october 27 shortness of breath in the er - capa - … · overview •different cases of shortness...
TRANSCRIPT

Shortness of Breath in the ER
October 27th,2017
Stéphane Léveillé CD
Physician Assistant ER & OR
Kirkland & District Hospital

• Disclosure • I attest that my presentation will provide a balanced view of
therapeutic options and will be entirely free of promotional bias.
• that neither I nor my spouse has a current financial relationship with the grantor and/or any commercial interest(s) that may have a direct interest in the subject matter of the CPD program.

Overview • Different Cases of Shortness of Breath seen in
the Emergency
• Shortness of Breath 1. Determine the severity of the Shortness of breath,
2. Distinguish the source (Cause) of the shortness of breath,
3. Understand the evidence for various treatments for acute
shortness of breath,
4. Don’t judge a books by it’s cover
• Elderlies are more fragile
• Not because they are young means they are healthy.

Overview

Case Study 03 March
78 year old female, Healthy,
Triage: Presents to the Emergency department with the primary complaint of cough X 3 weeks, clear mucous expectorant, increase Shortness of Breath with exertion, not sleeping well, sore back from coughing. Tried Benelyn syrup yesterday with no relief.
Past Medical History:
• Hypothyroidism
Allergies:
• Sulfa
• Surgical Tape
Vitals: Blood pressure 181/103, Pulse 91, Temperature 35.3, Respiratory Rate 20
Oxygen saturation 95% room air
Repeat vitals: BP 161/86, P 80, O2 sat 96% room air

Case Study
Assessment: 78 year old female, cough X 3 weeks, began with chest cold and head aches, mild fever – resolved, light cough present, had sinus congestion – resolved, ribs sore with cough, denies Chest pain.
Exam: Well, Blood pressure up slightly,
No respiratory distress
chest good – no wheezing, no crackles, congested
Cardio Vascular System – Normal, no murmurs
Plan: Biaxin 500mg BID X 7 days, Return if not resolving
Discharge Diagnosis: Upper Respiratory Infection (URI)

Case Study Returned 28 March
78 year old female, seen in ER March 3rd
Triage: Complaining of Short of Breath for a few weeks but today feeling much
worse, was on antibiotic for chest infection, finished on March 10th, was
Prescribed a new puffer last week but not helping.
Past Medical History:
• Hypothyroidism
Allergies:
• Sulfa
• Surgical Tape
Vitals: BP 191/116, P 138, T35.8, RR 30, O2 sat 94%

Case Study Assessment: 78 year old female presented to Emergency Department with a main complaint of Shortness of Breath for the past few weeks but has been getting some back discomfort since yesterday. This morning when she was walking out to the vehicle she had some increase shortness of breath and decide to come to the Emergency Department. The patient was put on antibiotic March 3rd and had taken all of the antibiotics. Also, the patient is on a puffer but states that it does not appear to be helping her at this time.
Past Medical History:
• Hypothyroidism
• HTN
Past Surgical History:
• 2014 -Uterine Prolapse, Cystocele
• 2014 -Vaginal Hysterectomy
• 2001 - Left Mastectomy (Carcinoma)
• 2000 - Left Breast biopsy (no malignancy)
Family History:
• Father died of lung cancer
• Brother died of Leukemia
Social History: Live at home with husband
Retire Secretary
Non smoker
Alcohol – Has a glass of wine at supper with her meal
Exam: Ear, nose and throat – Normal
Heart – Irregular heart rhythm, no murmurs heard
Respiratory – good air entry left lung field
- decrease air entry right lung field
- No wheezing or crackles heard
No pitting edema lower limbs
Investigation: Chest Xray
Blood work: CBC, Lytes, BUN, Cr, BS, Trop, LFT’s, INR, PTT, Ca++,
Mg+, Phosphate
Electrocardiogram

Electrocardiogram

Chest X-Ray

Chest X-Ray

Laboratory Investigations
Hematology
WBC 8.8 RBC 4.62 Hgb 140 Plt Count 348
Chemistry
Na 129 K+ 4.5 Cl 95 Urea 5.9
GFR 89 Cr 57 Glu 7.1 Ca+ 2.26
Phos 1.22 Mg+ 0.75 GGT 118 AST 37
ALT 43 Alk Phos 144 Trop 0.01
Coagulation
INR 1.1 aPTT 28

WHAT’S NEXT

What is next:
1. New onset Atrial Fibrillation
2. Pleural effusion right lung
3. Blood work is Normal with mild elevation in the liver function test
GGT 118 Alk Phos 144
Plan:
Intravenous
Catheter
Medication: Metoprolol 5mg IV
Furosemide 20mg IV
Investigation: Computed Tomography (CT) Scan of chest
Admit to Hospital

C.T Scan
Look at the CT Scan here…….

Chest Tube

Lateral view
Admission to Hospital
Put on Beta blocker (Bisoprolol),
Levonox.
Current medication: Coversyl, Synthroid
Transferred to Sudbury to see Specialist 5 April
Thoracic surgeon - Repeat CT: Chest, Abdomen and Pelvic
- Bronchoscope
- Thoracoscope
- Biopsy
Oncology consult - Metastatic Adenocarcinoma (Ovarian)

Conclusion Case Study
78 year old female
Metastatic Adenocarcinoma (Ovarian)
Treatment : Palliative systemic treatment with Chemo therapy.
Any
Question
Case Study #2 9 June
43 year old Male, otherwise Healthy,
Triage: Presents to the Emergency department with the primary complaint of Shortness of breath for the past weeks, no expectorant, increase Shortness of Breath with exertion, not sleeping well. Recently had surgery, right hip replacement on June 6th, post motorcycle accident.
Past Medical History: Healthy
Age 4, Broke right Femur, Tibia and Fibula
Past Surgical History: 2013 Right Hip replacement
1998 Right shoulder – labrum tear, AC tear
1997 Left Knee - Meniscal tear
1994 Right elbow – Bursectomy
Family History: Father decease age 41 – Mining accident

Case Study #2 Social History: Married 20 years
3 children at home
Smoker 1PK/Day 30 years
Alcohol – Occasion
Drugs - None
Medication : Xeralto post operation and Tylenol #3, PRN
Allergies: Penicillin
Vitals: Blood pressure 107/74, Pulse 63, Temperature 36.6, Respiratory Rate 18
Oxygen saturation 97% room air

Case Study #2
Assessment: 43 year old male, complaint increase shortness of breath and chest pain. Describes it as a squeezing pain in the center of the chest. It is non-radiant, not associated with sweating but breathlessness. Denies fever, chills. Pain lasting for hours.
Exam: Ear, nose and throat – Normal
Heart – regular heart rhythm, no murmurs heard
Respiratory – good air entry bilat
- No wheezing or crackles heard
No pitting edema lower limbs
Investigation: Chest Xray
Blood work: CBC, Lytes, BUN, Cr, BS, Trop,, INR,D-Dimer

Chest X-Ray

Laboratory
WBC 7.3 RBC 3.43 Hgb 101
Plt Count 147 Na 138 K+ 3.6
Cl 100 Urea 4.5 Cr 78 EGFR 94 Glu 7.8 CK 987
Trop 0.01 INR 1.4 D-Dimer 987

Case Study #2
Diagnosed: SOB NYD
Plan - Discharged home
- Felt unwell for about a week and then the symptoms improved
IS THIS IT…………….NOT

Case Study #2 28 July
43 year old Male, otherwise Healthy,
Triage: Presents to the Emergency department with the primary complaint of Shortness of breath, increase shortness of breath on exertion. not sleeping well. Denies fever, chills or cough
Past Medical History: Healthy
Age 4, Broke right Femur, Tibia and Fibula
Past Surgical History: 2013 Right Hip replacement
1998 Right shoulder – labrum tear, AC tear
1997 Left Knee - Meniscal tear
1994 Right elbow – Bursectomy
Family History: Father decease age 41 – Mining accident
uncle on mother’s side with Cardiomegaly Unknown
Grand Mother (mother’s side) sudden death, Cardio infact.

Case Study #2
Social History: Married 20 years
3 children at home
Smoker 1PK/Day 30 years
Alcohol – Occasion
Drugs - None
Medication : Xeralto post operation and Tylenol #3, PRN
Allergies: Penicillin
Vitals: Blood pressure 110/72, Pulse 72, Temperature 35.6, Respiratory Rate 28
Oxygen saturation 95% room air

Case Study #2
Assessment: 43 year old male, complaint increase shortness of breath and shortness of breath on exertion. Describes it as a squeezing in the center of the chest. It is non-radiant, not associated with sweating but breathlessness. Denies fever, chills.
Exam: Ear, nose and throat – Normal
Heart – regular heart rhythm, no murmurs
heard
Respiratory – good air entry bilat
- No wheezing or crackles heard
No pitting edema lower limbs
Investigation: Chest Xray
Blood work: CBC, Lytes, BUN, Cr, BS,
Trop,, INR,D-Dimer

Chest X-Ray

Laboratory
Every test was normal, with the exception of the D-Dimer which was 2160
WHAT NEXT ….
Computed Tomography Scan (CT) Pulmonary Angio
Report: revealed no definite evidence for a pulmonary embolus. There was mediastinal adenopathy. Uncertain significance. No evidence of pleural effusion, pneumothorax or pneumonia..
Cardiac Echo
Report: Left ventricle enlargement 72mm and left atrium 54mm
Ejection fraction 28

Specialist Internal Medicine Consult
- Shortness of breath most likely to a viral cardiomyopathy.
- Start medication 40mg Furosemide, Digoxin 3.125 and slow K 2 tabs od.
- Urgent referral to Cardiologist Mount Sinai Toronto.
Cardiologist Consult
- Admit to Intensive Care Unit (1 week).
- Testing during admission
- Muga Heart scan (multiple-gated acquisition) Nuclear imaging : EF 24%
- MRI (Magnetic Resonance Imaging) : Negative, nil acute
- Angiogram : Negative
- All blood work : Negative
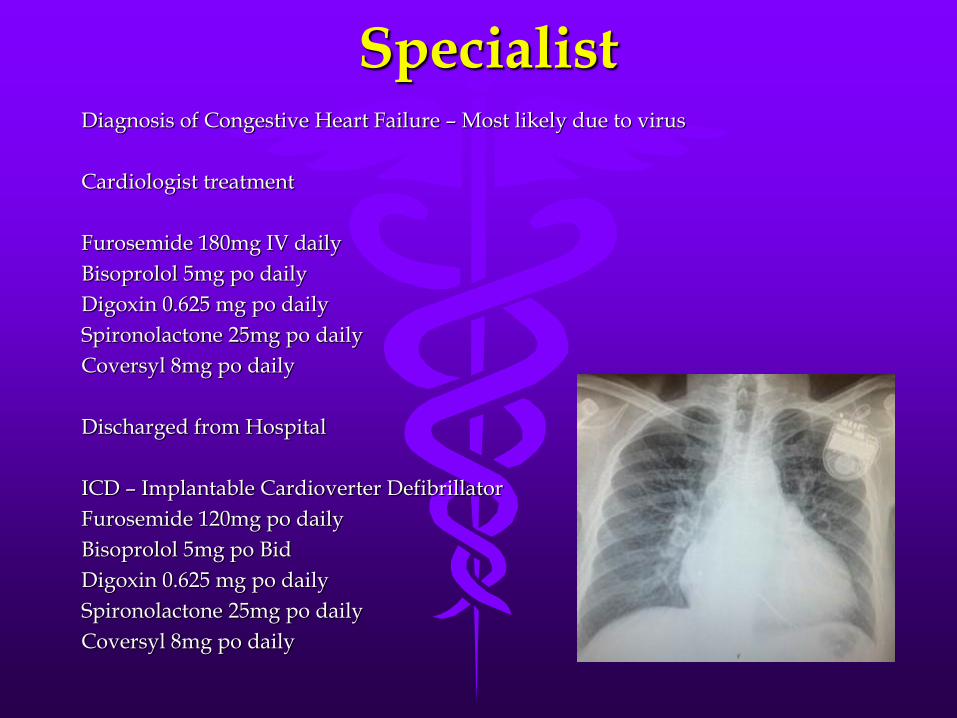
Specialist Diagnosis of Congestive Heart Failure – Most likely due to virus
Cardiologist treatment
Furosemide 180mg IV daily
Bisoprolol 5mg po daily
Digoxin 0.625 mg po daily
Spironolactone 25mg po daily
Coversyl 8mg po daily
Discharged from Hospital
ICD – Implantable Cardioverter Defibrillator
Furosemide 120mg po daily
Bisoprolol 5mg po Bid
Digoxin 0.625 mg po daily
Spironolactone 25mg po daily
Coversyl 8mg po daily

Conclusion Case Study
Patient is 5 years post insertion of ICD
- Check-up - Having unsustain V.T (no shock)
- Mild SOBOE
- EF 22%
- Continues with daily activities
- Cardiologist - Genetic testing done +
- Family members tested
- Son has the Gene
- Sister and her 2 daughters have Gene
- At risk for sudden death…

Conclusion
1. Not all shortness of breath are simple as a common cold
2. Always expect the worst in Shortness of breath
3. Don’t treat the age, treat the condition and acuteness
4. Symptoms can be sneaky, be careful, not because they are SOB mean that they have a lung issue, it can also be cardiac.

Questions &
Discussion