of s has evolved from a high-risk technology with blood flow and...brain temperature, pacop, paoz,...
TRANSCRIPT
REVIEW ARTICLE
Cerebral Blood Flow and Metabolism During Cardiopulmonary Bypass Randall M. Schell, MD, Frank H. Kern, MD, William J. Greeley, MD, Scott R. Schulman, MD, Peter E. Frasco, MD, Narda D. Croughwell, CRNA, Mark Newman, MD, and J.G. Reves, MD
Duke University Medical Center, Department of Anesthesiology, The Heart Center, Durham, North Carolina
ince the 1950s, cardiopulmonary bypass (CPB) has evolved from a high-risk technology with S 50% mortality into a safe and effective procedure
performed routinely at many hospitals throughout the world. Yet despite the successful application of this technology and nearly 40 yr of investigation, the effect of CPB on human physiology remains incompletely understood. Marked changes in systemic flow, tem- perature, perfusion pressure, arterial blood gases, and hematocrit are artificially controlled and regulated by the perfusion team and are never completely normal. Of great concern is the effect these physiologic changes have on the brain.
Recent reports suggest that neuropsychologic dys- function may occur in -20-70% of patients after car- diac surgery with cardiopulmonary bypass and frank stroke in -2-5%. As progress was made in myocardial protection with a decrease in overall mortality rates for cardiac surgery (1 1, morbidity, especially inade- quate brain protection with resultant neuropsycho- logic dysfunction, has become a more prominent con- cern. We recently have reviewed the subject of central nervous system injury after cardiac surgery (2,3), and concluded that although the cause(s) of cerebral injury has not been elucidated fully, further investigations of
Abbreviations: CBF = blood flow; CMR = cerebral metabolic rate; CMR02 = cerebral metabolic rate for oxygen; CPB = cardiopulmonary bypass; CPP = ce- rebral perfusion pressure; CVR = cerebral vascular resistance; ICP = intracranial pressure; MAP = mean arterial pressure; TCA = total circulatory ar- rest.
This work was funded in part by Grant R 0 1 AG9663-01 from the National Institutes of Health and the Hartford Foundation/ American Federation for Aging Research (to R. M. S.).
Accepted for publication September 29, 1992. Address correspondence and reprint requests to Dr. J. G. Reves,
Department of Anesthesiology, Duke University Medical Center, Durham, NC 27710.
the effects of CPB on cerebral blood flow and cerebral metabolism are still needed. This knowledge serves as the scientific basis for the control of physiologic vari- ables during CPB.
CBF/CMR Physiology
The brain is dependent on mitochondria1 aerobic oxi- dation of glucose for energy. Approximately 60% of this energy is utilized to maintain and restore ionic gradi- ents necessary for depolarization and repolarization of neuronal membranes and 40% to maintain cellular in- tegrity (4,5). The brain stores little glucose and contains low concentrations of ATP; therefore, maintenance of an adequate CBF and metabolic substrate is critical. Although the brain comprises only 2% of body weight, its high metabolic rate requires 15% of the cardiac out- put. In the unanesthetized patient, cerebral metabolism (CMR02) is -3.5 mL/100 g/min. Global CBF is -50 mL/100 g/min, 80% of the flow directed to gray matter and 20% to white matter (Table 1) (6). The brain nor- mally extracts approximately 25% of the oxygen sup- plied. CBF and CMR02 are not uniform throughout the brain, as would be predicted from the fluctuating states of cerebral activity. Cerebral blood flow is regulated to supply the metabolic needs of regional areas of the brain. Changes in cerebral metabolism are associated with parallel changes in CBF. This is termed Vlow- metabolism coupling” and is part of the process of ce- rebral autoregulation. Perfusion pressure-flow auto- regulation also exists. This form of autoregulation maintains a constant CBF over a wide range of systemic perfusion pressures (assuming CMR02 remains con- stant). If CBF is independent of the perfusion pressure within the autoregulatory range, then pressure-flow autoregulation is intact. If CBF parallels changes in the MAP (within the normal autoregulatory range), pressure-flow autoregulation is lost. Many physiologic variables influence CBF and /or CMR02 including brain temperature, Pacop, Paoz, blood viscosity, mean arterial pressure outside the autoregulatory range,
01993 by the International Anesthesia Research Society 0003-2999/93/$5.00 Anesth Analg 1993;76849-65 849

850 REVIEW ARTICLE SCHELL ET AL. CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
ANESTH ANALG 1993;76:849-65
Table 1. Cerebral Physiologic Values (5, 6)
CBF (gray matter) -80 mL/100 g/min CBF (white matter) -20 mL/100 g/min Global CBF -50 mL/100 g/min CMRO;! -3.5 mL/100 g/min
JV saturation >60 % JV Po2 >35 mm Hg
CBF/CMR02 - 15-20
JV = jugular venous; CBF = cerebral blood flow; CMROz = cerebral met- abolic rate for oxygen; Poz = partial pressure of oxygen.
intracranial pressure (ICP), and central venous pres- sure (Table 2).
Table 2. Physiologic Variables and Their Effect on Cerebral Blood Flow (CBF)
Variable Effect on CBF
1 paco2 t paco2 1 Paol (< -50 mm Hg) t P ~ O ~ 1 Blood viscosity t MAP (within MAP -50-
150 mm Hg) t ICP t CVP t Cardiac output
1 t T
t) or 1 7 t)
Potentially L Potentially 1
t)
CBF In humans, CBF varies linearly with the Paco2 in the range of ~20-80 mm Hg. Within the range of normal Pacoz values there is an -1 mL/100 g/min change in CBF for each 1 mm Hg parallel change in Paco2 in adults (7). Carbon dioxide is a potent cerebrovasodi- lator.
CBF is not affected by the Pao2 except during un- physiologic Paoz values. Pao2 values less than 50 mm Hg cause cerebrovasodilation, which overrides metab- olism and pressure-flow autoregulation (8). Very high Paoz values slightly increase cerebrovascular resistance and decrease CBF.
CBF increases with decreasing viscosity (hematocrit) (9-11).
C M R Cerebral metabolism decreases exponentially with re- ductions in temperature. On average CMR02 is re- duced -7% for each degree centigrade decrease in body temperature. The multiple by which the rates of cerebral metabolic processes decrease for each 10°C de- crease in temperature (Qlo) for adults during CPB is 2.8 (12). The type and depth of anesthesia also affect the
Cerebral Perfusion Pressure (CPP)
CMR02.
Despite marked changes in MAP and cardiac output, cerebral autoregulation maintains a constant CBF by varying cerebrovascular resistance (CVR). CPP de- pends on MAP and ICP (CPP = MAP - ICP or venous pressure) thus, MAP is the predominant determinant of CPP (5,6).
CBF and Cerebral Ischemia Cerebral ischemia occurs when the CBF is too low to meet the neuronal demand for oxygen and glucose. The degree of CBF reduction and the length of time the brain is without adequate oxygen delivery are the pri- mary determinants of ischemic injury. At normother- mia, thresholds (13) of CBF have been described (Table
~~~
MAP = mean arterial blood pressure; CVP = central venous pressure; ICP = intracranial pressure; Paoz = partial pressure of oxygen in arterial blood; Pacoz = partial pressure of carbon dioxide in arterial blood.
3) where electroencephalogram (EEG) silence, ionic failure, and cell death occur. These thresholds are al- tered dramatically by hypothermia and anesthetics. For example, during moderate hypothermic CPB, CBF may be as low as 10-20 mL/100 g/min (14); however, CMR02 may be only -0.5 mL/100 g/min (12,151. At moderate hypothermia, oxygen demand is reduced significantly and these flows exceed cerebral metabolic demand, as reflected by very narrow arterial venous oxygen gradients.
Pharmacologic Agents and CBF/CMR02 Anesthetics and CBF/CMR02 Anesthetic agents and the depth of anesthesia directly affect CMR02 and CBF. The anesthetic should be stan- dardized when CBF and CMR measurements are ob- tained. We will review briefly the effects of commonly used anesthetics on CBF, CMRO2, and cerebral auto- regulation.
Opioids. During cardiac anesthesia, opioids are rarely administered as the sole anesthetic but rather in combination with a hypnotic and amnestic drug such as midazolam or isoflurane. The effect of narcotic an- esthesia on CBF and/or CMR02 has not been eluci- dated fully and is confounded frequently by other non- opioid anesthetics. Human studies suggest that fentanyl and sufentanil affect a modest reduction in CBF and CMR02 while maintaining cerebral autoreg- ulation (16-18).
In morphine-lorazepam-premedicated subjects re- ceiving an anesthetic induction with 10 pg/kg sufen- tanil, CBF and CMR02 were reduced by 25% and 21%, respectively (16). Similarly, a 25% reduction in CBF was demonstrated with 100 pg/kg fentanyl and 0.4 mg/kg diazepam anesthesia induction (1 7). When low-dose sufentanil (0.5 pg/kg) was administered as a single agent to unpremedicated healthy volunteers, a signif- icant effect on CBF could not be demonstrated (18).
ANESTH ANALG 1993;76049-65
REVIEW ARTICLE SCHELL ET AL. 851 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
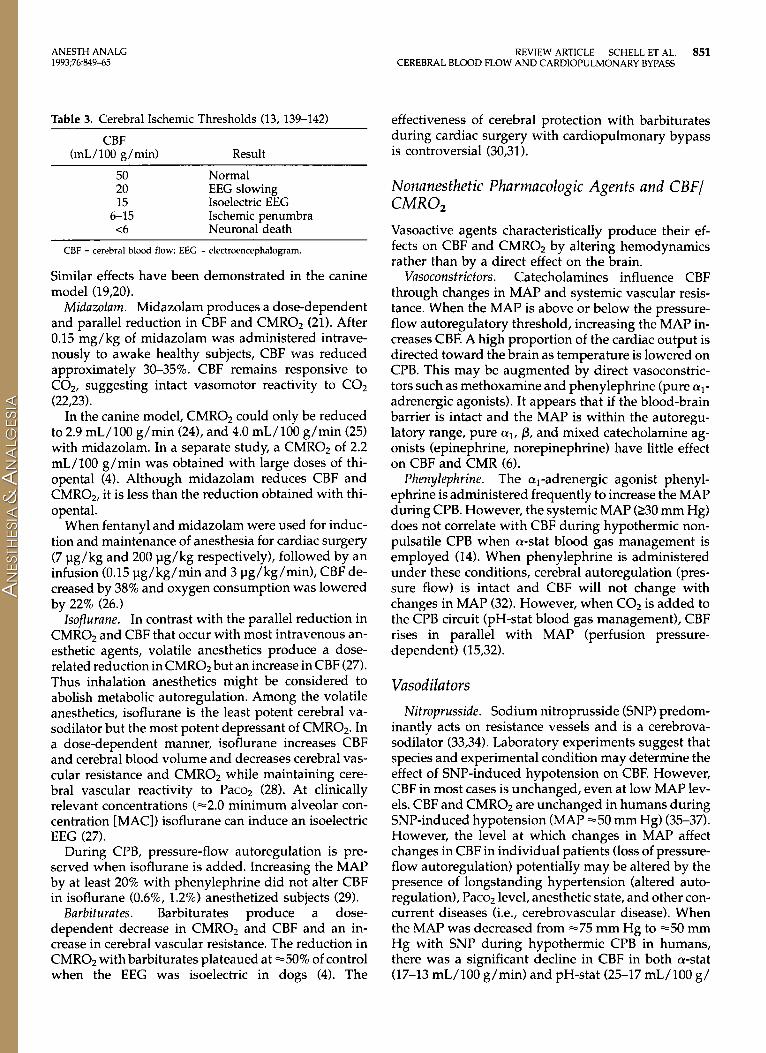
Table 3. Cerebral Ischemic Thresholds (13, 139-142)
CBF (mL/100 g/min) Result
effectiveness of cerebral protection with barbiturates during cardiac surgery with cardiopulmonary bypass is controversial (30,311.
50 Normal 20 EEG slowing 15 Isoelectric EEG
<6 Neuronal death 6-1 5 Ischemic penumbra
CBF = cerebral blood flow; EEG = electroencephalogram.
Similar effects have been demonstrated in the canine model (19,201.
Midazolam. Midazolam produces a dose-dependent and parallel reduction in CBF and CMR02 (21). After 0.15 mg/kg of midazolam was administered intrave- nously to awake healthy subjects, CBF was reduced approximately 30-35%. CBF remains responsive to COP, suggesting intact vasomotor reactivity to C 0 2 (22,23).
In the canine model, CMR02 could only be reduced to 2.9 mL/100 g/min (24), and 4.0 mL/100 g/min (25) with midazolam. In a separate study, a CMR02 of 2.2 mL/100 g/min was obtained with large doses of thi- opental (4). Although midazolam reduces CBF and CMR02, it is less than the reduction obtained with thi- opental.
When fentanyl and midazolam were used for induc- tion and maintenance of anesthesia for cardiac surgery (7 pg/kg and 200 pg/kg respectively), followed by an infusion (0.15 pg/kg/min and 3 pg/kg/min), CBF de- creased by 38% and oxygen consumption was lowered by 22% (26.)
Isoflurane. In contrast with the parallel reduction in CMR02 and CBF that occur with most intravenous an- esthetic agents, volatile anesthetics produce a dose- related reduction in CMR02 but an increase in CBF (27). Thus inhalation anesthetics might be considered to abolish metabolic autoregulation. Among the volatile anesthetics, isoflurane is the least potent cerebral va- sodilator but the most potent depressant of CMR02. In a dose-dependent manner, isoflurane increases CBF and cerebral blood volume and decreases cerebral vas- cular resistance and CMR02 while maintaining cere- bral vascular reactivity to Paco2 (28). At clinically relevant concentrations (=2.0 minimum alveolar con- centration [MAC]) isoflurane can induce an isoelectric EEG (27).
During CPB, pressure-flow autoregulation is pre- served when isoflurane is added. Increasing the MAP by at least 20% with phenylephrine did not alter CBF in isoflurane (0.6%, 1.2%) anesthetized subjects (29).
Barbiturates. Barbiturates produce a dose- dependent decrease in CMR02 and CBF and an in- crease in cerebral vascular resistance. The reduction in CMR02 with barbiturates plateaued at =50% of control when the EEG was isoelectric in dogs (4). The
Nonanesthetic Pharmacologic Agents and CBF/ C M R 0 2 Vasoactive agents characteristically produce their ef- fects on CBF and CMR02 by altering hemodynamics rather than by a direct effect on the brain.
Vasoconstrictors. Catecholamines influence CBF through changes in MAP and systemic vascular resis- tance. When the MAP is above or below the pressure- flow autoregulatory threshold, increasing the MAP in- creases CBF. A high proportion of the cardiac output is directed toward the brain as temperature is lowered on CPB. This may be augmented by direct vasoconstric- tors such as methoxamine and phenylephrine (pure a,- adrenergic agonists). It appears that if the blood-brain barrier is intact and the MAP is within the autoregu- latory range, pure al, p, and mixed catecholamine ag- onists (epinephrine, norepinephrine) have little effect on CBF and CMR (6).
Phenylephrine. The al-adrenergic agonist phenyl- ephrine is administered frequently to increase the MAP during CPB. However, the systemic MAP (230 mm Hg) does not correlate with CBF during hypothermic non- pulsatile CPB when a-stat blood gas management is employed (14). When phenylephrine is administered under these conditions, cerebral autoregulation (pres- sure flow) is intact and CBF will not change with changes in MAP (32). However, when C02 is added to the CPB circuit (pH-stat blood gas management), CBF rises in parallel with MAP (perfusion pressure- dependent) (1 5,32).
Vasodilators Nitroprusside. Sodium nitroprusside (SNP) predom-
inantly acts on resistance vessels and is a cerebrova- sodilator (33,34). Laboratory experiments suggest that species and experimental condition may determine the effect of SNP-induced hypotension on CBF. However, CBF in most cases is unchanged, even at low MAP lev- els. CBF and CMR02 are unchanged in humans during SNP-induced hypotension (MAP -50 mm Hg) (35-37). However, the level at which changes in MAP affect changes in CBF in individual patients (loss of pressure- flow autoregulation) potentially may be altered by the presence of longstanding hypertension (altered auto- regulation), Paco2 level, anesthetic state, and other con- current diseases (i.e., cerebrovascular disease). When the MAP was decreased from =75 mm Hg to =50 mm Hg with SNP during hypothermic CPB in humans, there was a significant decline in CBF in both a-stat (17-13 mL/l00 g/min) and pH-stat (25-17 mL/100 g/
852 REVIEW ARTICLE SCHELL ET AL. CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
ANESTH ANALG 1993;76:849-65
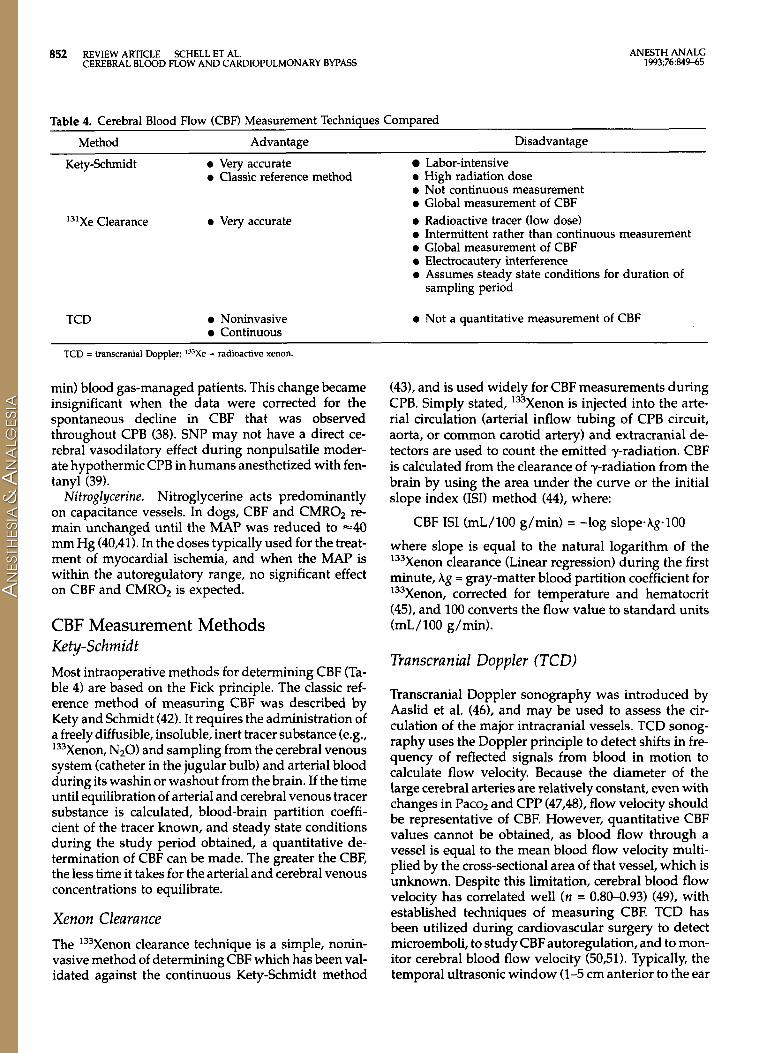
Table 4. Cerebral Blood Flow (CBF) Measurement Techniques Compared Method Advantage Disadvantage
Kety-Schmid t 0 Very accurate Labor-intensive 0 Classic reference method 0 High radiation dose
131Xe Clearance 0 Very accurate
TCD 0 Noninvasive 0 Continuous
0 Not continuous measurement 0 Global measurement of CBF 0 Radioactive tracer (low dose) 0 Intermittent rather than continuous measurement 0 Global measurement of CBF 0 Electrocautery interference 0 Assumes steady state conditions for duration of
sampling period
0 Not a quantitative measurement of CBF
TCD = transcranial Doppler; 133Xe = radioactive xenon.
min) blood gas-managed patients. This change became insignificant when the data were corrected for the spontaneous decline in CBF that was observed throughout CPB (38). SNP may not have a direct ce- rebral vasodilatory effect during nonpulsatile moder- ate hypothermic CPB in humans anesthetized with fen- tanyl (39).
Nitroglycerine. Nitroglycerine acts predominantly on capacitance vessels. In dogs, CBF and CMROz re- main unchanged until the MAP was reduced to -40 mm Hg (40,411. In the doses typically used for the treat- ment of myocardial ischemia, and when the MAP is within the autoregulatory range, no significant effect on CBF and CMROZ is expected.
CBF Measurement Methods Kety-Schrn id t Most intraoperative methods for determining CBF (Ta- ble 4) are based on the Fick principle. The classic ref- erence method of measuring CBF was described by Kety and Schmidt (42). It requires the administration of a freely diffusible, insoluble, inert tracer substance (e.g., '33Xenon, NzO) and sampling from the cerebral venous system (catheter in the jugular bulb) and arterial blood during its washin or washout from the brain. If the time until equilibration of arterial and cerebral venous tracer substance is calculated, blood-brain partition coeffi- cient of the tracer known, and steady state conditions during the study period obtained, a quantitative de- termination of CBF can be made. The greater the CBF, the less time it takes for the arterial and cerebral venous concentrations to equilibrate.
Xenon Clearance The '33Xenon clearance technique is a simple, nonin- vasive method of determining CBF which has been val- idated against the continuous Kety-Schmidt method
(43), and is used widely for CBF measurements during CPB. Simply stated, '33Xenon is injected into the arte- rial circulation (arterial inflow tubing of CPB circuit, aorta, or common carotid artery) and extracranial de- tectors are used to count the emitted y-radiation. CBF is calculated from the clearance of y-radiation from the brain by using the area under the curve or the initial slope index (ISI) method (44), where:
CBF IS1 (mL/100 g/min) = -log slope-Ag.100
where slope is equal to the natural logarithm of the '33Xenon clearance (Linear regression) during the first minute, Ag = gray-matter blood partition coefficient for '33Xenon, corrected for temperature and hematocrit (451, and 100 converts the flow value to standard units (mL/100 g/min).
Transcranial Doppler (TCD)
Transcranial Doppler sonography was introduced by Aaslid et al. (46), and may be used to assess the cir- culation of the major intracranial vessels. TCD sonog- raphy uses the Doppler principle to detect shifts in fre- quency of reflected signals from blood in motion to calculate flow velocity. Because the diameter of the large cerebral arteries are relatively constant, even with changes in Pacoz and CPP (47,48), flow velocity should be representative of CBF. However, quantitative CBF values cannot be obtained, as blood flow through a vessel is equal to the mean blood flow velocity multi- plied by the cross-sectional area of that vessel, which is unknown. Despite this limitation, cerebral blood flow velocity has correlated well ( n = 0.80-0.93) (49), with established techniques of measuring CBF. TCD has been utilized during cardiovascular surgery to detect microemboli, to study CBF autoregulation, and to mon- itor cerebral blood flow velocity (50,51). Typically, the temporal ultrasonic window (1-5 cm anterior to the ear
ANESTH ANALG 1993;76:849-65
REVIEW ARTICLE SCHELL ET AL. 853 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
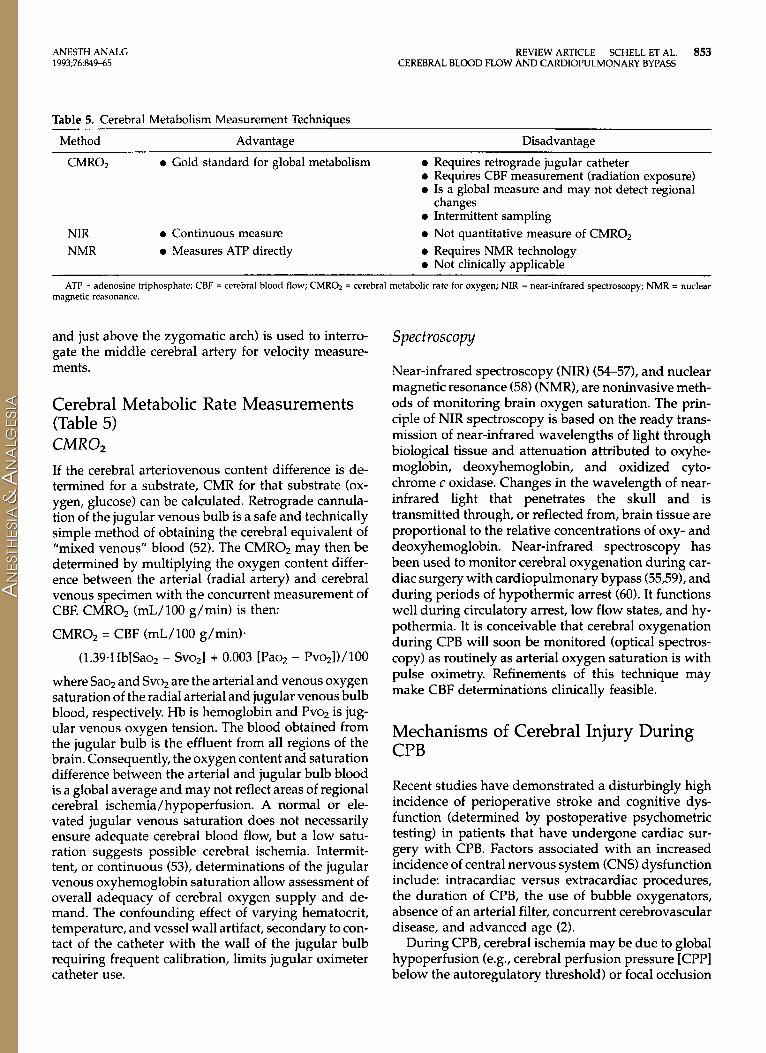
Table 5. Cerebral Metabolism Measurement Techniques Method Advantage Disadvantage
CMR02 0 Gold standard for global metabolism 0 Requires retrograde jugular catheter 0 Requires CBF measurement (radiation exposure) 0 Is a global measure and may not detect regional
0 Intermittent sampling changes
NIR 0 Continuous measure 0 Not quantitative measure of CMROz NMR 0 Measures ATP directly 0 Requires NMR technology
0 Not clinically applicable ATP = adenosine triphosphate; CBF = cerebral blood flow; CMROz = cerebral metabolic rate for oxygen; NIR = near-infrared spectroscopy; NMR = nuclear
magnetic reasonance.
and just above the zygomatic arch) is used to interro- gate the middle cerebral artery for velocity measure- ments.
Cerebral Metabolic Rate Measurements (Table 5) CMR02 If the cerebral arteriovenous content difference is de- termined for a substrate, CMR for that substrate (ox- ygen, glucose) can be calculated. Retrograde cannula- tion of the jugular venous bulb is a safe and technically simple method of obtaining the cerebral equivalent of "mixed venous" blood (52). The CMROz may then be determined by multiplying the oxygen content differ- ence between the arterial (radial artery) and cerebral venous specimen with the concurrent measurement of CBF. CMROZ (mL/100 g/min) is then:
CMR02 = CBF (mL/100 g/min).
(1.39.Hb[Saoz - Svozl + 0.003 [Paoz - Pvozl)/lOO
where Saoz and Svoz are the arterial and venous oxygen saturation of the radial arterial and jugular venous bulb blood, respectively. Hb is hemoglobin and Pvoz is jug- ular venous oxygen tension. The blood obtained from the jugular bulb is the effluent from all regions of the brain. Consequently, the oxygen content and saturation difference between the arterial and jugular bulb blood is a global average and may not reflect areas of regional cerebral ischemia/hypoperfusion. A normal or ele- vated jugular venous saturation does not necessarily ensure adequate cerebral blood flow, but a low satu- ration suggests possible cerebral ischemia. Intermit- tent, or continuous (531, determinations of the jugular venous oxyhemoglobin saturation allow assessment of overall adequacy of cerebral oxygen supply and de- mand. The confounding effect of varying hematocrit, temperature, and vessel wall artifact, secondary to con- tact of the catheter with the wall of the jugular bulb requiring frequent calibration, limits jugular oximeter catheter use.
Spectroscopy
Near-infrared spectroscopy (NIR) (54-571, and nuclear magnetic resonance (58) (NMR), are noninvasive meth- ods of monitoring brain oxygen saturation. The prin- ciple of NIR spectroscopy is based on the ready trans- mission of near-infrared wavelengths of light through biological tissue and attenuation attributed to oxyhe- moglobin, deoxyhemoglobin, and oxidized cyto- chrome c oxidase. Changes in the wavelength of near- infrared light that penetrates the skull and is transmitted through, or reflected from, brain tissue are proportional to the relative concentrations of oxy- and deoxyhemoglobin. Near-infrared spectroscopy has been used to monitor cerebral oxygenation during car- diac surgery with cardiopulmonary bypass (55,59), and during periods of hypothermic arrest (60). It functions well during circulatory arrest, low flow states, and hy- pothermia. It is conceivable that cerebral oxygenation during CPB will soon be monitored (optical spectros- copy) as routinely as arterial oxygen saturation is with pulse oximetry. Refinements of this technique may make CBF determinations clinically feasible.
Mechanisms of Cerebral Injury During CPB
Recent studies have demonstrated a disturbingly high incidence of perioperative stroke and cognitive dys- function (determined by postoperative psychometric testing) in patients that have undergone cardiac sur- gery with CPB. Factors associated with an increased incidence of central nervous system (CNS) dysfunction include: intracardiac versus extracardiac procedures, the duration of CPB, the use of bubble oxygenators, absence of an arterial filter, concurrent cerebrovascular disease, and advanced age (2).
During CPB, cerebral ischemia may be due to global hypoperfusion (e.g., cerebral perfusion pressure [CPPI below the autoregulatory threshold) or focal occlusion

854 REVIEW ARTICLE SCHELL ET AL. CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
ANESTH ANALG 1993;76649-65
Table 6. Perioperative Factors Adversely Effecting Normal Cerebral Autoregulation
1. Hypertension 2. Insulin-dependent diabetes 3. Cerebrovascular disease 4. Temperature (deep hypothermia) 5. pH-stat blood gas management 6. Extremes of age (?)
of the cerebral vasculature due to emboli. Focal ische- mia appears to produce the preponderance of neuro- logic events that occur during cardiac surgery. Micro- emboli can be found in all patients (arterial-line blood) undergoing CPB (61,62). These microemboli have been detected by middle cerebral artery transcranial doppler and retinal angiographic techniques (51,63). The ana- tomical correlate of the neurologic deficits resulting from microemboli after cardiac surgery may be focal dilatations or very small aneurysms in terminal arte- rioles and capillaries of the cerebral circulation (64). The use of membrane oxygenators (65-671, arterial fil- ters (68), and more complete heparinization (69) have been suggested as means for decreasing the incidence of microembolic phenomenon but do not eliminate them. Microembolization remains an identifiable cause of cerebral dysfunction. Debris from the surgical field and embolization of ventricular air likely account for the incidence of neurologic injury following open car- diac procedures.
Echocardiography is one technology which may be used to reduce the risk of microemboli. Echocardio- graphy can predict an aortic cannulation site free from atherosclerotic plaques and identify residual intracar- diac air which may be evacuated before aortic cross- clamp removal, thereby decreasing the risk of signifi- cant cerebral emboli (70,711.
Global hypoperfusion may likewise be a mechanism for cerebral injury following cardiac surgery. CPB is associated with periods of low systemic flow and re- duced perfusion pressure, reduced hemoglobin levels resulting in decreased oxygen content, altered cerebral autoregulation, and changing cerebral metabolic de- mands (temperature). These factors may affect the re- lationship of CBF and CMR02. Reductions in the CBF/ CMR02 ratio may place the brain at greater risk for cerebral hypoperfusion. Maintaining an appropriate flow-metabolism ratio presumably is essential to re- ducing neuropsychologic morbidity following CPB.
Preoperative Clinical Conditions The preoperative identification of one or more of the following clinical conditions may uniquely affect CBF and CMR during CPB and require alterations in the routine clinical management of the patient (see also Table 6).
Hypertension Cerebral blood flow remains constant in normal hu- mans between a cerebral perfusion pressure of approx- imately 50-150 mm Hg. Over this range, alterations in CPP are accompanied by compensatory changes in ce- rebral vascular resistance to normalize CBF. Uncon- trolled hypertension however, leads to a shift of this autoregulatory curve to the right (72). This is most likely due to structural thickening and luminal narrow- ing of cerebral resistance vessels (73). Although pressure-flow autoregulation is not lost, CBF becomes pressure-dependent at both extremes of the autoregu- latory curve. Long-term antihypertensive therapy, es- pecially in young patients, may reverse this autoreg- ulatory adaptation to hypertension (74). Pressure-flow autoregulation may return toward normal after several weeks in treated hypertensive patients (5). Whether these changes are reversible in the elderly, chronically hypertensive patient is unknown (75).
The lower limit of the autoregulatory threshold in individual hypertensive patients will vary; therefore, a higher perfusion pressure on CPB may be required to assure adequate cerebral perfusion.
Insulin-dependen t Diabetes Insulin-dependent diabetic patients placed on cardio- pulmonary bypass have evidence of impaired metabolism-flow autoregulation (76).
In an investigation of 23 patients, it was demon- strated that diabetic patients do not increase CBF like nondiabetic patients when the perfusate temperature is increased (76). To compensate for failure to deliver more oxygen at normothermia, more oxygen was ex- tracted from the blood (decreased jugular venous sat- uration). Greater extraction of oxygen is a normal com- pensatory mechanism to assure adequate O2 delivery when metabolism-flow autoregulation fails to main- tain CBF.
Aging Age appears to be a major risk factor contributing to a negative neurologic outcome after cardiac surgery (1,2,77,78). Although aging is associated with reduc- tions in both CMR02 and CBF (79,801, the response of the cerebral circulation to changes in arterial pressure and Paco2 appear to be intact (81-83). In a study of the effect of age on CBF and cerebral blood flow autoreg- ulation during cardiopulmonary bypass, age did not appear to interfere with pressure-flow autoregulation (80). The sample size was small (n = 20) and the results of the investigation are considered preliminary.
The mechanism(s) of increased neurologic risk with aging is unknown but may involve increased micro- emboli, cerebrovascular disease, and / or aberrations in
ANESTH ANALG 1993;76:849-65
REVIEW ARTICLE SCHELL ET AL. 855 CEREBRAL BLOOD FLOW A N D CARDIOPULMONARY BYPASS
Table 7. Effect of Hypothermia on the Cerebral Metabolic Rate for Oxygen (CMR02) and Cerebral Blood Flow (CBF) During Cardiopulmonary Bypass (CPB)
Temperature CMR02 (Mean) CBF (Mean) ("C) (mL/100 g/min) (mL/100 g/min)
Awake/normal (5,6) 37 -3.5 -50 Murkin (15) =35 (pre-bypass) 1.67 25
Govier (14) 34.5 * 1.1 (pre-bypass) 20.4 f 6.5 13.3 f 6.5 9.1 f 2.4
Croughwell (12) 37 * 0.7 1.4 f 0.34 35 * 9.0 27 f 2.0 0.5 2 0.2 21 * 6.8
26 0.42 14-15
28 ? 3.6 26.1 & 1.7
Values are mean or mean * SD when available
cerebral autoregulation with incomplete global ische- mia.
Cerebrovascular Disease In most clinical series, prior cerebrovascular event or transient ischemic attack is associated with an in- creased risk of neurologic morbidity following CPB. The effect of bilateral carotid artery disease on CBF dur- ing CPB has been investigated. In a study of CBF dur- ing CPB (moderate hypothermia and MAP > 50 mm Hg) in 24 patients with cerebrovascular disease, seven with severe bilateral carotid artery disease, no differ- ence in CBF was observed between the study and con- trol group. CBF measured in the group with bilateral carotid artery disease was similar in each hemisphere and was normal (84). The effect of bilateral 80% carotid obstruction in a 66-yr-old patient undergoing cardiac surgery was investigated, and marked reductions in perfusion pressure were not accompanied by abnor- mally low global cerebral blood flow measurements using '33Xenon clearance (85). Although global CBF re- mained intact in these studies, the presence of extra- and intracranial obstructive vascular disease in cardiac surgery patients, and its impact on care, await further investigation and the development of better techniques to assess regional CBF and metabolism during cardio- pulmonary bypass.
Factors During Cardiopulmonary Bypass That Affect CBF/CMR02 Temperature The brain temperature is an important determinant of cerebral blood flow during CPB. CBF and CMR02 are markedly reduced by hypothermia (Table 7).
When the major external factors manipulated during cardiopulmonary perfusion are evaluated (cerebral perfusion pressure, pump flow, Paco2 and tempera- ture), temperature is the single most important element influencing CBF during CPB (14,86,87).
CMR02. Hypothermia is characteristically utilized for brain protection during CPB because it reduces ce- rebral metabolism -7%/"C and prolongs the brain's tolerance for ischemia. The CMR may be divided into a component associated with electrophysiologic func- tion (60%) and another for maintenance of cellular in- tegrity (40%) (4,88). Hypothermia is unique, as it pro- portionally decreases the rate of energy use associated with both of these components of CMR. The relation- ship of temperature to CMR02 in man can be computed and is expressed as the Qlo, or the multiple by which the rate of global metabolism decreases for each 10°C reduction in body temperature. In adult patients un- dergoing cardiac surgery (12), the median Qlo was 2.8 and a mathematical expression of the effect of temper- ature on CMR02 was expressed as:
CMR02 = 0.021 e0.1147 X TNp
where TNP is the nasopharyngeal temperature in "C. In infants and children undergoing congenital heart sur- gery (87), the Qlo was 3.6 and the mathematical ex- pression of the relationship:
CMR02 = 0.019 e0.1171 X TNP
These relationships of temperature to oxidative metab- olism can be used to compute the duration of cerebral protection afforded by hypothermia (i.e., circulatory ar- rest), assuming that the sole protective effect of hypo- thermia is related to a change in CMR02 (87-90).
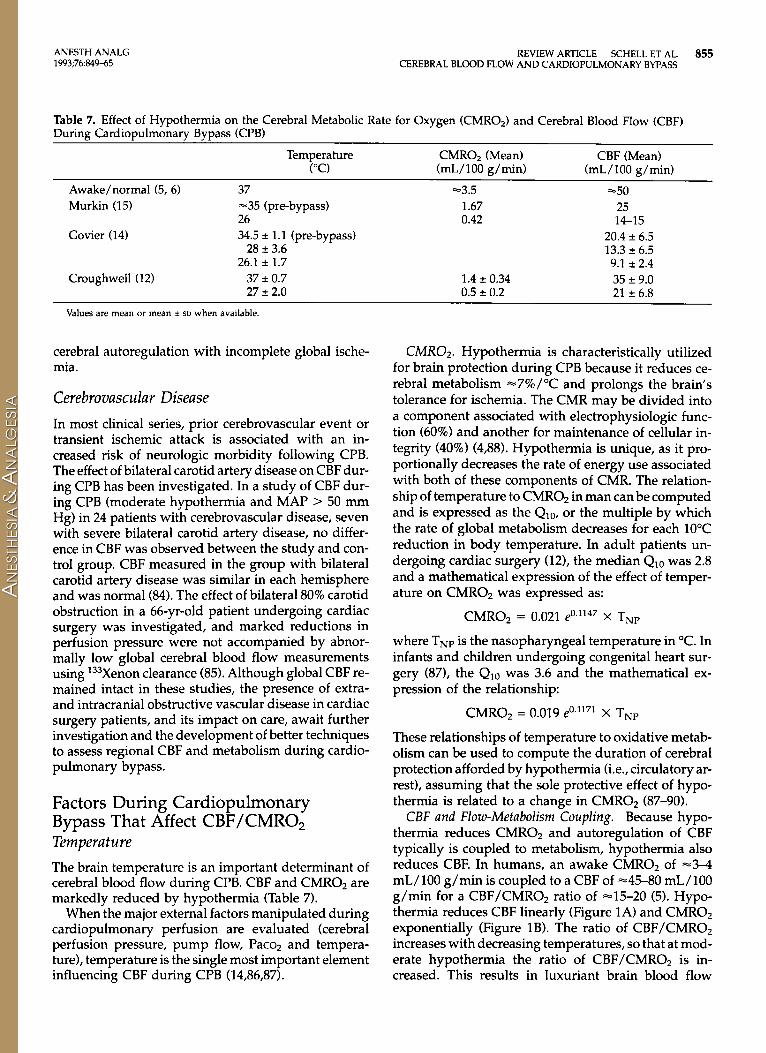
CBF and Flow-Metabolism Coupling. Because hypo- thermia reduces CMR02 and autoregulation of CBF typically is coupled to metabolism, hypothermia also reduces CBF. In humans, an awake CMR02 of -3-4 mL/100 g/min is coupled to a CBF of -45-80 mL/100 g/min for a CBF/CMR02 ratio of ~1.5-20 (5). Hypo- thermia reduces CBF linearly (Figure 1A) and CMR02 exponentially (Figure 1B). The ratio of CBF/CMR02 increases with decreasing temperatures, so that at mod- erate hypothermia the ratio of CBF/CMR02 is in- creased. This results in luxuriant brain blood flow
856 REVIEW ARTICLE SCHELL ET AL. ANESTH ANALG 1993;76:84945 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
A 100
60
.. .
40 U ' 10 20
Ternperatu?e "C
3 1 B
.*a 2 I . I
CMROZ .i/
Figure 1. A, plot demonstrating the linear relationship of cerebral blood flow (mL/100 g/min [CBF]) and temperature ("C) during cardiopulmonary bypass. (Adapted and reprinted with permission [lOSl) 8, plot demonstrating the exponential relationship of the ce- rebral metabolic rate for oxygen (mL/100 g/min [CMROJ) and temperature ("C) during cardiopulmonary bypass. (Adapted and reprinted with permission 1871.) CBF = cerebral blood flow; CMROz = cerebral metabolic rate for oxygen.
02/87]. With mild-moderate degrees of hypothermia, pressure-flow autoregulation is intact (14,15).
Deep Hypotherrnia. Deep hypothermic temperatures of 15-20°C increase the ratio of CBF/CMR02 and result in a loss of pressure-flow autoregulation. Severe tem- perature reductions impair cerebral vascular relaxation (911, which has been described as a cold-induced va- soparesis (92). The loss of vascular relaxation results in a disruption of pressure-flow autoregulation such that changes in CPP will result in corresponding directional changes in CBF.
Hypothermia confers protection with global ische- mia, allowing prolonged periods of circulatory arrest without neurologic dysfunction. However, hypother- rnia is not always present at those periods of highest risk for embolization during CPB (i.e., aortic cross- clamp and removal, aortic cannulation), and the pro- tective effect in focal cerebral ischemia remains unclear (93). Despite its widespread use during myocardial re- vascularization, a study comparing the effects of dif- fering levels of hypothermia on neurologic outcome has yet to be performed. The benefits of moderate hy- pothermia for cerebral protection during cardiac sur- gery are unproven.
Systemic Flow The systemic flow rate during CPB customarily is based on body surface area, degree of hypothermia, and adequacy of organ perfusion as determined by whole body oxygen consumption, arterial blood gases,
and acid-base balance (14,94,95). Although pump flow rates in adults characteristically range between =1.6- 2.4 L/min/m2 (=40-70 mL/kg/min) no standard flow rate is optimal for cerebral perfusion under all clinical conditions.
In the unanesthetized and normothermic state, the brain receives -15% of the cardiac output. During steady state hypothermic CPB, mean cerebral blood flow was -600 mL/min at a CPB flow of 2.4 L/min/ m2. Cerebral oxygen consumption remained constant to a flow of 1.6 L/min/m2 at which point the cerebral flow fell to -400 mL/min (96). Using Qlo data from adults during hypothermic CPB (12, a reduction in pump flow rate down to 0.6 L/min/m2 should sustain cerebral metabolic demands at a temperature of 27°C.
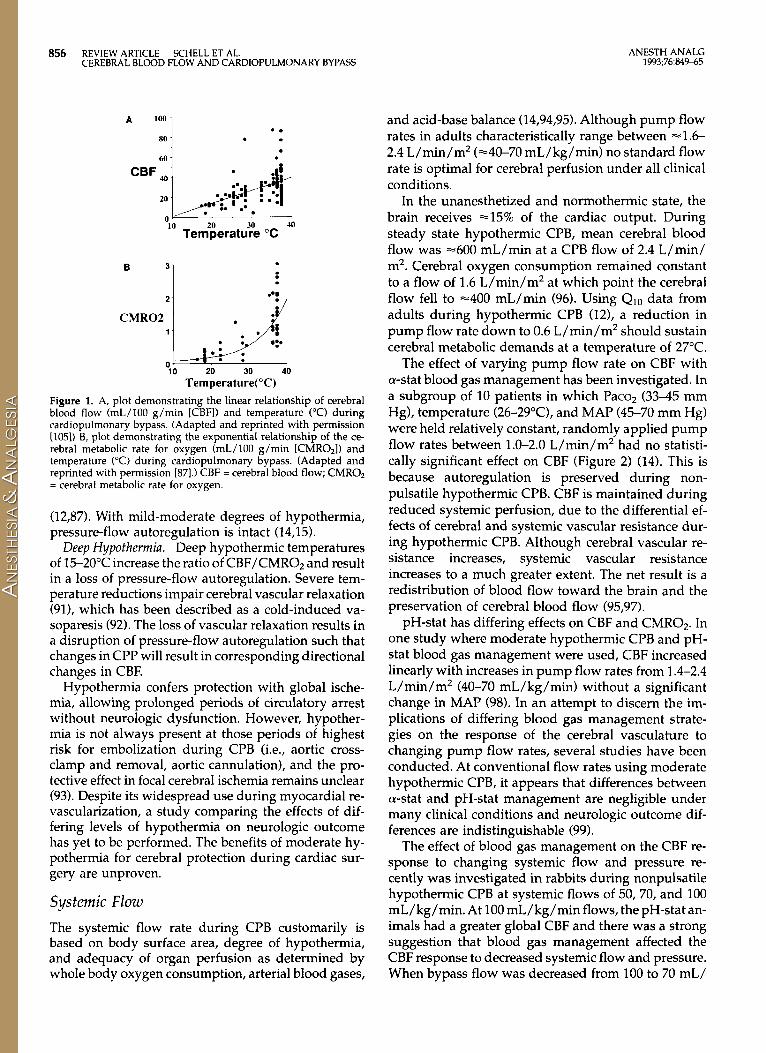
The effect of varying pump flow rate on CBF with a-stat blood gas management has been investigated. In a subgroup of 10 patients in which Paco2 (33-45 mm Hg), temperature (26-29"C), and MAP (45-70 mm Hg) were held relatively constant, randomly applied pump flow rates between 1.0-2.0 L/min/m2 had no statisti- cally significant effect on CBF (Figure 2) (14). This is because autoregulation is preserved during non- pulsatile hypothermic CPB. CBF is maintained during reduced systemic perfusion, due to the differential ef- fects of cerebral and systemic vascular resistance dur- ing hypothermic CPB. Although cerebral vascular re- sistance increases, systemic vascular resistance increases to a much greater extent. The net result is a redistribution of blood flow toward the brain and the preservation of cerebral blood flow (95,97).
pH-stat has differing effects on CBF and CMR02. In one study where moderate hypothermic CPB and pH- stat blood gas management were used, CBF increased linearly with increases in pump flow rates from 1.4-2.4 L/min/m2 (40-70 mL/kg/min) without a significant change in MAP (98). In an attempt to discern the im- plications of differing blood gas management strate- gies on the response of the cerebral vasculature to changing pump flow rates, several studies have been conducted. At conventional flow rates using moderate hypothermic CPB, it appears that differences between a-stat and pH-stat management are negligible under many clinical conditions and neurologic outcome dif- ferences are indistinguishable (99).
The effect of blood gas management on the CBF re- sponse to changing systemic flow and pressure re- cently was investigated in rabbits during nonpulsatile hypothermic CPB at systemic flows of 50, 70, and 100 mL/kg/min. At 100 mL/kg/min flows, the pH-stat an- imals had a greater global CBF and there was a strong suggestion that blood gas management affected the CBF response to decreased systemic flow and pressure. When bypass flow was decreased from 100 to 70 mL/
ANESTH ANALG 1993;76:849-65
Figure 2. No significant relationship is demon- strated between pump flow during cardiopulmon- ary bypass and cerebral blood flow. There are 44 hidden observations, that is, data points superim- posed on each other. (Reprinted with permission 1141.)
'"
1 f '" ; loo
g 75 0
L O
1 5 -- 0 --
REVIEW ARTICLE SCHELL ET AL. 857 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
--
. -- -. -- -L-----
' * r.15 * p..11
-- . I 1
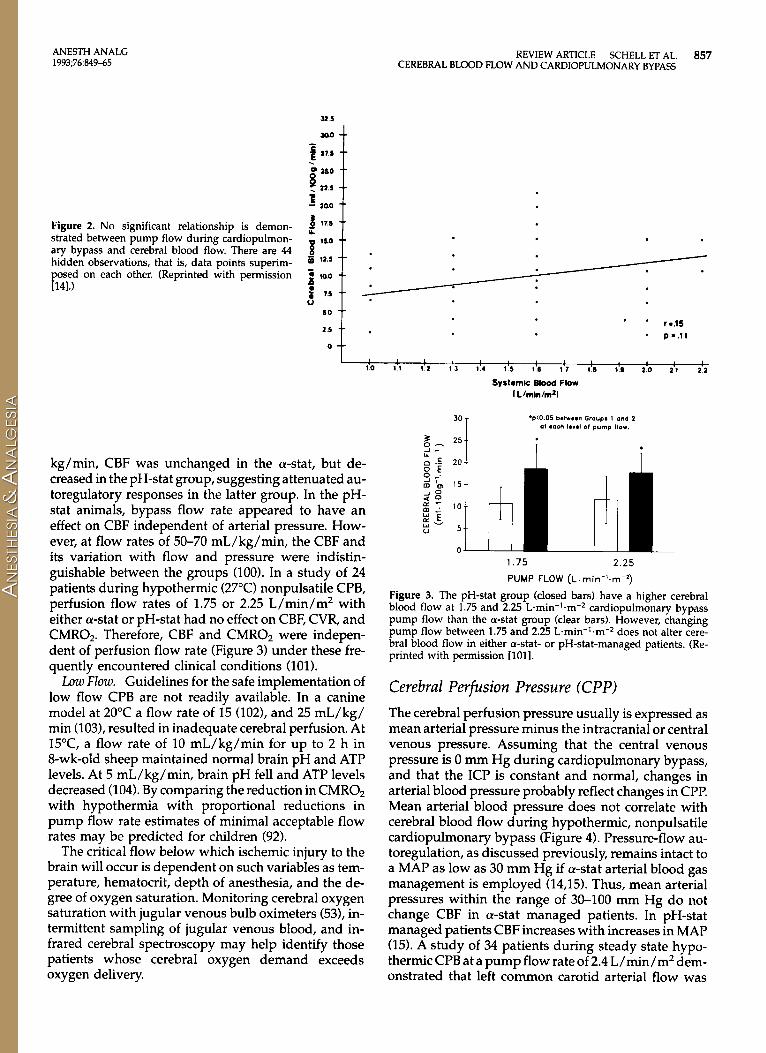
kg/min, CBF was unchanged in the a-stat, but de- creased in the pH-stat group, suggesting attenuated au- toregulatory responses in the latter group. In the pH- stat animals, bypass flow rate appeared to have an effect on CBF independent of arterial pressure. How- ever, at flow rates of 50-70 mL/kg/min, the CBF and its variation with flow and pressure were indistin- guishable between the groups (100). In a study of 24 patients during hypothermic (27°C) nonpulsatile CPB, perfusion flow rates of 1.75 or 2.25 L/min/m2 with either a-stat or pH-stat had no effect on CBF, CVR, and CMR02. Therefore, CBF and CMR02 were indepen- dent of perfusion flow rate (Figure 3) under these fre- quently encountered clinical conditions (101).
Low Flow. Guidelines for the safe implementation of low flow CPB are not readily available. In a canine model at 20°C a flow rate of 15 (102), and 25 mL/kg/ min (103), resulted in inadequate cerebral perfusion. At 15T, a flow rate of 10 mL/kg/min for up to 2 h in 8-wk-old sheep maintained normal brain pH and ATP levels. At 5 mL/kg/min, brain pH fell and ATP levels decreased (104). By comparing the reduction in CMR02 with hypothermia with proportional reductions in pump flow rate estimates of minimal acceptable flow rates may be predicted for children (92).
The critical flow below which ischemic injury to the brain will occur is dependent on such variables as tem- perature, hematocrit, depth of anesthesia, and the de- gree of oxygen saturation. Monitoring cerebral oxygen saturation with jugular venous bulb oximeters (53), in- termittent sampling of jugular venous blood, and in- frared cerebral spectroscopy may help identify those patients whose cerebral oxygen demand exceeds oxygen delivery.
1.75 2.25 PUMP FLOW (L.rnin-'.m-l)
Figure 3. The pH-stat group (closed bars) have a higher cerebral blood flow at 1.75 and 2.25 L.min-'.m-2 cardiopulmonary bypass pump flow than the a-stat group (clear bars). However, changing pump flow between 1.75 and 2.25 L.min-'.m-2 does not alter cere- bral blood flow in either a-stat- or pH-stat-managed patients. (Re- printed with permission [loll.
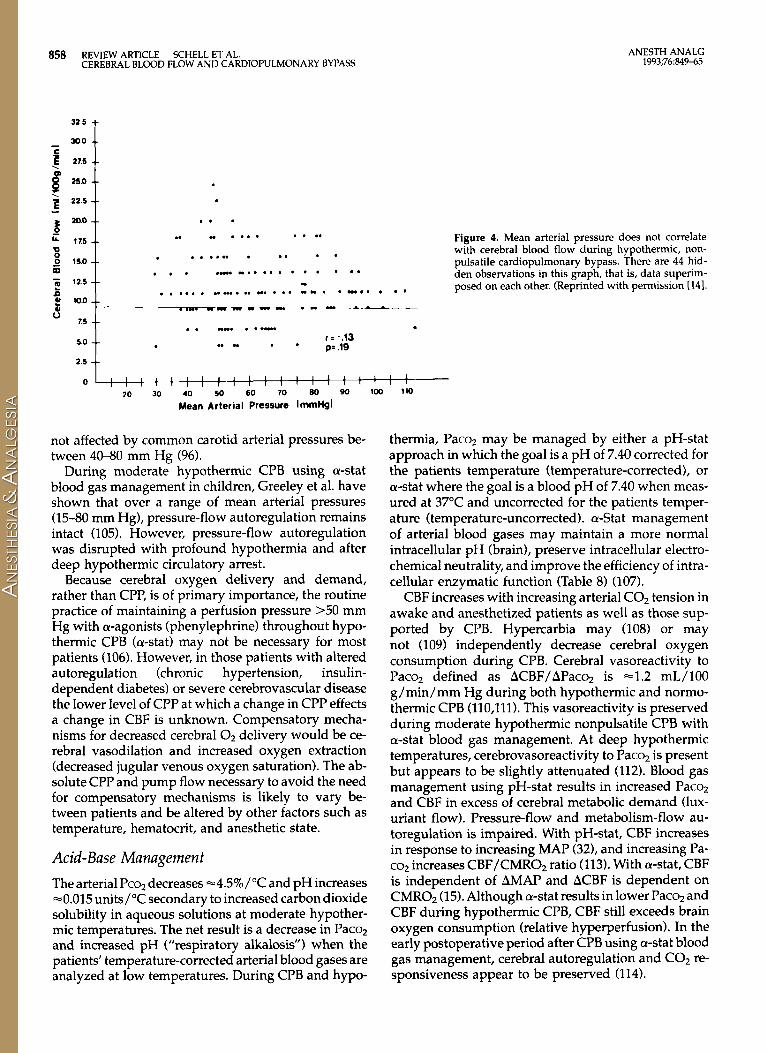
Cerebral Perfusion Pressure (CPP) The cerebral perfusion pressure usually is expressed as mean arterial pressure minus the intracranial or central venous pressure. Assuming that the central venous pressure is 0 mm Hg during cardiopulmonary bypass, and that the ICP is constant and normal, changes in arterial blood pressure probably reflect changes in CPP. Mean arterial blood pressure does not correlate with cerebral blood flow during hypothermic, nonpulsatile cardiopulmonary bypass (Figure 4). Pressure-flow au- toregulation, as discussed previously, remains intact to a MAP as low as 30 mm Hg if a-stat arterial blood gas management is employed (14,151. Thus, mean arterial pressures within the range of 30-100 mm Hg do not change CBF in a-stat managed patients. In pH-stat managed patients CBF increases with increases in MAP (15). A study of 34 patients during steady state hypo- thermic CPB at a pump flow rate of 2.4 L/min/m2 dem- onstrated that left common carotid arterial flow was
858 REVIEW ARTICLE SHELL ET AL. CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
ANESTH ANALG 1993;76:849-65
. . . " .... .... Figure 4. Mean arterial pressure does not correlate .. . .n . .. . . with cerebral blood flow during hypothermic, non-
pulsatile cardiopulmonary bypass. There are 44 hid- den observations in this graph, that is, data superim- posed on each other. (Reprinted with permission [141.
.. . . . . . . . . . . . . .-. w . .
w ...... .. ... . . . . ...... ... " " . -.. ". c.l-..-- 1 - - -*.--_ ~. lo*)
mew. ..- r.5 * * * .. . . r = -.13 p= .19 .. w . .
2.5
not affected by common carotid arterial pressures be- tween 40-80 mm Hg (96).
During moderate hypothermic CPB using a-stat blood gas management in children, Greeley et al. have shown that over a range of mean arterial pressures (15-80 mm Hg), pressure-flow autoregulation remains intact (105). However, pressure-flow autoregulation was disrupted with profound hypothermia and after deep hypothermic circulatory arrest.
Because cerebral oxygen delivery and demand, rather than CPP, is of primary importance, the routine practice of maintaining a perfusion pressure >50 mm Hg with a-agonists (phenylephrine) throughout hypo- thermic CPB (a-stat) may not be necessary for most patients (106). However, in those patients with altered autoregulation (chronic hypertension, insulin- dependent diabetes) or severe cerebrovascular disease the lower level of CPP at which a change in CPP effects a change in CBF is unknown. Compensatory mecha- nisms for decreased cerebral O2 delivery would be ce- rebral vasodilation and increased oxygen extraction (decreased jugular venous oxygen saturation). The ab- solute CPP and pump flow necessary to avoid the need for compensatory mechanisms is likely to vary be- tween patients and be altered by other factors such as temperature, hematocrit, and anesthetic state.
Acid-Base Management The arterial Pcoz decreases -4.5%/"C and pH increases -0.015 units/"C secondary to increased carbon dioxide solubility in aqueous solutions at moderate hypother- mic temperatures. The net result is a decrease in Pacoz and increased pH ("respiratory alkalosis") when the patients' temperature-corrected arterial blood gases are analyzed at low temperatures. During CPB and hypo-
thermia, Paco2 may be managed by either a pH-stat approach in which the goal is a pH of 7.40 corrected for the patients temperature (temperature-corrected), or a-stat where the goal is a blood pH of 7.40 when meas- ured at 37°C and uncorrected for the patients temper- ature (temperature-uncorrected). a-Stat management of arterial blood gases may maintain a more normal intracellular pH (brain), preserve intracellular electro- chemical neutrality, and improve the efficiency of intra- cellular enzymatic function (Table 8) (107).
CBF increases with increasing arterial C02 tension in awake and anesthetized patients as well as those sup- ported by CPB. Hypercarbia may (108) or may not (109) independently decrease cerebral oxygen consumption during CPB. Cerebral vasoreactivity to Paco2 defined as ACBF/APacq is -1.2 mL/100 g/min/mm Hg during both hypothermic and normo- thermic CPB (110,111). This vasoreactivity is preserved during moderate hypothermic nonpulsatile CPB with a-stat blood gas management. At deep hypothermic temperatures, cerebrovasoreactivity to Paco2 is present but appears to be slightly attenuated (112). Blood gas management using pH-stat results in increased Pacoz and CBF in excess of cerebral metabolic demand (lux- uriant flow). Pressure-flow and metabolism-flow au- toregulation is impaired. With pH-stat, CBF increases in response to increasing MAP (321, and increasing Pa- co2 increases CBF/CMR02 ratio (113). With a-stat, CBF is independent of AMAP and ACBF is dependent on CMROZ (15). Although a-stat results in lower Paco2 and CBF during hypothermic CPB, CBF still exceeds brain oxygen consumption (relative hyperperfusion). In the early postoperative period after CPB using a-stat blood gas management, cerebral autoregulation and CO2 re- sponsiveness appear to be preserved (114).
ANESTH ANALG 1993;76:84945
REVIEW ARTICLE SCHELL ET AL. 859 CEREBRAL BLOOD FL.OW AND CARDIOPULMONARY BYPASS
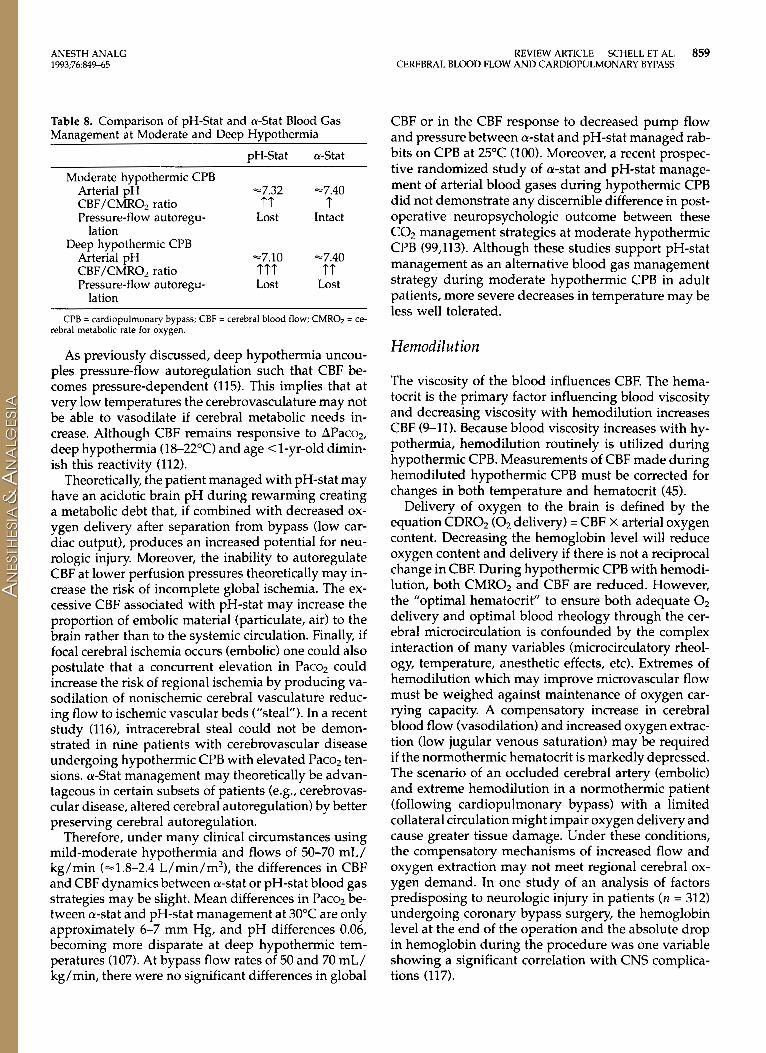
Table 8. Comparison of pH-Stat and a-Stat Blood Gas Management at Moderate and Deep Hypothermia
pH-Stat a-Stat
Arterial pH -7.32 -7.40
Pressure-flow autoregu- Lost Intact
Moderate hypothermic CPB
CBF/CMR02 ratio tt t lation
Deep hypothermic CPB Arterial pH -7.10 =7.40 CBF/CMR02 ratio ttt tt Pressure-flow autoregu- Lost Lost
lation CPB = cardiopulmonary bypass; CBF = cerebral blood flow; CMROz = ce-
rebral metabolic rate for oxygen.
As previously discussed, deep hypothermia uncou- ples pressure-flow autoregulation such that CBF be- comes pressure-dependent (115). This implies that at very low temperatures the cerebrovasculature may not be able to vasodilate if cerebral metabolic needs in- crease. Although CBF remains responsive to APaco2, deep hypothermia (18-22°C) and age <I-yr-old dimin- ish this reactivity (112).
Theoretically, the patient managed with pH-stat may have an acidotic brain pH during rewarming creating a metabolic debt that, if combined with decreased ox- ygen delivery after separation from bypass (low car- diac output), produces an increased potential for neu- rologic injury. Moreover, the inability to autoregulate CBF at lower perfusion pressures theoretically may in- crease the risk of incomplete global ischemia. The ex- cessive CBF associated with pH-stat may increase the proportion of embolic material (particulate, air) to the brain rather than to the systemic circulation. Finally, if focal cerebral ischemia occurs (embolic) one could also postulate that a concurrent elevation in Paco2 could increase the risk of regional ischemia by producing va- sodilation of nonischemic cerebral vasculature reduc- ing flow to ischemic vascular beds (“steal”). In a recent study (116), intracerebral steal could not be demon- strated in nine patients with cerebrovascular disease undergoing hypothermic CPB with elevated Pacoz ten- sions. a-Stat management may theoretically be advan- tageous in certain subsets of patients (e.g., cerebrovas- cular disease, altered cerebral autoregulation) by better preserving cerebral autoregulation.
Therefore, under many clinical circumstances using mild-moderate hypothermia and flows of 50-70 mL/ kg/min (=1.8-2.4 L/min/m2), the differences in CBF and CBF dynamics between a-stat or pH-stat blood gas strategies may be slight. Mean differences in Paco2 be- tween a-stat and pH-stat management at 30°C are only approximately 6-7 mm Hg, and pH differences 0.06, becoming more disparate at deep hypothermic tem- peratures (107). At bypass flow rates of 50 and 70 mL/ kg/min, there were no significant differences in global
CBF or in the CBF response to decreased pump flow and pressure between a-stat and pH-stat managed rab- bits on CPB at 25°C (100). Moreover, a recent prospec- tive randomized study of a-stat and pH-stat manage- ment of arterial blood gases during hypothermic CPB did not demonstrate any discernible difference in post- operative neuropsychologic outcome between these COz management strategies at moderate hypothermic CPB (99,113). Although these studies support pH-stat management as an alternative blood gas management strategy during moderate hypothermic CPB in adult patients, more severe decreases in temperature may be less well tolerated.
Hemod ilu tion
The viscosity of the blood influences CBF. The hema- tocrit is the primary factor influencing blood viscosity and decreasing viscosity with hemodilution increases CBF (9-11). Because blood viscosity increases with hy- pothermia, hemodilution routinely is utilized during hypothermic CPB. Measurements of CBF made during hemodiluted hypothermic CPB must be corrected for changes in both temperature and hematocrit (45).
Delivery of oxygen to the brain is defined by the equation CDR02 (0, delivery) = CBF X arterial oxygen content. Decreasing the hemoglobin level will reduce oxygen content and delivery if there is not a reciprocal change in CBF. During hypothermic CPB with hemodi- lution, both CMR02 and CBF are reduced. However, the “optimal hematocrit” to ensure both adequate O2 delivery and optimal blood rheology through the cer- ebral microcirculation is confounded by the complex interaction of many variables (microcirculatory rheol- ogy, temperature, anesthetic effects, etc). Extremes of hemodilution which may improve microvascular flow must be weighed against maintenance of oxygen car- rying capacity. A compensatory increase in cerebral blood flow (vasodilation) and increased oxygen extrac- tion (low jugular venous saturation) may be required if the normothermic hematocrit is markedly depressed. The scenario of an occluded cerebral artery (embolic) and extreme hemodilution in a normothermic patient (following cardiopulmonary bypass) with a limited collateral circulation might impair oxygen delivery and cause greater tissue damage. Under these conditions, the compensatory mechanisms of increased flow and oxygen extraction may not meet regional cerebral ox- ygen demand. In one study of an analysis of factors predisposing to neurologic injury in patients ( n = 312) undergoing coronary bypass surgery, the hemoglobin level at the end of the operation and the absolute drop in hemoglobin during the procedure was one variable showing a significant correlation with CNS complica- tions (117).
860 REVIEW ARTICLE SCHELL ET AL. ANESTH ANALG 1993;76849-65 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
Pulsatile Versus Nonpulsatile Perfusion The institution of nonpulsatile bypass may reduce CBF and CMR02 independently (118). The relative contri- bution of nonpulsatile cerebral perfusion during CPB to CNS injury is unknown, and the debate over the merits of pulsatile perfusion continues. However, ev- idence for microvasculature dysfunction with nonpul- satile perfusion can be found in many studies. In a study using normothermic pulsatile CPB, capillary flow in the microvasculature of the omentum was maintained, whereas with nonpulsatile perfusion, flow slowed and virtually ceased. At flow rates of 60 and 75 mL/kg/min pulsatile perfusion resulted in a higher pH, reduced base deficit, and improved total body ox- ygen consumption compared with nonpulsatile perfu- sion (11 9). Cerebral capillary collapse, intravascular sludging in the conjunctiva and cerebral circulation, and neuropathologic changes in arterial boundary zones (120), have been demonstrated in dogs under- going nonpulsatile perfusion and eliminated in dogs perfused with pulsatile flow.
Nonpulsatile perfusion may unfavorably alter cere- bral microcirculatory flow, whereas pulsatile flow may minimize the cerebral microcirculatory shunt during CPB. Astudy of 23 patients undergoing CPB with either pulsatile or nonpulsatile perfusion demonstrated a lower CVR in the pulsed patients. Although there was no difference in CMR02 between the groups during and just after CPB, the cerebral arterial venous oxygen difference of the pulsatile group was greater. This sug- gests that pulsatile flow may attenuate the microcir- culatory shunt that occurs with CPB (121). Although these differences are small, pulsatile perfusion may provide better perfusion at marginal pump flow rates such as low flow hypothermic CPB. Improvements in brain pH, Pco2, and Po2 have been demonstrated in a canine model when nonpulsatile perfusion was com- pared with pulsatile perfusion at a flow rate of 25 mL/ kg / min (103,122).
At lower flow rates, and with longer perfusion pe- riods, pulsatile assistance may be more beneficial (122). However, the effect of pulsatile perfusion on CMR02 and CBF under frequently encountered clinical condi- tions is likely far outweighed by other perfusion vari- ables (i.e., temperature, Paco2).
Time on Cardiopulmonary Bypass It has been suggested that CPB is associated with ce- rebral microvascular obstruction from accumulated microemboli and /or progressive cerebral vasoconstric- tion. A decline in CBF with time on CPB was first sug- gested in 1988 (32). In adult patients undergoing hy- pothermic (28°C) CPB, CBF was determined after the aorta was cross-clamped and body temperature stabi- lized for at least 5 min. A repeat CBF determination was
made after 20-30 min and a decline in CBF of -1 % /min was observed. In this study, nasopharyngeal temper- ature remained constant. However, as the CBF deter- minations were made shortly after aortic cross-clamp brain temperature (not reflected in NPT) and CMR02 may have declined concomitantly. However, the ob- served time-dependent reduction in CBF was not ac- companied by a concomitant decline in CMR02, sug- gesting that the ability of CBF to meet metabolic demand decreases with time on CPB (123). Using mul- tivariate statistical methods, time on CPB had no effect on CPB in another study (14).
A recent canine study from the same investigative group did not support the clinical observation. CBF was measured with radioactive microspheres for a longer study period (270 min vs -30 min) in a nor- mothermic ( n = 10) and hypothermic (28°C) ( n = 11) group during stable CPB. At 90,150, and 210 min, CBF did not decline during stable hypothermia. In normo- thermic animals, CBF remained constant with only an insignificant decrease overall (124). During low-flow (0.5 L/min/m2) hypothermic (18OC) CPB, CBF also did not change with time (125). If a time-dependent decline in CBF occurred when the systemic flows (low flow CPB) are only 25% of full-flow CPB, the risk of inad- equate cerebral perfusion with time on CPB would be increased,
Longer cooling periods may be required for brain temperature equilibration and stable reproducible con- ditions for CBF determinations (100,109). In a rabbit CPB model using microsphere methodology for CBF determinations, CBF and CMR02 did not change be- tween 30 and 90 min of CPB at normothermia and be- tween 60 and 90 min in hypothermic (27°C) animals. However, 41 2 6 min were required for cortical tem- perature equilibration (109).
Although time has been suggested as an etiology for a decrease in CBF, this may reflect the inability of su- perficial temperature monitoring to adequately reflect true brain temperature. We do not believe that duration of CPB, per se is associated with a reduction in CBF because CBF returns to control levels with re- warming (14,15,105). The role that the duration of CPB plays on the intraoperative CBF/CMR02 meas- urements and etiology of postoperative neuropsycho- logic deficits after cardiac surgery awaits further in- vestigation.
Glucose Management
Although the absolute glucose level may not directly affect CBF and CMR02 during CPB, elevated glucose levels at the time of neuronal ischemia may increase cerebral injury. When the cellular demand for oxygen
ANESTH ANALG 1993;76849-65
REVIEW ARTICLE SCHELL ET AL. 861 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
exceeds supply, anaerobic glycolytic conversion of glu- cose to lactate occurs, producing an increased intra- cellular hydrogen ion and lactate concentration. With
hyperglycemia and the period of neurologic risk is un- known.
complete cerebral ischemia (e.g., TCA), the intracellu- lar lactate concentration is proportional to the cerebral Rewarming/After CPB stores of glucose at the time i f the insult. The intra- cellular cerebral stores, as well as the continued deliv- ery of glucose to anaerobically metabolizing brain, may make lactate concentrations greater with incomplete global ischemia (126,127). Inefficient production, as well as rapid depletion of ATP, occurs with anaerobic glycolysis. Increased intracellular acidosis enhances neuronal cell injury. Experimental models of global is- chemia consistently have demonstrated glucose- induced enhancement of ischemic injury (128). How- ever, the association between glucose levels and neurologic injury after focal ischemia has been incon- sistent (128).
Because cardiac surgery with CPB is associated with inhibition of insulin secretion and hyperglycemia (129,1301, and a concurrent risk of global and/or focal cerebral ischemia, maintaining euglycemia is recom- mended. Although maintenance of euglycemia during CPB seems a simple and beneficial goal, there is little evidence that neurologic outcome is worse with hy- perglycemia during CPB and/or TCA. A study of 60 patients undergoing moderate hypothermic, nonpul- satile CPB found no effect of relative hyperglycemia (221 2 58 mg/dL, mean 2 SD) on postoperative neu- ropsychologic performance. However, the range of blood glucose levels was relatively narrow 103-379 mg/dL (131). Recently glucose-containing pump prim- ing solutions (D5LR, 20 mL/kg) were compared with a nonglucose-containing prime. Although measured se- rum glucose levels were three to four times higher with the glucose prime, no increase in gross neurologic in- jury could be demonstrated (132). The lack of formal- ized neuropsychologic testing, however, limits these results. A recent retrospective study evaluated the role of hyperglycemia in 34 children undergoing deep hy- pothermic circulatory arrest. The hyperglycemic pa- tients trended toward a worse neurologic outcome, although this did not reach statistical significance (133).
Insulin-dependent diabetics lose the normal cou- pling of cerebral blood flow and metabolism during hypothermic CPB. Due to the inability to increase CBF like nondiabetics, oxygen extraction increases when the perfusate temperature is increased (76). These patients may be at increased risk for cerebral ischemia during low-flow or low-pressure CPB.
The critical level of hyperglycemia at which insulin therapy should be initiated is unknown. Because there is a normal hysteresis between brain and systemic glu- cose levels after insulin therapy, the time that should be allowed between treatment of a patient with
Following moderate hypothermic continuous CPB, CMR02 and CBF return to or exceed prebypass levels in nondiabetic adults (15,96,134,135). Adult patients with diabetes, however, lose cerebral flow-metabolism autoregulation. They fail to increase CBF to meet met- abolic needs during the rewarming period of CPB (76).
Warming from moderate hypothermic CPB has been associated with jugular venous desaturation &Sat < 50%) as detected by intermittent jugular bulb sampling (136), and with continuous oximeter catheters in the jugular bulb (53). JvSat reflects the balance of cerebral oxygen supply and demand. Increased oxygen extrac- tion, and therefore, lower JvSat would be the compen- satory response when oxygen demand is increased more than oxygen supply. Although Jv desaturation (JvSat < 50%) recently was identified in 25% of patients at normothermia following hypothermic CPB, it was not associated with impaired postoperative neuropsy- chologic test performance (136,137).
Cerebral autoregulation and C02 responsiveness are preserved after CPB (138). The CBF response to changes in arterial Pacoz or mean arterial pressure are maintained in the immediate (3-8 h) post-CPB period (114).
Cerebral blood flow, CMR02, and oxygen extraction increase above pre-bypass measurements in children following continuous flow CPB. There is a cerebral hy- peremic response with increased oxygen extraction and metabolism after a period of hypothermic, he- modiluted nonpulsatile perfusion. However, after CPB with deep hypothermic TCA, the CBF and CMR02 are below baseline measurements, although flow- metabolism coupling remains intact. The lack of a hy- peremic response to cerebral hypoxia and acidosis is abnormal, suggesting microcirculatory dysfunction after TCA (86,87,105,115).
Summary Although much has been learned about cerebral phys- iology during CPB in the past decade, the role of al- terations in CBF and CMR02 during CPB and the un- fortunately common occurence of neuropsychologic injury still is understood incompletely. It is apparent that during CPB temperature, anesthetic depth, CM- R02, and Paco2 are the major factors that effect CBF. The systemic pressure, pump flow, and flow character (pulsatile versus nonpulsatile) have little influence on CBF within the bounds of usual clinical practice. Al- though cerebral autoregulation is characteristically
862 REVIEW ARTICLE SCHELL ET AL. CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
ANESTH ANALG 1993;7684945
Pump Flow (21.8 Ilminlm2)
Mean Blood Pressure (230 m m h ) Pa02 (Normal Clinical Values) Temperature
Dnp hypo--
Anesthetic Depth Temperature CMRO2
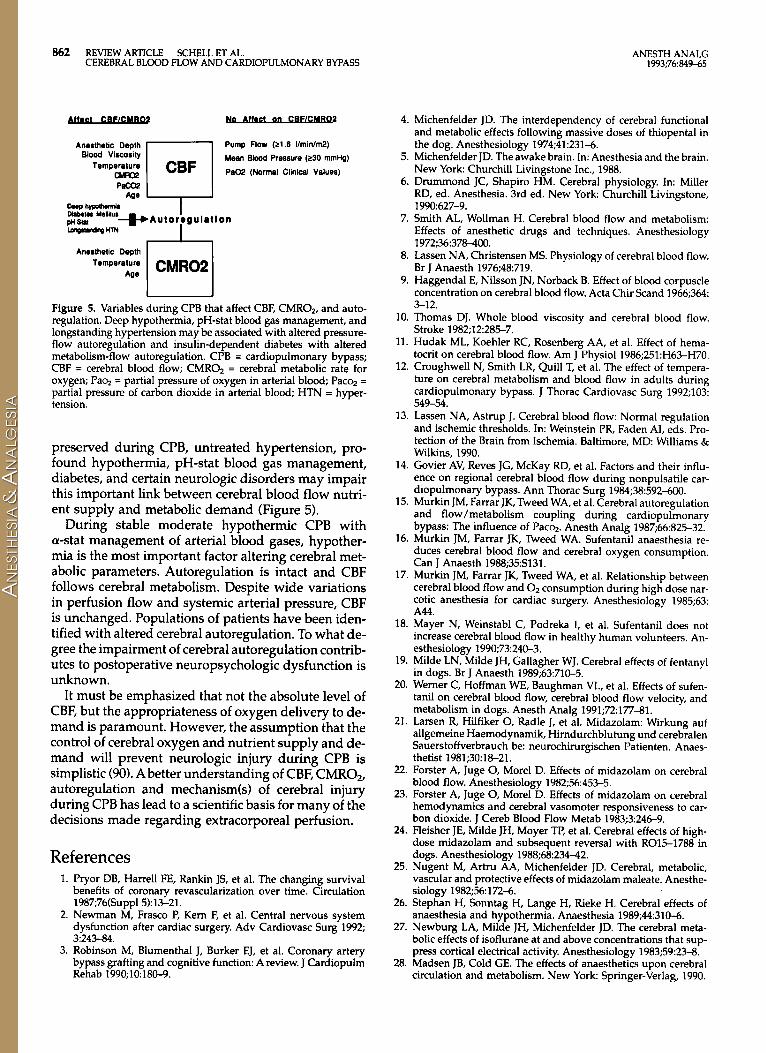
Figure 5. Variables during CPB that affect CBF, CMR02, and auto- regulation. Deep hypothermia, pH-stat blood gas management, and longstanding hypertension may be associated with altered pressure- flow autoregulation and insulin-dependent diabetes with altered metabolism-flow autoregulation. CPB = cardiopulmonary bypass; CBF = cerebral blood flow; CMR02 = cerebral metabolic rate for oxygen; Pa% = partial pressure of oxygen in arterial blood; Pacq = partial pressure of carbon dioxide in arterial blood; HTN = hyper- tension.
preserved during CPB, untreated hypertension, pro- found hypothermia, pH-stat blood gas management, diabetes, and certain neurologic disorders may impair this important link between cerebral blood flow nutri- ent supply and metabolic demand (Figure 5).
During stable moderate hypothermic CPB with a-stat management of arterial blood gases, hypother- mia is the most important factor altering cerebral met- abolic parameters. Autoregulation is intact and CBF follows cerebral metabolism. Despite wide variations in perfusion flow and systemic arterial pressure, CBF is unchanged. Populations of patients have been iden- tified with altered cerebral autoregulation. To what de- gree the impairment of cerebral autoregulation contrib- utes to postoperative neuropsychologic dysfunction is unknown.
It must be emphasized that not the absolute level of CBF, but the appropriateness of oxygen delivery to de- mand is paramount. However, the assumption that the control of cerebral oxygen and nutrient supply and de- mand will prevent neurologic injury during CPB is simplistic (90). A better understanding of CBF, CMR02, autoregulation and mechanism(s) of cerebral injury during CPB has lead to a scientific basis for many of the decisions made regarding extracorporeal perfusion.
References 1. Pryor DB, Harrell FE, Rankin JS, et al. The changing survival
benefits of coronary revascularization over time. Circulation 1987;76(Suppl 5):13-21.
2. Newman M, Frasco P, Kern F, et al. Central nervous system dysfunction after cardiac surgery. Adv Cardiovasc Surg 1992; 3:243-84.
3. Robinson M, Blumenthal J, Burker EJ, et al. Coronary artery bypass grafting and cognitive function: A review. J Cardiopulm Rehab 1990;lo 180-9.
4. Michenfelder JD. The interdependency of cerebral functional and metabolic effects following massive doses of thiopental in the dog. Anesthesiology 1974;41:231-6.
5. Michenfelder JD. The awake brain. In: Anesthesia and the brain. New York Churchill Livingstone Inc., 1988.
6. Drummond JC, Shapiro HM. Cerebral physiology. In: Miller RD, ed. Anesthesia. 3rd ed. New York Churchill Livingstone,
7. Smith AL, Wollman H. Cerebral blood flow and metabolism: 1990~627-9.
Effects of anesthetic drugs and techniques. Anesthesiology 1972;36:378-400.
8. Lassen NA, Christensen MS. Physiology of cerebral blood flow. Br J Anaesth 1976;48:719.
9. Haggendal E, Nilsson JN, Norback 8. Effect of blood corpuscle concentration on cerebral blood flow. Acta Chir Scand 1966;364: 3-12.
10. Thomas DJ. Whole blood viscosity and cerebral blood flow. Stroke 1982;12:285-7.
11. Hudak ML, Koehler RC, Rosenberg AA, et al. Effect of hema- tocrit on cerebral blood flow. Am J Physiol 1986;251:H63-H70.
12. Croughwell N, Smith LR, Quill T, et al. The effect of tempera- ture on cerebral metabolism and blood flow in adults during cardiopulmonary bypass. J Thorac Cardiovasc Surg 1992;103: 549-54.
13. Lassen NA, Astrup J. Cerebral blood flow: Normal regulation and ischemic thresholds. In: Weinstein PR, Faden AI, eds. Pro- tection of the Brain from Ischemia. Baltimore, MD Williams & Wilkins, 1990.
14. Govier AV, Reves JG, McKay RD, et al. Factors and their influ- ence on regional cerebral blood flow during nonpulsatile car- diopulmonary bypass. Ann Thorac Surg 1984;38:592-600.
15. Murkin JM, Farrar JK, Tweed WA, et al. Cerebral autoregulation and flow/metabolism coupling during cardiopulmonary bypass: The influence of Paco2. Anesth Analg 1987;66:825-32.
6. Murkin JM, Farrar JK, Tweed WA. Sufentanil anaesthesia re- duces cerebral blood flow and cerebral oxygen consumption. Can J Anaesth 1988;35:S131.
7. Murkin JM, Farrar JK, Tweed WA, et al. Relationship between cerebral blood flow and 0 2 consumption during high dose nar- cotic anesthesia for cardiac surgery. Anesthesiology 1985;63: A44.
8. Mayer N, Weinstabl C, Podreka I, et al. Sufentanil does not increase cerebral blood flow in healthy human volunteers. An- esthesiology 1990;73240-3.
19. Milde LN, Milde JH, Gallagher WJ. Cerebral effects of fentanyl in dogs. Br J Anaesth 1989;63:710-5.
20. Werner C, Hoffman WE, Baughman VL, et al. Effects of sufen- tanil on cerebral blood flow, cerebral blood flow velocity, and metabolism in dogs. Anesth Analg 1991;72:177-81.
21. Larsen R, Hilfiker 0, Radle J, et al. Midazolam: Wirkung auf allgemeine Haemodynamik, Hirndurchblutung und cerebralen Sauerstoffverbrauch be: neurochirurgischen Patienten. Anaes- thetist 1981;301621.
22. Forster A, Juge 0, Morel D. Effects of midazolam on cerebral blood flow. Anesthesiology 1982;56:453-5.
23. Forster A, Juge 0, Morel D. Effects of midazolam on cerebral hemodynamics and cerebral vasomoter responsiveness to car- bon dioxide. J Cereb Blood Flow Metab 1983;3:246-9.
24. Fleisher JE, Milde JH, Moyer TI', et al. Cerebral effects of high- dose midazolam and subsequent reversal with RO15-1788 in dogs. Anesthesiology 1988;68:234-42.
25. Nugent M, Artru AA, Michenfelder JD. Cerebral, metabolic, vascular and protective effects of midazolam maleate. Anesthe- siology 1982;56172-6.
26. Stephan H, Sonntag H, Lange H, Rieke H. Cerebral effects of anaesthesia and hypothermia. Anaesthesia 1989;44:310-6.
27. Newburg LA, Milde JH, Michenfelder JD. The cerebral meta- bolic effects of isoflurane at and above concentrations that sup- press cortical electrical activity. Anesthesiology 1983;59:23-8.
28. Madsen JB, Cold GE. The effects of anaesthetics upon cerebral circulation and metabolism. New York Springer-Verlag, 1990.
ANESTH ANALG 1993;76@49-65
REVIEW ARTICLE SCHELL ET AL. 863 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
29. Aladj LJ, Croughwell N, Smith LR, Reves JG. Cerebral blood flow autoregulation is preserved during cardiopulmonary by- pass in isoflurane-anesthetized patients. Anesth Analg 1991;72:
30. Nussmeier NA, Arlund C, Slogoff SL. Neuropsychiatric com- plications after cardiopulmonary bypass: Cerebral protection by a barbiturate. Anesthesiology 1986;64:165-70.
31. Zaidan JR, Klochany A, Martin WM, et al. Effect of thiopental on neurologic outcome following coronary artery bypass graft- ing. Anesthesiology 1991;74:406-11.
32. Rogers AT, Stump DA, Gravlee GP, et al. Response of cerebral blood flow to phenylephrine infusion during hypothermic car- diopulmonary bypass: Influence of Pacq management. Anes- thesiology 1988;69:547-51.
33. Ivankovich AD, Miletich DJ, Albrecht RF, Zahed B. Sodium ni- troprusside and cerebral blood flow in anesthetized and unanesthetized goat. Anesthesiology 1976;44:21-6.
34. Michenfelder JD, Milde JH. The interaction of sodium nitro- prusside hypotension, and isoflurane in determining cerebral vasculature effects. Anesthesiology 1988;69:870-75.
35. Larsen R, Teichmann J, Hilfiker 0, et al. Nitroprusside- hypotension: Cerebral blood flow and cerebral oxygen con- sumption in neurosurgical patients. Acta Anaesth Scand 1982;
36. Bunemann L, Jensen K, Thomsen L, Riisager S. Cerebral blood flow and metabolism during controlled hypotension with sodium-nitroprusside and general anaesthesia for total hip re- placement. Acta Anaesthesiol Scand 1987;31:487-90.
37. Pinaud M, Souron R, Lelausque J, et al. Cerebral blood flow and cerebral oxygen consumption during nitroprusside-induced hypotension to less than 50 mm Hg. Anesthesiology 1989;70: 255-60.
38. Rogers AT, Prough DS, Stump DA, et al. Cerebral blood flow does not change following sodium nitroprusside infusion dur- ing hypothermic cardiopulmonary bypass. Anesth Analg 1989; 681 22-6.
39. Rogers AT, Prough DS, Gravlee GP, et al. Sodium nitroprusside infusion does not dilate cerebral resistance vessels during hy- pothermic cardiopulmonary bypass. Anesthesiology 1991;74: 820-6.
40. Colley PS, Sivarajan M. Regional blood flow in dogs during halothane anesthesia and controlled hypotension produced by nitroprusside or nitroglycerin. Anesth Analg 1984;63:503-10.
41. Artru AA, Wright K, Colley PS. Cerebral effects of hypocapnia plus nitroglycerine induced hypotension in dogs. J Neurosurg
42. Kety S, Schmidt CF. The determination of cerebral blood flow in man by the use of nitrous oxide in low concentrations. Am J Physiol 1945;143:5346.
43. Spahn DR, Quill TJ, Hu Wei-Chih, et al. Validation of 133Xe clearance as a cerebral blood flow measurement technique dur- ing cardiopulmonary bypass. J Cereb Blood Flow Metab 1992; 12:155-61.
44. Obrist WD, Wilkinson WE. Stability and sensitivity of CBF in- dices in the noninvasive '33Xe method. In: Hartmann A, Hoyer S, eds. Cerebral blood flow and metabolism measurement. Berlin: Springer-Verlag, 1985:30-36.
45. Chen RYZ, Fan FC, Kim S, et al. Tissue-blood partition coeffi- cient for xenon: Temperature and hematocrit dependence. J Appl Physiol 1980;49:178-83.
46. Aaslid R, Markwalder T-M, Nornes H. Noninvasive transcra- nial doppler ultrasound recording of flow velocity in basal ce- rebral arteries. J Neurosurg 1982;57769-74.
47. Huber P, Harda J. Effect of contrast material, hypercapnia, hy- perventilation, hypertonic glucose and papaverine on the di- ameter of the cerebral arteries. Angiographic determination in man. Invest Radio1 1967;2:17-32.
48. Aaslid R. The doppler principle. In: Aaslid R, ed. Transcranial doppler sonography. New York Springer-Verlag, 1986;23-38.
49. Stump DA, Bowton DL, Prough DS, et al. Correlation of tran- scranial Doppler and cerebral blood flow in patients with post- dural headaches. Anesthesiology 1990;73:A480.
48-52,
26327-30.
1986;64:924-31.
50. van der Linden J, Wesslen 0, Ekroth R, et al. Transcranial doppler-estimated versus thermodilution-estimated cerebral blood flow during cardiac operations. Influence of temperature and arterial carbon dioxide tension. J Thorac Cardiovasc Surg 1991;10295-102.
51. Deverall PB, Padayachee TS, Parsons S, et al. Ultrasound de- tection of microemboli in the middle cerebral artery during car- diopulmonary bypass surgery. Eur J Cardiothorac Surg 1988;2: 256-60.
52. Goetting MG, Preston G. Jugular bulb catheterization: Experi- ence with 123 patients. Crit Care Med 1990;18:1220-3.
53. Nakajima T, Masakazu K, Hayashi Y, et al. Clinical evaluation of cerebral oxygen balance during cardiopulmonary bypass: On-line continuous monitoring of jugular venous oxyhemoglo- bin saturation. Anesth Analg 1992;74:630-5.
54. Jobsis-Vandervliet IT, Fox E, Sugioka K. Monitoring of cerebral oxygenation and cytochrome aa3 redox state. Int Anesthesiol Clin 1987;25:209-30.
55. Bracey VA, Greeley WJ, Greibel JA, et al. Evaluation of brain oxygenation during cardiopulmonary bypass and total circu- latory arrest in children by near infrared spectroscopy. Anes- thesiology 1990;73:A1109.
56. Prough DS, Scuderi PE, Lewis G, et al. Initial clinical experience using in vivo optical spectroscopy to quantify brain oxygen saturation. Anesthesiology 1990;73:A424.
57. Ferrari M, Wilson DA, Hanley DF, et al. Noninvasive determi- nation of hemoglobin saturation in dogs by derivative near- infrared spectroscopy. Am J Physiol 1989;256:H1493-99.
58. Martin GB, Nowak RM, Paradis N, et al. Characterization of cerebral energetics and brain pH by 31P spectroscopy after graded canine cardiac arrest and bypass reperfusion. J Cereb Blood Flow Metab 1990;10:221-26.
59. Tamura M. Non-invasive monitoring of brain oxygen metabo- lism during cardiopulmonary bypass by near-infrared spectro- photometry. Jpn Circ J 1991;55:330-5.
60. Silvay G, Koorn R, Bucek J, et al. Use of noninvasive cerebral optical spectroscopy in patients during cardiopulmonary by- pass. Anesth Analg 1992;74:S292.
61. Clark RE, Dietz DR, Miller JG. Continuous detection of micro- emboli during cardiopulmonary bypass in animals and man. Circulation 1976;54:74-8.
62. Orenstein JM, Sat0 N, Aaron B, et al. Microemboli observed in deaths following cardiac surgery. Hum Pathol1982;13:1082-90.
63. Blauth CI, Arnold JV, Schulenberg WE, et al. Cerebral micro- embolism during cardiopulmonary bypass. J Thorac Cardio- vasc Surg 1988;95:668-76.
64. Moody DM, Bell MA, Challa VR, et al. Brain microemboli dur- ing cardiac surgery or aortography. Ann Neurol1990;28477-86.
65. Solis RT, Kennedy PS, Beall AC, et al. Cardiopulmonary bypass: Microembolization and platelet aggregation. Circulation 1975; 52103-8.
66. Blauth C, Smith P, Newman S, et al. Retinal microembolism and neuropsychological deficit following clinical cardiopulmonary bypass: Comparison of a membrane and bubble oxygenator. Eur J Cardiothorac Surg 1989;3:135-8.
67. Yost G. The bubble oxygenator as a source of gaseous micro- emboli. Med Instrum 1985;19:67-9.
68. Semb BKH, Pedersen T, Hatteland K, et al. Doppler ultrasound estimation of bubble removal by various arterial line filters dur- ing extracorporeal circulation. Scand J Thorac Cardiovasc Surg 1982;16:55-62.
69. Young JA, Kisker CT, Doty DB. Adequate anticoagulation dur- ing cardiopulmonary bypass determined by activated clotting time and the appearance of fibrin monomer. Ann Thorac Surg 1978;26:231-40.
70. Topol EJ, Humphrey LS, Borkon AM, et al. Value of intraoper- ative left ventricular microbubbles detected by transesophageal 2-dimensional echocardiography in predicting neurologic out- come after cardiac operations. Am J Cardiol 1985;5677%5.
71. Barzilai B, Saffitz JE, Miller JG, et al. Qualitative ultrasonic char- acterization of the nature of atherosclerotic plaques in human aorta. Circ Res 1987;60:456-63.
864 REVIEW ARTICLE SCHELL ET AL. CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
ANESTH ANALG 1993;76:849-65
72. Strandgaard S, Olesen J, Skinhoj E, et al. Autoregulation of brain circulation in severe arterial hypertension. Br Med J 1973;l:
73. Barry DI. Cerebral blood flow in hypertension. J Cardiovasc Pharmacol 1985;7(suppl 2):S94-8.
74. Strandgaard S. Autoregulation of cerebral blood flow in hyper- tensive patients: The modifying influence of prolonged antihy- pertensive treatment on the tolerance to acute, drug induced hypotension. Circulation 1976;53:720-7.
75. Strandgaard S. Cerebral blood flow in the elderly: Impact of hypertension and antihypertensive treatment. Cardiovasc Drugs Ther 1991;4(Suppl6):1217-21.
76. Croughwell N, Lyth M, Quill T, et al. Diabetic patients have abnormal autoregulation during cardiopulmonary bypass. Cir- culation 1990;82(suppl IV):407-12.
77. Newman S. The incidence and nature of neuropsychologic mor- bidity following cardiac surgery. Perfusion 1989;4:93-100.
78. Stump DA, Newman SP, Coker LH, et al. The effect of age on neurologic outcome after cardiac surgery. Anesth Analg 1992; 74:S310.
79. Globus M, Melamed E. Progressive age-related decrease in re- gional cerebral blood flow in healthy subject. Isr J Med Sci 1985;
80. Brusino FG, Reves JG, Smith LR, et al. The effect of age on cerebral blood flow during hypothermic cardiopulmonary by- pass. J Thorac Cardiovasc Surg 1989;97541-7.
81. Lassen NA, Feinberg I, Lane MH. Bilateral studies of cerebral oxygen uptake in young and aged normal subjects and in pa- tients with organic dementia. J Clin Invest 1960;39:491-500.
82. Michenfelder JD, Theye RA. The relationship of age to canine cerebral metabolic rate. J Surg Res 1969;9:6458.
83. Simard D, Olesen J, Paulson OB, et al. Regional cerebral blood flow and its regulation in dementia. Brain 1971;94:273-88.
84. Johnsson P, Algotsson L, Ryding E, et al. Cardiopulmonary per- fusion and cerebral blood flow in bilateral carotid artery dis- ease. Ann Thorac Surg 1991;51:579-84.
85. Brusino FG, Reves JG, Prough DS, et al. Cerebral blood flow during cardiopulmonary bypass in a patient with occlusive cerebrovascular disease. J Cardiothorac Anesth 1989;3:87-90.
86. Greeley WJ, Ungerleider RM, Smith LR, Reves JG. Cardiopul- monary bypass alters cerebral blood flow in infants and chil- dren during and after cardiovascular surgery. Circulation 1988; 78(Pt 4):II356.
87. Greeley WJ, Kern FH, Ungerleider RM, et al. The effect of hy- pothermic cardiopulmonary bypass and total circulatory arrest on cerebral metabolism in neonates, infants and children. J Tho- rac Cardiovasc Surg 1991;101:783-94.
88. Michenfelder JD, Theye RA. The effects of anesthesia and hy- pothermia on canine cerebral ATP and lactate during anoxia produced by decapitation. Anesthesiology 1970;33:430-9.
89. Michenfelder JD, Milde JH. The relationship among canine brain temperature, metabolism, and function during hypother- mia. Anesthesiology 1991;75:130-6.
90. Todd MM, Warner DS. A comfortable hypothesis reevaluated: Cerebral metabolic depression and brain protection during is- chemia. Anesthesiology 1992;76:161-4.
91. Civalero LA, Moreno JR, Senning A. Temperature conditions and oxygen consumption during deep hypothermia. Acta Chir Scand 1962;123: 179-88.
92. Kern FH, Ungerleider RM, Reves JG, et al. The effect of altering pump flow rate on cerebral blood flow and cerebral metabolism in neonates, infants and children. Ann Thorac Surg 1992. In press.
93. Michenfelder JD, Milde JH. Failure of prolonged hypocapnia, hypothermia, or hypertension to favorably alter acute stroke in primates. Stroke 1977;8:87-91.
94. Fox LS, Blackstone EH, Kirklin JW. Relationship of whole body oxygen consumption to perfusion flow rate during profound hypothermic cardiopulmonary bypass an experimental study. J Thorac Cardiovasc Surg 1982;83:23948.
95. Fox LS, Blackstone EH, Kirklin JW, et al. Relationship of brain blood flow and oxygen consumption to perfusion flow rate
507-10.
21:662-5.
during profound hypothermic cardiopulmonary bypass an ex- perimental study. J Thorac Cardiovasc Surg 1984;87658-64.
96. Kono M. A clinical study on brain perfusion during cardiopul- monary bypass. J Jpn Assoc Thorac Surg 1990;38:970-81.
97. Tanaka J, Shiki K, Asou T, et al. Cerebral autoregulation during deep hypothermic nonpulsatile cardiopulmonary bypass with selective cerebral perfusion in dogs. J Thorac Cardiovasc Surg 1988;95:124-32.
98. Soma Y, Hirotani T, Yozu R, et al. A clinical study of cerebral circulation during extracorporeal circulation. J Thorac Cardio- vasc Surg 1989;97:187-93.
99. Bashein G, Townes BD, Nessly ML, et al. A randomized study of carbon dioxide management during hypothermic cardiopul- monary bypass. Anesthesiology 1990;72:7-15.
100. Hindman BJ, Funatsu N, Harrington J, et al. Differences in ce- rebral blood flow between alpha-stat and pH-stat management are eliminated during periods of decreased systemic flow and pressure. Anesthesiology 1991;74:1096-102.
101. Rogers AT, Prough DS, Roy RC, et al. Cerebrovascular and ce- rebral metabolic effects of alterations in perfusion flow rate dur- ing hypothermic cardiopulmonary bypass in man. J Thorac Cardiovasc Surg 1992;103:363-8.
102. Miyamoto K, Kawahima Y, Matsuda H, et al. Optimal perfusion flow rate for the brain during deep hypothermic cardiopulmon- ary bypass at 20°C. J Thorac Cardiovasc Surg 1986;92:1065-70,
103. Watanabe T, Hrita H, Kobayashi M, Wahio M. Brain tissue pH, oxygen tension and carbon dioxide tension in profoundly hy- pothermic cardiopulmonary bypass. J Thorac Cardiovasc Surg 1989;97396-401.
104. Swain ]A, McDonald TJ, Griffith PK, et al. Low-flow hypoth- ermic cardiopulmonary bypass protects the brain. J Thorac Car- diovasc Surg 1991;102:76-84.
105. Greeley WJ, Ungerleider RM, Kern FH, et al. Effects of cardio- pulmonary bypass on cerebral blood flow in neonates, infants, and children. Circulation 1989;8O(Suppl I):I209-1215.
106. Stanley TE, Smith LR, White WD, et al. Effect of cerebral per- fusion pressure during cardiopulmonary bypass on neuropsy- chiatric outcome following coronary artery bypass grafting. An- esthesiology 1990;73:A93.
107. Swan H. The importance of acid-base management for cardiac and cerebral preservation during open heart operations. Surg Gynecol Obstet 1984;158:391-414.
108. Prough DS, Rogers AT, Stump DA, et al. Hypercarbia depresses cerebral oxygen consumption during cardiopulmonary bypass. Stroke 1990;21:1162-6.
109. Hindman BJ, Dexter F, Cutkomp J, et al. Brain blood flow and metabolism do not decrease at stable brain temperature during cardiopulmonary bypass in rabbits. Anesthesiology 1992;n:
110. Prough DS, Stump DA, Roy RC, et al. Response of cerebral blood flow to changes in carbon dioxide tension during hypo- thermic cardiopulmonary bypass. Anesthesiology 1986;64: 576-81.
111. Johnsson P, Messeter K, Ryding E, et al. Cerebral vasoreactivity to carbon dioxide during cardiopulmonary perfusion at normo- thermia and hypothermia Ann Thorac Surg 1989;48:769-75.
112. Kern FH, Ungerleider RM, Quill TJ, et al. Cerebral blood flow response to changes in arterial carbon dioxide tension during hypothermic cardiopulmonary bypass in children. J Thorac Cardiovasc Surg 1991;101:618-22.
113. Prough DS, Stump DA, Troost BT. Pacoz management during cardiopulmonary bypass: Intriguing physiologic rationale, con- vincing clinical data, evolving hypothesis? Anesthesiology 1990;72:3-6.
114. McNeill BR, Murkin JM, Farrar JK, Gelb AW. Autoregulation and the COz responsiveness of cerebral blood flow after car- diopulmonary bypass. Can J Anaesth 1990;37313-7.
115. Greeley WJ, Ungerleider RM, Smith LR, Reves JG. The effect of deep hypothermic cardiopulmonary bypass and total circula- tory arrest on cerebral blood flow in infants and children. J Thorac Cardiovasc Surg 1989;97737-45.
342-50.
ANESTH ANALG 1993;76:849-65
REVIEW ARTICLE SCHELL ET AL. 865 CEREBRAL BLOOD FLOW AND CARDIOPULMONARY BYPASS
116. Gravlee GP, Roy RC, Stump DA, et al. Regional cerebrovascular reactivity to carbon dioxide during cardiopulmonary bypass in patients with cerebrovascular disease. J Thorac Cardiovasc Surg
117. Shaw PJ, Bates D, Cartlidge NEF, et al. Analysis of factors pre- disposing to neurological injury in patients undergoing coro- nary bypass operations. Q J Med 1989;72:633-46.
118. Creech 0, Bresler E, Halley M, Adam M. Cerebral blood flow during extracorporeal circulation. Surg Forum 1957;8:510-20.
119. Ogata T, Ida Y, Nonoyama A, et al. A comparative study of the effectiveness of pulsatile and nonpulsatile flow in extracorpo- real circulation. Arch Jpn Clin 1960;29:59.
120. Sandersen JM, Wright G, Sims FW. Brain damage in dogs im- mediately following pulsatile and non-pulsatile blood flows in extracorporeal circulation. Thorax 1972;2727586.
121. Kono M, Orita H, Shimanuki T, et al. A clinical study of cerebral perfusion during pulsatile and nonpulsatile cardiopulmonary bypass. J Jpn Surg SOC 1990;91:1016-22.
122. Watanabe T, Miura M, Orita H, et al. Brain tissue pH, oxygen tension, and carbon dioxide tension in profoundly hypothermic cardiopulmonary bypass. Pulsatile assistance for circulatory ar- rest, low-flow perfusion and moderate-flow perfusion. J Thorac Cardiovasc Surg 1990;100:274-80.
123. Prough DS, Rogers AT, Stump DA, et al. Cerebral blood flow decreases with time whereas cerebral oxygen consumption re- mains stable during hypothermic cardiopulmonary bypass in humans. Anesth Analg 1991;72:161-8.
124. Johnston WE, Vinten-Johansen J, DeWitt DS, et al. Rewarming injury impairs cerebral blood flow after hypothermic cardio- pulmonary bypass. Anesthesiology 1991;75:A543.
125. Schwartz AE, Michler RE, Young WL. Cerebral blood flow dur- ing low-flow hypothermic cardiopulmonary bypass in ba- boons. Anesth Analg 1992;74:S267.
126. Smith ML, Von Hanwehr R, Siesjo BK. Changes in extra- and intracellular pH in the brain during and following ischemia in hyperglycemic and moderately hypoglycemic rats. J Cereb Blood Flow Metab 1986;6:574-83.
127. Marsh WR, Anderson RE, Sundt TM. Effect of hyperglycemia on brain pH levels in areas of focal incomplete cerebral ischemia in monkey. J Neurosurg 1986;65:693-6.
128. Lanier WL. Glucose management during cardiopulmonary bypass: Cardiovascular and neurologic implications. Anesth Analg 1991;72:423-7.
1990;99:1022-9.
129. McKnight CK, Elliot MJ, Pearson DT, et al. The effects of four different crystalloid priming fluids upon the metabolic re- sponse to cardiac operations. J Thorac Cardiovasc Surg 1985; 9097-111.
130. Kuntschen FR, Gallett I'M, Hahn C. Glucose-insulin interac- tions during cardiopulmonary bypass. Hypothermia versus normothermia. J Thorac Cardiovasc Surg 1986;91:451-9.
131. Frasco P, Croughwell N, Blumenthal J, et al. Association be- tween blood glucose level during cardiopulmonary bypass and neuropsychiatric outcome. Anesthesiology 1991;75:A55.
132. Metz S, Keats AS. Benefits of a glucose containing priming so- lution for cardiopulmonary bypass. Anesth Analg 1991;72: 428-34.
133. Stewart DJ, Da Silva CA, Flegel T. Elevated glucose levels may increase the danger of neurologic deficit following profound hypothermic cardiac arrest. Anesthesiology 1988;68:653.
134. Lundar "Lindegaard KF, Frysaker T, et al. Cerebral perfusion during nonpulsatile cardiopulmonary bypass. Ann Thorac Surg 1985;40:144-50.
135. Johnsson P, Messeter K, Ryding E, et al. Cerebral blood flow and autoregulation during hypothermic cardiopulmonary bypass. Ann Thorac Surg 1987;3:386-90.
136. Croughwell ND, Frasco P, Blumenthal JA, et al. Warming dur- ing cardiopulmonary bypass is associated with jugular bulb desaturation. Ann Thorac Surg 1992;53:827-32.
137. Schell RM, Kern FH, Reves JG. The role of continuous jugular venous saturation monitoring during cardiac surgery with car- diopulmonary bypass. Anesth Analg 1992;74:627-9.
138. Venn GE, Sherry K, Klinger L, et al. Cerebral blood flow during cardiopulmonary bypass. Eur J Cardiothorac Surg 1988;2:360-3.
139. Branston NM, Symon L, Crockard HA, et al. Relationship be- tween the cortical evoked potential and local cortical blood flow following acute middle cerebral artery occlusion in the baboon. Exp Neurol 1974;45:195.
140. Astrup J, Symon L, Branston NM, et al. Cortical evoked poten- tial and extracellular potassium and hydrogen at critical levels of brain ischemia. Stroke 1977;8:51.
141. Jones TH, Morawetz RB, Crowell RM, et al. Thresholds of focal cerebral ischemia in awake monkeys. J Neurosurg 1981;54:773.
142. Sundt TM, Sharbrough FW, Piepgras DG, et al. Correlation of cerebral blood flow and electroencephalographic changes dur- ing carotid endarterectomy with results of surgery and hemo- dynamics of cerebral ischemia. Mayo Clin Proc 56533,1981.