ocd cnt premnath
TRANSCRIPT
OBSESSIVE COMPULSIVE
DISORDER
Premnath R.
Definition
Obsessive compulsive disorder is a disorder
characterized by two main clinical features, recurrent
obsessions or compulsions (or a combination of both)
that are severe enough to cause marked distress or
significant deterioration in general functioning.
Obsessions:
It is defined as unwanted, intrusive, persistent ideas, thoughts, impulses or images that cause marked anxiety or distress. The most common include repeated thoughts about contamination, imagining doing harm, repeated doubts, a need to have things in a particular order aggressive or horrific impulses of sexuality and violence.
(APA, 2000)
Compulsions:
It is defined as unwanted repetitive
behaviour patterns or mental acts that are
intended to reduce anxiety, not to provide
pleasure or gratification. The common
compulsions involve ordering and
arranging, checking, touching, praying,
focusing on a number etc.
(APA, 2000)
Epidemiology
•It is equally common in men and women.
•Age of onset; 6-15 in males & 20-29 in females
•Onset is usually in childhood or early adult life.
•The course is variable and more likely to be chronic.
•Lifetime prevalence 2-3%.
•It is the fourth most common psychiatric disorder
(Rasmussen & Eisen, 1992)
•Tenth leading cause of disability in the world(WHO)
•Remains a significant social and health service
concern with high degrees of personal disability, co-
morbidity and relatively poor long-term prognosis
(Eisen et al., 1999;)
Common Obsessions & Compulsions
Obsessions
• Contamination
• Pathological doubt
• Somatic
• Need for Symmetry
• Aggressive
• Sexual
• Blasphemous
Compulsions
• Checking
• Washing
• Counting
• Need to ask or confess
• Ordering & Arranging
• Hoarding
• Miscellaneous rituals
Classification
F42 Obsessive-compulsive disorder
F42.0 Predominantly obsessive thoughts or
ruminations
F42.1 Predominantly compulsive acts
F42.2 Mixed obsessional thoughts and acts
F42.8 Other obsessive-compulsive disorders
F42.9 Obsessive-compulsive disorder, unspecified
Etiology
• Genetic factors
• Biological factors
• Psychoanalytic theory
• Behaviour theory
Genetic factors
• Twin studies have consistently found a significantly
higher concordance rate for monozygotic twins
than for dizygotic twins.
• Family studies of these patients shown that 35% of
the first degree relatives of OCD patients are also
affected by the disorder.
Biological factors
• Abnormal levels of the neurotransmitter, serotonin
in individuals with OCD.
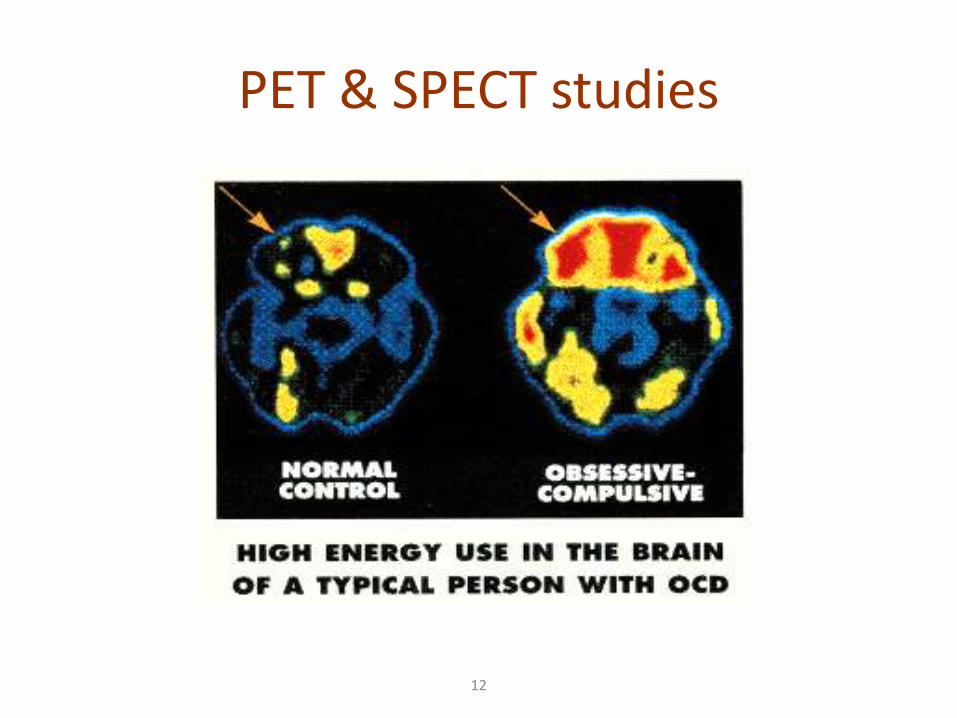
• PET & SPECT have shown increased metabolism
and blood flow in the frontal lobes, basal ganglia,
cingulum of patients with OCD.
• CT and MRI studies revealed, bilaterally decreased
size of caudate in patients with OCD. In some
patients, enlarged basal ganglia can be noted.
12
PET & SPECT studies
Psychoanalytic theory
• Individuals with OCD have weak, under developed
egos.
• Clients with OCD are regressed to developmentally
earlier stages of the infantile super ego, whose harsh,
punitive characteristics, which now reappear as part of
the psychopathology.
• Regression to the pre-oedipal, anal sadistic phase
combined with the use of specific ego defense
mechanisms (isolation, undoing, displacement,
reaction formation) produces the clinical symptoms
of obsessions and compulsions.
Behaviour theory
• This theory explains obsessions as a conditioned
stimulus to anxiety.
• Compulsions have been described as learned
behaviour that decreases the anxiety associated
with obsessions.
• This decrease in anxiety positively reinforces the
compulsive acts and they become stable learned
behaviour.
Clinical Features• Obsessional thoughts
Words, ideas and beliefs that intrude forcibly into patient’s mind. They are usually unpleasant and shocking to the patient and may be obscene or blasphemous.
• Obsessional image
These are vividly imagined scenes, often of a violent or disgusting kind involving abnormal sexual practices.
• Obsessional ruminations
These involve internal debates in which arguments for and against even the simplest everyday actions are reviewed endlessly.
• Obsessional impulses
These are urges to perform acts, usually of a violent
or embarrassing kind, such as injuring a child,
shouting in church.
• Obsessional rituals
These may include both mental activities counting
repeatedly in a special way or repeating a certain
form of words, and repeated but senseless
behaviors. Sometimes such compulsive acts may be
preceded by obsessional thoughts.
• Obsessive slowness
Severe obsessive ideas or extensive compulsive rituals characterize obsessionalslowness in the relative absence of manifested anxiety. This leads to marked slowness in daily activities.
Other features are
• Recognition that the thoughts are produced in his or her own mind.
• Lack of concentration and task completion.
• Impaired social or work functioning.
Course and prognosis
•Long and fluctuating course
•Prognosis appears to be worse when the onset is in
childhood, the personality is obsessional, symptoms
are severe, compulsions are bizarre, or there is a
coexisting major depressive disorder.
Diagnosis
• History collection, Mental Status Examination, Physical
examination
• Imaging studies like MRI, CT, PET
• Based on ICD criteria
• Rating scales to assess severity of OCD.
E.g. Y-BOCS (Yale-Brown Obsessive Compulsive Scale),
Maudsley Obsessive Compulsive Inventory.
TREATMENT
Pharmacotherapy
• Benzodiazepines; limited role
E.g. alprazolam, clonazepam
• Antidepressants;
SSRIs- e.g. Fluoxetine 20-80mg/day, Fluvoxamine
50-200mg/day, Paroxetine 20-40mg/day, and
Sertraline 50-200mg/day.
• Non-specific SRI- Clomipramine 75-300mg/day, was
the first drug used effectively in the treatment of OCD.
• Antipsychotics; Occasionally used in low doses in the
treatment of severe, disabling anxiety. E.g. haloperidol,
risperidone, aripiprazole, pimozide
• Buspirone has also been used beneficially as an adjunct
for augmentation of SSRIs.
Psychotherapy
• Psychoanalytic psychotherapy to those patients
who are psychologically oriented.
• Supportive psychotherapy to the clients as well
as the family members.
Behavior therapy
• Exposure and Response Prevention (ERP)
• Thought stoppage
• Relaxation technique
• Systematic desensitization
• Modeling
• Aversive conditioning techniques
• Exposure and Response Prevention (ERP):
It involves repeated exposure to the source of patient’s
obsession. Then the patient is asked to refrain from the
compulsive behavior that the patient usually performed
to reduce the anxiety.
For example, compulsive handwashers are encouraged
to touch contaminated objects and then refrain from
washing in order to break the negative reinforcement
chain.
• Thought stoppage: It help an individual to learn to stop
thinking unwanted thoughts. Steps are,
– Ask client to sit comfortably and ask to bring the
unwanted thoughts into the conscious mind at a rate
of one at a time.
– As soon as the thought forms, give the command
‘STOP’. Follow this with calm and deliberate
relaxation of muscles and diversion of thought to
something pleasant.
– Repeat the procedure to bring the unwanted thought
under control.

• Relaxation technique: Includes deep breathing
exercise, Progressive Muscle Relaxation, meditation,
imagery, music etc.
• Modeling- The person is exposed to a model behavior
and is induced to copy it.
• Aversive conditioning techniques- Pairing of pleasant
stimulus with unpleasant response, so that even in
absence of unpleasant response, the pleasant
stimulus becomes unpleasant by association.
Systematic desensitization-
It is based on work of Joseph Wolpe.
Desensitization (also known as exposure
therapy), is a cognitive-behavioral therapy in
which people are gradually exposed to the
frightening object or event until they become used
to it and their physical symptoms decrease.
Components of Desensitization
• Relaxation
• Hierarchy construction
• Visualizations
• Item presentation
• In vivo assignments
Procedure
• Teach progressive relaxation.
• The client is asked to outline an anxiety or phobia hierarchy, a step by step approximation of the feared situation in which the client, with guidance from the therapist, lists the lowest anxiety situation to the highest. This is called hierarchy construction.
• During visualization training, a client imagines himself in a variety of situations.
• In item presentations client relaxes and then
imagines himself in each of phobic situations on the
hierarchy he was created. It should be done in a slow
and systematic fashion: one item at a time.
• The client is advised to signal whenever anxiety is
produced. With each signal, he is asked to relax. After a
few trials, the client is able to control his anxiety.
• Thus gradually the hierarchy is climbed till the
maximum anxiety-provoking stimulus can be faced in
absence of anxiety.
Electroconvulsive therapy
• Indicated in patients with severe depression,
suicidal risk etc.
Psychosurgery
• The procedures used are Stereotactic limbic
leucotomy and Stereotactic subcaudate
tractotomy.
• It is available only at very few centers in the world.
NURSING MANAGEMENT
Assessment
• Collection of physical, psychological and social data
• Know the impact of obsessions and compulsions on
physical functioning, mood, self-esteem and
normal coping ability
• Identify defense mechanisms used, thought
content, potential for suicide, ability to function,
and social support system available.
Nursing diagnosis 1
• Severe Anxiety related to earlier life conflicts as evidenced by repetitive action (e.g., hand-washing), recurring thoughts (e.g., dirt and germs), decreased social and role functioning
Goals
• Demonstrates ability to cope effectively with stressful situations without resorting to obsessive thoughts or compulsive behaviors.
Interventions
• Establish relationship through use of empathy, warmth,
and respect.
• Verbalize empathy toward client’s experience rather than
disapproval or criticism.
• Assist client to learn stress management, (e.g., thought-stopping, relaxation exercises, imagery).
• Identify what the client perceives as relaxing (e.g.warmbath, music).
• Engage in constructive activities such as quiet games that require concentration.
• Encourage participation in a regular exercise program.• Give positive reinforcement for non-compulsive
behavior. Avoid reinforcing compulsive behavior. • Assist client to find ways to set limits on own behaviors.
At the same time allow adequate time during the daily routine for the ritual(s).
• Limit the amount of time allotted for the performance of rituals. Encourage client to gradually decrease this time.
• Discuss home situation, include family in discharge plan.
Nursing diagnosis 2
• Ineffective individual coping related to underdeveloped ego, punitive superego, avoidance learning, possible biochemical changes, evidenced by ritualistic behavior or obsessive thoughts.
Goal
• Demonstrates ability to cope effectively without resorting to obsessive-compulsive behaviors.
Interventions
• Work with patient to identify the situations that increase anxiety and result in compulsive acts.
• Encourage independence in patient and give positive reinforcement for independent behaviors.
• In the beginning of treatment, give plenty of time for ritualistic behavior. Do not be judgmental or verbalize disapproval of behavior.
• Support patient’s efforts to explore the meaning and purpose of behavior.
• Provide structured schedule of activities for the patient, including adequate time for completion of rituals.
• Gradually limit the amount of time allotted for ritualistic behavior as patient becomes more involved in unit activities.
• Give positive reinforcement for non-ritualistic behaviors.
• Help patient to learn techniques like thought stopping, relaxation and exercise.
Nursing diagnosis 3
• Impaired social interaction related to inability to control thoughts, images and impulses in a purposeful, voluntary manner.
Goal
• Verbalizes understanding that thoughts, impulses and images are involuntary and may worsen with stress.
Interventions
• Approach client in a calm, direct, non-authoritarian manner, using a soft tone of voice.
• Listen actively to the client’s obsessive themes no matter how absurd or incongruent they may seem.
• Assist client to gain control of overwhelming feelings and impulses through verbal interactions.
• Protect the client who is at the risk for suicide.
• Assist client in planning the rest periods between planned activities and rituals.
• In the beginning of treatment, give plenty of time for ritualistic behavior. Do not be judgmental or verbalize disapproval of behavior.
• Gradually limit the amount of time allotted for ritualistic behavior as patient becomes more involved in unit activities.
• Activate the client toward activities that will reduce stress or anxiety (warm bath, taking walk, listening to music etc.)
• Ask client to stay connected to family and friends.
• Ask client to choose one or two ‘worry periods’ each day,
time he can devote to obsessing. Choose a set and place.
During this time, focus only on negative thoughts or
urges. Don’t try to correct them. At the end of worry
period, take a few calming breaths, let the obsessive
thoughts or urges go, and return to normal activities. The
rest of the day, however, is to be designated free of
obsessions and compulsions. When thoughts or urges
come into patient during the day, write them down and
‘postpone’ them to worry period.
Nursing diagnosis 4
• Ineffective role performance related to the need to perform rituals, evidenced by inability to fulfill usual patterns of responsibility.
Goal
• Client resumes role-related responsibilities.
Interventions
• Determine patient’s previous role within the family and the extent to which this role is impaired by the illness.
• Encourage patient to discuss conflicts evident within the family system. Identify the responses of patient and family members.
• Explore available options for changes in role. Practice through role-play.
• Give patient lots of positive reinforcement for ability to resume role responsibilities by decreasing need for ritualistic behaviors.
