ocular surface squamous neoplasia
TRANSCRIPT
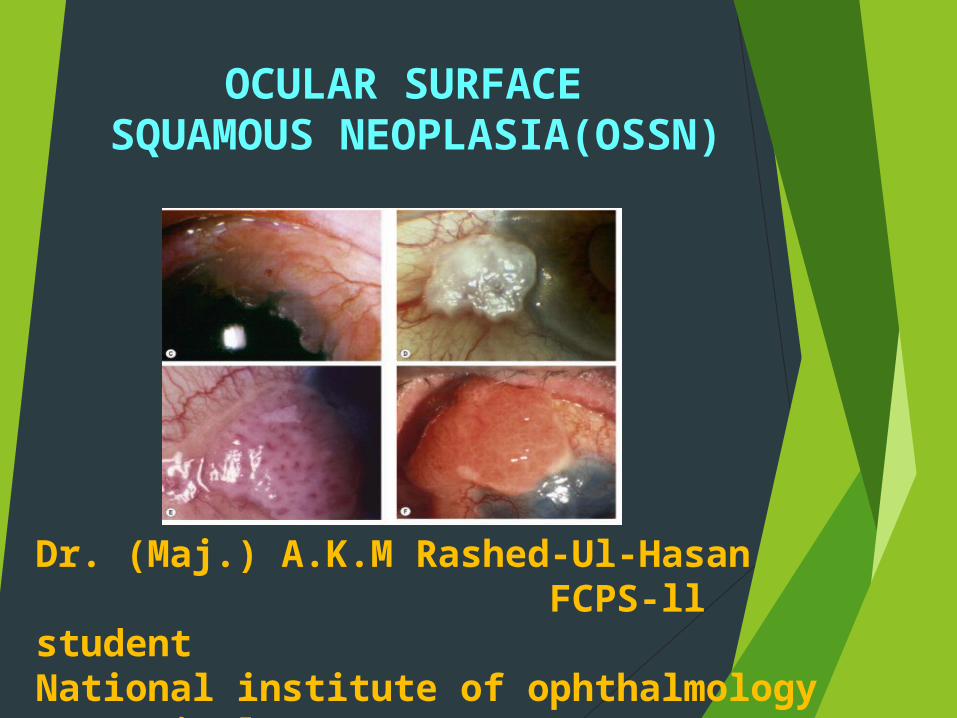
OCULAR SURFACE SQUAMOUS NEOPLASIA(OSSN)
Dr. (Maj.) A.K.M Rashed-Ul-Hasan FCPS-ll studentNational institute of ophthalmology & HospitalDhaka

OCULAR SURFACE denotes involvement of the conjunctiva or cornea
SQUAMOUS excludes other epithelial cells such as basal cells and melanocytes
NEOPLASIA includes both dysplastic and carcinomatous lesions.
Definition
The term Ocular Surface Squamous Neoplasia [OSSN] presently refers to the entire spectrum of dysplastic, pre-
invasive and malignant squamous
lesions of the conjunctiva and cornea
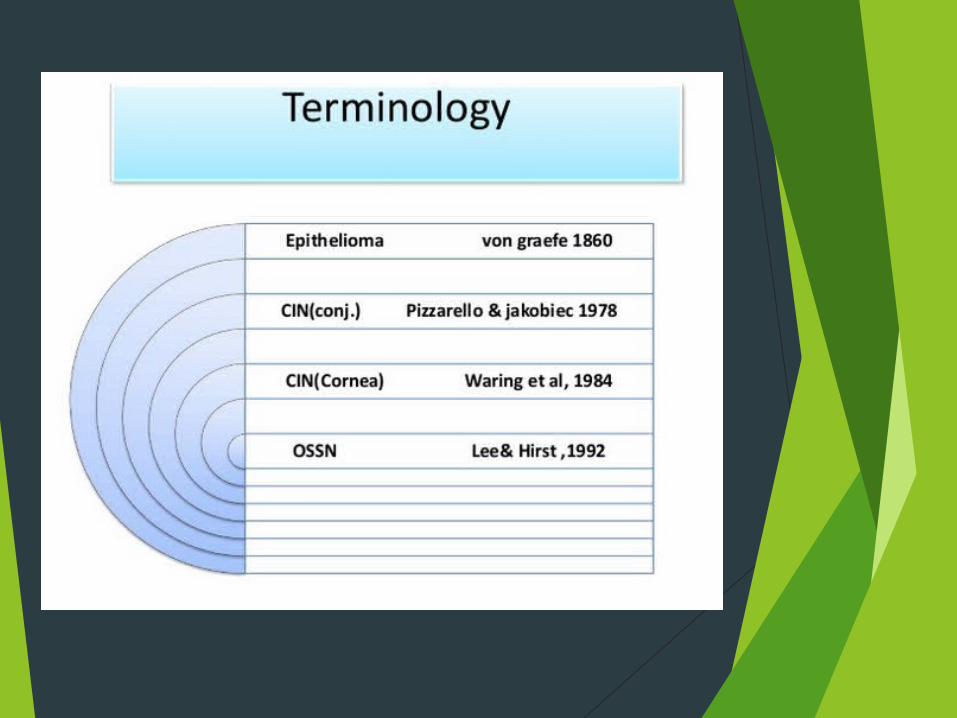
Lee and Hirst classified OSSN as:- I. BENIGN DYSPLASIA
• Pseudoepitheliomatous hyperplasia • Benign hereditary intraepithelial dyskeratosis
II. PREINVASIVE OSSN • Conjunctival/corneal carcinoma in situ
III. INVASIVE OSSN • Squamous carcinoma • Mucoepidermoid carcinoma – aggressive
Epidemiology Third most common ocular tumour after
melanoma and lymphoma Caucasians older age group(6-7 decade) Males >females Patiens with HIV and Xeroderma pigmentosum
present earlier
All young patients with OSSN should be screened for HIV.

Risk factors
Ultraviolet light Immunosuppression/ HIV Human papillomavirus (HPV)- Type 16
& 18
Mutation or deletions of tumor suppressor gene p53

Clinical Features Patients may be asymptomatic or present
with chronic redness and irritation of the eye.
Visual acuity is not affected unless there is extensive corneal involvement
In most cases, patient has the history of several months.

Location OSSN normally occurs in
Interpalpebral region arising from the limbal stem cells, involving the bulbar conjunctiva, the cornea or both of these structures
Clinically : The lesions are described as being
slightly elevated, variably shaped, relatively sharply demarcated from the surrounding normal tissues.
Accompanied by feeder blood vessels
Color vary from pearly gray to reddish gray depending on the vascularity of the tumor .
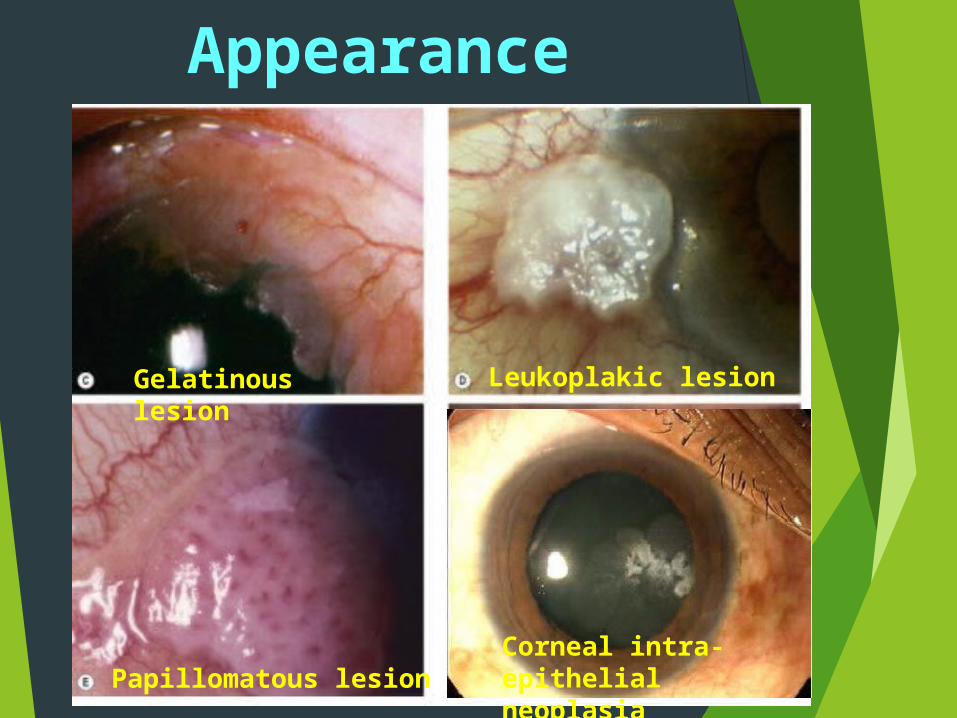
Gelatinous lesion Leukoplakic lesion
Papillomatous lesion Corneal intra-epithelial neoplasia
Appearance
In clinical practice, gelatinous type is the commonest. These lesion can be
Circumscribed, which are most common
Nodular variety, which has a propensity for rapid growth
Diffuse variety, the least common, which can masquerade as chronic conjunctivitis
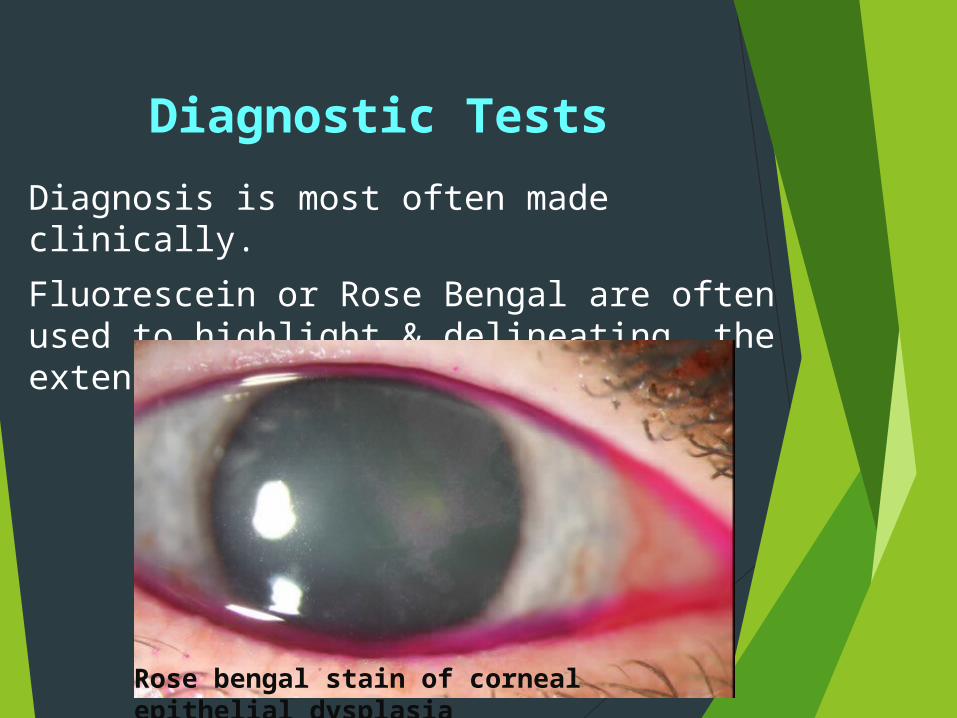
Diagnostic TestsDiagnosis is most often made clinically. Fluorescein or Rose Bengal are often used to highlight & delineating the extent the lesion.
Rose bengal stain of corneal epithelial dysplasia

a. Anterior Segment Optical Coherence Tomography (ASOCT)
b. Impression cytologyc. Confocal microscopyd. High frequency ultrasounde. Histopathology
Diagnostic Tests
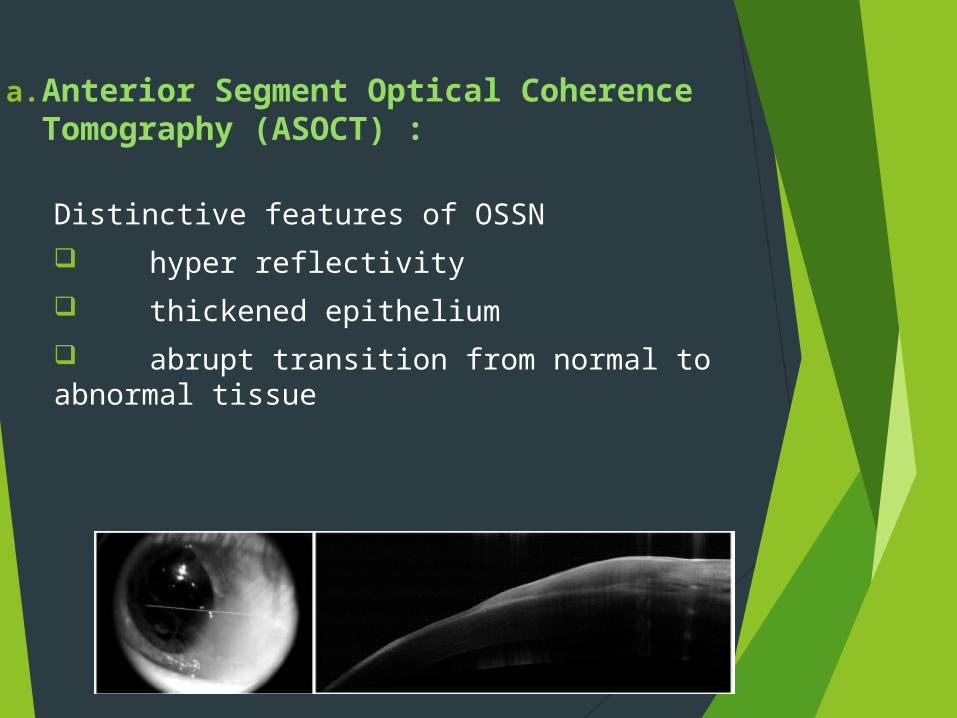
a. Anterior Segment Optical Coherence Tomography (ASOCT) :
Distinctive features of OSSN hyper reflectivity thickened epithelium abrupt transition from normal to abnormal tissue
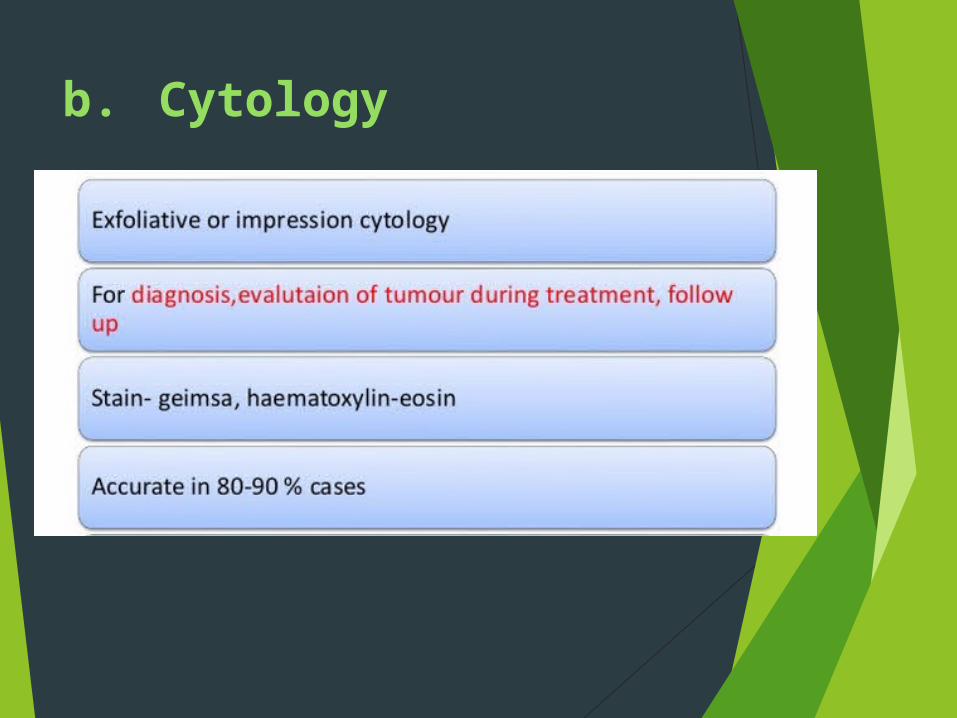
b. Cytology

c.Confocal microscopy
- helpful in guiding treatment since it is able to reveal cellular details.
- difficulte of use and limited field of view
d. Histopathology
DYSPLASIA:
Mild - less than a third thickness occupied by atypical cells
Moderate - three quarters thickness occupied by atypical cells
Severe - nearly full thickness occupied by atypical cells
d. Histopathology
CARCINOMA IN SITU: as above with loss of the normal surface layer
INVASIVE SQUAMOUS CELL CARCINOMA: as above with basal epithelial layer has been breached and invasion of the substantia propria has occurred.

d. Histopathology

d. Histopathology
Mild dysplasia
Severe dysplasia
Carcinoma in situ
Invasive SCC

e) High frequency ultrasound
extent of invasion into the eye in cases of SCC.
Differential Diagnosis
Pterygium Papilloma Pingueculum Nevus Malignant melanoma Pyogenic granuloma
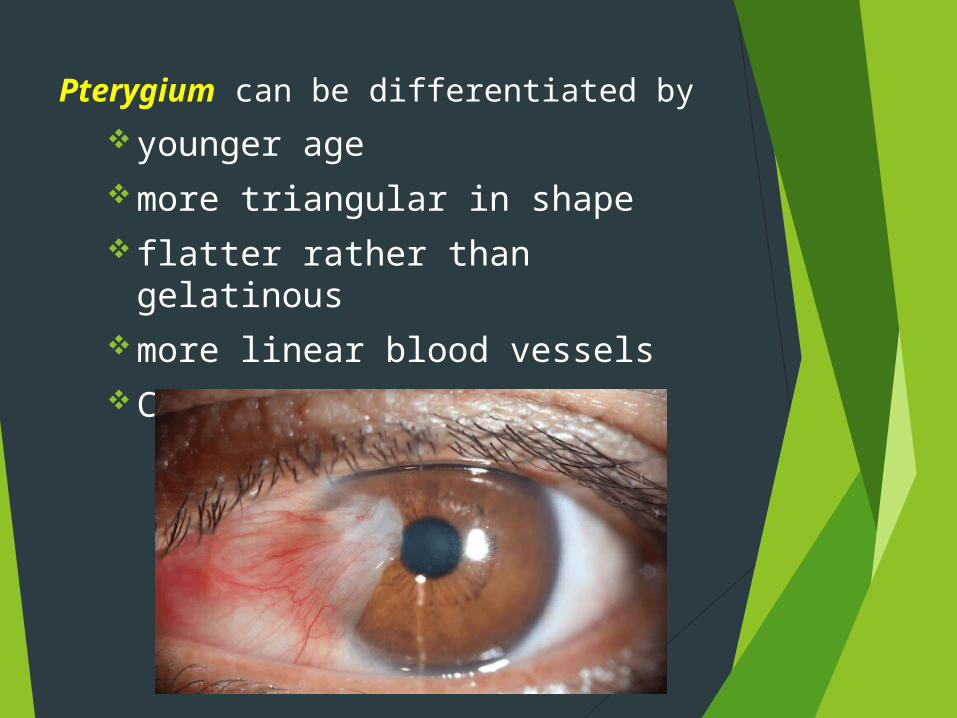
Pterygium can be differentiated byyounger agemore triangular in shapeflatter rather than gelatinousmore linear blood vesselsCause more symptoms
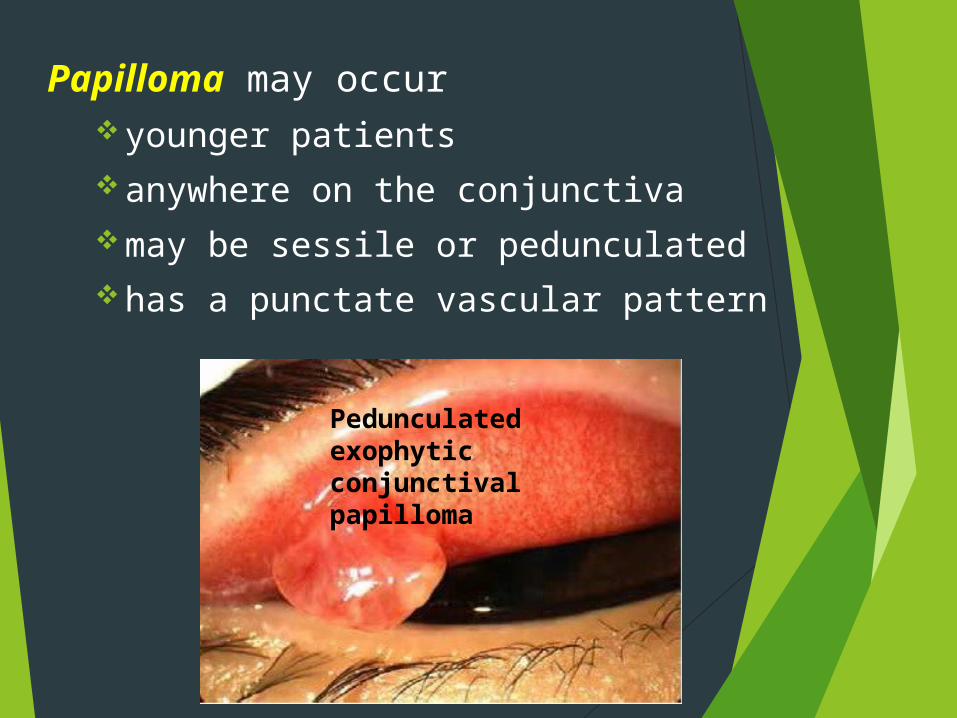
Papilloma may occur younger patientsanywhere on the conjunctivamay be sessile or pedunculatedhas a punctate vascular pattern
Pedunculated exophytic conjunctival papilloma

Malignant melanoma has a regular smooth surface, lacks gelatinous or leukoplakic
surface may be ulcerated
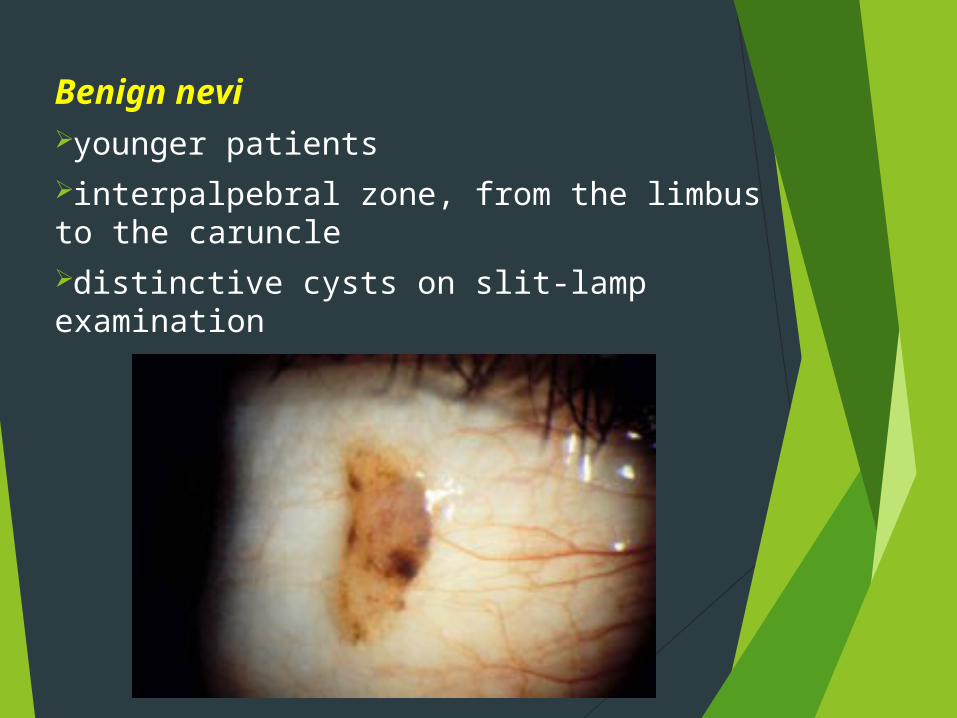
Benign neviyounger patientsinterpalpebral zone, from the limbus to the caruncledistinctive cysts on slit-lamp examination

Surgery ChemotheraphyCryotheraphy Radiotheraphy
Treatment

Surgical excision

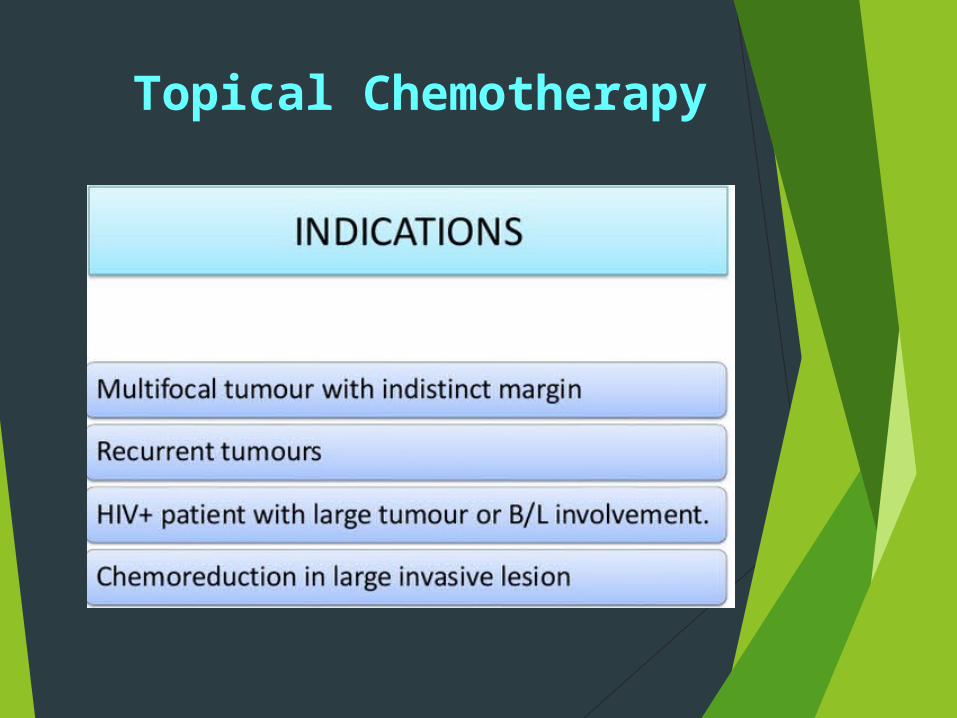
Topical Chemotherapy
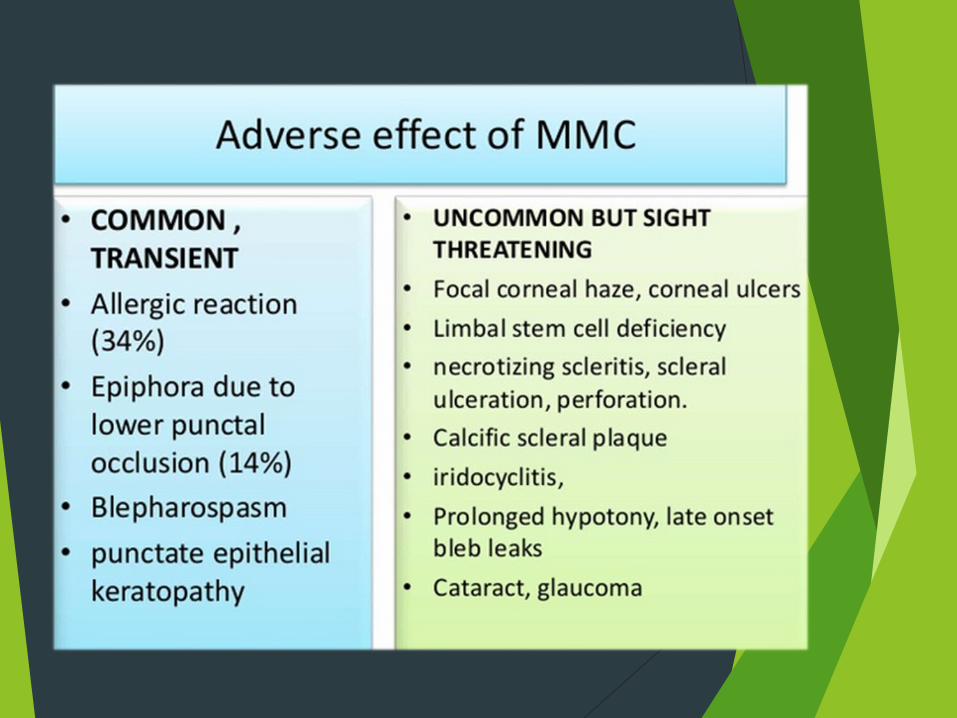
MITOMYCIN C Most commonly used A non cell cycle specific ALKYLATING
AGENT that acts by alkylating the cross-linked DNA and inhibits DNA, RNA, and protein synthesis
0.04% four times a day for 1 week with two to three cycles in alternate weeks
Success rates ranging from 87 to 100% have been reported.
5-FU
Pyrimidine analogue that acts by integrating with the DNA during S phase. It also interferes with RNA synthesis.
It is used as 1% topical solution four times a day for 1 week , followed by 30 days or 1–2 weeks off
Side effects are similar to MMC
Interferons
For OSSN: Topical IFN- α2b. 1 million IU/ml as 4 times a day until
resolution, and a month thereafter More expensive than MMC and 5 FU Requires prolonged treatment but
has a better safety profile

RadiotherapyPlaque brachytherapy
Radiation sources like Strontium 90, Rhuthenium 106 or I-125
ComplicationsConjunctival scarring Symblepharon Dry eye Cataract Scleral & Corneal ulceration.

SUMMARY
[1] Suspected OSSN < 3 clock hours
Excision biopsy + base/ edge cryotherapy +alchohol epitheliectomy is done.

[2] Suspected OSSN 3 – 6 clock hours –
A diagnostic biopsy is required
Pre-invasive lesions topical chemotherapy
Invasive lesions surgery + cryotherapy is done after chemoreduction with 4 to 6 cycles of topical chemotherapy.

[3] OSSN > 6 clock hours – A diagnostic biopsy is required. Pre-invasive lesions
Topical chemotherapy Invasive
Surgery + cryotherapy is done after chemoreduction with 4 to 6 cycles of topical chemotherapy.
If there is no response to chemotherapyPalliative radiotherapy or extensive surgery like enucleation / exenteration may be required.

Metastasis
Regional and systemic metastases are also uncommon.
Common sites of metastasis include pre-auricular , submandibular and cervical lymph nodes, parotid gland, lungs, and bone.
Recurrence
Ranges from 15-52%, average 30%
Higher in case of inadequate excision margins
More aggressive behaviour

Conclusion Good clinical exam is sufficient for
diagnosis.
Excision with cryotheraphy is successful but can be associated with recurrence rates
Chemotherapeutic agents are usefull alternative specially in recurrent, corneal & annular lesion.
