objectives peripheral nerve injury - asht · peripheral nerve injury nora barrett, ms, otr/l, cht...
TRANSCRIPT
Peripheral Nerve Injury
Nora Barrett, MS, OTR/L, CHT
February 10, 2018
Objectives
• Differentiate between segmental involvement and symptoms in peripheral nerve distribution
• Contrast the pathology and presentation of compression versus laceration in nerve injury
• Evaluate historical and current concepts of sensibility retraining in nerve injury
• Describe rehabilitation phases for UE nerve palsies• Select appropriate clinical examination techniques and
therapeutic interventions for common nerve compression syndromes
Fundamentals
(Bathen & Gupta, 2011; Freedman, Dholakia, Ivill, Hilibrand & Broyer, 2011; Hammert, 2013; McClure, 2011; Topp & Boyd, 2012)
PNS Anatomy• Unit = neuron
• Connective tissue• Provides nutrition, prevents compression, allows
lengthening, and speeds conduction• Endoneurium-surrounds the axon• Perineurium-surrounds fascicles, blood-nerve barrier• Epineurium-binds fascicles into named nerve
• Arteriae nervorum• Blood supply affected with nerve compression or traction,
impairing nerve conduction
• Nervi nervorum• Sensory and autonomic fibers to peripheral nerves
(Jarosz, 2009, CC 3.0; https://en.wikipedia.org/wiki/File:Neuron_Hand-tuned.svg)
DendriteAxon terminal
Schwann cellMyelin sheath
Node of RanvierSoma
Axon
Nucleus
PNS Anatomy• Efferent (motor) fibers – anterior horn cell
• Afferent (sensory) fibers – dorsal root ganglion
• Stellate ganglion at C7
• Mixed spinal nerves divide into 2 major branches/rami• Dorsal rami
• Supply muscles close to the vertebral column and the skin of the back
• Ventral rami• C5-T1 form the
brachial plexus(Mysid, 2006, CC 3.0;
https://en.wikipedia.org/wiki/File:Spinal_nerve.svg)
Brachial Plexus
(https://en.wikipedia.org/wiki/File:Brachial_plexus_2.svg)
Nerves• Roots – Trunks –
Divisions• Segmental involvement
• Dermatomes and myotomes
• Cords – Nerves • Peripheral nerve
distribution• Sensory and motor
symptoms

Cervical Screen • Observation/Inspection
• AROM
• PROM
• Neurological screen
• Special tests• Spurling’s
• Cervical distraction
• Upper limb tension test
• Bakody’s sign / shoulder abduction test (http://www.ehealthstar.com/test/spurlings-test-sign)
Clinical Prediction Rule For Cervical Radiculopathy
•Cervical rotation toward involved side <60°
•Positive upper limb tension testing•Positive cervical distraction•Positive Spurling’s Test
Segmental Testing
SEGMENT MYOTOME REFLEX DERMATOME
C2‐C4 Shoulder shrug Supraclavicular
C5 Shoulder abduction BicepsLateral arm (mid‐deltoid)
C6Elbow flexion, wrist
extensionBrachioradialis Thumb
C7Elbow extension, wrist flexion
Triceps MF
C8 Thumb abduction SF
T1Finger abduction, finger adduction
Medial proximal forearm
Anomalous Innervations
• Martin-Gruber anastomosis• Proximal forearm, AIN/median n. ulnar n.
• Marinacci anastomosis• Proximal forearm, ulnar n. median n.
• Riche-Cannieu anastomosis• Hand, deep/motor branch of the ulnar n. recurrent
branch of the median n.
• Berretini anastomosis• Hand, between the ulnar and median common digital
nerves(Doygan, Uysal, & Seker, 2009)
Pathophysiology of Nerve Injury
(Bathen & Gupta, 2011; Clark, Barr, & Safadi, 2003; Hammert, 2013; Jacoby, Eichenbaum, & Osterman, 2011; Mackinnon & Novak, 1984; Slutsky, 2011; Smith,
2011; Topp & Boyd, 2012; Walsh, 2012)
Classification• Seddon’s Neuropraxia / Sunderland’s I
• Local conduction block involving local demyelination
• Axon remains intact
• Conduction preserved proximal and distal to the lesion
• Good to excellent prognosis
• Recovery complete within weeks
Classification• Seddon’s Axonotmesis / Sunderland’s II
• Axon disruption with Wallerian degeneration• Conduction lost distal to lesion• Endoneurial tube intact• Prognosis is fair because supportive connective
tissue remains• Recovery time depends on the distance from the
injury to the innervated end organ• 1 mm/day
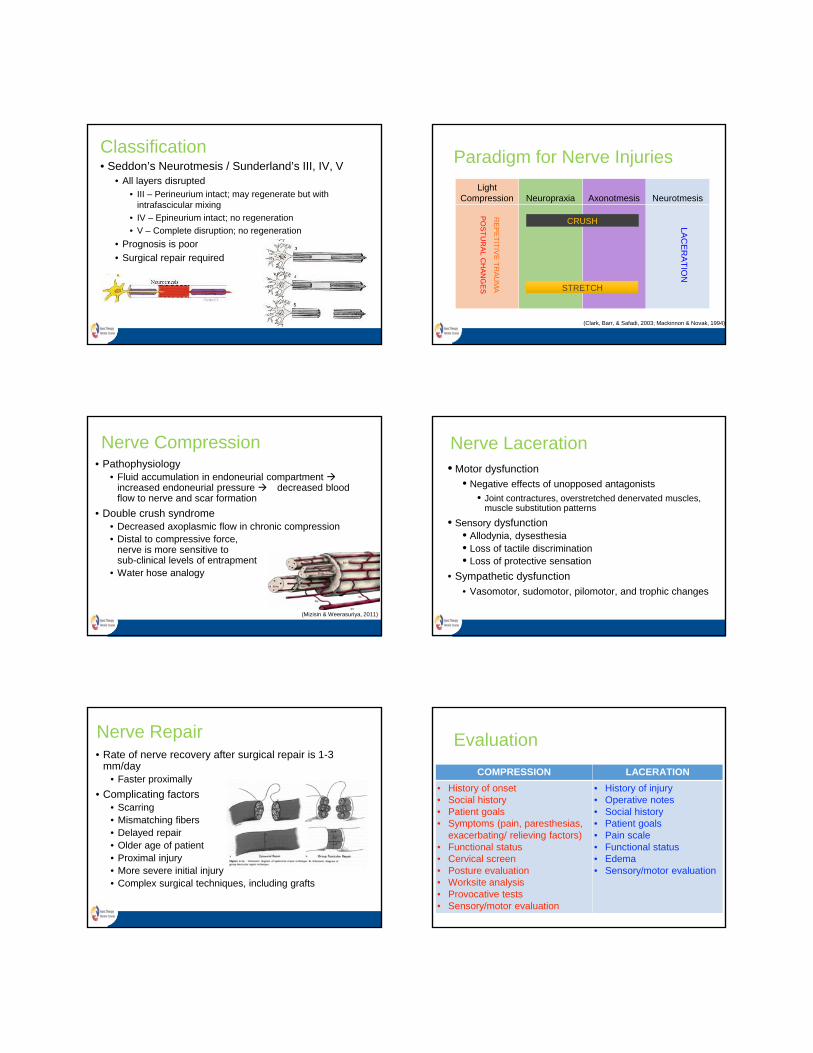
Classification• Seddon’s Neurotmesis / Sunderland’s III, IV, V
• All layers disrupted• III – Perineurium intact; may regenerate but with
intrafascicular mixing
• IV – Epineurium intact; no regeneration
• V – Complete disruption; no regeneration
• Prognosis is poor
• Surgical repair required
Light Compression Neuropraxia Axonotmesis Neurotmesis
Paradigm for Nerve Injuries
LAC
ER
AT
ION
PO
ST
UR
AL C
HA
NG
ES
CRUSH
RE
PE
TIT
IVE
TR
AU
MA STRETCH
(Clark, Barr, & Safadi, 2003; Mackinnon & Novak, 1994)
Nerve Compression• Pathophysiology
• Fluid accumulation in endoneurial compartment increased endoneurial pressure decreased blood flow to nerve and scar formation
• Double crush syndrome• Decreased axoplasmic flow in chronic compression• Distal to compressive force,
nerve is more sensitive to sub-clinical levels of entrapment
• Water hose analogy
(Mizisin & Weerasuriya, 2011)
Nerve Laceration• Motor dysfunction
• Negative effects of unopposed antagonists
• Joint contractures, overstretched denervated muscles, muscle substitution patterns
• Sensory dysfunction• Allodynia, dysesthesia• Loss of tactile discrimination• Loss of protective sensation
• Sympathetic dysfunction
• Vasomotor, sudomotor, pilomotor, and trophic changes
Nerve Repair• Rate of nerve recovery after surgical repair is 1-3
mm/day• Faster proximally
• Complicating factors• Scarring• Mismatching fibers• Delayed repair• Older age of patient• Proximal injury• More severe initial injury• Complex surgical techniques, including grafts
Evaluation
COMPRESSION LACERATION
• History of onset• Social history• Patient goals• Symptoms (pain, paresthesias,
exacerbating/ relieving factors)• Functional status• Cervical screen• Posture evaluation• Worksite analysis• Provocative tests• Sensory/motor evaluation
• History of injury• Operative notes• Social history• Patient goals• Pain scale• Functional status• Edema• Sensory/motor evaluation
Intervention
COMPRESSION LACERATION
• Patient education • Activity modification and
ergonomics• Postural exercises• Orthoses• Physical agent modalities• Manual therapy techniques• Nerve gliding• ROM• Targeted strengthening• Sensory reeducation
• Patient education• Pain management• Sensory reeducation/injury
prevention• Desensitization• Scar management• Orthoses • ROM • Motor reeducation following
tendon/nerve transfers
Addressing Sensory Dysfunction
(Bell Krotoski, 2011; Hsu et al., 2016; Lu et al., 2016; Rosen & Ludborg, 2011)
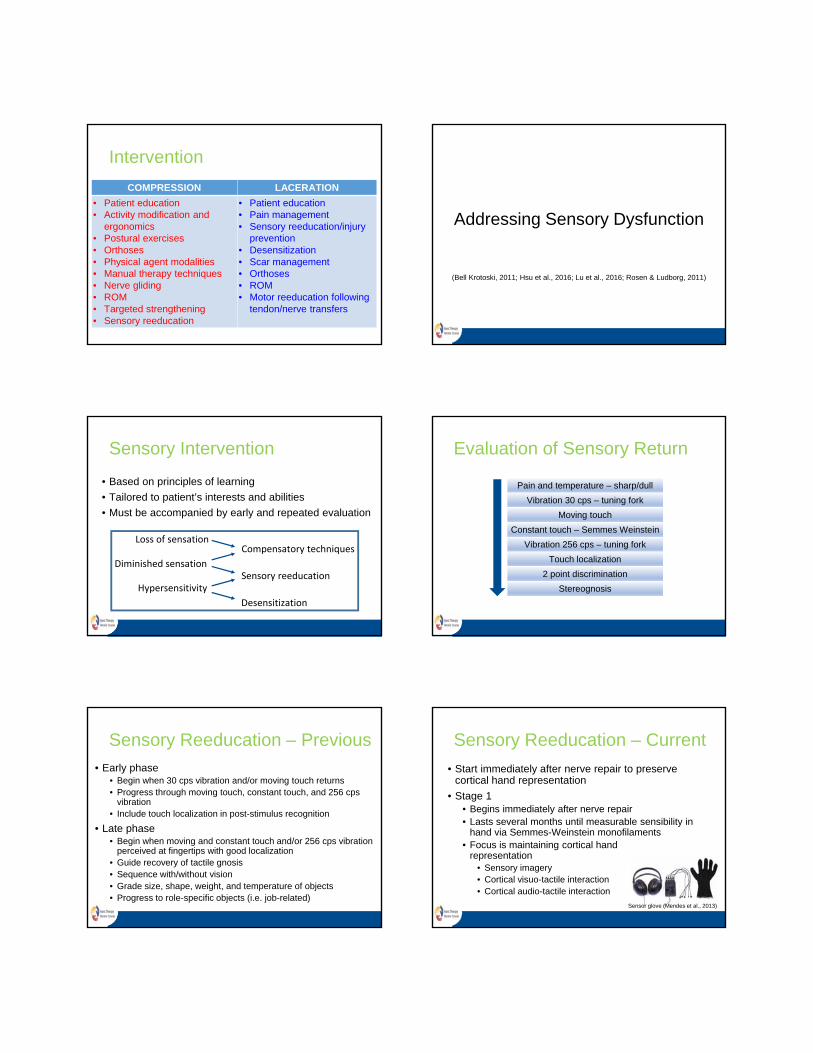
Sensory Intervention
• Based on principles of learning
• Tailored to patient’s interests and abilities
• Must be accompanied by early and repeated evaluation
Loss of sensation
Diminished sensation
Hypersensitivity
Compensatory techniques
Sensory reeducation
Desensitization
Evaluation of Sensory Return
Pain and temperature – sharp/dull
Vibration 30 cps – tuning fork
Moving touch
Constant touch – Semmes Weinstein
Vibration 256 cps – tuning fork
Touch localization
2 point discrimination
Stereognosis
Sensory Reeducation – Previous
• Early phase• Begin when 30 cps vibration and/or moving touch returns• Progress through moving touch, constant touch, and 256 cps
vibration• Include touch localization in post-stimulus recognition
• Late phase• Begin when moving and constant touch and/or 256 cps vibration
perceived at fingertips with good localization• Guide recovery of tactile gnosis• Sequence with/without vision• Grade size, shape, weight, and temperature of objects• Progress to role-specific objects (i.e. job-related)
Sensory Reeducation – Current
• Start immediately after nerve repair to preserve cortical hand representation
• Stage 1• Begins immediately after nerve repair• Lasts several months until measurable sensibility in
hand via Semmes-Weinstein monofilaments• Focus is maintaining cortical hand
representation• Sensory imagery• Cortical visuo-tactile interaction• Cortical audio-tactile interaction
Sensor glove (Mendes et al., 2013)
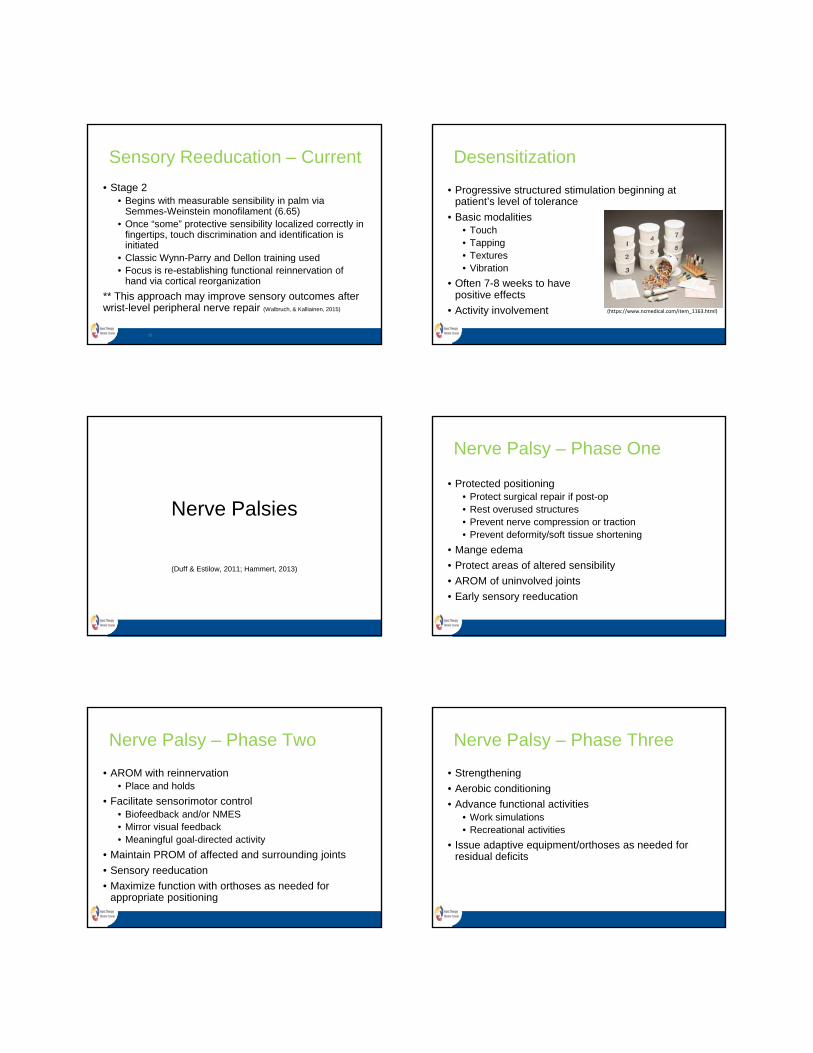
Sensory Reeducation – Current
• Stage 2• Begins with measurable sensibility in palm via
Semmes-Weinstein monofilament (6.65)• Once “some” protective sensibility localized correctly in
fingertips, touch discrimination and identification is initiated
• Classic Wynn-Parry and Dellon training used• Focus is re-establishing functional reinnervation of
hand via cortical reorganization
** This approach may improve sensory outcomes after wrist-level peripheral nerve repair (Walbruch, & Kalliainen, 2015)
25
Desensitization
• Progressive structured stimulation beginning at patient’s level of tolerance
• Basic modalities• Touch• Tapping • Textures • Vibration
• Often 7-8 weeks to have positive effects
• Activity involvement (https://www.ncmedical.com/item_1163.html)
Nerve Palsies
(Duff & Estilow, 2011; Hammert, 2013)
Nerve Palsy – Phase One
• Protected positioning• Protect surgical repair if post-op• Rest overused structures• Prevent nerve compression or traction• Prevent deformity/soft tissue shortening
• Mange edema
• Protect areas of altered sensibility
• AROM of uninvolved joints
• Early sensory reeducation
Nerve Palsy – Phase Two
• AROM with reinnervation• Place and holds
• Facilitate sensorimotor control• Biofeedback and/or NMES• Mirror visual feedback• Meaningful goal-directed activity
• Maintain PROM of affected and surrounding joints
• Sensory reeducation
• Maximize function with orthoses as needed for appropriate positioning
Nerve Palsy – Phase Three
• Strengthening
• Aerobic conditioning
• Advance functional activities• Work simulations • Recreational activities
• Issue adaptive equipment/orthoses as needed for residual deficits
Brachial Plexus Injuries• Obstetric or traumatic• Preganglionic vs. postganglionic
• Horner’s syndrome – avulsion of T1 nerve root
• Erb’s palsy• Upper trunk• “Waiter’s tip”—shoulder IR, elbow
extension, wrist/finger flexion• Klumpke’s palsy
• Lower trunk• May imitate ulnar nerve lesion
• Flail arm(http://erbpalsy.org/symptoms.html)
(Kang & Wolfe, 2011)
Proximal Nerve Palsies• Long thoracic nerve
• Functional loss: scapular winging
• Suprascapular nerve• Functional loss: weakness in abduction and ER
• Musculocutaneous nerve• Functional loss: biceps atrophy, weak elbow flexion in
supination, decreased sensation along radial aspects of forearm
• Axillary nerve• Functional loss: shoulder abduction/elevation/ER,
numbness of lateral upper arm
(Bednar & Wurapa, 2011)
Median Nerve PalsiesMuscle loss Functional deficit
HIGH LEVEL
PT, PQ* Forearm pronationFCR Weak wrist flexion / radial deviationFDS all digits, FDP index/long*
PIP/DIP flexion – absent index/long, weak ring/small
FPL* Loss of thumb IP flexionLOW
LEVELLumbricals index/long
MP flexion/IP extension deficit of index/long
APB, OP, superficial FPB
Loss of opposition, palmar abduction (deficits in functional prehension)
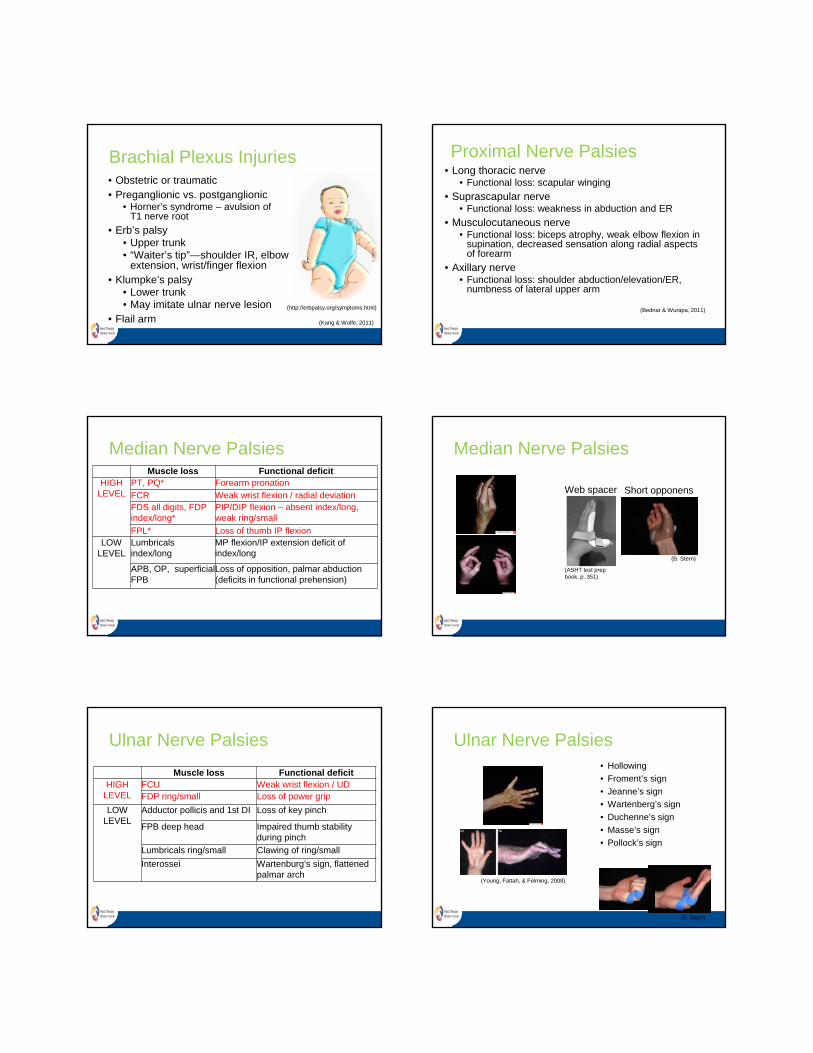
Median Nerve Palsies
Short opponens
(B. Stern)
Web spacer
(ASHT test prep book, p. 351)
Ulnar Nerve Palsies
Muscle loss Functional deficitHIGH
LEVELFCU Weak wrist flexion / UDFDP ring/small Loss of power grip
LOW LEVEL
Adductor pollicis and 1st DI Loss of key pinch
FPB deep head Impaired thumb stability during pinch
Lumbricals ring/small Clawing of ring/small
Interossei Wartenburg’s sign, flattened palmar arch
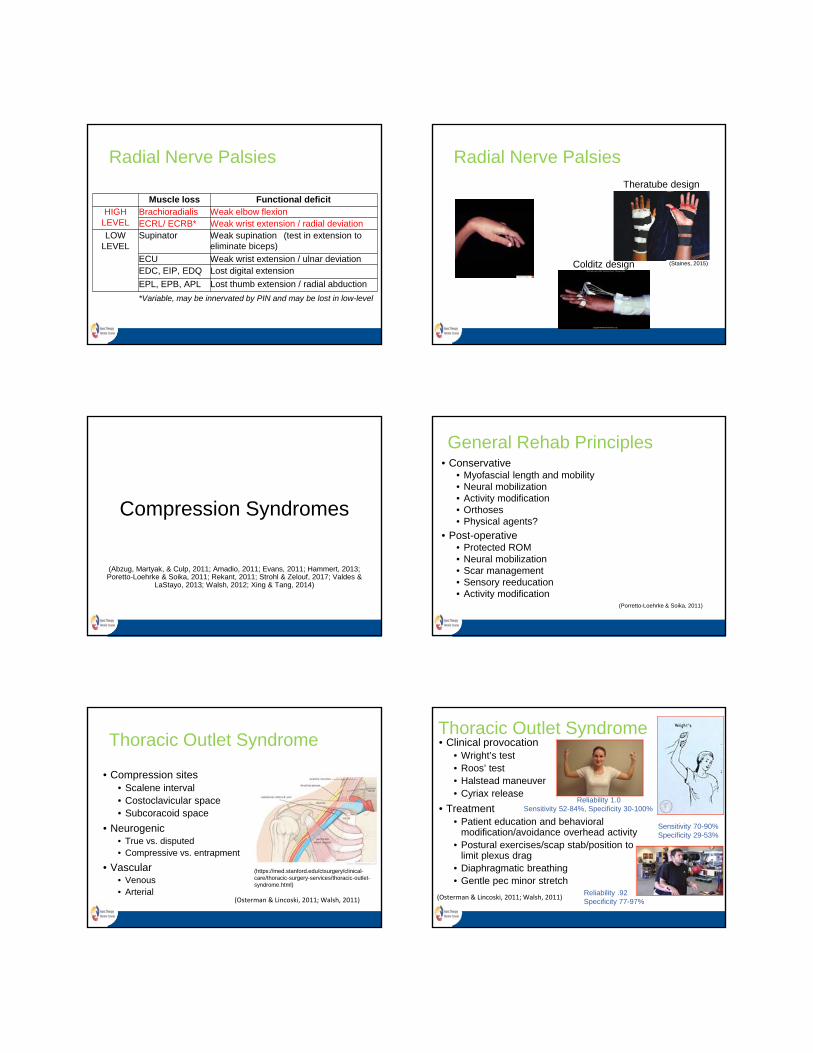
Ulnar Nerve Palsies• Hollowing
• Froment’s sign
• Jeanne’s sign
• Wartenberg’s sign
• Duchenne’s sign
• Masse’s sign
• Pollock’s sign
(Young, Fattah, & Felming, 2008)
(B. Stern)
Radial Nerve Palsies
Muscle loss Functional deficitHIGH
LEVELBrachioradialis Weak elbow flexionECRL/ ECRB* Weak wrist extension / radial deviation
LOW LEVEL
Supinator Weak supination (test in extension to eliminate biceps)
ECU Weak wrist extension / ulnar deviationEDC, EIP, EDQ Lost digital extension
EPL, EPB, APL Lost thumb extension / radial abduction
*Variable, may be innervated by PIN and may be lost in low-level
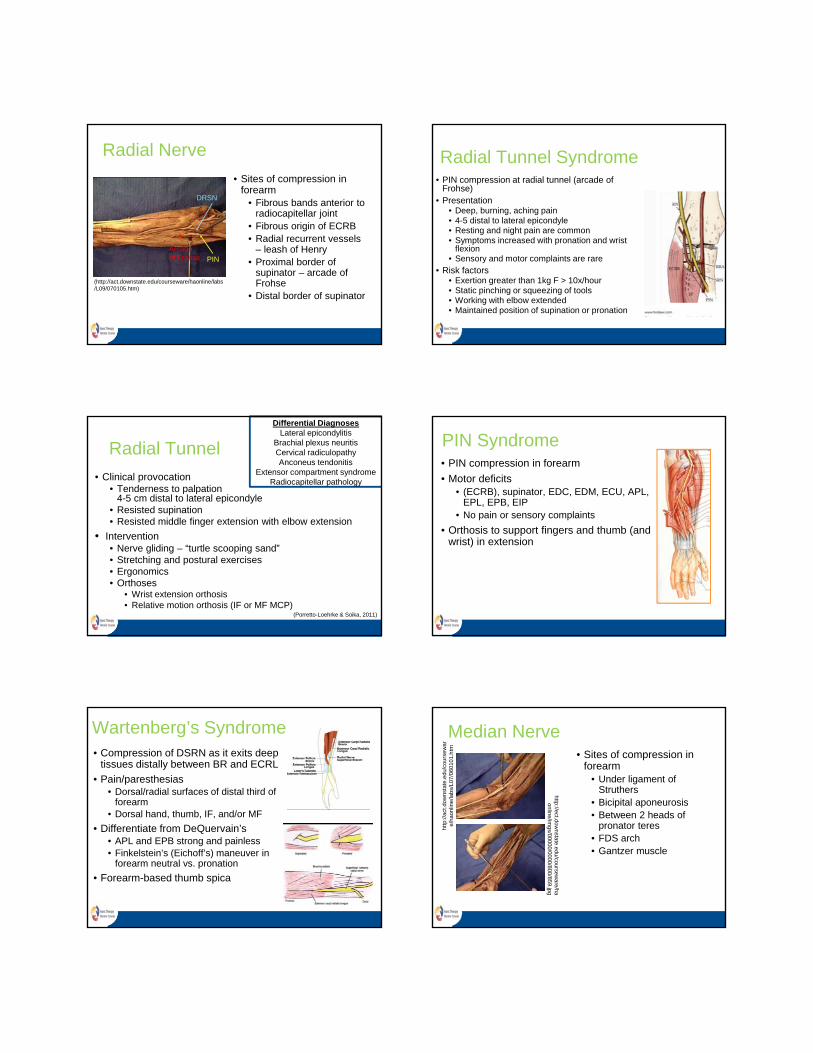
Radial Nerve Palsies
Colditz design (Staines, 2015)
Theratube design
Compression Syndromes
(Abzug, Martyak, & Culp, 2011; Amadio, 2011; Evans, 2011; Hammert, 2013; Poretto-Loehrke & Soika, 2011; Rekant, 2011; Strohl & Zelouf, 2017; Valdes &
LaStayo, 2013; Walsh, 2012; Xing & Tang, 2014)
General Rehab Principles• Conservative
• Myofascial length and mobility• Neural mobilization• Activity modification• Orthoses• Physical agents?
• Post-operative• Protected ROM• Neural mobilization• Scar management• Sensory reeducation• Activity modification
(Porretto-Loehrke & Soika, 2011)
Thoracic Outlet Syndrome
• Compression sites• Scalene interval• Costoclavicular space• Subcoracoid space
• Neurogenic• True vs. disputed• Compressive vs. entrapment
• Vascular• Venous• Arterial
(https://med.stanford.edu/ctsurgery/clinical-care/thoracic-surgery-services/thoracic-outlet-syndrome.html)
(Osterman & Lincoski, 2011; Walsh, 2011)
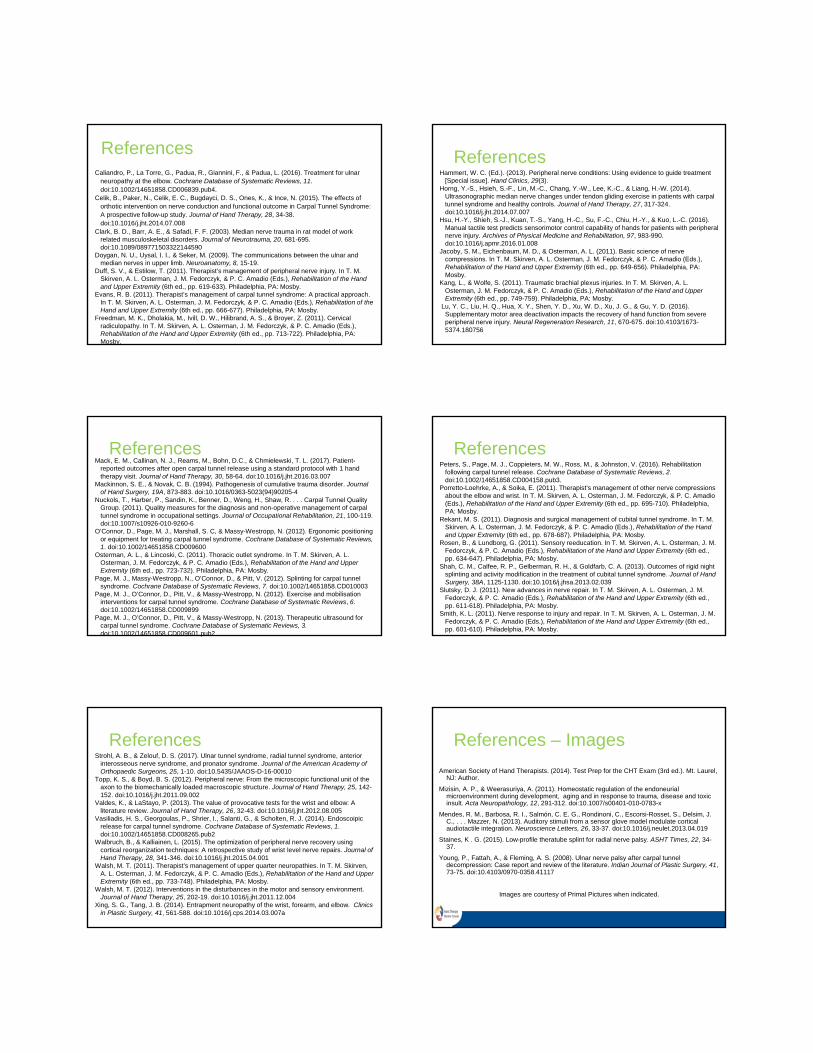
Thoracic Outlet Syndrome• Clinical provocation
• Wright’s test• Roos’ test• Halstead maneuver• Cyriax release
• Treatment• Patient education and behavioral
modification/avoidance overhead activity• Postural exercises/scap stab/position to
limit plexus drag• Diaphragmatic breathing• Gentle pec minor stretch
(Osterman & Lincoski, 2011; Walsh, 2011)
Reliability 1.0Sensitivity 52-84%, Specificity 30-100%
Reliability .92Specificity 77-97%
Sensitivity 70-90% Specificity 29-53%
Radial Nerve
• Sites of compression in forearm
• Fibrous bands anterior to radiocapitellar joint
• Fibrous origin of ECRB• Radial recurrent vessels
– leash of Henry• Proximal border of
supinator – arcade of Frohse
• Distal border of supinator
*Arcadeof Frohse PIN
DRSN
(http://act.downstate.edu/courseware/haonline/labs/L09/070105.htm)
Radial Tunnel Syndrome• PIN compression at radial tunnel (arcade of
Frohse)• Presentation
• Deep, burning, aching pain• 4-5 distal to lateral epicondyle• Resting and night pain are common• Symptoms increased with pronation and wrist
flexion• Sensory and motor complaints are rare
• Risk factors• Exertion greater than 1kg F > 10x/hour• Static pinching or squeezing of tools• Working with elbow extended• Maintained position of supination or pronation
Radial Tunnel
• Clinical provocation• Tenderness to palpation
4-5 cm distal to lateral epicondyle • Resisted supination• Resisted middle finger extension with elbow extension
• Intervention• Nerve gliding – “turtle scooping sand”• Stretching and postural exercises• Ergonomics • Orthoses
• Wrist extension orthosis• Relative motion orthosis (IF or MF MCP)
Differential DiagnosesLateral epicondylitis
Brachial plexus neuritisCervical radiculopathyAnconeus tendonitis
Extensor compartment syndromeRadiocapitellar pathology
(Porretto-Loehrke & Soika, 2011)
PIN Syndrome• PIN compression in forearm
• Motor deficits• (ECRB), supinator, EDC, EDM, ECU, APL,
EPL, EPB, EIP• No pain or sensory complaints
• Orthosis to support fingers and thumb (and wrist) in extension
Wartenberg’s Syndrome• Compression of DSRN as it exits deep
tissues distally between BR and ECRL
• Pain/paresthesias • Dorsal/radial surfaces of distal third of
forearm• Dorsal hand, thumb, IF, and/or MF
• Differentiate from DeQuervain’s• APL and EPB strong and painless • Finkelstein’s (Eichoff’s) maneuver in
forearm neutral vs. pronation
• Forearm-based thumb spica
Median Nerve
http
://ac
t.dow
nsta
te.e
du/c
ours
ewar
e/ha
onlin
e/la
bs/L
07/0
6010
1.h
tm
http://ect.downstate.edu/coursew
are/haonline/im
gs/00000/0000/800/859.jpg
• Sites of compression in forearm
• Under ligament of Struthers
• Bicipital aponeurosis• Between 2 heads of
pronator teres • FDS arch• Gantzer muscle

Pronator Syndrome
• Compression of median nerve in forearm
• Presentation• Non-localized forearm pain (volar proximal 2/3)
• No nocturnal pain• Exacerbated with repetitive forearm rotation
• Paresthesias in median nerve distribution including thenar eminence
• Note the palmar cutaneous branch• Subjective complaints of weakness• Negative Phalen’s
(http://ww
w.gm
s-books.de/book/living-textbook-hand-surgery/chapter/median-
nerve-compression-pronator-and-anterior)
Pronator Syndrome
(https://nervesurgery.wustl.edu/ap/sensation/Hand/MedianNerve/Pages/default.aspx)
(https://nervesurgery.wustl.edu/ev/upperextremity/median/Pages/PalmarCutaneousNerve.aspx)
Pronator Syndrome• Clinical Provocation
• Compression of pronator teres• Site-specific testing
• Resisted forearm pronation (PT)• Resisted elbow flexion in forearm supination (bicipital
aponeurosis)• Resisted MF PIP flexion (FDS arch)
Pronator Syndrome• Intervention
• Rest• Posterior elbow orthosis with 90° elbow flexion and
forearm neutral x 2 weeks – remove for gentle ROM• Avoid repetitive rotation and forceful grasp
• Address muscle imbalances • i.e. PT shortening
• Ergonomics• Physical agents• Nerve gliding
• “Lacertus tunnel”
clinicalgate.com
Anterior Interosseous Syndrome• Compression of AIN in forearm• Presentation
• No sensory complaints• Lost function of FPL and FDP to IF (& MF)
• Limitations in precision pinch• Weak pronation
• Test PT vs. PQ – elbow extension vs. flexion
• Intervention• Thumb orthosis to block IP hyperextension to
increase function and prevent FLP overstretching
• Patient education – avoid gripping and forearm rotation
Carpal Tunnel Syndrome
• Median nerve compression at wrist • Transverse carpal ligament
• Most common compression neuropathy
• Presentation• Nocturnal pain• Paresthesias of radial 3 1/2 digits• Thenar atrophy in advanced cases
(http://act.downstate.edu/courseware/haonline/labs/L08/070101.htm)

Carpal Tunnel Syndrome• Provocative tests
• Tinel’s- over carpal canal: Specificity 93%
• Phalen’s- passive wrist flexion 1 minute: Sensitivity 85% Specificity 89%
• Pressure Provocative Phalen’s: Sensitivity 96% with pressure in wrist flexion, 94% with pressure in wrist extension
• Durkan/Carpal compression test• Scratch collapse test: Sensitivity 69% Specificity 99%
• Berger test/Lumbrical incursion: Specificity 95% when includes wrist flexed
• Sensory testing and MMT
• Boston Carpal Tunnel Questionnaire (Symptom Severity Scale, Functional Status Scale)
Carpal Tunnel Syndrome• Intervention
• Wrist orthosis • 2° flexion, 3° degrees UD• Full-time vs night• MCP block? (Berger’s test)
• Physical agents• Nerve gliding• Tendon gliding exercises – avoid tight composite fist• Manual therapy (carpal mobs + flexor retinaculum
stretch)• Activity modification and ergonomics
(Brininger, et al., 2007; Horng et al., 2014; Nuckols et al., 2011; O’Connor et al., 2012; Page et al., 2013; Page, Massy-Westropp et al., 2012; Page, O’Connor et al., 2012)
Carpal Tunnel Syndrome• Surgical/electrodiagnostic consult
• Atrophy in opponens muscle• SW monofilament tests >3.61• Constant daytime paresthesia• No improvement in nocturnal pain• (+) provocative testing after 1 week of night orthosis
• Surgical release• Mini-open vs. endoscopic
• Post-op rehab
(Evans, 2011; Mack et al., 2017; Peters et al., 2016; Vasiliadis et al., 2014)
Ulnar Nerve
• Sites of compression at elbow
• Arcade of Struthers• Medial intermuscular
septum• Osborne’s band• Fibrous bands of FCU• Anconeus epitrochlearis(http://act.downstate.edu/courseware/haonli
ne/labs/L07/100103.htm)
Cubital Tunnel Syndrome• Ulnar nerve compression at elbow
• Presentation• Pain in medial proximal forearm• Paresthesias in ulnar nerve distribution
• Volar and dorsal• Weakness
Stage 1 Mild paresthesias Subjective weakness only
Stage 2A Moderate paresthesias Mild weakness
Stage 2B Moderate paresthesias Moderate weakness
Stage 3 Severe paresthesias Severe weakness, intrinsic atrophy
(Chiementi & Hammert in Hammert, 2013)
Cubital Tunnel Syndrome• Provocative tests
• Elbow flexion test• Tinel’s• Scratch collapse test
• MMT and sensory testing
• Activity analysis
• PRUNE
(Pixabay.com)
(Pixabay.com)
(Pexels.com)(pexels.com)

Cubital Tunnel Syndrome
• Intervention• Rest and protect
• (Night) orthosis in 30-45° comfortable elbow flexion, wrist/forearm neutral (Hely & Weber)
• Soft elbow pad during day• Nerve gliding• Physical agents • Activity modification and ergonomics• Postural exercises/movement training/core
strengthening
(Basson et al, 2017; Caliandro et al., 2016; Shah, Calfee, Gelberman & Goldfarb, 2013)
(http
://w
ww
.reh
abm
art.c
om/p
rodu
ct/p
adde
d-he
elel
bow
-pro
tect
ors
-749
2.ht
ml)
Cubital Tunnel Syndrome• Ulnar nerve decompression
• Fascial bridge between olecranon and medial epicondyle released
• Anterior subcutaneous transposition of ulnar nerve (with Eaton Sling)
• Ulnar nerve transferred anterior to medial epicondyle and held in place using flexor-pronator fascia
• Intramuscular transposition
• Anterior submuscular transposition of ulnar nerve• Ulnar nerve transferred anterior to medial
epicondyle and buried beneath muscle• Origin of flexor-pronator mass resected and
reattached
SMUT
Ulnar Tunnel Syndrome• Compression of ulnar nerve at
Guyon’s canal
• Presentation• Zone 1: motor and sensory• Zone 2: motor only• Zone 3: sensory only
• Causes• Space-occupying lesion• Hamate fracture• Handlebar’s palsy
(http://www.ehealthstar.com/anatomy/-)
http
://ac
t.dow
nsta
te.e
du/c
ours
ewar
e/h
aonl
ine/
labs
/L08
/040
101.
htm Ulnar Tunnel Syndrome
• Conservative management• Orthosis (neutral wrist)• Activity modification and ergonomics• Nerve gliding
• Post-operative management• Scar management• ROM• Intrinsic strengthening
Acknowledgments
• Mary Formby, OTR/L, CHT
• Lorna C. Kahn, PT, CHT
• Broca Stern, MOT, OTR/L, CHT
ReferencesAbzug, J., Martyak, G. G., & Culp, R. W. (2011) Other nerve compression syndromes of the
wrist and elbow. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 686-695). Philadelphia, PA: Mosby.
Amadio, P. C. (2011). Carpal tunnel syndrome: Surgeon’s management. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 657-665). Philadelphia, PA: Mosby.
Basson A, Oliver B, Ellis R et al.. The effectiveness of neural mobilization for meuromusculoskeletal conditions: a systematic review and meta-analysis. (2017) J Ortho Sports Phys Ther. 47(9):593-615. doi:10.2519/jospt.2017.7117.
Bathen, M., & Gupta, R. (2011). Basic science of peripheral nerve injury and repair. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 591-600). Philadelphia, PA: Mosby.
Bednar, J. M., & Wurapa, R. K. (2011). Common nerve injuries about the shoulder. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 760-769). Philadelphia, PA: Mosby.
Bell Krotoski, J. A. (2011). Sensibility testing: History, instrumentation, and clinical procedures. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 132-151). Philadelphia, PA: Mosby.
Brininger, T. L., Rogers, J. C., Holm, M. B., Baker, N. A., Li, Z. M., & Goitz, R. J. (2007). Efficacy of a fabricated customized splint and tendon and nerve gliding exercises for the treatment of carpal tunnel syndrome: A randomized controlled trial. Archives of Physical Medicine and R h bilit ti 88 1429 1435 d i 10 1016/j 2007 07 019
ReferencesCaliandro, P., La Torre, G., Padua, R., Giannini, F., & Padua, L. (2016). Treatment for ulnar
neuropathy at the elbow. Cochrane Database of Systematic Reviews, 11. doi:10.1002/14651858.CD006839.pub4.
Celik, B., Paker, N., Celik, E. C., Bugdayci, D. S., Ones, K., & Ince, N. (2015). The effects of orthotic intervention on nerve conduction and functional outcome in Carpal Tunnel Syndrome: A prospective follow-up study. Journal of Hand Therapy, 28, 34-38. doi:10.1016/j.jht.2014.07.008
Clark, B. D., Barr, A. E., & Safadi, F. F. (2003). Median nerve trauma in rat model of work related musculoskeletal disorders. Journal of Neurotrauma, 20, 681-695. doi:10.1089/089771503322144590
Doygan, N. U., Uysal, I. I., & Seker, M. (2009). The communications between the ulnar and median nerves in upper limb. Neuroanatomy, 8, 15-19.
Duff, S. V., & Estilow, T. (2011). Therapist’s management of peripheral nerve injury. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 619-633). Philadelphia, PA: Mosby.
Evans, R. B. (2011). Therapist’s management of carpal tunnel syndrome: A practical approach. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 666-677). Philadelphia, PA: Mosby.
Freedman, M. K., Dholakia, M., Ivill, D. W., Hilibrand, A. S., & Broyer, Z. (2011). Cervical radiculopathy. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 713-722). Philadelphia, PA: Mosby.
ReferencesHammert, W. C. (Ed.). (2013). Peripheral nerve conditions: Using evidence to guide treatment
[Special issue]. Hand Clinics, 29(3).Horng, Y.-S., Hsieh, S.-F., Lin, M.-C., Chang, Y.-W., Lee, K.-C., & Liang, H.-W. (2014).
Ultrasonographic median nerve changes under tendon gliding exercise in patients with carpal tunnel syndrome and healthy controls. Journal of Hand Therapy, 27, 317-324. doi:10.1016/j.jht.2014.07.007
Hsu, H.-Y., Shieh, S.-J., Kuan, T.-S., Yang, H.-C., Su, F.-C., Chiu, H.-Y., & Kuo, L.-C. (2016). Manual tactile test predicts sensorimotor control capability of hands for patients with peripheral nerve injury. Archives of Physical Medicine and Rehabilitation, 97, 983-990. doi:10.1016/j.apmr.2016.01.008
Jacoby, S. M., Eichenbaum, M. D., & Osterman, A. L. (2011). Basic science of nerve compressions. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 649-656). Philadelphia, PA: Mosby.
Kang, L., & Wolfe, S. (2011). Traumatic brachial plexus injuries. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 749-759). Philadelphia, PA: Mosby.
Lu, Y. C., Liu, H. Q., Hua, X. Y., Shen, Y. D., Xu, W. D., Xu, J. G., & Gu, Y. D. (2016). Supplementary motor area deactivation impacts the recovery of hand function from severe peripheral nerve injury. Neural Regeneration Research, 11, 670-675. doi:10.4103/1673-5374.180756
ReferencesMack, E. M., Callinan, N. J., Reams, M., Bohn, D.C., & Chmielewski, T. L. (2017). Patient-
reported outcomes after open carpal tunnel release using a standard protocol with 1 hand therapy visit. Journal of Hand Therapy, 30, 58-64. doi:10.1016/j.jht.2016.03.007
Mackinnon, S. E., & Novak, C. B. (1994). Pathogenesis of cumulative trauma disorder. Journal of Hand Surgery, 19A, 873-883. doi:10.1016/0363-5023(94)90205-4
Nuckols, T., Harber, P., Sandin, K., Benner, D., Weng, H., Shaw, R. . . . Carpal Tunnel Quality Group. (2011). Quality measures for the diagnosis and non-operative management of carpal tunnel syndrome in occupational settings. Journal of Occupational Rehabilitation, 21, 100-119. doi:10.1007/s10926-010-9260-6
O’Connor, D., Page, M. J., Marshall, S. C, & Massy-Westropp, N. (2012). Ergonomic positioning or equipment for treating carpal tunnel syndrome. Cochrane Database of Systematic Reviews, 1. doi:10.1002/14651858.CD009600
Osterman, A. L., & Lincoski, C. (2011). Thoracic outlet syndrome. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 723-732). Philadelphia, PA: Mosby.
Page, M. J., Massy-Westropp, N., O’Connor, D., & Pitt, V. (2012). Splinting for carpal tunnel syndrome. Cochrane Database of Systematic Reviews, 7. doi:10.1002/14651858.CD010003
Page, M. J., O’Connor, D., Pitt, V., & Massy-Westropp, N. (2012). Exercise and mobilisation interventions for carpal tunnel syndrome. Cochrane Database of Systematic Reviews, 6. doi:10.1002/14651858.CD009899
Page, M. J., O’Connor, D., Pitt, V., & Massy-Westropp, N. (2013). Therapeutic ultrasound for carpal tunnel syndrome. Cochrane Database of Systematic Reviews, 3. doi:10.1002/14651858.CD009601.pub2
ReferencesPeters, S., Page, M. J., Coppieters, M. W., Ross, M., & Johnston, V. (2016). Rehabilitation
following carpal tunnel release. Cochrane Database of Systematic Reviews, 2.doi:10.1002/14651858.CD004158.pub3.
Porretto-Loehrke, A., & Soika, E. (2011). Therapist’s management of other nerve compressions about the elbow and wrist. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 695-710). Philadelphia, PA: Mosby.
Rekant, M. S. (2011). Diagnosis and surgical management of cubital tunnel syndrome. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 678-687). Philadelphia, PA: Mosby.
Rosen, B., & Lundborg, G. (2011). Sensory reeducation. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 634-647). Philadelphia, PA: Mosby.
Shah, C. M., Calfee, R. P., Gelberman, R. H., & Goldfarb, C. A. (2013). Outcomes of rigid night splinting and activity modification in the treatment of cubital tunnel syndrome. Journal of Hand Surgery, 38A, 1125-1130. doi:10.1016/j.jhsa.2013.02.039
Slutsky, D. J. (2011). New advances in nerve repair. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 611-618). Philadelphia, PA: Mosby.
Smith, K. L. (2011). Nerve response to injury and repair. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 601-610). Philadelphia, PA: Mosby.
ReferencesStrohl, A. B., & Zelouf, D. S. (2017). Ulnar tunnel syndrome, radial tunnel syndrome, anterior
interosseous nerve syndrome, and pronator syndrome. Journal of the American Academy of Orthopaedic Surgeons, 25, 1-10. doi:10.5435/JAAOS-D-16-00010
Topp, K. S., & Boyd, B. S. (2012). Peripheral nerve: From the microscopic functional unit of the axon to the biomechanically loaded macroscopic structure. Journal of Hand Therapy, 25, 142-152. doi:10.1016/j.jht.2011.09.002
Valdes, K., & LaStayo, P. (2013). The value of provocative tests for the wrist and elbow: A literature review. Journal of Hand Therapy, 26, 32-43. doi:10.1016/j.jht.2012.08.005
Vasiliadis, H. S., Georgoulas, P., Shrier, I., Salanti, G., & Scholten, R. J. (2014). Endoscoipic release for carpal tunnel syndrome. Cochrane Database of Systematic Reviews, 1. doi:10.1002/14651858.CD008265.pub2
Walbruch, B., & Kalliainen, L. (2015). The optimization of peripheral nerve recovery using cortical reorganization techniques: A retrospective study of wrist level nerve repairs. Journal of Hand Therapy, 28, 341-346. doi:10.1016/j.jht.2015.04.001
Walsh, M. T. (2011). Therapist’s management of upper quarter neuropathies. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the Hand and Upper Extremity (6th ed., pp. 733-748). Philadelphia, PA: Mosby.
Walsh, M. T. (2012). Interventions in the disturbances in the motor and sensory environment. Journal of Hand Therapy, 25, 202-19. doi:10.1016/j.jht.2011.12.004
Xing, S. G., Tang, J. B. (2014). Entrapment neuropathy of the wrist, forearm, and elbow. Clinics in Plastic Surgery, 41, 561-588. doi:10.1016/j.cps.2014.03.007a
References – Images
American Society of Hand Therapists. (2014). Test Prep for the CHT Exam (3rd ed.). Mt. Laurel, NJ: Author.
Mizisin, A. P., & Weerasuriya, A. (2011). Homeostatic regulation of the endoneurial microenvironment during development, aging and in response to trauma, disease and toxic insult. Acta Neuropathology, 12, 291-312. doi:10.1007/s00401-010-0783-x
Mendes, R. M., Barbosa, R. I., Salmón, C. E. G., Rondinoni, C., Escorsi-Rosset, S., Delsim, J. C., . . . Mazzer, N. (2013). Auditory stimuli from a sensor glove model modulate cortical audiotactile integration. Neuroscience Letters, 26, 33-37. doi:10.1016/j.neulet.2013.04.019
Staines, K . G. (2015). Low-profile theratube splint for radial nerve palsy. ASHT Times, 22, 34-37.
Young, P., Fattah, A., & Fleming, A. S. (2008). Ulnar nerve palsy after carpal tunnel decompression: Case report and review of the literature. Indian Journal of Plastic Surgery, 41, 73-75. doi:10.4103/0970-0358.41117
Images are courtesy of Primal Pictures when indicated.