objectives - reachereache.info/wp-content/uploads/2015/03/low.conf_.-handouts.pdf · chair division...
TRANSCRIPT

3/18/2015
1
Promoting Healthy Physiologic Birth to Prevent Cesareans:
“It takes a village"
Lisa Kane Low PhD CNM FACNM FAANAssociate ProfessorSchool of Nursing
University of MichiganChair Division of Standards and Practice ACNM
This is an abridged slide set, absent many of the photos/images that will be used to support discussion and some of the animation of text that is
used to address some points.For a full set, you can email me at
Objectives1. Discuss the use of professional organization position statements from ACOG and U.S. midwifery organizations (ACNM, MANA, NACPM) which promote new models of care to reduce cesarean and promote healthy physiologic birth, to advocate for and implement change in maternity care units. 2. Describe care practices associated with promoting physiological birth by all members of the maternity care team. 3. List specific features of collaboration that promote implementation of physiologic birth care practices. 4. Describe opportunities to enhance collaboration among all maternity care team members to advocate for care practices to promote physiologic childbirth. 5. Identify key resources and tools to use that improve opportunities for collaborative approaches to supporting and promoting physiologic birth care practices (e.g. fetal monitoring, progress in labor, using doulas and spontaneous pushing in second stage).
• Up to one‐third of elective deliveries occur prior to documented fetal maturity.
• 53% of the disparity in cesarean section is related to labor induction and early admission.
• Patient centered care is talked about but rarely practiced.
• Communication errors are the leading primary cause of perinatal sentinel events.
• Up to 90% of birth trauma is preventable.
• Maternal Mortality in the US has increased at an annual rate of 2.1% for the last 20 years.
Cherouny, 2011 IHI

3/18/2015
2
To Err is Human
• Rates of injury due to medical error have remained essentially unchanged between 2000‐2008 at 10 NC hospitals (Landrigan et. al. 2010)
• Inspector General DHHS Medicare patients experienced substantial harm in U.S. hospitals in 2008 (Levinson, 2010)
• 1/3 patients are harmed during their hospital stay and traditional approaches to measuring adverse events, underestimate the safety breeches. (Classen, et.al, 2010).
Quality patient care in labor and delivery: A call to action. J Midwifery Womens Health. 2012;57(2):112‐113.

3/18/2015
3
Highly technological procedures in childbirth have been normalized without an associated improvement in outcomes.
Many different countries have created statements defining and describing “normal” birth, yet at that time, the U.S. did not have a similar, consensus‐driven statement about this fundamental concept in birth.
Context of “Normal Birth”
LTM III Initial Report www.childbirthconnection.org
A shared culture of dialogue, collaboration, and teamwork
United States Context
3 major midwifery organizations in the U.S.
History of independent action, not collaboration.
“Normal birth” was an idea we ALL could be passionate about!
Rationale for Creating the Statement
Midwives, as guardians of normal birth, are uniquely positioned to create this statement.
Need increased clarity and standardization to operationalize the concepts of “normal birth” in research & practices.
Increased clarity around the definition of normal birth may positively impact consultation and collaboration with other maternity care providers.
Develop a consensus statement to:
Provide a succinct definition of normal physiologic birth;
Identify measurable benchmarks to describe optimal processes and outcomes reflective of normal physiologic birth;
Identify factors that facilitate or disrupt normal physiologic birth based on the best available evidence;
Purpose

3/18/2015
4
Develop a consensus statement to:
Create a template for system changes in clinical practice, education, research, and health policy;
Improve the health of mothers and infants, while avoiding unnecessary and costly interventions.
Purpose
Definition of normal, physiologic birth: “A normal physiologic labor and birth is one that is powered by the innate human capacity of the woman and fetus”‐ accompanied by evidence based care.
Physiologic Birth is Characterized by
• Spontaneous onset and progression of labor;
• Includes biological and psychological conditions that promote effective labor;
• Results in the vaginal birth of the infant and placenta;
• Results in physiological blood loss;
• Facilitates optimal newborn transition through skin‐to‐skin contact and keeping the mother and infant together during the postpartum period; and
• Supports early initiation of breastfeeding.
Physiologic Birth is Disrupted by• induction or augmentation of labor; • an unsupportive environment, i.e., bright lights, cold room,
lack of privacy, multiple providers, lack of supportive companions, etc.;
• time constraints, including those driven by institutional policy and/or staffing;
• nutritional deprivation, e.g., food and drink; • opiates, regional analgesia, or general anesthesia; • episiotomy; • operative vaginal (vacuum, forceps) or abdominal
(cesarean) birth• immediate cord clamping; • separation of mother and infant; • and/or any situation in which the mother feels threatened
or unsupported.
For the woman:• Her individual health status and physical fitness; • Autonomy and self‐determination in childbirth; • Personal knowledge and confidence about birth, including cultural beliefs, norms, and practices and education about the value of normal physiologic birth;
• Fully informed, shared decision‐making; and • Access to health care systems, settings, and providers supportive of and skilled in normal physiologic birth.
For the Clinician:• Education, knowledge, competence, skill, and confidence in supporting physiologic labor and birth, including helping women cope with pain;
• Commitment to working with women through education to enhance their confidence in birth and diminish their fear of the process;
• Commitment to shared decision making; and
• Working within an infrastructure supportive of normal physiologic birth.

3/18/2015
5
For the Birth Setting:• Access to midwifery care for each woman; • Adequate time for shared decision making with freedom
from coercion; • No inductions or augmentations of labor without an
evidence‐based clinical indication; • Encouragement of nourishment (food and drink) during
labor as the woman desires; • Freedom of movement in labor and the woman’s choice of
birth position; • Intermittent auscultation of heart tones during labor unless
continuous electronic monitoring is clinically indicated; • Maternity care providers skilled in non‐pharmacologic
methods for coping with labor pain for all women; • Care that supports each woman’s comfort, dignity, and
privacy; and• Respect for each woman’s cultural needs.
Policy Recommendations:• Introduction of policies into hospital settings to support
normal physiologic birth; • Comprehensive examination and dissemination of the
evidence and care practices supportive of normal physiologic birth;
• Midwifery care as a key strategy to support normal physiologic birth
• Increasing the midwife workforce and enhancing regulations and funding strategies to support their practice;
• Competency‐based, inter‐disciplinary education programming for maternity health care clinicians and students on the application of care that promotes normal physiologic birth; and (see the Normal Birth Summit Statement)
• Development of a future research agenda on short and long‐term effects of normal physiologic birth.
AWHONN: The Role of the NurseThe support provided by the RN should include the following:• Assessment and management of the physiologic and
psychological processes of labor; • Facilitation of normal physiologic processes, such as the
women’s desire for movement in labor (Shilling, 2009);• provision of physical comfort measures, emotional and
informational support and advocacy (Adams & Bianchi, 2008);
• evaluation of fetal well‐being during labor; • instruction regarding the labor process; • role modeling to facilitate family participation during labor
and birth; direct collaboration with other members of the health care team to coordinate patient care.
Nurse Sensitive Quality Indicators• Triage of a Pregnant Woman and Her Fetus(es)• 02: Second Stage of Labor: Mother‐Initiated, Spontaneous Pushing• 03: Skin‐to‐Skin is Initiated Immediately Following Birth• 04: Duration of Uninterrupted Skin‐to‐Skin Contact.• 05: Eliminating Supplementation of Breast Milk Fed Healthy, Term
Newborns• 06: Protect Maternal Milk Volume for Premature Infants Admitted
to NICU• 07: Initial Contact with Mothers Following a Neonatal Transport • 08: Perinatal Grief Support • 09: Women’s Health and Wellness Coordination throughout the Life
Span• 10a: Labor Support Measure • 10b: Partial Labor Support• 11: Freedom of Movement during Labor
AWHONN 2014
Promoting Evidence Based CareObjectives
1. Discuss the use of professional organization position statements from ACOG and U.S. midwifery organizations (ACNM, MANA, NACPM) which promote new models of care to reduce cesarean and promote healthy physiologic birth, to advocate for and implement change in maternity care units. 2. Describe care practices associated with promoting physiological birth by all members of the maternity care team. 3. List specific features of collaboration that promote implementation of physiologic birth care practices. 4. Describe opportunities to enhance collaboration among all maternity care team members to advocate for care practices to promote physiologic childbirth. 5. Identify key resources and tools to use that improve opportunities for collaborative approaches to supporting and promoting physiologic birth care practices (e.g. fetal monitoring, progress in labor, using doulas and spontaneous pushing in second stage).

3/18/2015
6
Physiologic Care Practices
Phase of Physiologic Birth Associated Physiologic Care Practices
Spontaneous labor onset ‐ Avoid induction of labor when non‐indicated ‐ Shared decision making for preference‐sensitive
indications
Spontaneous progression of labor ‐ Encourage mobility‐ Continuous support (doula)‐ Comfort‐ Evidence‐based standards for augmentation
Physiologic second stage ‐ Encourage mobility, non‐supine positioning‐ Maternal‐directed pushing
Physiologic dyad transition ‐ Continuous skin‐to‐skin contact‐ Physiologic cord closure‐ Early breastfeeding and attachment
Joint Commission: Perinatal Care
• PC‐01 Elective Delivery
• PC‐02 Cesarean Section
• PC‐03 Antenatal Steroids
• PC‐04 Health Care‐Associated Bloodstream Infections in Newborns
• PC‐05 Exclusive Breast Milk Feeding
Improvable with Physiologic Care
Core Measure Set
Providers of Maternity Care:Roles in Promoting Physiologic Birth
Care Practice Associated with Dec Cesarean
Objectives1. Discuss the use of professional organization position statements from ACOG and U.S. midwifery organizations (ACNM, MANA, NACPM) which promote new models of care to reduce cesarean and promote healthy physiologic birth, to advocate for and implement change in maternity care units. 2. Describe care practices associated with promoting physiological birth by all members of the maternity care team. 3. List specific features of collaboration that promote implementation of physiologic birth care practices. 4. Describe opportunities to enhance collaboration among all maternity care team members to advocate for care practices to promote physiologic childbirth. 5. Identify key resources and tools to use that improve opportunities for collaborative approaches to supporting and promoting physiologic birth care practices (e.g. fetal monitoring, progress in labor, using doulas and spontaneous pushing in second stage).

3/18/2015
7
Optimal Models of Care:
• Members of the village……
Paradigms
• Collective support
• Working together
• Contributing to explanatory power
• Synergist effects vs competing paradigms

3/18/2015
8
Objectives1. Discuss the use of professional organization position statements from ACOG and U.S. midwifery organizations (ACNM, MANA, NACPM) which promote new models of care to reduce cesarean and promote healthy physiologic birth, to advocate for and implement change in maternity care units. 2. Describe care practices associated with promoting physiological birth by all members of the maternity care team. 3. List specific features of collaboration that promote implementation of physiologic birth care practices. 4. Describe opportunities to enhance collaboration among all maternity care team members to advocate for care practices to promote physiologic childbirth. 5. Identify key resources and tools to use that improve opportunities for collaborative approaches to supporting and promoting physiologic birth care practices (e.g. fetal monitoring, progress in labor, using doulas and spontaneous pushing in second stage).

3/18/2015
9
Who decides on the type or process for assessment of fetal well being?
3/18/2015
10
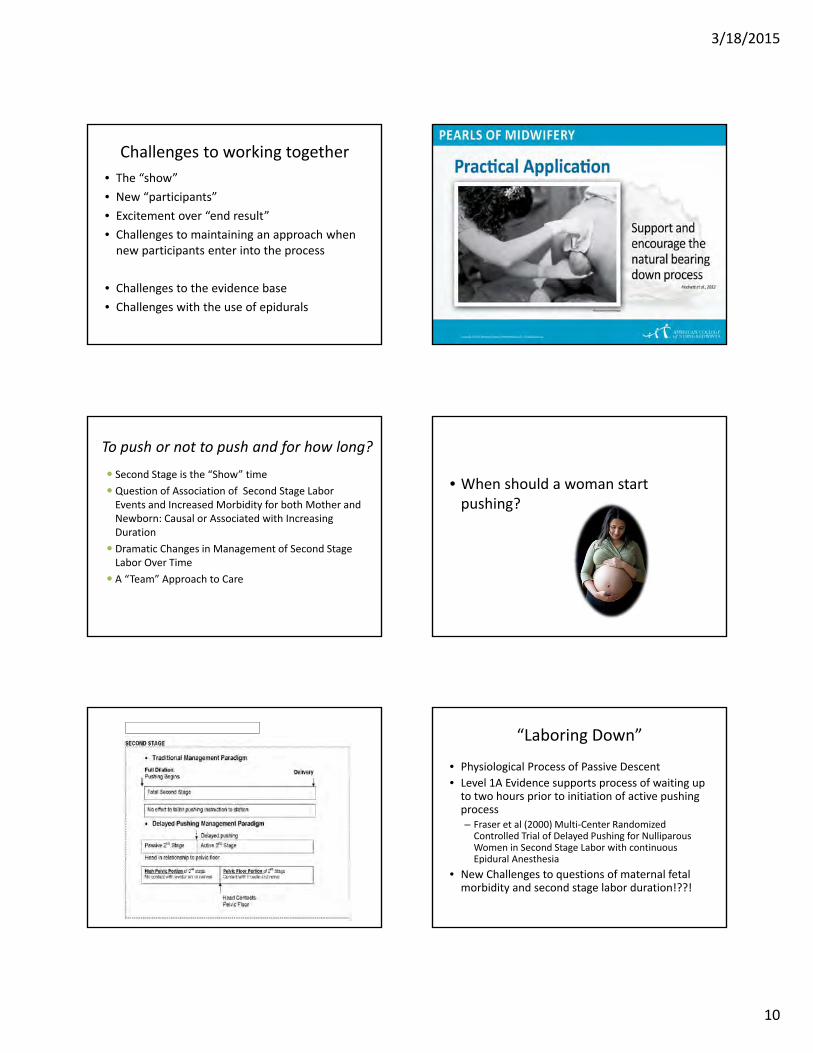
Challenges to working together
• The “show”
• New “participants”
• Excitement over “end result”
• Challenges to maintaining an approach when new participants enter into the process
• Challenges to the evidence base
• Challenges with the use of epidurals
To push or not to push and for how long?
Second Stage is the “Show” time
Question of Association of Second Stage Labor Events and Increased Morbidity for both Mother and Newborn: Causal or Associated with Increasing Duration
Dramatic Changes in Management of Second Stage Labor Over Time
A “Team” Approach to Care
• When should a woman start pushing?
Comparison of 2nd stage management “Laboring Down”
• Physiological Process of Passive Descent
• Level 1A Evidence supports process of waiting up to two hours prior to initiation of active pushing process– Fraser et al (2000) Multi‐Center Randomized Controlled Trial of Delayed Pushing for Nulliparous Women in Second Stage Labor with continuous Epidural Anesthesia
• New Challenges to questions of maternal fetal morbidity and second stage labor duration!??!

3/18/2015
11
Effect of Laboring Down on Time Does laboring down increase the second stage duration in total…sometimes
Increased total time, decreased active pushing time
> active pushing associated with changes in pH and maternal fatigue
Yet increased duration does not have negative effect on newborn outcomes
Focus is on active pushing time….which sometimes we initiate as providers
Positions to overcome pelvic constraints Duration of Second Stage
• How much time for overall pushing is too long
• Studies of Pelvic Floor Damage (Levator AniMuscle Tear on MRI) correlated with prolonged second stage >2.5 hours
» Kearney et al OB/GYN Jan 2006
• Confounding Variables and Cascade Effects
Delayed Pushing and Duration
Secondary Analysis of PEOPLE RCT comparing delayed to immediate onset pushing in the presence of an epidural
N= 1862
No negative neonatal effects with inc duration AFTER controlling for confounding factors
Maternal Morbidity inc sig after 2 hours for IP fever, and PPH

3/18/2015
12
Probability of NSVD with inc duration of second stage labor
Probability of spont vaginal delivery with well infant
(apgar/pH) decreases every hour of active pushing that passes
1‐2 hr OR 0.4; 95% CI 0.3‐0.62‐3 hr OR 0.1: 95% CI 0.09‐0.2;>3 hr OR 0.03; 95% CI 0.02‐0.05
Questions whether a woman should be encouraged to continue
to push after 2 hours of active pushing
without evidence of imminent delivery
Duration conclusions

3/18/2015
13
“If Doulas were a drug they would be required for all pregnant women”Penny Simkin
Epi-DOULA
What Collaboration does and dose not look like
• Support to Collaboration • Barriers to Collaboration
Picking the Model to Meet the Unique Needs Of
Women and Their Families in Their Communities

3/18/2015
14
Doing the “Labor Progress Dance”
Resources and Tools
Three Pronged Approach
Promoting Physiologic Birth as a Value Added Proposition to Health Care
Organizations and Systems

3/18/2015
15
• Audience– Clinicians and staff in the hospital setting– Maternity unit and health system leadership
• Goal– implement care process improvements that support, promote, and facilitate physiologic birth through dissemination of useful, actionable resources and case examples.
BirthTOOLS :Menu of Change
• For each focal area, the toolkit will include:
– review of evidence
– model unit policies
– clinical decision support tools (e.g. algorithms, checklists)
– guidelines and tools for auditing performance
– educational resources for clinicians and/or consumers
3/18/2015
16

3/18/2015
17
Promoting Physiologic Approaches to
Improve the Process and the Outcomes of Care for Mothers and
Babies

1
SUPPORTING HEALTHY AND NORMAL PHYSIOLOGIC CHILDBIRTH:
A CONSENSUS STATEMENT BY ACNM, MANA, AND NACPM∗
In 1996, the World Health Organization called for the elimination of unnecessary intervention in childbirth, 1 yet currently there are few resources to assist maternity care providers in achieving this goal. The purpose of this consensus statement is to explicitly identify key benchmarks of safe, healthy, and normal physiologic childbirth. This statement will assist maternity care providers, women, policymakers, and payers to protect, promote, and support human childbearing physiology and to avoid overuse of interventions, thus achieving better care, better health, and lower costs. This consensus statement represents the work of a task force comprised of representatives from three U.S. midwifery organizations whose members are experts on supporting women’s innate capacities to birth, and was externally reviewed by maternity care organizations and leaders. The specific aims of the consensus statement are to
• Provide a succinct definition of normal physiologic birth; • Identify measurable benchmarks to describe optimal processes and outcomes reflective of
normal physiologic birth; • Identify factors that facilitate or disrupt normal physiologic birth based on the best
available evidence; • Create a template for system changes through clinical practice, education, research, and
health policy; and • Ultimately improve the health of mothers and infants, while avoiding unnecessary and
costly interventions. This statement is placed in the context of the current, widespread application of technological interventions that lack scientific evidence to a primarily healthy birthing population .2 The use of obstetric interventions in labor and birth has become the norm in the United States. More than half of all pregnant women receive synthetic oxytocin to induce or augment labor,3 which demands additional interventions to monitor, prevent, or treat side effects. Nationally, one third of women deliver their babies via cesarean,4 a major abdominal surgery with potential for serious short- and long-term health consequences. For the mothers these consequences include, but are ∗ Note. ACNM=American College of Nurse-Midwives, http://www.midwife.org/; MANA=Midwives Alliance of North America, http://mana.org/; NACPM=National Association of Certified Professional Midwives, http://www.nacpm.org/. This document is intended for health care professionals and policymakers. A companion document for consumers is in development.

2
not limited to, postoperative infections, chronic pain, future cesarean births, and placental complications that can lead to hemorrhage, hysterectomy, and rarely, death.5,6 Infant risks include respiratory distress,7 and in subsequent pregnancies maternal risks include increased likelihood of preterm birth and associated morbidity and mortality. 8-12 Regardless of intervention or outcome, childbearing care perceived by the woman as disrespectful or traumatic is more likely to be associated with maternal psychological morbidity and potential for disrupted mother-infant attachment .13-16 Defining the normal physiology of childbirth This statement is grounded in scientific evidence and based on definitions drawn from the 2012 version of the Oxford English Dictionary, in which “normal” refers to typical or usual--a standard, and “physiology” refers to the functional processes of an organism, organ, or system. Thus, normal human physiology provides a framework to understand the optimal functioning of childbirth. For the purposes of this statement, birth includes the three stages of labor, the newborn transition, and the first hour after birth. A normal physiologic labor and birth is one that is powered by the innate human capacity of the woman and fetus. This birth is more likely to be safe and healthy because there is no unnecessary intervention that disrupts normal physiologic processes .17 Some women and/or fetuses will develop complications that warrant medical attention to assure safe and healthy outcomes. However, supporting the normal physiologic processes of labor and birth, even in the presence of such complications, has the potential to enhance best outcomes for the mother and infant.18-21
Normal physiologic childbirth • is characterized by spontaneous onset and progression of labor; • includes biological and psychological conditions that promote effective labor; • results in the vaginal birth of the infant and placenta; • results in physiological blood loss;22 • facilitates optimal newborn transition through skin-to-skin contact and keeping the
mother and infant together during the postpartum period; and • supports early initiation of breastfeeding.1
The following factors disrupt normal physiologic childbirth:
• induction or augmentation of labor;23-25 • an unsupportive environment, i.e., bright lights, cold room, lack of privacy, multiple
providers, lack of supportive companions, etc.;26,27 • time constraints, including those driven by institutional policy and/or staffing;28 • nutritional deprivation, e.g., food and drink;29 • opiates, regional analgesia, or general anesthesia;30,31 • episiotomy;32,33 • operative vaginal (vacuum, forceps) or abdominal (cesarean) birth;6,34 • immediate cord clamping;35-37 • separation of mother and infant;38 and/or • any situation in which the mother feels threatened or unsupported.39

3
The mechanisms and outcomes of physiologic childbirth Normal physiologic labor and birth has positive short- and long-term health implications for the mother and infant. Optimal physiologic function of the neuroendocrine system enhances the release of endogenous oxytocin and beneficial catecholamines in response to stress.40,41 These hormones promote effective labor patterns and protective physiologic responses, including enhanced endorphin levels, facilitation of cardio-respiratory transition and thermoregulation of the newborn, successful lactation, and enhanced bonding behavior between the mother and infant.38,42-44 When there is optimal physiologic functioning, women are less likely to require interventions to artificially augment labor, which can potentially interfere with their ability to cope with pain.44-47 When labor progresses spontaneously there is a reduced likelihood of fetal compromise or need for instrumental/surgical intervention.48 For most women, the short-term benefits of normal physiologic birth include emerging from childbirth feeling physically and emotionally healthy and powerful as mothers. Their infants will benefit from the ability of their mothers to respond to their needs and from the lack of exposure to medications that can affect neurological behavior. Long-term outcomes include beneficial effects for the woman’s physical and mental health and capacity to mother, enhanced infant growth and development, and potentially diminished incidence of chronic disease.49-56 Together, these outcomes are beneficial to the family and society through enhanced family functioning and cost effective care. Importantly, a focus on these aspects of normal physiologic birth will help to change the current discourse on childbirth as an illness state where authority resides external to the woman to one of wellness in which women and clinicians share decisions and accountability.57 Factors that influence normal physiologic childbirth There are multiple factors that influence the ability of a woman to give birth without intervention. These include the following: For the woman:
• Her individual health status and physical fitness; • Autonomy and self-determination in childbirth;58 • Personal knowledge and confidence about birth, including cultural beliefs, norms, and
practices and education about the value of normal physiologic birth;59 • Fully informed, shared decision-making; and • Access to health care systems, settings, and providers supportive of and skilled in normal
physiologic birth.60 For the clinician:
• Education, knowledge, competence, skill, and confidence in supporting physiologic labor and birth, including helping women cope with pain;
• Commitment to working with women through education to enhance their confidence in birth and diminish their fear of the process;
• Commitment to shared decision making; and • Working within an infrastructure supportive of normal physiologic birth.60

4
For the birth setting and environment:
• Access to midwifery care for each woman;18 • Adequate time for shared decision making with freedom from coercion; • No inductions or augmentations of labor without an evidence-based clinical indication;24 • Encouragement of nourishment (food and drink) during labor as the woman desires;61 • Freedom of movement in labor and the woman’s choice of birth position; • Intermittent auscultation of heart tones during labor unless continuous electronic
monitoring is clinically indicated;62 • Maternity care providers skilled in non-pharmacologic methods for coping with labor
pain for all women;63 • Care that supports each woman’s comfort, dignity, and privacy; and • Respect for each woman’s cultural needs.
Recommendations for policy, education, and research to promote normal physiologic childbirth include, but are not limited to, the following:
• Introduction of policies into hospital settings to support normal physiologic birth; • Comprehensive examination and dissemination of the evidence and care practices
supportive of normal physiologic birth; • Midwifery care as a key strategy to support normal physiologic birth • Increasing the midwife workforce and enhancing regulations and funding strategies to
support their practice; • Competency-based, inter-disciplinary education programming for maternity health care
clinicians and students on the application of care that promotes normal physiologic birth; and (see the Normal Birth Summit Statement)
• Development of a future research agenda on short and long-term effects of normal physiologic birth.2,64
Approved by the Boards of Directors of ACNM, MANA and NACPM, April 2012 Released May 14, 2012

5
REFERENCES
1. World Health Organization. Care in Normal Birth: A Practical Guide. World Health Organization; 1996.
2. Sakala C, Corry MP. Evidence-based maternity care: what it is and what it can achieve. New York, NY: Milbank Memorial Fund; 2008.
3. Declercq ER, Sakala C, Corry MP, et al. Listening to mothers II: Report of the Second National U.S. Survey of Women’s Childbearing Experiences. New York: Childbirth Connection; 2006.
4. Martin JA, Hamilton BE, Ventura SJ, et al. Births: preliminary data for 2010. Natl Vital Stat Rep. 2011; 60(2):1-25.
5. Guise JM, Eden K, Emeis C, et al. Vaginal birth after cesarean: new insights. Evidence report/technology assessment no.191. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
6. Koroukian SM. Relative risk of postpartum complications in the Ohio Medicaid population: vaginal versus cesarean delivery. Med Care Res Rev. 2004; 61(2):203-224.
7. Hansen AK, Wisborg K, Uldbjerg N, et al. Elective caesarean section and respiratory morbidity in the term and near-term neonate. Acta Obstet Gynecol Scand. 2007; 86(4):389-394.
8. Bager P, Wohlfahrt J, Westergaard T. Caesarean delivery and risk of atopy and allergic disease: meta-analyses. Clin Exp Allergy. 2008; 38(4):634-642.
9. Galyean AM, Lagrew DC, Bush MC, et al. Previous cesarean section and the risk of postpartum maternal complications and adverse neonatal outcomes in future pregnancies. J Perinatol. 2009; 29(11):726-730.
10. Kennare R, Tucker G, Heard A, et al. Risks of adverse outcomes in the next birth after a first cesarean delivery. Obstet Gynecol. 2007; 109(2 Pt 1):270-276.
11. Osborne C, Ecker JL, Gauvreau K, et al. First birth cesarean and risk of antepartum fetal death in a subsequent pregnancy. J Midwifery Womens Health. 2012; 57(1):12-17. doi:10.1111/j.1542-2011.2011.00142.x; 10.1111/j.1542-2011.2011.00142.x
12. Richter R, Bergmann RL, Dudenhausen JW. Previous caesarean or vaginal delivery: which mode is a greater risk of perinatal death at the second delivery? Eur J Obstet Gynecol Reprod Biol. 2006; 132(1):51-7.
13. Beck CT. Birth trauma: in the eye of the beholder. Nurs Res. 2004; 53(1):28-35. 14. Beck CT, Watson S. The impact of birth trauma on breastfeeding: a tale of two
pathways. Nurs Res. 2008; 57(4):228-236. 15. Beck CT. The anniversary of birth trauma: failure to rescue. Nurs Res. 2006; 55(6):
381-390. 16. Beck CT. Post-traumatic stress disorder due to childbirth: the aftermath. Nurs Res,
2004; 53(4):216-224. 17. Romano AM, Lothian JA. Promoting, protecting, and supporting normal birth: A look
at the evidence. J Obstet Gynecol Neonatal Nurs. 2008; 37(1):94-105. doi:10.1111/j.1552-6909.2007.00210.x
18. Hatem M, Sandall J, Devane D, et al. Midwife-led versus other models of care for childbearing women. Cochrane Database Syst Rev. 2008; Oct 8(4):CD004667.
19. Cragin L, Kennedy HP. Linking obstetric and midwifery practice with optimal outcomes. J Obstet Gynecol Neonatal Nurs. 2006; 35(6):779-785.

6
20. Murphy PA, Fullerton JT. Development of the optimality index as a new approach to evaluating outcomes of maternity care. J Obstet Gynecol Neonatal Nurs. 2006; 35(6):770-778.
21. Low LK, Seng JS, Miller JM. Use of the optimality index-United States in perinatal clinical research: a validation study. J Midwifery Womens Health. 2008; 53(4):302-309.
22. Dixon L, Fullerton JT, Begley C, et al. Systematic review: the clinical effectiveness of physiological (expectant) management of the third stage of labor following a physiological labor and birth. Int J Childbirth. 2011; 1(3):179-195.
23. Clark SL, Simpson KR, Knox GE, et al. Oxytocin: new perspectives on an old drug. Am J Obstet Gynecol. 2009; 200(1):35.e1-35.e6.
24. Mozurkewich E, Chilimigras JL, Berman DR, et al. Methods of induction of labour: a systematic review. BMC Pregnancy Childbirth. 2011; 11(84):1-19.
25. Smyth RM, Alldred SK, Markham C. Amniotomy for shortening spontaneous labour. Cochrane Database Syst Rev. 2007; Oct 17(4):CD006167.
26. Hodnett, ED, Downe, S, Walsh, D, et al. Alternative versus conventional institutional settings for birth. Cochrane Database Syst Rev. 2010; Sep (9):CD000012.
27. Hodnett ED, Gates S, Hofmeyr, GJ, et al. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2011; Feb 16(2):CD003766.
28. Zhang J, Troendle J, Reddy UM, et al. Contemporary cesarean delivery practice in the United States. Am J Obstet Gynecol. 2010; 203(4):326.e1-326.e10. doi:10.1016/j.ajog.2010.06.058
29. Singata M, Tranmer J, Gyte GM. Restricting oral fluid and food intake during labour. Cochrane Database Syst Rev. 2010; Jan 20(1):CD003930.
30. Bricker L, Lavender T. Parenteral opioids for labor pain relief: a systematic review. Am J Obstet Gynecol. 2002; 186(Suppl 5):S94-109.
31. Anim-Somuah M, Smyth RM, Jones L. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2011; Dec 7(12):CD000331.
32. Carroli, G., & Mignini, L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009; Jan 21(1):CD000081.
33. Viswanathan M, Hartmann K, Palmieri R, et al. The Use of Episiotomy in Obstetrical Care: A Systematic Review. Evidence reports/technology assessments, No. 112. Rockville,MD: Agency for Healthcare Research and Quality; 2005.
34. Demissie K, Rhoads GG, Smulian JC, et al. Operative vaginal delivery and neonatal and infant adverse outcomes: population based retrospective analysis. BMJ. 2004;329(7456):24-29.
35. Hutton EK, Hassan ES. Late vs early clamping of the umbilical cord in full-term neonates: systematic review and meta-analysis of controlled trials. JAMA. 2007;297(11):1241-1252.
36. Erickson-Owens DA, Mercer JS, Oh W. Umbilical cord milking in term infants delivered by cesarean section: a randomized controlled trial. J Perinatol. 2011; Nov 17. doi: 10.1038/jp.2011.159. [Epub ahead of print]
37. Mercer JS, Vohr BR, Erickson-Owens DA, et al. Seven-month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping. J Perinatol. 2010;30(1):11-16.
38. Moore E, Anderson G, Bergman N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2007;Jul 18(3):CD003519.
7
39. Beck CT. Birth trauma and its sequelae. J Trauma Dissociation . 2009;10(2), 189-203. 40. Bacigalupo G, Riese S, Rosendahl H, et al. (1990). Quantitative relationships between
pain intensities during labor and beta-endorphin and cortisol concentrations in plasma decline of the hormone concentrations in the early postpartum period. J Perinat Med. 1990;18(4):289-296.
41. Hoffman DI, Abboud TK, Haase HR, et al. Plasma beta-endorphin concentrations prior to and during pregnancy, in labor, and after delivery. Am J Obstet Gynecol. 1984;150(5 Pt 1):492-496.
42. Fourer M. Creating birth space to enable undisturbed birth. In Fahy K, Fourer M, Hastie, C, eds. Birth Territory and Midwifery Guardianship. Theory for Practice, Education and Research. New York, NY: Elsevier; 2008:57-77.
43. Unväs-Moberg K. The Oxytocin Factor. Tapping the Hormone of Calm, Love, and Healing. Cambridge, MA: Da Capo Press; 2003.
44. Taylor S, Klein L, Lewis B, et al. Biobehavioural responses to stress in females: tend-and-befriend, not fight-or-flight. Psychological Rev. 2000;107:411-429.
45. Neal JL, Lowe NK, Patrick TE, et al. What is the slowest-yet-normal cervical dilation rate among nulliparous women with spontaneous labor onset? J Obstet Gynecol Neonatal Nurs. 2010;39(4):361-9.
46. Lowe NK. The nature of labor pain. Am J Obstet Gynecol. 2002;186(5 Suppl Nature):S16-S24.
47. Simkin P, Bolding A. (2004) Update on nonpharmacologic approaches to relieve labor pain and prevent suffering. J Midwifery Womens Health. 2004;49:489-504.
48. Dunne C, Da Silva O, Schmidt G, et al. Outcomes of elective labour induction and elective caesarean section in low-risk pregnancies between 37 and 41 weeks' gestation. JOGC. 2009;31(12):1124-1130.
49. Cardwell CR, Stene LC, Joner G, et al. Caesarean section is associated with an increased risk of childhood-onset type 1 diabetes mellitus: a meta-analysis of observational studies. Diabetologia. 2008;51:726-735.
50. Schlinzig T, Johansson S, Gunnar A, et al. Epigenetic modulation at birth – altered DNA-methylation in white blood cells after caesarean section. Acta Paediatr. 2009;98: 1096-1099.
51. Toyokawa S, Uddin M, Koenen KC, et al. How does the social environment “get into the mind”? Epigenetics at the intersection of social and psychiatric epidemiology. Soc Sci Med. 2012;74:67-74.
52. Heim C, Binder EB. Current research trends in early life stress and depression: review of human studies on sensitive periods, gene-environment interactions, and epigenetics. Exp Neurol. 2012;233(1):102 -111.
53. Maghzi AH, Etemadifar M., Heshmat-Ghahdarijani K, et al. Delivery may increase the risk of multiple sclerosis. Mult Scler. 2012;18(4):468-471.
54. Xu XF, Du LZ. Epigenetics in neonatal diseases. Chin Med J. 2010;123(20):2948-2954.
55. Hyde M, Mostyn A, Modi N, et al. The health implications of birth by caesarean section. Biol Rev. 2012;87(1), 229 -243.
56. Kapellou O. Effect of caesarean section on brain maturation. Acta paediatr. 2011;100(11):1416 -1422.

8
57. Kennedy HP, Nardini K, McLeod-Waldo R, et al. Top-selling childbirth advice books: a discourse analysis. Birth. 2009;36(4):318-324.
58. Klein MC, Liston R, Fraser WD. Attitudes of the new generation of Canadian obstetricians: how do they differ from their predecessors? Birth. 2011;38(2):1-11.
59. van der Hulst LAM, Van Teijlingen ER, Bonsel GK. Does a pregnant woman's intended place of birth influence her attitudes toward and occurrence of obstetric interventions? Birth. 2004;31(1):28-33.
60. Kennedy HP, Grant J, Walton C, et al. Normalizing birth in England: a qualitative study. J Midwifery Womens Health. 2010;55(3): 262-269.
61. American College of Nurse-Midwives. Providing oral nutrition to women in labor. Clinical bulletin. http://www.midwife.org/siteFiles/education/Oral_Nutrition_to_Women_in_Labor_5_08.pdf. Published March, 2008. Accessed May 4, 2012.
62. American College of Nurse-Midwives. Intermittent auscultation for intrapartum fetal heart rate surveillance. Clinical bulletin. http://onlinelibrary.wiley.com/doi/10.1016/j.jmwh.2007.03.021/abstract?userIsAuthenticated=true&deniedAccessCustomisedMessage= . Pulished March, 2007. Accessed May 4, 2012.
63. Simkin PP, O’Hara M. Nonpharmacologic relief of pain during labor: systematic reviews of five methods. Am J Obstet Gynecol. 2002;186(5 Suppl Nature):S131-S159.
64. Childbirth Connection. Blueprint for action: steps toward a high-quality, high-value maternity care system. http://transform.childbirthconnection.org/blueprint/. Accessed May 4, 2012.

CHILDBIRTH TODAYSince 1996, the World Health Organization has called for eliminating unnecessary intervention in childbirth. Yet in the US, birth interventions have reached epidemic proportions. Sadly, there is a lack of resources available to women to help them achieve their goals of a normal, safe, and healthy birth.
The norm for birth in the US today includes the use of technology and interventions that are not proven to benefit healthy women and babies during childbirth.
More than half of women receive medication to start or speed up their labors. This requires additional monitoring and interventions to treat possible side effects, and can result in increased use of pain medication including epidurals.
One-third of US women deliver by cesarean section, a major abdominal surgery that has the potential for serious short- and long-term health consequences for both you and your baby.1
Often, vaginal birth is not an option for women who have already had a cesarean section.
If a woman receives care that she feels is traumatic or disrespectful, it affects her physical and emotional health, and interrupts the critical early bonding period with her baby.
1 See “What Every Pregnant Woman Needs to Know about Cesarean Section,” ChildbirthConnection.org, http://childbirthconnection.org/pdfs/cesareanbooklet.pdf
Normal, Healthy Childbirth for Women & Families: What You Need to Know
A woman’s guide to
understanding normal, healthy
birth and how it can improve
the health of her baby and her
health. Critical information to
help women make informed
decisions and avoid possibly
unnecessary and expensive
medical interventions, such as
cesarean sections.
COPYRIGHT 2014. AMERICAN COLLEGE OF NURSE-MIDWIVES. ALL RIGHTS RESERVED.

NORMAL BIRTH AND YOU | PAGE 2
UNDERSTANDING NORMAL, HEALTHY CHILDBIRTHNormal, healthy birth is a safe process that includes labor, birth, and the first hour after birth for both the mom and her baby. It does not routinely require medical intervention.
Characteristics of normal labor, birth and the first hour after birth include:
◆◆ Labor starts and progresses on its own.
◆ The process is supported by physical and psychological factors that promote effective labor.
◆ Labor results in a vaginal birth with normal blood loss.
◆ The mother and her baby stay together after birth, with the baby remaining directly on her skin.
◆ Breastfeeding begins right away.
YOUR BABY & YOUR BODY DURING A NORMAL, HEALTHY BIRTHDuring normal, healthy birth, your body releases hor-mones that help you labor effectively, cope with pain, and bond with your baby. These hormones also help your baby transition to life outside of the womb, main-tain a normal body temperature, breastfeed successfully, and bond more effectively.
When labor progresses naturally on its own, there is less chance that your baby will have difficulties during labor or that you will need a vacuum, forceps, or a cesarean birth.
A normal, healthy labor and birth occur as a result of the mother and baby’s natural abilities. This type of birth is more likely to be safe and healthy because the process occurs without unnecessary interventions.
Some women and babies have complications that require interventions to have a safe and healthy outcome. Supporting normal, healthy labor and birth continues to benefit these women and their babies as well.
DISRUPTIONS TO NORMAL, HEALTHY BIRTHMany things can disrupt the normal process of birth. Some examples to watch for:
◆◆ Medications to induce or speed up labor.
◆◆ Any environment that isn’t private or comfortable, or where people aren’t present to offer continuous support as desired.
◆◆ Time limits on the progress of labor.
◆◆ Restrictions on food and drink.
◆◆ Pain medications, epidurals, or anesthesia.
◆◆ Episiotomy.
◆◆ Cesarean, vacuum or forceps delivery.
◆◆ Early cutting of the umbilical cord before it has stopped pulsating.
◆◆ Separation of you and your baby after birth.
◆◆ Any situation where you feel threatened or unsupported.
HAVING A NORMAL, HEALTHY BIRTHMany things can influence your ability to have a normal, healthy birth without intervention. These include:
◆◆ Your overall good health and physical fitness.
◆◆ Your knowledge and confidence about birth (including cultural beliefs and practices and what you’ve been taught about birth).
◆◆ Having the chance to make informed decisions about your birth with your healthcare provider.

NORMAL BIRTH AND YOU | PAGE 3
◆◆ Having access to a healthcare system, healthcare professionals, and setting that supports you and helps meet your goal.
CHOOSING THE RIGHT HEALTHCARE PROVIDER Your healthcare provider can increase your confidence and address your concerns about giving birth. She or he should:
◆◆ Be committed to helping you learn about the birth process, while providing you with information so that you can make the best decisions for you and your baby.
◆◆ Allow you enough time to make decisions without feeling pressured.
◆◆ Know how to help you cope with pain in labor without using medications, and should assure your comfort, dignity and privacy.
◆◆ Respect your cultural beliefs and preferences.
◆◆ Have the education, knowledge, skills, and confidence to help you achieve your goals.
CHOOSING THE RIGHT BIRTH SETTING The location that you choose for birth should have poli-cies in place to support normal, healthy birth. These policies should allow you to:
◆◆ Go into labor spontaneously and not allow induc-tion of labor or the use of Pitocin to speed up your labor, without a compelling medical reason.
◆◆ Eat and drink during labor, if you want to.
◆◆ Move around freely in labor.
◆◆ Give birth in whatever position you feel comfortable.
◆◆ Receive support from people you choose.
BENEFITS OF A NORMAL, HEALTHY BIRTHA normal, healthy birth provides many important benefits to your baby and you, such as:
◆◆ Achieving better overall health for your baby.
◆◆ Enabling your baby to successfully adapt to life outside the womb.
◆◆ Feeling physically and emotionally well and confident as mothers.
◆◆ Being better able to respond to your baby’s needs.
In addition to both of you, your family and society also benefit from a normal, healthy birth. As more women experience normal labor and birth, the view of birth will change to one of wellness, rather than illness. It also helps to ensure that a woman and her healthcare provider act as partners, sharing decision making and responsibility.

NORMAL BIRTH AND YOU | PAGE 4
Unless there is a compelling medical reason, there is no need to be attached to an electronic fetal monitor. You should be given the option of having your baby’s heartbeat listened to at regular intervals.
MIDWIVES WORK COLLABORATIVELY TO SUPPORT NORMAL, HEALTHY BIRTHMidwives are experts in supporting women in normal, healthy childbirth. Together with healthcare professionals, policy makers, educators, researchers, and of course women, we are working collaboratively to educate all those impacted by childbirth. As a team, we are leading the way to:
◆◆ Encourage all birth settings to adopt supportive policies.
◆◆ Raise consumer awareness.
◆◆ Increase the availability of midwifery care for all women.
◆◆ Educate all healthcare professionals about the benefits of this process.
◆◆ Continue research efforts to support these goals.
midwife.orgmana.org nacpm.org
092514
ictcmidwives.org
lamaze.org
dona.org
ilca.org
centeringhealthcare.org
“Normal, Healthy Childbirth for Women & Families” has the support of the March of Dimes.
cfmidwifery.org
childbirthconnection.org
This document was created and approved by the three major midwifery organizations in the United States: American College of Nurse-Midwives, Midwives Alliance of North America and National Association of Certified Professional Midwives. Several other groups have endorsed it.
Encourage your health care provider to learn about resources for helping you achieve normal, healthy birth at www.birthtools.org.
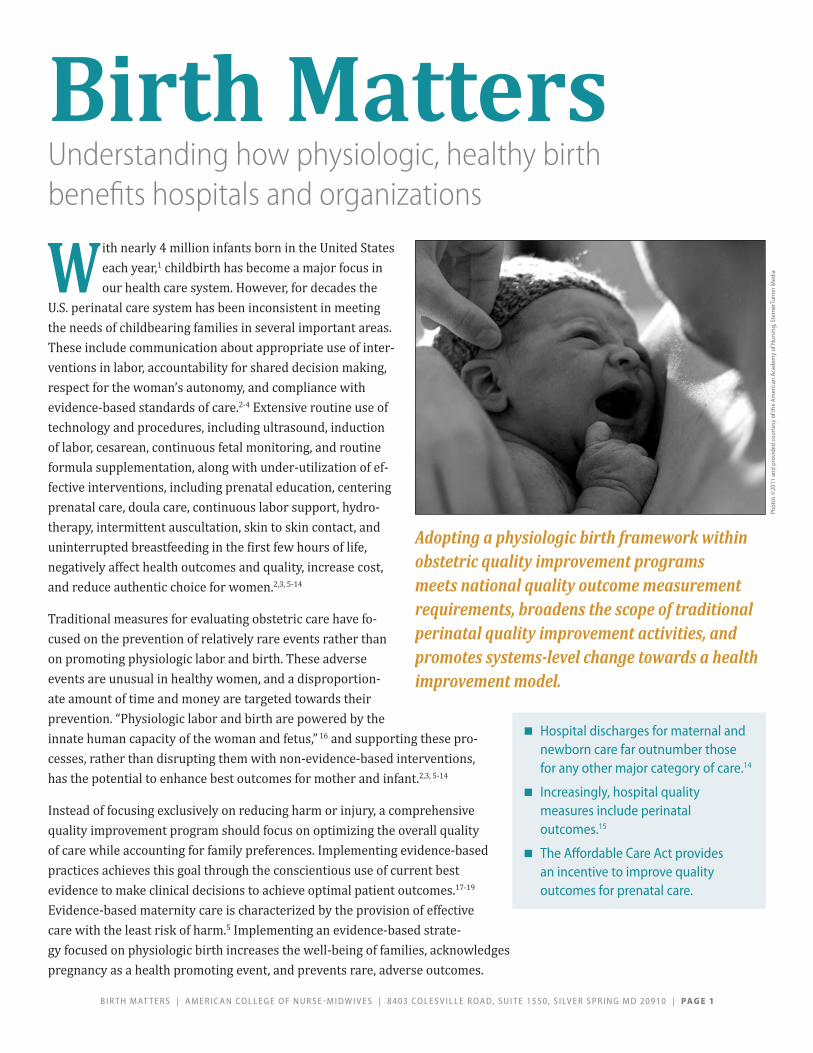
B I R T H M AT T E R S | A M E R I C A N C O L L E G E O F N U R S E - M I D W I V E S | 8 4 0 3 C O L E S V I L L E R O A D, S U I T E 1 5 5 0 , S I LV E R S P R I N G M D 2 0 9 1 0 | PA G E 1
W ith nearly 4 million infants born in the United States each year,1 childbirth has become a major focus in our health care system. However, for decades the
U.S. perinatal care system has been inconsistent in meeting the needs of childbearing families in several important areas. These include communication about appropriate use of inter-ventions in labor, accountability for shared decision making, respect for the woman’s autonomy, and compliance with evidence-based standards of care.2-4 Extensive routine use of technology and procedures, including ultrasound, induction of labor, cesarean, continuous fetal monitoring, and routine formula supplementation, along with under-utilization of ef-fective interventions, including prenatal education, centering prenatal care, doula care, continuous labor support, hydro-therapy, intermittent auscultation, skin to skin contact, and uninterrupted breastfeeding in the first few hours of life, negatively affect health outcomes and quality, increase cost, and reduce authentic choice for women.2,3, 5-14
Traditional measures for evaluating obstetric care have fo-cused on the prevention of relatively rare events rather than on promoting physiologic labor and birth. These adverse events are unusual in healthy women, and a disproportion-ate amount of time and money are targeted towards their prevention. “Physiologic labor and birth are powered by the innate human capacity of the woman and fetus,” 16 and supporting these pro-cesses, rather than disrupting them with non-evidence-based interventions, has the potential to enhance best outcomes for mother and infant.2,3, 5-14
Instead of focusing exclusively on reducing harm or injury, a comprehensive quality improvement program should focus on optimizing the overall quality of care while accounting for family preferences. Implementing evidence-based practices achieves this goal through the conscientious use of current best evidence to make clinical decisions to achieve optimal patient outcomes.17-19 Evidence-based maternity care is characterized by the provision of effective care with the least risk of harm.5 Implementing an evidence-based strate-gy focused on physiologic birth increases the well-being of families, acknowledges pregnancy as a health promoting event, and prevents rare, adverse outcomes.
Birth Matters Understanding how physiologic, healthy birth benefits hospitals and organizations
■■ Hospital discharges for maternal and newborn care far outnumber those for any other major category of care.14
■■ Increasingly, hospital quality measures include perinatal outcomes.15
■■ The Affordable Care Act provides an incentive to improve quality outcomes for prenatal care.
Adopting a physiologic birth framework within obstetric quality improvement programs meets national quality outcome measurement requirements, broadens the scope of traditional perinatal quality improvement activities, and promotes systems-level change towards a health improvement model.
Phot
os ©
2011
and
pro
vide
d co
urte
sy o
f the
Am
eric
an A
cade
my
of N
ursi
ng, S
tern
erTu
rner
Med
ia

PA G E 2 | B I R T H M AT T E R S | A M E R I C A N C O L L E G E O F N U R S E - M I D W I V E S | 8 4 0 3 C O L E S V I L L E R O A D, S U I T E 1 5 5 0 , S I LV E R S P R I N G M D 2 0 9 1 0
Physiologic Labor and Birth Practices Improve Quality Outcome MeasuresIncreasing access to care that promotes physiologic birth is a major national strategy for achieving high-quality maternity care. In 2012, the National Priorities Partnership Maternity Action Team, a multi-stakeholder group of leading national organizations and agencies, began to develop and implement a plan to reduce the rate of elective deliveries prior to 39 weeks gestation to 5% or less and to reduce the rate of cesar-ean birth in low-risk women to 15% or less.20 A major focus of this national effort is engaging consumers and profession-als in collaborative efforts to promote full-term, physiologic childbirth.
In concert with these initiatives, the American College of Nurse-Midwives (ACNM), Midwives Alliance of North America (MANA), and National Association of Certified Professional Midwives (NACPM) issued a consensus statement that identified practices and policies consistent with supporting physiologic approaches to childbirth.21 In 2014, the American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) promoted evidence-based approaches to safely avoid primary cesarean births.22 Together, obstetric, nursing, and midwifery organizations are promoting ways to increase evidence-based maternity care with the goal of improving birth outcomes and achieving safe, high quality, high value maternity care for women, newborns, and families.21-25
Who cares about perinatal quality measures?■■ Medicare: Inpatient Quality Reporting System
and EHR Incentive Program
■■ Medicaid: Core Set of Health Care Quality Measures for Enrolled Adults and Core Set of Children’s Health Care Quality Measures (CHIP)
■■ The Joint Commission: Performance Measures (5 perinatal quality measures required for hospitals with > 1,100 births/year)
■■ National Quality Forum: (14 endorsed perinatal and reproductive health measures)
■■ Health Care Providers
■■ Consumers
Phot
os ©
2011
and
pro
vide
d co
urte
sy o
f the
Am
eric
an A
cade
my
of N
ursi
ng, S
tern
erTu
rner
Med
ia
Operationally, and for the purpose of quality improvement, physiologic birth can be measured using 4 of the 14 perinatal and reproductive health measures endorsed by the National Quality Forum: elective induction of labor, incidence of episiotomy, cesarean section, and exclusive breast milk feeding.26 The implementation of physiologic birth will also improve outcomes on 3 of the 5 Joint Commission mandatory reporting core measures for hospitals with more than 1100 births per year.27-28
Collectively, these measures represent a hospital’s accountability to provide safe, reliable care for women and newborns when the majority of women begin labor spontaneously, give birth vaginally without unnecessary surgical interventions, and initiate exclusive breast milk feeding.
Joint Commission measures that improve with physiologic care:PC-01 Elective Delivery
PC-02 Cesarean Section
PC-05 Exclusive Breast Milk Feeding

B I R T H M AT T E R S | A M E R I C A N C O L L E G E O F N U R S E - M I D W I V E S | 8 4 0 3 C O L E S V I L L E R O A D, S U I T E 1 5 5 0 , S I LV E R S P R I N G M D 2 0 9 1 0 | PA G E 3
How promoting physiologic birth can benefit your institution…As reforms roll out, measures likely to be linked to payment and accreditation at your institution include
■■ cesarean birth (nulliparous, term, singleton, vertex)
■■ elective delivery before 39 weeks
■■ episiotomy
■■ exclusive breastfeeding during the hospital stay
■■ patient satisfaction measures
Institutions may also see a reduction in adverse events and related liability claims or payouts due to a reduced use of oxytocin, a high-alert medication implicated in half of obstetric claims.13
Why is physiologic birth good for my institution? Physiologic birth is associated with reduced health care costs and adverse iatrogenic events related to the overuse of medical interventions.3-4 Perinatal care data are increasingly available to the public for use when choosing health care providers and facilities. Hospitals that foster and encourage physiologic birth will perform higher on perinatal care quality measures and will attract more patients. Transparency is increasing as organizations providing health care are being held responsible for reporting outcomes, and consumers are becoming more educated about using those outcomes to make health care decisions. When consumers
are able to directly evaluate hospital performance measures, they will make deliberate choices about the hospitals and providers they use. Because women make the majority of the health care decisions for their families, institutions, providers, and health care insurers that establish positive relationships with women during their births are more likely to continue those relationships long-term.
Consumer satisfaction with maternity services is a long-standing outcome measure for quality of care.2, 7 Application of physiologic birth procedures reduces unnecessary interventions and their associated costs, promotes quality outcomes, and increases patient satisfaction. As a result, hospitals that promote physiologic labor and birth
practices have an opportunity to raise their quality-related reimbursement rates while reducing the cost of providing care.
Adopting a strategy that promotes physiologic labor and birth can have a positive effect on birth outcomes, reduce unwarranted variations in care, and improve quality and value. These goals are achievable through continuous quality improvement processes. A maternity unit that is committed to safety and quality will identify these aims as the ideal when planning, implementing, and evaluating quality improvement programs. Care that promotes, supports, and protects physiologic labor and birth and the judicious use of technology when indicated will help achieve these aims.
By fostering physiologic birth, institutions and insurers can encourage women to be healthy change agents in their own lives, the lives of their families, and in their communities.
Implementing healthy, physiologic birth will increase your facility’s bottom line: as positive birth experiences increase, patient satisfaction scores will improve and billing can be proactively aligned with future requirements.
Phot
os ©
2011
and
pro
vide
d co
urte
sy o
f the
Am
eric
an A
cade
my
of N
ursi
ng, S
tern
erTu
rner
Med
ia

PA G E 4 | B I R T H M AT T E R S | A M E R I C A N C O L L E G E O F N U R S E - M I D W I V E S | 8 4 0 3 C O L E S V I L L E R O A D, S U I T E 1 5 5 0 , S I LV E R S P R I N G M D 2 0 9 1 0
Birth Matters was developed under the leadership of ACNM in consultation with representatives from the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN), Childbirth and Postpartum Professional Association (CAPPA) and quality and safety leaders from various facilities across the U.S.
Information about the ACNM Healthy Birth Initiative can be found at www.midwife.org/ACNM-Healthy-Birth-Initiative. For clinician tools, please visit www.BirthTOOLS.org.
REFERENCES1. Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Matthews TJ. Birth: final
Data for 2012. Nat Vital Stat Rep. 2013;62(9):1-87. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf.
2. Romano AM, Lothian, JA. Promoting, protecting and supporting normal birth: a look at the evidence. J Obstet Gynecol Neonatal Nurs.2008; 37:94-105.
3. Declercq ER, Sakala C, Corry MP, Applebaum S, Herrlich A. Listening to Mothers III: Pregnancy and Birth. New York: Childbirth Connection; 2013.
4. Sakala C, Yang YT, Corry MP. Maternity Care and Liability: Pressing Problems, Substantive Solutions. New York: Childbirth Connection, January 2013.
5. Sakala C, Corry MP. Evidence-based maternity care: what it is and what it can achieve. http://www.milbank.org/uploads/documents/0809MaternityCare/0809MaternityCare.html. Published October, 2008. Accessed September 5, 2014.
6. Goer H, Romano A, Sakala C. Vaginal or Cesarean Birth: What is at Stake for Women and Babies? A Best Evidence Review. New York: Childbirth Connection; 2012.
7. Hodnett ED. Pain and women’s satisfaction with the experience of childbirth: a systematic review. Am J Obstet Gynecol. 2002;186:S160-S172
8. Hodnett ED, Gates S, Hofmeyr GJ, Sakala C. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2012;10:CD003766.
9. Ickovics JR, Kershaw TS, Westdahl C, et al. Group prenatal care and perinatal outcomes: a randomized controlled trial. Obstet Gynecol. 2007;110(2 Pt 1):330.
10. Gregory KD, Jackson S, Korst L, Fridman M. Cesarean versus vaginal delivery: whose risks? Whose benefits? Am J Perinatol. 2012;29:7-18.
11. Hyde MJ, Mostyn A, Modi N, Kemp PR. The health implications of birth by caesarean section. Biol Rev Camb Philos Soc. 2012;87:229-243.
12. Moore ER, Anderson GC, Bergman N, Dowswell T. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2012;5:CD003519
13. Simpson KR, Knox GE. Oxytocin as a high-alert medication: implications for perinatal patient safety. Am J Matern Child Nurs. 2009;34(1):8-15. doi: 10.1097/01.NMC.0000343859.62828.ee.
14. Agency for Healthcare Research and Quality. Health care cost and utilization project. http://www.ahrq.gov/research/data/hcup/index.html. Accessed September 17, 2014.
15. National Quality Forum. Patient safety collaboration. http://www.qualityforum.org/Setting_Priorities/NPP/NPP_Action_Teams.aspx. Accessed September 8, 2014
16. American College of Nurse-Midwives. What is physiologic birth? http://birthtools.org/Focus-on-Physiologic-Birth-2. Accessed September 5, 2014.
17. Closs SJ, Cheater FM. Evidence for nursing practice: a clarification of the issues. J Adv Nurs. 1999;30(1):10-17.
18. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences; 2001.
19. Sacket DL, Rosenberg WM, Muir Gray JA, Haynes RB, Richardson WS. Evidence-based medicine: what it is and what it isn’t. BMJ. 1996;312:71-72.
20. National Quality Forum. National priorities partnership maternity action team web meeting. http://www.google.com/url?sa=t&rct=j&q=&esrc=s&-frm=1&source=web&cd=3&ved=0CCkQFjAC&url=http%3A%2F%2Fwww.qual-ityforum.org%2FSetting_Priorities%2FNPP%2FMeetingSummary10102012.aspx&ei=dKsIVP11wYHKBN_8grgH&usg=AFQjCNEdlFT2xyF7d5UY7Nhq8NDpUbD9tg&bvm=bv.74649129,d.b2U. Accessed September 4, 2014.
21. American College of Nurse-Midwives, Midwives Alliance of North America, and National Association of Certified Professional Midwives. Supporting healthy and normal physiologic childbirth: a consensus statement by ACNM, MANA, AND NACPM. http://mana.org/pdfs/Physiological-Birth-Consensus-Statement.pdf. Accessed September 4, 2014.
22. American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. Obstetric care consensus: safe prevention of the primary cesarean delivery. http://www.acog.org/Resources-And-Publications/Obstetric-Care-Consensus-Series/Safe-Prevention-of-the-Primary-Cesarean-Delivery. Published March 2014. Accessed September 4, 2014.
23. American Academy of Family Physicians, American Academy of Pediatrics, American College of Nurse-Midwives, et al. Quality patient care in labor and delivery: a call to action. J Obstet Gynecol Neonatal Nurs. 2012;41:151–153. doi:10.1111/j.1552-6909.2011.01317.x.
24. International Childbirth Education Association. ICEA position paper: physiologic birth. http://icea.org/sites/default/files/Physiologic%20Birth%20PP-FINAL.pdf. Accessed September 17, 2014.
25. Association of Women’s Health, Obstetric and Neonatal Nurses. Health care decision making for reproductive care. J Obstet Gynecol Neonatal Nurs. 2009;38:742. doi: 10.1111/j.1552-6909.2009.01078.x.
26. National Quality Forum. Endorsement summary: perinatal and reproduc-tive health measures. http://www.qualityforum.org/Publications/2012/06/Perinatal_and_Reproductive_Health_Endorsement_Maintenance.aspx. Accessed September 8, 2014.
27. Zhani EE. The Joint Commission expands performance measurement requirements. http://www.jointcommission.org/the_joint_commission_expands_performance_measurement_requirements. Accessed September 8, 2014.
28. The Joint Commission. Perinatal care. https://manual.jointcommission.org/releases/TJC2013A/PerinatalCare.html. Published 2012. Accessed September 4, 2014.
All photos credited to the American Academy of Nursing are provided courtesy of the American Academy of Nursing’s Raise the Voice photojournalism project A Nursing Life: Serving the Nation. Sterner Turner Media, LLC 2011
100114