online health promoting communities design, implementation and
TRANSCRIPT

Linköping University Medical Dissertations No. 1321
Online health promoting communities Design, implementation and formative evaluation of an intervention
Joakim Ekberg
Division of Social Medicine and Public Health Science
Department of Medical and Health Sciences
Linköping University, Sweden
Linköping 2012

2
Joakim Ekberg, 2012
Cover illustration: The Opte Project by Barrett Lyon (http://opte.org).
Asia Pacific - Red
Europe/Middle East/Central Asia/Africa - Green
North America - Blue
Latin American and Caribbean - Yellow
RFC1918 IP Addresses - Cyan
Unknown - White
Published articles have been reprinted with the permission of the copyright
holders.
Printed in Sweden by LiU-Tryck, Linköping, Sweden, 2012
ISBN 978-91-7519-827-9
ISSN 0345-0082


4
“Mr. Bell, after careful consideration of your invention,
while it is a very interesting novelty, we have come to
the conclusion that it has no commercial possibilities."
-- J. P. Morgan's comments on behalf of the
officials and engineers of Western Union.



Contents
CONTENTS
ABSTRACT .................................................................................................................. 1
LIST OF PAPERS ........................................................................................................ 3
PREFACE ...................................................................................................................... 5
INTRODUCTION ....................................................................................................... 7
Obesity ................................................................................................................... 7
Childhood obesity ........................................................................................... 9
Previous research ............................................................................................... 10
Web-based interventions ............................................................................. 11
THEORETICAL BACKGROUND ......................................................................... 15
On Design ............................................................................................................ 15
Design methodology .................................................................................... 16
Information systems design ........................................................................ 16
Evaluation of information systems ................................................................ 17
Information system success ......................................................................... 17
Technology acceptance models .................................................................. 19
Convergence of communication and behaviour ...................................... 20
Contents
2
AIM .............................................................................................................................. 23
Specific aims of studies .................................................................................... 23
METHODS ................................................................................................................. 25
Studies I and II ................................................................................................... 26
Data collection ............................................................................................... 27
Data analysis .................................................................................................. 28
Study III ............................................................................................................... 29
Data collection ............................................................................................... 30
Data analysis .................................................................................................. 31
Study IV ............................................................................................................... 32
Case study setting ......................................................................................... 33
Data collection ............................................................................................... 33
Data analysis .................................................................................................. 34
RESULTS .................................................................................................................... 35
Study I .................................................................................................................. 35
Study II ................................................................................................................. 37
Study III ............................................................................................................... 39
Study IV ............................................................................................................... 46
DISCUSSION ............................................................................................................ 51
Relation with previous research ..................................................................... 53
Limitations .......................................................................................................... 55
Relevance for public health practice .............................................................. 57
Future research ................................................................................................... 59
Conclusions ......................................................................................................... 61
ACKNOWLEDGEMENTS ...................................................................................... 63
REFERENCES ............................................................................................................ 65

Abstract
1
ABSTRACT
In Sweden, obesity among children has not yet reached the epidemic
proportions reported from other parts of the world. However, among
adolescents, being overweight and self-consciousness regarding body shape,
diet and exercise influence social, psychological and physical health. Obese
children may be in need of secondary prevention because of adverse effects
related to obesity, but it is less obvious exactly what to prevent in the rest of
the population. General interventions to prevent overweight and obesity are
problematic because of the lack of associations for general application; there is
a need for personalized community-based health promotion. Online
interventions are especially suitable considering the amount of time
adolescents spend online.
This thesis takes a design approach to interventions and describes the design
of an online health promoting community as a path to health promotion
among adolescents. The first two studies use data from the first 15 years of a
1991 cohort living in Östergötland to determine the predictability of obesity
from childhood body mass index and to investigate interventions and
available evidence to suggest appropriate interventions. The next two studies
use these findings to design and formatively evaluate a health promotion
intervention.
In Study I we found reasons for offering population-based interventions
systematically from 5 years of age. It would be worthwhile identifying at an
early age those relatively few children with substantially increased risk of
maintaining obesity in adulthood and offering them interventions; but
interventions must be avoided when they are not necessary. The projections in
Study II indicate that more specified interventions would benefit adolescents
without increasing the costs. In Study III, we found than an online health
promoting community can be designed simply at relatively low cost and can
be negotiated to satisfy both the needs of the user community and public
health goals and service capabilities. In Study IV, a checklist for pre-launch
evaluation of online health promoting communities was developed and the
most important result was the delicate balance between community autonomy
and quality control. Future studies addressing health outcome constructs for
use in online health promoting community evaluations are warranted.

Abstract
2

List of Papers
3
LIST OF PAPERS
The thesis is based on the following papers, which are referred to in the text by
their Roman numerals:
I. Angbratt M, Ekberg J, Walter L, Timpka T: Prediction of obesity from
infancy to adolescence. Acta Paediatr 2012, 100(9):1249–1252.
II. Ekberg J, Angbratt M, Walter L, Nordvall M, Timpka T. History matters:
childhood weight trajectories as a basis for planning community-
based obesity prevention to adolescents. Int J Obes (Lond) 2012,
36(4):524–528.
III. Ekberg J, Timpka T, Angbratt M, Frank L, Norén A, Hedin L, Andersen E,
Gursky EA, Andersson Gäre B: Design of an online health promoting
community: negotiating user community needs with public health
goals and service capabilities. Submitted.
IV. Ekberg J, Gursky EA, Timpka T: Checklist for online health promoting
communities. Submitted.
These papers are printed with permission from the publishers.
The project was approved by the Ethics Committee of Linköping University,
Dnr: 033-600 and Dnr: 478-31.

List of Papers
4

Preface
5
PREFACE
This thesis follows the tradition of social medicine and public health in that a
population is examined and an intervention devised in analogy to a doctor–
patient relationship. I came to the field of social medicine from cognitive
science and found the concept of not only trying to understand behaviours of
cognitive systems but also, based on observation and theory, taking action to
design interventions to prevent disease and promote health exciting and
liberating.
The most prominent observation I have made is that design methodology
harmonizes astoundingly well with intervention design in social medicine and
public health, in that user needs are central and designs are evaluated based
on benefit.
Research is rather difficult, and even though this is my thesis, I have only done
a very small part of the overall efforts described herein. Without mentors in
academia and public health, my work would at best be an overview of the
literature.
I am sincerely grateful and humbled by the warm welcome into social
medicine I have had the pleasure to experience and I look forward to
contributing in years to come, albeit with but a small part, to social medicine
practice.
Joakim Ekberg

Preface
6

Introduction
7
INTRODUCTION
In Sweden, obesity among children has not yet reached the epidemic
proportions reported from other parts of the world1–3. However, among
adolescents, being overweight and self-consciousness regarding body shape,
diet and exercise influence social, psychological and physical health4–6. Obese
children may be in need of secondary prevention because of adverse effects
related to obesity7, but it is less obvious what exactly must be prevented
among the rest of the population. General interventions to prevent
underweight and obesity are problematic because of the lack of associations
for general application4,8; there is a need for personalized community-based
health promotion9. Online interventions are especially suitable considering the
amount of time adolescents spend online10.
OBESITY
Obesity is commonly defined as excessive accumulation of fat in adipose
tissue to the extent that health may be impaired11. In population surveys, body
mass index (BMI, calculated as weight in kilograms divided by the square of
height in meters) or Quetelet’s index, is commonly used as a proxy for body
fat content12. BMI has been shown to have a weak correlation with height and
a strong correlation with body fatness in adults13,14, although this relationship
varies according to body composition and proportions15.
According to a survey conducted in 2009, the prevalence of obesity among
adults in Sweden is 12% (13% in females, 12% in males) measured using a self-
administered questionnaire16,17 (Table 1), and the corresponding prevalence of
overweight is about 33% (27% in females, 41% in males). The prevalence of
obesity has increased nationally over time16–21 (Table 2), however, compared
with the rest of the world, the prevalence in Sweden and in other Nordic
counties such as Denmark22 (11.4%) is modest. The highest prevalence of
obesity in first-world counties is found in the United States23 (35.6%), New
Zealand (26.5%), Canada24 (23.1%), and the United Kingdom25 (22.7%).

Introduction
8
Table 1.Prevalence of adult overweight and adult obesity in Sweden
Overweight* Obese
Female Male Total Female Male Total
Ethic group
Other European countries (ethnic group) .30 .38 .34 .14 .18 .16
Other Nordic countries (ethnic group) .28 .45 .35 .18 .17 .18
Rest of the world (ethnic group) .21 .41 .29 .16 .15 .15
Sweden (ethnic group) .28 .41 .33 .11 .13 .12
Education
Long education .23 .34 .27 .06 .07 .06
Medium education .27 .40 .33 .09 .12 .11
Short education .28 .42 .34 .15 .17 .16
Socioeconomic status
High socioeconomic status .23 .42 .32 .07 .12 .09
Low socioeconomic status .26 .33 .29 .15 .17 .16
Employment
Employed .25 .42 .33 .09 .12 .11
Social servant .31 .32 .32 .25 .38 .29
Student .20 .18 .19 .13 .20 .16
Unemployed .54 .46 .50 .17 .15 .16
*Excluding obesity
According to the World Health Organization (WHO), at least 2.8 million
adults die each year as a result of being overweight or obese. In addition, 44%
of the diabetes burden, 23% of the ischaemic heart disease burden and
between 7% and 41% of certain cancer burdens are attributable to overweight
and obesity (http://www.who.int/mediacentre/factsheets/fs311/en/).

Introduction
9
Table 2.Prevalence of obesity over time in Sweden
Year Obesity (%) Sample
size
Age
(years)
Method and source
2009 12.0 20348 16–84 Self-administered questionnaire16
2000–2001 9.2 22706 16–84 Interviewer-administered questionnaire17
1998–1999 8.1 22698 16–84 Interviewer-administered questionnaire18
1997 7.0 11417 15–100 Self-administered questionnaire19
1996–1997 7.0 3781 16–84 Self-administered questionnaire20
1988–1989 5.4 3402 16–84 Self-administered questionnaire20
1980–1981 5.1 14476 16–84 Physical measurement21
The fundamental cause of obesity and overweight is an energy imbalance
between calories consumed and calories expended. The increase in obesity
globally can be accredited to an increased intake of energy-dense foods that
are high in fat, salt and sugars but low in vitamins, minerals and other
micronutrients in combination with a decrease in physical activity due to the
increasingly sedentary nature of many forms of work, changing modes of
transportation, and increasing urbanization (http://www.who.int/mediacentre/
factsheets/fs311/en/).
Childhood obesity
Childhood obesity is associated with a higher risk of persistent obesity,
premature death and disability in adulthood. But in addition to increased
future risks, obese children experience breathing difficulties, increased risk of
fractures, hypertension, and early markers of cardiovascular disease, insulin
resistance and psychological effects. According to the WHO, the number of
overweight children under the age of 5 years in 2010 is estimated to be over 42
million. However, estimates of childhood obesity are problematic because
BMI, as used to determine obesity, assumes full height.
BMI is not well suited for the purpose of measuring obesity in children during
development and alternate measurements have been used, such as relative
measurements whereby children over the 80th percentile of BMI for their age
and gender are said to be overweight, and children over the 95th percentile are
said to be obese26–28. Because this measurement is relative, a baseline
measurement, the International Obesity Task Force (IOTF) criteria29, was

Introduction
10
introduced to make comparisons possible, based on almost 200 000
individuals; adult BMI values were used to determine corresponding age- and
gender-specific BMI values suitable for children. Using longitudinal BMI data
in adulthood categories as reference, age-specific childhood BMIs have been
identified for classifying children as normal weight, overweight, and obese29,
and later also underweight30. These categories have been reported to have high
specificity but low sensitivity for predicting obesity and metabolic disorders in
young adulthood31.
It is thus an important aspect of working with risk groups that these
individuals are not considered to be diseased but at risk, and that
epidemiological findings do not necessarily hold for all individuals. The age-
specific childhood BMI value for obesity is not obesity as such, but is
nevertheless sometimes carelessly regarded as childhood obesity. When
talking about children classified as overweight, this problem becomes even
more entangled. A child classified as overweight according to the age- and
sex-adjusted childhood BMI criteria29 is thus at risk of being overweight in
adulthood, which in turn is considered a risk factor for obesity.
PREVIOUS RESEARCH
The irregular distribution of obesity within and between countries
demonstrates that lifestyle and social determinants have a significant influence
on the prevalence of obesity. The relative impact of the determinants is
unclear, but unhealthy diet, lack of exercise and a sedentary lifestyle have
frequently been put forth as factors32. One influential approach to lifestyle
changes has been various modes of providing information33. The purpose of
such interventions has been to increase awareness and knowledge, modify
attitudes and, as a result, alter behaviour34.
Community interventions follow five fundamental steps34. In the first step, a
community analysis to determine the assets, capacity and history of a local
community is performed. Analysis is the critical first step in shaping the
design of campaign interventions, and it is important to involve members of
the community at this stage. This provides the basis for an informed approach
to the second step, to design and initiate a campaign. A group of citizens and
professionals make preliminary decisions about objectives and interventions.

Introduction
11
The third step of implementation involves transforming the ideas into action,
with feedback and monitoring. The fourth step involves refining the
programme by reviewing the successes and problems. In the fifth step,
dissemination and durability, information on the project results and plans for
the sustainability of the projects are clearly communicated.
Web-based interventions
Recently, some health care services have moved from traditional health care
settings into Internet-based forums35–37, patient-governed Internet information
sites38, and support groups for disease self-management39. The well-
documented practice of computer-assisted therapy40 has moved from
dedicated workstations to the Internet, which has increased its availability and
lowered the demands on resources41.
There is now evidence that computer-based interventions outperform
traditional media regarding physical activity among adolescents42,43, but there
are also other studies that show no such difference44. In a recent review of
computer- and web-based interventions to increase psychical activity among
adolescents, most interventions resulted in a significant increase in physical
activity, but the findings were short lived45. Parental support has been shown
to be decisive for physical activity in a complex intervention with computer-
tailored feedback and changes to the school environment46. However, not all
new interactivity is beneficial and there is probably some overconfidence in
the bells and whistles of interactive media, such as interactive games. In a
study where games, quizzes, etc. were compared with traditional information
provision, traditional printed material actually outperformed the interactive
media approach47.
A review by Hamel et al.45 concluded that factors contributing to successful
interventions included conducting interventions at schools and using a theory
or model as framework45. Common theories used in computer- and web-based
interventions include Social Cognitive Theory48, the Transtheoretical Model49,
the Health Belief Model50, the Theory of Planned Behaviour51, and attitude,
social influence, social influence and self-efficacy models52. Previous research
also indicates that parental support is beneficial to the outcome of web-based
interventions53–55. Research on adolescent obesity demonstrates that
overweight adolescents are prone to use web-based interventions, and that

Introduction
12
due to the usually short-lived effects, one-shot interventions with minimal
supervision may not be the optimal solution56.
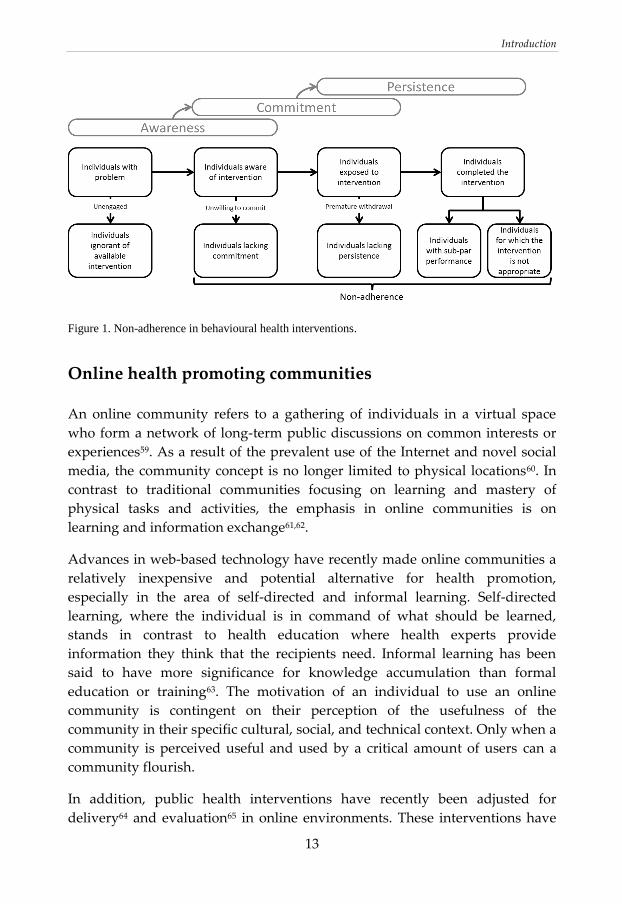
Non-adherence
The cognitive view of behavioural change can be summarized as requiring
that the intended recipients understand that they have a problem and are
aware of available treatment, commit to treatment whereby they are prepared
to perform often uncomfortable actions in divergence with their current
behaviour and beliefs, and persist in follow-up of the treatment when faced
with obstacles and difficulties in the treatment. However, a large proportion of
individuals who commit to behavioural change interventions fail to complete
the treatment for various and mostly unknown reasons57.
Adherence is sometimes defined as the extent to which a patient’s behaviour
on health matters coincides with medical advice58. Non-adherence to
interventions is a persistent and elusive phenomenon in health care and public
health. The refractory nature of this problem has led to the situation whereby
some level of non-adherence has come to be routinely accepted in the planning
of health interventions. Children with obesity and their parents are often fully
aware of the health risk of obesity, the strategies available to reduce weight
and become healthier, as well as the health benefits of reducing weight. Risk
information programs have been plentiful in this area and many children also
have a strong desire to lose weight, but fail to follow-up on the available
interventions. Some are unwilling to commit to lifestyle changes and break
unhealthy habits, and others make efforts but fail to maintain vigilance in their
efforts. Thus, both these groups are in need of support rather than even more
information (Figure 1).
Introduction
13
Figure 1. Non-adherence in behavioural health interventions.
Online health promoting communities
An online community refers to a gathering of individuals in a virtual space
who form a network of long-term public discussions on common interests or
experiences59. As a result of the prevalent use of the Internet and novel social
media, the community concept is no longer limited to physical locations60. In
contrast to traditional communities focusing on learning and mastery of
physical tasks and activities, the emphasis in online communities is on
learning and information exchange61,62.
Advances in web-based technology have recently made online communities a
relatively inexpensive and potential alternative for health promotion,
especially in the area of self-directed and informal learning. Self-directed
learning, where the individual is in command of what should be learned,
stands in contrast to health education where health experts provide
information they think that the recipients need. Informal learning has been
said to have more significance for knowledge accumulation than formal
education or training63. The motivation of an individual to use an online
community is contingent on their perception of the usefulness of the
community in their specific cultural, social, and technical context. Only when a
community is perceived useful and used by a critical amount of users can a
community flourish.
In addition, public health interventions have recently been adjusted for
delivery64 and evaluation65 in online environments. These interventions have

Introduction
14
usually focused on the prevention of specific impairments66,67 and reaching
adolescents and young adults64,68. Web-based disease prevention has matured
into a relatively inexpensive and potential alternative; however, few studies
have been published on web-based health promotion69,70.
The development of open source and easy-to-use content management
systems (CMSs) has made it possible to put a system for an online community
into action with relatively little effort and without the need for specialized
competence in software development and management. Despite the apparent
potential of online health promoting communities, not much guidance is
available for developers on the basic design features characterizing successful
applications. An online health promoting community has the potential to
promote health and advance new means of dialogue between public health
representatives and the general public. However, an online health promoting
community must be managed and even if advances in web-based technologies
simplify the initiation of online communities, management and maintenance
must be sustainable in a responsible manner.

Theoretical background
15
THEORETICAL BACKGROUND
ON DESIGN
Design deals with engineering of tools with a specific purpose in mind71. A
thing, process or action is teleological when it is the means to an end, i.e., a
telos or final cause. In science, teleological explanations are deliberately
avoided since the Novum Organum of Francis Bacon72, because whether they
are true or false is argued to be beyond the ability of human capacity to judge.
Whereas the natural sciences are void of teleological components, or at least
expected to be, the artificial world makes no sense without purpose. Purpose
is both the explanation of a tool, a tool is made for a specific purpose, and the
measurement to which a tool is evaluated. Specifically, the design of a tool is
the method by which to make something fulfil a specific purpose, and a tool is
successful only when it can be shown to fulfil the purpose for which it is
designed. Whereas natural science deals with hypotheses and theories in
which phenomena are explained and outcomes predicted, design deals with
tools and systems, where implementations are evaluated (Table 3).
Table 3.Differences between natural science and science of the artificial
Natural science Design
Study setting Phenomenon Problem
Deliverables Hypotheses and theories Tools and systems
Test Prediction Evaluation
Judgment True/false Good/bad
The context in which a tool is going to be used is of paramount importance,
not just because the tool is designed for a specific context but also because the
introduction of a new solution to a problem will alter the problem for which
the solution is designed73. This alteration is in part deliberate, referred to as
canonical performances, but also in part unexpected, referred to as exceptional
performances74. The alteration of context is sometimes referred to as task and
system tailoring where the use of a new solution is adopted75,76. The study of
canonical and exceptional performances has led to discoveries of often serious
misfortunes when introducing new tools, and has led to increased

Theoretical background
16
consideration for exceptional performances detrimental to the context in
which they are to be implemented77.
Design methodology
Design methodology is an interdisciplinary field involving research from
architecture, engineering and industrial design and was consolidated as a
scientific topic half a century ago78. Design methodology governs methods to
design or adjust systems in order to satisfy some desired need, whether it is a
bench to rest upon when rest is needed, an information system to store
massive epidemiological data when data needs to be securely stored, or a
computer program to compile reports when reports need to be produced.
Originally, design methodology was seen as pure engineering and problem
solving, but later evolved into a more creative field.
The term design is used extensively in everyday language and it is easy to
confuse and misunderstand what design denotes in the absence of a very
specific context. One central concept of design methodology is to separate its
construction on the one hand and the services it is supposed to provide and its
place in an organization on the other. Even though “to design” colloquially is
used to denote the actual construction of something, this is contrary to what
design denotes in design methodology. Design is rather the process of
determining what should be constructed.
Information systems design
The activity of design is to identify needs, establish requirements, develop
alternative solutions, build prototypes and evaluate competing solutions. This
means that during the process, the design will evolve based on repeated
evaluations of an iteratively adapted specification. This process is theoretically
without solution, only resolution, since new users and changes within the user
group context will change over time, also by the design (re)solution itself73. A
pragmatic solution to this process in software development is to release and
even sell an unpolished implementation. This has been made possible with the
advent of the Internet through patches and upgrades after release; for
example, the numerous updates in operating systems such as Microsoft

Theoretical background
17
Windows® and Mac OS® and programs such as Microsoft Office® and
iTunes®. This reflects back to the inherent “wickedness” of design problems,
that the solution and the problem are essentially the same; it is thus seemingly
impossible to take a step-by-step approach to design problems73.
EVALUATION OF INFORMATION SYSTEMS
Measurements in evaluation of information systems have varied over time and
between traditions from acceptance79, adoption80, user satisfaction81, system
effectiveness82, information influence83, individual and organizational
impacts84 to just not a failure85. Modern measurements of the success of
information systems stems from two originally rather disparate traditions. On
the one hand, methods and models have been developed from a systems
perspective whereby the measure of success of the implementation of an
information system is done via individual and organizational impact, or net
benefit84,86,87. On the other hand, methods and models have been developed
from a cognitive perspective to understand the use behaviour, and to measure
the success of an information system via use and user satisfaction88,89. Even
though use and user satisfaction is central in modern design evaluation, it has
been argued that user satisfaction alone cannot fully measure information
system success87.
Information system success
Evaluation of the success of the information systems in DeLone and McLean’s
model84,86 stems from the communication model of Shannon and Weaver82,90
and the information influence theory of Mason83. Much information system
management research, model validation, and model extensions have been
done since DeLone and McLean originally presented their model, especially
regarding the nature of use and the different levels of impact, and the
complications of having a model with the characteristics of both a process
model and a causal model87. The updated model presented in 200387 is both
simpler and more complex. It adds service quality to the two original system
characteristics and combines the two impact variables into one: net benefit
(Figure 2).

Theoretical background
18
Figure 2. Information systems success model86,87
.
The information system success model proposes that a system can be
evaluated in terms of information, system and service quality; these
characteristics affect the subsequent use or intention to use and user
satisfaction. As a result of using the system, certain benefits will be achieved.
The net benefits will (positively or negatively) influence user satisfaction and
the further use of the information system (Table 4). However, DeLone and
McLean stress the importance of context when using their model and
encourage adoption of variables from their general model to suit the context
for which the model is going to be used87.

Theoretical background
19
Table 4.Variables in the information system success model86,87
Variable Description
System quality The accuracy and efficiency of the communication system that produces
information
Information
quality
The success of the information in conveying the intended meaning
Service quality Tangibility, reliability, responsiveness, assurance/trust and empathy/benevolence
of the provided service
Intention to
use/use
Either an attitude variable (intention to use) or a behavioural variable (use)
User satisfaction User rating or feedback of the information system
Net benefit Context sensitive measure of the users net benefit depending on the aim of the
information system
Technology acceptance models
In contrast to the communication effectiveness approach82 in information
system success84, another tradition of information system evaluation stems
from a more user-centred approach, based on research in social psychology.
The technology acceptance model developed by Davis88 initially incorporated
the theory of reasoned action developed by Fishbein and Ajzen91 to explain
computer use behaviour. Fishbein and Ajzen’s theory has been used as the
basis for several information technology acceptance models92 and is based on
attitude and intention, and assumes that behaviour is determined by intention
to perform the behaviour91.
Ajzen later extended the theory of reasoned action to the theory of planned
behaviour to better address behaviours not completely in the user’s control by
adding the construct subjective norm51,93. Theory of planned behaviour has
been used extensively in the health care context and assuming that intention
predicts behaviour can be used to predict behaviour (Figure 3). Due to the
observation that even if people have the intention of carrying out an action,
the actual action is thwarted because they lack confidence or control over
behaviour, the theory of planned behaviour takes into account self-efficacy,
influenced by the social cognitive theory of Bandura94.

Theoretical background
20
Figure 3. The theory of planned behaviour51
.
Venkatesh and Davis51 later extended the technology acceptance model to
explain perceived usefulness and usage intentions and replaced the theory of
reasoned action with the more recent the theory of planned behaviour. The
extended model was tested in both voluntary and mandatory settings,
strongly supporting the extended model89. In an attempt to integrate the main
competing user acceptance models, Venkatesh et al.92 later formulated the
unified theory of acceptance and use of technology. This model was found to
outperform all individual models.
Convergence of communication and behaviour
Even though the two traditions have different starting points, effectiveness
based on communication theory and user satisfaction based on social
psychology both have merits. It certainly seems odd to equate satisfaction with
success of an information system because it fails to cover the task for which
the system is designed to improve. However, user satisfaction is a
fundamental component of success by proxy, because it is hard to imagine
satisfaction with a system that fails to deliver, and perceived usefulness and
ease of use are sensible measurements of user satisfaction (Table 5).

Theoretical background
21
Table 5.Two tradition of information system evaluation
Tradition System success User behaviour
Model Information system success Technology acceptance model
Area Communication Behaviour
Theoretical framework information influence theory theory of planned behaviour
Focus Effectiveness Usage
Activity Information system design Interaction design
Both traditions have been criticized, but they have been evaluated, adjusted
and refined more than any other model of information system usage and
success. A modern synthesis for design and evaluation of information system
success and usage can be said to rest on two traditions that complement each
other in terms of understanding the use and benefit of information systems
(Figure 4).
Figure 4.Author interpretation of the development of two converging traditions. Lines denote
developmental directions and dashed lines denote shared concepts and theories.

22

Aims
23
AIM
The overall aim of this study was to design, implement, and formatively
evaluate tools for use in a community-based health promoting intervention for
adolescents.
SPECIFIC AIMS OF STUDIES
To determine whether estimating body mass using only weight and
height data is associated with the corresponding estimate at the age of
15 years (Study I).
To use epidemiological data and a standardized economic model to
compare projected costs for obesity prevention in late adolescence
accrued using a cross-sectional weight classification for selecting
adolescents at age 15 years compared with a longitudinal classification
(Study II).
To examine what aspects of the structure and functions of an online
health promoting community are critical to satisfy the needs of the user
community and public health goals and service capabilities (Study III).
To develop a checklist for a pre-launch evaluation of online health
promoting communities. The checklist is required to take the
perspectives of both the user community and the health services into
account (Study IV).

24
Methods
25
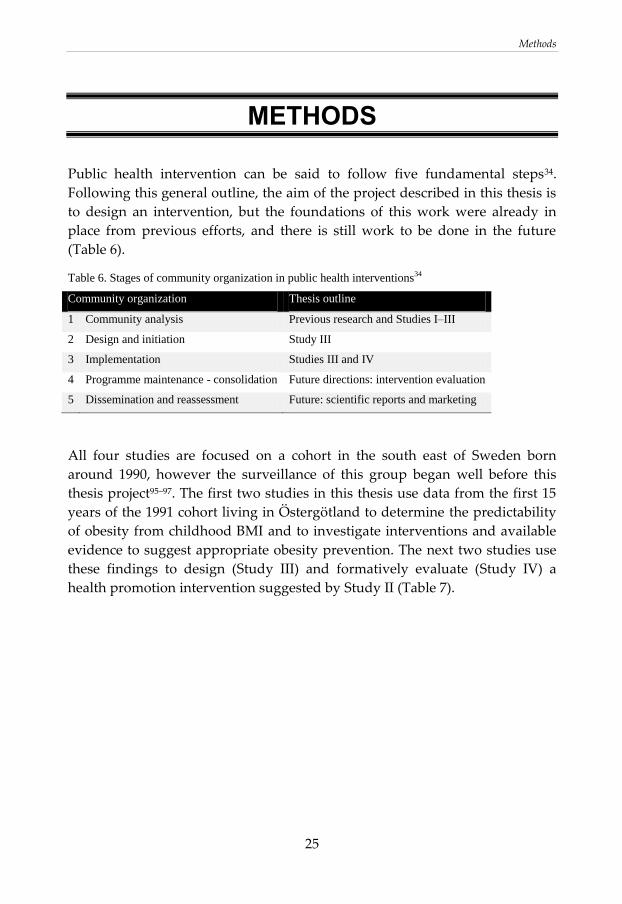
METHODS
Public health intervention can be said to follow five fundamental steps34.
Following this general outline, the aim of the project described in this thesis is
to design an intervention, but the foundations of this work were already in
place from previous efforts, and there is still work to be done in the future
(Table 6).
Table 6. Stages of community organization in public health interventions34
Community organization Thesis outline
1 Community analysis Previous research and Studies I–III
2 Design and initiation Study III
3 Implementation Studies III and IV
4 Programme maintenance - consolidation Future directions: intervention evaluation
5 Dissemination and reassessment Future: scientific reports and marketing
All four studies are focused on a cohort in the south east of Sweden born
around 1990, however the surveillance of this group began well before this
thesis project95–97. The first two studies in this thesis use data from the first 15
years of the 1991 cohort living in Östergötland to determine the predictability
of obesity from childhood BMI and to investigate interventions and available
evidence to suggest appropriate obesity prevention. The next two studies use
these findings to design (Study III) and formatively evaluate (Study IV) a
health promotion intervention suggested by Study II (Table 7).

Methods
26
Table 7.The four studies of the thesis
Study I Study II Study III Study IV
Method Epidemiological study Community-
based
participatory
research
Action research
Subjects All children born in 1991 participated in regular
measurements of weight and height at well-child
health centres and school health care assessments
in Östergötland County
Convenience sample of adolescents
born around 1991 from three
municipalities in the south east of
Sweden
Data Longitudinal
epidemiological data
Weight classification
trajectories
Focus groups
and participatory
design processes
The development
of an online health
promoting
community
Result Timing of interventions
based on saturation of
weight classification
Projection of cost for
obesity prevention in
late adolescence
An online health
promotion
community
Checklist for
online health
promoting
communities
STUDIES I AND II
The study cohort includes all children who participated in regular
measurements of weight and height at well-child health centres and school
health care assessments in Östergötland. Children for whom complete
measurements were available at all seven time points were included in Study
I, and all children for whom complete measurements at age 5, 10 and 15 years
were available were included in Study II (Figure 5).

Methods
27
Figure 5.Flowchart for Studies I and II.
Data collection
Data on weight and height were gathered from the children’s well-child health
centre records at birth and at age 1.5 years, 2.5 years and 5 years. Thereafter,
weight and height data were gathered from the school health service records
at 7, 10 and 15 years of age. At the 72 senior level schools in the county, the
registration of weight and height took place either in grade 8 or 9 (at age 14–
15 years).
In Study II, the children for whom complete measurements at age 5, 10 and 15
years were available were categorized into cross-sectional weight classes and
longitudinal weight trajectory groups when they were 15 years of age. The
cross-sectional and trajectory-based selection strategies for different
interventions were compared using the cost of service as the end point
measure.
For administrative reasons, schools in the county recorded weight and height
at different semesters, which influenced the exact measurement age (Table 8).

Methods
28
Reasons for missing data included incomplete health records, children moving
out of the county in their first 15 years, individuals declining to participate,
individuals with physical or mental disorders excluded by choice of their
school, and individuals with protected identity.
Table 8.Study cohort for Studies I and II
Study II
Expected
age
5 10 15
Girls Boys Girls Boys Girls Boys
Median 5.2 5.2 10.5 10.5 14.5 14.5
n 2059 2253 2059 2253 2059 2253
Study I
Expected
age
1.5 2.5 5 7 10 15
Girls Boys Girls Boys Girls Boys Girls Boys Girls Boys Girls Boys
Median 1.5 1.5 2.5 2.5 5.2 5.1 7.3 7.3 10.5 10.5 14.5 14.5
n 1718 1861 1718 1861 1718 1861 1718 1861 1718 1861 1718 1861
Data analysis
The ponderal index (PI) was used as the measure of body mass for each child
and set of measurements from birth to 1.5 years of age. The BMI was
calculated from 2.5 to 15 years. Overweight and obesity were defined
according to the recommendations of the International Obesity Task Force29.
From 2.5 years of age, the BMI values were also categorized into age- and
gender-adjusted classes29.
Correlations between the BMI recorded from birth to age 10 (at age 0, 1.5, 2.5,
5, 7, and 10 years) and the BMI at 15 years of age were computed pairwise.
Measurements of BMI, weight and height within the same subject are prone to
be correlated to some degree. To determine when this progression exhibited
saturation, statistical tests were performed using as the null hypothesis that
the correlation (r) between the measurements at specific ages and the
corresponding measurement at age 15 years was equal or less than limit values
suggested by the Cohen Scale98. This scale denotes a correlation of 0.5–1.0 as

Methods
29
large/strong, a correlation of 0.3–0.5 as moderate and a correlation of 0.1–0.3 as
small.
The cross-sectional selection strategy in Study II was based on the
organizational routines in the study county at the time of the final data
collection (2006–2007). The alternative trajectory-based selection strategy was
combined with weight–history sensitive interventions at four levels according
to the estimated risk for persistent obesity.
The children were classified into one of 9 trajectory groups according to their
history of weight classifications, and each trajectory was allocated to a
program level.
STUDY III
In Study II, the matching of obesity epidemiology with available interventions
in the region, situated in the south east of Sweden, indicated that the demand
for obesity prevention among adolescents was greater than the resources
available. Our projections indicated that obese adolescents would benefit from
more specialized interventions, but that there was also a need for an online
public health intervention.
Qualitative data from adolescents on health appraisals and perspectives on
health information were collected in a Swedish health service region. Using a
three-step analysis, the data were transformed to specify the structure and
functions of an online health promoting community intervention (Figure 6). In
the first step, the crude data were analysed and structured into health
information needs. The identified needs were then transformed into
requirements for an online health promoting community intervention by an
interdisciplinary expert team. In this context, needs refer to problems
expressed that warrant a solution; requirements are associated with the design
of an information system78. In the third step, a prototype based on the user-
derived requirements was compared with regional public health goals and
service capabilities by public health official representatives from the region,
and modified accordingly.

Methods
30
Figure 6. A three-step analysis to specify the structure and functions of an online health promoting
community intervention.
Data collection
The model population for the development of the online health promoting
community intervention consisted of high school students in their senior year.
For the design, a convenience sample (n=65) representing the population of
adolescents aged 15–20 years (n≈50 000) in the study region was used.
Qualitative data were collected using two sets of focus group interviews. The
topics for the first set of interviews were physical health, psychological health,
and health products; the second set of interviews covered health information
in the media, information needs and information-seeking behaviour. The
protocol for the focus group sessions is provided in Additional file 1 of Study
III. Focus group interview sessions were arranged with adolescents according
to two criteria: home community sociocultural profile (industrial–
technological, small business–church dominated, small business–agricultural)

Methods
31
and high school program profile (high school program in science, arts or
nursing). High schools corresponding to the listed program profiles in each
study community were contacted and asked for assistance with recruiting
students for focus group meetings. Initially, each student was asked to
participate in both focus groups but some cancellations occurred and stand-ins
were accepted. Of the 65 participating adolescents, 48 participated in both sets
of focus group interviews, 12 only in the first, and 5 only in the second. In total
18 focus group sessions took place.
Data from the focus groups were collected over a 2-month period in 2010. The
focus groups were video recorded and lasted for approximately 90 minutes for
the first occasion and 60 minutes for the second. In total, approximately 20
hours of video were collected. Two moderators were present at each focus
group: one moderating the discussion and the other making observations. The
data were collected by means of formal natural group discussion defined as a
group interview with invited people who already know each other99. The
resulting requirements and various prototypes were demonstrated and
discussed with representatives from regional public health services in
meetings and telephone conferences.
Data analysis
Needs
An analysis of health information exchange needs was performed using data
from the focus group meetings. Summaries from each focus group were
compiled as transcripts from the video recordings by one of the moderators
and sent to the second moderator of the focus group to make sure that the
summary was accurate. The transcribed content was coded based on themes
identified in the material by the first moderator.
Statements from the focus groups related to health information exchange were
identified and a summative content analysis of these units was performed to
identify specific user needs as related to an information system. In addition,
statements regarding content and topics of interest were used to assist in
drafting the content for the information system.

Methods
32
Requirements
A process to determine the user-derived system requirements was undertaken
based on the principles of design space analysis100,101 with design rationales
captured using an informal representation102. A design team consisting of two
computer scientists, an interaction designer, and a cognitive scientist drafted
the requirements for an online health promoting community based on the
health information exchange needs identified. The design decisions were then
constructed into a composite design rationale. A design rationale is an explicit
list of decisions made during a design process, and the reasons why those
decisions were made103. The design rationale primarily consisted of the
identified user needs, the user-derived requirements, technical and
organizational system solutions, alternative solutions, and the reason for their
rejection when applicable. The design rationale was also presented as a
prototype online health promoting community.
Policy goals and service capability
In the final step, the design rationale document and prototype were presented
to a panel of public health professionals representing the health service
providers in the region. The task presented to the panel was to assess the
prototype with regard to the regional public health goals and service
capability for an online health promoting intervention. Design solutions were
reviewed in sessions at which the expected positive and negative
consequences of each design solution were examined in light of its
hypothetical implementation in the study setting. When conflicts between
requirements, public health goals, and service capabilities were found, the
solutions were adjusted in order to neutralize the conflicts. These adaptations
were compiled, analysed for common features, and documented.
STUDY IV
Study IV was based on an action research design. Action research balances
problem-solving actions implemented in a context with analysis to understand
underlying causes104. In Study IV, the researchers participated as agents in the
development process and as observers of the same process. A prototype

Methods
33
checklist was developed from the literature on information system success and
applied for formative evaluation in a case study implementation of an online
health promoting community. The problem-solving actions in this process
were documented and analysed using qualitative methods.
Case study setting
The county in this case study (total population 420 000) is situated in the south
east of Sweden. To counteract the development of obesity among young
adults, a need for health promotion among this age group was identified in
the health policy for the county in Study II. On this initiative, public health
practitioners and researchers set out to develop a public health intervention
aimed at adolescents. A needs analysis was performed using data from focus
group interviews with adolescents in the region moderated by a researcher
together with one local public health representative. Following a requirements
analysis performed by an interdisciplinary expert team consisting of two
computer scientists, an interaction designer, and a cognitive scientist and
involving a sample of young adults, a prototype online health promoting
community was drafted using the website content management system
Joomla! (http://www.joomla.org). The resulting online health promoting
community design was demonstrated and discussed in meetings and
telephone conferences with representatives from regional public health
services, public health researchers and senior public health officials, and
adjusted accordingly.
Data collection
Constructs used in the evaluations of information system success were used as
the basis for the formation of a prototype online health promoting community
evaluation checklist. The criteria for concepts to be included in the checklist
were that they were applicable for evaluation of information system success
and available for application before the introduction of the online health
promoting community to the end users. A seminal overview article of the
information system success framework87 and research into information system
success was used as the starting point for assessment of relevant constructs.
An initial set of constructs was established from available and validated
evaluation instruments such as the SERVQUAL instrument105,106, Mirani and

Methods
34
Lederer’s instrument107, the adaptation by Martinsons et al.108 of the Balanced
Scorecard109, and Torkzadeh and Dolls’ instrument for measuring the
individual impact of information systems110, as well as others111–115. Six
preliminary constructs applicable to the success of online health promoting
communities were identified.
Formative evaluation data were collected from a process whereby an adjusted
checklist version was applied to evaluate the online health promoting
community in the case study. The online health promoting community, not yet
introduced to its end users, was assessed by the researchers using each
construct in the checklist. The assessment data were collected from the online
health promoting community requirements and design specifications, field
notes made during meetings with the online health promoting community
development team, and feedback reports from invited users. The specifications
were represented as design rationales whereby the identified user needs were
connected to alternative online health promoting community design solutions
and the rationale behind the design choices made during the implementation,
including why alternative solutions were rejected.
Data analysis
In the first step, constructs were excluded from the baseline checklist based on
the inclusion criteria for the checklist. In the second step, the remaining
constructs were adapted to the online health promoting community context,
forming the study checklist for the formative evaluation. The reasons for each
construct adaptation were recorded by the researchers.
In the third step of the analysis, the data from the formative evaluation of the
checklist were categorized and interpreted by the researchers. The data were
first categorized by the author, and the interpretations thereafter established
by the other two authors of Study IV. Disagreements were resolved by
discussions involving all authors. In the final step, the researchers
consolidated their analysis with the regional public health representatives.
Results
35
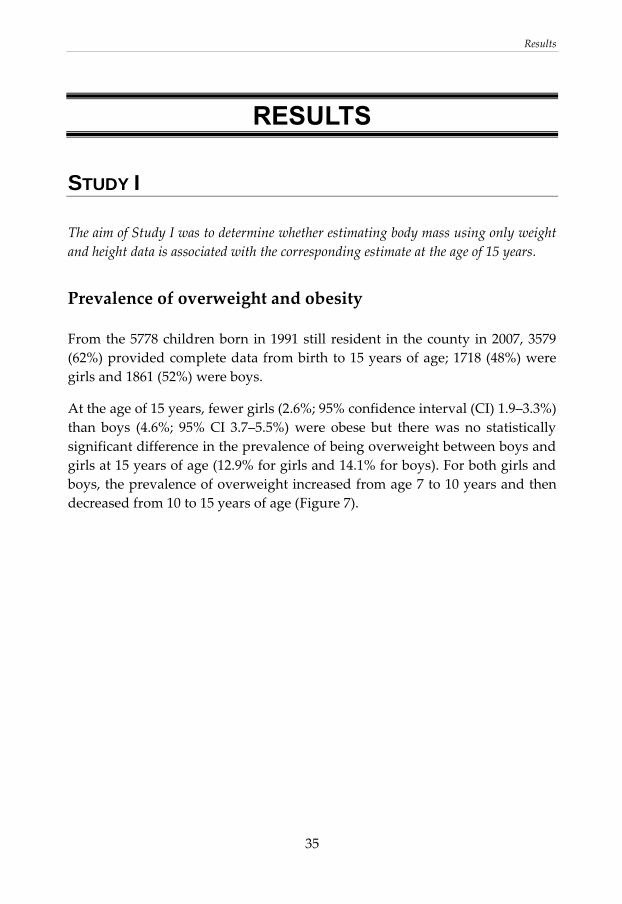
RESULTS
STUDY I
The aim of Study I was to determine whether estimating body mass using only weight
and height data is associated with the corresponding estimate at the age of 15 years.
Prevalence of overweight and obesity
From the 5778 children born in 1991 still resident in the county in 2007, 3579
(62%) provided complete data from birth to 15 years of age; 1718 (48%) were
girls and 1861 (52%) were boys.
At the age of 15 years, fewer girls (2.6%; 95% confidence interval (CI) 1.9–3.3%)
than boys (4.6%; 95% CI 3.7–5.5%) were obese but there was no statistically
significant difference in the prevalence of being overweight between boys and
girls at 15 years of age (12.9% for girls and 14.1% for boys). For both girls and
boys, the prevalence of overweight increased from age 7 to 10 years and then
decreased from 10 to 15 years of age (Figure 7).

Results
36
Figure 7.Prevalence of overweight and obesity displayed by age and sex.
Correlations between growth characteristics
The correlation between PI/BMI measurements and BMI at 15 years of age was
strong (significantly higher than r = 0.5) from 5 years of age (Figure 8).
Reviewing the individual data, 23% of the girls and 8% of the boys classified
as obese at 5 years of age were found to be normal weight at the age of 15
years. Only 6% of those who were obese at 5 years of age among both sexes
were of normal weight at the age of 10 years.

Results
37
Figure 8.Correlations between point estimates of PI/BMI at different ages with BMI at 15 years of age.
STUDY II
The aim of Study II was to use epidemiological data and a standardized economic
model to compare projected costs for obesity prevention in late adolescence accrued
using a cross-sectional weight classification for selecting adolescents at age 15 years
compared with a longitudinal classification.
Cross-sectional and trajectory-based classifications
At age 15 years, the study cohort comprised 82.3% normal weight adolescents,
13.8% overweight individuals and 3.8% obese adolescents. Of the 9 weight
trajectories, each trajectory had at least 7 children represented in the 1991
cohort (Table 9).
74.9% of the children were consistently classified as normal weight at age 10
and 15 years, 8.3% of the children were classified as overweight at age 10 and
15 years, and 2.4% of the children were consistently classified as obese at age
10 and 15 years. 4.1% of the children moved from being normal weight to
overweight during the period and 1.4% moved from being non-obese to being
obese.
Results
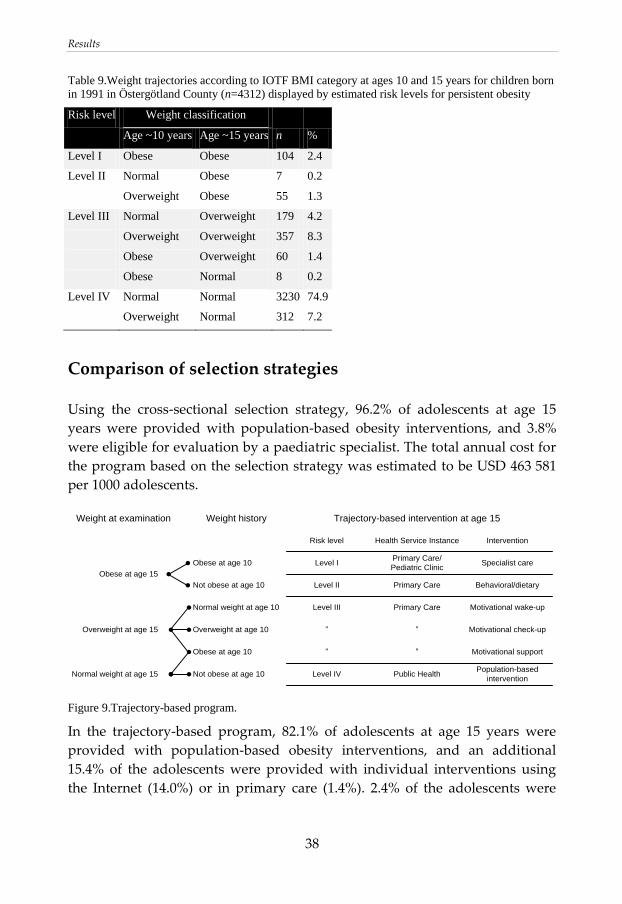
38
Table 9.Weight trajectories according to IOTF BMI category at ages 10 and 15 years for children born
in 1991 in Östergötland County (n=4312) displayed by estimated risk levels for persistent obesity
Risk level Weight classification
n % Age ~10 years Age ~15 years
Level I Obese Obese 104 2.4
Level II Normal Obese 7 0.2
Overweight Obese 55 1.3
Level III Normal Overweight 179 4.2
Overweight Overweight 357 8.3
Obese Overweight 60 1.4
Obese Normal 8 0.2
Level IV Normal Normal 3230 74.9
Overweight Normal 312 7.2
Comparison of selection strategies
Using the cross-sectional selection strategy, 96.2% of adolescents at age 15
years were provided with population-based obesity interventions, and 3.8%
were eligible for evaluation by a paediatric specialist. The total annual cost for
the program based on the selection strategy was estimated to be USD 463 581
per 1000 adolescents.
Weight at examination Weight history
Risk level Health Service Instance Intervention
Normal weight at age 15
Overweight at age 15
Obese at age 15
Not obese at age 10
Normal weight at age 10
Overweight at age 10
Obese at age 10
Obese at age 10
Not obese at age 10
Level IV
Level III
”
”
Level I
Level II
Public Health
Primary Care
”
”
Primary Care/
Pediatric Clinic
Primary Care
Population-based
intervention
Motivational wake-up
Motivational check-up
Motivational support
Specialist care
Behavioral/dietary
Trajectory-based intervention at age 15
Figure 9.Trajectory-based program.
In the trajectory-based program, 82.1% of adolescents at age 15 years were
provided with population-based obesity interventions, and an additional
15.4% of the adolescents were provided with individual interventions using
the Internet (14.0%) or in primary care (1.4%). 2.4% of the adolescents were
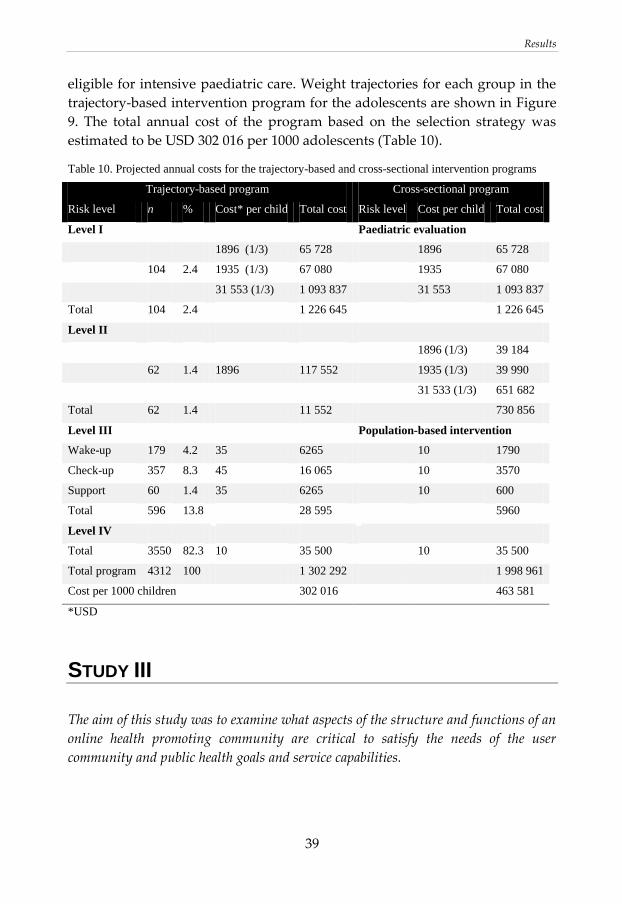
Results
39
eligible for intensive paediatric care. Weight trajectories for each group in the
trajectory-based intervention program for the adolescents are shown in Figure
9. The total annual cost of the program based on the selection strategy was
estimated to be USD 302 016 per 1000 adolescents (Table 10).
Table 10. Projected annual costs for the trajectory-based and cross-sectional intervention programs
Trajectory-based program Cross-sectional program
Risk level n % Cost* per child Total cost Risk level Cost per child Total cost
Level I Paediatric evaluation
1896 (1/3) 65 728 1896 65 728
104 2.4 1935 (1/3) 67 080 1935 67 080
31 553 (1/3) 1 093 837 31 553 1 093 837
Total 104 2.4 1 226 645 1 226 645
Level II
1896 (1/3) 39 184
62 1.4 1896 117 552 1935 (1/3) 39 990
31 533 (1/3) 651 682
Total 62 1.4 11 552 730 856
Level III Population-based intervention
Wake-up 179 4.2 35 6265 10 1790
Check-up 357 8.3 45 16 065 10 3570
Support 60 1.4 35 6265 10 600
Total 596 13.8 28 595 5960
Level IV
Total 3550 82.3 10 35 500 10 35 500
Total program 4312 100 1 302 292 1 998 961
Cost per 1000 children 302 016 463 581
*USD
STUDY III
The aim of this study was to examine what aspects of the structure and functions of an
online health promoting community are critical to satisfy the needs of the user
community and public health goals and service capabilities.

Results
40
Needs
The focus group transcript was divided into 505 statement units related to
health information exchange. These units were classified into ten categories of
user health information exchange needs (Table 11); content-related needs were
excluded. The most prominent content-related statements were about food,
exercise and well-being.

Results
41
Table 11. User health information exchange needs
Focus group context User health
information
exchange need
The adolescents exhibited impressive knowledge and had no shortage of simple
health advice; they rather challenged traditional tenets of diet and exercise, not
because they distrusted health advice, but because they distrusted everything.
They did not lack information, but rather a method to discern the true from the
false. Since almost everything health-related they know of is presented with the
agenda of selling them a product, their rule of thumb was to generally disregard
everything
The experience
should be
educational
Even though the adolescents disregarded information provided by health care
organizations, they did believe that physicians and nurses could provide
genuine useful advice. However, they also wanted a personal comment
regarding their questions, not general advice addressing everyone
Personal advice
from health
professionals
Exploring subjects and seeing the point of view of others in discussion forums
and boards was both appreciated and utilized among the adolescents; however,
they had experienced saturation where the discussion was halted either because
of lack of experts with more knowledge to inject into the discussion, or where a
debate turned sour ending without any means to verify or check the validity of
the claims given by either party
Discussions in
which experts
participate
The adolescents belong to a generation where most of their information sources
are online and funded by ads, and where additional pages, reloads, and links
increase the revenue of the website. It therefore was reported to be both a
tedious and confusing task to access the content sought after
Easy accessible
content
Most health-related information provided online was reported to be both
abstract and general, or specific but provided to sell products. This included
information from governmental sources and information from health care
providers. They reported a lack of information regarding the subjects they cared
about and wanted to know more about
Information about
our interests
Reading about faulty but widely held beliefs was seen as entertaining and
informative, and the adolescents were fully aware that commercial interests
both skewed the facts to push products, and outright lied if they could get away
with it. Having health professionals call this out was reported to be an exciting
prospect
Dismantling of
myths and
misconceptions
Diets and types of exercise were topics that were seen as very difficult to find
useful information. Information from commercial interests was entirely
distrusted, and since both diet and types of exercise are not only a comparison
of efficiency, but also experience, sharing experiences among themselves was
seen as valuable
Be able to share tips
and experiences
The aesthetics of websites was reported to be used as a tool to determine the
underlying agenda, trustworthiness, and target group of the website. In this
process, very attractive sites could be immediately dismissed because it was
apparent that such sites were drafted to push products. A clean, simple,
professional site with a clear manifesto and clear agenda was seen as important
for credibility among the adolescents
Professional and
serious

Results
42
One critique of communication from the scientific community and health care
providers was its reliance on a wall of text. Adolescents are sometimes accused
of lacking attention span and in need of simple accessible short bursts of
information. However, the adolescents reported that they were so overwhelmed
by information that it has become necessary to be able to use heuristics to
determine gold from grit. There was no aversion to in-depth information; rather
there is a need to have very concise and simple introductions
Concise
presentation
Even good communities were reported to be shunned because of bad manners
and uncivil conduct. Moreover, it was emphasized that once a community gets
a certain vibe, it sticks forever
Maintain a civil
discourse
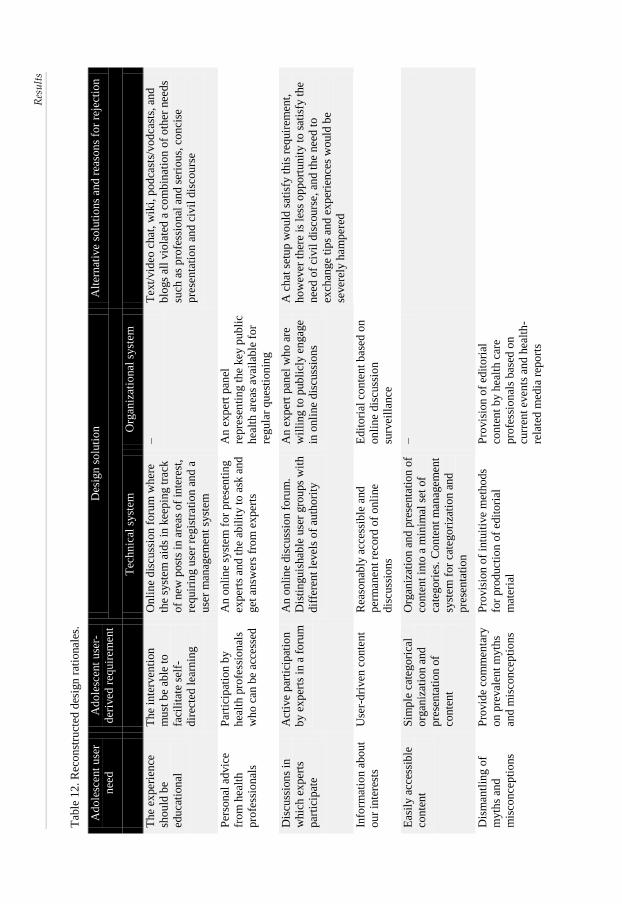
Requirements
The structures and functions identified as requirements to satisfy the
adolescents’ health information exchange needs included both technical and
organizational components. A composite design rationale for the online health
promoting community was completed by linking the identified user needs,
user-derived requirements, and technical and organizational system solutions.
When applicable, alternative solutions and the reason for their rejection were
also listed (Table 12).
Res
ult
s
43
Tab
le 1
2.
Rec
on
stru
cted
des
ign
rat
ional
es.
Ad
ole
scen
t u
ser
nee
d
Ad
ole
scen
t u
ser-
der
ived
req
uir
emen
t
Des
ign
so
luti
on
Alt
ern
ativ
e so
luti
ons
and
rea
son
s fo
r re
ject
ion
Tec
hn
ical
syst
em
Org
aniz
atio
nal
syst
em
Th
e ex
per
ien
ce
sho
uld
be
edu
cati
on
al
Th
e in
terv
enti
on
mu
st b
e ab
le t
o
faci
lita
te s
elf-
dir
ecte
d l
earn
ing
On
lin
e d
iscu
ssio
n f
oru
m w
her
e
the
syst
em a
ids
in k
eep
ing t
rack
of
new
post
s in
are
as o
f in
tere
st,
req
uir
ing u
ser
regis
trat
ion
an
d a
use
r m
anag
emen
t sy
stem
–
Tex
t/vid
eo c
hat
, w
iki,
po
dca
sts/
vo
dca
sts,
an
d
blo
gs
all
vio
late
d a
co
mb
inat
ion
of
oth
er n
eed
s
such
as
pro
fess
ion
al a
nd
ser
iou
s, c
on
cise
pre
sen
tati
on
an
d c
ivil
dis
cou
rse
Per
sonal
ad
vic
e
fro
m h
ealt
h
pro
fess
ion
als
Par
tici
pat
ion
by
hea
lth
pro
fess
ion
als
wh
o c
an b
e ac
cess
ed
An
on
lin
e sy
stem
fo
r p
rese
nti
ng
exp
erts
an
d t
he
abil
ity t
o a
sk a
nd
get
an
swer
s fr
om
ex
per
ts
An
ex
per
t pan
el
rep
rese
nti
ng t
he
key
pu
bli
c
hea
lth
are
as a
vai
lable
fo
r
regu
lar
qu
esti
on
ing
Dis
cuss
ion
s in
wh
ich
ex
per
ts
par
tici
pat
e
Act
ive
par
tici
pat
ion
by e
xp
erts
in a
fo
rum
An
on
lin
e dis
cuss
ion
fo
rum
.
Dis
tin
gu
ishab
le u
ser
gro
ups
wit
h
dif
fere
nt
level
s o
f au
tho
rity
An
ex
per
t pan
el w
ho
are
wil
lin
g t
o p
ub
licl
y e
ngag
e
in o
nli
ne
dis
cuss
ion
s
A c
hat
set
up
wo
uld
sat
isfy
th
is r
equir
emen
t,
ho
wev
er t
her
e is
les
s o
pp
ort
un
ity t
o s
atis
fy t
he
nee
d o
f ci
vil
dis
cou
rse,
an
d t
he
nee
d t
o
exch
ange
tips
and
ex
per
ience
s w
ould
be
sever
ely h
amp
ered
Info
rmat
ion
ab
out
ou
r in
tere
sts
Use
r-d
riven
co
nte
nt
Rea
son
ably
acc
essi
ble
and
per
man
ent
reco
rd o
f o
nli
ne
dis
cuss
ion
s
Ed
itori
al c
on
ten
t b
ased
on
on
lin
e dis
cuss
ion
surv
eill
ance
Eas
ily a
cces
sib
le
con
ten
t
Sim
ple
cat
ego
rica
l
org
aniz
atio
n a
nd
pre
sen
tati
on
of
con
ten
t
Org
aniz
atio
n a
nd
pre
senta
tio
n o
f
con
ten
t in
to a
min
imal
set
of
cate
go
ries
. C
on
ten
t m
anag
emen
t
syst
em f
or
cate
go
riza
tio
n a
nd
pre
sen
tati
on
–
Dis
man
tlin
g o
f
myth
s an
d
mis
con
cep
tio
ns
Pro
vid
e co
mm
enta
ry
on
pre
val
ent
myth
s
and
mis
con
cep
tio
ns
Pro
vis
ion
of
intu
itiv
e m
etho
ds
for
pro
duct
ion
of
edit
ori
al
mat
eria
l
Pro
vis
ion
of
edit
ori
al
con
ten
t b
y h
ealt
h c
are
pro
fess
ion
als
bas
ed o
n
curr
ent
even
ts a
nd
hea
lth
-
rela
ted
med
ia r
epo
rts

Res
ult
s
44
Be
able
to
sh
are
tips
and
exp
erie
nce
s
Pro
vid
e m
ean
s fo
r
use
rs t
o p
ost
co
nte
nt
An
on
lin
e fo
rum
wit
h r
egis
tere
d
use
r id
wit
h s
uit
able
cat
ego
ries
.
A u
ser
regis
trat
ion
an
d
man
agem
ent
syst
em
–
Use
r blo
gs.
Th
e in
tere
st i
n b
loggin
g w
as
asse
ssed
to
be
low
, an
d p
rob
lem
s o
f re
gu
lati
ng
wh
at w
as o
ff-t
op
ic m
ade
this
un
des
irab
le
Pro
fess
ion
al a
nd
seri
ou
s
A c
lean
an
d
min
imal
isti
c la
yo
ut
free
fro
m
com
mer
cial
inte
rest
s
A c
on
ten
t m
anag
emen
t sy
stem
wit
ho
ut
ads.
Des
ign
of
an
app
ropri
ate
layo
ut
Mai
nte
nan
ce o
f la
yo
ut
inte
gri
ty a
nd
co
nte
nt
man
agem
ent
Mai
nte
nan
ce o
f ac
tive
com
mu
nit
ies
wit
ho
ut
a
con
ten
t m
anag
emen
t sy
stem
is
pro
ne
to e
rrors
and
mis
takes
in
up
dat
es a
nd
lay
ou
ts.
A f
ree
and
sim
ple
co
nte
nt
man
agem
ent
syst
em w
ith
exte
nsi
ve
com
mu
nit
y s
up
po
rt d
ram
atic
ally
red
uce
s th
e lo
ad o
f m
ain
tenan
ce
Co
nci
se
pre
sen
tati
on
Co
nfo
rm c
on
ten
t to
blo
ges
qu
e (s
hort
an
d
swee
t) f
orm
at
A s
yst
em t
o p
ost
vid
eos
and
org
aniz
e sh
ort
art
icle
s
Uti
lize
blo
ges
qu
e
new
sfee
d a
nd
sh
ort
vid
eo
inte
rvie
ws
Ed
itori
al w
ork
on
co
nte
nt;
ho
wev
er,
the
wo
rk
load
in
vo
lved
was
dee
med
to
be
hig
h
Mai
nta
in a
civ
il
dis
cou
rse
Vig
ilan
t m
od
erat
ion
Pro
vid
e m
ean
s fo
r m
od
erat
ion
of
dis
cuss
ion
s
En
ou
gh
mo
der
ato
rs t
o
kee
p u
p w
ith o
nli
ne
acti
vit
y
Use
of
stri
ct r
ule
s of
con
duct
to
ed
uca
te u
sers
was
dis
cuss
ed,
bu
t th
ere
wil
l al
way
s b
e ab
use
on
lin
e

Results
45
Public health goals and service capabilities
The assessment of the design rationale document and prototype in light of the
regional public health goals and service capabilities raised concerns about
organizational aspects of the design solutions. No technical aspects of the
design solution were found to be problematic. In brief, compromises were
needed to resolve conflicts involving the management of organizational
resources and responsibilities.
Two conflicts arose about making a health panel available for questions from
adolescents and engaging practitioners in online discussions to meet the
adolescents’ needs (personal advice from health professionals and discussions in
which experts participate). With regard to the resources at hand, monitoring the
potentially vast number of questions and discussions was deemed to be too
high a workload for the practitioners. The compromise found was to use a
previously rejected design solution of using vodcasts. To produce the
vodcasts, it was decided to appoint a community manager to monitor the
discussion, collect questions and hot topics, and regularly interview the
practitioners. A similar problem occurred when the practitioners were
expected to produce editorial content as comments on current health-related
events and media reports to meet the need for dismantling of myths and
misconceptions. Because of the need for special care when producing material
for the public from health services, these editorials were deemed to demand
too much work. The compromise found was to transfer this responsibility to
public health academics because they are more familiar with producing
editorial material, and public communications from them would not be seen to
come from the regional health service.
The fourth conflict was on the choice of online health promoting community
editorial content based on monitoring of online discussions in order to meet
the adolescents’ need for information about our interests. It was speculated that
the editorial content would then be focused exclusively on topics with low
priority in public health policies, e.g. make-up and skincare products.
However, the practitioners were sympathetic to an approach to adapt the
editorial content to adolescents’ interests and a compromise was decided
whereby monitoring was to be accompanied by a clear statement of the
purpose and focus of the online health promoting community.

Results
46
The fifth conflict was about the moderators keeping up with the online activity
if the online health promoting community intervention was used extensively,
regarding the need to maintain a civil discourse. The compromise agreed on
involved recruiting moderators from members of the adolescent user
community based on exemplary conduct.
STUDY IV
The aim of Study IV was to develop a checklist for a pre-launch evaluation of online
health promoting communities. The checklist is to take into account both the user
community and health service perspectives.
The adjusted checklist for pre-launch evaluation of online health promoting
communities included the following constructs: information quality, service
quality and subjective norms (Table 13).
Table 13. Online health promoting community evaluation constructs
Construct - definition Construct evaluation questions
Information quality: Degree to which
information produced by the online health
promoting community has attributes of
content, accuracy, and format required by the
users114
The site provides…
…output that is exactly what you need
…accurate information
…information that is useful
Service quality: Degree to which users’
perceived and expected service align115
Online health promoting community staff give
prompt service to users
Online health promoting community staff have the
knowledge to do their job well
Online health promoting community has users’ best
interest at heart
Subjective norms: Degree to which individuals
perceive that others believe they should use
the website114
People who influence my behaviour think I should
use the site
People who are important to me think I should use
the site
I use the site because of the number of people I know
use it
In the following, each construct and its formative evaluation are reported in
the form of the definition of the construct, contextual adaptation of the
construct, formative evaluation in the case study project, and finally the

Results
47
constructed checklist applicable to both the end-user community and the
health care services. After using the preliminary checklist, some changes in
terms of the actual online health promoting community and in terms of
routines for the editorial work with the online health promoting community
were made (Tables 15–17). The application of the checklist to the study online
health promoting community is provided in Additional file 1 of Paper III.
Information quality
Construct definition: Information quality is defined as the degree to which
information produced by the website has the attributes of content, accuracy,
and format required by the users114.
Contextual adaptation of the construct: Information quality indicates that the
information is relevant and needed by the users with respect to content,
accuracy and format. The content is mainly decided on from the needs of the
users, but this has to be balanced by the purpose of the online health
promoting community from the health service standpoint. Perception of
trustworthiness is important for users, but quality assurance is a more
pressing priority for the health service. The contextual adaptation of the
construct resulted in check points for (1) content area, that the website was
about the right subject area; (2) trust, that the method of developing content
was sound and clearly communicated to the users; and (3) format, that the
content was presented in a way expected by the end users.
Formative evaluation in the case study project: One concern was that the
commitment of the health service to information quality was contingent on the
funding from a research project. For the project to be adapted for routine
practice, the health benefit of the online health promoting community needs to
be demonstrated. The consequence of the health service withdrawing their
commitment is a concern, and is one of the reasons why research projects of
this nature are difficult to carry out responsibly. There is no guarantee for the
user of the website that the service is reliable, which is an important factor for
information system success.

Results
48
Table 14. Information quality checklist
Information
quality
End-user community Health services
Content area Is the content (subject areas and framing)
of the online health promoting community
in sync with the needs of the users?
Is the content (subject areas) of the
online health promoting community in
sync with the intent of the health
service?
Is the framing of the content in sync with
the preferences of the users?
Is the framing of the content in sync with
the intent of the health service?
Trust Is it possible for the users to assess the
accuracy of the content?
Is there a method for quality assurance of
the content?
Is the source of the content clearly
communicated?
Is there an established guideline to
resolve misinformation and conflicting
information?
Is it possible to challenge the accuracy of
the information?
Is the responsibility for the accuracy of
the information clear?
Is there a clear distinction between user-
generated content and authorized content?
Is it clear by what authority, or role,
content is provided from the health
service?
Is there an established method for filtering
relevant content?
Is it possible to overview the extent of
discussions, commentaries and remarks
about content?
Format Is the content presented in formats that are
in sync with the user preferences?
Is the format for the content suitable for
the content provider to work with?
Service quality
Construct definition: Service quality is defined as the degree of alignment
between users’ expected and perceived service experiences115.
Contextual adaptation of the construct: User preferences of service quality are
not uniform, and for the health service, it is important to have sustainable
funding and personnel for the management of the website. The contextual
adaptation of the construct resulted in check points for (1) staff competence,
e.g. that the staff were qualified for the task, and that this was properly
communicated; (2) prompt service, that the health service had the capacity to
manage the online activity; and (3) empathy, that the staffs’ activities online
were unbiased and honest, and that this was communicated properly.
Formative evaluation in the case study project: A concern was raised
regarding having moderators from the community working voluntarily in the
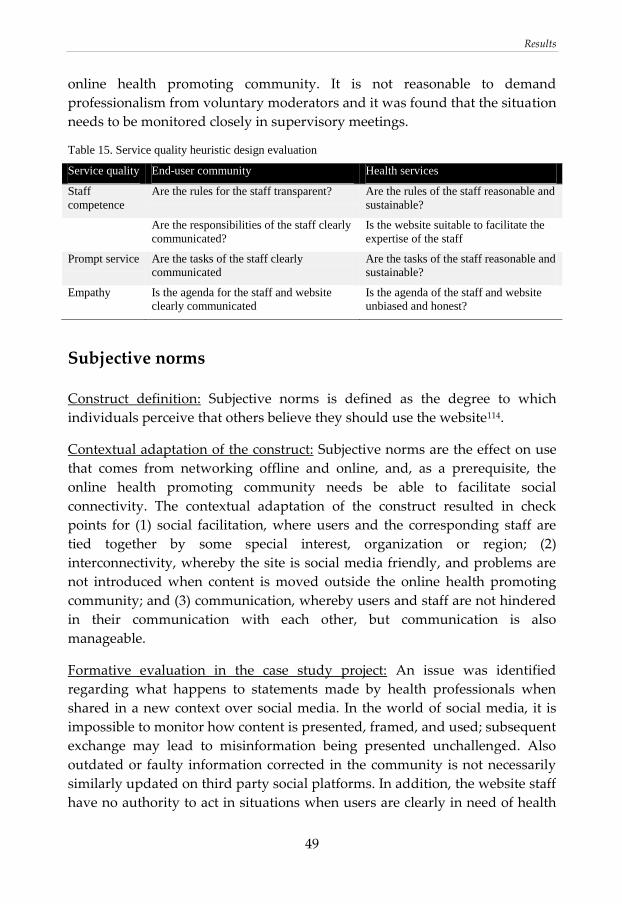
Results
49
online health promoting community. It is not reasonable to demand
professionalism from voluntary moderators and it was found that the situation
needs to be monitored closely in supervisory meetings.
Table 15. Service quality heuristic design evaluation
Service quality End-user community Health services
Staff
competence
Are the rules for the staff transparent? Are the rules of the staff reasonable and
sustainable?
Are the responsibilities of the staff clearly
communicated?
Is the website suitable to facilitate the
expertise of the staff
Prompt service Are the tasks of the staff clearly
communicated
Are the tasks of the staff reasonable and
sustainable?
Empathy Is the agenda for the staff and website
clearly communicated
Is the agenda of the staff and website
unbiased and honest?
Subjective norms
Construct definition: Subjective norms is defined as the degree to which
individuals perceive that others believe they should use the website114.
Contextual adaptation of the construct: Subjective norms are the effect on use
that comes from networking offline and online, and, as a prerequisite, the
online health promoting community needs be able to facilitate social
connectivity. The contextual adaptation of the construct resulted in check
points for (1) social facilitation, where users and the corresponding staff are
tied together by some special interest, organization or region; (2)
interconnectivity, whereby the site is social media friendly, and problems are
not introduced when content is moved outside the online health promoting
community; and (3) communication, whereby users and staff are not hindered
in their communication with each other, but communication is also
manageable.
Formative evaluation in the case study project: An issue was identified
regarding what happens to statements made by health professionals when
shared in a new context over social media. In the world of social media, it is
impossible to monitor how content is presented, framed, and used; subsequent
exchange may lead to misinformation being presented unchallenged. Also
outdated or faulty information corrected in the community is not necessarily
similarly updated on third party social platforms. In addition, the website staff
have no authority to act in situations when users are clearly in need of health

Results
50
care; and there was a lack of preparedness for how to assess serious health
issues online.
Table 16. Subjective norms heuristic design evaluation
Subjective
norms
End-user community Health services
Social
facilitation
Is the online health promoting
community tied to a geographic area
or organization?
Are the online health promoting
community staff tied to a region,
organization, or adequate profession?
Interconnectivity Is there functionality to connect
content and interaction with other
social media?
Are there any issues with content being
shared over social media?
Communication Is it possible to interact with other
users privately and publicly?
Is there functionality to connect with
individual users, for referral or
moderation?
Is there functionality to connect with
the staff, for questions or private
messaging?
Is there authority to connect with
individual users, for referral or
moderation?

Discussion
51
DISCUSSION
The overall aim of this thesis was to design, implement, and formatively
evaluate tools for use in a community-based health promoting intervention for
adolescents. To determine the requirements for the community-based
intervention, the target population was assessed to determine the health-
related needs and the current and evidence-based interventions available. In
this assessment, we observed a need among adolescents for a community-
based initiative, facilitating honest and unfiltered dialogue on health between
health professionals and young people. To determine the requirements for an
online health promoting community to meet this need, we initiated a
participatory design project together with regional public health services and
adolescents in the region. In the design of the online health promoting
community, conflicts involving the management of resources and
responsibilities in the public health organization were identified, and when
these were resolved, a preliminary version of the online health promoting
community was made available for tests. A checklist to be used to inform
online health promoting communities based on information system evaluation
research was formalized and formatively evaluated.
In Study I, we set out to determine the age for boys and girls at which PI⁄BMI
values begin to be associated with the corresponding measurements in late
adolescence. We found a strong correlation (r > 0.5) between the intra-
individual measurements from 5 years of age onwards. We also found that, in
our study cohort, 23% of the girls and 8% of the boys defined as obese at age 5
years were of normal weight at the age of 15 years. Combining the facts that so
few individuals had returned to normal weight from the age of 5 years and
that intra-individual BMI values were strongly correlated from 5 years up to
15 years of age, we conclude that there are reasons for offering population-
based interventions systematically from 5 years of age. This recommendation
is supported by the reports from Kim et al.116 who found that prevention at 5–8
years of age was more successful compared with prevention when the
children had reached 11–13 years. From the perspective of eventual health
risks as adults, it would be worthwhile identifying at an early age those
relatively few children with substantially increased risk of maintaining obesity

Discussion
52
in adulthood and offering them interventions; but interventions must be
avoided when they are not necessary.
Point estimates of childhood obesity using IOTF cut-off limits for BMI have
been found to have low sensitivity (6–15%) for predicting obesity and
metabolic disorders in young adulthood31. Study II was aimed at exploring
weight trajectories for identification of adolescents at risk for developing
obesity and metabolic disorders as adults, particularly children with a non-
obese childhood BMI, and projecting the costs for a trajectory-adjusted
strategy for obesity prevention. We used IOTF cut-off points to analyse the
weight classification trajectories of 4312 children up to age 15 years. The
present need for obesity prevention among adolescents is greater than the
resources available. Our projections indicate that the trajectory-based strategy
would benefit adolescents with more specified interventions without
increasing the costs. Online behavioural interventions open up the possibility
of providing obesity prevention programs to individuals at risk117. Promising
approaches include Internet-based coaching programmes for high-risk
patients118.
Based on the need found in Study II, Study III utilized design with
participating adolescents and representatives from regional public health to
develop and implement an online health promoting community. The study set
out to examine what aspects of the structure and functions of an online health
promoting community are critical to satisfy the needs of user communities and
public health goals and service capabilities. The most important observation
was that compromises in the online health promoting community design were
needed to resolve conflicts involving the management of resources and
responsibilities in the public health organization. In a comparable online
health promoting community development initiative in Ontario, Canada
(http://www.youthspark.ca), methods for systems development, sustainability,
and evaluation of an online health promoting community have been
comprehensively documented119. The current results add knowledge about
negotiation between public health interests and end-user needs in the online
health promoting community design process.
Study IV set out to develop a checklist for pre-launch evaluation of online
health promoting communities. Use of checklists has a long tradition in design
methodology and has also been used in the development of health information
websites120. Checklists are heuristic sets of constructs and guidelines not meant

Discussion
53
to be strictly adhered to. The objective of the current checklist is not to strive
for online health promoting community conformity, but instead to make sure
that central design questions are attended to and that there are clear
arguments supporting each divergent design decision121. The resulting
checklist includes the following constructs: information quality, service quality
and subjective norms. The most important result from its formative evaluation
was the delicate balance between community autonomy and quality control in
the formulation of the information and service quality constructs. In order to
empower an online community, some control over content and moderation
needs to be surrendered in a managed process.
RELATION WITH PREVIOUS RESEARCH
Obesity is a growing problem in developed nations122. Currently one-third of
US children are overweight or obese. Childhood overweight and obesity in
European countries range from 8% to 30%123. Although the situation in
Sweden is not as alarming as in the United States, still one-fifth of young
children are overweight and they remain so into adolescence as shown in
Study I. In addition to promoting poor self-esteem, which may negatively
impact social, psychological and educational development, paediatric and
adolescent obesity is associated with serious medical problems affecting the
cardiovascular and metabolic systems.
The proportion of obesity in the study cohort for this thesis project was
relatively constant at 2–3% through the school years for girls; obesity in boys is
steadily increasing over time. These findings are in concordance with previous
Swedish cross-sectional studies. The prevalence of overweight and obesity
among boys is often higher than in girls and higher at the younger age (4, 10
years) compared with adolescents (15–16 years)124–127. There are relatively few
longitudinal cohort studies of BMI development in Swedish children. Data
from a cohort (n = 3650) born between 1973 and 1975 in Gothenburg covering
annual BMI values from 2 years of age to 15 years of age have been reported128.
A similar data set was collected from children (n = 2591) born in the southern
suburbs of Stockholm in 1985–1987. A comparison of the BMI distribution
from 2 years of age to 15 years of age between these cohorts showed that from
the age of 7 years, the children born in 1985–1987 had higher BMI mean values
than their counterparts born 12 years earlier129. The authors concluded that

Discussion
54
school-aged children may be more susceptible to obesogenic environmental
exposure than younger children.
From the perspective of eventual health risks as adults, it would be
worthwhile identifying those relatively few children with substantially
increased risk of maintaining obesity in adulthood at an early age and offering
interventions; but interventions must be avoided when they are not necessary.
To identify children at risk, a simple decision protocol that can be used at well-
child centres and in school health care is needed to identify individuals who
are on trajectories that will lead to persisting obesity97. Correspondingly,
research is needed on cost-effective treatment programmes for young obese
children. Present evidence suggests that long-term family-based behavioural
interventions can achieve lasting weight reduction in this category of
children130.
Evidence on overweight and obesity based on weight history makes it possible
to improve the performance of selection strategies when adolescents are
provided with specific obesity preventive services. Using a projection from
epidemiological data, Study II demonstrated that by basing the selection of
adolescents for obesity prevention on weight trajectories, the load on highly
specialized paediatric care can be reduced by one-third and total health service
costs for obesity management among adolescents reduced by one-third. One
out of five children can be selected for individualized interventions, such as
motivational interviewing131. However, before use in policies and prevention
program planning, the findings warrant confirmation in prospective cost–
benefit studies.
Web technology is becoming increasingly prevalent in health services132,133. In
a recent review of computer and web-based interventions to increase physical
activity among adolescents, most interventions led to a significant increase in
physical activity, but the effects were short-lived45. Experiences from smoking
cessation programs suggest that using only Internet initiatives based on social
cognitive theory is not effective134, but that a combination of cell phone
technologies, peer-to-peer contact and web-based information on health and
coping strategies can be a promising long-term treatment option135. An online
health promoting community is a community-based, long-term and inclusive
health promotion approach99. Recently, online communities have been used in
health services for self-management136 and communities of practice137. When
such online health promoting communities are developed on a large scale, the

Discussion
55
existing models for health promotion program implementation and evaluation
must also be extended to fit the virtual setting. For instance, a possible
problem with an online health promoting community initiative is that it may
encourage young people to post and discuss health issues and problems in a
manner that they later may come to regret. Even though it is easy to censor
content after the fact, information online tends to persist. However, the
development of privacy guidelines for social media and maturation of online
behaviour may lessen the risks of sharing online138.
There are several different uses for the checklist developed in Study IV. For
instance, it can be used in conjunction with practical development guides for
health promotion web resources119 to cross-validate results from requirements
analyses and ensure that design specifications have a reasonable scope. In
website design, a site can be redesigned or re-imagined after implementation,
based on the availability of technologies such as cascading style sheets (CCS)
and CMSs without having to alter the underlying technical architecture139.
However, first implementations become more or less fixed once the basic style
of the website has become known and used. The logotype, layout, and colour
scheme are intimately associated with a website image and radical re-
imagination is more consequential the longer the time lapse after launch. The
combination of the stickiness of website images and technical flexibility make
it possible to allow stakeholders to improve the website using participatory
methods140.
LIMITATIONS
One limitation of Studies I and II is that the children were followed only to 15
years of age. However, Wardle et al.124 found that obesity already existing in
early adolescence (11 years of age) is a clear indication for persisting obesity,
and Whitaker et al.141 have found that four out of five obese teenagers remain
obese in adulthood. BMI was not originally designed for the purpose of
assessing obesity in growing children. Alternative classifications of BMI
measurements in children have been used, e.g. relative classifications where
children over the 80th percentile for their respective age and gender are
classified as overweight and those over the 95th percentile as obese26–28.
However, the IOTF criteria29 are based on an international cohort consisting of
almost 200 000 individuals and relate to the risk for adult morbidity. The

Discussion
56
results of Studies I and II were presented according to these criteria to make
the broadest comparisons possible.
When interpreting Study II, it must be taken into consideration that the results
are limited in several aspects. The economic projections were not calculated
from costs recorded in the study county. As the aim was to compare
hypothetical intervention strategies, standardized cost data from the literature
were used. Similarly, a marginal costs model assuming the presence of a
health service infrastructure was used for the analysis. This model also
included some hypothetical elements. For instance, in Sweden pharmaceutical
treatment for obesity can only be supplied to patients less than 18 years of age
after permission from the Medical Products Agency. The Medical Products
Agency can at short notice allow prescription of a specific drug to an
individual patient by issuing a special license on a named patient basis. To
establish the superiority of the trajectory strategy, it must be adapted,
implemented and evaluated within a health service context, and the factual
costs recorded and analysed. Furthermore, we did not record a metabolic
profile at age 15 years and have not collected BMI data in adulthood; the
detailed metabolic risk for each trajectory group is thus not known for this
population. Weight-related data may be lacking in school health care records
at present and documentation from earlier interventions may be unavailable.
However, with the wider use of electronic health records, the possibility of
using weight trajectories to inform screening of adolescents when they leave
school health care will increase.
Study III has several limitations that need to be taken into account when
interpreting the results. Community-based participatory research methods
have inherent methodological challenges. Allowing practitioners and the
target community to influence the qualitative analysis process may be
interpreted as surrendering control of the study. However, in accordance with
the suggested increased use of qualitative data from in-depth interviews and
observations for evaluating the context, process, impact, and outcome of
community-based interventions142–147, we contend that the participatory
method used in this study is adequate for capturing the context and process of
the community development. In such interventions, experimental control may
be incongruous when taking the different sociopolitical structures of
communities into account143,145,148. To ensure contextual soundness, in this
study, the practitioners were included in their actual professional roles, and
the adolescents were the users, rather than merely informants. In addition,
Discussion
57
including young people from the end-user community from several
municipalities and school programs in the research was an attempt to decrease
the threats to soundness that are associated with a convenience sample and
that the adolescents would be disingenuous.
There are also important limitations that must be taken into account when
considering application of the results of Study IV. A checklist based on
measures of information system success87 risks focusing online health
promoting community design on tangible features that characterize successful
online communities, rather than supporting health promotion success.
Focusing on information system success rather than use alone may be one way
to lessen this problem. Research on online communities has identified several
constructs shown to be associated with both the use and perceived net benefit
of online communities as an information system144. The contextual adaptation
of the constructs in this study resulted in items for content area, trust, format,
staff competence, prompt service, empathy, social facilitation, inter-
connectivity and communication. Nonetheless, these constructs cannot be
regarded as a final set. For instance, no construct presently addresses online
moral conduct, although the service quality construct covers the consequences
of biases and lack of transparency. Vibrant communities exist today where the
discourse is characterized as uncivil and destructive. It is currently held that
online conduct is less civil than the offline counterpart, and the anonymity of
the Internet has been proposed as an explanation149. More importantly, no
construct addresses health benefits per se. Health outcomes from an online
health promoting community are difficult to determine in pre-launch
evaluations. In contrast to online disease prevention efforts150, online health
promoting community outcomes are also challenging to define in the
summative evaluation context. The checklist presented in this study is based
on the tradition of information system success87, with emphasis on providing
benefit to communities as defined by the community. However, the benefits
determined by the community may or may not correspond to the public health
goals.
RELEVANCE FOR PUBLIC HEALTH PRACTICE
The study cohort in this thesis project can be considered representative in that
14% were overweight and 4% were obese at 15 years of age. The proportion of
those overweight was highest (17%) at the age of 10 years. The proportion of

Discussion
58
obesity was relatively constant at 2–3% through the school years for girls;
obesity in boys is steadily increasing over time.
In the continuing efforts to prevent disease and promote health, every public
health intervention must be evaluated in terms of benefit and side effects.
Often the most effective approach to obesity prevention also brings forth
stigmatization, which is seldom considered and evaluated in efficacy trials and
randomized controlled studies151. For instance, the very concept of overweight
in childhood is by definition merely an epidemiological association with
corresponding adult overweight classification29. When working with children
classified as overweight in this manner, it is thus an intervention for a risk
factor (overweight in childhood) for a risk factor (overweight in adulthood) for
obesity. In such cases, much care must be taken to avoid exposing children to
harmful social and psychological interventions.
Childhood obesity determined by the IOTF reference BMI cut-off points has
been found to have a high specificity (97–99%) for predicting obesity and
metabolic disorders in young adulthood31. That is, only a very small
percentage of the individuals who are categorized in the low-risk groups in
adulthood were obese as children. There are therefore reasons for categorizing
children determined obese by the IOTF reference BMI cut-offs separately and
providing them with extra resources for treatment and prevention. Moreover,
our recent observations and those of others suggest that children belonging to
the constant overweight (8.3% of the population at age 15 years in Study II)
and turning overweight (4.1% of the population) trajectories should also be
considered as candidates for individual obesity prevention before they
develop obesity in adulthood.
Before public health providers invest resources in putting an online health
promoting community design into routine practice, the design should be
evaluated with regard to health effects and use patterns in the intended
population. There is a need to evaluate both the use and effectiveness of the
system using several methods, including web surveys, focus groups and
controlled effectiveness studies. The large-scale implementation of an online
health promoting community design in a practice setting, which is necessary
for such an evaluation, is associated with methodological challenges.
Participatory design proponents suggest that because the social factors
important for the implementation are highlighted in a participatory design
approach, the resulting systems are more sustainable compared with those

Discussion
59
developed using traditional systems development methods152. However,
participatory methods have also been criticized for neglecting the later
technical development stages153 and being unrealistic with regard to the
resources demanded of practitioners154. Techniques such as the Voice of the
Customer table and House of Quality 155 are well-established but time- and
resource-consuming approaches to the problem of system accurateness.
Action research, as used in Study IV, is a contextual research approach104 and
therefore generalizations, if done at all, should be done with caution. To
ensure contextual soundness, health service practitioners participated in this
study in their actual professional roles, and young people participated as
online health promoting community users, rather than merely informants. The
practitioners and young people thus both represented and reflected the
infrastructure and processes of the Swedish health services and general
society. The needs analysis, design, and validation of the online health
promoting community were embedded in its regional context. Although the
development of the initial version of the checklist was influenced by the
experience and prejudices of the researchers, the formative evaluation data
comprised factual decisions and adjustments made in the development
process, thus limiting researcher influence. It may thus be possible that vital
aspects of a pre-launch online health promoting community evaluation
checklist eluded analysis in this study, but it is less likely that unfounded
design arguments were introduced as data. Before using the checklist, a
comparison of the infrastructure and processes of the study context from
which the checklist was abstracted with the target context is needed in order to
determine what aspects of the checklist are irrelevant156.
FUTURE RESEARCH
Future studies to address evaluation of online health promoting communities
are warranted. However, measuring community empowerment is associated
with several methodological challenges. A central concept in design
methodology is that the design itself will change the context for which it is
designed71,73. Furthermore, due to the sociotechnical development of the
community, an adequate design at launch will probably not be appropriate for
long, and the design will develop alongside the community structure and
needs. Thus, traditional requirements for intervention evaluation such as
Discussion
60
blinding and using static exposure are easily violated in the evaluation of
online health promoting communities.
A proper evaluations framework of online health promoting communities
should include the success of the community intervention both as an
information system84 and as a health promoting initiative34. The former
answers the question if the community can be reached by the means of an
online health promoting community and the latter if the intervention
influences the community as intended. The first set of challenges is the
measurement of community reach and influence on regional health services.
Quantitative measures such as traffic, user experience questionnaires88 and
information system assessment114,115 can be complemented by qualitative
measures such as content analysis of online activity and focus groups of
satisfied and dissatisfied user groups99. However, as the design evolves based
on continuous feedback from its community, the methods for book-keeping of
feedback when adjusting the design over time needs to be addressed. For
instance, a comment on a specific feature may be irrelevant, because the
feature has already been modified due to previous feedback.
The second set of challenges is the measurement of health outcomes of health
promoting initiatives. In contrast to disease prevention, it is more difficult to
define and measure outcomes in health promotion157. However, as described
in this thesis, there have been several attempts to formalize and operationalize
behaviour based on self-efficacy with similarities to the health promotion
concept of empowerment48,51. Self-efficacy is a general characteristic associated
with empowerment and, without a specific intention, self-efficacy risks being
too general to be of any use in health promotion. One direction put forth in the
literature is to use health-specific self-efficacy associated with weight loss158,159.
However, more research on the application of psychological constructs in
health promoting interventions is going to be needed. If the theory of planned
behaviour is valid, self-efficacy can be used as a quantitative measure of
empowerment. But as put forth by researchers in community-based
participatory research, using simple quantitative measurements to
operationalize social systems is ill-advised142–147. Another direction for the
future is to discern the goals and intentions of subjects through the use of
qualitative approaches such as interviews and focus group interviews, more
akin to approaches in community-based participatory research144,145,148.

Conclusions
61
CONCLUSIONS
In Study I we found a strong correlation (r > 0.5) between the intra-
individual BMI measurements from 5 years of age onwards and reasons
for offering population-based interventions systematically from 5 years
of age. It would be worthwhile identifying those relatively few children
with substantially increased risk of maintaining obesity in adulthood at
an early age and offer interventions; but interventions must be avoided
when they are not necessary.
The projections in Study II indicate that a trajectory-based strategy for
categorizing adolescents at age 15 years with regard to obesity
interventions would benefit adolescent populations with more specified
interventions without increasing the costs.
In Study III, we found than an online health promoting community can
be designed simply at relatively low cost and can be negotiated to
satisfy both the needs of the user community and public health goals
and service capabilities. The main results were that compromises in the
online health promoting community design were needed to resolve
conflicts involving the management of organizational resources and
responsibilities.
In Study IV, a checklist for pre-launch evaluation of online health
promoting communities was developed and included the following
constructs: information quality, service quality and subjective norms.
The most important result from a formative evaluation was the delicate
balance between community autonomy and quality control in the
formulation of the information and service quality constructs.
62

Acknowledgements
63
ACKNOWLEDGEMENTS
Many people have influenced and helped me to get to this point, too many to
mention individually. However, there are a few that I wish to explicitly thank.
My supervisor Toomas Timpka has been an inspiration, leading by example
rather than by canon, and has opened my eyes to the peculiar world of
academia, interdisciplinary collaboration and action research, and at this point
I consider him a dear friend.
My co-supervisor Nils Dahlbäck has provided support and brilliant insight into
interdisciplinary research, but most of all awakened my interest in
interdisciplinary research at my very first encounter with cognitive science.
My co-supervisor Henrik Eriksson has patiently provided invaluable advice
and much appreciated reality checks, even though my ideas through the years
caused him to be confused.
To my friend Jenny Jacobsson for many a fiery and intriguing discussion, face to
face, over the phone, by mail, Skype, day or night, I am immensely grateful for
the opportunity to have been confused together.
Marianne Angbratt for being an invaluable ally and friend when working with
obesity prevention strategies, opening doors everywhere and sharing her
immense experience of public health practice.
My friends in public health, Linda Frank, Anna-Maria Norén, Boel Andersson
Gäre, Emelie Andersen and Lena Hedin, who helped turn intricate and
unfathomable visions into a practical intervention.
My mentor in global public health, Elin Gursky, for invaluable advice, support
and critique.
Lars Valter, Armin Spreco, and especially Örjan Dahlström, for valuable advice
and insight into medical statistics.
Maria Nordwall and Marie Teder for inviting me to the world of paediatrics,
primary care and nursing reality.
Acknowledgements
64
Kajsa Bendtsen, without whom getting anything done seems impossible. Your
patience and support making everything run smoothly is immensely
appreciated.
The adolescents, who participated both as participatory designers and
informants in focus groups, from the counties in Östergötland, Jönköping and
Kalmar.
Participating school health nurses in the schools of Östergötland, getting to
know you when collecting the data has made a lasting impression on me.
Lorna O’Brien for invaluable assistance in correcting the English in our texts.
And finally my family for supporting my choice of work, my wife Sara and my
sons Valona and Enzo.

References
65
REFERENCES
1. Lissner L, Sohlström A, Sundblom E, Sjöberg A: Trends in overweight
and obesity in Swedish schoolchildren 1999–2005: has the epidemic
reached a plateau? Obes Rev. 2010 11(8):553–559.
2. Bergström E, Blomquist HK: Is the prevalence of overweight and obesity
declining among 4-year-old Swedish children? Acta Paediatr. 2009
98(12):1956–1958.
3. Sjöberg A, Lissner L, Albertsson-Wikland K, Mårild S: Recent
anthropometric trends among Swedish school children: evidence for
decreasing prevalence of overweight in girls. Acta Paediatr. 2008
97(1):118–123.
4. Shaw SM, Kemeny L: Fitness promotion for adolescent girls: the impact
and effectiveness of promotional material which emphasizes the slim
ideal. Adolescence. 1989, 24(95):677–687.
5. Setiloane K. Being overweight: negative outcomes for African American
adolescents. Nutr Health. 2004, 18(1):61–66.
6. Powers PS, Bruty H: Pharmacotherapy for eating disorders and obesity.
Child Adolesc Psychiatr Clin North Am. 2009, 18(1):175–187.
7. Owen CG, Whincup PH, Orfei L, Chou QA, Rudnicka AR, Wathern AK,
Kaye SJ, Eriksson JG, Osmond C, Cook DG: Is body mass index before
middle age related to coronary heart disease risk in later life? Evidence
from observational studies. Int J Obes (Lond). 2009, 33(8):866–77.
8. Carter OB: The weighty issue of Australian television food advertising
and childhood obesity. Health Promot J Austr. 2006, 17(1):5–11.
9. Anderson AS: How to implement dietary changes to prevent the
development of metabolic syndrome. Br J Nutr. 2000 83(Suppl 1):S165–
168.
10. Kind T: The Internet as an adjunct for pediatric primary care. Curr Opin
Pediatr. 2009, 21(6):805–810.
11. WHO: Obesity: Preventing and Managin the Global Epidemic. Report of
a WHO consultation, World Health Organ Tech Rep Ser. 2000, 894:i-xii, 1–
253.

References
66
12. Gray DS, Fujioka J: Use of reative weight and body mass index for the
determination of adiposity. J Clin Epidemiol. 1991, 44:545–550.
13. Revicki DA, Israel RG: Relationship between body mass indices and
measures of body adiposity. Am J Publ Health. 1986, 76:992–994.
14. Keys A, Fidanza F, Karvonen MJ, Kimura N, Taylor HL: Indices of
relative weight and obesity. J Chron Dis. 1971, 25:329–343.
15. Garn SM, Leonard WR, Hawthorne VM: Three limitations of the body
mass index. Am J Clin Nutr. 1986, 44:996–997.
16. Statistics Sweden: Undersökning av levnadsförhållanden (ULF) [Survey of
Living Conditions]. Available from www.scb.se. Örebro: Statistics Sweden,
2004 [in Swedish].
17. Statistics Sweden: Undersökning av levnadsförhållanden (ULF) [Survey of
Living Conditions]. Available from www.scb.se. Örebro: Statistics Sweden,
2009 [in Swedish].
18. Vaz de Almeida MD, Graça P, Afonso C, D'Amicis A, Lappalainen R,
Damkjaer S: Physical activity levels and body weight in a nationally
representative sample in the European Union. Public Health Nutr. 1999,
2:105–113.
19. Lissner L, Johansson SE, Qvist J, Rössner S, Wolk A: Social mapping of
the obesity epidemic in Sweden. Int J Obes Relat Metab Disord. 2000,
24:801–805.
20. Lindström M, Isacsson SO, Merlo J: Increasing prevalence of overweight,
obesity and physical inactivity. Eur J Public Health. 2003, 13:306–312.
21. Borg S, Persson U, Odegaard K, Berglund G, Nilsson JA, Nilsson PM:
Obesity, survival, and hospital costs - findings from a sceening project
in Sweden. Value Health. 2005, 8(5):562–571.
22. Ekholm O, Kjøller M, Davidsen M, Hesse U, Eriksen L, Illemann
Christensen A, Grønbæk M: Sundhed og sygelighed i Danmark 2005 &
udviklingen siden 1987. Copenhagen: Statens Institut for Folkesundhed,
2006 [in Danish].
23. Flegal KM, Caroll MD, Ogden CL, Curtin LR: Prevalence and Trends in
Obesity Among US Adults, 1999–2008 (NHANES). JAMA. 2010,
303(3):235–241.
References
67
24. Tjepkema M: Measured Obesity. Adult obesity in Canada: Measured Height and
Weight. Ottawa: Statistics Canada, 2004.
25. Department of Health: Health Survey for England. National Statistics,
England, 2002.
26. Dietz WH: Health consequences of obesity in youth: childhood
predictors of adult disease. Pediatrics. 1998, 2:518–525.
27. Reilly JJ, Armstrong J, Dorosty AR, Emmett PM, Ness A, Rogers I, Steer C,
Sherriff A: Early life risk factors for obesity in childhood: cohort study.
BMJ 2005, 330:1357.
28. McCallum Z, Gerner B: Weighty matters – an approach to childhood
overweight in general practice. Aust Fam Physician 2005, 34:745–748.
29. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH: Establishing a standard
definition for child overweight and obesity worldwide: international
survey. BMJ. 2000, 320(7244):1240–1243.
30. Cole TJ, Flegal KM, Nicholls D, Jackson AA: Body mass index cut offs to
define thinness in children and adolescents: international survey. BMJ.
2007, 335(7612):194.
31. Janssen I, Katzmarzyk PT, Srinivasan SR, Chen W, Malina RM, Bouchard
C, Berenson GS: Utility of childhood BMI in the prediction of
adulthood disease: comparison of national and international references.
Obes Res. 2005, 13:1106–1115.
32. Van der Ploeg HP, Chey T, Korda RJ, Banks E, Bauman A: Sitting time
and all-cause mortality risk in 222 497 Australian adults. Arch Intern
Med. 2012, 172(6):494–500.
33. Carson KV, Verbiest ME, Crone MR, Brinn MP, Esterman AJ, Assendelft
WJ, Smith BJ: Training health professionals in smoking cessation.
Cochrane Database Syst Rev. 2012, 5:CD000214.
34. Bracht N, Kingsbury L, Rissel C: A five-stage community organization
model for health promotion. In: Bracht N (ed.). Health Promotion at the
Community Level: New advances. Thousand Oaks, CA.: Sage Publications,
1999.
35. Delbanco T, Berwick DM, Boufford JI, Edgman-Levitan S, Ollenschläger G,
Plamping D, Rockefeller RG: Healthcare in a land called PeoplePower:
nothing about me without me. Health Expect. 2001, 4(3):144–150.

References
68
36. Delbanco T, Sands DZ: Electrons in flight--e-mail between doctors and
patients. N Engl J Med. 2004, 350(17):1705–1707.
37. March S, Spence SH, Donovan CL: The efficacy of an Internet-based
cognitive-behavioral therapy intervention for child anxiety disorders. J
Pediatr Psychol 2009, 34(5):474–487.
38. Frost JH, Massagli MP: Social uses of personal health information within
PatientsLikeMe, an online patient community: what can happen when
patients have access to one another's data. J Med Internet Res. 2008,
10:e15.
39. Afrin LB, Greenland WJ, Finch NJ: Support group webcasting: a
feasibility assessment. AMIA Annu Symp Proc. 2005:880.
40. Marks I, Shaw S, Parkin R: Computer-aided treatments of mental health
problems. Clin Psychol Sci Pract. 1998, 5:151–170.
41. Andersson G, Carlbring P: Internet and cognitive behaviour therapy:
new opportunities for treatment and assessment. Cogn Behav Ther. 2003,
32:97–99.
42. Casazza K, Ciccazzo M: The method of delivery of nutrition and physical
activity information may play a role in eliciting behavor changes in
adolecents. Eating Behav. 2007, 8(1):73–82.
43. Tate DF, Wing RR, Winett RA. Using Internet technology to deliver a
behavioral weight loss program. JAMA. 2001, 285(9):1172–1177.
44. Haerens L, Maes L, Vereecken C, De Henaux S, Moreno L, De
Bourdeaudhuij ID: Effectiveness of a computer tailored physical
activity intervention in adolescents compared to a generic advice.
Patient Educ Couns. 2009, 77(1):38–41.
45. Hamel LM, Robbins LB, Wilbur J: Computer- and web-based
interventions to increase preadolescent and adolecent physical activity:
a systematic review. J Adv Nurs. 2010, 67(2):251–268.
46. Haerens L, Bourdeaudhuij ID, Maes K, Cardon G, Deforche B: School-
based randomized controlled trial of a physical activity intervention
among adolescents. J Adolesc Health. 2007, 40(3):258–265.
47. Marks JT, Campbell MK, Ward DS, Ribisl KM, Wildemuth BM, Symons
MJ: A comparison of web and print media for physical activity
promotion among adolescent girls. J Adolesc Health. 2006, 39(1):96–104.

References
69
48. Bandura A: Social cognitive theory. In: Vasta R (ed.) Annals of Child
Development. Vol 6. Greenwhich, CT: JAI Press; 1989;1-60
49. Prochaska JO, Velicer WF: The transtheroretical model of health behavior
change. Am J Health Promot. 1997, 12(1):38–48.
50. Rosenstock IM: The health belief model and preventive health
behaviour. Health Educ Monogr. 1974, 2:328–335.
51. Ajzen I: The theory of planned behavior. Org Behav Hum Decis Process.
1991, 50(2):179–211.
52. De Vries H, Backbier E, Kok G, Dijkstra M: The impact of social
influences in the context of attitude, self efficacy, intention, and
previous behaviour as predictor of smoking onset. J Appl Soc Psychol.
1995, 25(3):237–257.
53. Prochaska JJ, Rogers MW, Sallis JF: Association of parent and peer
support with adolescent physcial activity. Res Q Exercise Sport. 2002,
73(2):206–210.
54. Duncan NR, Duncan TE, Strycker LA: Sources and types of social support
in youth physical activity. Health Psychol. 2005, 24(1):3–10.
55. Robbins LB, Stommel M, Hamel LM: Social support for physical activity
of middle school students. Public Health Nurs. 2008, 25(5):451–460.
56. Williamson DA, Walden HM, White MA, York-Crowe E, Newton RL Jr,
Alfonso A, Gordon S, Ryan D: Two year internet-based randomized
controlled trial for weight loss in African American girls. Obesity. 2006,
14(7):1231–1243.
57. Hogue A, Henderson CE, Dauber S, Barajas PC, Fried A, Liddle HA:
Treatment adherence, competence, and outcome in individual and
family therapy for adolescent behavior problems. J Consult Clin Psychol.
2008, 76(4):544–555.
58. Sackett DL, Haynes RB, Gibson ES: Patient compliance with
antihypertensive regimens. Patient Couns Health Educ. 1978, 1:18–21.
59. Rheingold H: The Virtual Community. New York: Addison-Wesley; 1993.
60. Johnson CM: A survey of current research on online communities of
practice. Internet High Educ. 2001, 4:45–60.
61. Lave J, Wenger E: Situated Learning: Legitimate Peripheral Participation.
Cambridge: Cambridge University Press; 1991.

References
70
62. Ekberg J, Ericson L, Timpka T, Eriksson H, Nordfeldt S, Hanberger L,
Ludvigsson J: Web 2.0 systems supporting childhood chrionic disease
management: design guidelines based on information behaviour and
social learning theories. J Med Syst. 2010, 34(2):107–117.
63. Livingstone DW: Researching expanded notions of learning and work
and underemployment: findings of the first Canadian survey of
informal learning practices. Int Rev Educ. 2000, 46:491–514.
64. Hyden C, Cohall A: Innovative approaches to using new media and
technology in health promotion for adolescents and young adults.
Adolesc Med State Art Rev. 2011, 22(3):498–520, xi–xii.
65. Crutzen R, Roosjen JL, Poelman J: Using Google Analytics as a process
evaluation method for Internet-delivered interventions: an example on
sexual health. Health Promot Int. 2012, doi:10.1093/heapro/das008.
66. Silberman J, Schwartz S, Giuseffi DL, Wang C, Nevedal D, Bedrosian R:
Reductions in employee productivity impairment observed after
implementation of web-based worksite health promotion programs. J
Occup Environ Med. 2011, 53(12):1404–1412.
67. Maon S, Edirippulige S, Ware R, Batch J: The use of web-based
interventions to prevent excessive weight gain. J Telemed Telecare. 2012,
18(1):37–41.
68. Whiteley LB, Mello J, Hunt O, Brown LK: A review of sexual health web
sites for adolescents. Clin Pediatr (Phila). 2012, 51(3):209–213.
69. Schneider F, van Osch L, de Vries H: Identifying factors for optimal
development of health-related websites: a delphi study among experts
and potential future users. J Med Internet Res. 2012, 14(1):e18.
70. Harris PR, Sillence E, Briggs P: Perceived threat and corroboration: key
factors that improve a predictive model of trust in internet-based health
information and advice. J Med Internet Res. 2011, 13(3):e51.
71. Simon H: Science of the Artificial. Cambridge, MA: MIT Press; 1969.
72. Bacon F: Novum Organum Scientiarum. 1620 (English translation by
Spedding J, Ellis RL, Heath DD, 1863). Available at
http://www.constitution.org/bacon/nov_org.htm).
73. Rittel HW, Webber MM: Dilemmas in a general theory of planning.
Policy Sci. 1973, 4:155–169.

References
71
74. Hollnagel E, Woods D: Joint Cognitive Systems. Boca Raton, FL: CRC Press;
2005.
75. Cook RI, Woods DD: Adapting to new technology in the operating room.
Hum Factors. 1996, 38(4):593–613.
76. Ashby WR: An Introduction to the Cybernetics. London: Methuen & Co;
1956.
77. Ash JS, Berg M, Coiera E: Some unintended consequences of information
technology in health care: the nature of patient care information
system-related errors. J Am Med Inform Assoc. 2004, 11(2):104–112.
78. Löwgren J: Applying design methodology to software development.
Proc. Symp. Designing Interactive Systems (DIS ’95). New York: ACM Press;
1995:87–95.
79. Bowles K: The barriers and benefits of nursing information systems.
Comput Nurs. 1997, 15(4):191–196.
80. Romano CA: Diffusion of technology innovation. Adv Nurs Sci. 1990,
13(2):11–21.
81. Doll WJ, Xia W, Torkzadeh G: A confirmatory factor analysis of the
enduser computing satisfaction instrument. MIS Q. 1994, 4:453–461.
82. Shannon CE, Weaver W: The Mathematical Theory of Communication.
Urbana, IL: University of Illinois Press; 1969.
83. Mason RO: Measuring information output: a communication systems
approach. Inform Manage. 1978, 1(5):219–234.
84. DeLone WH, McLean ER: Information systems success: the quest for the
dependent variable. Inform Syst Res. 1992, 3(1):60–95.
85. Van Der Meijden MJ, Tange H J, Troost J, Hasman A: Determinants of
success of inpatient clinical information systems: a literature review. J
Am Med Inform Assoc. 2003, 10(3):235–243.
86. DeLone WH, McLean ER: Information systems success revisited. In:
Proceedings of the 35th Hawaii International Conference on System Sciences
(HICSS 02). Washington, DC: IEEE Computer Society; 2002:238–249.
87. DeLone WH, McLean ER: The DeLone and McLean model of
information systems auccess: a ten-year update. J Manage Inform Syst.
2003, 19(4):9–30.
88. Davis FD: Perceived usefulness, perceived ease of use, and user
acceptance of information technology. MIS Q. 1989, 13:319–340.

References
72
89. Venkatesh V, Davis FD: A theoretical extension of the Technology
Acceptance Model: four longitudinal field studies. Manage Sci. 2000,
46(2):186–204.
90. Shannon CE: A mathematical theory of communication. Bell Syst Tech J.
1948, 27:379–412, 623–656.
91. Fishbein M, Ajzen I: Belief, Attitude, Intention, and Behavior: An Introduction
to Theory and Research. Reading, MA: Addison-Wesley; 1975.
92. Venkatesh V, Morris MG, Davis GB, Davis FD: User acceptance of
information technology: toward a unified view, MIS Q. 2003, 27(3):425–
478.
93. Armitage CJ, Conner M: Efficacy of the Theory of Planned Behaviour: a
meta-analytic review. Br J Soc Psychol. 2001, 40(Pt 4):471–499.
94. Bandura A: Exercise of personal agency through the self-efficacy
mechanism. In: Schwartzer R (ed.). Self-efficacy: Thought Control Through
Action. Washington DC: Hemisphere; 1992.
95. Angbratt M, Eriksson E, Funcke S, Nilsson U, Säterskog C, Söderlind M:.
Kartläggning av barns vikt och viktutveckling i Östergötland. Rapport 2003:2.
Linköping: Folkhälsovetenskapligt Centrum; 2003 [in Swedish].
96. Angbratt M, Ekberg J, Walter L: Uppföljning av ungdomars vikt i
Östergötland – vad har hänt med 91-orna? Rapport 2008:7. Linköping:
Folkhälsovetenskapligt Centrum; 2008 [in Swedish].
97. Timpka T, Angbratt M, Bolme P, Hermansson G, Hager A, Valter L: A
high-precision protocol for identification of preschool children at risk
for persisting obesity. PLoS ONE 2007; 2:e535.
98. Cohen J: Statistical Power Analysis for the Behavioral Sciences. 2nd edition.
Rahway, NJ: Lawrence Erlbaum; 1988.
99. Green J, Thorogood N: Qualitative Methods for Health Research (Introducing
Qualitative Methods Series). 2nd edition. London: Sage; 2009.
100. Maclean A. Young RM, Moran T: Design rationale: the argument behind
the artifact, SIGCHI Bull. 1989, 20:247–252.
101. Bellotti VME, MacLean A, Moran T: Structuring the design space by
formulating appropriate design rationale questions. SIGCHI Bull. 1991,
23(4):80–81.

References
73
102. Lee J: Design rationale systems: understanding the issues. IEEE Expert.
1997, 12(3):78–85.
103. Jarczyk AP, Löffler P, Shipman FM: Design rationale for software
engineering: a survey. 25th Hawaii International Conference on System
Sciences. 1992, 2:577–586.
104. Reason P, Bradbury-Huang H: Handbook of Action Research. 2nd edition.
London: Sage; 2007.
105. Kettinger WJ, Lee CC: Perceived service quality and user satisfaction
with the information services function. Decision Sci. 1995, 25(5–6):737–
765.
106. Pitt, LF, Watson RT, Kavan CB: Service quality: a measure of
information systems effectiveness. MIS Q. 1995, 19(2):173–188.
107. Mirani R, Lederer AL: An instrument for assessing the organizational
benefits of IS projects. Decision Sci. 1988, 29(4):803–838.
108. Martinsons M, Davison MR, Tse D: The balanced scorecard: a
foundation for the strategic management of information systems.
Decision Support Syst. 1999, 25(1):71–88.
109. Kaplan RS, Norton DP: Translating Strategy Into Action: The Balanced
Scorecard. Boston, MA: Harvard Business School Press; 1996.
110. Tokzadeh G, Doll WJ: The development of a tool for measuring the
perceived impact of information technology on work. Omega 1999,
27(3):327–339.
111. Bailey JE, Pearson SW: Development of a tool for measuring and
analysing computer user satisfaction. Manage Sci. 1983, 29(5):530–545.
112. Ives B, Olsen M, Baroudi JJ: The measurement of user information
satisfaction. Commun ACM. 1983, 26(10):785–793.
113. Shirani A, Aiken M, Reithel B: A model of user information satisfaction.
Data Base. 1994, 25(4):17–23.
114. Schaupp LC, Belanger F, Fan W: Examining the success of websites
beyond e-commerce: an extension of the IS success model. J Comput
Inform Syst 2009, summer:42–52.
115. Parasuraman A: Customer service in business-to-business markets: an
agenda for research. J Business Industr Market. 1998, 13(4/5):309–321.
116. Kim J, Must A, Fitzmaurice GM, Gillman MW, Chomitz V, Kramer E,
McGowan R, Peterson KE: Incidence and remission rates of overweight

References
74
among children aged 5 to 13 years in a district-wide school surveillance
system. Am J Public Health 2005, 95:1588–1594.
117. McCoy MR, Couch D, Duncan ND, Lynch GS. Evaluating an internet
weight loss program for diabetes prevention. Health Promot Int 2005;
20:221–228.
118. Goessens BMB, Visseren FLJ, de Nooijer J, van den Borne HW, Algra A,
Wierdsma J, van der Graaf Y, SMART Study Group: A pilot-study to
identify the feasibility of an Internet-based coaching programme for
changing the vascular risk profile of high-risk patients. Patent Educ
Couns 2008, 73:67–72.
119. Valaitis R, O’Mara L, Bezaire, S: Tailoring Online Health Promotion: A
Toolkit for Communities. Produced by Huron County Health Unit and
McMaster University, School of Nursing; 2007.
120. Freund T, Freund M, Mahler C, Schwantes U, Ose D, Joos S, Szecsenyi J:
Family practice web sites: new perspectives for patient care and health
information? Fam Med 2010, 42(7):501–506.
121. Sjöberg C: Voices in design: argumentation in participatory
development. PhD Thesis No. 436. Linköping, Sweden: Linköping
University; 1994.
122. Yaynos AF, O’Donohue WT: Universal childhood and adolescent
obesity prevention programs: review and critical analysis. Clin Psychol
Rev. 2012, 32:383–399.
123. van Stralen MM, te Velde SJ, van Nassau F, Brug J, Grammatikaki E,
Maes L, De Bourdeaudhuij I, Verbestel V, Galcheva S, Iotova V, Koletzko
BV, von Kries R, Bayer O, Kulaga Z, Serra-Majem L, Sánchez-Villegas A,
Ribas-Barba L, Manios Y, Chinapaw MJ; ToyBox-study group: Weight
status of European preschool children and associations with family
demographics and energy balance-related behaviours: a pooled
analysis of six European studies. Obes Rev. 2012, 13(Suppl 1):29–41.
124. Wardle J, Brodersen NH, Cole TJ, Jarvis MJ, Boniface DR: Development
of adiposity in adolescence: five year longitudinal study of an
ethnically and socioeconomically diverse sample of young people in
Britain. BMJ 2006, 332:1130–1135.

References
75
125. Holmbäck U, Fridman J, Gustafsson J, Proos L, Sundelin C, Forslund A:
Overweight more prevalent among children than among adolescents.
Acta Paediatr 2007, 96:577–581.
126. Sjöberg A, Hallberg L, Hoglund D, Hulthen L: Meal pattern, food choice,
nutrient intake and lifestyle factors in the Goteborg Adolescence
Study. Eur J Clin Nutr 2003, 57:1569–1578.
127. Werner B, Bodin L: Obesity in Swedish schoolchildren is increasing in
both prevalence and severity. J Adolesc Health 2007, 41:536–543.
128. He Q, Albertsson-Wikland K, Karlberg J: Population-based body mass
index reference values from Gothenburg, Sweden, from birth to 18
years of age. Acta Paediatr 2000, 89:582–592.
129. Eriksson M, Rasmussen F, Nordqvist T: Changes in shape and location
of BMI distributions of Swedish children. Acta Paediatr 2005, 94:1558–
1565.
130. The Cochrane Collaboration; Oude Luttikhuis H, Baur L, Jansen H,
Shrewsbury VA, O'Malley C, Stolk RP, Summerbell CD: Interventions for
Treating Obesity in Children. London: The Cochrane Library; 2009.
131. Söderlund LL, Nordqvist C, Angbratt M, Nilsen P: Applying
motivational interviewing to counselling overweight and obese
children. Health Educ Res 2009; 24:442–449.
132. Nicholas J: The role of internet technology and social branding in
improving the mental health and wellbeing of young people. Perspect
Public Health. 2010, 130(2):86–90.
133. Mockford C, Stansizewska S, Griffiths F, Herron-Marx S: The impact of
patient and public involvement of UK NHS health care: a systematic
review. Int J Qual Health Care. 2011, doi:10.1093/intqhc/mzr066.
134. Mason D, Gilbert H, Sutton S: Effectiveness of web-based tailored
smoking cessation advice reports (iQuit): a randomised trial. Addiction.
2012, doi:10.1111/j.1360-0443.2012.03972.x.
135. Bredryen H, Drozd F, Kraft P: A digital smoking cessation program
delivered through internet and cell phone without nicotine
replacement (happy ending): randomized controlled trial. J Med Internet
Res 2008, 28:10(5):e51.

References
76
136. Li LC, Townsend AF, Badley EM: Self-management intervention in the
digital age: new approaches to support people with rheumatologic
conditions. Best Pract Res Clin Rheumatol. 2012, 26:321–333.
137. Barnett RS, Jones SC, Bennett S, Iverson D, Bonney A: General practice
training and virtual communities of practice – a review of the literature.
BMC Fam Pract. 2012, 13:87.
138. Subrahmanyam K, Greenfield P: Online communication and adolescent
relationships. Future Child. 2008, 18(1):119–146.
139. Hirschheim R: Assessing participative systems design: some
conclusions from an exploratory study. Inform Manage 1983, 6:13–32.
140. Clemensen J, Larsen SB, Kyng M, Kirkevold M: Participatory design in
health sciences: using cooperative experimental methods in developing
health services and computer technology. Qual Health Res 2007,
17(1):122–130.
141. Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH: Predicting
obesity in young adulthood from childhood and parental obesity. N
Engl J Med 1997, 37:869–873.
142. Israel BA, Schulz AJ, Parker EA, Becker AB: Review of community-based
research: assessing partnership approaches to improve public health.
Annu Rev Public Health. 1998, 19:173–202.
143. Susser M: The tribulations of trials-intervention in communities. Am J
Public Health. 1995, 85:156–158.
144. Israel BA, Cummings KM, Dignan MB, Heaney CA, Perales DP, Simons-
Morton BG, Zimmerman MA: Evaluation of health education programs:
current assessment and future directions. Health Educ Q. 1995, 22:364–
389.
145. Mittelmark MB, Hunt MK, Heath GW, Schmid TL: Realistic outcomes:
lessons from community-based research and demonstration programs
for the prevention of cardiovascular diseases. J Public Health Policy. 1993,
14:437–462.
146. Koepsell TD, Wagner EH, Cheadle AC, Patrick DL, Martin DC, Diehr PH,
Perrin EB, Kristal AR, Allan-Andrilla CH, Dey LJ: Selected
methodological issues in evaluating community-based health

References
77
promotion and disease prevention programs. Annu Rev Public Health.
1992, 13:31–57.
147. Sorensen G, Emmons K, Hunt MK, Johnston D: Implications of the
results of community intervention trials. Annu Rev Public Health. 1998,
19:379–416.
148. Green LW, Richard L, Potvin L: Ecological foundations of health
promotion. Am J Health Promot. 1996, 10:270–281.
149. Suler J: The online disinhibition effect. Cyberpsychol Behav 2004,
7(3):321–326.
150. Wieland LS, Flazon L, Sciamanna CN, Trudeau KJ, Brodney S, Schwartz
JE, Davidson KW: Interactive computer-based interventions for weight
loss or weight maintenance in overweight or obese people (Review).
2012. Cochrane Database Syst Rev 2012, (8):CD007675.
151. Giel KE, Zipfel S, Alizadeh M, Schäffeler N, Zahn C, Wessel D, Hesse FW,
Thiel S, Thiel A. Stigmatization of obese individuals by human resource
professionals: an experimental study. BMC Public Health. 2012, 12(1):525.
152. Floyd C, Mehl WM, Reisin FM, Schmidt G, Wolf G. Out of Scandinavia:
alternative approaches to software design and system development.
Human–Comput Interact 1989, 4(4):253–350.
153. Tollmar K. Towards CSCW design in the Scandinavian tradition.
Doctoral Thesis. Stockholm: Department of Numerical Analysis and
Computer Science, Stockholm University; 2001.
154. Hirschheim R: Assessing participative systems design: some
conclusions from an exploratory study. Inform Manage 1983, 6:13–32.
155. Hallberg N, Timpka T, Eriksson H: The medical software quality
deployment method. Methods Inform Med. 1999, 38:66–73.
156. Mendel P, Meredith LS, Schoenbaum M, Sherborne CD, Wells KB:
Interventions in organizational and community context: a framework
for building evidence on dissemination and implementation in health
service research. Adm Policy Ment Health. 2008, 35:21–37.
157. Nordenfelt L: On medicine and health enhancement – towards a
conceptual framework. Med Health Care Philos. 1998, 1:5–12.

References
78
158. Brug J, Hopsers HJ, Kok G: Differences in psychosocial factors and fat
consumption between stages of change for fat reduction. Psychol Health.
1997, 12(5):719–727.
159. Bagozzi RP, Edwards EA: Goal setting and goal pursuit in the
regulation of body weight. Psychol Health. 1998, 13(4):593–621.