of the mitral valve - bhvs · imaging & pathology of the mitral valve madalina garbi md ma frcp...
TRANSCRIPT

Imaging & pathology of the mitral valve
Madalina Garbi MD MA FRCP King’s College Hospital NHS Foundation Trust

MV disease prognosis & management
↓↑ valve morphology
& LV
MITRAL STENOSIS
Imaging & pathology of the mitral valve

MITRAL STENOSIS Rheumatic
commissural fusion, leaflets thickening, chords thickening & fusion => funnel shape

MITRAL STENOSIS
Calcific no commissural fusion => smile shaped orifice
thin leaflet tips / calcified leaflet base
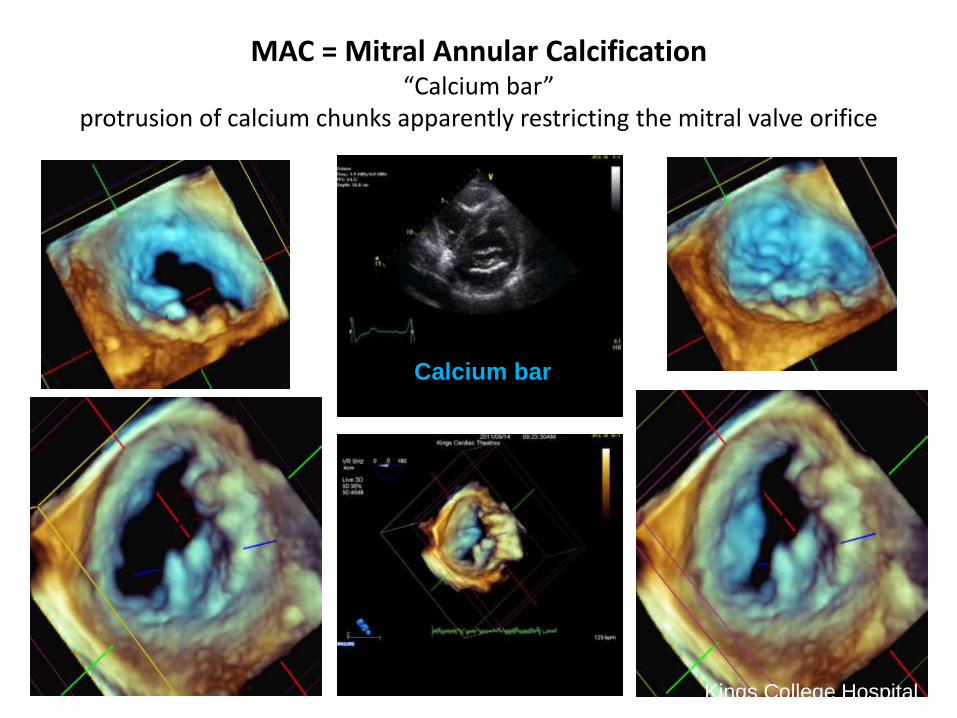
MAC = Mitral Annular Calcification “Calcium bar”
protrusion of calcium chunks apparently restricting the mitral valve orifice
Calcium bar
Kings College Hospital
MITRAL REGURGITATION
Imaging & pathology of the mitral valve

ESC / EACTS Valve disease management guidelines 2012
The role of the imaging cardiologist
→ LV serial assessment
→ Select cases for the “mitral surgeon” Barlow valves Young patients Asymptomatic Anterior leaflet / bi-leaflet prolapse D. Adams et al. Eur Heart J 2010
→ Characterise disease Experience
Mitral valve quantification
S. Chandra et al. (R. Lang) Circ Cardiovasc Imaging 2011
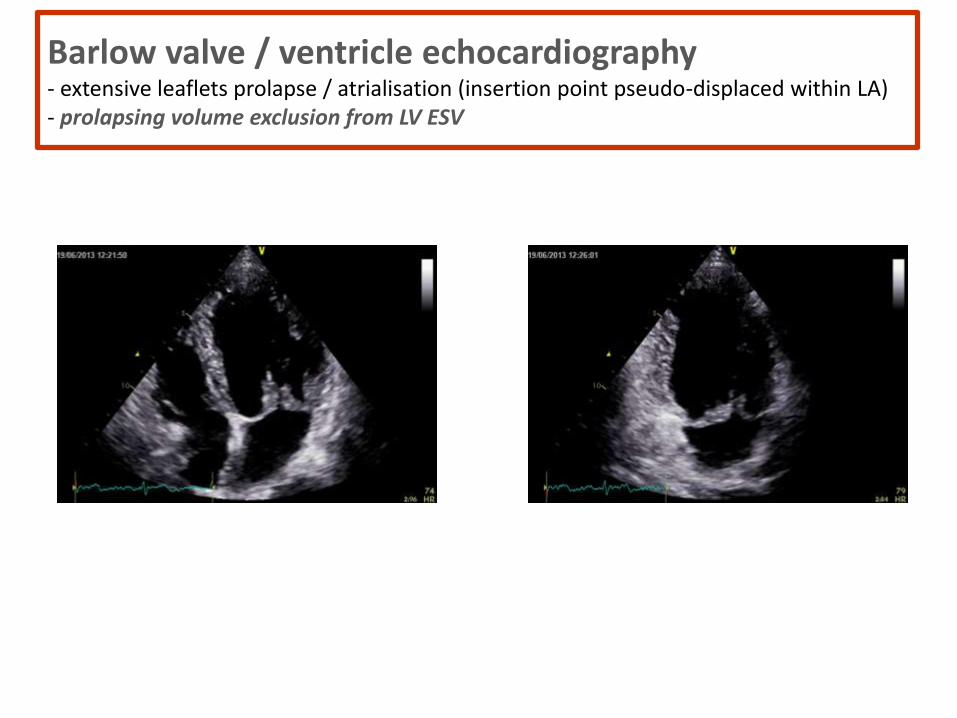
Barlow valve / ventricle echocardiography - extensive leaflets prolapse / atrialisation (insertion point pseudo-displaced within LA) - prolapsing volume exclusion from LV ESV

Characterise disease
Select surgeon Barlow
Anterior leaflet / bi-leaflet
Help surgeon decide strategy Minimally invasive - right thoracotomy (not in Barlow)
Resection (P leaflet) / excess tissue repositioning (A leaflet) Neo-chords (both leaflets)
Annulus size (bigger in Barlow)

3D echo => electronic dissection Example: anterior mitral valve leaflet cleft & ostium primum ASD

3D makes it easy
Anonymised

Ostium primum / TV-MV planes
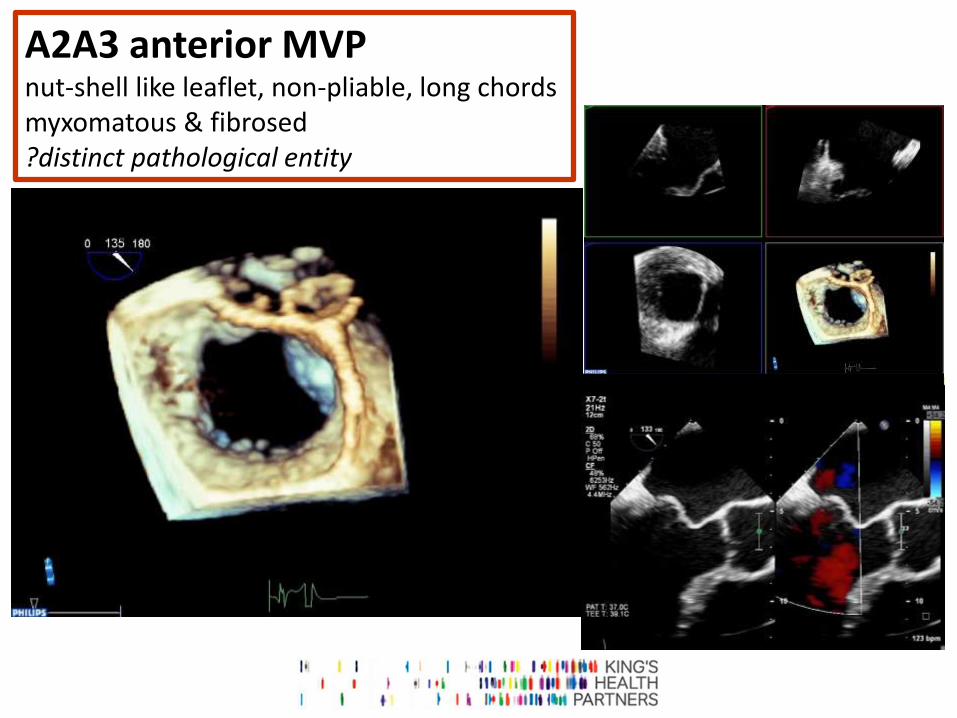
A2A3 anterior MVP nut-shell like leaflet, non-pliable, long chords myxomatous & fibrosed ?distinct pathological entity
Anonymised
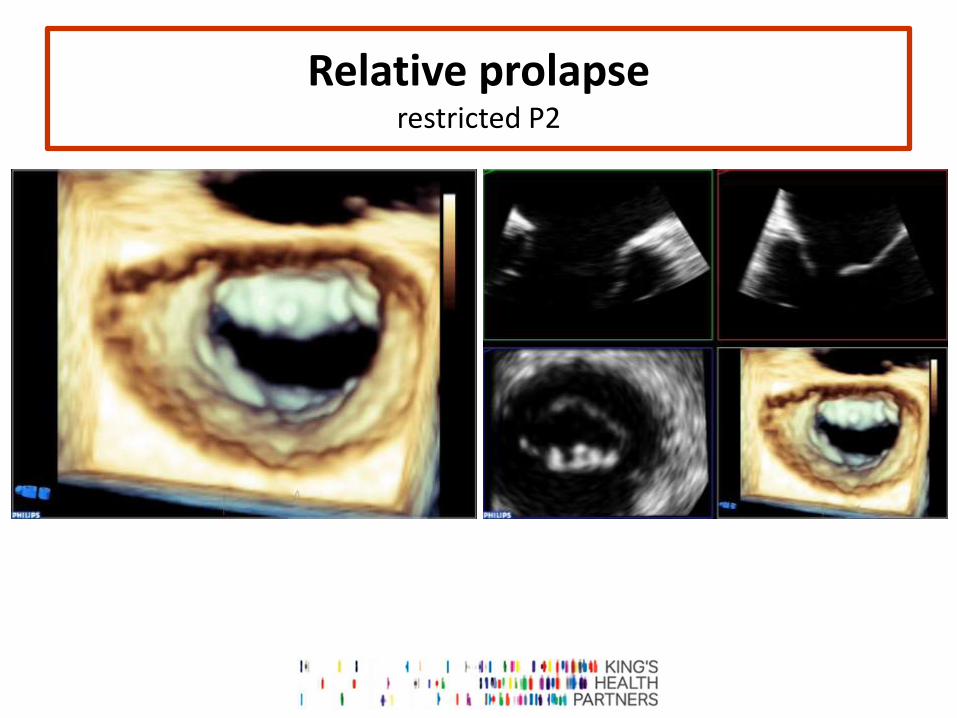
Relative prolapse restricted P2
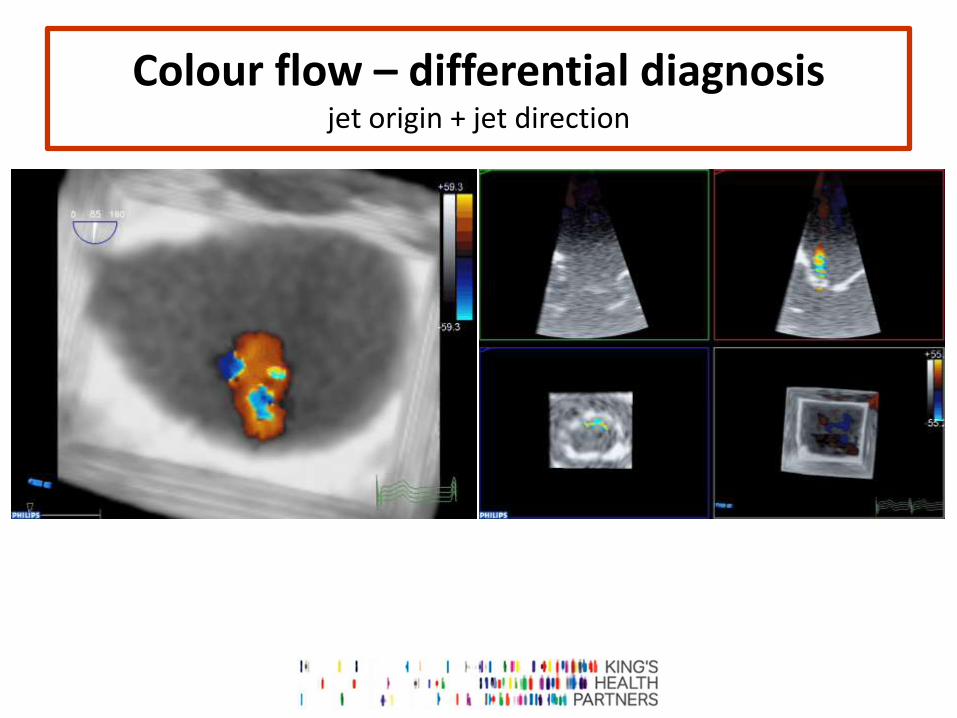
Colour flow – differential diagnosis jet origin + jet direction

Characterise disease
BARLOW FIBROELASTIC DEFICIENCY
Thick leaflets Extensive tissue redundancy
Multi-scallop / multi-segment prolapse Leaflet “atrialisation”
Thickened / elongated / ruptured chords Dilated annulus
More circular annulus
Thin leaflets No tissue redundancy
Single scallop / segment involvement Prolapsing / flail involved segment
Elongated / ruptured involved chords Annulus < 32 mm
Oval shaped annulus
+ Forme fruste
Co-existent pathology
Adapted from Anyanwu & Adams Semin Thorac Cardiovasc Surg 2007

Characterise disease – experience / quantification P2
? Only P2 or complex disease

Characterise disease – experience / quantification P2
? Only P2 or complex disease visual assessment compares with background

3D Mitral Valve
Quantification
Normal Billowing height
< 1mm
Degenerative MV disease
Billowing height > 1mm
Barlow Billowing volume
> 1.15ml
Fibroelastic deficiency
Billowing volume < 1.15ml
S. Chandra et al. (R. Lang) Circ Cardiovasc Imaging 2011

3D MVQ bonus
Anterior leaflet length
Posterior leaflet length (ratio)
Aorto – mitral angle
…

Fibroelastic deficiency

FED P2
Courtesy Prof David Adams, Mitral Valve Repair Reference Centre, Mount Sinai Hospital, New York

FED P2 Triangular Resection Gap closure
True size 26mm Physio Annuloplasty ring
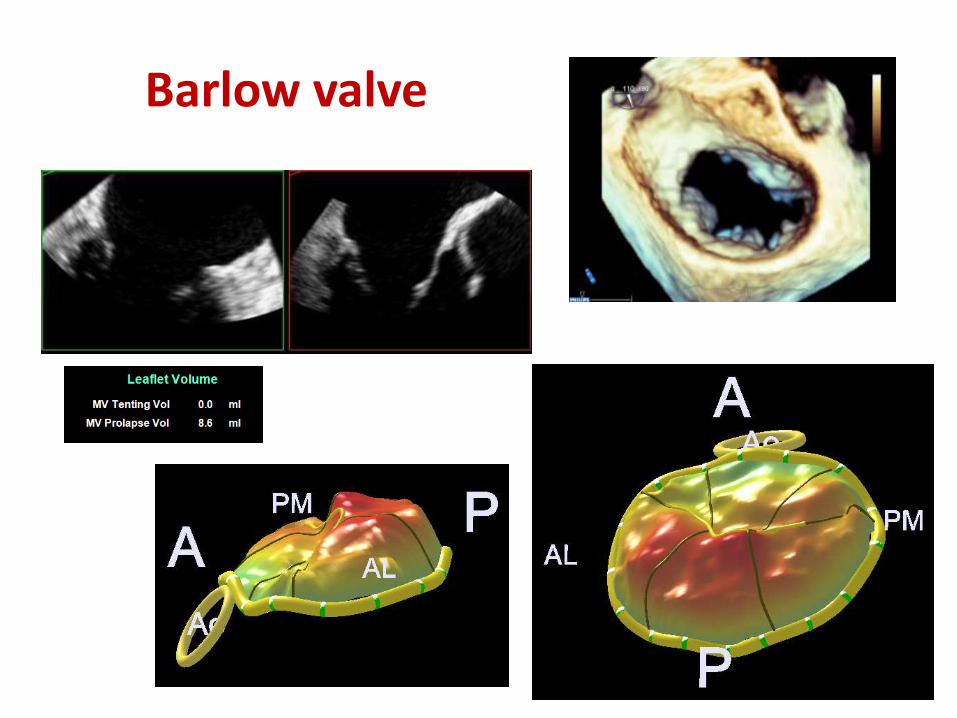
Barlow valve

Barlow P3

BARLOW P2

BARLOW P2

BARLOW P2 sliding plasty
Quadrangular resection P2
Sliding leaflet plasty
Neo-chord to P2
True size 35mm ATS Simulus
Annuloplasty Band

Multi-segmented Barlow’s
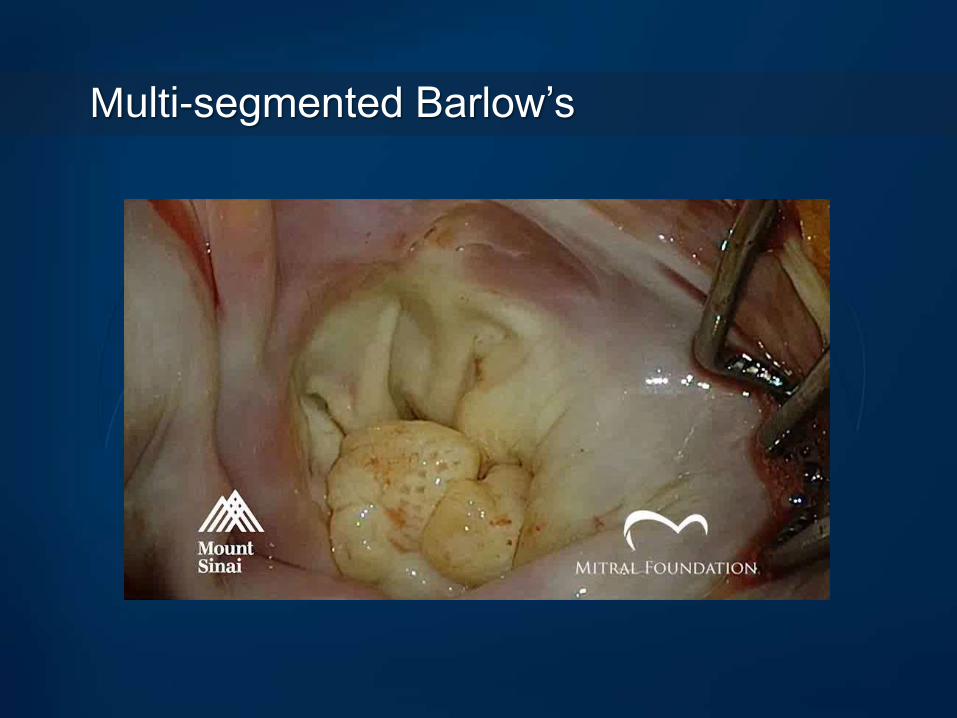
Multi-segmented Barlow’s

1.15ml surgeon ? flail P2, elderly patient

FED P2

Mitral valve surgeon ? Young patient, asymptomatic

Barlow / FF P2

Bi-leaflet involvement “mitral surgeon” job

Before and after assessing the method

Relative anterior leaflet prolapse (restricted posterior leaflet) MVQ experience back-up / substitute
CONCLUSION
Imaging of the mitral valve
morphology / pathology assessment
LV assessment
helps guide the patient towards the right surgeon
may help plan the procedure