ohio justice alliance for community corrections october 13, 2011
TRANSCRIPT

Ohio Justice Alliance for Community Corrections
October 13, 2011
MHAC’s Mission
Foster education and awareness of mental health issues while advocating for public policies and strategies that
provide an effective, well-funded mental health system that serves those in
need, resulting in a stronger community.
What the MHAC Does The MHAC provides a unique forum for interested
organizations to share experiences, needs and expectations of the mental health system; to set priorities and an agenda for change; and to speak with one voice on the public policies and funding issues that impact mental health.
Work to create change leading to an effective, efficient, and integrated mental health system
Promote diversifying resources to support maintenance and improvements to the current system of mental health service delivery
Increase awareness, knowledge, and understanding of mental health and the impact of untreated mental illness on the community

By The Numbers: Developing a Common
Understanding for the Future of Behavioral Health Care
Completed in partnership with The Center for Community Solutions
Purpose was to:Consolidate and highlight existing statewide
data on behavioral health to better inform policy decisions

Content Introduction Community Behavioral Health System Medicaid Spending for Individuals Previously
Treated in the Community System Hospitals and Emergency Departments Long-term Care Adult and Juvenile Justice Primary and Secondary Education Premature Death Recommendations

Landscape
Over 2.8 million Ohioans have a diagnosable mental illness
Over 550,000 adult Ohioans have a severe mental illness
Over 851,000 Ohioans have a substance dependence or abuse disorder
Roughly 50% of individuals with a severe mental illness are also affected by substance abuse

Landscape
Many individuals who need behavioral health treatment receive it; too many others do not
Treatment and supportive services ideally should be available early enough to prevent the need for more costly interventions
Adult Criminal Justice ODRC provided the data for this section of
the report ODRC provides outpatient care,
prescription drugs, residential care and acute care psychiatric treatment
Every new inmate receives a mental health evaluation at reception and further evaluations if necessary

Mental Health Caseload Inmates are assigned to the “mental health
caseload” if: They are on psychotropic medications prior to entry
into the prison system and their evaluation indicates the need to continue medication and/or other treatments
They are referred based on the initial and detailed screenings at reception
Referrals from self or staff
Inmates not on the “mental health caseload” can receive crisis services and/or up to 3 clinical contacts.

Mental Health Caseload Numbers
20.4% of the inmate population is on the mental health caseload
44.3% of the mental health caseload (9% of the entire inmate population) has a severe mental illnessThis is higher than in the general population
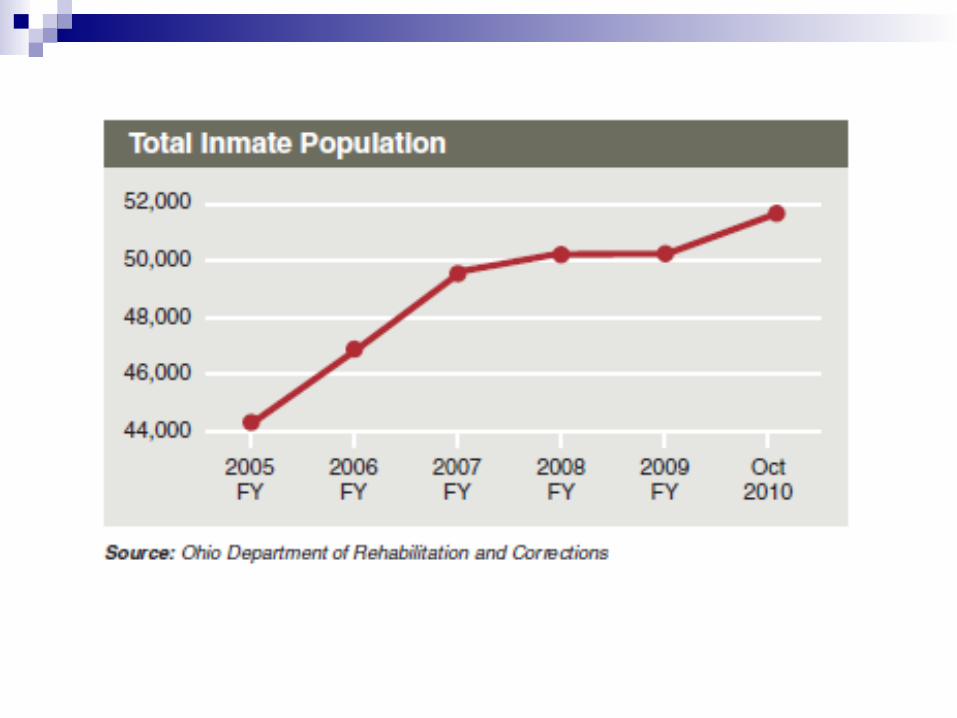
The number of inmates on the mental health caseload grows proportionately to the growth of the total inmate population

Recovery Services for Substance Disorders
35% of inmates receive recovery services Less than 1% of inmates utilize both
substance abuse treatments and mental health services
Unlike mental health services, substance abuse treatments are voluntary

Intake Study – Mental Health 67% of inmates did not have a history of a
mental illness 29% received treatment for a mental
illness prior to incarceration 4% either self-disclosed a mental illness or
showed evidence of a mental illness Less than 1% had a diagnosis of a mental
illness but had not received treatment prior to incarceration

Intake Study – Substance Disorders
Over 78% of inmates showed evidence of recent drug abuse Including 1.7% who reported receiving treatment in
the last 6 months
About 90% of inmates had a history of drug abuse Including 33% that had received treatment more than
6 months prior to their arrest
49% of inmates have recent alcohol abuse 70% of inmates have a history of alcohol abuse


Average Length of Stay
Less than 12% of inmates on the mental health caseload are serving sentences less than 1 year
The average length of stay is 3 times as long for individuals on the mental health caseload6 years and 2.5 months vs. 2 years


Recidivism
36% of individuals admitted to prison because of a probation violation have mental health needs
Recidivism rates for individuals with and without severe mental illnesses are similar

Forensic Hospital Population
Forensic patients use half of the state psychiatric bed days during the year
Forensic hospital bed days are used for:Restoring competency to stand trail Individuals deemed Not Guilty by Reason of
Insanity Individuals deemed Incompetent to Stand
Trail - Unrestorable

Juvenile Justice DYS provided the data for this section of
the report DYS is responsible to confine and provide
services to youth that have been adjudicated for a felony and committed to a facility.
Not all youth adjudicated for a felony are committed to DYS
Rate of commitment is 17%


Mental Health Caseload Growth
From 2006 to 2010, the percent of youth on the mental health caseload grew by 14.5%
49.5% of youth in DYS facilities are on the mental health caseload
6% were on a mental health unit

Average Length of Stay
Youth on the mental health caseload stay twice as long as the total DYS population22 months for youth on the mental health
caseload11.9 months for the total DYS population


Juvenile Diversion Behavioral Health/Juvenile Justice
Initiative diverts youth to community treatment
Youth display improved functioning levels, decreased drug utilization and less risk for out of home placement after the program
Youth also have decreased juvenile court involvement after the program

Recommendations - Funding
If state policies change to require treatment instead of incarceration, then appropriate and adequate funding for behavioral health services must be allocated to build capacity to ensure services are available to all those in need.

Recommendations - Policy
Federal and State rules and regulations around “aging out of foster care” need to be examined to allow for youth who turn 18 in the ODYS system to utilize the expansion of Medicaid for foster children.

Recommendations - Policy
Improve connections and access to services for individuals leaving the custody of the adult and juvenile criminal justice system. Individuals with behavioral health disorders leaving state institutions must be connected with and have access to a continuum of adequate and appropriate community based services, including behavioral health services.

Recommendations - Policy
ODRC should revisit policies around recovery services to refocus on appropriate and adequate treatment and education for alcohol and other drug abuse.

Recommendations – Additional Data
Centralized data on the mental health caseload and spending for individuals incarcerated in jails.
Further research on why prisoners on the ODRC mental health caseload are incarcerated 3 times longer than those not on the caseload and juveniles on the ODYS mental health caseload are incarcerated 2 times longer than those who are not.

Elizabeth Cornachione
Program and Policy Director
Mental Health Advocacy Coalition (MHAC)
216-432-7262
mentalhealthadvocacy.org
facebook.com/MHAC.Ohio
Questions & Answers