nursing and midwifery pressure ulcer prevention and care
TRANSCRIPT

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 1 Review Date: March 2020
Policy Established
Policy Review Period/Expiry
March 2020
Last Updated
June 2018
Policy Manager Caroline McLean
Policy Group Tayside Tissue Viability Network
Sub Group
Nursing and Midwifery
Pressure Ulcer Prevention and Care for Adults in the Home or Homely Setting
This policy does apply to Medical/Dental Staff
UNCONTROLLED WHEN PRINTED
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 2 Review Date: March 2020
Version Control Version Number
Purpose/Change Author Date
1.0 Sue Mackie June 2012
2.0 As a result of actions from complaints/incidents
Sue Mackie January 2014
3.0 Updated national guidance Sue Mackie December 2015
3.1 Change noting when a LAER is to be undertaken
Sue Mackie March 2016
3.2 Updated Policy Caroline McLean June 2018
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 3 Review Date: March 2020
CONTENTS
Page Number
1 Purpose Scope and Definition
4
2 Statement of Policy
6 - 13
3 Responsibility and Organisational Arrangement
13 - 16
4 Key Contacts
16
5 References 17
6 Appendices 18
Appendix 1: Scottish Adapted European Pressure Ulcer Advisory Panel
(EPUAP) and NATVNS, Scotland Pigmented Skin
18 – 19
Appendix 2a: PURA 20 – 21
Appendix 2b: Assessment Chart for Wound Management 22 - 27
Appendix 3: Skin Care Guidance for Reablement/Care at Homes Services 28 - 30
Appendix 4: SSKIN Care Bundle Chart 31 - 32
Appendix 5: NHST Guidelines for the use of Small Devices in the treatment and
prevention of Grade 1 Pressure Ulcer Information
33 - 40
Appendix 6: Mattress Decision Making Tool 41
Appendix 7: Semi Fowler Position – 30 degree tilt 42
Appendix 8: Policy Training Plan 43 - 44
Appendix 9: Policy Approval Checklist 45 - 46
Appendix 10: Equality Impact Assessment 47 - 62
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 4 Review Date: March 2020
PREVENTION AND MANAGEMENT OF PRESSURE ULCERS
1 INTRODUCTION
Pressure Ulcers are caused when an area of skin and/or the tissues below are damaged as a result of being placed under sufficient pressure or distortion to impair the blood supply. Pressure Ulcers are a complex health issue and represent a major burden on not only the individual, but also commissioners and providers of healthcare. They can reduce quality of life, and lead to other life threatening complications for individuals.
2 PURPOSE SCOPE AND DEFINITION
This policy is based on the best available evidence at the time of development and applies to all health care staff within NHS Tayside and all three Health and Social Care Partnership (HSCPs). However when professional clinical judgement overri des this policy the registered nurse/midwife/AHP must document clearly their rationale within the person`s records. Health and social care integration In April 2016, following the implementation of the Public Bodies (Joint Working) (Scotland) Act 2014, 31 Health and Social Care Partnerships were established. The aim of health and social care integration is to:
● To meet the changing needs of our nation, investment, while necessary, must be
matched with reform to drive further improvements in our services. Our services will increasingly face demands from people with long-term conditions needing support from health and social care. These challenges were recognised in the Audit Scotland report, NHS in Scotland 2016, and underline the importance of bringing together the different programmes of work to improve health and social care services.
● Improve the quality and consistency of care for individuals and where appropriate, their families – they should be at the centre of decisions that affect them. They should be given more freedom, choice, dignity and control over their care. Care planning should anticipate an individuals` health and care needs – both by helping those with chronic and other complex conditions to manage their needs more proactively, and focusing on prevention and early intervention approaches to support health throughout people`s lives. This is not always a question of ‘more’ medicine, but making sure that the support fits with, and is informed by, individuals needs. Success should be measured by better outcomes for individuals, not simply on whether processes and systems have been followed. As set out in the Healthcare Quality Strategy for Scotland, it is an approach to health which is rooted in the principles of care that is person-centred, safe and effective.
● provide seamless, collaborative care that enables individuals to stay in their homes or homely setting, where it is safe for them to do so, and ensure that resources are used effectively and efficiently to deliver services that meet the needs of the growing population of people with longer term and often complex needs.
Related Healthcare Improvement Scotland work progra mmes
The Scottish Individuals Safety Programme (SPSP) was established to improve the safety of healthcare and reduce the level of harm experienced by people using healthcare services. SPSP activity supports National Health and Wellbeing Outcome 7: People using Health and Social Care services are safe from harm.
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 5 Review Date: March 2020
As part of the programme, there is an aim to reduce pressure ulcers in hospitals and care homes by 50% by December 2017. This work with care homes is delivered in partnership with Scottish Care and the Care Inspectorate. SPSP will support delivery of this aim by working with care providers to:
● Understand their data in relation to processes and outcomes
● Collaborate with and learn from other care providers, and
● Test and implement interventions that will improve outcomes for people in health and care settings.
The aim of this policy is to :
• Ensure everyone is provided with optimum person centred evidence based pressure ulcer
prevention.
• Standardise the assessment and care of people with/or at risk of developing pressure ulcers.
• Ensure each person has the correct pressure relieving aids to meet their clinical needs.
• Set the minimum standard for the maintenance of knowledge and skills related to pressure area care.
• Comply with Health Improvement Scotland Pressure Ulcer Prevention Standards (2016). • Comply with Health and Social Care Standards- My support, my life (2017)
• Comply with Health and Social Care Partnerships (Joint Working) (Scotland) Act 2014.
These standards have been developed for the prevention and management of pressure ulcers within health and social care services and take into account of the national health and wellbeing outcomes and revised National Health and Social Care Standards, June 2017.
Terminology
Wherever possible, we have incorporated generic terminology which can be applied across all health and social care settings. The term ‘person’ or ‘people’ is used to refer to the person receiving care or support. The term ‘representative’ is used to refer to any person the individual wishes to be involved in their care. This includes, but is not limited to, carers, family (including parents for babies and young children), or independent advocates.
Definition Pressure Ulcers: “A localised injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of pressure, or in combination with shear” (EPUAP, 2014)

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 6 Review Date: March 2020
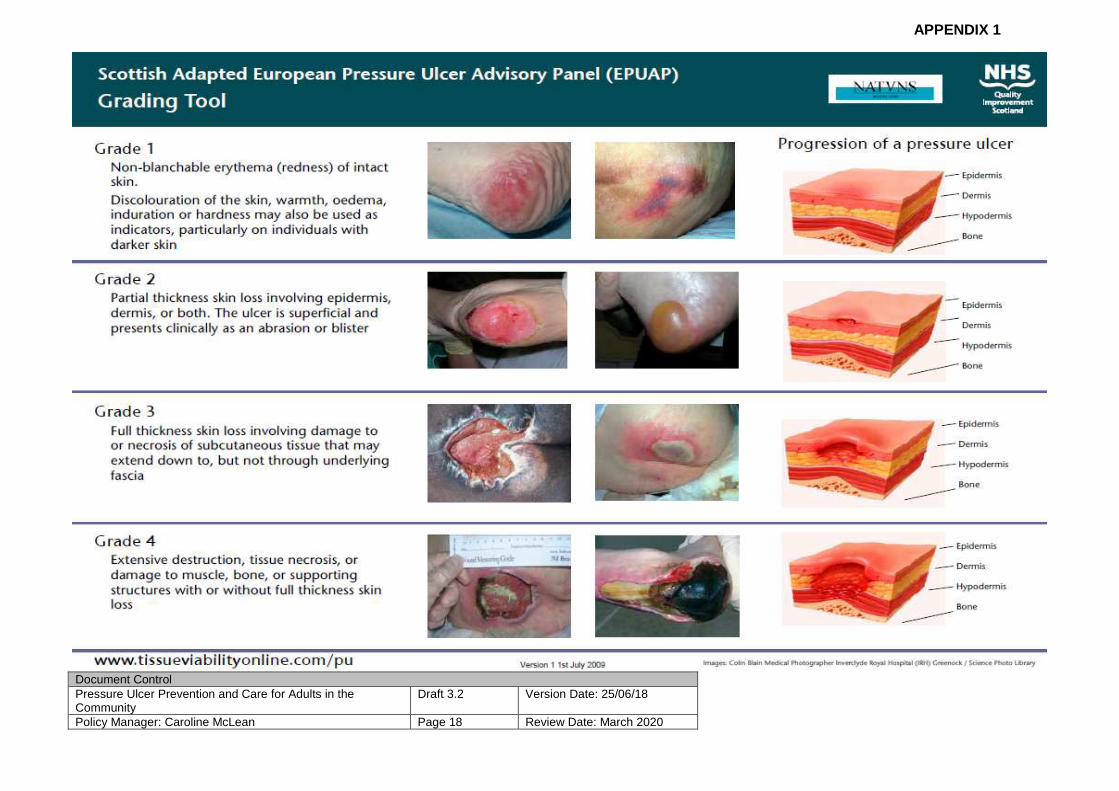
Stage of Pressure Ulcer (also known as grade or cla ssification):
EPUAP`s description of the level of skin tissue damage caused by pressure on a scale of 1-4. See appendix 1 for full classifications.
Avoidable Pressure Ulcer: “Avoidable” means that the person receiving care developed a pressure ulcer and the provider of care did not do one of the following: evaluate the person`s clinical condition and pressure ulcer risk factors; plan and implement interventions that are consistent with the person`s needs and goals; and recognised standards of practice; monitor and evaluate the impact of the interventions; or revise the interventions as appropriate.” (National Individuals Safety Agency, 2010)
Unavoidable Pressure Ulcer: “Unavoidable” means that the person receiving care developed a pressure ulcer even though the provider of the care had evaluated the person`s clinical condition and pressure ulcer risk factors; planned and implemented interventions that are consistent with the person`s needs and goals; and recognised standards of practice; monitored and evaluated the impact of the interventions; and revised the approaches as appropriate; or the individual person refused to adhere to prevention strategies in spite of education of the consequences of non-adherence. (National Individuals Safety Agency, 2010)
3.0 POLICY STATEMENTS
Person Centred Care and Individuals Involvement
All treatment and care carried out by healthcare professionals should take into account individual needs and preferences. People and/or their carers will have the opportunity to make informed decisions about their care and treatment, in partnership with health and social care professionals. Individuals and/or their carer`s who are deemed at risk will be informed (when possible) of their risks and given practical information on how they can help themselves to reduce the risks. Health Professionals are advised to respect and incorporate the knowledge and experience of people who have or have had a pressure ulcer. This advice will be given verbally and supported by the provision of relevant leaflets.
3.1 Assessment
• A complete skin assessment is carried out as part of the risk assessment on first contact with health or social care staff. Care home and social care internal or commissioned services staff may use an initial screening tool in order to escalate concerns to the relevant healthcare professional.
• All individuals will have a Pressure Ulcer Risk Assessment (PURA) carried out at first contact with NHST health professionals using the NHS Tayside PURA THB 620. The use of risk assessment tools should not take precedence over clinical judgement. See appendix 2a
• All individuals who have a PPURA assessment completed will be issued with a pressure ulcer individual leaflet. Pressure Ulcer Leaflet
• Skin assessment should include assessment of all pressure risk areas on the body, inspected for local heat, oedema, induration (hardness) especially in individuals with darkly pigmented skin (EPUAP, NPUAP 2014). Health and social care staff have a duty to review
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 7 Review Date: March 2020
• all relevant risk factors at each contact. If there is a change in circumstances/condition or treatment, the risk will be escalated where appropriate, re-assessed and interventions reviewed and adjusted accordingly (see appendix 2b)
• Risk assessments should be used to determine the plan of care to alleviate factors that cause pressure ulcers. For example, poor mobility, incontinence, poor nutrition and not as a tool to determine the pressure relieving device alone. For incontinent individuals refer to the Scottish Excoriation & Moisture Related Skin Damage Tool found within the NHST Wound Formulary (section 6)
• Following the assessment, if the person is at risk, the appropriate pressure ulcer treatment plan will be identified, discussed and agreed with the person/carer.
Documentation
The following do’s and don’ts should be adhered to when writing in the person`s records/documentation to describe the skin integrity.
• Incorrect Terminology SKIN INTACT RED AREA SKIN BROKEN SKIN Marking
• Correct Terminology
NO RED OR BROKEN AREAS PERSISTENT ERYTHEMA BUT BLANCHING NON BLANCHING ERYTHEMA – GRADE 1 GRADE 2 GRADE 3 GRADE 4 SUB CATEGORIES – UNSTAGEABLE OR SUSPECTED DEEP TISSUE INJURY – PURPLE AREA
– WARM-BOGGY TO TOUCH
• A photograph will be taken (following NHS Tayside Policy – Photography & Video Recordings of Persons for Clinical and Service use) of any pressure ulcer grade 2 and above, or unstageable and suspected deep tissue injury with a dated measurement showing the size of the area (link to policy)
• Any pressure ulcer Grade 2 or above must be reported through the appropriate incident reporting system, e.g. DATIX / MOSIAC
• All pressure ulcers should be documented on the safety cross by the health or social care team providing the persons care.
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 8 Review Date: March 2020
2.3 Prevention
The goals of prevention are: • To identify individuals at risk of developing a pressure ulcer.
• Identify and implement interventions related to the specific risk factors.
• Protect against the adverse effects of pressure, shear and friction.
• Improve the outcomes for people at risk of pressure damage through timely evaluation of nursing/midwifery interventions and educational programmes to healthcare providers’ individuals and families.
2.3.1 Skin Inspection and Grading of Pressure Ulcer s
• The frequency of the Skin inspection should be based on the PPURA assessment and
associated risk factors and documented in the plan of care. The most vulnerable areas of risk for each person; typically heels, sacrum and ischial tuberosities are the areas most affected by friction, pressure or shearing, and from interventions such as anti-embolism stockings, clothing, and other invasive devices such as catheters, IV devices, Naso Gastric tubes, plaster casts and splints
• Skin inspection will be used to decide the re-positioning frequency and this must be stated on the SSKIN assessment chart. If a person does not wish to be re-positioned this should be marked on the SSKIN chart and also documented on the ongoing record, that the person has been informed of the potential consequence of skin damage. (See appendix 4)
• Individuals/carers who are willing and able should be encouraged, following education to inspect their own skin. The use of a mirror is recommended. It may be difficult to assess erythema in persons with darkly pigmented skin, therefore other signs such as heat, oedema, discolouration and induration might be observed.
• NHST guidelines on the use of small devices to prevent pressure ulcers should be used (available on Staffnet and via the Wound Management Formulary) (See appendix 5)
• If a pressure damage is identified this should be referred to the appropriate healthcare professional for further assessment and treatment.
• The grading of any pressure ulcers will be undertaken by a registered practitioner on detection or at first contact. The grade, site, description, measurement, condition and possible cause of the ulcer will be documented on the treatment plan, and treated in accordance with the NHS Tayside Wound Management Formulary.
• The updated Scottish Adapted (2015) European Pressure Ulcer Advisory Panel (EPUAP) grading and moisture lesion tool will be used to assess and document pressure ulcer. A laminated copy of both tools will be held in a resource folder for staff to reference – available to order from Tayside Print - order number THB MR (374)
2.3.2 Bed and Mattresses Allocation
• Do not base the selection of support surface solely on the risk assessment. Clinical
judgement following regular skin inspection is required to check if the current intervention is sufficient to alleviate pressure damage
• Community equipment stores have a variety of mattresses that have different properties to suit individual patient and carer needs and preferences, alongside the logistics of managing and maintaining the equipment in a variety of home settings. Each equipment loan store has
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 9 Review Date: March 2020
a decision making tool to outline the properties of each mattress to enable District Nursing Teams to select the most appropriate device (See Appendix 6)
• Equipment in the loan stores can be supplied for the following risk categories:-
o At risk or low risk – patients who are low risk of developing an ulcer whose current mattress does not provide any pressure relief may benefit from an overlay mattress (some modern mattresses in the home do provided pressure relief).
o High risk – patients who are at high or very high risk of developing a pressure ulcer, but can be repositioned or can/will re position themselves in bed. These patients will require a Reactive Surface – reactive surfaces range from simple foam, gel and non powered, air filled surfaces, through to low-air-loss and air –fluidised beds. By increasing the surface area that supports the body, the applied pressure is lowered. However, unless the patient is repositioned, the pressure remains constant and may still be sufficient to occlude the circulation to the tissue (Phillips et al 2012)
o Very High risk – patients who are at high or very high risk of developing a pressure ulcer, but cannot or will not be repositioned in bed, or they have a grade 3 or 4 pressure ulcer on their sacrum, and spend a large proportion of their day in bed or other high risks such as a paraplegia/sensory impairment. These patients will require an Active surface. These are powered devices designed to periodically redistribute pressure by repeatedly loading and unloading pressure.
• If there is extensive fluid exudate, an air fluidised bed or equivalent flotation type mattress could be used until the amount of seepage is reduced
• The need for any powered mattress must be re-assessed as soon as the individuals’ risk factors decrease to ensure the effective use of resources
• Individuals who require pressure relief should not be nursed on top of the bed covers. The bed linen must be loosely fitted to prevent a hammock effect that would negate the pressure relieving properties of the mattress (see appendix 4)
• For specialised bed rental follow NHS Tayside Policy for and the use and maintenance of beds (link to policy)
2.3.3 Re-Positioning
• All individuals at risk of pressure ulcer development will be re-positioned regularly (NICE
2014), This will be negotiated and agreed with carers or family and documented in care plan. Healthcare staff should also consider the comfort needs of individuals when deciding the repositioning schedule. Repositioning frequency will be determined by the individuals’ tissue tolerance; his/her level of activity and mobility, general medical condition, treatment objectives and assessment of the skin condition at each re-position event. If the individuals’ skin is not responding to the regime, consider increasing the frequency and method of repositioning
• Self Care – individuals who are at risk and who can self care or require prompting will be given advice and a leaflet on actions they can take to reduce the risks. In partnership and agreement with the individuals, they will be afforded the opportunity to check and record their own skin integrity and re-position themselves. The assessor is responsible for documenting this agreement in the nursing/midwifery care plan. Ask individuals to report any pain that may prevent them from re-positioning themselves
• Avoid subjecting the skin to shear and friction forces by using the correct moving and handling techniques. Ensure correct use of equipment such as slings, hoists and glide sheets
• Avoid postures that increase shear and friction such as 90 degree side lying, or semi recumbent position which increases pressure and shear on the sacrum and heels
•
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 10 Review Date: March 2020
• To avoid positioning individuals on bony prominences and maximising weight distribution the 30 degree tilt will be used ensuring the knee section is raised prior to elevating the head end (see appendix 7)
• Whenever possible, do not position individuals onto a body surface that is still reddened from a previous episode of pressure loading (EPUAP, NPUAP 2014)
2.3.4 Seating
• Limit the time an individual is seated in a chair without pressure relief. Individuals at risk of pressure ulcers should not be seated for more than 2 hours at any one time without being re-positioned utilising strategies to relieve pressure such as frequent standing or mobilising. Sitting in a chair increases the risk of pressure ulcer development/deterioration, as pressure is concentrated on one area.
• The ideal seating position maximises weight distribution:
o The back and head support should maintain maximum contact to fully support the individuals back and head
o The individual’s feet must be supported to attain maximum load distribution. If a height adjustable chair is not available a footstool can be used (assess risks of individuals falling or tripping during transfer before use)
o The ideal sitting position is where the hips, knees and feet are at 90 degree angles. This can be achieved with an adjustable chair, or the use of high specification foam cushions. Thighs must be fully supported along their length
• Individuals with grade 1 or 2 pressure ulcers located on their sacrum will have a pressure reducing cushion on the chair. Limit the time an individual is seated in a chair. Individuals with a sacral pressure ulcer should be advised not to be seated for more than 2 hours at any one time without repositioning and utilising strategies to relieve pressure such as frequent standing or mobilising when suitable
• It is not advised for individuals with grade 3/4 ulcers on the sacral area to sit in a chair, as the individuals’ weight cannot be distributed and the focus of pressure is on the pressure ulcer. If possible, individuals remain on the profiling bed and the chair position of the bed utilised. Mobilisation regimes are to be actively encouraged. However, individual choice, their clinical condition and professional judgement need to be exercised to ensure that care is individuals focussed. If it is not possible or the individuals refuses, limit the time to less than one hour and no longer than three times a day
• If pressure areas deteriorate despite the above, seek advice from the Escalation Process for Tissue Viability and Pressure Ulcer Advice (see appendix 8)
• It should be documented in individual notes frequency of pressure relief intervals and advice given to the individual and carers.
2.3.5 Use of Aids
The following will not be used as pressure relieving aids:
• Water filled gloves • Synthetic Sheepskins • Doughnut-type devices
2.3.6 Prevention of Heel Ulcers
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 11 Review Date: March 2020
Individuals at particular risk of developing heel ulcers are individuals with one or a combination of:
• Frailty
• Neuropathy
• Vascular Insufficiency
• Diabetes – All Diabetic individuals will be assessed using the CPR feet guide
• Immobility during surgery
• Critically ill
• Cognitive impairment/Delirium
• Raising the knee section of a profiling bed reduces pressure on the heels and should where possible be utilised on all individuals unless there are clinical contra indications
• Elevate heels completely in such a way as to distribute weight of the leg along the calf without putting all the pressure on the Achilles tendon. The knee should be in slight flexion. A soft pillow along the length of the calf (not under the Achilles tendon) has been shown to be effective (EPUAP 2014)
• Educate individuals and carers to inspect their heels when bathing or dressing and report any redness, blisters or bruises to healthcare provider as soon as possible. Heels should be inspected by a member of the District Nursing Service on a regular basis and frequency should be recorded in patient notes. For inspection the use of a mirror may be useful to see the heels
• Use NHST Guidance On the use of small devices to prevent pressure ulcers, found within section 6 of the wound management formulary (link to section 6)
• The best heel pressure-reducing products reduce pressure, friction, and shear; separate and protect the ankles; maintain heel suspension; and prevent foot drop. They should also be comfortable for the individuals, easy for you to use, and permit re-positioning without increasing pressure in other areas. Remove boots or braces every shift and inspect the individual's skin for redness from the device
• To prevent heel ulcers from friction, use either a silicone pad, or polyurethane foam dressing
• District Nurse should ensure that the Diabetic Handbook is followed for patients with diabetes and patients with vascular disease are regularly monitored to ensure optimum condition of lower limbs
• Individuals with Diabetes who have any wound on the foot should be referred to podiatry
• Individuals with complex foot wounds can also be referred to podiatry for assessment
2.4 Skin and Wound Care Moisture:
• The NHS Tayside Continence guide available on the Tayside Area Formulary (section 20) will be used to assess excoriated skin and moisture lesions
• Only one pad should be used at one time. Body worn pads do not work when flat on a bed and should be used with fitting pants to hold the body worn pads in place
• The ongoing nursing record will contain evidence that the advice of a continence advisor was sought where continence management products are compromised by pressure ulcer prevention strategies
•

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 12 Review Date: March 2020
• Soap and water should not be used on individuals with or at risk of excoriation. A skin cleansing agent will be used following episodes of incontinence. (refer to section 20 Tayside Area Formulary), Skin cleansers that are PH neutral are acceptable. This needs to be discussed with carers. Do not vigorously rub the skin
• Barrier creams and sprays will be used to prevent skin damage, however must be used sparingly as per manufacturers instruction to prevent blocking the absorbency of pads
• For individuals with severe diarrhoea, Faecal collectors can be used – follow NHST faecal management systems guidelines available on the Intranet
Dry Skin : • Non-perfumed moisturisers are used at least twice daily on individuals with dry skin; apply
sparingly to prevent clogging, as dry skin is a significant and independent risk factor for pressure ulcer development (EPUAP, NPUAP 2014). The NHS Tayside continence skin care guideline (2014) suggests suitable moisturisers to be used to treat dry areas
Wound Care : • The NHS Tayside Wound Management Formulary (available on the formulary tab on the
home page on Staffnet) will be utilised to decide the most appropriate dressing • A specialist wound referral pathway is available in the formulary tab on staffnet
• District nurses will use the NHST wound chart (THB MR 609) to document wound assessment and interventions.
• Products that promote a moist wound environment are used for all skin damage unless contraindicated by the individual’s condition
• Pressure Ulcers of grade 3 or 4, or unstageable that do not respond to treatments following four weeks of the recommendations within the wound formulary, and following all aspects of this policy should be referred to the most appropriate speciality; Vascular, or Plastic Surgery for further advice
• All health records must note the site, condition and dressing utilised and will demonstrate evidence of ongoing assessment and skin and wound care using the THB MR 609 form
• Guidelines on the management of Diabetic Foot Ulceration can be obtained from the NHS Tayside Diabetes MNC Handbook and the NHST Wound Management Formulary section 15
2.5 Discharge – Transfer
The nurse responsible for arranging the discharge/transfer of individuals with a pressure ulcer or at risk of developing an ulcer will ensure that the receiving nurse/hospital/area has written information on:
• Individuals’ risk status, treatment plan A, B or C • Whether the ulcer was present on admission or hospital acquired • DATIX completed • Grade, description, size and site of ulcer • Nursing intervention, such as dressings and re positioning regime.
Complex cases will be discussed with the District Nursing team and if appropriate arrange a hospital visit.

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 13 Review Date: March 2020
For individuals who are at risk or have an established ulcer and require long distance ambulance transfer, the ambulance staff must be informed of the need for particular care with moving and handling and the need for the individuals to provide some change in their position at least 6 hourly for those at risk, and at least 4 hourly for those at high risk.
2.6 Education and Training
Each provider of Pressure Ulcer Care - :
Line managers are required to ensure that evidence of yearly update’s and education for all assessors and providers pressure ulcer care and prevention by
• Completing the Learn Pro Module (previously NES resource pack) every 3 years available through Staffnet and thereafter; evidence of a yearly competency assessment recorded within the clinical area and supported by the department link nurse
• Each area will have a plan in place to ensure all staff have appropriate training plans in place. Yearly competency assessment should be downloaded and available for completion at an allocated time to suit the business need of each Individual area.
3 RESPONSIBILITY AND ORGANISATIONAL ARRANGEMENTS
3.1 Responsibility
• People will be equal partners with their health and social care professionals, they will work together to help older people and those with more complex needs receive the right support at the right time, and where possible, live well and independently.
• People will be supported to have confidence, knowledge, understanding and skills to live well, on their own terms; with whatever conditions they have access to greater support from a range of services beyond health, with a view to increasing their resilience and reinforcing their whole wellbeing.
• Maintain accurate records of assessment intervention and evaluation in accordance with NHS Tayside standards for record keeping and NHS Tayside Community Nursing Guidance.
• Local policy and guidelines are supported by all care giving staff to ensure patient centred care i.e. Skin Care Policy for Reablement and Care at Home. (see appendix 5)
3.2 Accountability and Governance
Pressure ulcer prevention is complex, as ulcers are often caused by a combination of factors which require a multidisciplinary and holistic approach to a person`s care. Continuity of care is crucial for success in preventing pressure damage in the “at risk” person. Risk factors such as poor nutrition, previous history of ulcers, diabetes, poor posture, mobility and the presence of co-morbidities need to be included in the prevention care plan/pathway and where necessary referred to the appropriate discipline so that appropriate and timely interventions can be implemented to help minimise those risk factors. All staff disciplines have a role to play in pressure ulcer prevention, ensuring a consistent and standardised approach to ensuring concordance to Essence of Care Standards within their care setting.
• Each individual nurse/midwife is accountable for making evidence based assessment and
decisions in accordance with this policy
• Community staff will ensure that when delegating care to Health Care Assistants, they ensure that Health Care Assistants understand this policy and implications for their practice.
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 14 Review Date: March 2020
• They have the necessary knowledge and skills relating to pressure ulcer observation, re-positioning, 30 degree tilt, cleansing and moisturising agents and the required communication and documentation required for the care plan
• The Line manager will keep a record of nurses who have read the policy and updated their knowledge yearly
• Each clinical area will implement and monitor pressure ulcer management processes and outcomes using Clinical Quality Indicators
• Grade 2 pressure ulcers and above that have developed in the clinical area will be reported through the ward safety Cross, and a Datix/MOSIAC adverse event management system completed
• A Local Adverse Event Review will be carried out by the Head of Nursing/Manager for all Grade 3 or 4 pressure ulcers that develop under the care of NHS Tayside staff.
Duty of Candour
The purpose of the new duty of candour provisions is to support the implementation of consistent responses across health and social care providers when there has been an unexpected event or incident that has resulted in death or harm, that is not related to the course of the condition for which the person is receiving care.
The principles of candour already inform the approach that is taken in many organisations. The professional duty currently applies to many health and social care professionals across Scotland as this is a part of the requirements of their practice by their professional regulators.
Key Principles:
• Providing health and social care services is associated with risk and there are unintended or unexpected events resulting in death or harm from time to time.
• When this happens, people want to be told honestly what happened, what will be done in response, and to know how actions will be taken to stop this happening again to someone else in the future.
• There is a need to improve the focus on support, training and transparent disclosure of learning to influence improvement and support the development of a learning culture across services.
• Candour is one of a series of actions that should form part of organisational focus and commitment to learning and improvement.
• Transparency, especially following unexpected harm incidents is increasingly considered necessary to improving the quality of health and social care.
• Being candid promotes accountability for safer systems, better engages staff in improvement efforts, and engenders greater trust in individuals and service users.
3.3 Clinical Effectiveness - Standards and Guidel ines
During 2016, the implementation of the Public Bodies (Joint Working) (Scotland) Act 2014 the publication of the Scottish Government`s National Clinical Strategy and the chief Medical Officer`s annual report 2015-16, Realising Realistic Medicine all built upon the 2020 vision and the Quality Strategy. The Scottish Governments recently published Health and Social Care Plan clearly sets out changes to the environment in which we operate and the ambition to move significant resources from institutional models of care provision towards services that support people to live longer, healthier lives at home or in a homely setting. Making Care Better – Better
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 15 Review Date: March 2020
Quality Health and Social Care for Everyone in Scot land. A Strategy for supporting better care in Scotland 2017 – 2022 Health Improvement Sco tland
Five Strategic Priorities are:
• Enable people to make informed decisions about their own care and treatment
• Help Health and social care organisations to redesign and continuously improve services
• Provide evidence and share knowledge that enables people to get the best out of the services they use and help services to improve
• Provide and embed quality assurance that gives people confidence in the quality and sustainability of services and supports providers to improve
• Make best use of all resources
What is a standard?
• A standard is a statement of an expected level of service which demonstrates delivery of person-centred, safe and effective healthcare, and promotes understanding, comparison and improvement of that care
• Standards can be used for National consistency and/or for local improvement (Health Improvement Scotland September 2016)
Health Improvement Scotland introduced six performance standards for the prevention and management of pressure ulcers and can be used to reinforce national consistency and drive improvement within health and social care services responsible for pressure ulcer care, the standards are: Standard 1: Leadership and governance The organisation demonstrates leadership and a commitment to the prevention and management of pressure ulcers. Standard 2: Education, training and information The organisation demonstrates commitment to the education and training of staff involved in the prevention and management of pressure ulcers, appropriate to roles and workplace setting.
Information and support is available for people at risk of, or identified with, a pressure ulcer, and/or their representatives
Standard 3: Assessment of risk for pressure ulcer d evelopment
An assessment of risk for pressure ulcer development is undertaken as part of initial admission or referral, and informs care planning.
Standard 4: Reassessment of risk
Regular reassessment of risk for pressure ulcer development or further damage to an existing pressure ulcer is undertaken to ensure safe, effective and person-centred care
Standard 5: Care planning for prevention and treatm ent
A person-centred care plan is developed and implemented to reduce the risk of pressure ulcer development and to manage any existing pressure ulcers
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 16 Review Date: March 2020
Standard 6: Assessment, grading and care planning f or identified pressure ulcers
People with an identified pressure ulcer will receive a person-centred assessment, a grading of the pressure ulcer and an individualised care plan
3.4 In Summary:
The information, guidance and examples you need to develop best achievable practice in the prevention and management of pressure ulcers.
• a basis for developing and improving care • an educational tool for students at pre and post registration level and to stimulate learning
amongst teams. (see appendix 8) • helps promote effective interdisciplinary team working • helps determine whether a quality service is being provided • stimulates ideas and priorities for nursing research, and • stimulates ideas and priorities for continuous improvement.
Best practice statements address an area of care where there is variation in practice across Scotland since there is a limited amount of robust evidence available. They attempt to incorporate professional consensus in the absence of a rigorous evidence base.
4. KEY CONTACTS
Caroline McLean Prescribing Support Nurse (Registered Nurse) Chair: NHS Tayside Tissue Viability Network Realistic Medicine East Day Home Kings Cross Clepington Road Dundee DD3 8EA [email protected]
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 17 Review Date: March 2020
5. REFERENCES European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Prevention and Treatment of pressure: quick reference guide. Washington DC: National Pressure Ulcer Advisory Panel; 2014 Heyneman A, Beele H, Vanderwee K, Dehloor T, 2008. A Systematic Review of the use of Hydrocolloids in the Treatment of Pressure Ulcers. Journal of Clinical Nursing, 17 (9) p p. 1164-1173 (10). Blackwell Publishing. NATVNS Scotland. 2008 Tissue Viability Toolkit. NHS QIS Best Practice Statement 2005. The Treatment/Management of Pressure Ulcers. www.nhshealthquality.org NHS QIS Best Practice Statement 2005 and Revised Statement 2009 Pressure Ulcer Prevention http://www.nhshealthquality.org/ NHS Education for Scotland . The Prevention & Management of Pressure Ulcers –An Educational Workbook for Healthcare Staff 2009.Edinburgh NICE clinical guidelines 179 April 2014 Pressure Ulcers: Prevention and management of Pressure http://www.nice.org.uk/guidance/cg179/resources/guidance-pressure-ulcers-prevention-and-management-of-pressure-ulcers-pdf Health Improvement Scotland 2016, Standards for prevention and management of pressure ulcers, http://www.healthcareimprovementscotland.org/our_work/patient_safety/tissue_viability_resources/pressure_ulcer_standards.aspx Please note: that references preceding 2007 have be en archived and are still available from previous versions
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 18 Review Date: March 2020
APPENDIX 1
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 19 Review Date: March 2020
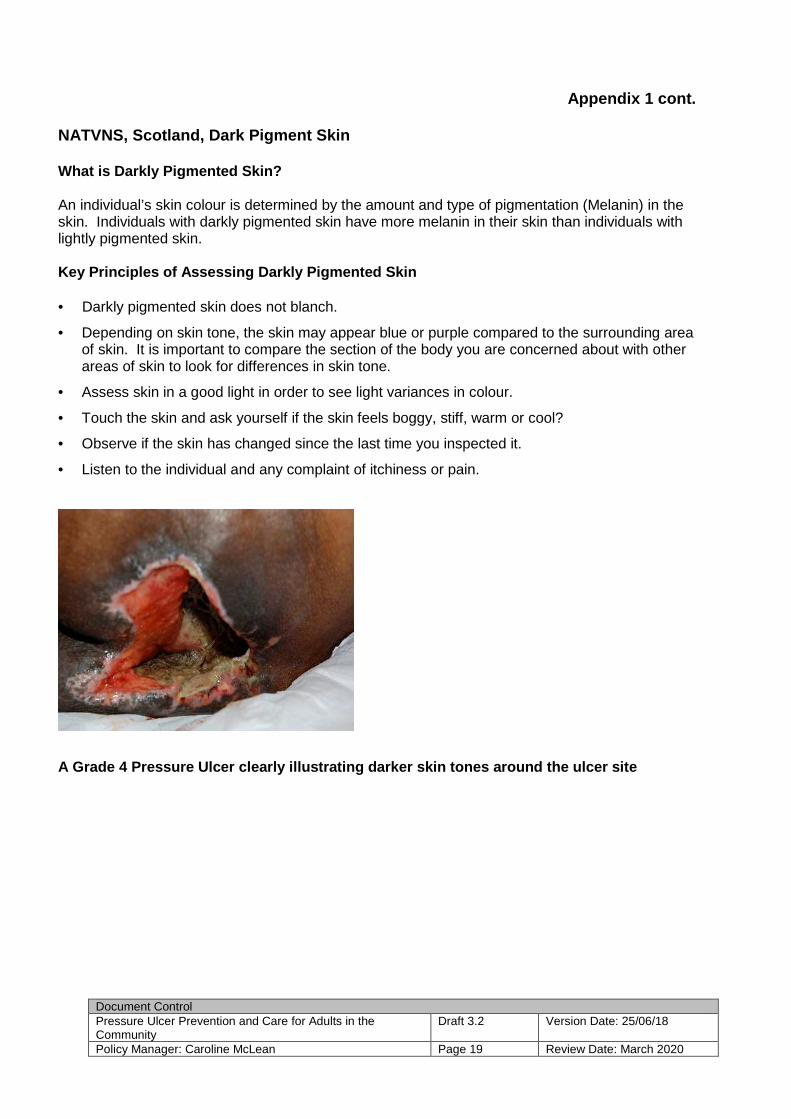
Appendix 1 cont. NATVNS, Scotland, Dark Pigment Skin What is Darkly Pigmented Skin? An individual’s skin colour is determined by the amount and type of pigmentation (Melanin) in the skin. Individuals with darkly pigmented skin have more melanin in their skin than individuals with lightly pigmented skin. Key Principles of Assessing Darkly Pigmented Skin • Darkly pigmented skin does not blanch.
• Depending on skin tone, the skin may appear blue or purple compared to the surrounding area of skin. It is important to compare the section of the body you are concerned about with other areas of skin to look for differences in skin tone.
• Assess skin in a good light in order to see light variances in colour.
• Touch the skin and ask yourself if the skin feels boggy, stiff, warm or cool?
• Observe if the skin has changed since the last time you inspected it.
• Listen to the individual and any complaint of itchiness or pain.
A Grade 4 Pressure Ulcer clearly illustrating darke r skin tones around the ulcer site

The following 6 questions must be completed with AL L patients within 6 hours of admission or for community staff, on the day of admission to the ser vice. Re-assessment required if patient condition
changes including the day of major surgery
(Please write Yes/No below)
1 Requires assistance and or aids to regularly relieve any pressure area (includes heels/head etc). Cannot or will not move independently or reposition on 3 areas, OR on an operating table for > 2hrs?
2 Incontinent - urine or faeces in contact with the skin?
3 BMI <18.5 or > 40 ? 4 Any Pressure ulcer or a previous pressure ulcer? 5 Compromised skin due to Frailty, Diabetes, Neurological deficit, Vascular
insufficiency, Cognitive impairment?
6 In your clinical judgement is the patient at risk despite scoring ‘no’ on the above?
Date Time Initial If Yes to any question, raise the PUP treatment plan and carry out a full assessment within 6 hours of admission (or day of admission to the DN service). Treatment plan B or C commenced ( circle) Date_____________ If No to all questions re-assess each shift, or if a change in clinical condition then record on traffic lights and implement. Treatment plan A, commenced Y / N Date____________ DATE & TIME
Pressure ulcer present on admission Y N from where? ____________
Raise a wound care plan for all ulcer stages 2-4 ( see last page) Report all grade 2 and above ulcers that develop in your area on Datix Date ulcer identified
Site of ulcer
Grade
If the same ulcer progressed to a higher grade state date and grade
DATIX ref. no if Developed in hospital
Photograph taken
Patient information leaflet given
RN signature
THB 620
WRITE OR ATTACH LABEL Surname…………………………Sex…………. Forename………………………………….. DOB and CHI………………………………
HOSPITAL/AREA............................................ WARD/AREA……………………………….
Pressure Ulcer Risk Assessment (PURA)
Appendix 2a
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 21 Review Date: March 2020
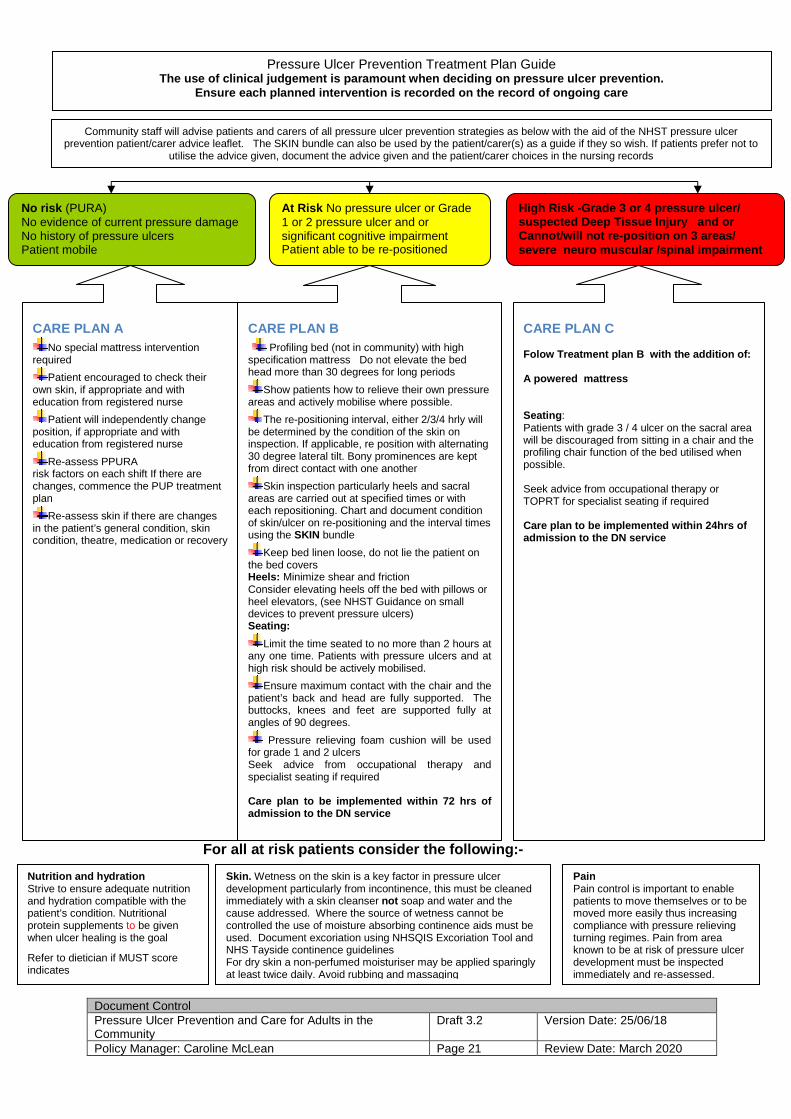
Pressure Ulcer Prevention Treatment Plan Guide The use of clinical judgement is paramount when dec iding on pressure ulcer prevention.
Ensure each planned intervention is recorded on the record of ongoing care
At Risk No pressure ulcer or Grade 1 or 2 pressure ulcer and or significant cognitive impairment Patient able to be re-positioned
Community staff will advise patients and carers of all pressure ulcer prevention strategies as below with the aid of the NHST pressure ulcer prevention patient/carer advice leaflet. The SKIN bundle can also be used by the patient/carer(s) as a guide if they so wish. If patients prefer not to
utilise the advice given, document the advice given and the patient/carer choices in the nursing records
CARE PLAN A No special mattress intervention
required
Patient encouraged to check their own skin, if appropriate and with education from registered nurse
Patient will independently change position, if appropriate and with education from registered nurse
Re-assess PPURA risk factors on each shift If there are changes, commence the PUP treatment plan
Re-assess skin if there are changes in the patient’s general condition, skin condition, theatre, medication or recovery
CARE PLAN B Profiling bed (not in community) with high specification mattress Do not elevate the bed head more than 30 degrees for long periods
Show patients how to relieve their own pressure areas and actively mobilise where possible.
The re-positioning interval, either 2/3/4 hrly will be determined by the condition of the skin on inspection. If applicable, re position with alternating 30 degree lateral tilt. Bony prominences are kept from direct contact with one another
Skin inspection particularly heels and sacral areas are carried out at specified times or with each repositioning. Chart and document condition of skin/ulcer on re-positioning and the interval times using the SKIN bundle
Keep bed linen loose, do not lie the patient on the bed covers Heels: Minimize shear and friction Consider elevating heels off the bed with pillows or heel elevators, (see NHST Guidance on small devices to prevent pressure ulcers) Seating:
Limit the time seated to no more than 2 hours at any one time. Patients with pressure ulcers and at high risk should be actively mobilised.
Ensure maximum contact with the chair and the patient’s back and head are fully supported. The buttocks, knees and feet are supported fully at angles of 90 degrees.
Pressure relieving foam cushion will be used for grade 1 and 2 ulcers Seek advice from occupational therapy and specialist seating if required Care plan to be implemented within 72 hrs of admission to the DN service
CARE PLAN C Folow Treatment plan B with the addition of: A powered mattress Seating : Patients with grade 3 / 4 ulcer on the sacral area will be discouraged from sitting in a chair and the profiling chair function of the bed utilised when possible. Seek advice from occupational therapy or TOPRT for specialist seating if required Care plan to be implemented within 24hrs of admission to the DN service
No risk (PURA) No evidence of current pressure damage No history of pressure ulcers Patient mobile
Nutrition and hydration Strive to ensure adequate nutrition and hydration compatible with the patient’s condition. Nutritional protein supplements to be given when ulcer healing is the goal
Refer to dietician if MUST score indicates
Skin. Wetness on the skin is a key factor in pressure ulcer development particularly from incontinence, this must be cleaned immediately with a skin cleanser not soap and water and the cause addressed. Where the source of wetness cannot be controlled the use of moisture absorbing continence aids must be used. Document excoriation using NHSQIS Excoriation Tool and NHS Tayside continence guidelines For dry skin a non-perfumed moisturiser may be applied sparingly at least twice daily. Avoid rubbing and massaging
Pain Pain control is important to enable patients to move themselves or to be moved more easily thus increasing compliance with pressure relieving turning regimes. Pain from area known to be at risk of pressure ulcer development must be inspected immediately and re-assessed.
For all at risk patients consider the following:-
High Risk -Grade 3 or 4 pressure ulcer/ suspected Deep Tissue Injury and or Cannot/will not re-position on 3 areas/ severe neuro muscular /spinal impairment
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 22 Review Date: March 2020
Assessment Chart for Wound Management
This booklet is to be completed for ONE wound only, Add individual inserts of Formal Wound Assessment & Wound Treatment Plan & Evaluation of Care if required
Consider f actors which could delay healing: DATIX Reference no. Immobility/Poor Nutrition/Diabetes/Incontinence/Respiratory/Circulatory Disease Anaemia/Medication/Wound Infection/Inatropes/Anti-Coagulants/Oedema/Steroids/ Chemotherapy
Pain :Assess using recognised pain assessment tool Is a symptom associated with actual or potential tissue injury, and assessment of pathophysiology of wound pain is prerequisite to treating it.
Allergies & Sensitivities
Body Diagram Front Back
Mark location with ‘X’
Feet Diagram
Right Left
Mark location with ‘X’ (refer to referral Pathway )
Table 1 Tick and specify below
Table 2 Date referred Initials
Leg Ulcer Dermatology Surgical Wound Plastics Foot Ulcer Podiatrist Pressure Ulcer (state grade)
Vascular
Other & specify Physiotherapist Dietitian
Has Ankle Brachial Pressure Index (ABPI) been obtai ned? (please circle below)
RIGHT LEG LEFT LEG YES NO N/A APBI result YES NO N/A APBI result Date obtained Initials Date obtained Initials
WRITE, IMPRINT OR ATTACH LABEL Surname ……………….... CHI No ….………….. Forenames ………………… Sex………………….. DoB ………………..
Appendix 2b

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 23 Review Date: March 2020
Initial Wound Assessment Complete on initial assessment and thereafter compl ete at every dressing change
Date of Assessment
Specify type of wound:
Wound Dimensions – Enter Size (refer to NHS Tayside Wound Guidance & Wound Manag ement Formulary) Length (cm) Width (cm) Depth (cm) Or trace wound circumference Photography obtained (enter Yes/No) Tissue type on wound bed Tick all relevant boxes &(refer to NHS Tayside Wound Guidance & Wound Management Formulary) Necrotic (Black) (picture 1)
Sloughy (Yellow/Green) (picture 2)
Granulating (Red) (picture 3)
Epithelialising (Pink) (picture 4)
Overgranulation (Red) (picture 5)
Wound exudate levels/ type Tick all relevant boxes & (refer to NHS Tayside Wou nd Guidance & Wound Management Formulary) Low Moderate High * Peri -wound skin Tick all relevant boxes & (refer to NHS Tayside Wou nd Guidance & Wound Management Formulary) Macerated (White) Oedematous * Erythema (Red)* Excoriated (Red) Fragile Dry/scaly Healthy/intact Signs of Infection : Yes/No, if yes complete below & (refer to NHS Tayside Wound Guidance & Wound Management Formulary on “© Management Of Suspected Infection in Chronic Wounds " Heat * New slough/necrosis(deteriorating wound bed)* Increasing pain* Increasing exudate* Increasing odour* Swab as per above guidance © Treatment objectives Tick all relevant boxes & (refer to NHS Tayside Wou nd Guidance & Wound Management Formulary) Debridement Absorption Hydration Protection Palliative / conservative Reduce bacterial load Initials Re-assessment date
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 24 Review Date: March 2020
Wound Treatment Plan and Evaluation of Care
To be completed when treatment or dressing type / regime altered
Date Cleansing Method
Dressing Choice Frequency
Evaluation and Healing Progress of Wound Rationale for change of dressing type (refer to NH S Tayside Wound Guidance/WMF)
Initials
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 25 Review Date: March 2020
To be completed when treatment or dressing type / regime altered
Date Cleansing Method
Dressing Choice Frequency
Evaluation and Healing Progress of Wou nd Rationale for change of dressing type (refer to NH S Tayside Wound Guidance/WMF)
Initials
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 26 Review Date: March 2020
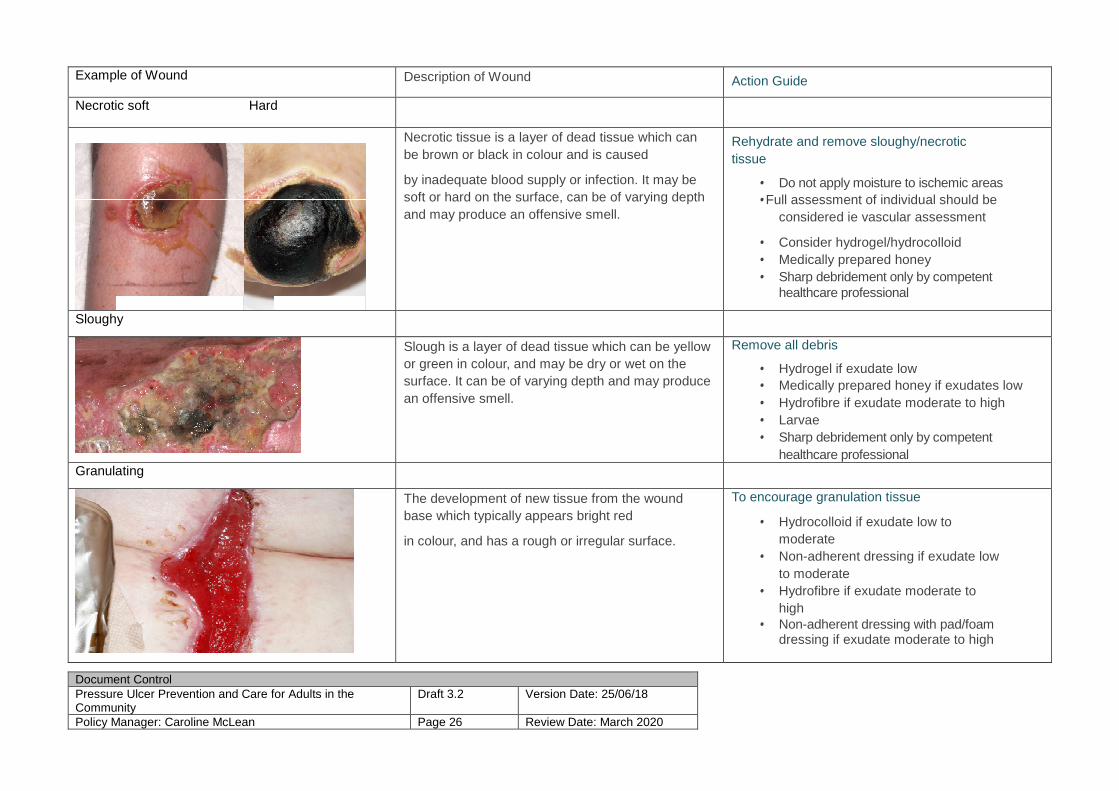
Example of Wound Description of Wound Action Guide
Necrotic soft Hard
Necrotic tissue is a layer of dead tissue which can be brown or black in colour and is caused
by inadequate blood supply or infection. It may be soft or hard on the surface, can be of varying depth and may produce an offensive smell.
Rehydrate and remove sloughy/necrotic tissue
• Do not apply moisture to ischemic areas • Full assessment of individual should be
considered ie vascular assessment
• Consider hydrogel/hydrocolloid • Medically prepared honey • Sharp debridement only by competent
healthcare professional
Sloughy
Slough is a layer of dead tissue which can be yellow or green in colour, and may be dry or wet on the surface. It can be of varying depth and may produce an offensive smell.
Remove all debris
• Hydrogel if exudate low • Medically prepared honey if exudates low • Hydrofibre if exudate moderate to high • Larvae • Sharp debridement only by competent
healthcare professional Granulating
The development of new tissue from the wound base which typically appears bright red
in colour, and has a rough or irregular surface.
To encourage granulation tissue
• Hydrocolloid if exudate low to moderate
• Non-adherent dressing if exudate low to moderate
• Hydrofibre if exudate moderate to high
• Non-adherent dressing with pad/foam dressing if exudate moderate to high
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 27 Review Date: March 2020
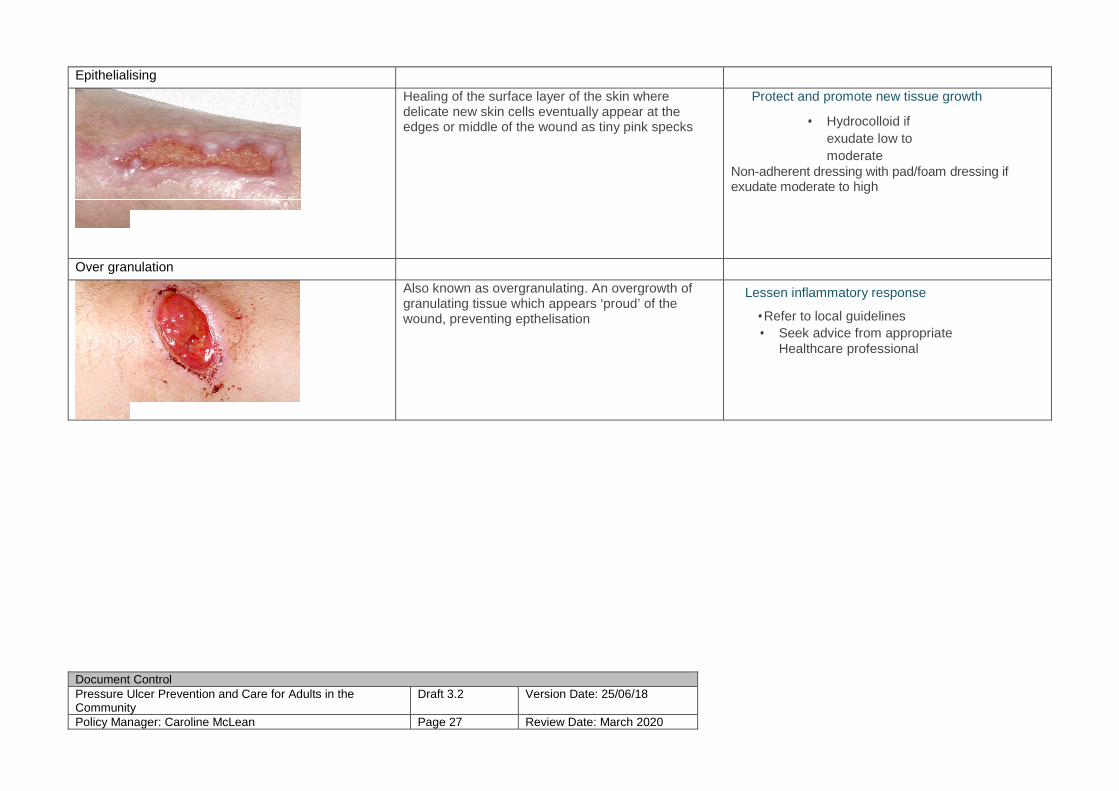
Epithelialising
Healing of the surface layer of the skin where delicate new skin cells eventually appear at the edges or middle of the wound as tiny pink specks
Protect and promote new tissue growth
• Hydrocolloid if exudate low to moderate
Non-adherent dressing with pad/foam dressing if exudate moderate to high
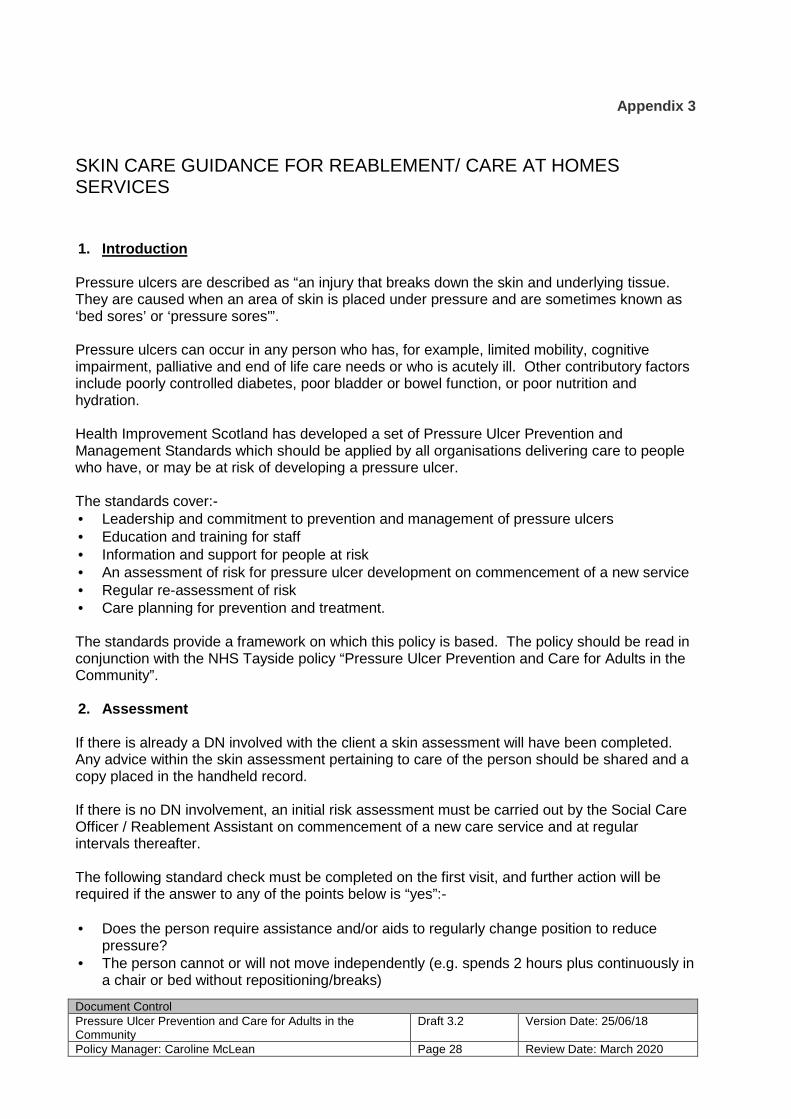
Over granulation
Also known as overgranulating. An overgrowth of granulating tissue which appears ‘proud’ of the wound, preventing epthelisation
Lessen inflammatory response
• Refer to local guidelines • Seek advice from appropriate
Healthcare professional
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 28 Review Date: March 2020
Appendix 3
SKIN CARE GUIDANCE FOR REABLEMENT/ CARE AT HOMES SERVICES
1. Introduction Pressure ulcers are described as “an injury that breaks down the skin and underlying tissue. They are caused when an area of skin is placed under pressure and are sometimes known as ‘bed sores’ or ‘pressure sores'”. Pressure ulcers can occur in any person who has, for example, limited mobility, cognitive impairment, palliative and end of life care needs or who is acutely ill. Other contributory factors include poorly controlled diabetes, poor bladder or bowel function, or poor nutrition and hydration. Health Improvement Scotland has developed a set of Pressure Ulcer Prevention and Management Standards which should be applied by all organisations delivering care to people who have, or may be at risk of developing a pressure ulcer. The standards cover:- • Leadership and commitment to prevention and management of pressure ulcers • Education and training for staff • Information and support for people at risk • An assessment of risk for pressure ulcer development on commencement of a new service • Regular re-assessment of risk • Care planning for prevention and treatment. The standards provide a framework on which this policy is based. The policy should be read in conjunction with the NHS Tayside policy “Pressure Ulcer Prevention and Care for Adults in the Community”. 2. Assessment If there is already a DN involved with the client a skin assessment will have been completed. Any advice within the skin assessment pertaining to care of the person should be shared and a copy placed in the handheld record. If there is no DN involvement, an initial risk assessment must be carried out by the Social Care Officer / Reablement Assistant on commencement of a new care service and at regular intervals thereafter. The following standard check must be completed on the first visit, and further action will be required if the answer to any of the points below is “yes”:- • Does the person require assistance and/or aids to regularly change position to reduce
pressure? • The person cannot or will not move independently (e.g. spends 2 hours plus continuously in
a chair or bed without repositioning/breaks)
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 29 Review Date: March 2020
• Incontinent of urine or faeces in contact with the skin? • Concerns around low weight or nutrition? • Has a pressure ulcer or history of pressure ulcer?
In addition, where possible, the SCO / RA should undertake a skin inspection, paying particular attention to pressure points and/or bony prominences, to include heels, ankles, bottom, sacrum, knees, elbows, ears and back of head. This should be done sensitively, with the person's knowledge and full participation where possible. Dignity and privacy should be respected at all times when re-positioning or assisting with personal care. If the person declines a skin inspection this should also be clearly documented in the handheld record.
• Any areas of concern identified should be documented in the hand held record, and reported to the coordinator. A referral should be made to the District Nursing service the same day.
The District Nurse will undertake a professional nursing assessment in accordance with NHS Tayside policy “Pressure Ulcer Prevention and Care for Adults in the Community” and provide a written care plan of necessary prescribed care and treatment and delegated care to the carer/agency. • Where there is delegated care from the District Nurse this will be documented in the NHST
care plan and shared with relevant agencies. The district nurse is the responsible and accountable clinical practitioner in relation to the pressure ulcer care of patients known to them and must act in line with their NMC Code in terms of delegation of care.
• The district nurse will review the care put in place as per the NHS Tayside policy “ Pressure Ulcer Prevention and Care for Adults in the Community and advise carers of updated plan
• Where necessary a social work review will be carried out to ensure changes to care delivery are incorporated into the Generic Personal Outcomes Plan (POP). Thereafter daily skin inspections should be carried out by the social care officer/RA staff and recorded. Any areas of concern or changes in the person's skin should be reported to the District Nursing service on the same day, or next day if after 5pm.
3. Prevention – Good Practice All people receiving a Reablement or Care at Home service should be encouraged to check their own skin every day, with reference to the Health Improvement Scotland Preventing Pressure Ulcers guide in their HHR.
Clients should be encouraged and supported to move regularly within their capabilities, and at least every two hours. Always use a Reablement approach. Consider using the chair exercises in the Preventing Pressure Ulcers Guide. Staff who are trained, may consider utilising strength and balance exercises.
Nutrition ; Good nutritional intake is crucial. If a client is not eating well or drinking adequate fluids, this should ALWAYS be recorded in the handheld record AND reported to the Line Manager or Key Worker. Advice should always be sought from the DN and/or GP, if this continues for more than a day. Skin : Moisture, specifically from incontinence, must be cleansed with a suitable skin cleanser. Do not use soap and water and skin should be dried carefully with a soft clean towel.
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 30 Review Date: March 2020
For dry skin a non perfumed moisturiser should be used sparingly WITHOUT rubbing and massaging. • A referral for continence advice / equipment can be sought through the DN. Pain – If a person's pain is poorly controlled, their movement may be impaired and risk of loss of skin integrity will increase. • Refer to the GP or DN on the same day 4 Further Information and Action From mid 2017 Coordinators and Supervisors in Reablement and Care at Home will be trained in delivering pressure ulcer prevention and pressure care management training to staff in the community. All SCOs and Reablement Assistants will be expected to undertake this as part of their basic training and will also receive reminders and updates through supervision, weekly newsletter, team meetings etc. Staff who have a particular interest will be offered the opportunity to become skin champions for their locality and will be supported to access more in-depth online training. All our clients now have the “Preventing Pressure Ulcers” guide in their handheld record and copies can be downloaded from the Health Improvement Scotland website in the Patient Safety section (tissue viability). Staff should be familiar with the leaflet and the advice there-in. Staff should highlight the leaflet to service users who may be at risk, and their families/carers. Being part of an integrated service provides an opportunity for health and social care services to work together much more effectively than in the past. Communication is key and any concerns with regard to skin integrity should ALWAYS not only be recorded in the handheld record, but also discussed with the line manager and referred on to a health professional as appropriate.
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 31 Review Date: March 2020
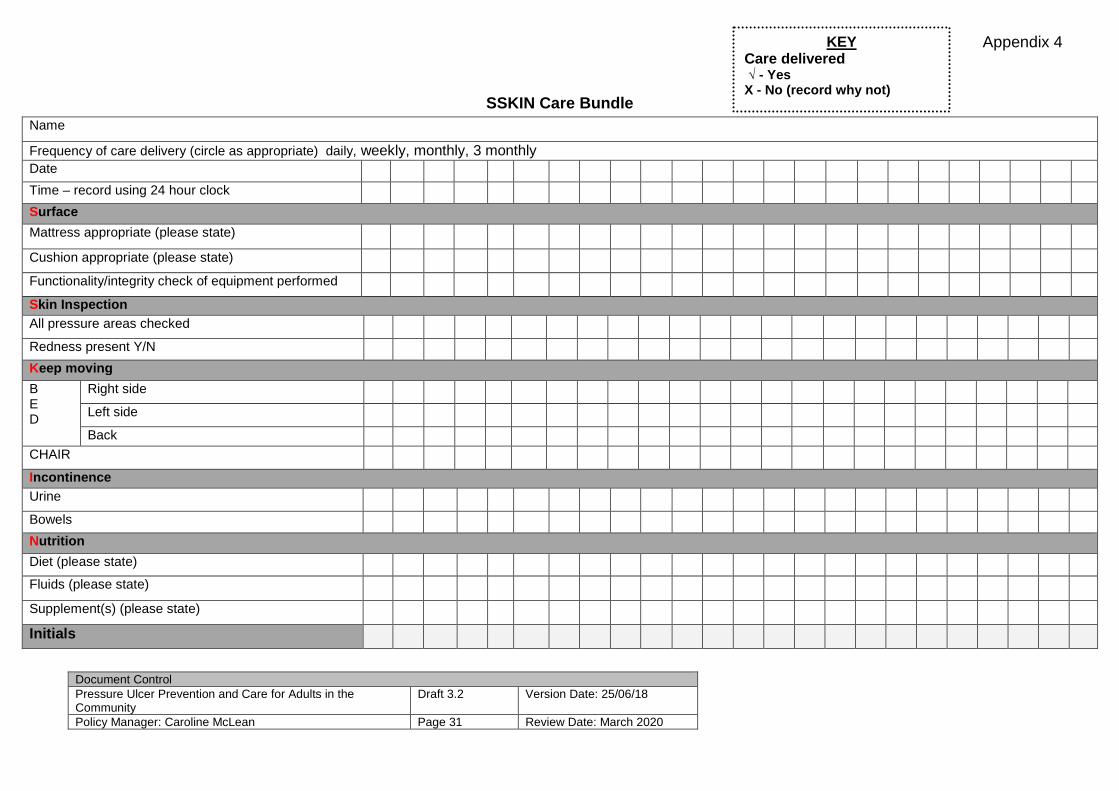
SSKIN Care Bundle
Name
Frequency of care delivery (circle as appropriate) daily, weekly, monthly, 3 monthly Date
Time – record using 24 hour clock
Surface
Mattress appropriate (please state)
Cushion appropriate (please state)
Functionality/integrity check of equipment performed
Skin Inspection All pressure areas checked
Redness present Y/N
Keep mo ving
B E D
Right side
Left side
Back
CHAIR
Incontinence Urine
Bowels
Nutrition
Diet (please state)
Fluids (please state)
Supplement(s) (please state)
Initials
KEY Care delivered √ - Yes X - No (record why not)
Appendix 4
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 32 Review Date: March 2020
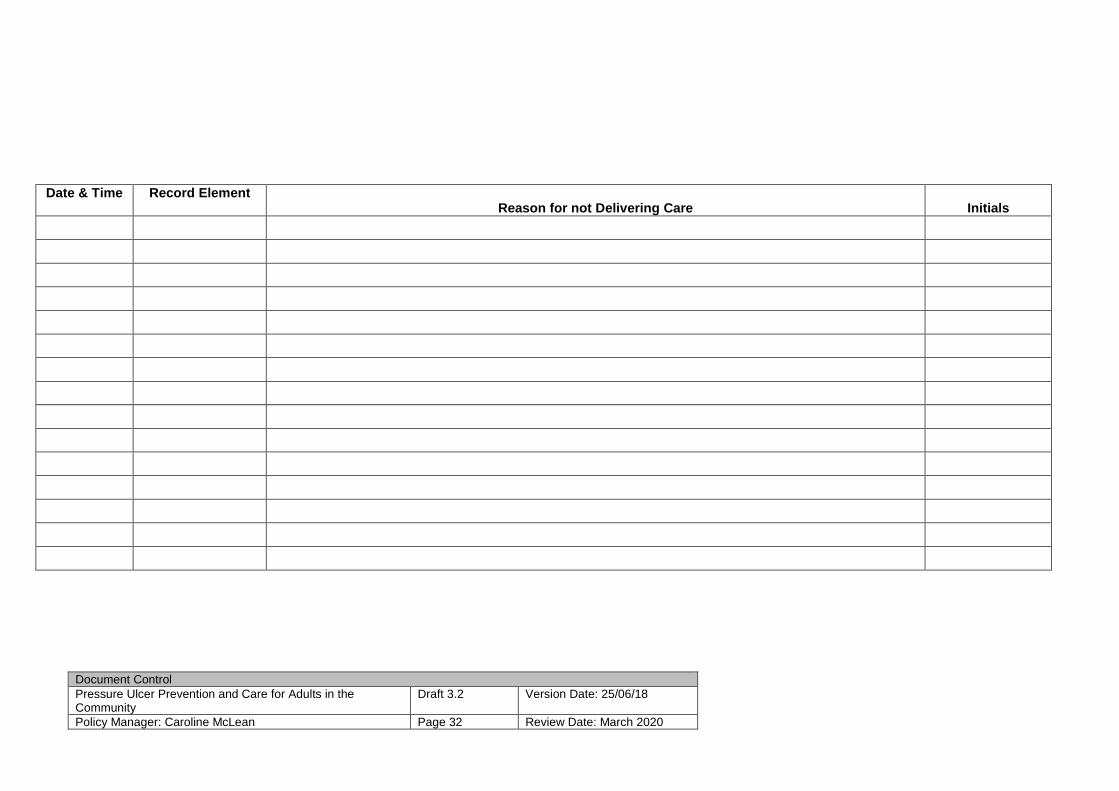
Date & Time Record Element Reason for not Delivering Care
Initials
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 33 Review Date: March 2020
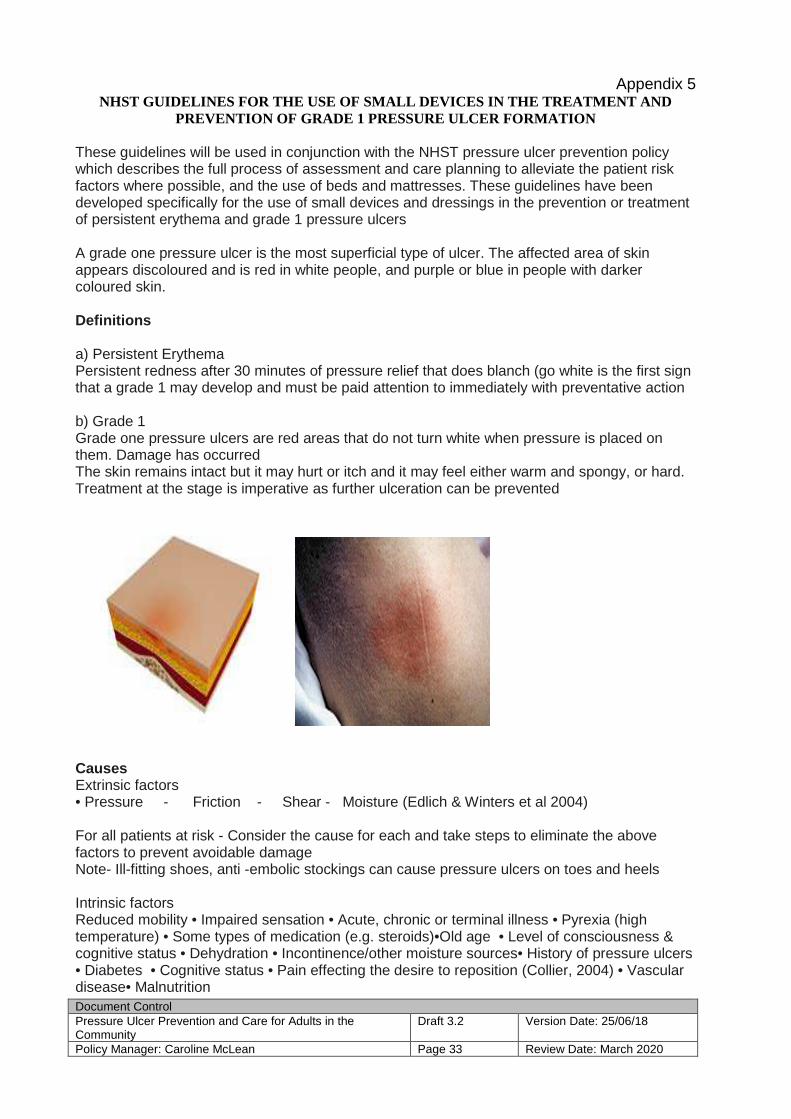
Appendix 5 NHST GUIDELINES FOR THE USE OF SMALL DEVICES IN THE TREATMENT AND
PREVENTION OF GRADE 1 PRESSURE ULCER FORMATION
These guidelines will be used in conjunction with the NHST pressure ulcer prevention policy which describes the full process of assessment and care planning to alleviate the patient risk factors where possible, and the use of beds and mattresses. These guidelines have been developed specifically for the use of small devices and dressings in the prevention or treatment of persistent erythema and grade 1 pressure ulcers A grade one pressure ulcer is the most superficial type of ulcer. The affected area of skin appears discoloured and is red in white people, and purple or blue in people with darker coloured skin. Definitions a) Persistent Erythema Persistent redness after 30 minutes of pressure relief that does blanch (go white is the first sign that a grade 1 may develop and must be paid attention to immediately with preventative action b) Grade 1 Grade one pressure ulcers are red areas that do not turn white when pressure is placed on them. Damage has occurred The skin remains intact but it may hurt or itch and it may feel either warm and spongy, or hard. Treatment at the stage is imperative as further ulceration can be prevented
Causes Extrinsic factors • Pressure - Friction - Shear - Moisture (Edlich & Winters et al 2004) For all patients at risk - Consider the cause for each and take steps to eliminate the above factors to prevent avoidable damage Note- Ill-fitting shoes, anti -embolic stockings can cause pressure ulcers on toes and heels Intrinsic factors Reduced mobility • Impaired sensation • Acute, chronic or terminal illness • Pyrexia (high temperature) • Some types of medication (e.g. steroids)•Old age • Level of consciousness & cognitive status • Dehydration • Incontinence/other moisture sources• History of pressure ulcers • Diabetes • Cognitive status • Pain effecting the desire to reposition (Collier, 2004) • Vascular disease• Malnutrition
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 34 Review Date: March 2020
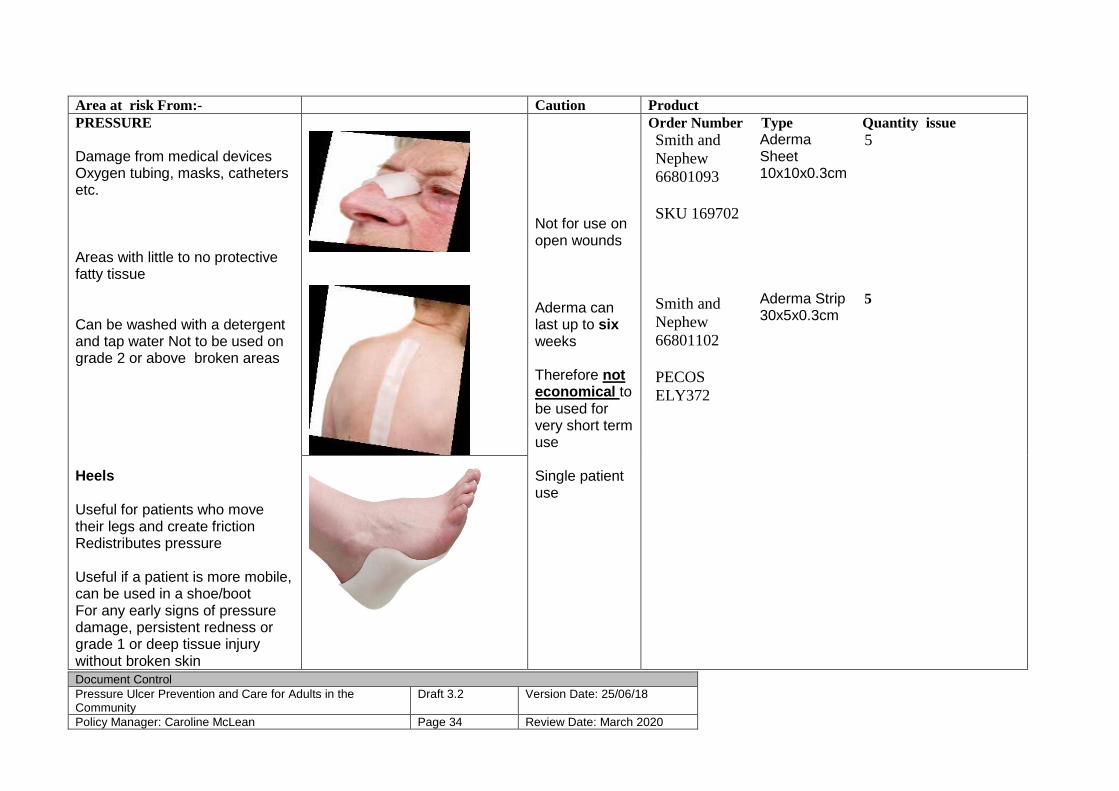
Area at risk From:- Caution Product PRESSURE Damage from medical devices Oxygen tubing, masks, catheters etc. Areas with little to no protective fatty tissue Can be washed with a detergent and tap water Not to be used on grade 2 or above broken areas Heels Useful for patients who move their legs and create friction Redistributes pressure Useful if a patient is more mobile, can be used in a shoe/boot For any early signs of pressure damage, persistent redness or grade 1 or deep tissue injury without broken skin
Not for use on open wounds Aderma can last up to six weeks Therefore not economical to be used for very short term use Single patient use
Order Number Type Quantity issue Smith and Nephew 66801093 SKU 169702
Aderma Sheet 10x10x0.3cm
5
Smith and Nephew 66801102 PECOS ELY372
Aderma Strip 30x5x0.3cm
5
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 35 Review Date: March 2020
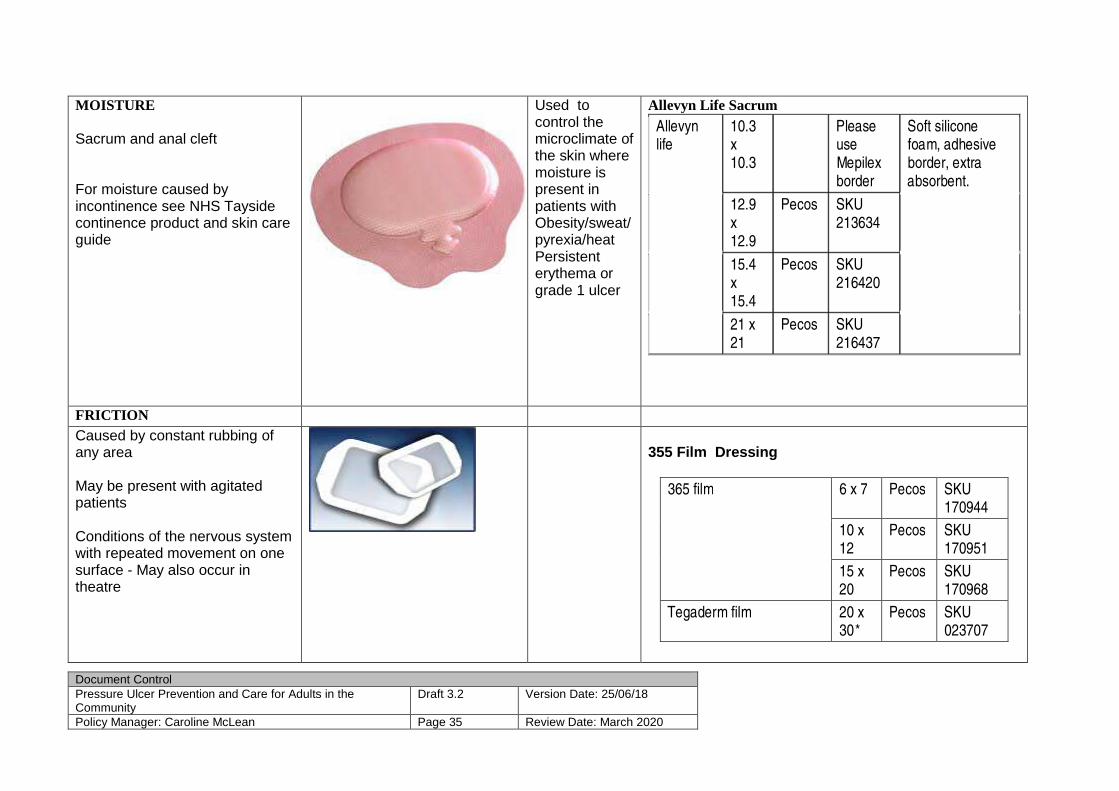
MOISTURE Sacrum and anal cleft For moisture caused by incontinence see NHS Tayside continence product and skin care guide
Used to control the microclimate of the skin where moisture is present in patients with Obesity/sweat/pyrexia/heat Persistent erythema or grade 1 ulcer
Allevyn Life Sacrum
Allevyn life
10.3 x 10.3
Please use Mepilex border
Soft silicone foam, adhesive border, extra absorbent.
12.9 x 12.9
Pecos SKU 213634
15.4 x 15.4
Pecos SKU 216420
21 x 21
Pecos SKU 216437
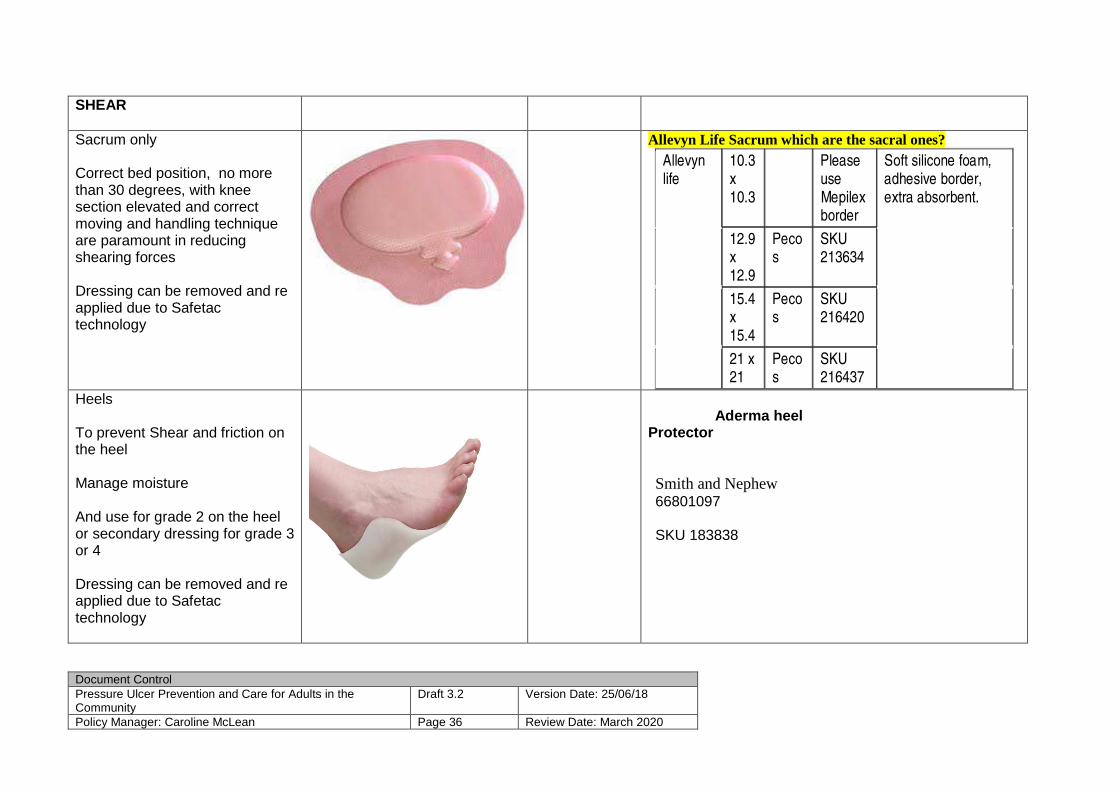
FRICTION Caused by constant rubbing of any area May be present with agitated patients Conditions of the nervous system with repeated movement on one surface - May also occur in theatre
355 Film Dressing
365 film 6 x 7 Pecos SKU 170944
10 x 12
Pecos SKU 170951
15 x 20
Pecos SKU 170968
Tegaderm film 20 x 30*
Pecos SKU 023707
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 36 Review Date: March 2020
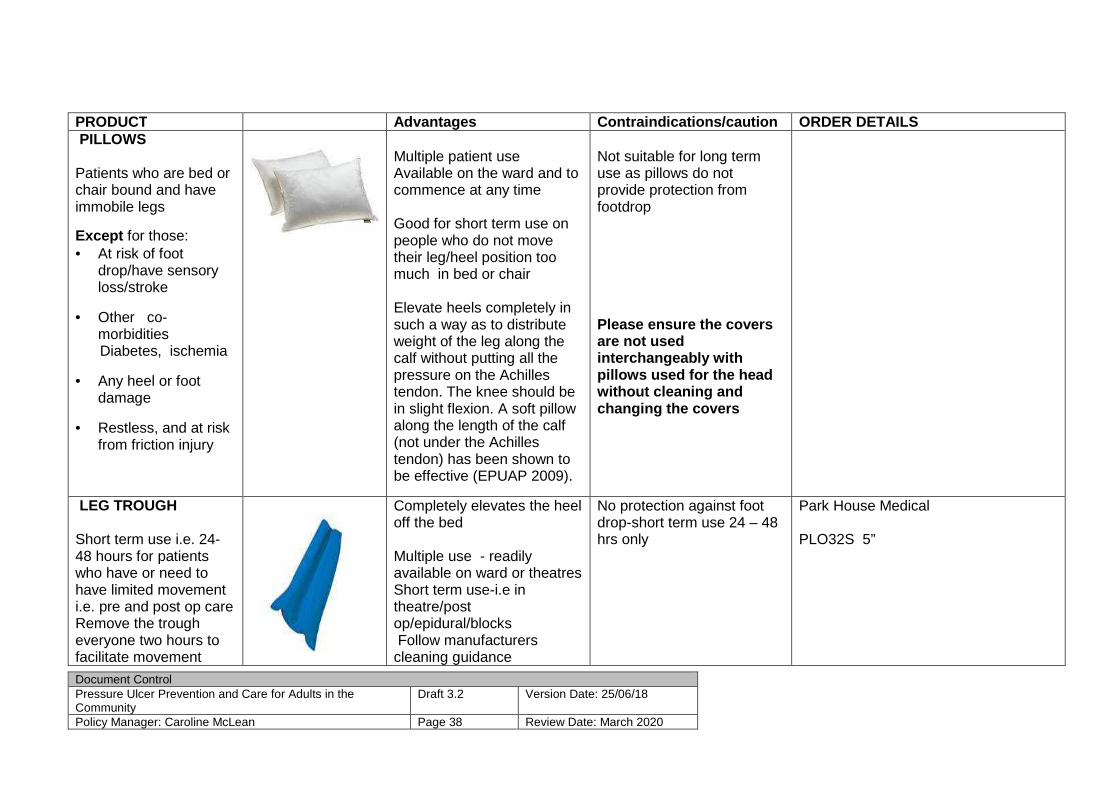
SHEAR
Sacrum only Correct bed position, no more than 30 degrees, with knee section elevated and correct moving and handling technique are paramount in reducing shearing forces Dressing can be removed and re applied due to Safetac technology
Allevyn Life Sacrum which are the sacral ones?
Allevyn life
10.3 x 10.3
Please use Mepilex border
Soft silicone foam, adhesive border, extra absorbent.
12.9 x 12.9
Pecos
SKU 213634
15.4 x 15.4
Pecos
SKU 216420
21 x 21
Pecos
SKU 216437
Heels To prevent Shear and friction on the heel Manage moisture And use for grade 2 on the heel or secondary dressing for grade 3 or 4 Dressing can be removed and re applied due to Safetac technology
Aderma heel Protector Smith and Nephew 66801097 SKU 183838

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 37 Review Date: March 2020
HST Guidelines for the use of heel elevators upda ted 2017 There is a paucity of clinical evidence; about the selection of an optimal device for preventing heel PU, however as heel ulcers are the second most common pressure ulcer in NHS Tayside, some guidelines based on a combination of existing evidence and clinical experience are required to ensure a consistent approach to the reduction in heel ulcer development. While pressure redistribution devices may reduce tissue interface pressures at the heels, expert opinion and clinical experience concur that elevation of the heel is indicated to both reduce pressure and prevent shear and friction caused by frequent movement of the heel due to restlessness, reflex movements of the legs, or voluntary movement. A variety of heel protection devices are available that are designed to both relieve tissue interface pressure and protect the heel from shear and friction. Considerations for selecting an optimal heel protection device include its ability to elevate the heel off the underlying support surface while preventing foot-drop and rotation of the leg, the boot's ability to wick away temperature, its ability to be cleaned, whether it allows patient ambulation, its ability to remain in place despite patient movement, and its ability to remain in place without causing pressure to other surfaces of the foot. J Wound Ostomy Continence Nurse. 2009 Nov-Dec; 36(6):602-8. The following table is a guideline only. When choo sing a device for heel elevation consider the objectives of care for the individual and the following: Comfort Mobility in bed/theatre. Are the patient’s legs likely to stay in one position in the bed? Are they at risk of friction and shear forces? Length of time of immobility Co-morbidities such as diabetes, vascular impairment, neuropathy, stroke Safety - is the patient at any further risk of falls if they mobilise with a secured device on the foot Existing heel ulcers and location of heel ulcer Registered nurses can supply the undernoted equipme nt for the prevention of heel ulcers however for complex issues and patients with diabetes who have any ulcer on the foot Refer to the following Orthotics Podiatry Diabetic nurse Refer to physio for mobility/drop foot issues when required Refer to Pressure Ulcer Prevention Policy NHST for further guidance.
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 38 Review Date: March 2020
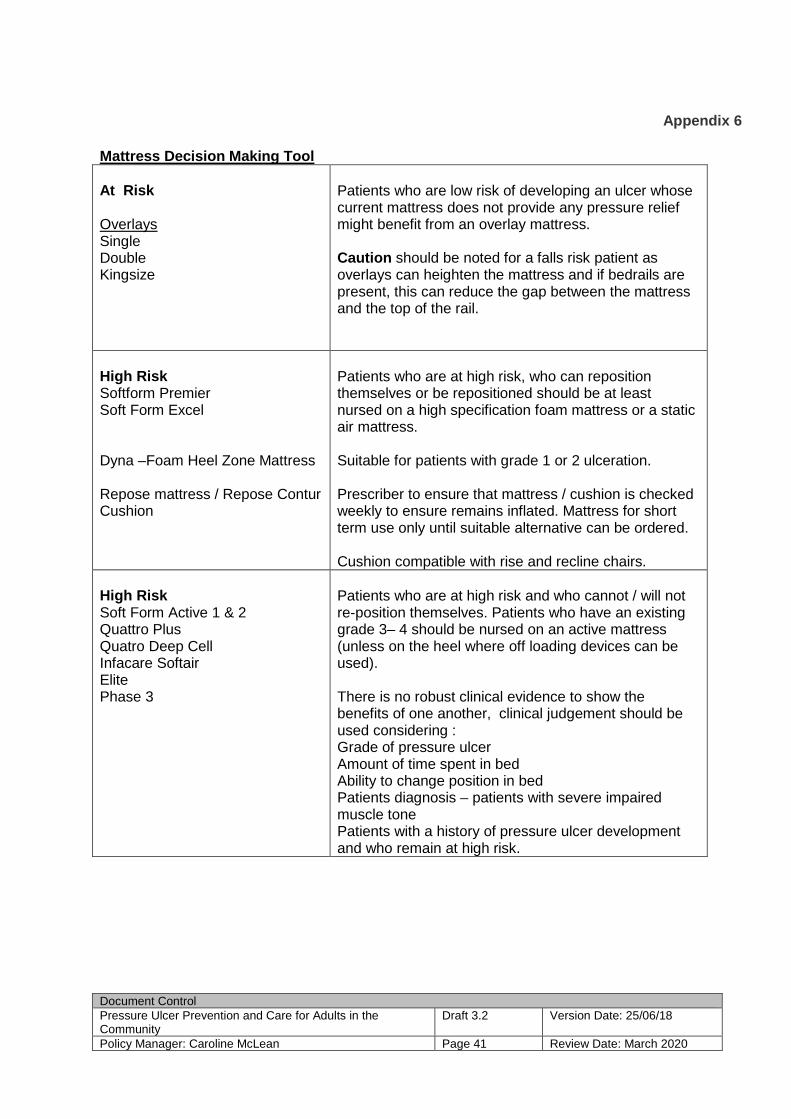
PRODUCT Advantages Contraindications/caution ORDER DETAILS PILLOWS Patients who are bed or chair bound and have immobile legs
Except for those: • At risk of foot
drop/have sensory loss/stroke
• Other co-morbidities
Diabetes, ischemia
• Any heel or foot damage
• Restless, and at risk from friction injury
Multiple patient use Available on the ward and to commence at any time Good for short term use on people who do not move their leg/heel position too much in bed or chair Elevate heels completely in such a way as to distribute weight of the leg along the calf without putting all the pressure on the Achilles tendon. The knee should be in slight flexion. A soft pillow along the length of the calf (not under the Achilles tendon) has been shown to be effective (EPUAP 2009).
Not suitable for long term use as pillows do not provide protection from footdrop
Please ensure the covers are not used interchangeably with pillows used for the head without cleaning and changing the covers
LEG TROUGH Short term use i.e. 24-48 hours for patients who have or need to have limited movement i.e. pre and post op care Remove the trough everyone two hours to facilitate movement
Completely elevates the heel off the bed Multiple use - readily available on ward or theatres Short term use-i.e in theatre/post op/epidural/blocks Follow manufacturers cleaning guidance
No protection against foot drop-short term use 24 – 48 hrs only
Park House Medical PLO32S 5”

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 39 Review Date: March 2020
PRODUCT Advantages Contraindications ORDER DETAILS REPOSE Bed/chairbound With or without existing heel ulcers N.B. • Those at risk of
footdrop or rotation of the ankle should have a PODUS boot
Can be used for multiple patients – ensure manufacturers cleaning guidance is adhered to Can held as stock for high risk people Can be secured to the patient, loosely with a light tubular bandage - do not secure on any patient who may be confused or disorientated as they may try to walk with the Repose in situ. Education video available http://reposedirect.com/
. Patient should not be mobilised with the Repose in position Ensure the knee is slightly bent and supported May not protect from foot drop associated with stroke/spasticity/existing footdrop Not as suitable if the heel ulcer is at the medial or lateral side of the heel, use the PODUS
Available on contract One pair Foot protector and pump Frontier medical group Code 650110 Warranty period one year
Talarmade DAP 600 Static Air Heel Protection Boot
Single patient use only Cover can be wiped down if lightly soiled Secures to the patient
Patient should not be mobilised with the DAP 600 in position Ensure the knee is slightly bent and supported May not protect from foot drop associated with stroke/spasticity/existing footdrop
SKU 193653 Static Air Heel Protection

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 40 Review Date: March 2020
PODUS Expected to be immobile for more than a week and/or At risk of foot drop or rotation of foot Existing heel ulcer Co-morbidities PVD Diabetes Sensory loss
Single patient use Lining can we washed or purchased for a single patient use For prevention/relief of ulcer in high risk patients For any patient with an existing ulcers Provides a more rigid support
Not suitable for ambulation, transfer only
Request through TORT centre ext 36292 Or hold a ward stock for high risk areas PB/STDS Kare Orthopaedics Podus Boot with Strap 1,1,TA379 Podus Boot Complete 1,1,TA379
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 41 Review Date: March 2020
Appendix 6
Mattress Decision Making Tool At Risk Overlays Single Double Kingsize
Patients who are low risk of developing an ulcer whose current mattress does not provide any pressure relief might benefit from an overlay mattress. Caution should be noted for a falls risk patient as overlays can heighten the mattress and if bedrails are present, this can reduce the gap between the mattress and the top of the rail.
High Risk Softform Premier Soft Form Excel Dyna –Foam Heel Zone Mattress Repose mattress / Repose Contur Cushion
Patients who are at high risk, who can reposition themselves or be repositioned should be at least nursed on a high specification foam mattress or a static air mattress. Suitable for patients with grade 1 or 2 ulceration. Prescriber to ensure that mattress / cushion is checked weekly to ensure remains inflated. Mattress for short term use only until suitable alternative can be ordered. Cushion compatible with rise and recline chairs.
High Risk Soft Form Active 1 & 2 Quattro Plus Quatro Deep Cell Infacare Softair Elite Phase 3
Patients who are at high risk and who cannot / will not re-position themselves. Patients who have an existing grade 3– 4 should be nursed on an active mattress (unless on the heel where off loading devices can be used). There is no robust clinical evidence to show the benefits of one another, clinical judgement should be used considering : Grade of pressure ulcer Amount of time spent in bed Ability to change position in bed Patients diagnosis – patients with severe impaired muscle tone Patients with a history of pressure ulcer development and who remain at high risk.
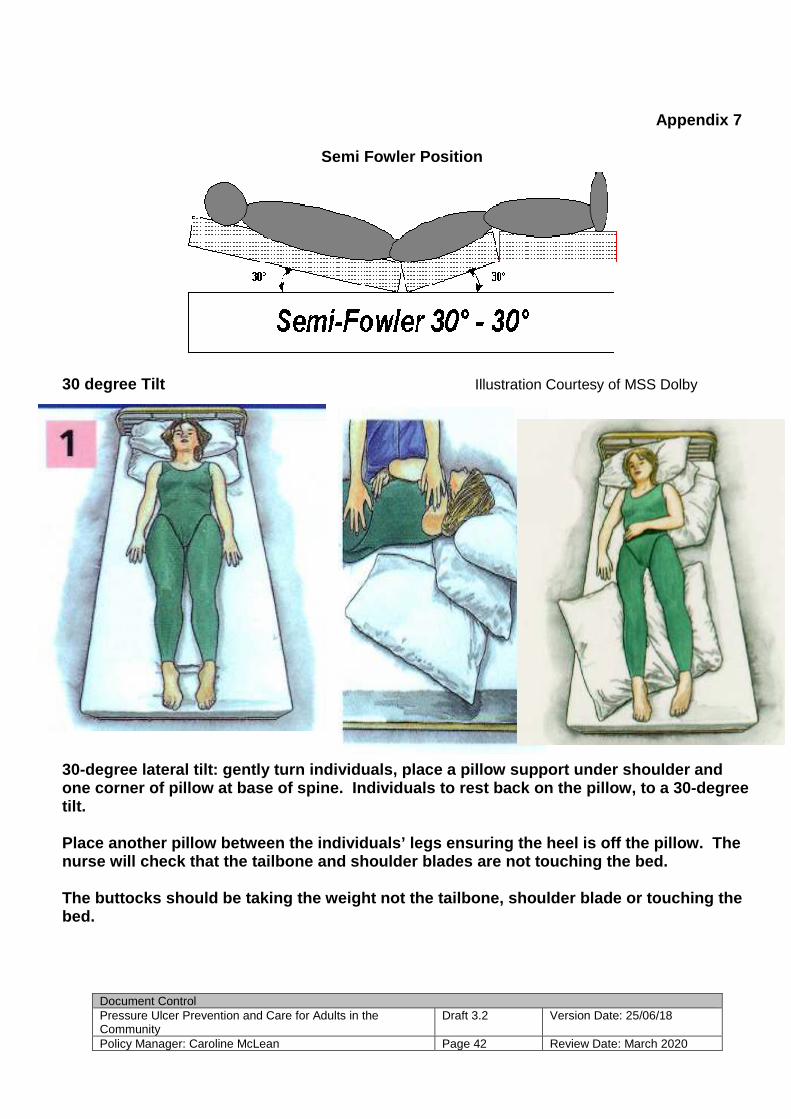
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 42 Review Date: March 2020
Appendix 7
Semi Fowler Position
30 degree Tilt Illustration Courtesy of MSS Dolby 30-degree lateral tilt: gently turn individuals, pl ace a pillow support under shoulder and one corner of pillow at base of spine. Individuals to rest back on the pillow, to a 30-degree tilt. Place another pillow between the individuals’ legs ensuring the heel is off the pillow. The nurse will check that the tailbone and shoulder bla des are not touching the bed. The buttocks should be taking the weight not the ta ilbone, shoulder blade or touching the bed.
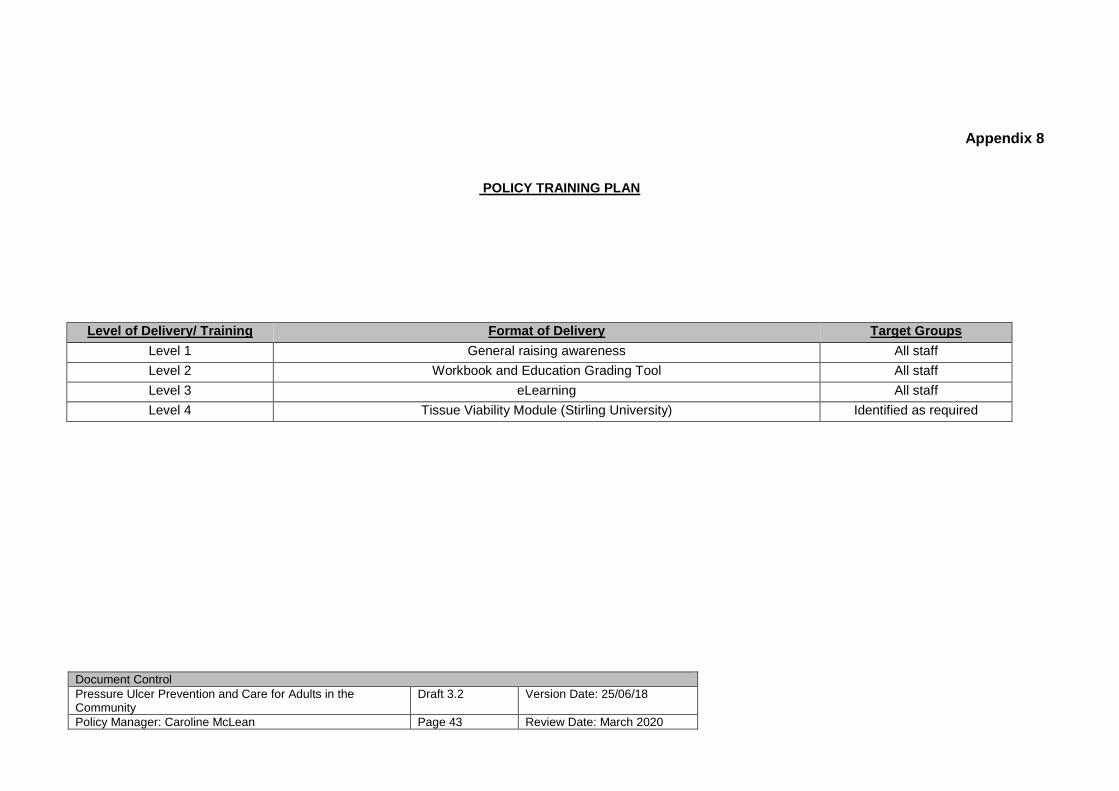
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 43 Review Date: March 2020
Appendix 8
POLICY TRAINING PLAN
Level of Delivery/ Training Format of Delivery Target Groups
Level 1 General raising awareness All staff
Level 2 Workbook and Education Grading Tool All staff
Level 3 eLearning All staff
Level 4 Tissue Viability Module (Stirling University) Identified as required
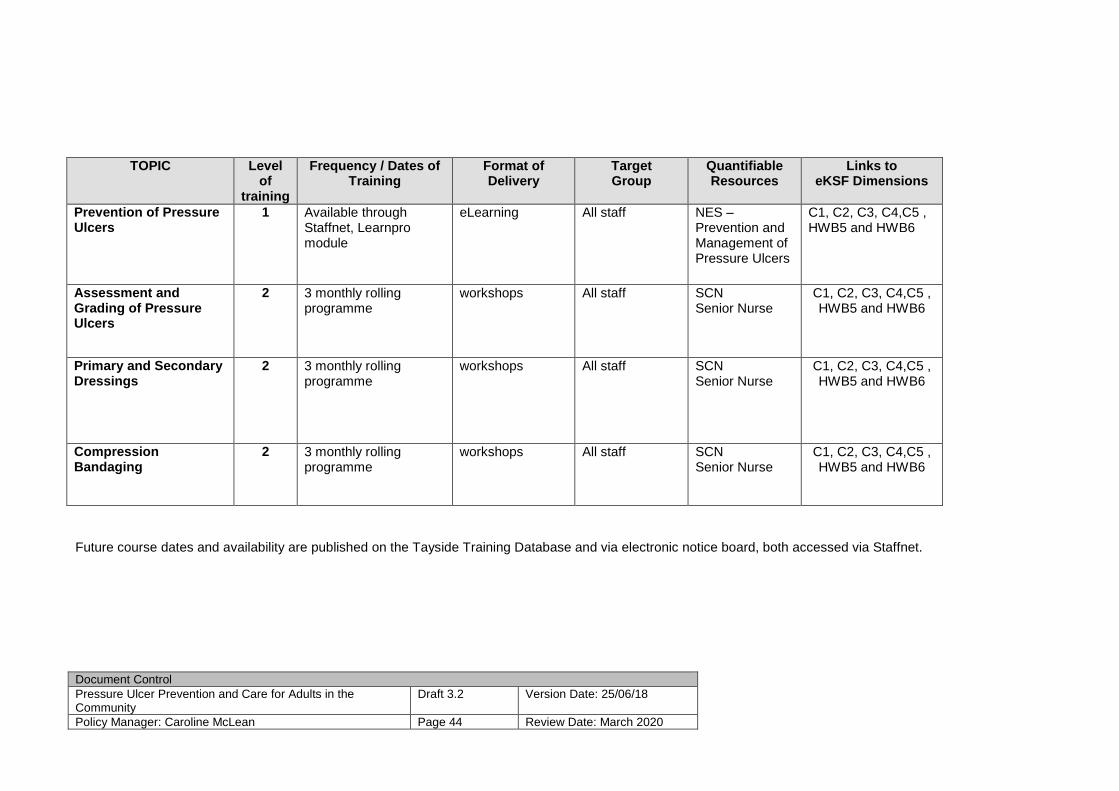
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 44 Review Date: March 2020
TOPIC Level of
training
Frequency / Dates of Training
Format of Delivery
Target Group
Quantifiable Resources
Links to eKSF Dimensions
Prevention of Pressure Ulcers
1 Available through Staffnet, Learnpro module
eLearning All staff NES – Prevention and Management of Pressure Ulcers
C1, C2, C3, C4,C5 , HWB5 and HWB6
Assessment and Grading of Pressure Ulcers
2 3 monthly rolling programme
workshops All staff SCN Senior Nurse
C1, C2, C3, C4,C5 , HWB5 and HWB6
Primary and Secondary Dressings
2 3 monthly rolling programme
workshops All staff SCN Senior Nurse
C1, C2, C3, C4,C5 , HWB5 and HWB6
Compression Bandaging
2 3 monthly rolling programme
workshops All staff SCN Senior Nurse
C1, C2, C3, C4,C5 , HWB5 and HWB6
Future course dates and availability are published on the Tayside Training Database and via electronic notice board, both accessed via Staffnet.
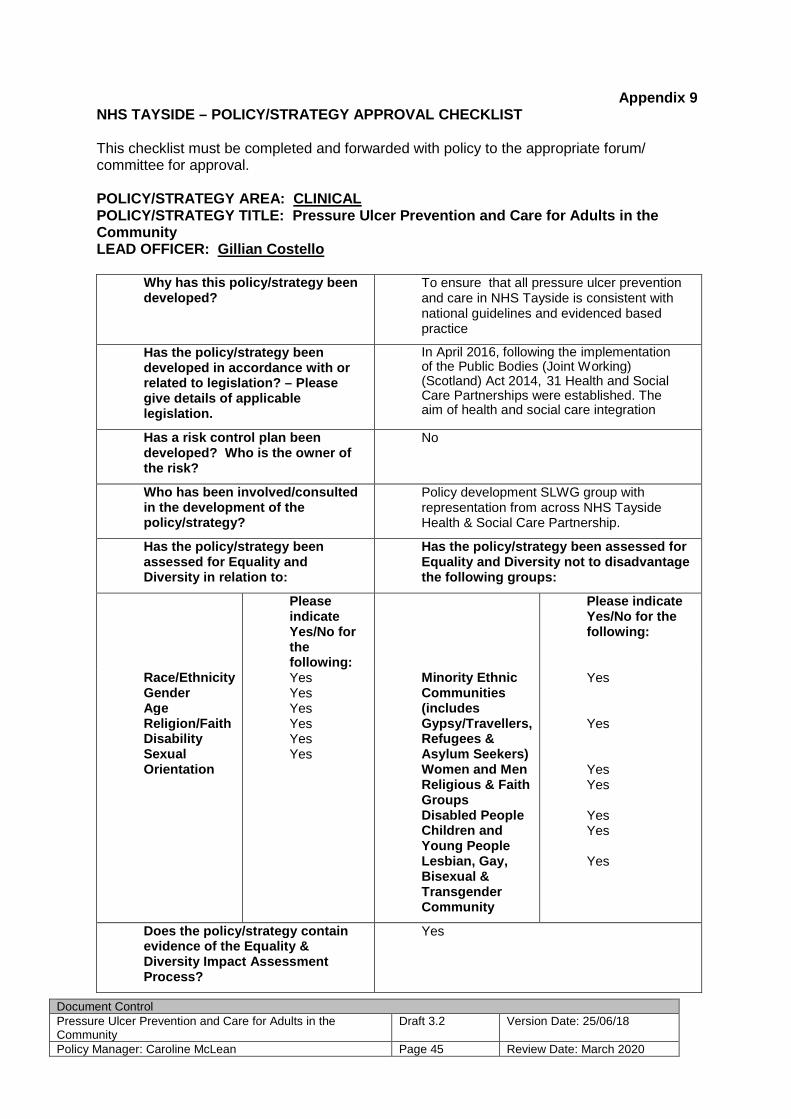
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 45 Review Date: March 2020
Appendix 9 NHS TAYSIDE – POLICY/STRATEGY APPROVAL CHECKLIST
This checklist must be completed and forwarded with policy to the appropriate forum/ committee for approval. POLICY/STRATEGY AREA: CLINICAL POLICY/STRATEGY TITLE: Pressure Ulcer Prevention a nd Care for Adults in the Community LEAD OFFICER: Gillian Costello
Why has this policy/strategy been developed?
To ensure that all pressure ulcer prevention and care in NHS Tayside is consistent with national guidelines and evidenced based practice
Has the policy/strategy bee n developed in accordance with or related to legislation? – Please give details of applicable legislation.
In April 2016, following the implementation of the Public Bodies (Joint Working) (Scotland) Act 2014, 31 Health and Social Care Partnerships were established. The aim of health and social care integration
Has a risk control plan been developed? Who is the owner of the risk?
No
Who has been involved/consulted in the development of the policy/strategy?
Policy development SLWG group with representation from across NHS Tayside Health & Social Care Partnership.
Has the policy/strategy been assessed for Equality and Diversity in relation to:
Has the policy/strategy been assessed f or Equality and Diversity not to disadvantage the following groups:
Please indicate Yes/No for the following:
Please indicate Yes/No for the following:
Race/Ethnicity Gender Age Religion/Faith Disability Sexual Orientation
Yes Yes Yes Yes Yes Yes
Minority Ethnic Communities (includes Gypsy/Travellers, Refugees & Asylum Seekers) Women and Men Religious & Faith Groups Disabled People Children and Young People Lesbian, Gay, Bisexual & Transgender Community
Yes Yes Yes Yes Yes Yes Yes
Does the policy/strategy contain evidence of the Equality & Diversity Impact Assessment Process?
Yes

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 46 Review Date: March 2020
Is there an implementation plan? Yes
Which officers are responsible for implementation?
Caroline McLean
When will the policy/strategy take effect?
June 2018
Who must comply with the policy/strategy?
All nursing and AHP staff
How will they be informed of their responsibilities?
Policy emailed to Clinical Leads Cascade training at ward level
Is any training require d? Yes Education on the Policy and associated documentation and care
If yes, has any been arranged? Rolling monthly Educational Programme.
Are there any cost implications? No
If yes, please detail costs and note source of funding
N/A
Who is responsible for auditing the implementation of the policy/strategy?
Senior Charge Nurse
What is the audit interval? Weekly or longer with the implementation of national nursing quality indicators
Who will receive the audit reports? Nursing & Midwifery Directorate NHS Scotland
When will the policy/strategy be reviewed and by whom? (please give designation)
Bi annually, Nursing & Midwifery Directorate
Name: Gillian Costello Date: June 2018

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 47 Review Date: March 2020
Appendix 10
EQUALITY IMPACT ASSESSMENT
Manager Caroline McLean
Group Pressure Ulcer Prevention and Care
for Adults in Community
Established
June 2009
Last updated
June 2017
Review / Expiry
April 2019
UNCONTROLLED WHEN PRINTED
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 48 Review Date: March 2020
Section 1 (This is mandatory and should be completed in all cases) Part A – Overview Name of Policy, Service Improvement, Redesign or St rategy: Pressure Ulcer Prevention and Care for Adults in Community Lead Director of Manager:
Caroline McLean What are the main aims of the Policy, Service Impro vement, Redesign or Strategy?
To ensure that all adult in individuals within NHS Tayside receive the optimal care to prevent the development of pressure ulcers
Description of the Policy, Service Improvement, Red esign or Strategy – What is it? What does it do? Who does it? And wh o is it for?
This policy has been developed for the prevention and management of pressure ulcers within health and social care services and take into account of the national health and wellbeing outcomes and revised National Health and Social Care Standards, June 2017.
The aim of this policy is to :
• Ensure everyone is provided with optimum person centred evidence based pressure ulcer prevention.
• Standardise the assessment and care of people with/or at risk of developing pressure ulcers.
• Ensure each person has the correct pressure relieving aids to meet their clinical needs.
• Set the minimum standard for the maintenance of knowledge and skills related to pressure area care.
• Comply with Health Improvement Scotland Pressure Ulcer Prevention Standards (2016)
• Comply with Health and Social Care Standards- My support, my life (2017)
• Comply with Health and Social Care Partnerships (Joint Working) (Scotland) Act 2014
To meet the changing needs of our nation, investment, while necessary, must be matched with reform to drive further improvements in our services. Our services will increasingly face demands from people with long-term conditions needing support from health and social care. These challenges were recognised in the Audit Scotland report, NHS in Scotland 2016, and underline the importance of bringing together the different programmes of work to improve health and social care services.

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 49 Review Date: March 2020
What are the intended outcomes from the proposed Po licy, Service Improvement, Redesign or strategy? – What will happen as a resul t of it?- Who benefits from it and how? A sustained reduction in individuals developing a pressure ulcer Name of the group responsible for assessing or cons idering the equality impact assessment? This should be the Policy Working Grou p or the Project team for Service Improvement, Redesign or Strategy. Tissue Viability Network
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 50 Review Date: March 2020
SECTION 1 Part B – Equality and Diversity Impacts Which equality group or Protected Characteristics d o you think will be affected? Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
1.1 Will it impact on the whole population? Yes or No. If yes will it have a differential impact on any of the groups identified in 1.2. If no go to 1.2 to identify which groups.
Yes No
1.2 Which of the protected characteristic(s) or groups will be affected? • Minority ethnic population (including
refugees, asylum seekers & gypsies/ travellers)
• Women and men • People in religious/faith groups • Disabled people • Older people, children and young
people • Lesbian, gay, bisexual and transgender
people • People with mental health problems • Homeless people • People involved in criminal justice
system • Staff • Socio-economically deprived groups

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 51 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
1.3 Will the development of the policy, strategy or service improvement/ redesign lead to: • Discrimination • Unequal opportunities • Poor relations between equality groups
and other groups • Other
No

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 52 Review Date: March 2020
SECTION 2 – Human Rights and Health Impact Which Human Rights could be affected in relation to article 2, 3, 5, 6, 9 and 11. (ECHR: European Conv ention on Human Rights) Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
2.1
On Life (Article 2, ECHR)
• Basic necessities such as adequate nutrition, and safe drinking water
• Suicide • Risk to life o /from others • Duties to protect life from risks by self/
others • End of life questions
No
2.2
On Freedom from ill -treatment (Article 3, ECHR)
• Fear, humiliation • Intense physical or mental suffering or
anguish • Prevention of ill-treatment • Investigation of reasonably
substantiated allegations of serious ill-treatment
• Dignified living conditions
No
2.3 On Liberty (Article 5, ECHR)
• Detention under mental health law • Review of continued justification of
detention • Informing reasons for detention
No
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 53 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
2.4 On a Fair Hearing (Article 6, ECHR)
• Staff disciplinary proceedings • Malpractice • Right to be heard • Procedural fairness • Effective participation in proceedings
that determine rights such as employment, damages/compensation
No
2.5 On Private and family life (Article 6, ECHR)
• Private and Family life • Physical and moral integrity (e.g.
freedom from non-consensual treatment, harassment or abuse
• Personal data, privacy and confidentiality
• Sexual identity • Autonomy and self-determination • Relations with family, community • Participation in decisions that affect
rights • Legal capacity in decision making
supported participation and decision making, accessible information and communication to support decision making
• Clean and healthy environment
No
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 54 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
2.6 On Freedom of thought, conscience and religion (Article 9, ECHR)
• To express opinions and receive and impart information and ideas without interference
No
2.7 On Freedom of assembly and association (Article 11, ECHR)
• Choosing whether to belong to a trade union
No
2.8 On Marriage and founding a family
• Capacity • Age
No
2.9 Protocol 1 (Article 1, 2, 3 ECHR)
• Peaceful enjoyment of possessions
No
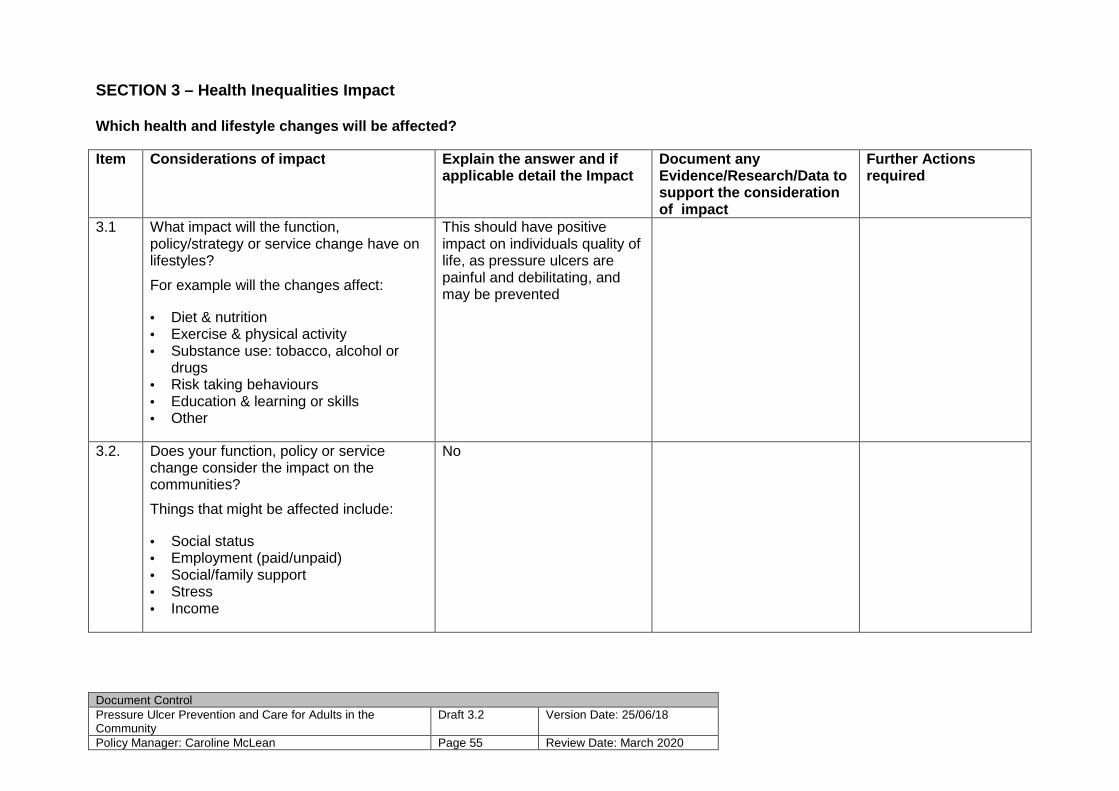
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 55 Review Date: March 2020
SECTION 3 – Health Inequalities Impact Which health and lifestyle changes will be affected ? Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
3.1 What impact will the function, policy/strategy or service change have on lifestyles?
For example will the changes affect: • Diet & nutrition • Exercise & physical activity • Substance use: tobacco, alcohol or
drugs • Risk taking behaviours • Education & learning or skills • Other
This should have positive impact on individuals quality of life, as pressure ulcers are painful and debilitating, and may be prevented
3.2. Does your function, policy or service change consider the impact on the communities?
Things that might be affected include: • Social status • Employment (paid/unpaid) • Social/family support • Stress • Income
No
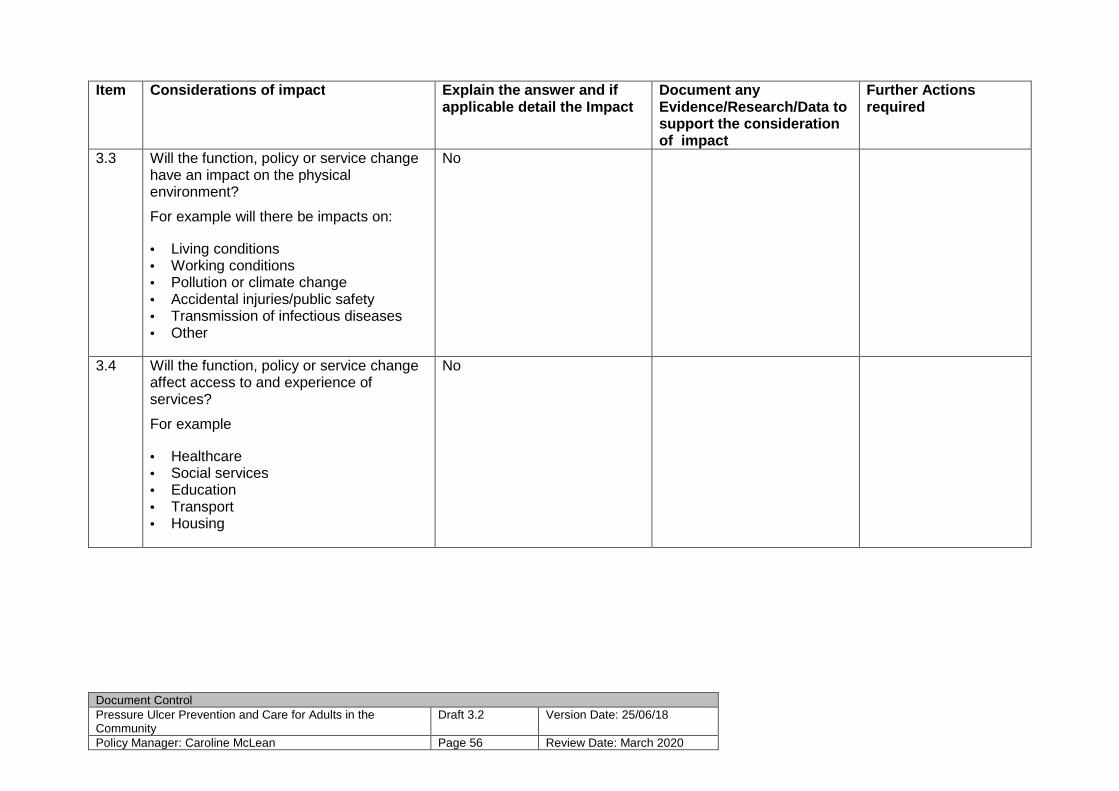
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 56 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
3.3 Will the function, policy or service change have an impact on the physical environment?
For example will there be impacts on: • Living conditions • Working conditions • Pollution or climate change • Accidental injuries/public safety • Transmission of infectious diseases • Other
No
3.4 Will the function, policy or service change affect access to and experience of services?
For example • Healthcare • Social services • Education • Transport • Housing
No
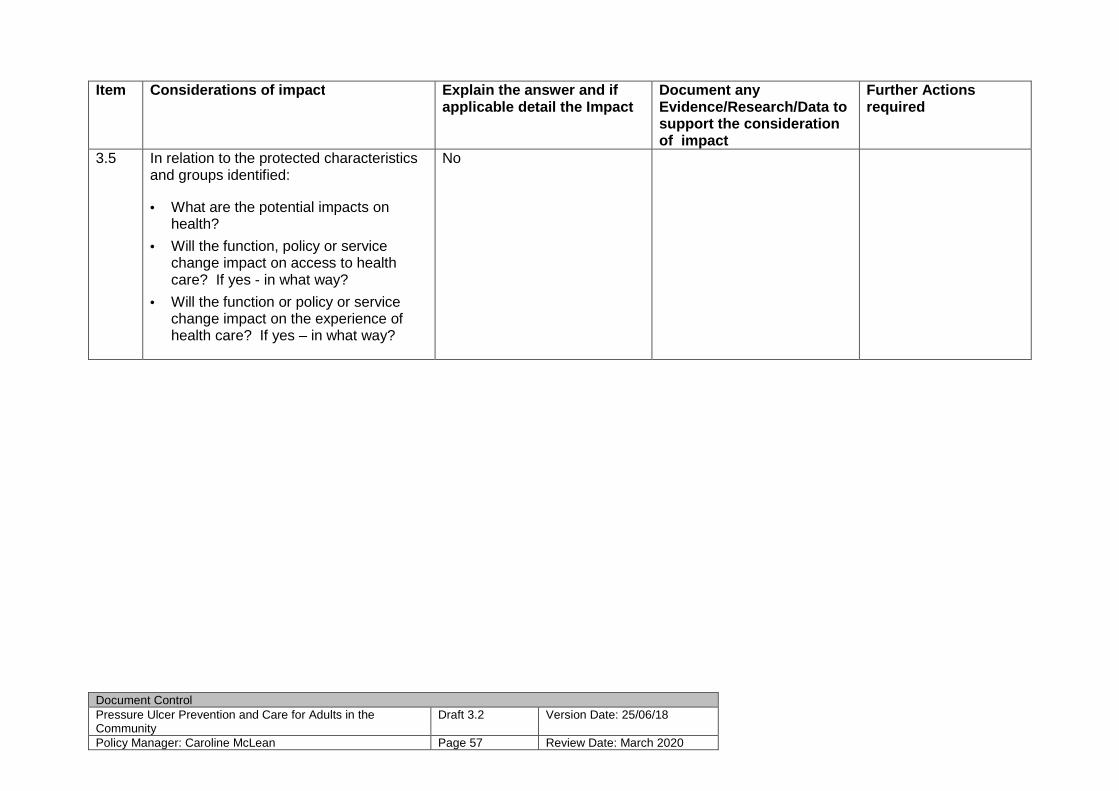
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 57 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
3.5 In relation to the protected characteristics and groups identified: • What are the potential impacts on
health?
• Will the function, policy or service change impact on access to health care? If yes - in what way?
• Will the function or policy or service change impact on the experience of health care? If yes – in what way?
No
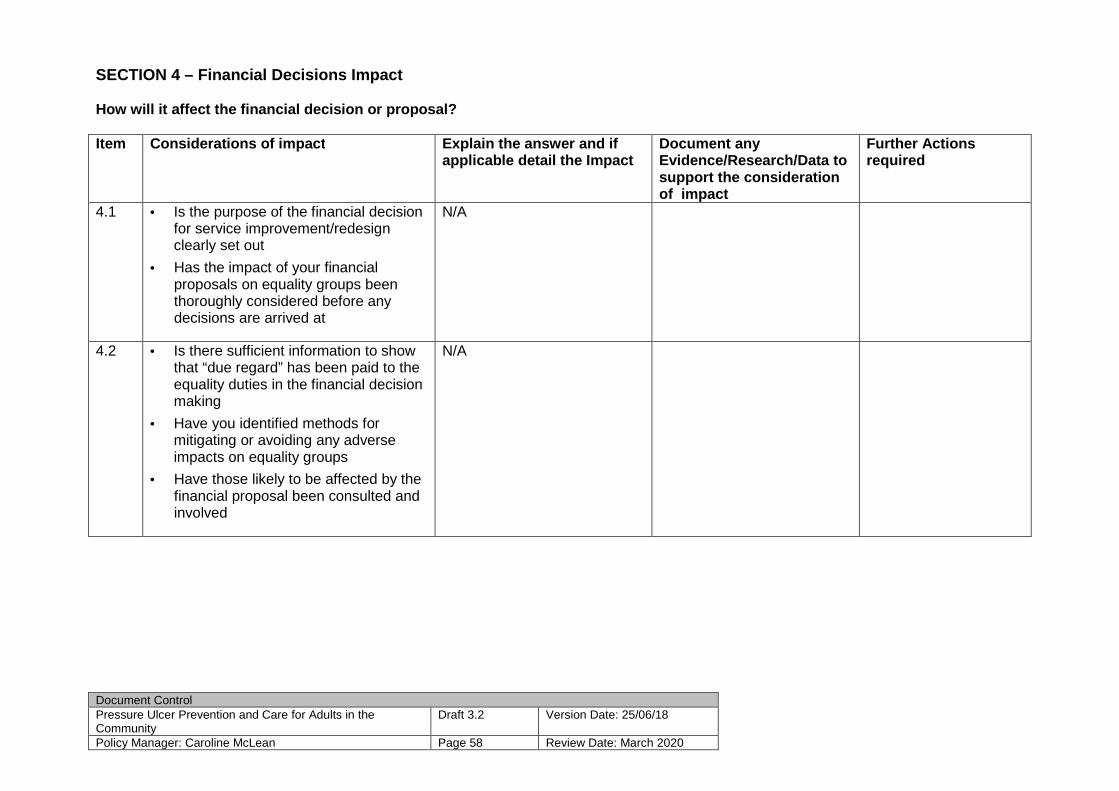
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 58 Review Date: March 2020
SECTION 4 – Financial Decisions Impact How will it affect the financial decision or propos al? Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
4.1
• Is the purpose of the financial decision for service improvement/redesign clearly set out
• Has the impact of your financial proposals on equality groups been thoroughly considered before any decisions are arrived at
N/A
4.2 • Is there sufficient information to show that “due regard” has been paid to the equality duties in the financial decision making
• Have you identified methods for mitigating or avoiding any adverse impacts on equality groups
• Have those likely to be affected by the financial proposal been consulted and involved
N/A
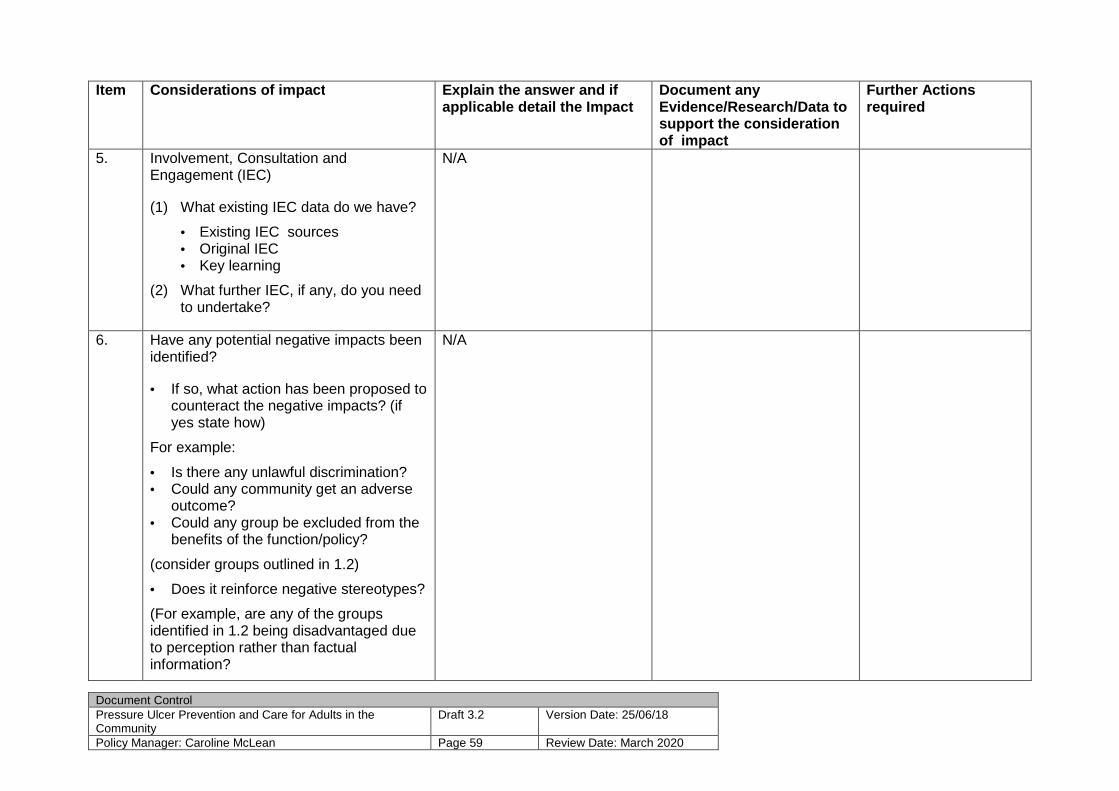
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 59 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
5. Involvement, Consultation and Engagement (IEC) (1) What existing IEC data do we have?
• Existing IEC sources • Original IEC • Key learning
(2) What further IEC, if any, do you need to undertake?
N/A
6. Have any potential negative impacts been identified? • If so, what action has been proposed to
counteract the negative impacts? (if yes state how)
For example:
• Is there any unlawful discrimination? • Could any community get an adverse
outcome? • Could any group be excluded from the
benefits of the function/policy?
(consider groups outlined in 1.2)
• Does it reinforce negative stereotypes?
(For example, are any of the groups identified in 1.2 being disadvantaged due to perception rather than factual information?
N/A

Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 60 Review Date: March 2020
Item Considerations of impact Explain the answer and if
applicable detail the Impact Document any Evidence/Research/Data to support the consideration of impact
Further Actions required
7. Data & Research
• Is there need to gather further evidence/data?
• Are there any apparent gaps in knowledge/skills?
N/A
8. Monitoring of outcomes
• How will the outcomes be monitored? • Who will monitor? • What criteria will you use to measure
progress towards the outcomes?
All areas will submit a Datix/Mosiac report if a grade 2-4 pressure ulcer develops. Qlikview will provide a dashboard display of number of pressure ulcers occurring
9. Recommendations State the conclusion of the Impact Assessment
There will be no adverse impact on equality diversity and human rights
10. Completed function/policy
• Who will sign this off? • When?
This is an updated policy not a new policy Tissue Viability Network NHS Tayside Nurse Director
11. Publication
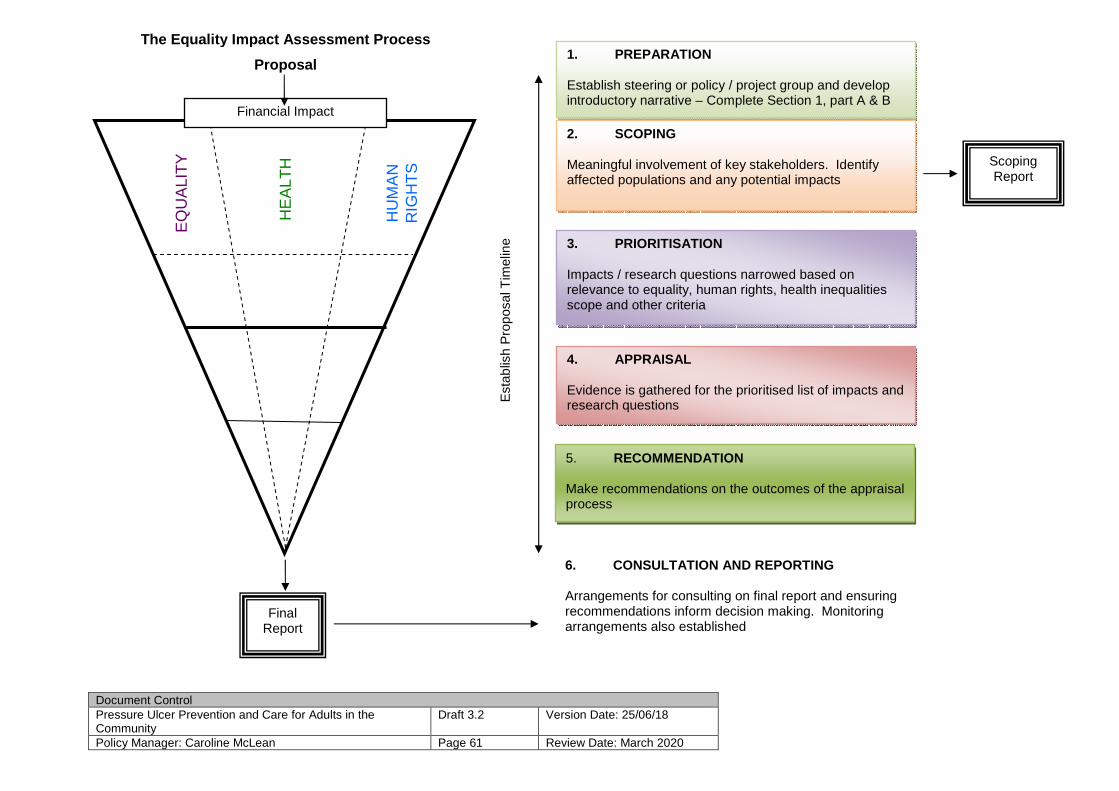
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 61 Review Date: March 2020
1. PREPARATION
Establish steering or policy / project group and develop introductory narrative – Complete Section 1, part A & B
2. SCOPING Meaningful involvement of key stakeholders. Identify affected populations and any potential impacts
3. PRIORITISATION Impacts / research questions narrowed based on relevance to equality, human rights, health inequalities scope and other criteria
4. APPRAISAL Evidence is gathered for the prioritised list of impacts and research questions
5. RECOMMENDATION Make recommendations on the outcomes of the appraisal process
Final Report
6. CONSULTATION AND REPORTING Arrangements for consulting on final report and ensuring recommendations inform decision making. Monitoring arrangements also established
Scoping Report
Financial Impact
Est
ablis
h P
ropo
sal T
imel
ine
The Equality Impact Assessment Process
Proposal
EQ
UA
LIT
Y
HE
ALT
H
HU
MA
N
RIG
HT
S
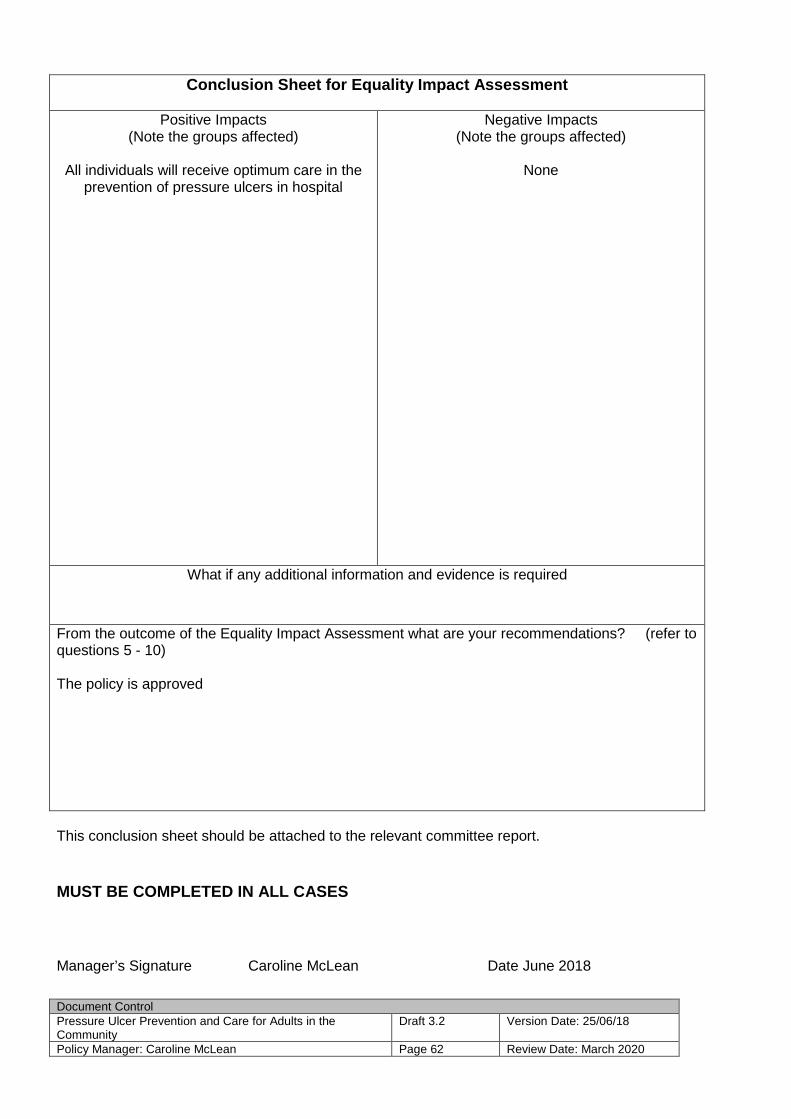
Document Control Pressure Ulcer Prevention and Care for Adults in the Community
Draft 3.2 Version Date: 25/06/18
Policy Manager: Caroline McLean Page 62 Review Date: March 2020
Conclusion Sheet for Equality Impact Assessment
Positive Impacts (Note the groups affected)
All individuals will receive optimum care in the
prevention of pressure ulcers in hospital
Negative Impacts (Note the groups affected)
None
What if any additional information and evidence is required
From the outcome of the Equality Impact Assessment what are your recommendations? (refer to questions 5 - 10) The policy is approved
This conclusion sheet should be attached to the relevant committee report.
MUST BE COMPLETED IN ALL CASES
Manager’s Signature Caroline McLean Date June 2018