‘x-ray on arrival’ with clear instructions of the limb/joint required
and is within this protocol.
Investigation
Criteria
Calcaneus – AP and Axial
Non operatively treated
At 1/2/3 weeks to check alignment and at 6 & 12 weeks to check healing
Operatively treated
At 1/2/6/12 weeks to check healing
Foot – DP and Oblique and/or Lateral
Non operatively treated
At 1/2/3 weeks to check alignment and at 6 weeks to check healing
Operatively treated
At 1/2/6 weeks to check healing
Ankle – AP and Lateral
Non operatively treated
At 1/2/3 weeks to check alignment and at 6 & 12 weeks to check healing
Operatively treated
At 1/2/6/12 weeks to check healing
Tibia and Fibula – AP and Lateral
Non operatively treated
At 1/2/3 weeks to check alignment and at 6/12 weeks to check healing
Operatively treated
At 1/2/6/12/16 weeks to check healing
Femur – AP and lateral Non operatively treated
At 1/2/3 weeks to check alignment and at 6/12 weeks to check healing
Operatively treated
At 1/2/6/12/16 weeks to check healing
Wrist – DP and Lateral
Non operatively treated
At 1/2/3 weeks to check alignment and at 6 weeks to check healing
Operatively treated

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 38 of 40 Version 5.5
At 1/2 & 6 weeks to check healing
Forearm – AP and Lateral
Non operatively treated
At 1/2/3 weeks to check alignment and at 6 weeks to check healing
Operatively treated
At 1, 2 & 6 weeks to check healing Elbow – AP and Lateral
Non operatively treated
At 1/2/6/12 weeks to check alignment and healing
Operatively treated
At 1/6/12 weeks to check alignment and healing
Humerus – AP and lateral
Non operatively treated
At 1/2/3 weeks to check alignment and at 6 weeks to check healing
Operatively treated At 1, 2 & 6 weeks to check healing
Shoulder – AP and axial
Non operatively treated
At 1/2/6 weeks to check alignment and healing
Operatively treated
At 1/6/12 weeks to check alignment and healing
Clavicle – AP and 30 degree angle
Non operatively treated
At 1/2/6 weeks to check alignment and healing
Operatively treated
At 1/6/12 weeks to check healing

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 39 of 40 Version 5.5
Protocol 21 Senior Orthopaedic Nurses in Fracture Clinic, Alex Orthopaedic Centre
Follow up X rays undertaken to assess alignment and bony healing in fracture clinic (ALX)
Investigation Criteria
Ankle fractures AP(Mortise) and Lateral views Weight bearing if possible (6 and 12 weeks)
Non operatively treated at 1/2/3 weeks to check alignment and
at 6 & 12 weeks to check healing Operatively treated
at 1/2/6/12 weeks to check healing
Proximal tibial fractures and fractures of the tibial shaft AP and Lat views (weight bearing if possible)
Non operatively treated at 1/2/3 weeks to check alignment and
at 6/12 weeks to check healing Operatively treated
at 1/2/6/12/16 weeks to check healing
Metatarsal, phalangeal fractures and Lisfranc injuries
Non operatively treated at 1/2/3 weeks to check alignment and
at 6 weeks to check healing Operatively treated
at 1/2/6 weeks to check healing
Talar and Calcaneal fractures Non operatively treated at 1/2/3 weeks to check alignment and
at 6/12 weeks to check healing Operatively treated
at 1/2/6/12 weeks to check healing
Wrist and forearm fractures in children (NOT torus fractures) AP and Lateral views
Non operatively treated At 1/2/6 weeks to check alignment and
healing Operatively treated (K wiring / Plating / Nailing)
At 1,2 and 6 weeks to check healing
Wrist fractures in adults AP and Lateral views
Non operatively treated at 1/2/3 weeks to check alignment and
at 6 weeks to check healing Operatively treated
at 1,2 and 6 weeks to check healing
Clavicle fractures AP and 30 degree inclined views
Non operatively treated Children: at 6 & 12 (if necessary) weeks
to check healing Adults: at 1/6/12 weeks
Operatively treated Adults: at 1/6/12 weeks
Proximal Humeral fractures in adults Non operatively treated

Protocol 21
Nurse/Non Medical Requested X-Rays
WAHT-NUR-060 Page 40 of 40 Version 5.5
AP and Lateral views (+Axial if comfortable) At 1/2/6 weeks to check for alignment and healing
Operatively treated At 1/6/12 weeks to check healing
Elbow fractures in children (Supracondylar / lateral and medial condyle / radial neck) AP and Lateral views
Non operatively treated 1/2/6 weeks to check alignment and
healing Operatively treated
1/6 weeks to check alignment and healing
Elbow fractures in adults (Distal humeral, Olecranon, radial head and neck) AP and Lateral views
Non operatively treated 1/2/6/12 weeks to check alignment and
healing Operatively treated
1/6/12 weeks to check alignment and healing
Hand fractures in adults and children AP/Oblique/Lateral views
Non operatively treated At 1/4 weeks to check for alignment and
healing Operatively treated
At 1/4 weeks to check healing
Hip and Femoral fractures (Usually adults) Almost all are operatively treated At 6/12 weeks for all Delayed unions may require further
imaging, check against last letter
1. Appropriate radiographs for any limb or joint may also be ordered if the clinic letter from the
patient’s previous attendance in fracture clinic states ‘X ray on arrival’ with clear instructions
on the limb /joint to be x rayed.
2. In case of any doubt, this should be clarified with a doctor in the fracture clinic.
3. If the radiographer is not happy with the request, clarification should be sought from the
Consultant in the fracture clinic.
4. All staff requesting x-rays must have successfully completed an appropriate training
programme either recognised by the Trust or supported by the Training and Development
team and appropriate clinicians. All practitioners will be registered on the Trust list of
referrers as per IR(ME)R rules.
5. All staff completing the programme will be expected to demonstrate knowledge of:
6. Trust protocol for nursing and non-medical staff requesting x-rays
7. Implications and hazards of radiological examinations
8. Ionising Radiation (Medical Exposure) Regulations- IR(ME)R 2000
9. Locally agreed protocols for the individual referrer
10. Professional accountability and responsibility as outlined in the NMC Scope for Professional
Practice and the individual professions’ Codes of Professional Conduct