ohss
TRANSCRIPT
www.company.com
AICOG 2015
OVARIAN HYPER STIMULATION
SYNDROME
D
ARA DR SUNDAR NARAYANAN
YANAN
www.company.com
AICOG 2015
• Ovarian hyper stimulation syndrome
(OHSS) is an exaggerated response to
ovulation induction.
• The OHSS is typically associated with
exogenous gonodotrophin stimulation and
is rarely observed with oral ovulation
induction agents.
www.company.com
AICOG 2015
• OHSS is usually a self-limiting disorder
• Milder forms resolves spontaneously within
few days, but may persist for longer periods
and progress to severe disease especially if
conception occurs.
www.company.com
AICOG 2015
• More over there is a significant increase in pregnancy related complications among OHSS affected pregnancies.
• There fore it is the responsibility of the treating physician to well aware of this iatrogenic disease, prevention and management of its complications.
www.company.com
AICOG 2015
• Rates of occurrence
• Mild : 8-23%
• Moderate : 1-7%
• Severe : 0.25%
• Mortality
• 3/100,000 cycles
www.company.com
AICOG 2015
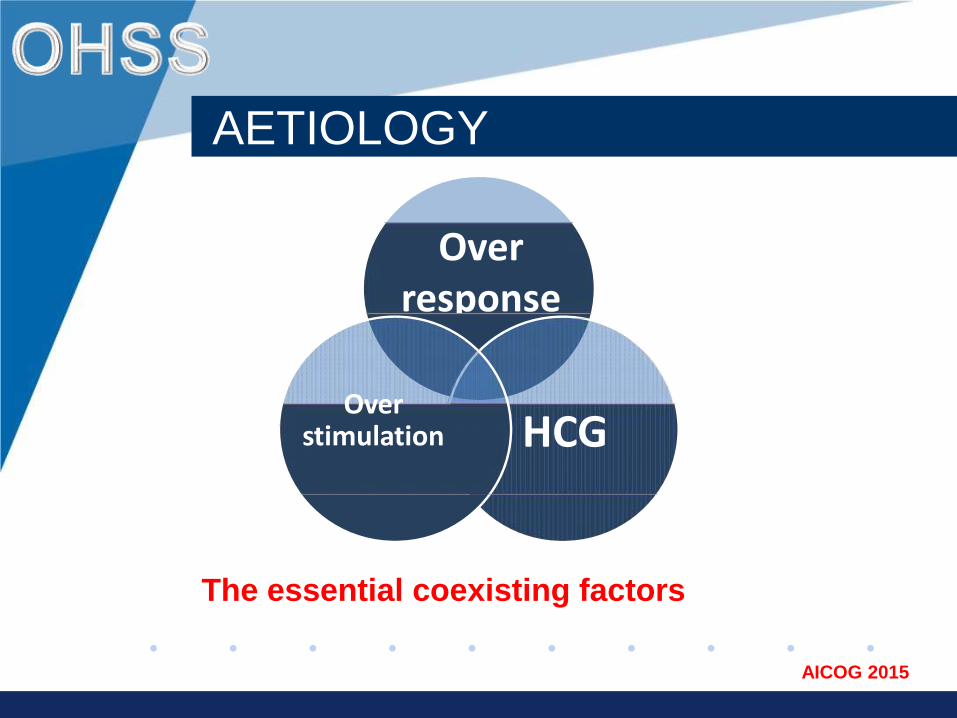
The essential coexisting factors
CO
Overresponse
HCG
simple model
Over stimulation pregnancy,
AETIOLOGY
www.company.com
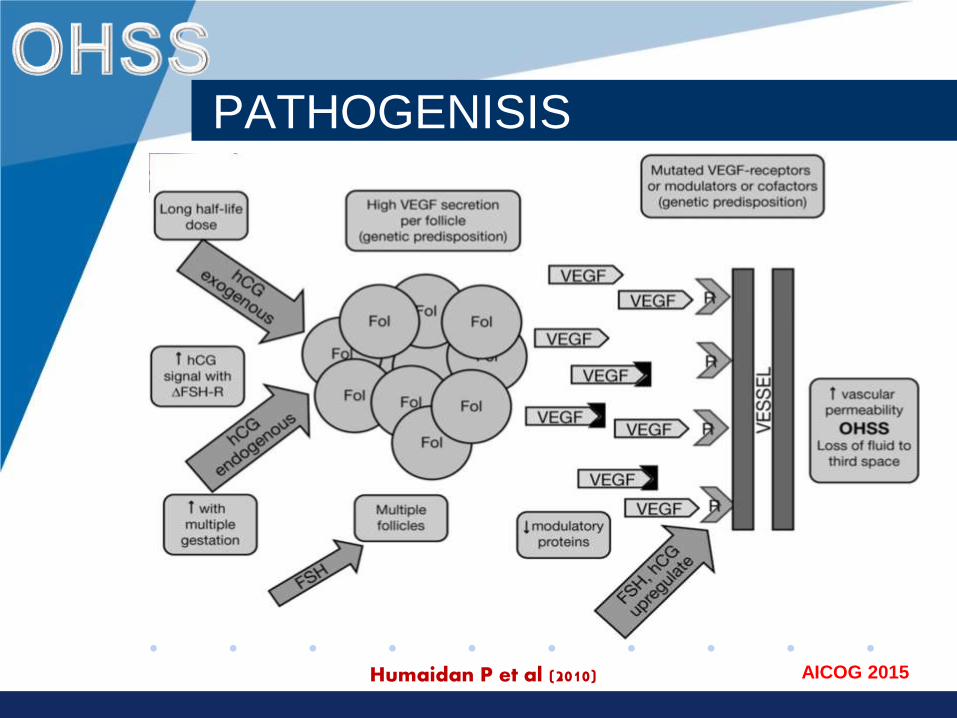
AICOG 2015Humaidan P et al (2010)
PATHOGENISIS
www.company.com
AICOG 2015
•Vascular endothelial growth factor (VGEF)is the main mediator of these exaggerated response.
•Secondary mediators include renin -
angiotensin system and platelet‐derived factors.
•Associated increased capillary permeability leads to ASCITES, Pleural /Pericardial effusions.
•Ovarian enlargement may lead to torsion or cyst rupture.
www.company.com
AICOG 2015
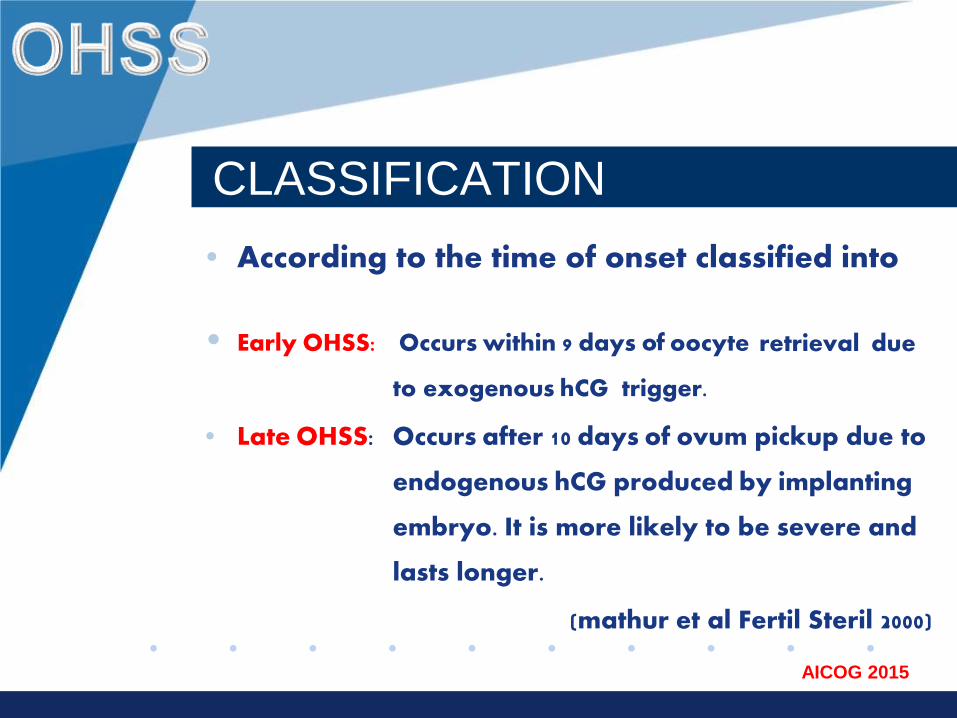
CLASSIFICATION
• According to the time of onset classified into
• Early OHSS: Occurs within 9 days of oocyte retrieval due
to exogenous hCG trigger.
• Late OHSS: Occurs after 10 days of ovum pickup due to
endogenous hCG produced by implanting
embryo. It is more likely to be severe and
lasts longer.
(mathur et al Fertil Steril 2000)
www.company.com
AICOG 2015
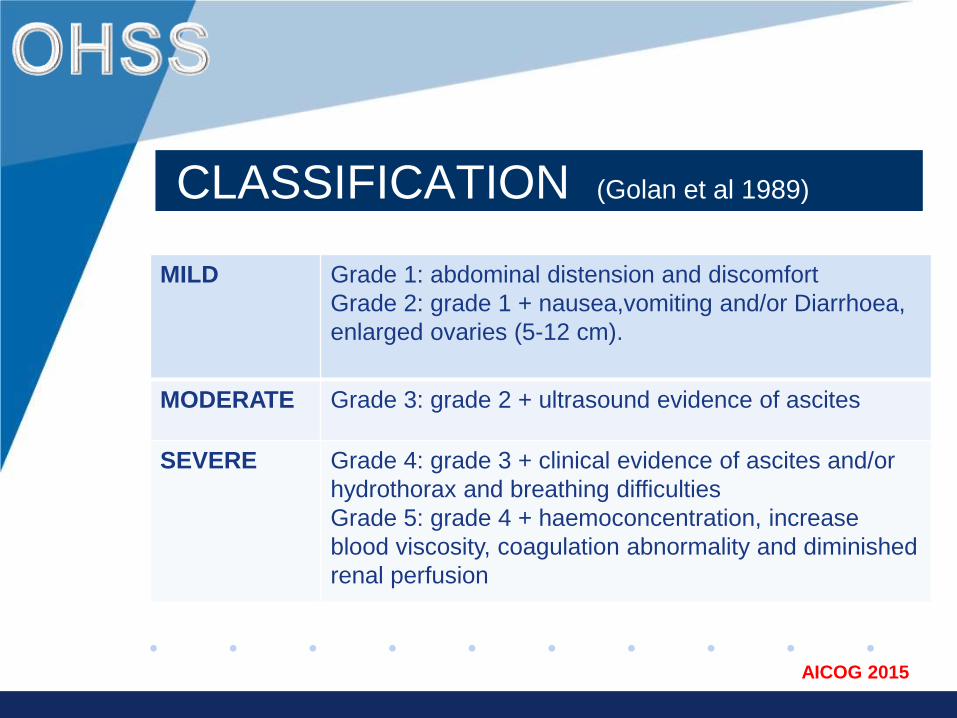
CLASSIFICATION (Golan et al 1989)
MILD Grade 1: abdominal distension and discomfort
Grade 2: grade 1 + nausea,vomiting and/or Diarrhoea,
enlarged ovaries (5-12 cm).
MODERATE Grade 3: grade 2 + ultrasound evidence of ascites
SEVERE Grade 4: grade 3 + clinical evidence of ascites and/or
hydrothorax and breathing difficulties
Grade 5: grade 4 + haemoconcentration, increase
blood viscosity, coagulation abnormality and diminished
renal perfusion
www.company.com
AICOG 2015
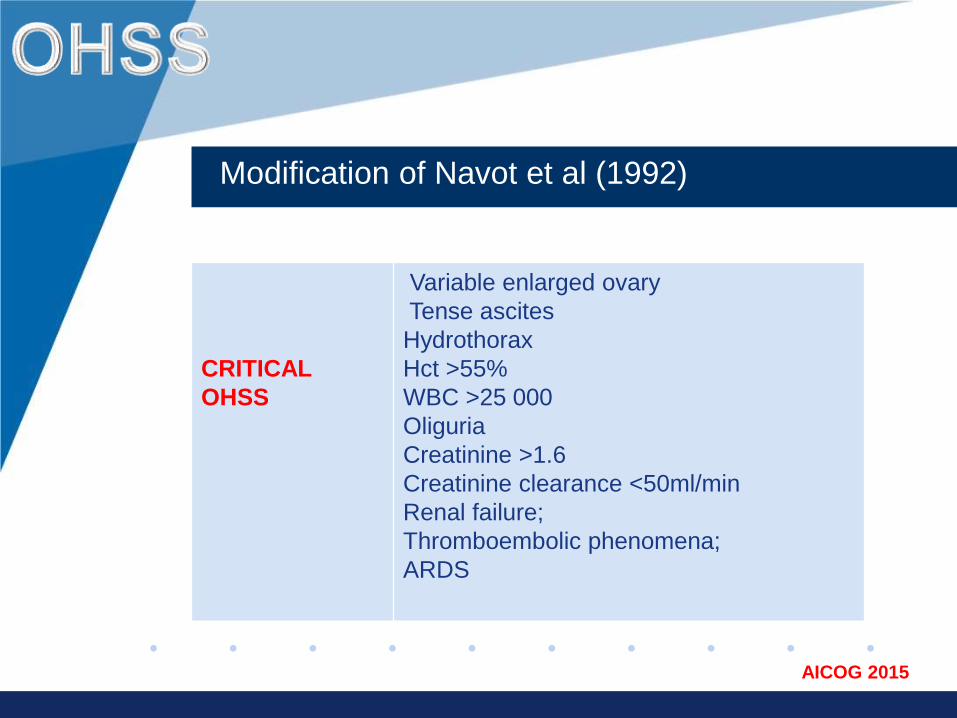
Modification of Navot et al (1992)
CRITICAL
OHSS
Variable enlarged ovary
Tense ascites
Hydrothorax
Hct >55%
WBC >25 000
Oliguria
Creatinine >1.6
Creatinine clearance <50ml/min
Renal failure;
Thromboembolic phenomena;
ARDS
www.company.com
AICOG 2015
MANAGEMENT
• PREDICTION
• PREVENTION
– Primary
– Secondary
• POST - OHSS MANAGEMENT
www.company.com
AICOG 2015
PREDICTION
• Young patients • Lean women• Polycystic Ovarian syndrome• Previous OHSS• Increased antral follicular count (> 10 per ovary)• Increased anti mullerian hormone levels (>3.3
ng/ml)• High or rapidly rising E2 levels (> E2 5,000 pg/ml)• High number of follicles (≥18)
www.company.com
AICOG 2015
PRIMARY PREVENTION
• Insulin- Sensitizing agents
• Reducing dose of gonadotropins
• GnRH antagonists protocols• Low dose of hCG /r hcg/r LH• Alternative agents to hcg
• Avoiding hCG for Luteal support
• In vitro oocyte maturation (IVM)
www.company.com
AICOG 2015
INSULIN SENSITIZERS
• Metformin suppresses insulin levels &decreases ovarian androgen production with improved ovulatory rates.
• Metformin treatment before or during ART cycles decreased the risk of OHSS in PCOS women.
(Cochrane Database of Systematic Reviews 2014)
www.company.com
AICOG 2015
REDUCED GONADOTROPHIN
• Chronic low dose step up protocol results in better pregnancy rates with reduced incidence of OHSS compared to high dose regimens in IUI cycles.
• Minimal stimulation / natural cycle IVF.
• Using r FSH instead of urinary FSH have no effect in reducing the incidence of OHSS.
• (Cochrane Database of Systematic Reviews 2011)
www.company.com
AICOG 2015
ANTAGONIST PROTOCOL
• The use of antagonist compared with long GnRH agonist protocols was associated with a large reduction in OHSS and there was no evidence of a difference in live-birth rates.
• The added advantage being possibility of using agonist instead of hcg to trigger final oocyte maturation.
(Cochrane Database of Systematic Reviews 2011)
www.company.com
AICOG 2015
LOW DOSE HCG / R- LH
• The trigger of oocyte maturation with low dose of hCG in high-risk patients reduces the risk of OHSS. (kolibianakis et al 2007,ying et al 2013).
• No evidence of difference between rhCG or rhLH and uhCG in achieving final follicular maturation with equivalent pregnancy rates and OHSS incidence.
(Cochrane Database of Systematic Reviews 2011)
www.company.com
AICOG 2015
GNRH AGONIST TRIGGER
• Use of GnRH agonists instead of HCG for trigger results in a lower incidence of OHSS but extremelyhigh early pregnancy loss due to luteolysis.
• Luteal rescue is still possible with low dose hcg (1500 IU) with comparable pregnancy rates and minimal risk of OHSS. (humaidan et al 2012)
• GnRH agonist could be useful for cryopreservation & and donor/ recipient cycles.
(Cochrane Database of Systematic Reviews 2014)
www.company.com
AICOG 2015
OVAIDING HCG FOR LPS
• Progesterone, hCG or GnRH agonists are used for LPS but use of hCG was linked to significantly higher risk of OHSS.
• Progesterone seems to be the best option as LPS in high risk patients with out the risk of OHSS.
(Cochrane Database of Systematic Reviews 2011)
www.company.com
AICOG 2015
IN VITRO MATURATION
• It is an attractive strategy to prevent OHSS
in PCOS patients. It involves earlier retrieval
of immature oocytes at the germinal-vesiclestage followed by IVM & ICSI
•Though promising data on the IVM technique
have been published, unfortunately there is still
no evidence from RCTs upon which to base any
practice recommendations.
Cochrane Database of Systematic Reviews 2013
www.company.com
AICOG 2015
SECONDARY PREVENTION
•Cycle cancellation•Coasting•Cryopreservation• Intravenous albumin and HES•Dopamine agonists•Calcium gluconate infusion•Luteal phase antagonist
www.company.com
AICOG 2015
CANCELLATION
• Cycle cancellation before administration of hcg is an effective strategy for the prevention of OHSS.
• May be acceptable in an IUI cycle but not in an IVF cycle because of the financial burden and psychological stress to the patient.
www.company.com
AICOG 2015
COASTING
• Coasting involves withholding furthergonadotropin stimulation & delaying hCGadministration until E2 levels plateau ordecrease significantly
• There was no evidence to suggest a benefit of using coasting to prevent OHSS compared with no coasting or other interventions.
(Cochrane Database of Systematic Reviews 2011)
www.company.com
AICOG 2015
CRYOPRESERVATION
• Cryopreservation involves freezing of all embryos to be thawed & implanted at a later date.
• Early OHSS may occur but it almost eliminates the risk of late OHSS.
• Though reduced pregnancy rates from frozen-thawed embryos was a concern, the introductionof vitrification technique shows promising results.
(CDC Report 2005,Fertil Steril 2008)
www.company.com
AICOG 2015
IV ALBUMIN vs HES
• There is limited evidence of benefit from intra-venous albumin administration at the time of oocyte retrieval in the prevention of severe OHSS.
• Where as Hydroxyethyl starch markedly decreases the incidence of severe OHSS and this is a cheaper, potentially safer alternative to albumin.
(Cochrane Database of Systematic Reviews 2011)
www.company.com
AICOG 2015
DOPAMINE AGONIST
• Cabergoline appears to reduce the risk of OHSS in high-risk women, especially for moderate OHSS. (0.5 mg daily for 8 days post hcg trigger)
• The use of cabergoline does not affect the pregnancy outcome nor is there an increased risk of adverse events.
(Cochrane Database of Systematic Reviews 2012)
www.company.com
AICOG 2015
CA GLUCONATE / ANTAGONIST
• Calcium infusion (10 ml of 10% IV Ca gluconatein 2oo ml saline for 3 days post OPU) can effectively prevent severe OHSS and decreases OHSS occurrence rates. (Naredi &Karunkaran 2013)
• Antagonists 0.25 mg daily from day 5 -8 post OPU with or without embryo transfer causes rapid resolution of early onset severe OHSS. (Lainas et al 2012,2013).
www.company.com
AICOG 2015
RECOMMENDED
• Metformin co‐treatment in PCOS.
• Lower starting dose of FSH
• GnRH antagonist protocol
• GnRH agonist trigger
• Avoiding hCG for luteal support
• Dopamine agonists
• Elective single embryo transfer
• Cryopreservation of all embryos
(Canadian task force 2014)
www.company.com
AICOG 2015
NOT RECOMMENDED
• Intravenous albumin during OPU
• Coasting > 3 days
• Using one type of FSH versus another
• Lowering dose of hCG for final oocyte
maturation
• Using rec LH instead of hCG for trigger
(Canadian task force 2014)
www.company.com
AICOG 2015
MANAGEMENT
• Out patient management is the norm in mild to moderate OHSS.
• Monitor hematological & renal parameters
• USG to asses severity of OHSS
• Adequate oral hydration to prevent haemoconcentration / oliguria
• GNRH antagonist & dopamine agonist to control early OHSS.
www.company.com
AICOG 2015
CRITICAL OHSS
• Multi disciplinary management in a intensive care unit
• Strict fluid & electrolyte management
• Crystalloids & HES for hydration
• IV albumin if required
• Thromboprophylaxsis
• Paracentesis/culdocentesis/pleuracentesisrelieves abdominal tension & dysnoea. It also promotes diuresis & clinical resolution.
www.company.com
AICOG 2015
• Antagonist protocol with agonist trigger and vitrification of all embryos for subsequent transfer in natural / estrogen administered cycles (segmentation of IVF) seems to be the best available option at present to reduce the incidence and severity of OHSS.
• Further research is needed to explore possibilities of fresh embryo transfer to reduce the cost and improve outcome.

www.company.com
AICOG 2015
THANK YOU