of pediatric trauma
TRANSCRIPT
Of Pediatric TraumaOf Pediatric TraumaOf Pediatric Trauma
Mike Schmit, M.D., FACS, FASMBS
Medcenter One
Bismarck, ND
Mike Schmit, M.D., FACS, FASMBS
Medcenter One
Bismarck, ND
The Problem….
� “Trauma is the leading cause of morbidity and mortality in the US pediatric population”
� 20,000 die each year
◦ For every death - 40 hosp, and 1120 treated in ER
� 50,000/yr acquire permanent disabilities
�Most secondary to blunt mech
History
� Peter Kottmeier 1962
� Resources for Optimal Care of the Injured Patient – ACS, 1976
�NPTR, 1985
� 81 accredited Pediatric centers
� Jan 14, 2010 – AAP
◦ www.healthychildren.com

Kids….The differenceKidsKids…….The difference.The difference
� Should not be treated as “little adults”◦ Anxiety, unfamiliar individuals and surroundings
� Respond differently
� Less body fat, smaller body mass, more elastic connective tissue
� Close approximation of internal organs combined with a very pliable skeletal structure
� Should not be treated as “little adults”◦ Anxiety, unfamiliar individuals and surroundings
� Respond differently
� Less body fat, smaller body mass, more elastic connective tissue
� Close approximation of internal organs combined with a very pliable skeletal structure
Kids….The differenceKidsKids…….The difference.The difference
�Hypothermia���� The injured child’s vicious enemy◦ Bair Huggers/ Heat lamps
◦ Trauma Bay ���� >80 - 85 degrees
◦ Fluid warmers…
� Children under 4 yrs of age◦ Increased metabolic rate
◦ O2 demand 2X greater than adults
◦ “Secondary injury”
�Hypothermia���� The injured child’s vicious enemy◦ Bair Huggers/ Heat lamps
◦ Trauma Bay ���� >80 - 85 degrees
◦ Fluid warmers…
� Children under 4 yrs of age◦ Increased metabolic rate
◦ O2 demand 2X greater than adults
◦ “Secondary injury”

Kids….The DifferenceKidsKids…….The Difference.The Difference
� Children are resilient, however…
◦ The period of “meta stability”decreases with age
◦ Some describe the “platinum half-hour”
� Case in point…
◦ If presenting with hypotension, 30% of blood volume has been lost
� Your already way behind…
� Children are resilient, however…
◦ The period of “meta stability”decreases with age
◦ Some describe the “platinum half-hour”
� Case in point…
◦ If presenting with hypotension, 30% of blood volume has been lost
� Your already way behind…

Primary SurveyPrimary SurveyPrimary Survey
� ABCDE’s – Same priorities
� Inadequate ventilation remains the single most common cause of cardio-respiratory arrest in the injured child
◦ Secure airway expediently
◦ Proper equipment ready and functional
◦ Broselow?
� ABCDE’s – Same priorities
� Inadequate ventilation remains the single most common cause of cardio-respiratory arrest in the injured child
◦ Secure airway expediently
◦ Proper equipment ready and functional
◦ Broselow?
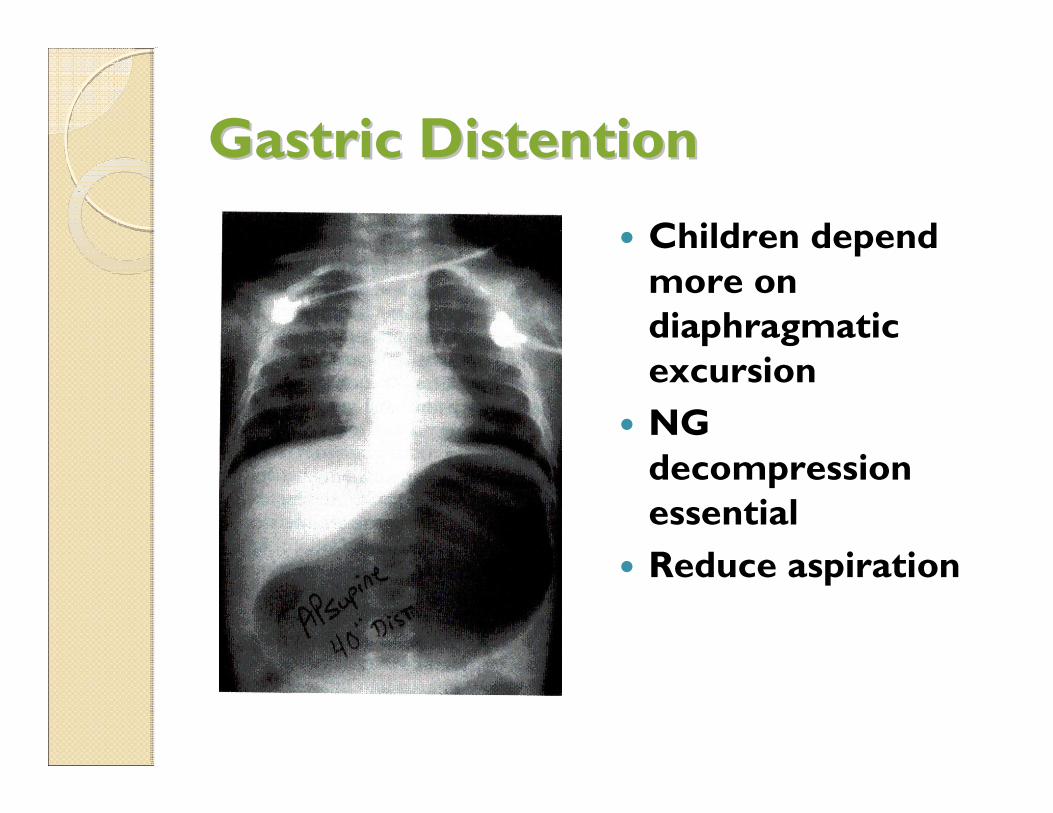
Gastric DistentionGastric Distention
� Children depend more on diaphragmatic excursion
� NG decompression essential
� Reduce aspiration
Intubation - PediatricIntubation Intubation -- PediatricPediatric
� DAI plus…
◦ Atropine (0.1-0.5 mg)
◦ Cardiac output is RATE dependent –The ability to increase stroke volume is very limited
◦ Vagal response, dries secretions
� Placement
◦ ET tip at sternal notch
◦ Depth(CM)=0.5(age) + 12
� DAI plus…
◦ Atropine (0.1-0.5 mg)
◦ Cardiac output is RATE dependent –The ability to increase stroke volume is very limited
◦ Vagal response, dries secretions
� Placement
◦ ET tip at sternal notch
◦ Depth(CM)=0.5(age) + 12

Intubation - PediatricIntubation Intubation -- PediatricPediatric
� Tube size estimation◦ Nail of 5th digit
◦ >2yrs���� (16 + age)/4
�Under 8 years of age, use uncuffedtube◦ Cricoid ring acts as a physiological “cuff”
� Avoid excess cricoid pressure ◦ May cause airway to collapse
� Tube size estimation◦ Nail of 5th digit
◦ >2yrs���� (16 + age)/4
�Under 8 years of age, use uncuffedtube◦ Cricoid ring acts as a physiological “cuff”
� Avoid excess cricoid pressure ◦ May cause airway to collapse

Intubation - PediatricIntubation Intubation -- PediatricPediatric
� Prone to bronchial intubation◦ Infant 4 to 5 cm
◦ Child 7 to 8 cm
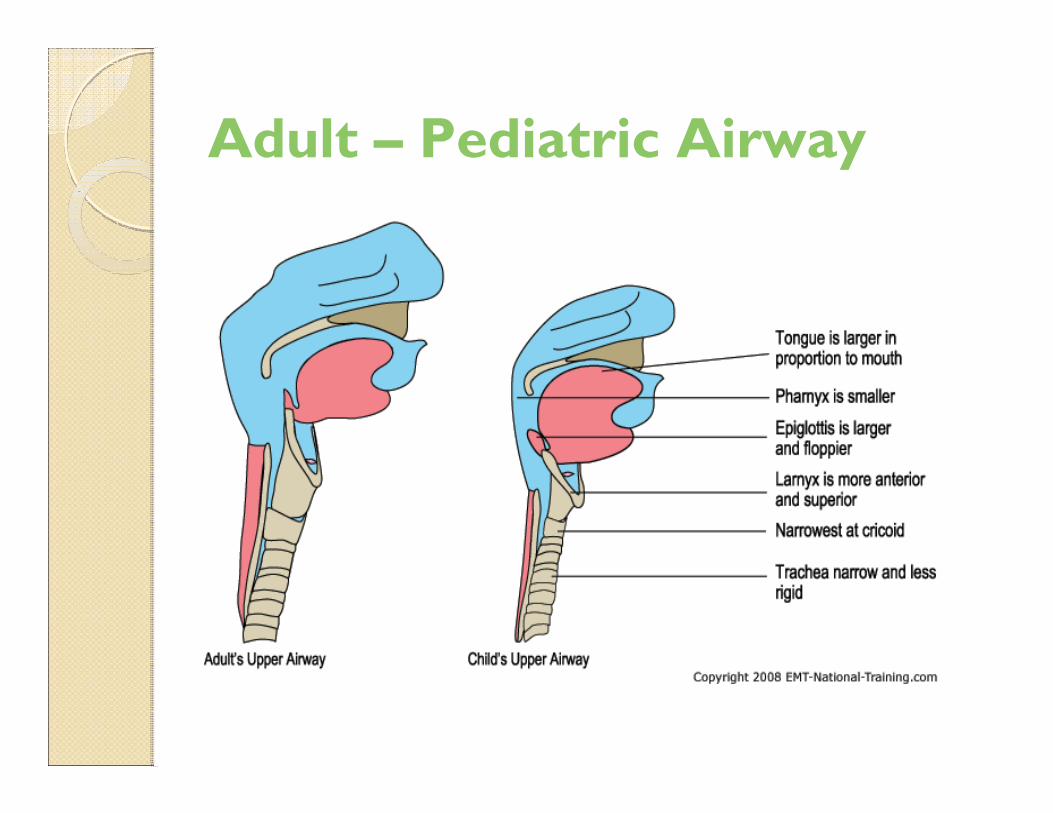
� Narrow airway prone to obstruction◦ Relatively large tongue and debris
◦ Secretions
� Very anterior and superior larynx
� Large epiglottis (“Omega”)
� Smallest diameter at cricoid ring – Not the vocal cords
� Be aware – Dislodged ET tube
� Prone to bronchial intubation◦ Infant 4 to 5 cm
◦ Child 7 to 8 cm
� Narrow airway prone to obstruction◦ Relatively large tongue and debris
◦ Secretions
� Very anterior and superior larynx
� Large epiglottis (“Omega”)
� Smallest diameter at cricoid ring – Not the vocal cords
� Be aware – Dislodged ET tube
Adult – Pediatric Airway

Surgical Pediatric AirwaySurgical Pediatric AirwaySurgical Pediatric Airway
� Needle jet insufflation◦ 12 to 16 gauge needle
◦ Oxygenation, NOT ventilation
◦ Temporary
� Surgical cricothyroidotomy◦ Reserved for >8 yrs
◦ Infants/Children ���� high risk of damage
� Percutaneous◦ Gaining acceptance….
� Needle jet insufflation◦ 12 to 16 gauge needle
◦ Oxygenation, NOT ventilation
◦ Temporary
� Surgical cricothyroidotomy◦ Reserved for >8 yrs
◦ Infants/Children ���� high risk of damage
� Percutaneous◦ Gaining acceptance….

Ventilation - Pediatric
� Remember rates differ
� Bag mask devices – pediatric
◦ Iatrogenic barotrauma
�Hypoxia – Number one cause of cardiac arrest in the child
�High index of suspicion
◦ Mediastinum very mobile
◦ Simple pneumothorax…
� Remember rates differ
� Bag mask devices – pediatric
◦ Iatrogenic barotrauma
�Hypoxia – Number one cause of cardiac arrest in the child
�High index of suspicion
◦ Mediastinum very mobile
◦ Simple pneumothorax…

Venous Access - PediatricVenous Access Venous Access -- PediatricPediatric
� Usually the most difficult procedure◦ Hypotension/hypovolemia
◦ Landmarks obscured
� ATLS suggests two attempts ◦ 90 seconds
� Intraosseous (Children <6yrs)◦ EZ IO
◦ Temporary (4 to 6 hours)
◦ Large volumes safe (100ml/min)
◦ All resuscitative drugs, blood products safe
◦ Never place distal to fractures
� Usually the most difficult procedure◦ Hypotension/hypovolemia
◦ Landmarks obscured
� ATLS suggests two attempts ◦ 90 seconds
� Intraosseous (Children <6yrs)◦ EZ IO
◦ Temporary (4 to 6 hours)
◦ Large volumes safe (100ml/min)
◦ All resuscitative drugs, blood products safe
◦ Never place distal to fractures

Intraosseous PlacementIntraosseousIntraosseous PlacementPlacement
� 2 CM below tibialtuberosity
� 3 CM above femoral condyle
� 4 to 6 hours
◦ Establish venous access
� E-Z IO
� 2 CM below tibialtuberosity
� 3 CM above femoral condyle
� 4 to 6 hours
◦ Establish venous access
� E-Z IO

Venous Access - PediatricVenous Access Venous Access -- PediatricPediatric
� Venous cutdown(Children >6yrs)
◦ Ankle
◦ Groin
◦ Basilic vein
◦ External jugular
� Central approach
� Venous cutdown(Children >6yrs)
◦ Ankle
◦ Groin
◦ Basilic vein
◦ External jugular
� Central approach
Pediatric Injuries: Some DifferencesPediatric Injuries: Pediatric Injuries:
Some DifferencesSome Differences

Intracranial InjuryIntracranial InjuryIntracranial Injury
� CNS – Most commonly injured system
� Common in children <12 months◦ Most vulnerable <3 months
� Early recognition and resuscitation◦ SBP >80mm Hg
◦ Hypotension���� The single most common cause of secondary injury
◦ O2 Saturation >95%
� Implement ICP early (Esp if GCS <8)
� Ventriculostomy���� Immediate response
� CNS – Most commonly injured system
� Common in children <12 months◦ Most vulnerable <3 months
� Early recognition and resuscitation◦ SBP >80mm Hg
◦ Hypotension���� The single most common cause of secondary injury
◦ O2 Saturation >95%
� Implement ICP early (Esp if GCS <8)
� Ventriculostomy���� Immediate response

Intracranial InjuryIntracranial InjuryIntracranial Injury
� Subdural hematomas◦ Common with infants and adolescents
◦ Mortality up to 35 – 40%
� Epidural hematomas◦ Uncommon in children <4 yrs of age
◦ Risks increases with progression through childhood
◦ Mortality 4 – 5%
� Subdural hematomas◦ Common with infants and adolescents
◦ Mortality up to 35 – 40%
� Epidural hematomas◦ Uncommon in children <4 yrs of age
◦ Risks increases with progression through childhood
◦ Mortality 4 – 5%
Intracranial InjuryIntracranial InjuryIntracranial Injury
� Elevated ICP in children◦ >15mm Hg in a child <6yrs
◦ >20mm Hg in a child >6yrs
◦ Both lasting more than 15 minutes
� Critical value of CPP is >50mm Hg
� ICP should be kept <20
�Hyperventelation?◦ Hypocapnic induced vasoconstriction
� Early CT scanning
� Elevated ICP in children◦ >15mm Hg in a child <6yrs
◦ >20mm Hg in a child >6yrs
◦ Both lasting more than 15 minutes
� Critical value of CPP is >50mm Hg
� ICP should be kept <20
�Hyperventelation?◦ Hypocapnic induced vasoconstriction
� Early CT scanning
Intracranial InjuryIntracranial InjuryIntracranial Injury
� Mannitol (0.25 mg/kg) ���� Reduces pressure within 15 minutes◦ May repeat 4 times to osmolarity of 310 to 320 mOsm
� Lasix (1mg/kg) ���� Also decreases CSF � Post traumatic seizures common in children◦ Dilantin (10 mg/kg), Lidocaine (1mg/kg)◦ Give early in resuscitation ���� Neuroprotective
� Avoid seizures and fever!◦ Increased metabolic demand◦ “Secondary injury”
� Mannitol (0.25 mg/kg) ���� Reduces pressure within 15 minutes◦ May repeat 4 times to osmolarity of 310 to 320 mOsm
� Lasix (1mg/kg) ���� Also decreases CSF � Post traumatic seizures common in children◦ Dilantin (10 mg/kg), Lidocaine (1mg/kg)◦ Give early in resuscitation ���� Neuroprotective
� Avoid seizures and fever!◦ Increased metabolic demand◦ “Secondary injury”
Spinal Cord InjurySpinal Cord InjurySpinal Cord Injury
�Uncommon (<2% injured children)
� Vehicular Crashes
�Only 1/3 with cervical bony injuries will have neurologic injury
◦ Only ½ of these have radiographic findings (J Pediatric Surgery 2001)
� Immobilization
�Uncommon (<2% injured children)
� Vehicular Crashes
�Only 1/3 with cervical bony injuries will have neurologic injury
◦ Only ½ of these have radiographic findings (J Pediatric Surgery 2001)
� Immobilization
Clearing ImmobilizationClearing ImmobilizationClearing Immobilization
� Clinical clearance◦ No midline cervical tenderness
◦ No distracting injuries
◦ Alert, no intoxication
◦ No neurological deficits
� Cross table lateral ���� 85% Sensitivity◦ Technique difficult
� CT Scan?
� Re-examination ���� DOCUMENT!!
� Any question…keep immobilized
� Clinical clearance◦ No midline cervical tenderness
◦ No distracting injuries
◦ Alert, no intoxication
◦ No neurological deficits
� Cross table lateral ���� 85% Sensitivity◦ Technique difficult
� CT Scan?
� Re-examination ���� DOCUMENT!!
� Any question…keep immobilized

Spinal Cord InjurySpinal Cord InjurySpinal Cord Injury
� SCIWORA
◦ Present with brief sensory or motor deficits
◦ Progress to severe neurological deficit over next 4 hours (J Neurosurgery 1988)
� Due to extreme ligamentous laxity
◦ Cord (0.5cm), and vertebra (2cm)
◦ Age 0-2 ���� Very flexible (2cm)
◦ Age 2-8 ���� More restricted (1-2cm)
◦ Age >8 ���� Similar to adult distraction
� Pseudosubluxation
� SCIWORA
◦ Present with brief sensory or motor deficits
◦ Progress to severe neurological deficit over next 4 hours (J Neurosurgery 1988)
� Due to extreme ligamentous laxity
◦ Cord (0.5cm), and vertebra (2cm)
◦ Age 0-2 ���� Very flexible (2cm)
◦ Age 2-8 ���� More restricted (1-2cm)
◦ Age >8 ���� Similar to adult distraction
� Pseudosubluxation

SCIWORASCIWORASCIWORA

Thoracic Injuries - PediatricThoracic Injuries Thoracic Injuries -- PediatricPediatric
� Not common – high mortality
� 2ndmost common cause of death
� Pliable rib cage and increased mediastinalmobility
� 85% due to vehicular mechanisms
� 20% will require intubation
◦ Usually to treat CNS injury
◦ Pulmonary contusion
� Most injuries treated same as in adult
� Not common – high mortality
� 2ndmost common cause of death
� Pliable rib cage and increased mediastinalmobility
� 85% due to vehicular mechanisms
� 20% will require intubation
◦ Usually to treat CNS injury
◦ Pulmonary contusion
� Most injuries treated same as in adult
Thoracic Injuries - PediatricThoracic Injuries Thoracic Injuries -- PediatricPediatric
� Main injuries seen in the child include pulmonary contusions and hematomas
� Ribs very pliable◦ Mult fractures ���� Keep in mind intentional abuse
◦ “More than 2 less than 2”
� Traumatic asphyxia and tracheobronchial injury more common than◦ Pneumothorax
◦ Aortic rupture
◦ Flail chest
� Petechiae/Hemorrhage across face, neck, upper chest, conjunctiva◦ Abrupt retrograde high pressure in SVC
� Main injuries seen in the child include pulmonary contusions and hematomas
� Ribs very pliable◦ Mult fractures ���� Keep in mind intentional abuse
◦ “More than 2 less than 2”
� Traumatic asphyxia and tracheobronchial injury more common than◦ Pneumothorax
◦ Aortic rupture
◦ Flail chest
� Petechiae/Hemorrhage across face, neck, upper chest, conjunctiva◦ Abrupt retrograde high pressure in SVC

Thoracic Injuries - PediatricThoracic Injuries Thoracic Injuries -- PediatricPediatric
� Recognition may be elusive
◦ 2/3 of children will present to ED with stable vital signs
� Thoracotomy rare, indications remain:
◦ Massive bleeding
◦ Massive air leak
◦ Cardiac tamponade
◦ Penetrating trauma, no vital signs in ER
� High index of suspicion for other injuries
� Recognition may be elusive
◦ 2/3 of children will present to ED with stable vital signs
� Thoracotomy rare, indications remain:
◦ Massive bleeding
◦ Massive air leak
◦ Cardiac tamponade
◦ Penetrating trauma, no vital signs in ER
� High index of suspicion for other injuries

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Penetrating injuries rare
◦ Involve small intestine usually
◦ Treated with adult protocols
◦ Incidence increasing
� Blunt more common
◦ 90% children with abdominal injuries
◦ Generally liver and spleen
◦ Overall mortality ���� <5%
◦ For abuse/assault victims ���� 12.5%
� Penetrating injuries rare
◦ Involve small intestine usually
◦ Treated with adult protocols
◦ Incidence increasing
� Blunt more common
◦ 90% children with abdominal injuries
◦ Generally liver and spleen
◦ Overall mortality ���� <5%
◦ For abuse/assault victims ���� 12.5%
Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Rib cage small, cannot provide adequate protection
◦ Liver, spleen, kidneys vulnerable
� Pelvis small – Bladder an intra-abdominal organ
�Undeveloped abdominal musculature
� Rib cage small, cannot provide adequate protection
◦ Liver, spleen, kidneys vulnerable
� Pelvis small – Bladder an intra-abdominal organ
�Undeveloped abdominal musculature
Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Diagnosis can be very difficult◦ Distracting injuries
◦ Unfamiliar surroundings
◦ Intense anxiety from separation
� Most injuries treated non-operative◦ Began in 1960’s (Shaftan)
◦ By 1970 (Adhesive SBO after negative Lap)� Mortality 1.6%
� Morbidity 19%
� Re-admission rate 3%
� Diagnosis can be very difficult◦ Distracting injuries
◦ Unfamiliar surroundings
◦ Intense anxiety from separation
� Most injuries treated non-operative◦ Began in 1960’s (Shaftan)
◦ By 1970 (Adhesive SBO after negative Lap)� Mortality 1.6%
� Morbidity 19%
� Re-admission rate 3%

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� OPSS
◦ 1.5% of splenectomized children
◦ 50 fold increase in mortality from septicemia
◦ Greatest in first 2 years after splenectomy
◦ Children <5 yrs of age
� Should receive daily antimicrobial prophylaxis
� Splenic anatomy
◦ Thick fibrous capsule
◦ >95% salvage rate (Pediatric centers)
� OPSS
◦ 1.5% of splenectomized children
◦ 50 fold increase in mortality from septicemia
◦ Greatest in first 2 years after splenectomy
◦ Children <5 yrs of age
� Should receive daily antimicrobial prophylaxis
� Splenic anatomy
◦ Thick fibrous capsule
◦ >95% salvage rate (Pediatric centers)

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Splenic injury observation
◦ 77% grade 1 and 2 injuries will show radiographic resolution in 6 weeks
◦ 8 - 20% for grade 3 to 5
◦ Recommend 4 to 7 day hospital stay
� Repeat CT?
◦ 3 weeks “quiet” activity ���� home
◦ Full activity ���� 3 months post injury
◦ No CT if doing well clinically
◦ Delayed failure?
� First 12 to 24 hours most common
� Splenic injury observation
◦ 77% grade 1 and 2 injuries will show radiographic resolution in 6 weeks
◦ 8 - 20% for grade 3 to 5
◦ Recommend 4 to 7 day hospital stay
� Repeat CT?
◦ 3 weeks “quiet” activity ���� home
◦ Full activity ���� 3 months post injury
◦ No CT if doing well clinically
◦ Delayed failure?
� First 12 to 24 hours most common

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Intervention of spleen injury
◦ Close monitoring/frequent exam
◦ Require transfusion of more than half of their blood volume (40ml/kg) within 24 hours
◦ Hemodynamic stability is the key
� Intervention of spleen injury
◦ Close monitoring/frequent exam
◦ Require transfusion of more than half of their blood volume (40ml/kg) within 24 hours
◦ Hemodynamic stability is the key

Abdominal Injuries - PediatricAbdominal Injuries Abdominal Injuries -- PediatricPediatric
� Concept now applied to liver and renal trauma◦ Portal vein, hepatic veins, and SVC intact
� Pancreas remains controversial◦ Verified ductal injury� Drainage
� Resection (Distal)
� Splenic preservation remains important
� Will tolerate up to 75% distal resection
� Concept now applied to liver and renal trauma◦ Portal vein, hepatic veins, and SVC intact
� Pancreas remains controversial◦ Verified ductal injury� Drainage
� Resection (Distal)
� Splenic preservation remains important
� Will tolerate up to 75% distal resection
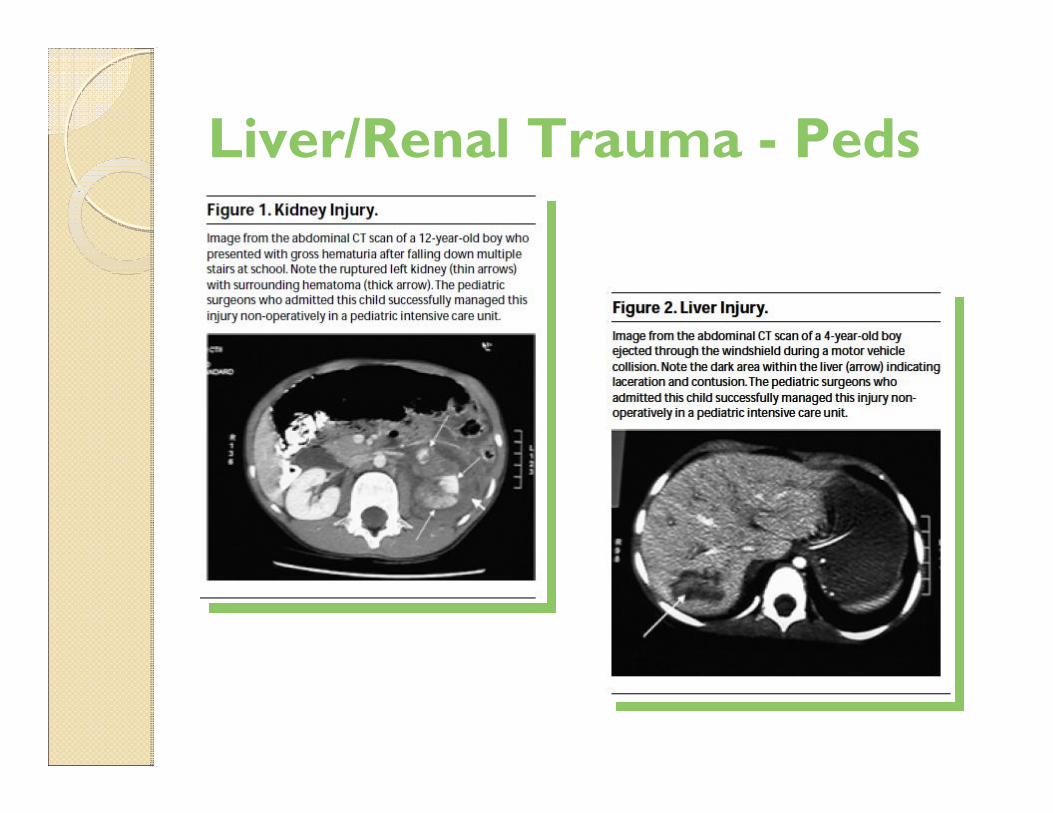
Liver/Renal Trauma - Peds

“Seat-Belt” Sign““SeatSeat--BeltBelt”” SignSign
� Impact usually severe
� Small bowel, stomach, colon, lumbar spine, pancreas, mesentery
� Initial imaging negative
◦ Potential for injury remains high
� Impact usually severe
� Small bowel, stomach, colon, lumbar spine, pancreas, mesentery
� Initial imaging negative
◦ Potential for injury remains high
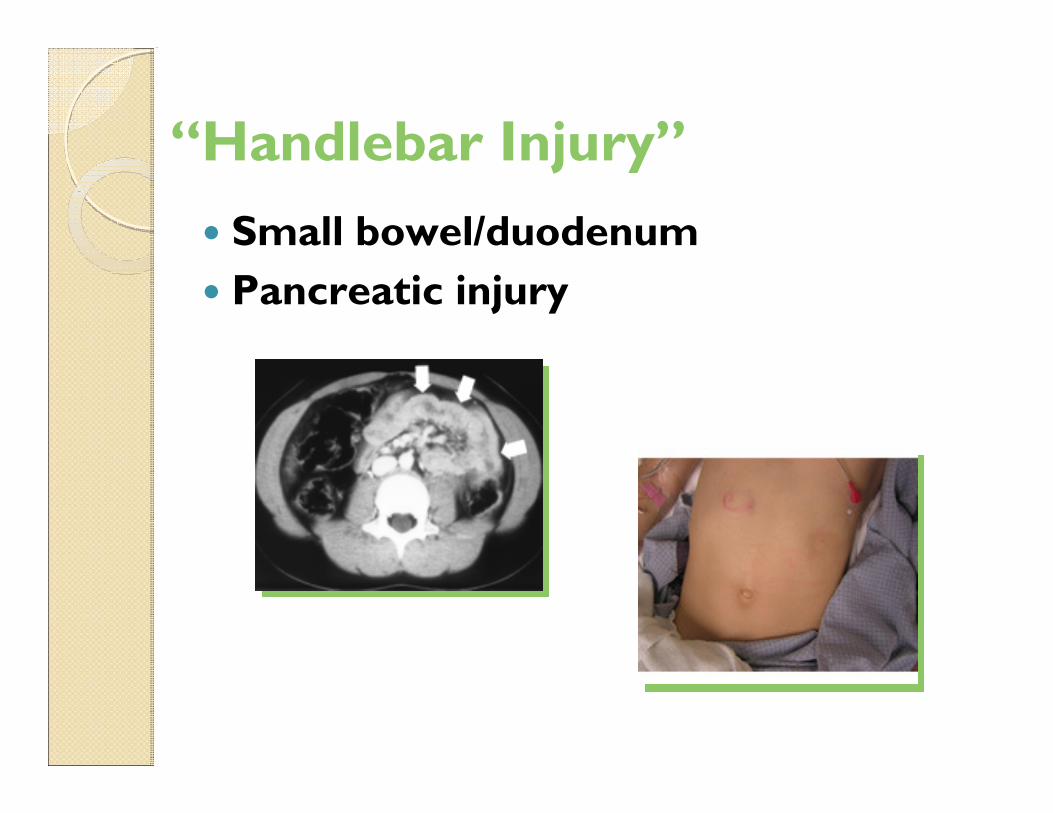
“Handlebar Injury”
� Small bowel/duodenum
� Pancreatic injury

Air BagsAir BagsAir Bags
� Air bag morbidity/mortality
�Mechanisms
◦ Proximity to bag
◦ Can cause SCIWORA
◦ Basilar skull fractures
� Deploy at 150 mph
◦ Second generation
� Air bag morbidity/mortality
�Mechanisms
◦ Proximity to bag
◦ Can cause SCIWORA
◦ Basilar skull fractures
� Deploy at 150 mph
◦ Second generation

SummarySummarySummary
� Head injury remains most significant cause of morbidity and mortality
� Critically injured children must be kept normothermic
� Observational treatment
� Essential to avoid hypovolemicshock
� Avoid “secondary” injury
� Head injury remains most significant cause of morbidity and mortality
� Critically injured children must be kept normothermic
� Observational treatment
� Essential to avoid hypovolemicshock
� Avoid “secondary” injury

SummarySummarySummary
� Care of the injured child is a complex process – which differs from the adult population
� ABCDE’s - ATLS
� High level of suspicion
� Occult injuries
� Intentional abuse
� The single most important take home point remains ���� Prevention
� Care of the injured child is a complex process – which differs from the adult population
� ABCDE’s - ATLS
� High level of suspicion
� Occult injuries
� Intentional abuse
� The single most important take home point remains ���� Prevention