obstetric fistula
TRANSCRIPT
Obstetric Fistula
Dr. A. P. Soibi-HarryDept. of Obstetrics & Gyneacology
Lagos University Teaching Hospital

Outline
• Introduction• Brief History• Epidemiology• Etiology• Pathogenesis• Classification• Clinical Presentation• Diagnosis• Management• Prevention• Recent advances• Conclusion• Reference

Introduction
“Every minute, a woman dies in pregnancy or childbirth, and for
every woman who dies, 20-30 others will survive but with morbidity, one
of which is obstetric fistula” Source: G. Lewis, WHO Press.

Definition– obstetric fistula is an abnormal communication between the vagina
and the bladder or rectum.
– Occurred in the course of pregnancy and results in uncontrolled passage of urine, feaces or flatus into the vagina.
– Psychosocial injury

Brief history• The oldest evidence of obstructed labor:
• In the remains of Queen Henhenit, of Egypt c. 2050 BC.
• 1923: review of the Queen’s mummy found a defect in the bladder communicating directly with the vagina.
• 1663: Von Roonhuyse - surgical principles of VVF repair
• 1838: Dr. John Peter Mettauer - first American to perform a successful VVF repair
• 1852: James Marion Sims- refined and described technique for the surgical treatment of VVF using a transvaginal approach
• 1855: The first fistula hospital was opened in New York.
• 1888: Trendelenburg successfully performed a transabdominalVVF repair.
• 1975: The second and worlds largest fistula hospital was opened in Addis Ababa by Catherine and Reginald Hamlin.

Epidemiology 1• Globally:
WHO estimates -> 2 million women live with untreated fistula, with about 50,000 -100,000 new cases each year.
• Almost all cases live in sub-Saharan Africa and south Asia.
• The reported incidence rates of vesicovaginal fistula in West Africa range between 1– 4 per 1,000 deliveries.
• Nigeria accounts for 40% of the worldwide fistula prevalence with approximately 20,000 new cases occurring each year.
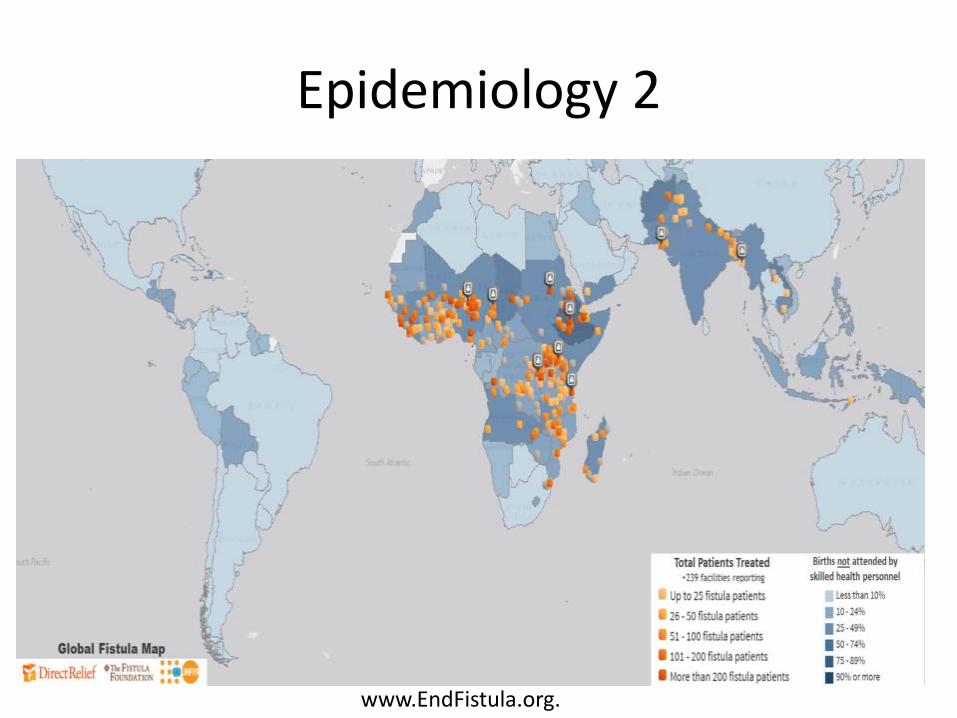
Epidemiology 2
www.EndFistula.org.

Epidemiology 3
2.1/1000 deliveries
Etiology• Obstructed labour- >80%
• Lack of access to emergency obstetric care
• Iatrogenic causes:
– Caesarian section
– Repair of ruptured uterus
– Forceps Delivery
– Destructive operations

• Risk Factors
– Poverty
– Early marriage and child bearing age
– Harmful traditional practices:
• Female genital mutilation
• Gishiri- 15% fistula cases in Northern Nigeria
• Caustic soda exposure
– Infections – schistosomiasis, lymphogranulomaVenerum, tuberculosis

Obstetric fistula pathway

Pathogenesis

Classification of Obstetric fistulas
• Site of Injury
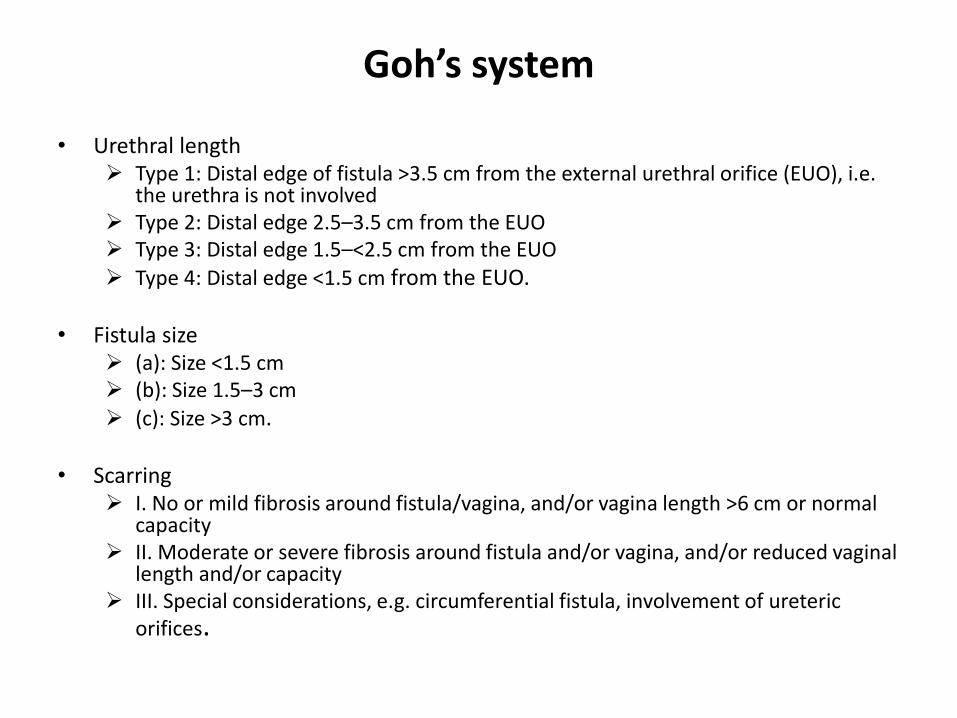
Goh’s system
• Urethral length Type 1: Distal edge of fistula >3.5 cm from the external urethral orifice (EUO), i.e.
the urethra is not involved Type 2: Distal edge 2.5–3.5 cm from the EUO Type 3: Distal edge 1.5–<2.5 cm from the EUO
Type 4: Distal edge <1.5 cm from the EUO.
• Fistula size (a): Size <1.5 cm (b): Size 1.5–3 cm
(c): Size >3 cm.
• Scarring I. No or mild fibrosis around fistula/vagina, and/or vagina length >6 cm or normal
capacity II. Moderate or severe fibrosis around fistula and/or vagina, and/or reduced vaginal
length and/or capacity III. Special considerations, e.g. circumferential fistula, involvement of ureteric
orifices.
Waaldijk’s system
• Type I: – Fistula =5 cm from the External Urethral Orifice and therefore not
involving the closing mechanism.
• Type II: – Fistula <5cm from the EUO therefore involves the closing mechanism
A. Without total involvement of the urethra: – (a) without a circumferential defect
– (b) with a circumferential defect
B. With total involvement of the urethra: – (a) without a circumferential defect
– (b) with a circumferential defect.
• Type III: Miscellaneous fistulae, e.g. uretero-vaginal and other exceptional fistulae.
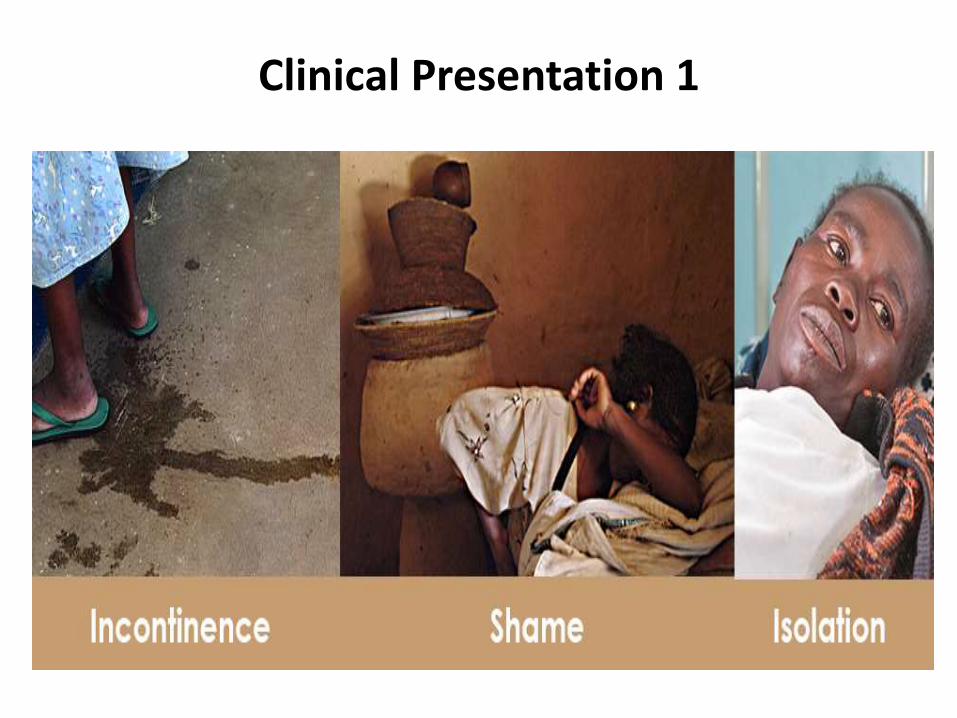
Clinical Presentation 1

Clinical Presentation 2• Constant urine drainage per vagina
• Excoriation of skin around the vulva
• Recurrent cystitis or UTI
• Unexplained fever, hematuria, flank discomfort and suprapubic pain
• Flatulence and or fecal incontinence
• Foul-smelling vaginal discharge
• Decubitus ulcers
• Psychosocial problems- social recluse; depression, low self-esteem, and insomnia

The Obstructed Labour Injury Complex
Obstructed Labour
Urologic Injury
GyneacologicalInjury
Gastrointestinal Injury
Neurological Injury
Psychosocial Injury
Fetal Injury
Dermatological Injury
Musculoskeletal Injury

Diagnosis
• History
• Physical Examination
• Investigations• FBC, Serum E/U/CR, Urine for urinalysis and M/C/S, Abdominopelvic USS
• 3 swab test
• Cystourethroscopy
• Intravenous Urogram


Figure 1. Obstetric vesico-vaginal fistula from prolonged obstructed labor.
Wall LL (2012) Obstetric Fistula Is a “Neglected Tropical Disease”. PLoS Negl Trop Dis 6(8): e1769. doi:10.1371/journal.pntd.0001769http://www.plosntd.org/article/info:doi/10.1371/journal.pntd.0001769

Sim’s Position

3 Swab test
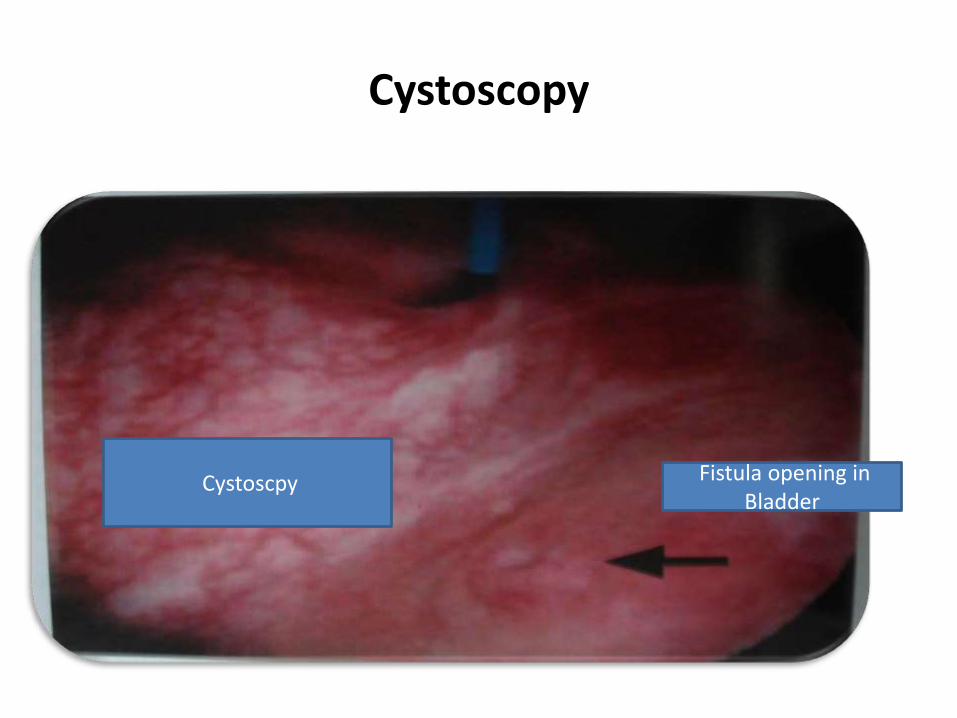
Fistula opening in Bladder
Cystoscpy
Cystoscopy

Management
• Conservative Management
• Surgical Therapy
• Nonsurgical Intervention
CONSERVATIVE MANAGEMENT
• Indications
– Simple fistulae
– <1 cm in size
– Diagnosed within 7 days of occurrence
• Continuous bladder drainage– By transurethral or suprapubic catheter for up to 4-6 weeks.
• Small fistulas may resolve spontaneously or decrease in size.

NON SURGICAL INTERVENTION
• Electrocautery fulguration
• Fibrin glue
• Laser welding with Nd YAG(neodymium-doped yttrium aluminium laser)
• Psychosocial counseling and rehabilitation

Surgical Management
• FISTULA REPAIR IS NOT AN EMERGENCY
• Most surgeons advise waiting at least 3 months from time of injury before operating.
• In the early months, the surrounding tissues are oedematousand hyperemic, making them friable and difficult to handle.

Preoperative care
• Improve the patient’s general condition- Nutrition, Infection, Dermatitis, Urine acidification, Psyche.
• Contractures should be treated before surgery if possible.
• Encourage liberal clear fluid intake until about 4hrs before surgery.
• Bowel preparation should include enema the night before.


Intraoperative Care
• Anesthesia: Spinal or GA
• Antibiotics: broad spectrum
• Suture material: – Vicryl 2-0 - bladder and vagina
– Polydioxanone 4-0 - ureter

Patient positioning

ROUTE OF REPAIR
• Depends upon access to the fistula site, mobility of the vagina
and surgeon expertise.
SITE APPROACH
LOW FISTULAUrethralJuxtaurethral
VAGINAL
CIRCUMFERENTIALLOSS OF BLADDER NECK
COMBINED ABDOMINOVAGINAL
MIDVAGINAL FISTULA TRANSVAGINAL
HIGH VAGINAL FISTULAPost hysterectomy Juxtacervical
ABDOMINAL OR VAGINAL

Principles of fistula repair
• First attempt is best .
Tissue mobilization
Hemostasis
Adequate exposure
Aseptic measures
Tension free closure
Reinforcement
Expertise

Repair of Vesicovaginal Fistula
• Vaginal approach
– Flap splitting technique
– Saucerization
– Latzko technique
• Abdominal approach– Transvesical repair
– Transperitoneal repair
– Combined repair

Abdominal approach
• Indications– High inaccessible fistula
– Multiple fistulas
– Involvement of uterus or bowel
– Need for ureteral re-implantation
– Complex fistula

Post-operative Management
• Continuous bladder drainage 10-14 days
• Vaginal packing for 24hrs
• Maintain output at 100ml / hr
• Antimicrobials
• Plenty of fluids for continuous bladder drainage
• Watch for any bladder block, fluid imbalance

Discharge Advice
• To pass urine frequently
• Avoid sexual intercourse for at least 3 months
• To defer pregnancy for at least 1 year
• Subsequent deliveries should be abdominal
• If repair fails, local repair should be reattempted after 3 months

Rectovaginal Fistula
• DEFINITION:Abnormal communication between the rectum and vagina with involuntary escape off flatus and/or feces into the vagina resulting in fecal incontinence.
• Clinical presentation:• Involuntary escape of flatus and/or feces into the vagina
• Foul smelling vaginal discharge with periodic uncontrolled escape of gas
• Appear immediately or 7-10 days after delivery

• Confirmation– Thin Probe is passed from the vagina through the fistulous tract into the rectum/anal canal– Methylene blue dye test– Examination under anaesthesia
• INVESTIGATIONS– Barium enema– Gastrograffin Enema– Barium meal+ follow through– Sigmoidoscopy– CT scans– MRI– Ultrasound

CLASSIFICATION
• Based on anatomical location of vaginal opening– Low - vaginal opening near the posterior fourchette
– Mid - from the level of the cervix to just superior to the posterior fourchette
– High -the fistula is in the area of the posterior fornix.
• Simple vs Complex– Simple are small fistulas
– Complex are large

Management
• SURGERY
Route:– Transvaginal Approach
– Transanal Approach
– Abdominal Approach
Timing: – Wait 8-12 weeks before surgical intervention to allow surrounding
inflammation to resolve completely

Prevention 1
• Primary Prevention– Girl Child Education– Women’s empowerment– Collaboration with religious and cultural practitioners
– Delayed age at child birth/access to contraceptives– Widespread antenatal care coverage and policies– Nutritious diet since childhood– Political will
• Secondary Prevention– Prevention of the 3 stages of Delay– Trained birth attendants and early referrals– Availability of emergency obstetric care

Prevention 2
– Caesarian section in indicated cases– Avoidance of difficult forceps and destructive operations– Prolonged Catheter drainage in prolonged or obstructed labour.
• Tertiary Prevention – Subsidized treatment – Rehabilitation– Re-integration into the society
The Nigerian Scenario
• Federal ministry of health: National strategic framework for the elimination of obstetric fistula in Nigeria 2011-2015 Provide framework to train health workers and guide them in the
provision of holistic, simple, affordable and evidenced based care for obstetric fistula patients.
http://www.fistulacare.org/pages/da/files/5/5.4/Nigeria_National_Strategy_2011-2015.pdf
• 23rd May- International Day to End Obstetric fistula

Fistula Centres 1
• Babbar Ruga Hospital, Katsina State
• Birnin Kebbi Specialist Fistula Center, Kebbi State
• Faridat Yakubu General Hospital, Zamfara State
• Laure Fistula Center at Murtala Mohammed Specialist Hospital, Kano State
• Maryam Abacha Women and Children’s Hospital (MAWCH), SokotoState

Fistula Centres 2
• National Fistula Center, Ebonyi State
• Ningi General Hospital, Bauchi State
• Ogoja General Hospital, Cross River State
• Sobi Specialist Hospital, Kwara State
• University College Hospital Ibadan, Oyo State

Conclusion
www.opfistula.org


References• Vesicovaginal Fistula: A Review of Nigerian Experience by M. A.
Ijaiya et al. West African Journal of Medicine Vol. 29, No. 5 September–October 2010
• Zacharin RF. A history of obstetric vesicovaginal fistula. ANZ Journal of Surgery,2000, 70:851-854.
• Maternal Mortality in 2000: Estimates developed by WHO, UNICEF and UNFPA,Geneva, World Health Organization, 2003,www.who.int/reproductive-health/publications.
• The World Health Report, 2005–Make every mother and child count, 2005, Geneva
References• Arrowsmith S, Hamlin C, Wall L. Obstetric labour injury complex:
obstetric fistula formation and the multifaceted morbidity of maternal birth trauma in the developing world. CME review article. Obstet Gynecol Surv 1996; 51: 568–74.
• Goh JWT, Krause HG. Female Genital Tract Fistula. Brisbane: University of Queensland Press, 2004.
• Waaldijk K. Step by Step Surgery of Vesico-Vaginal Fistulas. Edinburgh: Champion Press, 1994. Waaldijk K. The immediate management of fresh obstetric fistula. American Journal of Obstetrics and Gynecology. 2004, 191 :795-9.
Waaldijk K. Surgical classification of obstetric fistula. International Journal of Gynecology and Obstetrics, 1995, 49 :161-163.
• Obstetric fistula is a preventable and curable cause of maternal mortality and morbidity with Nigeria accounting for about 10% of global mmr.
• However it has continued to be a hidden condition because it affects the the most marginalized members of the society-poor,young,illiterate girls and women.
• We all as obstetricians and gynecologist have an oppurtunity to turn despair to hope and restore dignity to these women.