onel josc 18 jan 2011 health for north east london update
DESCRIPTION
ONEL JOSC 18 Jan 2011 Health for north east London update. Introduction. Overview and context Joint meeting of JCPCTs decision making - recap Independent Reconfiguration Panel – timeline and implications Priorities/next steps Response to JOSC. H4NEL overview and context. - PowerPoint PPT PresentationTRANSCRIPT

1
ONEL JOSC 18 Jan 2011 Health for north east London update

2
Introduction
• Overview and context• Joint meeting of JCPCTs decision making -
recap• Independent Reconfiguration Panel –
timeline and implications• Priorities/next steps• Response to JOSC
3
H4NEL overview and context
• Programme proposals approved by JCPCT on 15th December 2010 subject to assurances
• Redbridge OSC decided to refer programme to Secretary of State on 4th January 2011 – likely to result in an IRP review
• From 1 April new INEL / ONEL commissioning structures take effect and GP commissioners increased role in line with White Paper.

4
Decisions – urgent and emergency care and maternity
• Reduce from six hospitals with A&E, urgent surgery, inpatient services, critical care and maternity delivery to five
• Provide these services at The Royal London, Queen’s, Whipps Cross, Homerton and Newham
• Enhance urgent care at all hospitals, with better and quicker access to tests, consultants and specialist advice
• Develop ‘campus’ model of maternity care – with new midwifery-led unit at Queen’s.

5
Decisions – vision for King George
• King George to provide urgent care and extended range of walk-in and planned care services, including 24/7 short stay assessment and treatment services for adults and children.
• Planned surgery to move from Queen’s to King George except where there are benefits in co-locating services or clinical need.
• Other services to include: • Antenatal and postnatal care • Diagnostics - e.g. x-ray, ultrasound, ECG, pathology • Child health centre • Outpatient facilities and diagnostic services • Cancer day care (Cedar unit)• Renal (kidney) dialysis • Inpatient and day care rehabilitation services
6
Decisions – children
• Provide more specialist care for children at The Royal London and
Queen’s and improve the services available at other hospitals. • Medical care
• Early senior assessment to reduce admissions and minimise unnecessary lengths of stay.
• Stronger links to be developed between hospital and community-based services.
• Children requiring inpatient care to be under the care of a designated paediatrician, even those admitted to an adult ward.
• Surgical care:
• Where safe and appropriate, surgery on children over six months can take place at any hospital in the sector (all hospitals to meet high standards).
• Transfer children under six months requiring surgery to The Royal London, except for minor ophthalmic surgery (at any hospital), and neonates already at Homerton.
• Transfer children requiring specialist care to The Royal London / improved services at Queen’s or another centre e.g. Great Ormond Street (as now).
7
GP commissioner views
• GP commissioning boards approved the recommendations as the majority of GPs in inner and outer north east London support the vision, although had concerns about how the proposals would be implemented.
• Approvals were made subject to assurances that:
GPs would be involved in developing detailed models, phasing of changes, timing of decisions and care pathways; and signing off ‘system readiness’
8
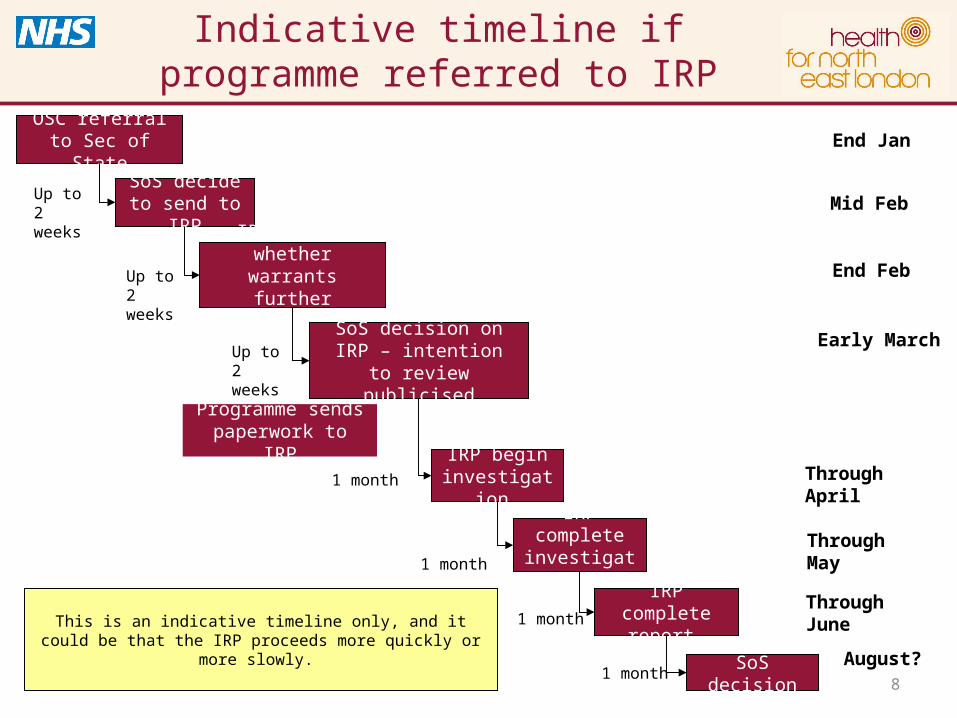
Indicative timeline if programme referred to IRP
OSC referral to Sec of State
SoS decide to send to IRP
End Jan
Up to 2 weeks
IRP decide whether warrants further
investigation Up to 2 weeks
End Feb
SoS decision on IRP – intention to review
publicised
Up to 2 weeks
Programme sends paperwork to IRP
IRP begin investigation 1 month Through April
Through MayIRP complete investigation 1 month
IRP complete report 1 month
SoS decision1 month
Through June
August?
Mid Feb
Early March
This is an indicative timeline only, and it could be that the IRP proceeds more quickly or more slowly.

9
Priorities/next steps
• Developing mechanisms to deliver changes that reflect changing commissioning context leadership role of GPs and partnership working with local authorities
• Establishing gateway assurance process • Implementation planning including
• Developing clinical models further with focus on urgent /emergency care models for KGH & Queen’s and Maternity
• Detailed capital and activity modelling • Develop benefits framework to measure performance and manage
delivery of benefits• Continued communications & engagement with patients, public and
other stakeholders• Continued clinical engagement and relationship with external
scrutiny mechanisms

10
Potential phases of change - Maternity and Newborn Care
Proposal Preliminary thinking re phases of change
Assurances sought
Aims: •to deliver improved outcomes, patient choice and patient experience across the whole maternity pathway. •to increase capacity across the sector to match forecast increases in demand in a way that evens-out activity at Whipps Cross, Newham and Queen’s.
•In addition to phased reconfiguration changes set out here a whole system improvement programme would be put in place to deliver the overall vision for services across the whole maternity pathway.
Phase one •King George Hospital closes to obstetric deliveries •(Co-located MLU developed at Queen’s Hospital, Barking MLU opened)
Phase two •additional capacity at Whipps Cross & Newham - review community midwifery arrangements and pathways.
Phase three •additional capacity at Whipps Cross and Newham - review community midwifery arrangements and pathways.
•Protocols and procedures to support home deliveries and standalone midwifery units.
•Assurance that, before active move to increase births in out of hospital settings:
• Risks related to home deliveries and standalone midwifery units will be mitigated
• Workforce skills and capability within midwifery service will be addressed
•Greater emphasis on role of GPs in maternity care, in particular antenatal care & safeguarding mothers and babies.
•Further consideration of the safety and sustainability of proposed MLUs at Barking & KGH.
•Improvements to maternity capacity and quality at Queen’s and Whipps Cross before changes are implemented.

11
Potential phases of change - Urgent and Emergency Care
Proposal Preliminary thinking re phases of change
Assurances sought
Aim: to deliver improved patient experience and outcomes, with reduced reliance on A&E and inpatient admissions.
A whole system urgent and emergency care pathway improvement programme would run alongside proposed phases of change to deliver desired improvements across the whole pathway.
NB: Changes to the urgent and emergency care pathway at King George Hospital are contingent on capacity release – length of stay improvement and / or reduced admissions as per the planning assumptions set out in activity and capacity chapter and commissioning strategy plans.
Phase one:•overnight closure of A&E, and / or •close to paediatric blue light ambulances and overnight admissions, and / or •all unplanned surgery transfers to Queen’s.
Phase two:•close to blue light ambulances, and/or •all acute admissions streamed via A&E hospitals / acute assessment units ( consultant-led inpatient medical care continues at King George Hospital for post acute phase of care)
Phase three: •All non-elective medical and surgical care consolidated to A&E hospital sites.
• Adequate capacity in primary and community services to manage urgent care needs.
• Strategy for managing A&E demand and a turnaround plan for services provided by BHRUT
• GP out-of-hours services are fully integrated into the 24/7 urgent care model.
• Provision of improved senior clinical cover across specialties
• Clear communications strategy for patients regarding access to urgent care.

12
Potential phases of change - King George Hospital Vision
Proposal Preliminary thinking re phases of change
Assurances sought
Vision for King George Hospital to be further enhanced and embedded in local GP commissioning plans. Further work to extend links to community and mental health services provided by NELFT to be explored.
Phase one:• GP practice relocated / developed
at King George Hospital site (focus on urgent and unplanned primary care and primary care for unregistered patients)
• Urgent care centre and ambulatory emergency care model developed
• Transfer first tranche elective work
• Renal dialysis
Phase two: • Develop child health centre
(relocate CDC and CAMHs) • Develop rehab model and direct
referral pathways for GPs • Second tranche elective work
transferred etc
• Sustained improvement in A&E performance and bed capacity at Queen’s before services are transferred from KGH including:
•Demonstrable progress in reducing admission rates and lengths of stay
•Evidence that the UCC is working effectively.
• Review potential for GP-led admitting beds at King George.
• Local primary care leadership to finalise UCC / short stay assessment service model for KGH.

13
Summary of changes – children & young people
Paediatric Medical care Paediatric Surgical care Assurances sought
• Individualised assessment and treatment of children to ensure care is provided by the service best placed to meet their needs
• Early senior assessment to determine the best treatment - emphasis on reducing admissions and minimising clinically unnecessary lengths of stay.
• Clear protocols for transfer of children with complex conditions from their local hospital to Queen’s / Royal London (when appropriate).
• Stronger links and development of service between hospital and community-based children’s services to facilitate community-based care.
• Children requiring inpatient care under the care of a designated paediatrician, even those admitted to an adult ward.
• The location of paediatric surgery must focus on: age of child; surgical and anaesthetic competencies available; type of surgery and the condition of the child.
• surgery on children over six months of age can take place at any hospital in the sector (though all hospitals must meet agreed high standards), improving outcomes and minimising transfers.
• Transfer children under six months requiring surgery, to RLH, except those requiring minor ophthalmic surgery (at any hospital), and neonates already at Homerton.
• Transfer children who require specialist / high dependency care to RLH or Queen’s or a tertiary centre (such as GOSH), as happens now.
• Proposals will address current workforce challenges, ensuring patients have access to earlier senior clinical review.
• Changes will create sufficient capacity to meet future demand.
• Strong local services retained and minimal number of children transferred out of borough.
• Further work on optimum care pathways, patient flows & community based pathways (esp for young people with LTCs).
• Mechanisms to monitor changes to patient flows incl. peer review & audit.
• BHRUT continue to develop & extend range of local services. Clear referral criteria for children transferring to other trusts
• Adoption of best practice for ambulatory care pathways. Consultant led ‘hot clinics’ should be consistently available.

14
Clinical assurance gateways ~ ‘system readiness’
planningpreparatory
implementationfinal
implementation
Phase of Change - Planning Gateway: signs off detailed plan for implementation of proposed phase of change, reviews interdependencies and agrees ‘whole system
readiness indicators’.
Decision Making Gateway: signs off system readiness for implementation of proposed phase of change, including any final steps preparatory to change.
If required further Gateway/s can be requested prior to full implementation.
Phase of Change ~ implementation complete.
review benefits delivery
Benefits realisation Gateway: are intended benefits being delivered? Are any revisions to model or delivery arrangements required to improve benefits delivery?

15
Responding to JOSC
• Travel• Mental health• Birth registrations

16
Responding to JOSC - travel
We are working with the Travel Advisory Group on the priorities they have identified of:
• Bus routes (esp into Queen’s)• Accessibility of key stations• Car parking• Information on access and travel

17
Responding to JOSC - travel
To date we have: • Identified mechanisms for influencing bus routes• Ascertained that there are firm, funded plans to
improve accessibility of key stations• Discussed aspects of car parking policies that
the group might seek to influence • Commenced baseline assessment of north east
London NHS travel plans

18
Responding to JOSC - travel
Next steps will include: • Supporting local gathering of evidence to submit
regarding bus routes• Seeking to provide the user perspective in planning
accessibility improvements to stations by connecting LINks to this work
• Focusing on how the NHS can provide better information to patients and visitors on travel and access to services
• Support improvement to travel plans to good practice standards
• Full report of activities relating to travel will be provided by TAG including recommendations for future work in March.

19
Responding to JOSC – mental health
The JCPCTs accepted: • The importance of mental health as central to
improving health and wellbeing• That opportunities to improve mental health
would be found in implementation of changes (e.g. in urgent care services
• The need to support GP commissioners to continue with review and transformation of mental health services underway in north east London.
20
Responding to JOSC – mental health
Implementation of Health for north east London will include consideration of mental health needs of people using acute services – the interface issues especially urgent care
It will not focus on improving mental health services for people outside of this group, these improvements will be driven forward by mental health commissioners in emerging commissioning structures, supported across London by CSL work

21
Timeline overview
Begin transfer of birthing from
KGH
Consultation
2009 – Mar 10
Local clinicians develop
proposals
Begin transfer of A&E from
KGH
April – Dec 10
2011 20122013 –
20142008 –
2009
JAN 2011
Analyse consultation
feedback and revise proposals
Barking Birthing centre to open.
Queen’s midwifery-led unit to open
Independent review
Develop detailed plans
Queen’s A&E to be ‘system-ready’