office management of common breast complaintsfcm.ucsf.edu/sites/fcm.ucsf.edu/files/08 policar-office...
TRANSCRIPT

Office Management of Common Breast Complaints
Michael Policar, MD, MPHClinical Professor of Ob, Gyn, and Repro SciencesUCSF School of [email protected]
Annual Review of Family MedicineUCSF Mission BayDecember 7, 2017

• There are no relevant financial relationships with any commercial interests to disclose

Learning Objectives
• List 5 treatments for cyclic bilateral mastalgia• List 5 causes of galactorrhea, other than pregnancy• Describe the 7 categories of BI-RADS reports in
breast diagnostic imaging
Obstet Gynecol 2016;127 (6):e141-e156
https://qap.sdsu.eduhttp://qap.sdsu.edu/screening/breastcancer/bda/index.html

https://www.nccn.org/professionals/physician_gls/pdf/breast-screening.pdf

BIRADS: Breast Imaging Reporting and Data SystemMammogram, Ultrasonography, MRI
Assessment % pts
Cancer risk
Recommendation
0 Incomplete Further imaging12
NegativeBenign finding
93.9 Essentially 0% risk
Routine screening
3 Probably benign 5.6 >0% ≤2% Short-interval (6 month) follow-up

BIRADS: Breast Imaging Reporting and Data SystemMammogram, Ultrasonography, MRI
Assessment % pts Cancer risk Recommendation
4 Suspicious 0.4 50% Biopsy4A Low suspicion 2% to ≤10%4B Moderate suspicion >10% to ≤50%4C High suspicion >50% to <95%5 Highly suggestive 0.1 >95% Biopsy
6 Known biopsy-proven malignancy
N/A Surgical excision

Mammographic Breast Density
• 3-5x greater risk of breast cancer in women with high breast density on mammography vs. women with low breast density
• Breast density decreases with – Advancing age– Menopause – Heavier body weight– Earlier childbearing– Higher density in women using hormone therapy
• Increase in mammographic breast density score over time is an important risk factor for breast cancer
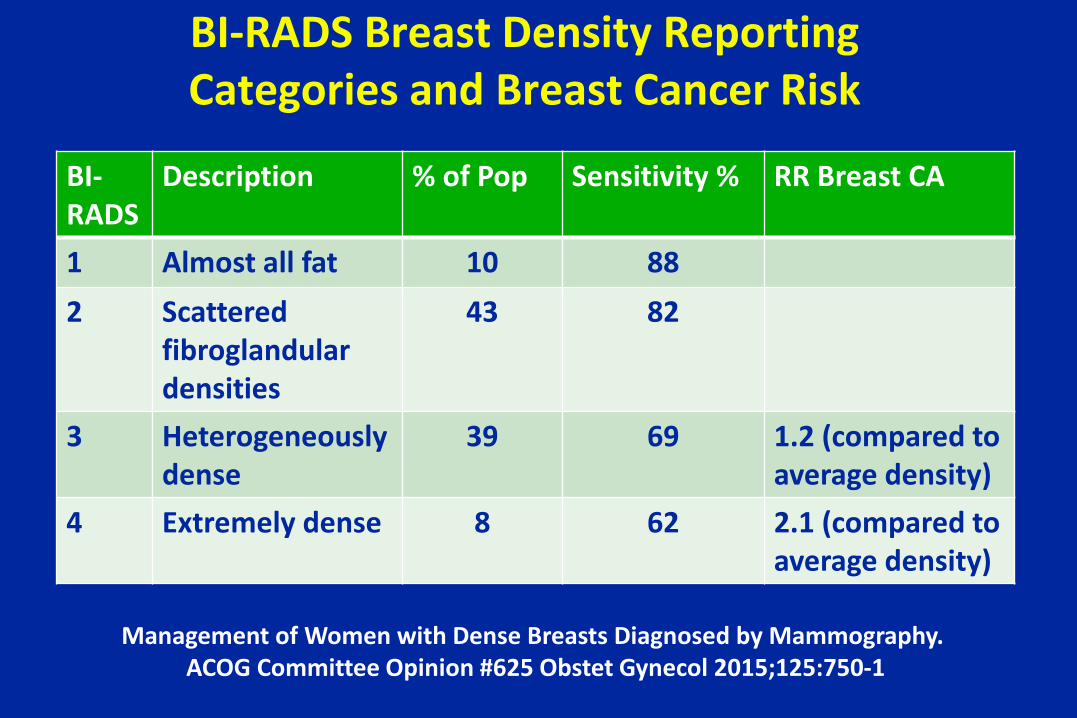
BI-RADS Breast Density Reporting Categories and Breast Cancer Risk
Management of Women with Dense Breasts Diagnosed by Mammography. ACOG Committee Opinion #625 Obstet Gynecol 2015;125:750-1
BI-RADS
Description % of Pop Sensitivity % RR Breast CA
1 Almost all fat 10 882 Scattered
fibroglandulardensities
43 82
3 Heterogeneously dense
39 69 1.2 (compared to average density)
4 Extremely dense 8 62 2.1 (compared to average density)

Mammographic Breast Density
• Longitudinal Measurement of Clinical Mammographic Breast Density (K Kerlikowske JNCI 2007;99:386)– Less density is associated with lower breast ca risk– Increased density over time (average 3 years) is
associated with increased in breast cancer risk•1 2 (5.6x risk) compared to cat 1•1 3 (10x risk) “
• Density changes should be factored into risk calculations


CA Law: Breast Density Reporting
• 2013 CA law requires patients be informed if "dense breast tissue" on screening mammography
• When mammography is the only screening test, sensitivity decreases by 10-20% if "dense breasts“
• Screening mammography recommendations the same for women with dense breasts as others
• If interested in options, a risk assessment is appropriate
– Other "screening options" include screening MRI, ultrasound, and tomosynthesis ("3D mammography")
http://www.cancer.gov/bcrisktool


http://www.halls.md/breast/riskcom.htm

Abnormal Breast Findingsin Primary Care
• Breast nodularity• Breast pain (mastalgia, mastadynia)
– Bilateral– Unilateral
• Nipple discharge (spontaneous)• Breast lump

FCC and Mastalgia: What’s the Difference?
FCC(morphology)
Mastalgia(sydrome)Both

Fibrocystic Change (FCC)
• Pathology– Cysts within ducts and increased fibrous tissue
• Epidemiology– > 50% of reproductive aged women– 10% of women under 21 years old – Abates with menopause; fat replaces fibrous tissue
• Symptoms– Either cyclic mastalgia or asymptomatic– Pain, tenderness in lumpy areas of breast

Fibrocystic Change (FCC)
• Findings– Symmetric (mirror image) nodularity– Consistency commonly like a “bag of beans”– Nodularity often prominent in upper outer region
• Cancer risk depends upon biopsy findings– Non-proliferative (70%): No increased risk– Proliferative (25%): 2x risk– Atypical ( 4%): 5x risk– Atypical + family hx 11x risk
Cyclic Bilateral Mastalgia (Mastadynia)
• 47% of breast-related visits in women 40-69 yo• Symptoms
– Pain maximal pre-menstrually, wanes with menses– Dull, full, achy, or heavy– Tender (equal or asymmetric); usually worse in UOQ

Cyclic Bilateral Mastalgia
• Non-medical management– Reassure patients that they do not have cancer– Well-fitting bra, especially for exercise and athletics– Elimination of caffeine (coffee, tea, cola, chocolate) has
not been shown to decrease symptoms– Consider Evening primrose oil (EPO) 1,500 mg BID
•RCT: 45% had some improvement (vs. 19% placebo)– Vitamin E (600 U/day)…not supported in RCT– Vitamin A (150,000 IU/ day)…no RCT

Cyclic Bilateral Mastalgia: Drugs
• Topical diclofenac 50 mg gel TID• Mild oral analgesics, starting premenstrually• OC’s help 70-90% of women
– Continuous OC regimen (no hormone-free interval)• Bromocriptine (5 mg QD): 80% had less pain, nodularity• Danazol (200 mg QD): 90% had reduction in pain• Tamoxifen (10 mg QD): 90% had reduction in pain• All treatments: 50% relapse rate
Non-Cyclical Mastalgia
• Less common, more likely pathologic• Usually focal, unilateral• Differential diagnosis
– Breast cyst– Fibroadenoma– Breast abscess– Rarely, breast cancer (inflammatory carcinoma)
• Diagnostic imaging– Breast ultrasound + diagnostic mammogram
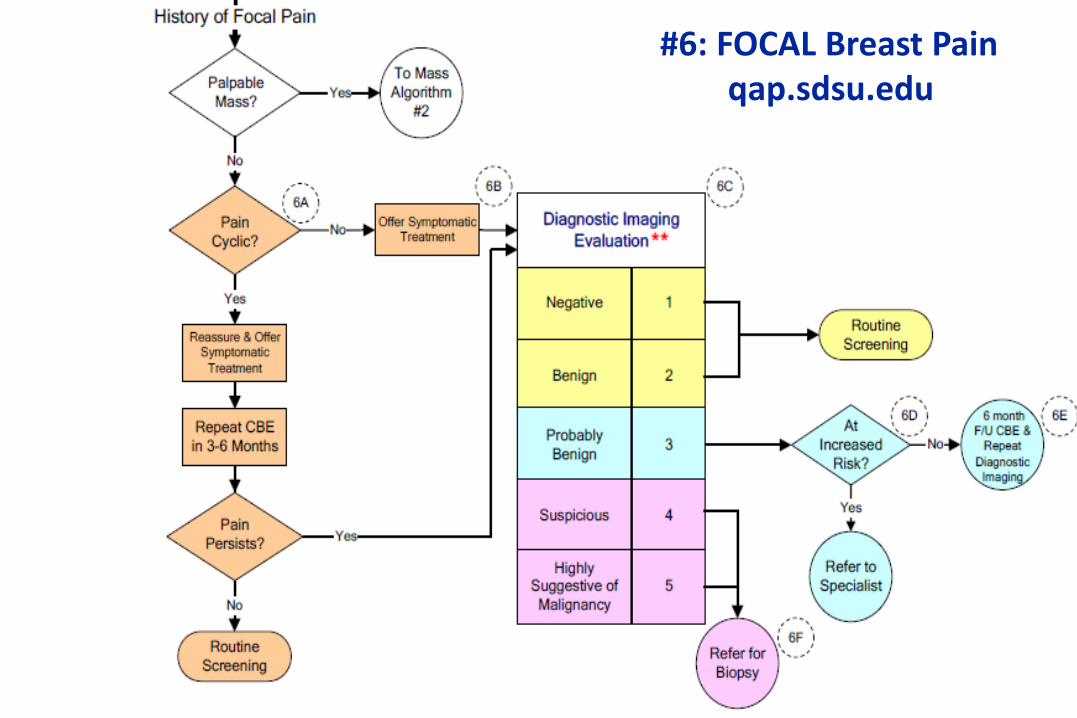
#6: FOCAL Breast Painqap.sdsu.edu
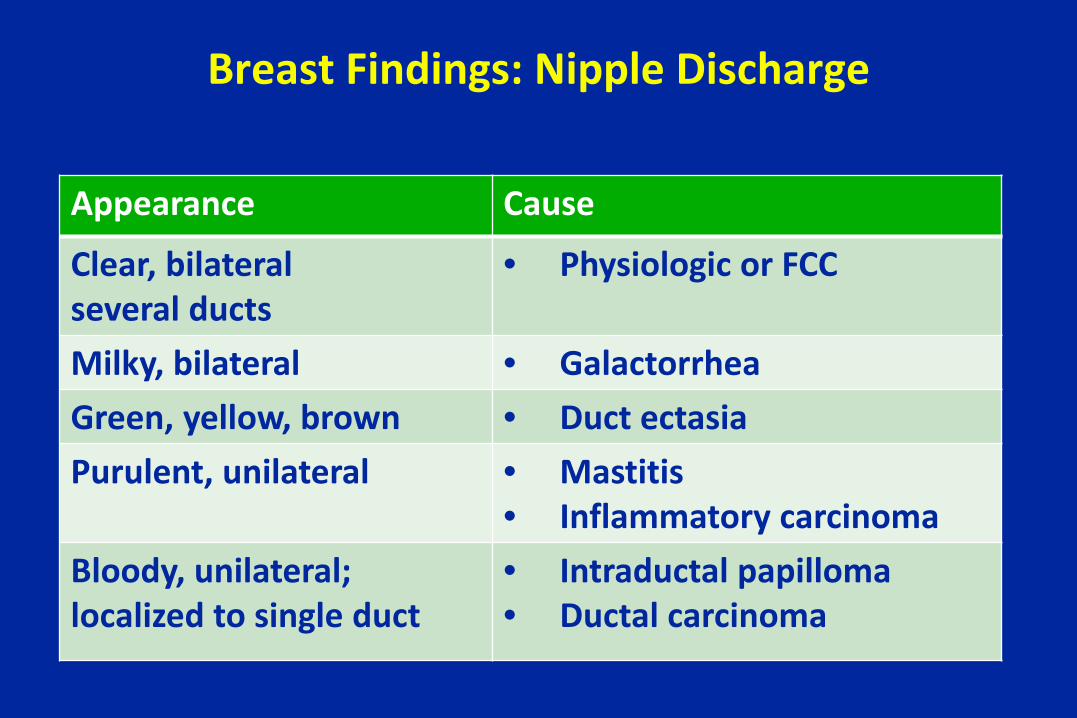
Breast Findings: Nipple Discharge
Appearance Cause
Clear, bilateralseveral ducts
• Physiologic or FCC
Milky, bilateral • GalactorrheaGreen, yellow, brown • Duct ectasiaPurulent, unilateral • Mastitis
• Inflammatory carcinomaBloody, unilateral; localized to single duct
• Intraductal papilloma• Ductal carcinoma
Intraductal Papilloma
• Solitary papillomas can present as bloody, serous, or clear nipple discharge
• Most common in women 30–50; typically 2–4 mm
• DCIS has been diagnosed in solitary papillomas, but usually not associated with cancer
• If atypia is present on core biopsy of an intraductal papilloma, surgical excision is recommended

ACOG Practice Bulletin #1642016

Inappropriate Lactation: Galactorrhea
% of cases Cause45 % Idiopathic20 % Pituitary tumors10 % • Estrogen-containing contraceptives
• Drugs (dopamine inhibitors)5 % Primary hypothyroidism20 % Miscellaneous
• Neurogenic (breast stim, post-herpetic)• Parapituitary lesions• Post-partum lactation, <1 yr of wean’g

Galactorrhea: Idiopathic
• Diagnosis of exclusion– 40-50% of all galactorrhea cases
• Normal or minimally elevated PRL• Most have normal (ovulatory) menstrual pattern• If galactorrhea + PRL < 50 ng/mL + regular menstrual
cycling, further W/U is not necessary• Management is expectant
– Repeat PRL annually if galactorrhea continues– Dopamine agonist for infertility, breast discomfort

Galactorrhea: Pituitary Tumors
• Prolactinoma as cause of galactorrhea– 20% of all galactorrhea cases– 34% if galactorrhea-amenorrhea present
• Prolactinomas most common PRL secreting tumor– Almost all are benign, rarely invasive– Microadenoma (< 10 mm)– Macroadenoma (> 10 mm): supra sellar growth
• Presence of adenoma is not a contraindication to either pregnancy or use of hormonal contraception

Galactorrhea: Hormonal Contraceptives
• Estrogen stimulates PRL + reduced dopamine (PIF)• Galactorrhea most common during hormone-free days
(loss of E+P “brake” on lactation)• OC users have (average) 22% increase in PRL level, but
usually in within normal range• When PRL level is elevated
– Usually under 50 ng/ml– Never more than 100 ng/ml
• PRL resolves within 6 months of discontinuation

Galactorrhea: Medications
• Act through reduction of hypothalamic dopamine• Antipsychotics
– Clozapine, risperidone, olanzapine • Antidepressants
– SSRIs: fluoxitine, citalopram, paroxitine– Tricyclics: amitriptyline, imipramie
• Anxiolytics: alprazolam, buspirone, diazepam• H2 blockers: cimetidine, famotidine • Others: metoclopramide, opiates, cocaine

Galactorrhea: Exam and Lab Evaluation
• Examine breasts for masses; nipple discharge– Galactorrhea issues from multiple ducts– Almost always bilateral (one side can be dominant)– White or clear discharge– Fat globules on microscopy
• Visual field examination not helpful• Lab tests
– Prolactin (PRL), with no recent nipple stimulation – TSH

Galactorrhea: Imaging Studies
• To image sella turcica, order either – Thin section coronal CT scan with contrast– “Pituitary MRI”
•MRI more accurate; but expense, time – Skull film with “cone down” is no longer available
• Indications– Menstrual abnormality + galactorrhea or PRL– Prolactin > 100 ng/ml– CNS symptoms: headaches, visual changes

Galactorrhea: Management (1)
Galactorrhea
• PRL < 100 ng/mL and• Normal menses
• PRL > 100 ng/mL or• Abnormal menses or• HA, visual change
Sellar imaging• Head CT or• Pituitary MRI
• PRL, TSH
Asymptomatic
Expectantmanagement
Infertility ORBreast discomfort
Dopamineagonist
Fritz & Speroff. Clinical Gynecologic Endocrinology and Infertility, 8th ed

Galactorrhea Management (2)Galactorrhea + irregular menses orPRL >100 or headache, visual change
Sellar imaging
< 100 ng/mL andNormal imaging
Normal TSH
ElevatedTSH
Expectantmanagement
Thyroidreplacement
> 100 ng/mL orAbnormal imaging
Normal pituitary
Abnormal pituitary
Next slide
Fritz & Speroff. Clinical Gynecologic Endocrinology and Infertility, 8th ed

Galactorrhea Management (3)
AbnormalPituitary
Prolactinoma Non-Prolactinoma
Microadenoma Macroadenoma
Expectantmanagement
Dopamineagonist
further growthSurgery
+ Radiation

Breast Trauma
Breast Cyst: Background
• Pathology: variant of FCC; not precancerous• Epidemiology
– Most common cause of mass in 30-50 yo women– Rare (but possible) < 30 and post-menopausally
• Symptoms– Frequently, but not always, pain and tenderness– Often worse pre-menstrually, then regresses
• Signs– Unilateral smooth, spherical, ballotable mass


Breast Cyst: Management
• Suspected breast cyst: (office) needle aspiration– Mass deflates + clear fluid: no further evaluation– Bloody fluid: send for cytology; biopsy – Mass remains: manage as dominant nodule
• If needle aspiration unavailable, refer to radiologist for diagnostic mammogram + ultrasound
• If frequent recurrences or tenderness– Attempt caffeine restriction, OC’s, ? Vitamin E– If cyst recurs twice, consider excision

Fibroadenoma: Background
• Pathology: solid (fibrous) spherical benign neoplasm• Epidemiology
– Av. age: 25; 12% of masses in menopausal women– 10% of all breast neoplasms
• Findings– 1-3 cm painless spherical dominant mass– Rubber ball firmness; multi-lobed or grooved– Mammographic characteristics
•Mass with clear borders (“halo” effect )• Calcifies post-MP into “popcorn” pattern


Fibroadenoma: Management
• Must differentiate from cancer; diagnosis based upon– Tissue sample: FNAC or open biopsy, or – Typical diagnostic mammogram findings– Not diagnosed by clinical impression alone
• Management options include– Surgical excision: unclear dx, older age group, large size,
psychologically disturbing to woman, or– Observation with yearly CBE + mammogram
•Hormonal contraceptives can be used in women with breast fibroadenomas

Breast Cancer: Presentation
• Often asymptomatic• Early signs
– Unilateral non-tender breast nodule; most often UOQ– Rarely, nodule can be tender if inflammatory changes
• Later signs– Dimpling or “peau d’orange” of overlying skin– Fixation to underlying pectoral muscles– Hypervascularity– Unilateral, recent onset nipple inversion– Palpable axillary or spraclavicular lymph adenopathy

Recur>1x
Follow
Breast Nodule
Office Aspiration
Cystic Solid
Cyst
Residual Mass Bloody
CNB/FNAB
ResultNo
Yes
Follow
Diagnostic MG + Ultrasound
Clear
FindingsProceduresDiagnosesOutcomes

Malignant(breast cancer)
Fibroadenoma(or other benign)
Atypical orNon-diagnostic
Biopsy (Excisional, core cutting, stereotactic)
Benign Malignant
Oncologic Evaluation
Sxs or fastgrowing? Yes
ExcisionalBiopsy
NoFollow
CNB/FNAB
Consultradiologist
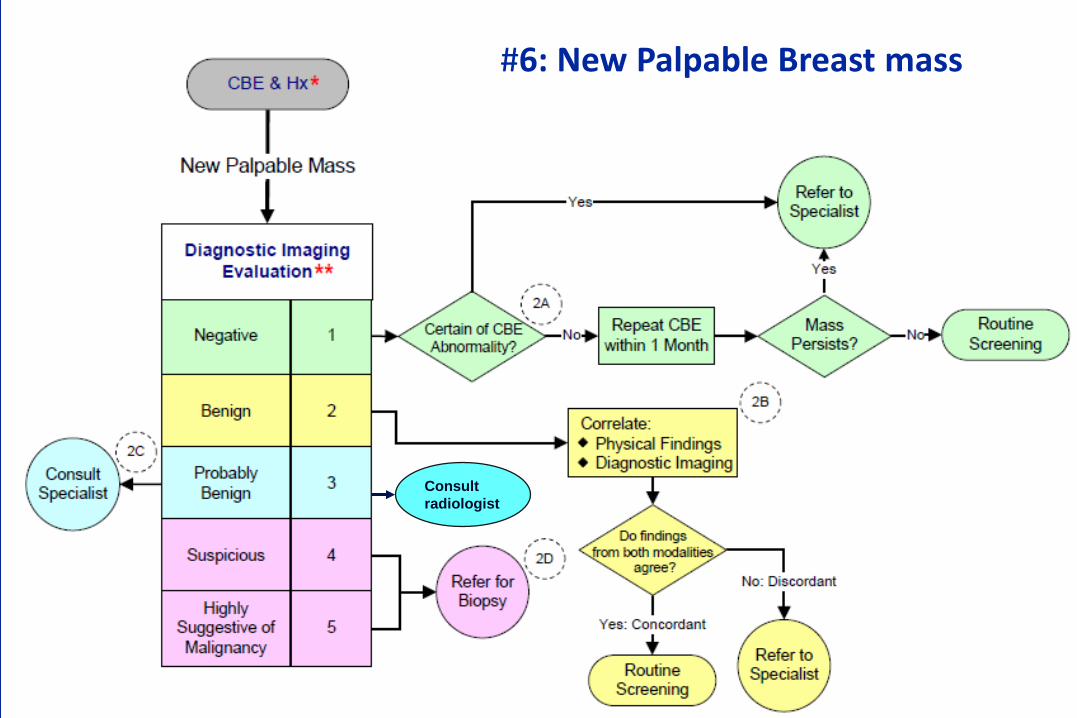
#6: New Palpable Breast mass

Which Type of Breast Biopsy?
CNB: Core Needle Biopsy• Large-bore (12–16 gauge) cutting needle• Can be attached to vacuum-assist• CNB now is preferred breast biopsy method
– Few complications– Minimizes surgical changes to the breast– Can place a clip to mark the lesion undergoing
biopsy (reference in future imaging studies)
ACOG Practice Bulletin #164, 2016
Which Type of Breast Biopsy?
FNAC: Fine Needle Aspiration Cytology
• Small-bore (21–25 g) needle for cytologic specimen
• Inexpensive and minimally invasive but requires pathologist with expertise in interpretation
• Findings of atypia or malignancy require a follow-up tissue biopsy
ACOG Practice Bulletin #164, 2016

Which Type of Breast Biopsy?
Excisional biopsy • Not as first line tissue diagnosis• Not amenable to stereotactic or ultrasound-guided
biopsy 2o to location, imaging findings, or implants• If CNB is non-diagnostic or discordant with clinical exam
or imaging findings – eg, a BI-RADS 4 or 5 mammography result with
normal-appearing breast tissue on core needle biopsy
ACOG Practice Bulletin #164, 2016

Palpable Mass: Clinical Evaluation
• “Triple Diagnosis” misses very few cancers– Physical exam – Diagnostic mammogram + breast ultrasound – CNB or FNAB
• Management– If all 3 negative, f/u exam q3-6 mos x 1 year– If all 3 suggestive of malignancy, refer for definitive
treatment– If any one test suggestive of malignancy, refer for
core or excisional breast biopsy

#7: Breast Biopsy

NCCN Algorithm
Breast Mass> 30 y.o.

Br MassUnder 30

Breast Disease: US MEC 2016
OC/ P/R
POP DMPA Imp-plant
LNG-IUS
Cu-IUC
Undiagnosed breast mass
2 2 2 2 2 1
Family history of breast cancer
1 1 1 1 1 1
Benign breast disease 1 1 1 1 1 1
Breast cancer; current 4 4 4 4 4 1Past breast cancer (no evidence of current disease for 5 years)
3 3 3 3 3 1

References
• ACOG Practice Bulletin #164. Diagnosis and Management of Benign Breast Disorders. Obstet Gynecol 2016;127 (6):e141-e156
• ACOG Practice Bulletin #179. Breast cancer risk assessment and screening in average risk women. Obstet Gynecol 2017;130: e1-16
• Cancer Detection Section, CDPH. Breast Cancer Diagnostic Algorithms for Primary Care Providers 4th edition. 2011.
– https://qap.sdsu.edu/screening/breastcancer/bda/flowcharts/
tools.html