objectives - allied health education
TRANSCRIPT

4/14/2014
1
Pharmacology and
Parkinson’s Disease:
What Every Therapist
Should Know
KIRK SEALE, PHARM D, MS
Disclosure
I have no actual or potentially relevant
financial relationship to disclose and no
conflict of interest in relation to this
program.
Objectives
Discuss the prevalence, the risk factors, and the diagnosis of Parkinson’s disease
Discuss the Clinical presentation of PD
Review common medications used to
treat PD
Examine medication strategies

4/14/2014
2
"The most humbling experience in my life has been
the time that I spent with families and with patients
suffering from Parkinson's..... time after time ...
we have uncovered simple issues and secrets that
have changed people's lives".
Michael S. Okum, MD University of Florida Center for Movement disorders
5,000
B.C.Mucuna Pruriens
"VELVET BEAN“
5,000 B.C.Mucuna Pruriens
"VELVET BEAN“

4/14/2014
3
http://visibleearth.nasa.gov/view_cat.php?scheme=COLLECTION
Risk Factors:
Advancing age
>60 y/o
Family history
first degree relative
Male’s White, Black, Hispanics
EnvironmentWillis AW, et al. Geographic and Ethnic Variation in Parkinson Disease: A Population-Based Study of US Medicare Beneficiaries,
Neuroepidemiology. 2010 April; 34(3): 143–151. Published online 2010 January 15
Diagnosis of Parkinson’s disease
No single method to make positive diagnosis
Relies heavily on
Risk factors
Medical / Medication history
Physical Exam

4/14/2014
4
DIAGNOSIS OF PARKINSON’S DISEASE
Progressive Supranuclear Palsy (PSP)
Multiple System Atropy (MSA)
Dementia with Lewy bodies (DLB)
Corticobasal Degeneration (CBD)
Multiple System Atropy (MSA)
Vascular Parkinsonism
DRUG INDUCED PARKINSONISM(pseudoparkinsonism)
Shin,HW, Chung SJ, Drug induced parkinsonism, J Clin Neurol. 2012 March; 8(1): 15–21.
Antipsychotics (Typical and Atypical)
METOCLOPRAMIDE (Reglan, Others)
Stimulants
SOME CALIUM CHANEL BLOCKERS
Nausea medications
Antiepileptic drugs
Reserpine- limited use
EXAMPLES:
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
SYMPTOMS OF
PARKINSON’S DISEASE
MOTOR SYMPTOMS NON-MOTOR
SYMPTOMS

4/14/2014
5
NON-MOTOR SYMPTOMS (C. A. P. S.)
Cognitive Disorders
Autonomic Dysfunction
Psychiatric Symptoms
Sleep Disorders
SYMPTOMS OF
PARKINSON’S DISEASE
MOTOR SYMPTOMS NON-MOTOR SYMPTOMS
_________________________
_________________________
_________________________
_________________________
_________________________
_C_______________________
_A_______________________
_P_______________________
_________________________
_S______________________
T.R.A.P.

4/14/2014
6
SYMPTOMS OF
PARKINSON’S DISEASE
MOTOR SYMPTOMS NON-MOTOR SYMPTOMS
_T________________________
_R________________________
_A________________________
_________________________
_P________________________
_C_______________________
_A_______________________
_P_______________________
_________________________
_S______________________
1) TREMOR
2) RIGIDITY
3) AKINESIA or
BRADYKINESIA
4) POSTURAL INSTABILITY
http://www.pharmacytimes.com/publications/issue/2010/March2010/FeatureParkinsons0310 Wick, Janette Y. Treating Parkinson's disease: The Pharmacist Role, Pharmacy Times, March 19, 2010.
MOTOR SYMPTOMS:
Begins:
Unilaterally
Localized
Non-purposeful movement
TREMOR
4/14/2014
7
Mr. B. described a “shaking” of his index
finger, however upon further Examination
you see a definite “pill rolling” of the index
finger and thumb.
PILL ROLLING TREMOR
COURTESY OF
http://www.youtube.com/watch?v=ZY1uEmgvp0U
RIGIDITY

4/14/2014
8
AKINESIA or BRADYKINESIA
A= Without, KINETIC = Movement
BRADY= Slow, KINETIC= Movement
Slowed movement and reaction times
Reflect repetitive movements
Irregular pattern with repetition
Appears to be related to the degree of
dopamine deficiency
Postural Instability
Impaired balance
Stiff muscles
Shuffling gait
Slowed reflexes
Occurs late in disease
Balance + gait training
PARKINSON’S DISEASE GAIT DEMONSTRATIONCourtsy of Yasser Metwally Professor of neurology
http://www.youtube.com/watch?v=j86omOwx0Hk&NR=1&feature=endscreen
4/14/2014
9
http://schoolworkhelper.net/parkinson%E2%80%99s-disease-symptoms-inheritance/
____________________________
_
_______________ ___
__________________
________________________
________
5 STAGES OF PARKINSON’S
STAGE ONE
STAGE TWO
STAGE THREE
STAGE FOUR
STAGE FIVE
______________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
______________________________________________
“MEDICATIONS ARE PROBABLY THE SINGLE MOST IMPORTANT HEALTH
CARE TECHNOLOGY IN PREVENTING
ILLNESS, DISABILITY AND DEATH IN
THE GERIATRIC POPULATION.”
Avorn J. Medication use and the elderly: current status and opportunities Health Affairs, 14, no. 1, (1995)

4/14/2014
10
© H
yb
rid M
edic
al
Anim
ati
on
© S
haro
n a
nd J
oel H
arr
is
Balance:
Acetylcholine
Dopamine

4/14/2014
11
Video Courtesy of Dr. Prodigious
http://www.youtube.com/watch?v=jyBakRkzswU
MEDICATION
THERAPY
Mr. B. is in good health and takes no medications.
Upon PE you notice there is a slight tremor of the head,
a stooped posture and he ambulates with slow
shuffling steps. He appears very unsteady.
His wife later confides in you that
He has been very forgetful lately and does not sleep well

4/14/2014
12
SYMPTOMS OF
PARKINSON’S DISEASE
MOTOR SYMPTOMS NON-MOTOR SYMPTOMS
_T____tremor______________
_R____rigidity?_____________
_A____bradykinesia_________
_________________________
_P____postural instability____
_C___________?___________
_A___________?___________
_P___________?___________
_________________________
_S___________?___________
MEDICATION TREATMENT
LEVODOPA (L-DOPA) Most commonly used
Most potent, most effective for PD
Usually combined with Carbidopa
(Sinemet).
Immediate release and Sustained release
Provides best symptomatic effects
Increases dopamine in the brain
CARbidopa

4/14/2014
13
Levodopa /Carbidopa (Sinemet) Side Effects
Nausea/ Vomiting
Drowsiness
Postural hypotension
Hallucinations / Very vivid dreams
Compulsive behavior
Anxiety, Nervousness, Agitation
Dyskinesias- usually with long-term use
Levodopa / Carbidopa
High protein diet interferes
with absorption
L-Dopa should be taken with: A) Carbidopa B) in the evening after
supperC) With a Big MacD) None of the above

4/14/2014
14
You are giving PT to Mr. B. currently taking L-Dopa/
Carbidopa for 5 years. He complains that his
medications seem to be less effective. The PD
symptoms reappear hours before the next scheduled dose
of his medications. This is referred to as?
A. FreezingB. Medication Non-Compliance
C. On-Off PhenomenonD. None of the above
ON-OFF PHASE VIDEO COURTESY OF
Professor Kurt Illig, University of Saint Thomas, St. Paul, MN
http://www.youtube.com/watch?v=sf1N0Zf5IqA

4/14/2014
15
On-Off Fluctuations
On period / Off period
Mornings or prior to next dose
High protein meals?
Timing is everything
Levodopa / Carbidopa
Immediate release – take 1 Hr after meals
Sustained release – with meals
ON-OFF treatment options:
Timing of medication
Diet
Release formulation
sustained vs immediate release
Other medications
Medication TreatmentDopamine Agonist
Can be used early in treatment
Generally used as add-on therapy to Levodopa/Carbidopa
Drugs most commonly used:
Primipexole (Mirapex)
Ropinirole (Requip, Requip XL)
Bromocriptine (Parlodel)
Apomorphone (Apokyn)- injection form only

4/14/2014
16
© S
haro
n a
nd J
oel H
arr
is
SIDE EFFECTS Dopamine Agonist
_____________________________
_____________________________
_____________________________
_____________________________
_____________________________
_____________________________
You are giving PT to a patient that has had PD for 7 years. You notice he is unable to move for short
periods of time. Even with encouragement he states “My feet feel like they are glued to the floor.” This PD phenomenon is referred to as:

4/14/2014
17
Freezing Of Gait
Disabling
May worsen as
disease progresses
Tend to occur
End of dosing interval
Can be unpredictable
Freezing of Gait Treatments:
Timing of medications
Dose increase
Dosing interval
Addition of other medications
MAO-B INHIBITORS
Eldepril (Selegiline)
Azilect (Rasagiline)
Help increase Dopamine in the brain

4/14/2014
18
© S
haro
n a
nd J
oel H
arr
is
Selegiline (Eldepril)
Eldepril (Selegiline)
May produce a wake enhancing effect
May lead to
Nervousness
Agitation
confusion
INSOMNIA
Take medication in AM.
SIDE EFFECTS MAO-B Inhibitors:
Insomnia – esp. with seleigline
Lightheadedness (postural hypotension)
Agitation
Vivid dreams
Hallucinations

4/14/2014
19
Freezing: Other Treatment Options:
Rhythmic auditory cues
Visual stimuli
Carrying out each sequence consciously
Use of correct walking aids
Use of correct footwear
Mr. B has been taking L-Dopa for more than 7 years plus
a dopamine agonist for his PD and Rasagiline for freezing episodes. During PT you notice abnormal involuntary movements of
his neck and arms. These abnormal involuntary movements are referred to as:
Video dyskinesia
Neal Hermanowicz, MDDepartment of NeurologyUniversity of California, Irvine
http://www.dailymotion.com/video/xgfy5m_parkinson-s-symptoms-what-is-dyskinesia_lifestyle#.UW7h2Mpu5_c

4/14/2014
20
NO EFFECT- off phase
DRU
G
CO
NCEN
TRATIO
N
TIME
DYKSINESIA OPTIONS:
TIMING??
Change in medication
Change in dosing
Other medications
Other treatments
Amantadine
Place in therapy:
Side effects Orthostatic hypotension
Edema of extremities
Confusion
Hallucinations
4/14/2014
21
COMT INHIBITORS
PREVENTING THE
PERIPHERAL BREAKDOWN
OF LEVODOPA
NEVER USED ALONE
DYSKINESIA, HYPERKINESIA
AND HALLUCINATIONS CAN
OCCUR
Anticholinergics:
Cogentin (Benztropine)
Artane (Trihexyphenidyl)
Limited use in the elderly
Side effects:
On the Horizon
Levodopa / Carbidopa ER Capsule (Rytary®)
•Pending FDA approval
• Novel formulation and dosage
• Immediate and ER components
• Longer duration of action
36.25/145 mg, 61.25/245 mg, 97.50/390 mg
• Early to Advanced PD
4/14/2014
22
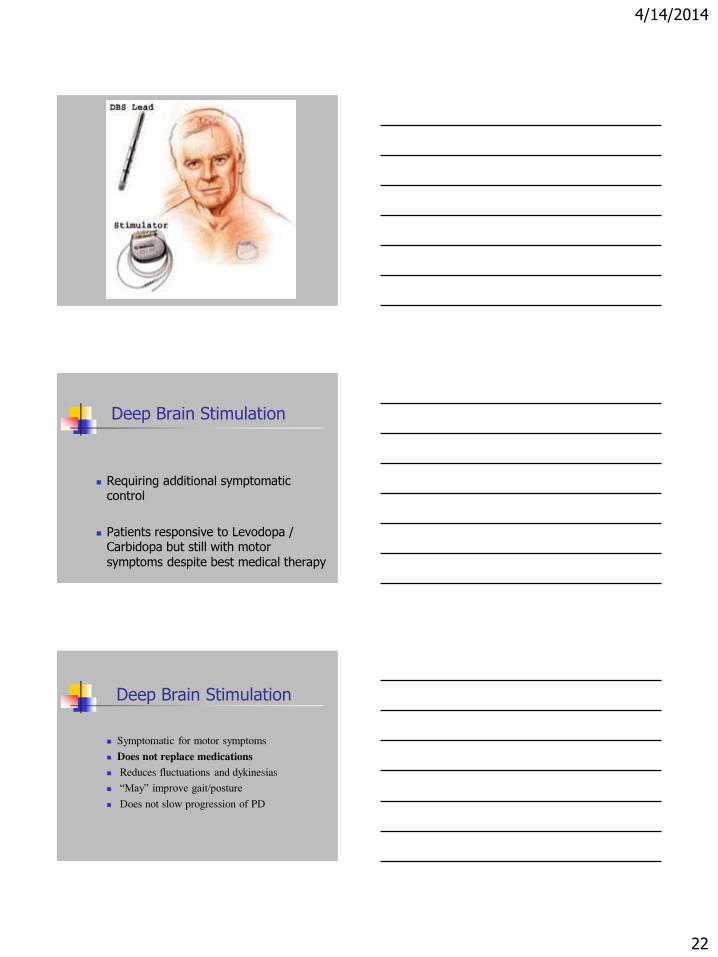
Deep Brain Stimulation
Requiring additional symptomatic control
Patients responsive to Levodopa / Carbidopa but still with motor
symptoms despite best medical therapy
Deep Brain Stimulation
Symptomatic for motor symptoms
Does not replace medications
Reduces fluctuations and dykinesias
“May” improve gait/posture Does not slow progression of PD

4/14/2014
23
BALANCE
“My point is, life is about balance.
The good and the bad.
The highs and the lows.
The pina and the colada.”