objectives to discuss study design issues –clinical study type –sample size –protocol
TRANSCRIPT

Objectives
• To discuss study design issues– Clinical study type– Sample size– Protocol

Study Designs
Descriptive Analytic Experimental
correlational
case report/case series
cross-sectional
case control
cohort
clinical trial
community trial

Experimental Designs• Experiment – a set of observations, conducted under
controlled circumstances, in which the scientist manipulates the conditions to ascertain what effect such manipulation has on the observations.
• Ideally only one factor is examined (however, biological variation exists)– Clinical Trials – (individual in a special environment are
randomized)
– Field Trials – (individuals in the community are randomized)
– Community Interventions – (whole communities are randomized)

Field Trials
• Differ from clinical trials in that subjects have not yet gotten disease– (1955) Salk vaccine for Polio– (1975) Vitamin C in preventing the
common cold)– (1982) MRFIT – a field trial of several
primary preventives of MI (N=12,866 and cost $115 million)

Community Intervention and Cluster Randomized Trials
• Community intervention is an extension of a field trial that involves intervention on a community-wide basis– (eg. Mass media campaigns)– (eg. Fluoridated water)
• Cluster randomization - groups of participants are randomized. The larger the cluster, the less that is accomplished by randomizing.

Study Protocol• Rationale and background• Objectives• Study Design• Inclusion/Exclusion• Definitions (intervention, measurements, adherence)• Study Flow chart• Sample Size calculation• Plan of analysis (interim analysis)• Appendices
– Questionnaires– Consent forms– Instructions to interviewers

Example of a flow chart for randomization

Example of a comparison table to demonstrate that randomization was successful

Objectives should be stated in terms of an hypothesis
• Null Hypothesis: There is no difference
Medication A will have not effect on disease progression
• Two tailed Hypothesis: There is some difference
Medication A will have some effect on disease progression
• One tailed Hypothesis: The difference is greater or less
Medication A will reduce deaths due to disease X
Medication A will increase deaths due to disease X

Hypothesis Testing
• Hypothesis testing involves conducting a test of statistical significance and quantifying the degree to which sampling variability may account for the results observed in a particular study
• When designing data collection tools, keep in mind your final analysis
Statistical Tests: 2 T-test Measures of Association: Odds Ratio, Relative Risk

Institutional Review Board
• To assure that the rights and privacy of patients is guaranteed
• To assure that patients have given informed consent
• Keep consent forms and IRB number handy
• Make sure that you have approval before starting

Phases of a Clinical Trial
• Phase I - safety (pharmacokenetics - to determine maximum tolerated dose)
• Phase II - Evidence of a response
• Phase III - Safety, efficacy
• Phase IV - Safety, Acceptability, Efficacy
Basic Study Design
• Control group
• Random allocation to intervention or no intervention (or new treatment v.s. standard of care)
• Follow-up to an endpoint

Study Diagram - Classic Randomized Controlled
Eligible SubjectPool R
Int
P/SC
LTF/C
O
O
LTF/C

Study Design - Cross-over
Study Eligibles R
E
C C
E

Types of Designs• Randomized controlled (classic)• Cross-over (subject is own control)• Withdrawl (to assess response to
discontinuation or reduction)• Factorial (compares two interventions to
control or single experiment)• Hybrid (when historical controls are available)• Equivalency (to determine if new is as good
as standard)

Response Variables (Outcomes)
• Write the question in advance• primary response variable should be measurable
in all subjects• a subject participation generally ends when the
primary response variable occurs (unless there are combinations of response variables to be assessed)
• response variables should be capable of unbiases assessments.
• Response variables should be ascertained as completely as possible

Response or Outcome variables
• You may have outcomes other than hard endpoints
• surrogate markers
• quality of life

Recruitment of Subjects• Generalizability can be compromised if better
follow-up can be assured.• Keep a log of who could be recruited and who
is being recruited to see if adaptations need to made.
• Explain study and keep good rapport with persons who can help you recruit
• Be realistic when planning• Don’t be too aggressive at recruitment
because you will suffer on follow-up

Purpose of Randomization • Produce comparable study groups
• Remove investigator bias in allocation of subjects
• Guarantees that statistical tests will have valid significance levels (probability)

Types of Randomization
• Fixed allocation
• Simple randomization
• block randomization
• stratified randomization
• baseline adaptive randomization
• response adaptive randomization

Methods for improving data quality
• Study protocol
• clearly defined measures on well constructed data collection tools
• training of data collection staff
• continuous assessment of follow-up
• data entry in-range and logical checks
• Monitoring of data collection
Blindness
• Bias is a error (systematic or non-systematic) or “difference between the true value and the actually obtained due to all causes other than sampling variability”
• unblinded, single blinded, double blinded, triple blinded

Survival Analysis
• This analysis used when subjects are entered over a period of time and have various lengths of follow-up.
• Dichotomous endpoints
• Kaplan Meier or Product Limit
• Cox Proportional Hazard modeling

Intent-to-treat Analysis
• For persons who cross-over to the other arm. You classify that person into the arm they were originally assigned.
• Less biased results than “as treated” because you maintain randomization.
• Only works if there is not a lot of crossing over very early in the study

Reasons for withdrawl of Subjects
• Ineligibility (misclassification, imprisonment, moved)
• Noncompliance (adverse effects of intervention, loss of interest, changes in underlying conditions, substance usage)
Incidence vs. Prevalence
• In infectious diseases of short duration, incidence may be close to prevalence
• In chronic diseases, prevalence will be far greater than incidence
• Monitor disease burden by prevalence
• Monitor efficacy of programs by incidence

Calculate an Incident Rate
Jan July Jan July Jan July Jan July Jan July Jan time at
1976 1976 1977 1977 1978 1978 1979 1979 1980 1980 1981 riskSub A *---------------------- 2.0 Sub B *---------------------------------x 3.0Sub C *--------------------------------------------------------- 5.0Sub D *--------------------------------------- 4.0Sub E *---------------------------x 2.5Total Years at risk 16.5
* = initiation of study ID=___cases/___person-years-- =Time followedx = development of disease
Measures of Associaton
• Since clinical trials are prospective and the intervention precedes the outcome, a relative risk is calculated.
• Covariates and confounders can be either controlled for in the design or adjusted for in the analysis

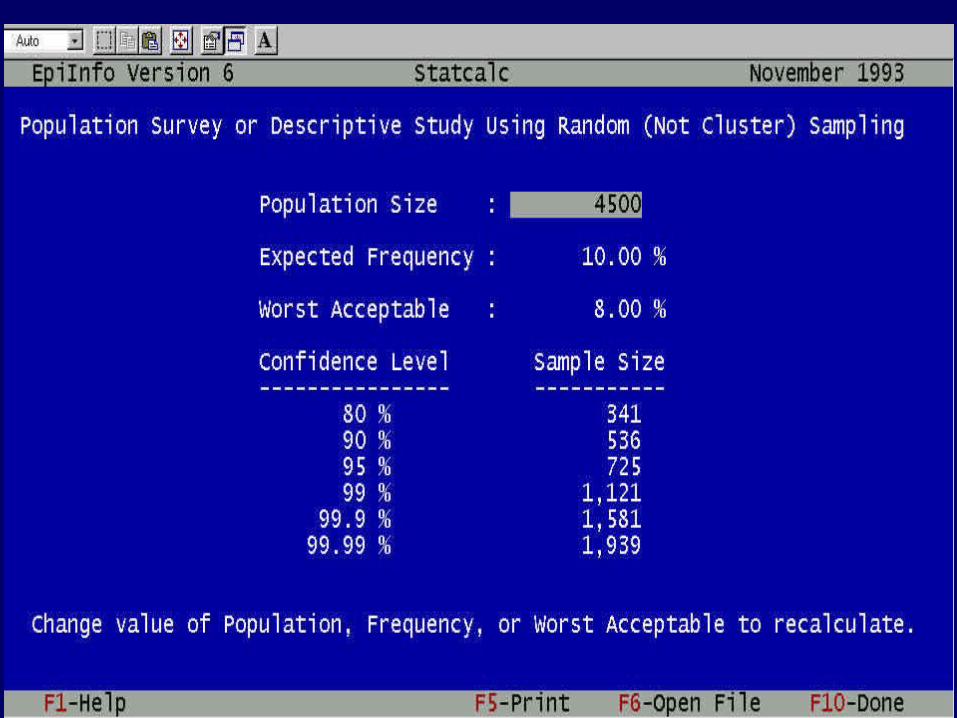
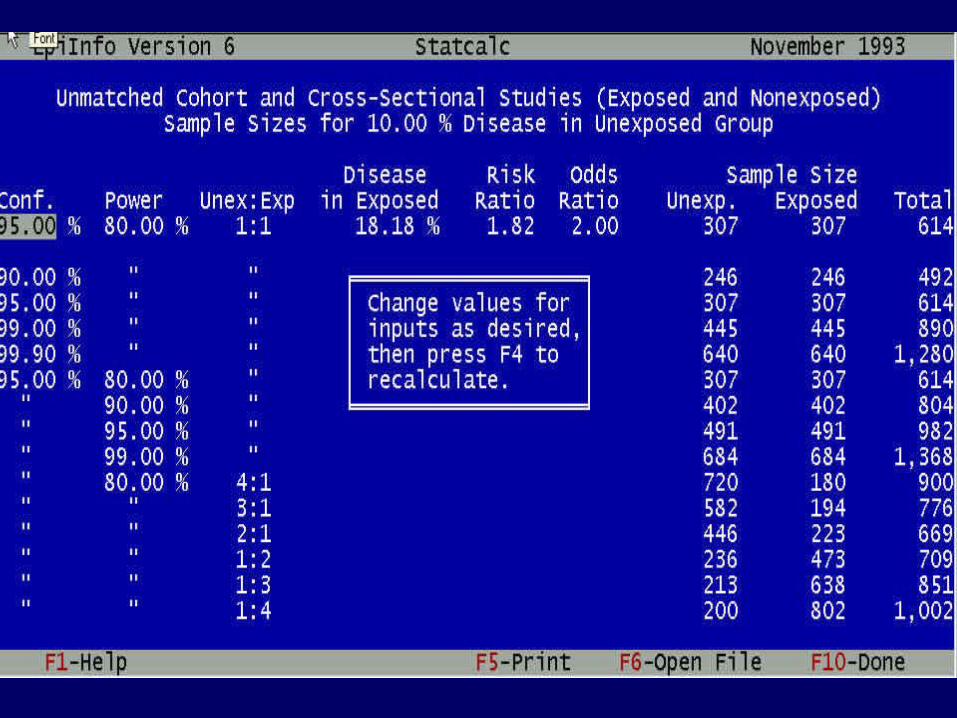
Sample Size Calculation
• Prevalence in the control group
• Difference you wish to detect
• Alpha you will accept (.05)
• Power you wish to have (.80)
• Number of controls per cases
• Should include an inflation factor to account for loss-to-follow-up

Sample Size will increase with:
• Decreasing significance levels
• Decreasing error (increasing power)
• Decreasing clinical significance (treatment differences)
• Increasing variability in the observed data

Sample Size and C.I.Ant Bite No Ant Bite
Cuts lawn 6 3Doesn’t cut lawn 4 7
Ant Bite No Ant BiteCuts lawn 60 30
Doesn’t cut lawn 40 70
O.R. 95% C.I. , P value = 1.83 (.74 - 4.55), P < .17
O.R. 95% C.I., P value = 1.83 (1.38 - 2.44) P <. 001




Example of a clinical trial – the MYRIAD study
• Perinatal prophylaxis for prevention of vertical transmission of HIV to children became available in 1994.
• This protocol require administration of ZDV during the third trimester of perinatal period, during birth process and to the child after birth.
• Since it became available, many children have received it and the transmission rate has gone dramatically down
• Now there is a push to eradicate perinatal transmission

Born1993-March 1998 in 29 States‡, United Stateswho Received or whose Mothers Received any ZDV*
0
20
40
60
80
100
* Any ZDV=Prenatal, intrapartum, or neonatal receipt of Zidovudine to reduce perinatal HIV transmission
Quarter-Year of Birth
1993N=1313
1994N=1271
1995N=1315
1996N=1260
1997N=1291
1998N=281
‡ Includes 29 areas that have conducted pediatric HIV Surveillance since 1993; data reported through March 1999
Percent of Perinatally HIV Exposed or Infected ChildrenPerc
ent
Rece
ivin
g Z
idovudin
e
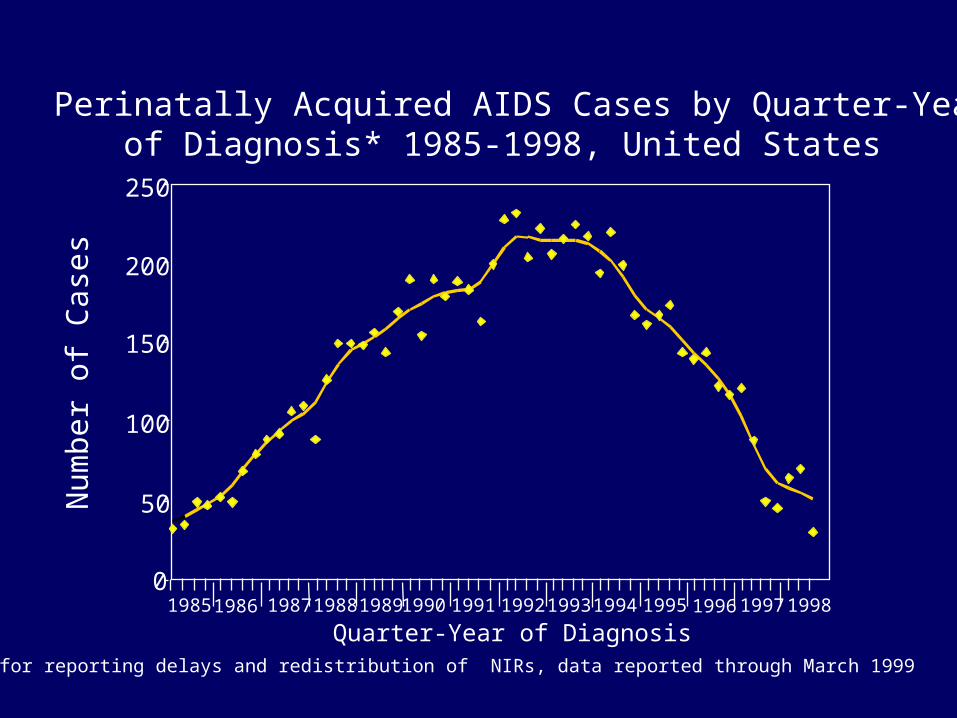
Perinatally Acquired AIDS Cases by Quarter-Yearof Diagnosis* 1985-1998, United States
Nu
mb
er
of
Case
s
Quarter-Year of Diagnosis
100
150
200
250
0
50
19861985 198719881989199019911992 19941993 1995199619971998
*Adjusted for reporting delays and redistribution of NIRs, data reported through March 1999

The Intervention• To eradicate the disease, researchers much target
women who come in late for prenatal care and don’t get access to the first phase of the perinatal prophylaxis.
• The multi-centered research group decides to adapt DOT (direct observation therapy) and use TOT (telephone outreach therapy) to improve adherence among women who come in late.
• Women who get randomized to the TOT arm will receive a cell phone for the 6 week period and will be responsible for calling in every day
• Women on both arms need to come in for 12 follow-up visits.

The study centers
New Orleans
Chicago
Miami
New YorkAtlanta

The intervention
Mom gives the medicine to the baby 4 times a day

The research groups (Domains)
Biomedical
Access to care
Barriers to prenatal care
Adherence to medication
Informed consent

The outcome
• The outcome of interest will be if the child receives the medication for the 6 week period– Refinement of the outcome is necessary– Inclusion/exclusion criteria need to be established– Each of the 5 sites can only provide 20 mom/child
pairs per year (it is a 5 year study). What kind of sample size do we need/can we get?
– What kind of confounders should we consider– Should incentives be given?– When should a woman be considered LTF?
Non-experimental (analytic) study designs
• Conducted because of ethics, cost or convenience
• Two primary types:– Cohort– Case-control