nutritional support in the next millennium john p. grant, md director nss duke university medical...
TRANSCRIPT

Nutritional Support in the Nutritional Support in the Next MillenniumNext Millennium
John P. Grant, MDDirector NSSDuke University Medical Center

Executive Summary
Malnutrition contributes to:
Morbidity
Mortality
LOS
Hospital Cost
Executive Summary Malnutrition contributes to: increased
morbidity, mortality, LOS, hospital cost.
Appropriate nutrition support can treat and prevent malnutrition and reduce complications.

Executive Summary Malnutrition contributes to: increased
morbidity, mortality, LOS, hospital cost.
Appropriate nutrition support can treat and prevent malnutrition and reduce complications.
Malnutrition is common in hospitalized patients.

Executive Summary
On review, most medical centers, including DUMC, have inadequate systems for:
– Identifying patients at risk of malnutrition, and
– Ensuring provision of appropriate nutrition care when identified.

1997 JCAHO Standards
Nutrition care practices will be standardized throughout the hospital.
When indicated by patient’s needs:
– Nutrition status will be assessed.
– For patients at nutritional risk:
Nutrition care will be planned and implemented.
Response to nutrition care will be monitored.
Most hospitals are not meeting the new standards for nutrition care

Executive Summary
Hospitals are:
– Currently absorbing increased costs of care and yet not achieving optimal patient outcomes, and

Executive Summary
Hospitals are:
– Currently absorbing increased costs of care and yet not achieving optimal patient outcomes, and
– Not fulfilling requirements of JCAHO standards for nutrition care.

Therefore,
We need to revisit the way we provide nutrition care...

Does malnutrition contribute to increased morbidity, mortality, LOS, and hospital cost?

Morbidity and Malnutrition
Risk factors for clean wound infections in 23,649 surgical patients at Foothills Hospital in Calgary, Alberta, 1967-1972.
Risk IncreaseMalnutrition 9.2 xObesity 7.5 xDiabetes 5.9 xAge > 50 1.9 xSteroids 1.4 x
Cruse, Arch Surg 107:206,1973

Mortality and Albumin
Review of 509 veterans at Hines IL VAMC found a linear relationship between 30-day mortality and serum albumin concentration. Percent Mortality = 132 - 37.3 [Alb]
Mortality was decreased in 15 patients who received 5 or more days of TPN
Reinhardt, JPEN 4:357, 1980

Prognostic Nutrition Index
Complications Monitored
Death PhlebitisSepticemia CHFIntraabdominal SepsisMIFistula Formation Resp. FailureUTI AtelectasisPneumonia Pulm. EmbolusWound Infection CVAWound Dehiscence Shock
Buzby, Surg Clin North Am 61:465, 1981

Prognostic Nutrition Index
Correlated standard nutrition assessment with patient outcome in 100 veterans undergoing elective abdominal surgery.
PNI(%) = 158 - 16.6 [Alb] - 0.78 [TSF] -
0.2 [TFN] - 5.8 (DTHR)
Buzby, Surg Clin North Am 61:465, 1981

Prognostic Nutrition Index
Prospective study in 161 elective abdominal surgery patients demonstrated:
% Complications % Death
PNI < 40 8.0 3.0
PNI 40-49 30.0* 4.3
PNI 50 46.0* 33*
*p<.01
Buzby, Surg Clin North Am 61:465, 1981

Malnutrition and M&M
Nutrition status determined by:% UBW, % IBW, AMC, Albumin.
Compared outcome in 215 non-cancer patients undergoing major and minor vascular, and abdominal surgery.
Warnold, Ann Surg 199:299, 1984

Malnutrition and M&M
If two or more assessment parameters were abnormal:
Hospital stay was prolonged from 14 to 29 days (p<.01).
Overall frequency of complications increased from 23 to 48% (p<.01).
Serious complications increased from 9 to 31% (p<.01).
Warnold, Ann Surg 199:299, 1984
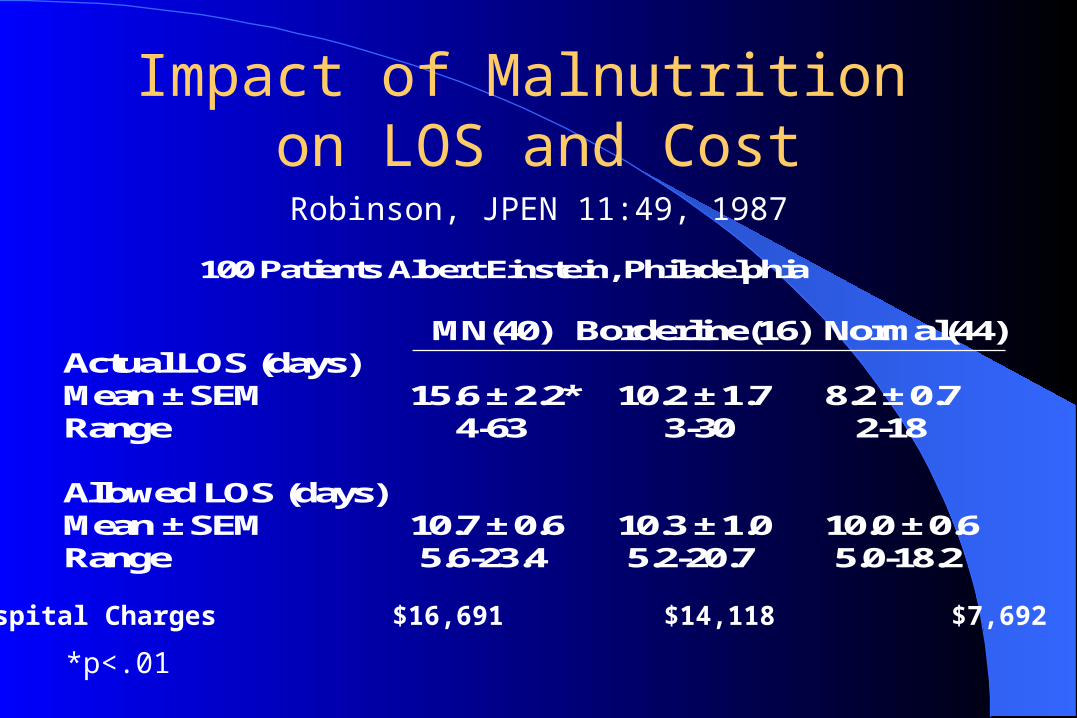
Impact of Malnutrition on LOS and Cost
MN(40) Borderline(16) Normal(44)Actual LOS (days) Mean ± SEM 15.6 ± 2.2* 10.2 ± 1.7 8.2 ± 0.7Range 4-63 3-30 2-18
Allowed LOS (days) Mean ± SEM 10.7 ± 0.6 10.3 ± 1.0 10.0 ± 0.6Range 5.6-23.4 5.2-20.7 5.0-18.2
LOS > allowed 18 (45%) 6 (37%) 13 (30%)LOS < allowed 18 (45%) 7 (44%) 21 (61%)LOS = allowed 4 (10%) 3 (19%) 4 (9%)
100 Patients Albert Einstein, Philadelphia
Robinson et al., JPEN 11:49, 1987
*p<.01
Hospital Charges $16,691 $14,118 $7,692
Robinson, JPEN 11:49, 1987

Impact of Malnutrition on LOS, Total Charges, and Cost of Hospitalization
D ia g n o s is # P a t ie n ts (% ) A v e L O S (d ) C h a r g e s $ C o s t $
P n e u m o n ia M N 1 2 7 (6 3 ) 1 0 .9 ± 0 .0 * 7 9 0 2 ± 7 7 0 * 3 5 2 1 ± 3 8 0 * N o r m a l 7 8 (3 7 ) 8 .4 ± 0 .7 4 9 7 9 ± 5 0 5 2 1 4 0 ± 2 1 4
In f la m m a to r y B o w e l D is e a s e M N 5 2 (4 4 ) 8 .8 ± 1 .0 4 8 9 0 ± 4 5 2 * 1 8 8 6 ± 1 7 8 * N o r m a l 6 5 (5 6 ) 7 .0 ± 0 .6 3 6 7 2 ± 3 1 9 1 3 7 2 ± 11 2
F x H ip /P e lv is M N 1 8 (4 5 ) 1 5 .9 ± 2 .1 5 2 7 6 ± 11 7 0 2 6 4 9 ± 6 7 9 N o r m a l 2 2 (5 5 ) 1 4 .8 ± 2 .2 3 7 1 0 ± 7 7 8 1 5 8 7 ± 2 6 0
7 7 1 P a t ie n ts in Tw o A c u te C a r e H o s p ita ls
R e il ly e t a l . , J P E N 1 2 :3 7 1 , 1 9 8 8 .*p<.05
Reilly, JPEN 12:371, 1988
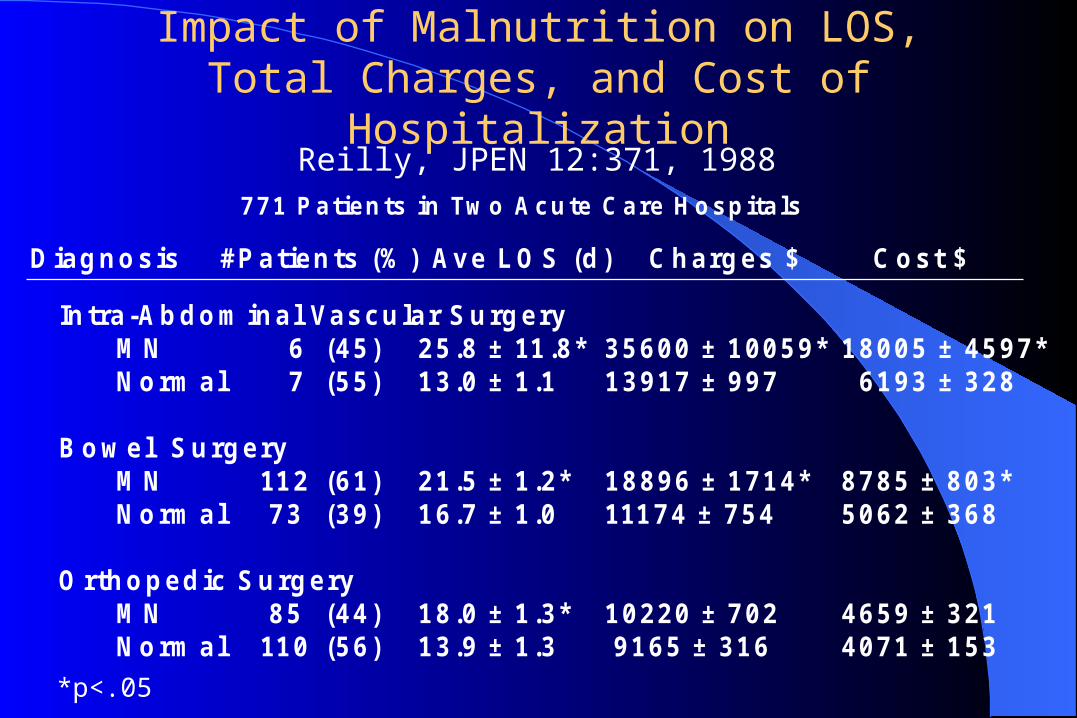
Impact of Malnutrition on LOS, Total Charges, and Cost of Hospitalization
In tra -A b d o m in a l Va s c u la r S u rg e ry M N 6 (4 5 ) 2 5 .8 ± 11 .8 * 3 5 6 0 0 ± 1 0 0 5 9 * 1 8 0 0 5 ± 4 5 9 7 * N o rm a l 7 (5 5 ) 1 3 .0 ± 1 .1 1 3 9 1 7 ± 9 9 7 6 1 9 3 ± 3 2 8
B o w e l S u rg e ry M N 11 2 (6 1 ) 2 1 .5 ± 1 .2 * 1 8 8 9 6 ± 1 7 1 4 * 8 7 8 5 ± 8 0 3 * N o rm a l 7 3 (3 9 ) 1 6 .7 ± 1 .0 111 7 4 ± 7 5 4 5 0 6 2 ± 3 6 8
O rth o p e d ic S u rg e ry M N 8 5 (4 4 ) 1 8 .0 ± 1 .3 * 1 0 2 2 0 ± 7 0 2 4 6 5 9 ± 3 2 1 N o rm a l 11 0 (5 6 ) 1 3 .9 ± 1 .3 9 1 6 5 ± 3 1 6 4 0 7 1 ± 1 5 3
7 7 1 P a tie n ts in Tw o A c u te C a re H o s p ita ls
R e illy e t a l., J P E N 1 2 :3 7 1 , 1 9 8 8 .
D ia g n o s is # P a t ie n ts (% ) Av e L O S (d ) C h a rg e s $ C o s t $
*p<.05
Reilly, JPEN 12:371, 1988

Impact of Malnutrition on LOS, Total Charges, and Cost of Hospitalization
For every DRG, the presence of malnutrition increased the mean LOS (1.1 to 12.8 excess days).
Average hospital cost increased by $1,738 and charges by $3,557 per patient.
A complication in a malnourished patient increased cost/charges by $2,996/$6,157.
Reilly, JPEN 12:371, 1988

Degree of Malnutrition and LOS
Status #Patients (%) Average LOS (days)
Normal 226 (45) 7.74Mild 94 (19) 8.18Moderate 45 (9) 9.71Severe 135 (27) 11.98
Messner et al. Society Gastroent Nurses & Assoc 202:205, 1981
500 Consecutive Patients Huntington VAMC
Messner, Gastroenterol Nurs 13:202, 1991 COPD, Cancer, Cardiovascular Disease, Alcoholism

Degree of Malnutrition and LOS
245 general surgery patients, 131 were found malnourished by Alb < 3.2 and recent weight loss > 10% (53%).
Colon Ca, Perforated Diverticular Disease, SBO, Gastric or Eso Ca.
LOSNormal 16.5 ± 10.7Malnourished 23.5 ± 16.5
Shaw-Stiffel, Nutrition 9:140, 1993

Degree of Malnutrition and LOS
173 medical patients in Metro Health Center, Cleveland, Ohio
LOS Hosp cost Self care
MN 6d* $6,196* 41%*
Normal 4d $4,563 66%
*p < .05
Chima, J Am Diet Assoc 97:975, 1997

Impact of Malnutrition on LOS and Total Hospitalization Charges
LOS Hospital charges
Alb <3.4 8.6d* $50,108*
Alb >3.4 5.2d $33,720
TLC <1200 5.7d* $42,098*
TLC > 1200 5.4d $32,544
Lavernia et al., J Am Coll Nutr 18:271, 1999
119 pts underwent hip or knee replacement
*p < 0.005

Can appropriate nutrition support treat and prevent malnutrition and reduce complications?

Anorexia NervosaSerial Assessments
0
50
100
150
200
250
1 3 5 7 9 11 13
Albumin x 10
Transferrin mg%
Weight pounds
Weeks

Crohn’s Disease

Enterocutaneous Fistulas

Impact of Refeeding on M&M
204 patients tested for DTHR to common antigens preoperatively
# Pts Sepsis Death
Anergic 12 17% 33%
Normal 192 4% 3%
MacLean, Ann Surg 186:241, 1977

Impact of Refeeding on M&M
60 anergic patients were given nutrition support preoperatively and re-tested for DTHR to common antigens.
# Pts Sepsis Death
Anergic 30 63% 67%
Normal 30 47% 6.7%
MacLean, Ann Surg 186:241, 1977

Impact of Refeeding on M&M
Prospective non-randomized study of 161 patients who, by physician preference, received 7-10 days of TPN prior to elective abdominal surgery or not.
Buzby, Surg Clin North Am 61:465, 1981

Nutrition Support in Burn Patients
Impact of nutrition support in 70 malnourished patients with 20% or more body surface burn.
Wt loss LOS Cost5% Dextrose 13% 36 $24,200Nutrition 3%* 29* $17,800*
Weinsier, J Burn Care Rehab 6:436, 1985
*p<.02

Postoperative Nutrition Support
35 non-malnourished patients after radical cystectomy for cancer were randomized to receive 7 days 5% dextrose or 7 days TPN postoperatively.
Ave. Hosp Days5% Dextrose 24TPN 17 (p<.002)
Askanazi, Ann Surg 203:236, 1986

VAMC Multicenter Study of Preoperative TPN
395 malnourished G&T patients were randomized to receive either 7-15 days of TPN or early surgery.
#Pts Complications
TPN 130 19.2%*
No TPN 265 36.6%
VA Trial, N Engl J Med 325:525, 1991
*p < .0005

How common is malnutrition in hospitalized patients?

Prevalence of Malnutrition
Blackburn, JAMA 230:858, 1974– 50% incidence in New England Deaconess Hospital,
Boston
Mullen, JPEN 1:39, 1977– 40% incidence in surgical patients at Philadelphia
VAMC Willcutts, JPEN 1:25, 1977
– 65% incidence in community hospital, Mass Coats, J Am Diet Assoc 93:27, 1989
– 46% of general medicine patients in teaching hospital

Prevalence of Malnutrition
VA Clinical Trial, N Engl J Med 325:525, 1991– 34% G&T surgery patients
Shaw-Stiffel, Nutrition 9:140, 1993– 53% general surgery patients Bridgeport Hosp, Conn
Guo, Br J Oral Maxillofac Surg 34:325, 1996– 35% in H&N Cancer patients in Beijing, China
Chima, J Am Diet Assoc 97:975, 1997– 32% of medical patients in Metro Health Center,
Cleveland, Ohio

Duke Nutrition Service In a one month period in 1997:
# Pts % At Risk
Medical 318 32
Surgical 209 31
Women/Peds 133 21
194 patients found at risk were recommend to undergo a full nutritional assessment.

Progression of Malnutrition
134 consecutive admissions to general medicine service at University of Alabama, Birmingham, underwent initial nutrition assessment and again at 2 weeks, if still hospitalized.
48% were initially malnourished.
69% were malnourished at 2 weeks.
Weinsier, Am J Clin Nutr 32:418, 1979

Progression of Malnutrition
Up to 70% of patients transferred from hospitals to long-term care facilities have evidence of malnutrition.
Federer, Am Diet Assoc, 1968
Does your hospital have an effective system to identify malnourished patients?

Duke Nutrition Service
Current method is an admission nutrition screen by the Nutrition Service (ward dietitians).
Evaluated if: a high risk diagnosis, high risk dietary order (cl liq, npo), or answer “yes” to any of the nutrition questions on the Universal Nursing Admission Form.

Duke Nutrition Service
Assessment is primarily a global evaluation and chart review.
Assessment is “hit and miss” depending on available chart data and dietitian time.

DRG Coding by Medical Records
In 1996, of 25,961 discharges, only 81 patients were coded as malnourished at the time of discharge.

DRG Coding by Medical Records
In 1996, of 25,961 discharges, only 81 patients were coded as malnourished at the time of discharge.
In 1997, of 26,386 discharges, 105 patients were coded as malnourished at the time of discharge.

DRG Coding by Medical Records
Assuming a 40% rate of malnutrition, DUMC fails to identify and report approximately 10,000 cases/year of malnutrition present at the time of discharge.

DRG Coding by Medical Records
Assuming a 40% rate of malnutrition, DUMC fails to identify and report approximately 10,000 cases/year of malnutrition present at the time of discharge.
When malnutrition is recorded as a comorbid condition, DRG reimbursement increases by an average of $2,436 per patient.

DRG Coding by Medical Records
Failure to recognize and document malnutrition at DUMC results in an loss in revenue of up to:*
10,000 Pts X $2,436/Pt =
$ 24,360,000 / year !
*Note: Multiple comorbidities reduce individual payments.

Is there a system in place in your hospital to ensure provision of appropriate nutrition care if patients are identified as malnourished?

Duke Nutrition “System”
There are over 51 different functional units providing nutrition care to DUMC patients.

Duke Nutrition Service (Dietary Services)Sarah W. Stedman Center for Nutritional StudiesGeriatric Research Education and Clinical CenterRice Diet Program/Heart Disease Reversal ClinicDuke Center for LivingDiet and Fitness CenterComprehensive Adult Diabetes ProgramComprehensive Cancer CenterEndocrinology ClinicMaternal-Fetal Medicine/High Risk ClinicCystic Fibrosis CenterLenox Baker Children’s HospitalRehabilitation CenterDialysis UnitClinical Research UnitPediatric Nutrition ServiceAdult Nutrition Service
Duke Nutrition System
There are over 51 different functional units providing nutrition care to DUMC patients.
There is no coordination between these units or between inpatient and outpatient nutrition care.

Duke Nutrition System
There are over 51 different functional units providing nutrition care to DUMC patients.
There is no coordination between these units or between inpatient and outpatient nutrition care.
There is no continuity of care, even during extended medical illnesses.

Results of Current System
Due to suboptimal recognition, recording, and treatment of malnutrition, the health system is: – Absorbing increased cost of care– Failing to receive appropriate
reimbursement– Not obtaining optimal patient
outcome

Proposal
Establish Clinical Nutritionas a well funded program
in most hospitals

Program StructureChairperson
Director, Adult NSSClinicalFaculty
Dietitian Coordinator
Adult NSS Team
TraumaCenter
DigestiveHealth
CysticFib/Pulm
Surgery Medicine RenalSolid Org
TransplantAdult BM
TransplantOncology
Tier 2RD's
ProgramDirector
Other
Tier 1RD's
NurseCoordinator

Clinical Nutrition Program Purpose
Nutrition care should be seen as a continuum.

Nutrition Care as a Continuum
Nutrition evaluation and care should begin with a patient’s initial contact with the health system.
– It should encompass outpatient management, inpatient care, and home based care, as needed.
Clinical Nutrition Program Purpose
Nutrition care should be seen as a continuum.
Nutrition care should be patient centered.

Patient Centered Care
Care should focus on:
– Enhanced quality of life
– Complication avoidance
– Maximization of functional outcome
– Cost containment
– And patient/family satisfaction

Clinical Nutrition Program Purpose
Nutrition care should be seen as a continuum.
Nutrition care should be patient centered.
Nutrition care should incorporate multidisciplinary expertise.

Multidisciplinary Expertise
Primary Care Physicians
Nurses
Pharmacists
Dietitians
Social Workers
Home Care Providers

Outpatient Activity
PatientScreening
PatientAssessment
Developmentof NutritionCare Plan
Implementationof NutritionCare Plan
Evaluation ofCare Setting
PatientMonitoring
PatientReassessmentand Updatingof NutritionCare Plan
OutpatientCare
Monitoring
Not at Risk
At Risk
AcuteInpatient
CareRequired
InpatientCare NotRequired
GoalsAchieved
Change inStatus
Monitor

Inpatient Activity
Admission
PatientScreening
PatientAssessment
Developmentof NutritionCare Plan
Implementationof NutritionCare Plan
Evaluation ofCare Setting
PatientMonitoring
PatientReassessmentand Updatingof NutritionCare Plan
DischargePlanning
Monitor
Not at RiskAt Risk
AcuteInpatient
CareRequired
InpatientCare NoLongerRequired
GoalsAchieved
Change inStatus
Monitor

Clinical Nutrition Program Activities
Develop and implement a program for nutritional screening of all patients in the health system.

Clinical Nutrition Program Activities
Develop and implement a program for nutritional screening of all patients in the health system.
All malnourished patients should be appropriately coded in the medical record to achieve optimal DRG reimbursement.

Clinical Nutrition Program Activities
Whenever possible, nutritional repletion should be undertaken early, especially prior to elective hospitalization.

Clinical Nutrition Program Activities
Ensure that nutrition care is given in the most cost effective and risk-free manner:
Dietary Modifications
Nutrition Supplements
Enteral Nutrition (gastric vs jejunal)
Total Parenteral Nutrition

Clinical Nutrition Program Activities
Work to minimize complications of nutrition support:
Sepsis
Nutrient Intolerance
Fluid and Electrolyte Imbalances
Nutrient Deficiencies
Mechanical Problems

Clinical Nutrition Program Activities Facilitate transition of patients into the
outpatient/home setting -- coordinate nursing, social work, physical therapy, and physician management with nutrition care.
To include:
– Home Total Parenteral Nutrition– and Home Enteral Nutrition
Conclusion
Craftsman Analogy

The Craftsman

A Portal to the Millennium
There is a major opportunity for a quantum jump in quality of health care if we more appropriately address and improve nutritional evaluation and status of our patients.
Clinical Nutrition Program

A Portal to the Millennium
We can be more effective health care providers if we can secure healthier patients to apply our judgment and skills.
The “new health care environment” will eventually force this move. We now have an opportunity to be the leaders and garner the benefits for our patients.
Clinical Nutrition Program

Nutritional Support in the Nutritional Support in the Next MillenniumNext Millennium
John P. Grant, MDDirector NSSDuke University Medical Center