operative treatment of cervical spondylotic myelopathy
TRANSCRIPT
COPYRIGHT © 2006 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
1619
Current Concepts Review
Operative Treatment of Cervical Spondylotic Myelopathy
BY RAJ D. RAO, MD, KRISHNAJ GOURAB, MD, AND KENNY S. DAVID, MD
➤ Nonoperative treatment with collar immobilization and modification of activities improves functional status in se-lected patients with mild cervical spondylotic myelopathy. Careful monitoring of these patients is necessary asneurological deterioration can occur in spite of this treatment.
➤ Early operative management is beneficial for most patients with moderate or severe myelopathy.
➤ The primary aims of operative intervention for the treatment of cervical spondylotic myelopathy are decompressionof the spinal cord and stabilization of levels at which excessive motion may be contributing to the myelopathy.
➤ Anterior operative approaches are preferred in patients with compression of the spinal cord at one, two, or threedisc levels and those with loss of cervical lordosis. A higher rate of approach and graft-related complicationsgenerally favor a posterior approach when more than three levels are involved.
➤ Appropriate operative management results in satisfactory recovery from myelopathy in most cases, with im-provement more likely in patients who have operative treatment earlier in the course of the disease and in thosewith less comorbidity.
Cervical spondylotic myelopathy is a leading cause of spinalcord dysfunction in the adult population. Affected patientsrepresent a large subset of individuals who undergo operativetreatment of degenerative cervical conditions. In a study of450 patients undergoing anterior neck surgery for the treat-ment of degenerative disc disease, 61% presented with radicu-lar symptoms, 16% had pure myelopathic symptoms, and theremaining 23% had a combination of myelopathy andradiculopathy1.
The subtle clinical findings of early cervical spondyloticmyelopathy make diagnosis difficult, and true natural historystudies are unavailable. The patients or their relatives noticeincreasing awkwardness with gait and balance that they at-tribute to old age or arthritis of the lower extremity joints. Pa-tients may report an insidious onset of clumsiness or diffusenumbness in the hands, resulting in worsening of handwritingor other fine motor skills and difficulty with grasping or hold-ing. Physical examination shows exaggerated deep tendonreflexes, clonus, diminished superficial reflexes, and the pres-ence of pathologic reflexes. Spasticity, motor weakness, andloss of proprioception contribute to the functional disabilityof the upper and lower limbs. Severely affected individuals arequadriparetic or quadriplegic when first seen2. In an effort todescribe the natural history of this condition, Clarke and Rob-inson described the progression of disease in a group of 120patients (including thirty-seven patients who did not receive
treatment, twenty-nine patients who were treated medically,and an additional fifty-four patients) until the time of sur-gery3. Medical treatment consisted of varying periods of collarimmobilization, bed rest, and neck traction. The authorsfound that 5% of their patients had a rapid onset of symptomsfollowed by a long period of quiescence, 20% showed gradualbut steady progression of signs and symptoms, and 75%showed stepwise deterioration of clinical function with inter-vening variable periods of quiescent disease. Operative inter-vention is a consideration in the cases of most patients withclinically evident cervical spondylotic myelopathy, given therisk of neurologic deterioration. However, a standard treat-ment algorithm is precluded by (1) the variability in initialpresentation and subsequent course of the disease and (2) thelack of prospective, randomized studies that stratify treat-ment options for patients with varying severity of myelopathy.A prospective multicenter study conducted by the CervicalSpine Research Society demonstrated that operative and non-operative treatment were equally prescribed to patients withcervical spondylotic myelopathy even when the difference be-tween the two groups with regard to the clinical stage at thetime of presentation was “not unusually large.”4
The operative treatment of degenerative cervical disor-ders has evolved over the past seventy-five years. Mixter andBarr initially described a posterior approach in 1934, whenthey performed cervical laminectomy5. In the 1970s, various

1620
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
techniques of laminoplasty were introduced as a less destabi-lizing alternative to laminectomy6,7. Concurrently, the 1950ssaw increasing popularity of anterior procedures, with Robin-son and Smith8, Cloward9 and Simmons and Bhalla10 describ-ing anterior decompression and fusion techniques involvingthe use of iliac crest bone graft. Increasing familiarity with theanterior approach led to the development of multiple-levelanterior reconstruction and instrumentation. The goals ofoperative treatment with all of these techniques have been toprevent deterioration and, in some cases, to reverse the myel-opathy by (1) decompressing the spinal cord, (2) stabilizingthe spine in cases in which segmental motion may be a con-tributory factor, and (3) secondarily improving cord perfusionby decompressing obstructed spinal vessels.
Nonoperative Treatment of Cervical MyelopathyPatients with mild myelopathy are occasionally offered a trialof observation or nonoperative management, but nonopera-tive management is generally not successful in reversing orpermanently halting the progress of cervical spondylotic myel-opathy. In a prospective, randomized study of patients with“mild to moderate” cervical spondylotic myelopathy, Kadankaet al. reported similar outcomes following either conservative oroperative treatment after a follow-up period of three years11.Conservative treatment consisted of intermittent cervical im-mobilization in a soft collar, anti-inflammatory medicationsand bed rest, active discouragement of high-risk activities, andavoidance of physical overloading, exposure to cold, movementon slippery surfaces, manipulation therapies, and vigorous orprolonged flexion of the head. In a more recent study, the au-thors reported that a greater anteroposterior diameter of thespinal canal, larger transverse area of the spinal cord, and oldage were associated with a better response to this conservativetreatment12. Matsumoto et al. retrospectively reviewed the re-sults of conservative management in a study of twenty-sevenpatients with mild to moderate myelopathy due to soft discherniation13. Conservative treatment consisted of cervical brac-ing with a rigid neck brace and restriction of activities. Seven-teen (63%) of the twenty-seven patients had improvement orstabilization of clinical function, and an operation was avoidedover a mean duration of follow-up of 3.9 years. Ten (37%) ofthe twenty-seven patients showed neurologic deterioration orfailed to show an improvement and were offered an operationat a mean of nine months after the time of presentation. Opera-tively and nonoperatively managed patients showed similar re-covery at the time of the final follow-up, suggesting that a trialof nonoperative treatment did not decrease the potential for ul-timate recovery of patients with mild myelopathy.
Indications for Operative Treatment of Cervical MyelopathyPatients with severe or progressive clinical myelopathy withconcordant radiographic evidence of spinal stenosis are candi-dates for operative intervention. For patients with clinically evi-dent but nonprogressive disease, there are no clearly establishedguidelines with regard to the indications for operative treatment.
Most studies on the operative treatment of cervical spondyloticmyelopathy have been retrospective in nature. A constellation offindings, including patient symptoms, alteration in gait, otherevidence of long tract dysfunction, decreased function in theupper or lower extremities, the duration of symptoms, comor-bidities, and radiographic findings all contribute to the surgeon’sdecision to recommend operative intervention.
The Role of Clinical Findings in Indicating Operative TreatmentSymptoms and signs of long tract dysfunction, including mo-tor weakness, hyperreflexia, spasticity, ataxia, pathologic re-
TABLE I Japanese Orthopaedic Association Criteria6 for the Evaluation of Operative Results in Patients with Cervical Myelopathy*
I. Upper extremity function
Impossible to eat with either chopsticks or spoon (0 points)
Possible to eat with spoon, but not with chopsticks (1 point)
Possible to eat with chopsticks but inadequate (2 points)
Possible to eat with chopsticks but awkward (3 points)
Normal (4 points)
II. Lower extremity function
Impossible to walk (0 points)
Need cane or aid on flat ground (1 point)
Need cane or aid only on stairs (2 points)
Possible to walk without cane or aid, but slow (3 points)
Normal (4 points)
III. Sensory
Upper extremity
Apparent sensory loss (0 points)
Minimal sensory loss (1 point)
Normal (2 points)
Lower extremity
Apparent sensory loss (0 points)
Minimal sensory loss (1 point)
Normal (2 points)
Trunk
Apparent sensory loss (0 points)
Minimal sensory loss (1 point)
Normal (2 points)
IV. Bladder function
Complete retention (0 points)
Severe disturbance (1 point)
Inadequate evacuation of bladder
Straining
Dribbling of urine
Mild disturbance (2 points)
Urinary frequency
Urinary hesitancy
Normal (3 points)
*Total normal score = 17 points.

1621
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
flexes, and myelopathic hand findings, are evaluated in combi-nation to help to determine whether operative intervention isindicated14. In a study of 146 patients who underwent an opera-tion for the treatment of myelopathy, motor weakness (129 pa-tients; 88.4%) and spasticity (115 patients; 78.8%) were the twomost common preoperative findings15. Wada et al. used a com-bination of neurological symptoms, preoperative functionalscoring with use of the Japanese Orthopaedic Association(JOA) system (Table I), and radiographic findings to deter-mine the need for operative treatment16. The most commonlyseen myelopathic symptoms in that series were clumsiness ofthe hands, unsteady gait, and numbness in the extremities.Operative treatment was recommended when these symptomswere present in combination with a JOA score of <13 pointsand spinal cord compression on imaging studies.
Development of a myelopathic gait is an important in-dication for operative intervention. The gait abnormality maybe spastic or ataxic, depending on whether the lateral or pos-terior cord is primarily affected. Bohlman, in a study of seven-teen patients who underwent an operation for the treatmentof cervical myelopathy, reported gait disturbances in all seven-teen patients, with fifteen patients demonstrating stumblingand falling17. Okada et al. reported on thirty-seven patientswith either myelopathy (thirty-two patients) or myeloradicul-opathy (five patients) who underwent anterior corpectomy18.All patients had sensory abnormalities and hyperreflexia, butthe authors used gait disturbance as the primary indicationfor operative treatment.
Axial pain along the posterior part of the neck or radiat-ing into the shoulder girdles is frequently present in patientswith cervical spondylotic myelopathy and does not play a ma-jor role in indicating operative treatment. The axial pain inthese patients may represent muscle fatigue or referred painfrom degenerative changes in the spinal column, or it may be amanifestation of upper cervical radiculopathy. The Lhermittesign, or shock-like sensations in the trunk and legs provokedby neck movement, coughing, or sneezing, is found in somepatients with cervical spondylotic myelopathy.
The Role of Duration of Symptoms in the Operative DecisionProlonged compression of the spinal cord can result in irre-versible histological and physiological changes such as intra-neural fibrosis, demyelination, and loss of neurons within thespinal cord19. The results of operative treatment generally arebetter in patients who undergo decompression early ratherthan late20,21. In a prospective study of 146 patients with cervi-cal spondylotic myelopathy, Suri et al. noted that patients withless than a one-year duration of symptoms showed signifi-cantly greater motor recovery following operation than didthose with a longer duration of symptoms (p < 0.05)15. Tanakaet al., in a study of forty-seven patients who were more thansixty-five years old, found that the preoperative duration ofsymptoms strongly influenced recovery of function followingoperative treatment20. The authors recommended that decom-pressive surgery should be attempted even in patients who are
more than eighty years old, provided that the duration ofsymptoms is less than three years, the inability to walk hasbeen present for less than three months, and the patient isphysically able to undergo an operation. In another study, im-provement in gait following laminoplasty was reported in92% (eleven) of twelve patients in whom symptoms had beenpresent for less than eighteen months, as opposed to 77%(ten) of thirteen patients with a longer duration of symptomsbefore the operation21.
In contrast, some authors have reported no correlationbetween the duration of preoperative symptoms and the clini-cal outcome following an operation. Arnasson et al. reportedon a group of thirty-eight patients with cervical myelopathywho underwent anterior decompression with or without fu-sion (five patients), laminectomy (twenty-nine patients), ornonoperative treatment (four patients)22. The authors foundthat the clinical outcome following operative intervention wasnot influenced by the duration of preoperative symptoms.
Radiographic Factors Indicating Operative ManagementMeasurement of the midsagittal canal diameter may be carriedout on plain radiographs (Fig. 1, a) or, more accurately, on ax-ial computed tomography images or magnetic resonance im-ages. The normal midsagittal canal diameter from C3 to C7 is17 to 18 mm, and patients with an osseous canal measuring<13 mm are considered developmentally stenotic23. Many pa-tients with symptomatic cervical spondylotic myelopathy havesome degree of developmental osseous canal stenosis, with su-perimposed degenerative changes at the facet joints, discs, andligamentum flavum that further contribute to canal and neu-roforaminal narrowing. Static or dynamic translation betweenvertebral bodies may further decrease the available canal areaand precipitate the development of myelopathy (Fig. 1). Al-though evidence to support these radiographic criteria in thedegenerative cervical spine is lacking, vertebral olisthesis of>3.5 mm between adjacent cervical vertebral bodies fre-quently is used in clinical practice as an indicator of excessivetranslation between the vertebral bodies, favoring surgical in-tervention. So-called dynamic stenosis is a more recently de-scribed measure of canal space and mobility and is assessedon a lateral radiograph made with the neck in extension. Adistance of <12 mm between the posteroinferior lip of thevertebral body and the anterosuperior margin of the immedi-ately caudal lamina is suggestive that the spinal cord is beingpinched with intersegmental motion.
Magnetic resonance imaging may show focal areas ofsignal changes within the cervical spinal cord at or adjacent tosites of maximal compression. Low-signal abnormalities onT1-weighted images and high-signal abnormalities on T2-weighted images have both been associated with greater clinicaldisability or decreased neurologic recovery following de-compressive surgery15,24,25. These changes, generally referred toas myelomalacia, may represent intraspinal edema, neuronaldeath, proliferation of neuroglial cells, and/or demyelination.Earlier operative intervention may be indicated for patients

1622
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
with these changes in an attempt to halt or reverse the changeswithin the substance of the spinal cord24,26.
Comorbidity Affecting Operative InterventionThe patient’s overall medical condition should be considered inthe decision leading to operative treatment because outcome isinfluenced by underlying medical comorbidity, particularly inelderly patients. Hypertension, diabetes mellitus, coronary in-sufficiency, cardiomyopathy, pulmonary problems, previouscerebral infarction, gastrointestinal ulcers, and benign pros-tatic hypertrophy may be present; in two previous studies, suchcomorbidities were found in up to 70% (fourteen) of twentypatients with an age of more than seventy years for whom oper-
ative intervention was being considered for the treatment ofcervical spondylotic myelopathy27,28. Close medical monitoringin the perioperative period is essential, but surgery can never-theless result in aggravation of the underlying medical condi-tions or delirium in these patients27. Functional deterioration inthe postoperative period may also result from cerebral infarc-tion or aggravation of diabetes mellitus28. Age-related changesin the spinal cord, coexistent osteoarthritis of the lower limbs,lumbar spinal stenosis, and peripheral neuropathy can hamperrecovery following operative treatment28,29. Although the rates offunctional recovery are lower in older patients27,28, the potentialfor neurologic stabilization or improvement makes operativetreatment a consideration in this age-group even in the pres-ence of comorbid factors20,27,28.
Choosing the Operative ProcedureThe primary goal of surgical intervention in patients with cer-vical spondylotic myelopathy, regardless of whether an ante-rior or posterior approach is used, is expansion of the spinalcanal. Appropriate and early decompression restores and im-proves spinal cord morphology23, reverses cord edema15,30, andlikely improves blood supply to the cord, aiding neurologicalrecovery. The secondary goals of operative treatment are toachieve a successful fusion where abnormal segmental mobil-ity may contribute to repeated injury of the cord and to pre-vent development of late deformity that can compromise thesurgical outcome.
Both anterior and posterior approaches to the cervicalspine allow decompression of the spinal cord and nerve roots,correction of deformity, and stabilization of the spinal col-umn. The choice between an anterior, posterior, or combinedapproach for decompression of a stenotic spinal canal is basedprimarily on (1) the sagittal alignment of the spinal column,(2) the extent of disease, (3) the location of compressive ab-normality, (4) the presence of preoperative neck pain, and (5)previous operations. Additional considerations that influencethe choice of approach include (1) the increased risk of post-operative dysphagia and laryngeal nerve injury followingmultiple-level or prolonged anterior surgery, (2) injury to thestabilizing posterior muscular and ligamentous structureswith the posterior approach, and (3) inadequate exposure atthe C7-T1 level through the anterior approach in individualswith a short, muscular neck.
Role of Cervical Spine Alignment in Selection of Operative ApproachPosterior decompression for the treatment of myelopathy isgenerally contraindicated for patients who have neutral or ky-photic sagittal alignment of the cervical spinal column. Lami-nectomy or laminoplasty in a patient with a kyphotic orneutrally aligned spinal column will not allow posterior trans-lation of the spinal cord away from the anterior compressiveabnormality. Sodeyama et al. showed that the peak postopera-tive dorsal translation of the spinal cord was greatest (peakshift, 3.1 mm) in patients who had a lordotic spinal curve, less(peak shift, <3 mm) in patients who had a straight spine, and
Fig. 1
Illustration depicting the radiographic criteria used in the assessment
of cervical stenosis and myelopathy. a, The midsagittal diameter of the
spinal canal is measured as the distance from the middle of the dorsal
surface of the vertebral body to the nearest point on the spinolaminar
line. Patients in whom the osseous canal measures <13 mm are con-
sidered to be developmentally stenotic. b, A distance of <12 mm from
the posteroinferior corner of a vertebral body to the anterosuperior
edge of the lamina of the immediately caudal vertebra with the neck in
extension is suggestive of dynamic stenosis. c, Olisthesis of >3.5 mm
is a measure of excessive translation between the vertebral bodies.
The signal changes within the substance of the spinal cord, noted on
T1 and T2-weighted magnetic resonance imaging in some patients, are
represented diagrammatically.

1623
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
least (peak shift, <2 mm) in patients who had a kyphotic or anS-shaped cervical spinal curve31. Better recovery of myelopathyhas also been reported following laminoplasty in patientswithout preoperative kyphosis32.
Kawakami et al. reported that preoperative and postop-erative cervical spine sagittal alignment had no bearing onpostoperative recovery of myelopathy33. The authors recom-mended anterior discectomy and fusion for patients with oneor two-level disc involvement without developmental canalstenosis (anteroposterior diameter, ≥ 13 mm) and lamino-plasty for those with involvement of three levels or more andfor those with developmental stenosis (even if they had a one-level lesion). Chiba et al. hypothesized that slack in the spinalcord induced by decreased disc height in patients with multiple-level cervical spondylotic myelopathy allowed for an accept-able recovery following posterior decompression, even in thepresence of a kyphotic or straight spine34.
Role of Extent of Disease InvolvementFor patients with one or two-level involvement, most sur-geons prefer an anterior procedure33,35. Yonenobu et al., in astudy of patients with cervical spondylotic myelopathy, re-ported that patients with one or two-level involvement weremanaged with anterior cervical discectomy or corpectomy,patients with involvement of four levels or more were man-aged with laminectomy, and patients with involvement ofthree levels were managed with any of the three procedures35.Patients who underwent corpectomy maintained the gain infunctional recovery better than those who underwent eitherof the other two procedures. The authors recommended thatcorpectomy should be used for the treatment of spondylosisinvolving as many as three levels and that laminectomy bereserved for the treatment of spondylosis involving four lev-els or more.
Corpectomy may be considered (1) for a patient withdevelopmental stenosis as evidenced by an osseous antero-posterior canal diameter of <13 mm, (2) for a patient with alarge posterior osteophyte adjacent to the end plate, (3) for apatient who has a free disc fragment that has migrated poste-rior to the vertebral body, and (4) as an alternative to multiple-level interbody fusion to reduce the number of requiredfusion surfaces. Correction of a fixed kyphotic deformity inthe cervical spine can be more reliably achieved with corpec-tomy than with multiple-level anterior cervical discectomyand fusion.
The prevalence of dysphagia and graft-related compli-cations increases as the number of levels that are included inan anterior fusion increases, and this fact must be kept inmind when deciding on the approach. Persistent difficultywith swallowing or potentially substantial voice changes canoccur in some patients following prolonged or difficult ante-rior surgery.
Role of Dimensions of the Cervical Spinal CanalSevere developmental stenosis involves the entire cervicalspine and generally requires a posterior approach. Sodeyama
et al. recommended posterior decompression of the cervicalspinal cord in patients with myelopathy who had a spinal ca-nal diameter of <11 mm and multiple-level impingement of thespinal cord31. Conversely, Kadoya et al. thought that multiple-level anterior discectomy and fusion accompanied by osteo-phyte removal provided satisfactory decompression of thespinal cord in patients with myelopathy even in the presenceof a congenitally stenotic canal (<12 mm)36. The authors basedtheir choice on myelographic findings, which showed that thecord compression was primarily due to the osteophytes andnot to the canal stenosis.
Role of the Location of the AbnormalityThe choice between an anterior and a posterior approach forthe treatment of a stenotic spinal canal should take into con-sideration the anatomic location of the abnormality. Ante-rior approaches allow good visualization of abnormalitiesthat are located ventral to the cord and obviate the need to workaround the cord. Herkowitz et al. reported an excellent orgood result in ten (91%) of eleven patients undergoing ante-rior discectomy and fusion for the treatment of myelopathyor axial neck pain resulting from central soft disc hernia-tions37. Posterior compression of the spinal cord resultingfrom buckling of the ligamentum flavum or shingling of thelaminae in a patient with hyperlordosis favors a posteriorapproach31.
Role of Preoperative Neck PainPreoperative neck pain is a relative contraindication to lami-noplasty. Disruption of the posterior paraspinal musculaturefrom a posterior approach can aggravate axial neck pain.Ratliff and Cooper, in a review of the literature on lamino-plasty, reported that the postoperative prevalence of neckpain ranged from 6% to 60% among different series and sug-gested that the true prevalence may actually be higher asneck pain was frequently not reported in the studies thatwere reviewed38. Axial pain is not a major concern followinganterior surgery.
Role of Previous SurgeryIn patients who have undergone previous operations on thecervical spine through an anterior or posterior approach, revi-sion surgery that is performed through an alternate approachavoids having to dissect through scar tissue and disrupted ana-tomic planes. Scar tissue tethering the esophagus, trachea, andlaryngeal neurovascular structures makes an injury to thesestructures more likely with repeat intervention. Additionalfactors that should be considered when deciding on the ap-proach for revision surgery include the time that has elapsedsince the previous operation, the maturity of scar tissue, andthe ease of performing the planned intervention through theapproach. Revision anterior surgery is best carried outthrough the previous approach when feasible. When a con-tralateral anterior approach is contemplated, preoperativelaryngoscopy will rule out subclinical vocal cord paresis on thepreviously treated side.

1624
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
Operative Options for and Issues Related to Anterior Surgical Approaches to Cervical Spondylotic MyelopathyAnterior Cervical Discectomy and FusionAnterior cervical discectomy and fusion allows for theremoval of disc material and posterior osteophytes impingingon the spinal cord and nerve roots at or immediately adjacentto the level of the disc space (Fig. 2, A). The cartilaginous endplate is completely removed, but we prefer to maintain the in-tegrity of the thin osseous end plate because we think that thiscontributes to the mechanical stability of the graft-host inter-face and helps to maintain lordotic alignment. Distraction ofthe disc space results in indirect decompression of the fora-men and canal to a varying degree and is followed by insertionof an appropriately sized bone graft into the interspace. Therecommended height of the graft in most cases is 2 mm morethan the initial disc height in order to avoid the loss of heightthat sets in after graft incorporation39.
The advantages of the procedure are the ability to de-compress the anterior spinal cord through an approach along
fascial planes, the relative preservation of the stability of thespinal column, and the low prevalence of graft extrusion ormigration. Anterior cervical discectomy and fusion requiresless exposure of the spinal cord than corpectomy does, but thedecreased visualization of the spinal cord may increase the riskof incomplete decompression of the cord or injury to the cord.Anterior cervical discectomy and fusion is not recommendedas the primary treatment for patients with severe congenitalcanal stenosis because the overall anteroposterior diameter ofthe canal is not increased by the procedure.
Cervical CorpectomyThe term subtotal corpectomy refers to removal of a 15 to 19-mm anterior midline trough in the vertebral body down to theposterior longitudinal ligament or dura, with removal of thecephalad and caudad discs (Figs. 2, B and Figs. 3-A through 3-G). Corpectomy allows expansion of a narrow osseous canaland allows for simultaneous removal of large osteophytesfrom the vertebral end plates impinging on the spinal cord ornerve roots. Undercutting large osteophytes from adjacent
Fig. 2
Illustration depicting common anterior procedures used in cervical myelopathy. A, Anterior cervical
discectomy and insertion of a bone spacer for fusion. B, Anterior cervical corpectomy and insertion
of a bone strut graft. C, Anterior cervical discectomy followed by insertion of a bone spacer for fu-
sion and anterior plating. D, Anterior cervical corpectomy, strut graft insertion, and anterior plating.

1625
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
levels is also safer through a corpectomy trough as opposed toworking through a narrow disc space with limited visualiza-tion. The lateral extent of decompression is limited by the fo-ramen transversarium, which houses the vertebral artery.Computerized tomography shows that a total central decom-pression of approximately 15 mm at C3 to 19 mm at C6 pro-vides a safety margin of 5 mm to the medial border of theforamen transversarium40,41. The superior surfaces of the sub-axial cervical vertebrae are marked by an upward ridge ontheir lateral and posterior lateral margins, known as the un-cus. Anatomic landmarks such as the medial margin of theuncus, the medial margin of the longus colli muscle, and thenatural curve of the vertebral end plate can be used to main-tain midline orientation. This helps to avoid inadvertent ver-tebral artery injury resulting from lateral wall violation.
Intraoperative indicators of an adequate decompressionare (1) a 15 to 19-mm-wide trough that allows for the place-ment of an appropriately sized graft or cage, (2) symmetricproximity to the lateral edges of the disc space as identified bythe uncus, and (3) visual confirmation of spinal cord decom-pression. Ultrasonography is used by some surgeons to assessthe adequacy of decompression, with a clear spinal cord imageon the axial projection being a demonstrable end point of ade-quate anterior decompression42,43.
Various modifications of the corpectomy techniquehave been described. For patients without developmentalstenosis of the canal but with large osteophytes adjacent to thedisc space at one level, some authors have combined a discec-tomy with limited resection of the adjacent vertebral body14.The authors of one report described resection of the anteriortwo-thirds of the vertebral body44. Those authors suggestedthat this partial anterior corpectomy allowed greater intraop-erative visualization of the interface between the adjacent discsand the posterior longitudinal ligament, allowed easier re-moval of osteophytes, and decreased the number of surfaces atwhich fusion was required in comparison with a multiple-level discectomy and fusion. Combining a corpectomy with anadjacent discectomy may avoid the biomechanical instabilityassociated with multiple-level corpectomies.
Resection of Posterior Osteophytes as Part of the DecompressionResection of posterior osteophytes has been reported to allowearlier decompression of the spinal cord and improvedrecovery36. Resection of posterior and lateral osteophytes alsomay allow more reliable improvement in patients with associ-ated radicular symptoms. However, the removal of osteophytesis associated with an increased risk of injury to the spinal cord.Yonenobu et al. reported worsening of myelopathy in one ofseventy-five patients as a result of cord damage that occurred inassociation with the resection of osteophytes during anteriorcervical discectomy and fusion45. The authors recommendedcorpectomy over anterior cervical discectomy and fusion forpatients with posterior osteophytes that are large enough to re-quire removal.
There is conflicting information on whether osteophytes
will resorb following a solid fusion. Connolly et al.46 and Rob-inson et al.47 reported complete resorption of osteophytesfollowing a solid fusion. Conversely, Stevens et al.48 reviewedcomputerized tomographic myelograms for fifty-three patientstwelve years following anterior interbody fusion and reportedthat osteophyte resorption did not occur in any patient. Theyrecommended that all osteophytes should be systematically re-moved during the operation to minimize the chances of persis-tent symptoms.
Removal of the Posterior Longitudinal Ligament as Part of the DecompressionRemoval of a thickened or ossified posterior longitudinal liga-ment during anterior cervical discectomy and fusion allows formore thorough decompression but increases the risk of cordcontusion and postoperative hematoma1,17. An intact posteriorlongitudinal ligament contributes to the stability of the spinalcolumn and adds a margin of safety by helping to prevent graftextrusion posteriorly into the spinal cord. Yamamoto et al. re-ported the presence of a disc fragment behind the posterior lon-gitudinal ligament in three (5%) of fifty-five patients49. If a rentin the posterior longitudinal ligament is noted during the oper-ation, or if imaging studies suggest that there is a fragment be-hind the posterior longitudinal ligament, resection of theposterior longitudinal ligament allows for the performance of asafe exploration to rule out persistent compression of the spinalcord and/or nerve roots by an extruded disc fragment.
Addition of Levels with Mild Radiographic Findings to the OperationWith multiple-level degenerative disc changes, a single level thatis responsible for the myelopathy frequently cannot easily beidentified. In addition, there is concern that untreated segmentsshowing mild degenerative changes or intervertebral translationadjacent to the site of the proposed operative intervention mayresult in recurrent postoperative myelopathic changes. For thesereasons, some authors have suggested that all levels of radio-graphically demonstrable compression should be dealt with atthe time of surgery35,42. Shoda et al. recommended extending thefusion to any adjacent segment that displayed dynamic stenosisin addition to the primary stenotic levels50. Tani et al. attemptedto minimize perioperative complications in patients with multi-ple-level disease by limiting operative intervention to a singlemost symptomatic level51. Those authors used intraoperativespinal cord evoked potentials to identify the disc level that wascausing the greatest conduction delay. This approach risks leav-ing behind clinically important compressive abnormalities inuntreated areas. The benefits of including all levels must beweighed against the increased time and risk of the operation.
Bone Graft Options Following Discectomy and CorpectomyAutogenous iliac crest bone traditionally has been the pre-ferred choice of bone graft for multiple-level anterior cervicaldiscectomy and fusion. A tricortical horseshoe-shaped graft isharvested from the iliac crest with use of a low-speed oscillat-

1626
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
Fig. 3-A
Figs. 3-A through 3-G A forty-seven-year-old woman presented
with a six-month history of neck pain, numbness in both upper ex-
tremities, and profound weakness with hand function bilaterally.
Figs. 3-A through 3-E Preoperative T2-weighted sagittal image
(Fig. 3-A) and axial images at C3-C4 (Fig. 3-B), C4-C5 (Fig. 3-C),
C5-C6 (Fig. 3-D), and C6-C7 (Fig. 3-E), showing severe stenosis,
particularly at C4-C5 and C5-C6, resulting from a combination of
spondylotic changes and superimposed disc protrusion. Signal
changes within the substance of the spinal cord can be seen pos-
terior to the C4-C5 disc space.
Fig. 3-B
Fig. 3-C
Fig. 3-D
Fig. 3-E

1627
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
ing saw and is inserted into the interspace with the corticalportion facing anteriorly. The use of allograft bone avoids themorbidity associated with the harvesting of autogenous bonebut traditionally has been associated with higher rates of non-union following arthrodeses involving more than one level52.Samartzis et al. recently described equivalent rates of fusion inassociation with allograft and autograft when used for proce-dures involving as many as three levels that were performedwith current surgical techniques and anterior cervical plates53.Those authors suggested that preparation of the end plates,sizing of the graft, recessing the graft 2 mm from the anteriormargin of the vertebral body, and segmental screw fixationwere more important than the type of graft used. The use ofstructural supports such as metallic cages (Fig. 3-F) or syn-thetic spacers in conjunction with local autograft or allograftavoids the morbidity associated with the harvesting of autoge-nous bone, but long-term results will be needed before thismethod achieves general acceptance.
Autogenous iliac crest bone is also the preferred graftchoice to span the defect created by a one-level or two-level cor-pectomy. For patients with longer corpectomy defects or thosein whom the iliac crest is mechanically insufficient, a fibularstrut is preferred. A fibular allograft avoids donor-site morbid-ity, reduces operative time and intraoperative blood loss, andhas been shown to be biomechanically superior to the iliac crestwhen tested under axial loading54. The risk of disease transmis-sion is low55.
Graft failure following anterior discectomy or corpec-
tomy occurs through displacement, fracture, resorption, col-lapse, or penetration of the graft into the cephalad or caudadvertebral bodies. Autogenous iliac crest graft has been associ-ated with rates of collapse ranging from 4% (four of 100)56 to14% (nine of sixty-three)57. Allograft generally has been associ-ated with higher rates of collapse. Brown et al. reported collapsein 28% (fifteen) of fifty-three patients who were managed withiliac crest allograft as compared with 16% (seven) of forty-fivepatients who were managed with iliac crest autograft57. Thenumber of graft-related complications increases as the numberof levels undergoing corpectomy increases58. Anterior platingcan help to decrease the prevalence of graft displacement fol-lowing multiple-level corpectomy, but some authors neverthe-less have recommended second-stage posterior stabilizationfollowing a corpectomy of three levels or more59,60.
Role of Anterior Plating in Reconstruction of the Cervical Spinal Column Following Anterior Cervical Discectomy and Fusion or CorpectomyPlate fixation following anterior cervical discectomy and fu-sion or cervical corpectomy (Fig. 2, C and D) does not addsubstantially to the duration of an operation or the prevalenceof complications. Anterior plating improves the rate of fusion,reduces the length and type of postoperative immobilization,reduces the prevalence of graft-related complications, andleads to less postoperative kyphosis, particularly in patientsundergoing two or more levels of anterior cervical discectomyand fusion61-63. An appropriate plate length is selected to main-
Fig. 3-F
Figs. 3-F and 3-G Radiographs made after the patient was managed with corpectomy of the C5 and C6 vertebral bodies,
strut-grafting with use of a titanium mesh cage packed with local autogenous bone, and the application of an anterior cervi-
cal plate from C4 to C7.
Fig. 3-G

1628
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
tain a minimum distance of 5 mm between the ends of theplate and the adjacent discs. This helps to decrease adjacentdisc level ossification64. Segmental screw fixation should beobtained when possible, and all screws should be locked to theplate53. Dynamic or semiconstrained devices that allow slidingor toggling of the screw within the plate were developed to re-duce stress-shielding of the graft and to allow for increasedcompressive forces on the graft. The inherent lack of longitu-dinal rigidity of dynamic systems can be a disadvantage insome situations, allowing migration of the graft into adjacentend plates or drifting of the plate toward adjacent disc spaces.Drawbacks of anterior plate fixation include (1) difficultieswith fixation in osteoporotic bone, (2) the risk of esophagealinjury or airway obstruction from loose and migrating im-plants, (3) increased cost, and (4) the slight increase in opera-tive duration, blood loss, and intraoperative risk that theadded procedure entails.
When plating has been performed following single-levelanterior cervical discectomy and fusion, some authors have re-ported no improvement in fusion rates or overall clinicaloutcome61,65. Conversely, Wang et al. reported less graft subsi-dence, less segmental kyphosis, a lower prevalence of pseudar-throsis (4.5% [two of forty-four] compared with 8.3% [three ofthirty-six]; p = 0.653), and a higher percentage of good or excel-lent outcomes when patients who had been managed with plat-ing were compared with patients who had not been managedwith plating66. In another study, computerized analysis of thelateral radiographs for fifty-one patients who had had single ormultiple-level anterior cervical discectomy and fusion demon-strated a significant (p = 0.0001) beneficial effect of the plate inmaintaining sagittal alignment postoperatively67.
Anterior cervical plating has been shown to decrease theprevalence of graft-related complications following corpec-tomy. Epstein compared patients who underwent single-levelcorpectomy with and without plating. Among the forty-eightpatients who were managed without an anterior cervical plate,73% went on to have fusion whereas 10.3% required reopera-tion for graft-related complications or a pseudarthrosis68. Amongthe eight patients who were managed with an anterior cervicalplate, there were no graft-related complications. However, onepatient had development of a pseudoarthrosis and under-went elective posterior wiring and fusion six months afterthe index procedure to prevent future plate loosening. Fail-ure rates of 50% (six of twelve)59 to 71% (five of seven)60 fol-lowing three-level corpectomy, grafting, and plating haveprompted some authors to recommend the addition of pos-terior instrumentation whenever three-level corpectomy andfusion are performed.
Success of Fusion Following Anterior Operative TreatmentFusion following anterior discectomy or corpectomy is deter-mined by the radiographic observation of bridging trabecu-lae across all graft-host bone interfaces, with no motion at thefused levels noted on dynamic radiographs. A change in in-terspinous distance on flexion and extension radiographs is
an accurate technique for detecting lack of fusion69,70. The rateof fusion following single-level anterior cervical discectomyand fusion generally ranges from 80% to 95% (88% of 202 inthe study by Cauthen et al.70, 90% [242 of 269] in the study byMartin et al.71, and 95% [thirty-nine of forty-one] in thestudy by Zdeblick and Ducker52). Some authors have reportedhigher nonunion rates following multiple-level anterior cer-vical discectomy and fusion, with the rates increasing as thenumber of fused levels increases. Bohlman et al. reported thatthe rate of fusion following anterior cervical discectomy andfusion without instrumentation was 89% (fifty-five of sixty-two) after one-level procedures, 73% (thirty-five of forty-eight) after two-level procedures, and 73% (eight of eleven)after three-level procedures, with a failure of fusion in the onepatient who underwent a four-level procedure69. The lowerfusion rate following operative intervention at multiple levelsis explained by the increased number of fusion interfaces, in-creased motion resulting from multiple discectomies, and in-creased compressive loads across multiple segments leadingto a higher rate of graft failure. More recent long-term studieshave demonstrated no significant difference (p > 0.05) in fu-sion rates in association with the use of either allograft or au-tograft at two and three levels with anterior discectomy andanterior plating53. Compared with multiple-level anterior cer-vical discectomy and fusion, anterior cervical corpectomy re-duces the number of surfaces at which fusion is required butcreates a mechanically more demanding environment for thegraft resulting from greater bone resection and graft lengths.In a retrospective review of 249 cases of anterior corpectomyover one to five vertebral levels with use of autogenous iliaccrest or fibular graft without instrumentation, Wang et al. re-ported fusion with no displacement of the graft in 94% (233)of their 249 patients58. The authors reported that graft dis-placement was directly related to the number of vertebralbodies removed, the use of longer grafts, and fusions endingcaudally at the C7 level.
Immobilization Following Anterior SurgeryFollowing anterior surgery, patients are immobilized in a cer-vical or cervicothoracic orthosis, depending on the numberof levels involved and the use of internal fixation. Whilesome authors have recommended immobilization in a softbrace for one or two weeks following a single level anteriordiscectomy and fusion with instrumentation65, most haverecommended the use of a rigid cervical orthosis for four tosix weeks. Some authors have recommended that patientsundergoing multiple-level corpectomy without internal fixa-tion should be immobilized in a halo orthosis until the fu-sion shows signs of consolidation58. We prefer to use internalfixation supplemented with a rigid cervicothoracic orthosisfor these patients. Skin under the brace should be checkedregularly for areas of breakdown, and halo pins should becleaned daily. These braces restrict the ability of the patientto look down at the feet, and myelopathic patients need to beparticularly careful during the first few days of brace wear toavoid falling.

1629
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
Fig. 4
Posterior Surgery in Cervical Spondylotic MyelopathyLaminoplastyLaminoplasty increases the effective di-ameter of the spinal canal from C3-C7by shifting the laminae dorsally withuse of either a so-called single doorwith a single lateral hinge or a doubledoor with lateral hinges on both sides(Fig. 4). In contrast to laminectomy, lami-noplasty retains a covering of posteriorlaminar bone and ligamentum flavumover the spinal cord, minimizes instabil-ity, limits constriction of the dura fromextradural scar formation72,73, and obvi-ates the need for fusion.
The single-door technique of lami-noplasty involves the creation of bi-lateral troughs at the junction of thelateral masses and the laminae with useof a 3 to 4-mm high-speed burr. On theside that is selected to be the hinge side,the trough stops just superficial to theanterior cortex of the lamina. On theopen side, the osteotomy is completedthrough the anterior cortex of the lam-ina with a burr or 1-mm Kerrison ron-geur. The ligamentum flavum betweenC2 and C3 and between C7 and T1 isthen divided, and the canal is expandedby lifting the C3 through C7 laminaedorsally as a block with use of the con-tralateral trough as the hinge (Fig. 4,A)74. For double-door laminoplasty, bi-lateral troughs are made at the junctionsof the lateral masses and the laminae andthe spinous process is osteotomized inthe midline. The two halves of the lam-ina are swung open using the lateraltroughs as hinges (Fig. 4, B). Propo-nents of the double-door technique citethe relative safety and ease of openingthe spinous process in the midline andthe lack of troublesome bleeding fromlaterally situated epidural veins as ad-vantages of this technique)75,76. Compar-ative studies of double and single-doorlaminoplasties have demonstrated nosignificant difference between the twotypes of procedures with regard to neu-rological outcomes75,76.
Earlier descriptions of lamino-plasty kept the door open with use ofsuture or wire tethering the spinousprocess to the hinge side facet joint orcapsular tissue74. More recent techniques
Illustrations depicting common techniques used for cervical laminoplasty. A, Single-door lamino-
plasty. Sutures are placed through the spinous process to the articular capsule on the hinge
side to hold the lamina elevated. B, Double-door laminoplasty. The spinous process is osteoto-
mized in the midline, and the two halves are pried open on laterally based hinges. Structural
bone graft or a spacer fills the defect between the split spinous processes and prevents clo-
sure of the laminoplasty doors. C, Single-door laminoplasty with use of bone graft or spacer to
prop the door open. D, Single-door laminoplasty with use of a laminoplasty plate. E, Unilateral
muscle-stripping approach to maintain the integrity of soft tissues on the contralateral side.
The laminae on one side are exposed with preservation of the nuchal, supraspinous, and inter-
spinous ligaments. The spinous processes are osteotomized at their bases and are reflected to
the intact side, allowing exposure of the posterior laminar bone. The arrows indicate the plane
of the osteotomy and exposure.
1630
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
Fig. 5-C
Fig. 5-A
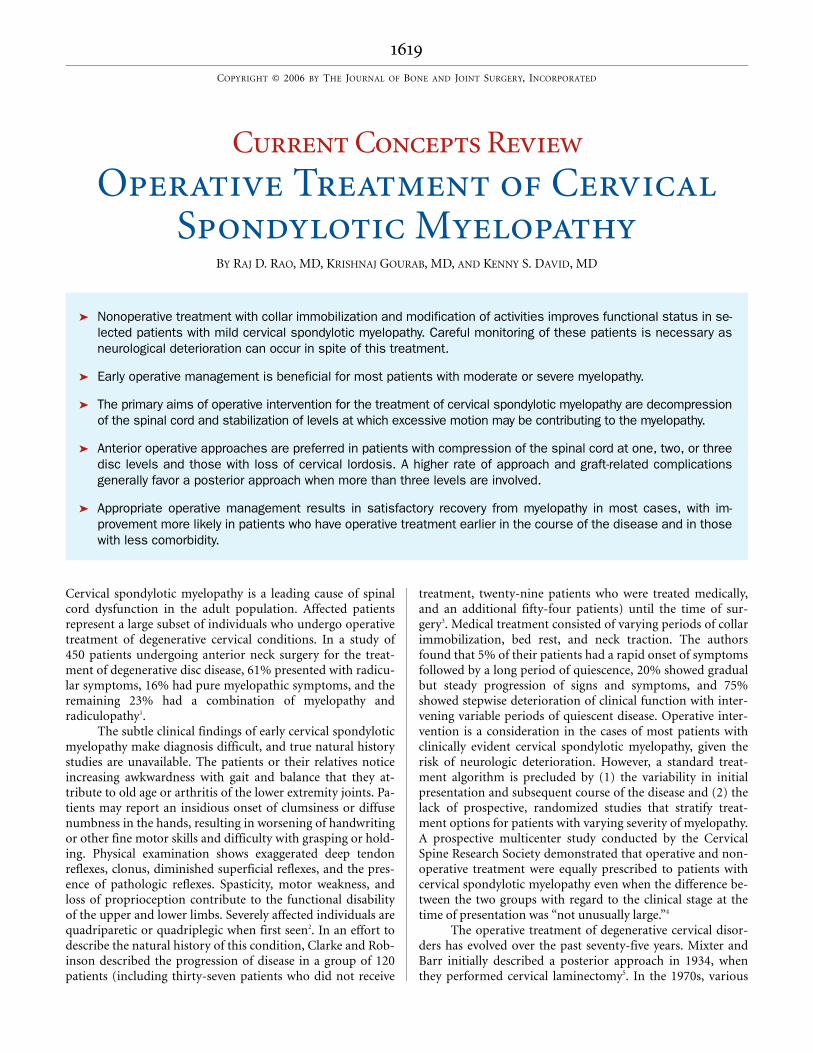
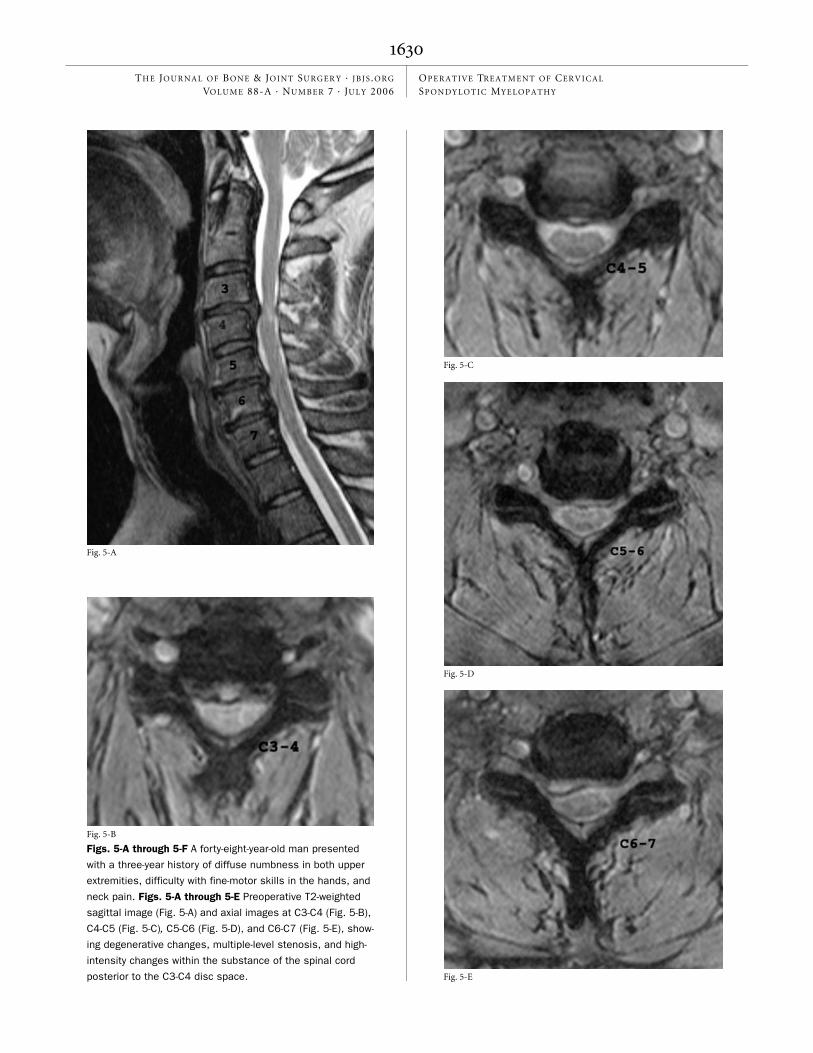
Figs. 5-A through 5-F A forty-eight-year-old man presented
with a three-year history of diffuse numbness in both upper
extremities, difficulty with fine-motor skills in the hands, and
neck pain. Figs. 5-A through 5-E Preoperative T2-weighted
sagittal image (Fig. 5-A) and axial images at C3-C4 (Fig. 5-B),
C4-C5 (Fig. 5-C), C5-C6 (Fig. 5-D), and C6-C7 (Fig. 5-E), show-
ing degenerative changes, multiple-level stenosis, and high-
intensity changes within the substance of the spinal cord
posterior to the C3-C4 disc space.
Fig. 5-B
Fig. 5-D
Fig. 5-E

1631
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
include insertion of an autogenous spinous process graft, al-lograft bone, or synthetic spacers to keep the door open (Fig.4, C). Fixation with use of miniplates fixed to the lamina andlateral mass has been reported by multiple authors, withoutmajor complications (Fig. 4, D and Figs. 5-A through 5-F)77-79.
LaminectomyLaminectomy is a useful alternative for multiple-level decom-pression in patients with preserved cervical lordosis, particu-larly elderly patients, in whom comorbidities increase theoperative risk. The lateral margins of the laminectomy are atthe junctions of the lateral masses and laminae. Foraminot-omy is considered following both laminectomy and lamino-plasty in patients who have foraminal stenosis resulting froma disc protrusion or foraminal osteophytes and concordantradicular symptoms. Segmental stability is maintained dur-ing the foraminotomy by resecting no more than 25% of thefacet joint80,81.
All levels with radiographic evidence of stenosis shouldbe included in the decompression. Limiting the number of seg-ments that are decompressed does not influence the develop-ment of postlaminectomy kyphosis or instability82-84 and mayresult in recurrent symptoms resulting from progression of dis-ease at adjacent segments85. A laminectomy that does not extend
cephalad enough may result in dorsal kinking of the spinal cordand increased postoperative neurologic findings. Inclusion ofC2 and T1 in the laminectomy increases the likelihood ofkyphosis and instability. Concern about postlaminectomy ky-phosis and instability has led to the development of the lami-nectomy with fusion and posterior instrumentation.
Adequacy of DecompressionVisible expansion of the dural sac intraoperatively and pulsa-tion of the dura after opening of the laminoplasty doors orfollowing laminectomy suggest good canal expansion74. Alaminoplasty opening gap of 8 to 10 mm results in adequatedecompression, with an average increase in the canal diame-ter of 3 to 4.6 mm86. Ishida et al. found better recovery frommyelopathy in patients in whom the transverse width of thelaminoplasty window was at least 70% of the transverse widthof the spinal canal and in whom the sagittal diameter of thecanal was increased to ≥15 mm73. The degree of canal expan-sion that is achieved correlates with recovery following sur-gery. Hirabiyashi et al. reported a significant difference in therecovery rate between patients with an increase of >5 mm inthe anteroposterior canal diameter and patients with an in-crease of <2 mm (p < 0.05)87. Kohno et al. found that patientswho showed good recovery from myelopathy after lamino-plasty had expansion of the anterior-posterior canal diame-ter to 12.8 mm88.
Itoh and Tsuji did not find any correlation between ca-nal expansion and recovery from myelopathy in a series ofthirty patients who underwent laminoplasty86. Increased ex-pansion of the canal does not result in better decompressionin all cases because the spinal cord is limited in its capacity tomigrate dorsally as a result of the tether of the roots anteriorlyor adhesions between an ossified posterior longitudinal liga-ment and the dura. Attempting excessive canal expansion mayalso predispose the patient to nerve-root palsy resulting fromundue stretch on the tethering nerve roots.
Instrumentation Following LaminectomyInstrumentation provides immediate stability to the cervicalspine, increases the fusion rate, and obviates dynamic factorscontributing to cord compression and myelopathy89-93. Instru-mentation options for posterior cervical fixation include sub-laminar and facet wires connected to a longitudinal rod orrectangular construct91 and interspinous wires93. Lateral massand cervical pedicle-based screw fixation systems92,94,95 are al-ternative options for patients with deficient posterior ele-ments but currently are not approved for clinical use in theUnited States by the Food and Drug Administration.
Heller et al. reported on complications following instru-mentation with use of 654 lateral mass screws in seventy-eightpatients96. Nerve-root injury was the most common complica-tion, associated with 0.6% (four) of the 654 screws placed, andwas related to improper drilling technique or the use of an ex-cessively long screw. Facet violation was seen in associationwith 0.2% (one) of the 654 screws. No case of vertebral arteryinjury was reported in that series. The rate of reoperation due
Fig. 5-F
Radiograph made after the patient underwent a lami-
noplasty with use of mini-plates. After surgery, the
patient reported improvement in upper-extremity sen-
sations and function and resolution of neck pain.

1632
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
to radiculopathy resulting from malpositioned lateral massscrews has been reported to range from 3% (one of thirty-eight patients)92 to 14% (three of twenty-one patients)97.
Pedicle screws have a higher pullout strength than lat-eral mass screws do98, and they may allow for better correc-tion of deformity. Abumi et al., in a study of forty-six patientswho underwent cervical pedicle fixation, reported that theprevalence of pedicle cortical penetration was 5.3% (ten of190)95. None of the patients had a neurovascular complica-tion. There were no cases of screw pullout, breakage, or loos-ening. Preoperative evaluation with use of computerizedtomography helps to ensure adequate pedicle morphologyand surgical planning.
Posterior Fusion Following LaminectomyThe rate of fusion following laminectomy and bone-graftingalone has been reported to range from 65.2% (thirty offorty-six patients)99 to 79% (twenty-seven of thirty-four pa-tients)100. The addition of instrumentation enhances the fu-sion rate. Callahan et al. reported a fusion rate of 96% (fiftyof fifty-two) in association with posterolateral bone-graftingand facet wiring; both cases of pseudarthrosis in that serieswere attributed to improper bone-grafting technique89. Us-ing clearly defined and much stricter criteria to determinenonunion (abnormal motion between segments, hardwarefailure, and radiolucency around the screws), Heller et al. re-ported nonunion in 38% (five) of thirteen patients who un-derwent laminectomy with lateral mass screw-and-plateinstrumentation94.
Immobilization Following Posterior SurgeryFollowing laminoplasty, patients are mobilized in a soft or rigidcervical collar. Patients may begin isometric neck exerciseswhile still wearing the collar. The cervical orthosis is generallyworn for six33 to twelve weeks16, but shorter periods of bracewear may reduce the prevalence of posterior neck and shouldergirdle pain16,101 following laminoplasty. Unrestricted activity, in-cluding sports activity, was permitted in one series after thegraft on the open-door side of the laminoplasty showed radio-graphic evidence of union102. Following laminectomy with fu-sion and posterior instrumentation, a rigid cervical collar isworn for four to eight weeks92,97. This time is increased to two tothree months for patients with osteoporosis or those with fixa-tion at more than four levels95.
Outcome Following Operative Treatment of Cervical MyelopathyPredictive Factors for OutcomePatients who are more than seventy-five years old generallyhave greater comorbidity and do not have the recovery fol-lowing an operation that can be expected from younger pa-tients28. Lumbar canal stenosis, hip osteoarthritis, and cardiacdysfunction can all contribute to overall disability, impairedwalking ability, and a worsening Nurick grade103 (Table II).Kawaguchi et al. reported less improvement following surgeryfor the treatment of myelopathy in patients who were more
than seventy years old and attributed this finding to age-related changes within the myelinated fibers and motor neu-rons of the spinal cord27. Operative intervention that is carriedout earlier in the course of the disease also appears to result ina better prognosis in terms of neurological recovery. In onestudy, patients in whom the operation was performed withinthree years after the onset of symptoms and within threemonths after the loss of walking capacity had a better chanceof recovery of gait and upper limb function20. In anotherstudy, 92% (eleven) of twelve patients who had had symptomsfor less than eighteen months had an improvement in gait asopposed to 77% (ten) of thirteen patients who had presentedlater21. Other factors that have been linked with poorer out-comes following operative treatment include more severe my-elopathy at the time of presentation104,105, preoperative bladderdysfunction21, and postoperative kyphosis88,106.
Increased T2-weighted magnetic resonance imaging sig-nal changes are frequently present within the substance of thecervical spinal cord and may represent cord edema or irrevers-ible changes such as gliosis or microcavitation. Some authorshave reported that isolated T2-weighted signal changes haveno correlation with the severity of myelopathy15,24, but thereappears to be consensus that recovery from myelopathy fol-lowing an operation is better in patients who do not demon-strate these signal changes24,25.
The degree of preoperative cord compression has beenrelated to postoperative recovery. Fukushima et al. reportedthat patients in whom the transverse area of the cord mea-sured <0.45 cm2 at the site of maximum compression onpreoperative axial magnetic resonance imaging scans hadless recovery of neurologic function following surgery107. Ina similar study, Fujiwara et al. found better recovery follow-ing surgery in patients in whom the transverse area of thecord measured ≥0.30 cm2 on preoperative computed tomog-raphy myelography23. Patients with multisegmental areas ofcord compression also have been reported to have poorerresults following surgery than those with focal areas ofcompression15.
TABLE II Nurick Grades for the Severity of Myelopathy103
Grade Findings
0 Signs or symptoms of root involvement but without evidence of spinal cord disease
1 Signs of spinal cord disease but no difficulty in walking
2 Slight difficulty in walking that does not prevent full-time employment
3 Difficulty in walking that prevents full-time employ-ment or the ability to do all housework
4 Able to walk only with someone else’s help or with the aid of a frame
5 Chairbound or bedridden

1633
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
Recovery of Neurologic FunctionDecompression of the spinal cord in patients with cervical my-elopathy results in stabilization of or improvement in long-tractspinal cord function in most cases. Function is better in patientswho have good restoration of spinal canal dimensions followingdecompression, those who have earlier decompression, andthose without substantial comorbidity. Gait improves in pa-tients with cervical myelopathy following both anterior andposterior decompression of the spinal cord. Emery et al. re-ported on 106 patients with cervical myelopathy who under-went either anterior discectomy or corpectomy and fusion14.Eighty-two (77%) of the 106 patients had preoperative gait ab-normalities. Thirty-eight (46%) of these eighty-two patientshad recovery of normal gait and thirty-three (40%) had an im-provement in gait, with the average Nurick grade improvingfrom a preoperative value of 2.4 to a postoperative value of 1.2.Okada et al. reported on thirty-seven patients who had had oneto four-level decompression and arthrodesis18. The average du-ration of follow-up was four years. No patient had had normallower limb motor function preoperatively, but normal functionwas seen in seventeen (46%) of the thirty-seven patients post-operatively. Improvement in gait and lower extremity functionis similar to that following laminoplasty108.
Patients with cervical spondylotic myelopathy may presentwith predominantly hand symptoms, with motor and sensoryabnormalities in the upper and lower extremities being appar-ent on further examination. Myelopathic hand manifesta-tions are commonly described as “numb, clumsy hands”109.These findings are more frequent in patients with upper cervi-cal spine stenosis and may result from a combination of ante-rior horn cell dysfunction, venous stasis, and ischemia of thecentral grey matter and/or the pyramidal tract110-112. Most pa-tients have substantial improvement in hand function afterthe operation. Lee et al. reported improvement in terms ofnondermatomal hand tingling and numbness in 87% (thir-teen) of fifteen patients and improvement in terms of upperextremity weakness in 71% (ten) of fourteen patients eigh-teen to forty-three months following laminoplasty21. Otherauthors have reported an increased ability to rapidly grip andrelease the hand following surgery for the treatment of cervi-cal spondylotic myelopathy27,113.
The prevalence of sensory abnormalities has variedwidely among various reports on patients undergoing opera-tive treatment of cervical myelopathy, from 58% (sixty-oneof 105)114 to 84% (eighty-nine of 106)14. Sensory deficits haveincluded dermatomal anesthesia, nondermatomal paresthe-sias, and loss of pinprick, proprioceptive, and vibratory sen-sations in the upper and/or lower extremities. Emery et al.,in a study of eighty-nine patients managed with anterior dis-cectomy or corpectomy, reported complete recovery of sen-sory deficit in forty-three patients (48%), partial recovery inthirty-five patients (39%), no change in ten patients (11%),and worsening in one patient (1%)14. Okada et al., in a studyof thirty-seven patients with cervical myelopathy, reportedthat definite preoperative sensory loss was noted in the up-per limbs, trunk, and lower limbs of twenty-seven, thirteen,
and twenty-four patients, respectively18. Following anteriorcorpectomy, these changes were noted in only eight, zero,and three patients, respectively. Edwards et al. reported im-provement in sensory symptoms in 69% of thirteen patientswho had undergone laminoplasty for the treatment of cervi-cal spondylotic myelopathy115.
Comparative Outcome Between Anterior and Posterior SurgeryWada et al.16 retrospectively reviewed the clinical course oftwenty-three patients who had been managed with subtotalcorpectomy and fusion and twenty-four patients who hadbeen managed with laminoplasty over a ten to eighteen-yearperiod. Spondylotic myelopathy was present over an average2.3 levels in the corpectomy group and 2.5 levels in the lami-noplasty group. No significant difference in neurological re-covery was found between the two groups at one or five yearsafter the operation or at the time of the final follow-up.Sakaura et al. compared two groups of patients ten and fif-teen years after laminoplasty and anterior cervical discectomyand fusion, respectively116. The preoperative extent of diseasewas similar in both groups. Neurological function improvedafter surgery in both groups, with no significant differencesbetween the two groups with regard to the JOA score or therecovery rate. Those authors found greater adjacent-segmentdeterioration following the use of an anterior operative ap-proach and increased postoperative kyphosis and axial painfollowing the use of a posterior approach. The authors recom-mended laminoplasty for patients with cervical myelopathydue to disc herniations, except for patients with a single-leveldisc herniation without developmental canal stenosis. Yone-nobu et al. reported an overall slightly higher recovery frommyelopathy in patients who underwent anterior subtotalcorpectomy and fusion as compared with patients who un-derwent laminoplasty117. On further analysis, those authorsfound that patients with a canal diameter of <12 mm hadbetter recovery following laminoplasty, suggesting that thiswas a better option for patients with a developmentally nar-row canal.
Maintenance of Neurological Recovery Over the Long-TermA general trend is observed in the pattern of recovery follow-ing the operative treatment of myelopathy. Recovery that isobtained in the immediate postoperative period is followed bycontinued improvement over the next few years and then bysome deterioration in functional status thereafter. This pat-tern is seen following both anterior and posterior operativetreatment. Wada et al., in a retrospective review of twenty-three patients with cervical spondylotic myelopathy who weremanaged with anterior subtotal corpectomy and fusion, re-ported an improvement in the mean JOA score from 7.9 pre-operatively to 13.3 at one year and to 13.9 at five years16. At amean of fifteen years after surgery, the mean JOA score was13.4. In a cohort of twenty-four patients who underwent lami-noplasty, the average JOA score was 7.4 preoperatively, 13.1 at

1634
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
one year, 12.9 at five years, and 12.2 at a mean 11.7 years16.Kawaguchi et al., in a study of the results of laminoplasty, re-ported that the mean preoperative JOA score of 9.1 points im-proved to 13.4 at six months and to 13.9 at five years and thendecreased to 13.4 at the time of the final follow-up at an aver-age of 13.2 years29.
The causes of late deterioration are distinct followinganterior and posterior procedures. The most common causeof recurrent symptoms following anterior operative treatmentis deterioration of an adjacent segment; other causes mayinclude inadequate decompression at the time of the initialoperation, pseudarthrosis, graft or implant failure, continuedgrowth of osteophytes, or ligamentum flavum infolding.Common causes of recurrent myelopathy following poste-rior operative treatment include the development of kypho-sis, instability, the spread of ossification of the posteriorlongitudinal ligament, and the development of stenosis atnew levels. Late deterioration of neurological symptoms ismore frequent following laminectomy without fusion85,118.
Consequences and Complications Following Operative TreatmentPostoperative Neck PainIn the study by Hosono et al., posterior neck and shouldergirdle pain was present following laminoplasty in 60%(forty-three) of seventy-two patients, with 25% (eighteen) ofthe seventy-two patients reporting severe axial pain as thechief complaint119. Soft-tissue injury following a posteriorapproach, facet arthrosis, preoperative stiffness, and olderage have all been implicated in the pathogenesis of axialpain. Operative modifications such as coronal osteotomy ofthe spinous processes during the approach with subsequentreattachment after laminoplasty120 (Fig. 4, E)120 or combininglaminectomy at selected levels with either partial laminec-tomy or interlaminar decompression121 help to preserve someof the extensor muscle and ligament attachments and havebeen reported to lower the prevalence of axial pain and stiff-ness following multiple-level posterior decompression122,123.The duration of postoperative immobilization also may have abearing on the prevalence of postoperative axial pain16,101, lead-ing some authors to encourage early active mobilization. Manypatients have resolution of symptoms within a year.
Yonenobu et al. noted that the prevalence of postoper-ative pain was highest following laminoplasty (60% of 203),followed by laminectomy (27% of 115) and then by anteriordecompression (19% of 209)118. Wada et al. reported moder-ate to severe axial neck pain in 40% of twenty-four patientsat an average 11.7 years following laminoplasty and in 15%of twenty-three patients an average of fifteen years followingsubtotal corpectomy (p < 0.05)16. Conversely, Kawakami etal. reported less axial pain at 5.6 years following lamino-plasty than following anterior cervical fusion at one or twolevels and suggested that a shorter period of immobiliza-tion following laminoplasty prevents muscle atrophy andfacet joint contracture, thereby minimizing postoperativestiffness33.
Postoperative StiffnessA decrease in the range of motion of the neck occurs in somepatients following laminoplasty and is presumed to occur as aresult of interlaminar or facet fusion on the hinge side or con-tracture of the posterior muscles and ligaments. Kawai et al.reported an appreciable loss in range of motion in thirty-four(72%) of forty-seven patients who were followed for two tofifteen years after laminoplasty124. Range of motion is also lostfollowing laminectomy with fusion, and Callahan et al. re-ported that as much as 12° of flexion, 16° of rotation, and 6° oflateral flexion can be expected to be lost for each level in-cluded in the posterior fusion89. Some authors believe that thedecrease in range of motion following laminoplasty is benefi-cial because it prevents further instability and retards the pro-gression of spondylosis74,125.
A decrease in the range of motion of the neck followinganterior cervical discectomy and fusion is not an importantconcern. Many patients will note an increase in range of mo-tion accompanying the pain relief following the operation.One study demonstrated no difference in the range of motionof the neck following anterior cervical discectomy and fusionat one and two levels but revealed a slight decrease in range ofmotion one year after anterior cervical discectomy and fusionat four levels126. Range of motion decreases following corpec-tomy and fusion and is proportional to the number of levelsfused. Hanai et al. reported on thirty myelopathic patientswho were followed for three years after corpectomy and fusioninvolving an average of 3.4 levels127. The average preoperativesagittal range of motion was 56°. The range of motion de-creased by an average 15.2° in the three-level corpectomygroup (eighteen patients) and by an average of 29.6° in thefour-level corpectomy group (twelve patients).
Postoperative StabilityLaminectomy alone, especially in children and young adultsor in patients with preexisting kyphosis or segmental mobility,can result in further instability, kyphosis, and worsening ofneurologic deficit. Yonenobu et al., in a report on 115 patientswho were managed with laminectomy for the treatment ofmyelopathy resulting from either spondylosis or ossificationof the posterior longitudinal ligament, noted that 21% of thepatients had postoperative neurologic deterioration due to in-stability of the cervical spine118. In another study of patientswho underwent laminectomy without fusion for the treat-ment of cervical spondylotic myelopathy, 14% (three) oftwenty-two patients with a preoperative lordotic cervical spinehad development of postoperative kyphosis whereas 30% (six)of twenty patients with a straight spine and 67% (two) ofthree patients with preoperative kyphosis had an increase inkyphosis83. In studies in which posterior instrumentation hasbeen used, laminectomy with fusion has maintained lordosisclose to the preoperative value90,92.
The development of instability following laminectomymay be partly dependent on the degree of degenerativechanges already present in the cervical spine. Yasuoka et al. re-ported on a large series of 1577 adult patients who had been

1635
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
followed for a minimum of five years after laminectomy84.When the patients who had had trauma and those who hadbeen managed with facetectomy were excluded, none of thepatients had development of a deformity substantial enoughto warrant a second operation.
Some loss of lordosis is common, but severe postoper-ative kyphosis is infrequent following laminoplasty115,116,128.Preservation of the soft-tissue attachments to the C2 spinousprocess following laminoplasty decreases the likelihood ofdevelopment of deformity in the cervical spine. In patientsundergoing laminoplasty, unilateral exposure followed bycoronal osteotomy of the spinous process and en bloc reflec-tion of the spinous processes and attached soft tissues to thecontralateral side minimizes the injury to the posterior soft-tissue tether120,122.
Development of overt instability following anteriordiscectomy is uncommon even without an attempt at fusion.Many patients will go on to have spontaneous fusion114. Theinsertion of a graft and anterior plating following discec-tomy helps to maintain, and in some cases increases, cervicallordosis67. Multiple-level anterior corpectomy with graftingand anterior instrumentation effectively reconstructs cervi-cal alignment; in one study, it led to improved lordosis com-pared with laminoplasty115.
Adjacent Segment Degeneration Following OperationIn many cases, loss of recovery from myelopathy over the longterm is attributed to degenerative changes adjacent to previ-ously fused segments in the cervical spine. However, the oc-currence of these degenerative changes needs to be viewed inthe context of the natural progression of the spondylotic pro-cess with age and the ubiquitous presence of degenerativechanges in an elderly but asymptomatic population. In ananalysis of 374 patients at a maximum of twenty-one years fol-lowing anterior cervical fusion, Hilibrand et al. reported that2.9% of the patients had development of symptomatic adja-cent-segment disease each year129. Kaplan-Meier survivorshipanalysis indicated that the risk of development of adjacent-segment disease within ten years following anterior cervicalfusion was 25.6%. Adjacent-segment disease developed ear-lier in patients who had preexisting degenerative changes atsegments adjacent to the fusion. The C5-C6 and C6-C7 lev-els were most vulnerable to adjacent-segment disease butare also naturally most likely to show degenerative changes.The authors concluded that adjacent-segment disease was morelikely to be a manifestation of the natural history of spondylosisrather than a consequence of fusion. Recently publishedbiomechanical data suggest that anterior cervical discec-tomy and fusion with anterior plating does not predispose toadjacent-segment deterioration130.
Adjacent-segment degeneration also has been reportedfollowing other forms of operative intervention on the cervi-cal spine. In one study, 3.8% (three) of seventy-eight patientshad development of adjacent-segment degeneration within2.5 years after laminectomy and fusion, with two patients re-
quiring a repeat operation for this condition96. Wada et al.studied adjacent-segment degeneration in twenty-three pa-tients following anterior corpectomy and fusion over an aver-age of 2.5 levels and found that 38% of the patients haddevelopment of olisthesis at an adjacent segment and that54% of the patients had development of osteophytes and disc-space narrowing at adjacent levels16. However, only one patientrequired a repeat operation for recurrent myelopathy over afollow-up period of fifteen years.
Neurological ComplicationsPatients with myelopathy are at risk for worsening of the neu-rological status intraoperatively. Active range of motion of theneck should be provocatively tested prior to the induction ofanesthesia, and care should be taken to avoid intubation or in-traoperative alignment of the neck in positions that result inneurological symptoms. Manipulation of the vertebral bodiesduring the operation should be minimized. Somatosensoryand motor evoked potentials should be checked prior to posi-tioning and throughout the procedure to help to detect anyinjury to the spinal cord.
Intraoperative spinal cord injury can result from directtrauma, ischemia, stretch, or hypothermia. In a survey ofsurgeons who performed anterior discectomy and fusionprocedures, 311 neurological complications were reportedamong 36,657 cases131. The most common postoperative compli-cations were radiculopathy (40%; 124 of 311), substantialpermanent myelopathy (25%; seventy-eight of 311), and re-current laryngeal nerve palsy 17% (fifty-two of 311). Yonenobuet al. reported that the prevalence of spinal cord dysfunctionfollowing laminectomy was 3.5% (three of eighty-five) andattributed this finding to the development of an epidural he-matoma and postoperative swelling of the nuchal muscles,compressing the exposed spinal cord132. No myelopathic com-plications occurred in ninety-five patients who were man-aged with laminoplasty.
Postoperative C5 radiculopathy is a well-recognized com-plication that occurs following both anterior and posterior de-compression of the spinal cord. Possible etiologies for the palsyinclude traction on the short C5 root resulting from posteriormigration of the cord into the space created by a laminoplasty,closure of the laminoplasty door resulting in nerve impinge-ment, and impingement of the ventral aspect of the spinal cordagainst the edges of a corpectomy trough118,132,133. Yonenobu et al.reported that the prevalence of C5 palsy was 3.9% (eight of 204)following anterior procedures, 4.2% (four of ninety-five) fol-lowing laminoplasty, and 1% (one of eighty-five) followinglaminectomy132. The clinical presentation is usually one of se-vere shoulder and upper arm pain, followed by weakness of thebiceps and deltoid occurring one to three days after the opera-tion. Spontaneous recovery can be expected, although this maytake twelve months in some cases. Concurrent foraminotomymay help to diminish the prevalence of this condition followinglaminoplasty134.
The prevalence of recurrent laryngeal nerve palsy fol-lowing an anterior cervical approach has been reported to

1636
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
range from 2% (thirteen of 650)135 to 11% (nine of eighty-five)136. The actual prevalence of this complication may beunderreported because common symptoms of hoarseness,aspiration, or cough are minor, transient, and frequently seenin association with endotracheal intubation. Mechanisms ofinjury to the nerve include direct surgical trauma, pressureor stretch-induced neurapraxias, postoperative edema, andstretch resulting from retraction on the intralaryngeal courseof a laryngeal nerve tethered by the endotracheal tube135.Avoidance of prolonged retraction, knowledge of the anat-omy, careful dissection, and deflation of the endotrachealtube cuff after retractor placement all may help to diminishthe prevalence of this complication. The course of the recur-rent laryngeal nerve is more protected within the tracheo-esophageal groove on the left side, but it is unclear whetherthe laterality of the approach affects the prevalence of thiscomplication. Injury to the superior laryngeal nerve leads toeasy voice fatigue and difficulty with high-pitched tones. It mostfrequently occurs inadvertently during anterior approachesto the upper cervical segments.
Injury to the sympathetic nerves results in Horner syn-drome and commonly occurs in association with prolonged ormore vigorous retraction, revision surgery, and operations in-volving lower cervical and cervicothoracic levels. Patients gen-erally do not have symptoms other than a drooping eyelid,and most patients have resolution of these findings within sixmonths. Bertalanffy and Eggert reported Horner syndrome infive (1.1%) of 450 patients who underwent anterior cervicaldiscectomy for the treatment of myelopathy, radiculopathy,and myeloradiculopathy1.
DysphagiaDysphagia is a frequent and transient occurrence followinganterior cervical spinal approaches. Hematomas; local edema;denervation of the pharyngeal plexus; adhesions betweenthe esophagus, trachea, and prevertebral fascia; and dis-placed graft or instrumentation are all potential causes. Ba-zaz et al. reported that the prevalence of dysphagia was ashigh as 50% (ninety-nine of 197) at one month after theoperation and decreased to 12.5% (nineteen of 152) at oneyear137. Dysphagia occurred more frequently when the pro-cedure involved multiple levels or was performed in women.There was no correlation with the type of procedure (cor-pectomy or discectomy, primary or revision surgery), thevertebral level at which the operation was performed, orthe addition of anterior plating. Esophageal perforation re-sulting from anterior migration of screws or plates occursinfrequently138,139.
Vertebral Artery InjuriesVertebral artery injuries occur during operations performedthrough an anterior approach for the treatment of cervicalspondylotic myelopathy; such injuries can result from a loss oforientation to the midline during corpectomy, lateral dissec-tion in the foraminal region, or unrecognized anomalies in thecourse of the vessel140. The width of the corpectomy trough
should be restricted to 15 to 19 mm to avoid inadvertent in-jury to the vertebral artery. The medial margin of the longuscolli muscles, uncovertebral joints, and the natural curvatureof the vertebral end plates all help to orient the surgeon withrespect to the midline. Eleraky et al.141 reported vertebral ar-tery injury in four of 185 patients undergoing corpectomy.Treatment options include ligation, exposure and direct re-pair, and endovascular stent placement. In most cases, thecontralateral vertebral artery provides sufficient collateral cir-culation to the hindbrain, but neurologic deficit can occasion-ally result.
Intraoperative Spinal Cord MonitoringElectrophysiologic monitoring aims to detect intraoperativecompromise of the long tracts of the spinal cord and to allowearlier correction of any surgical or anesthetic event thatmay have precipitated these changes. Somatosensory evokedpotentials represent potentials conducted from the ulnar,median, or posterior tibial nerves through the dorsal col-umns to electrodes located over the cranium or the uppercervical spine. Motor evoked potentials monitor the ventralcolumns of the spinal cord and are frequently used in combi-nation with somatosensory evoked potentials for intraopera-tive monitoring. Motor evoked potentials record peripheralmuscle potentials in response to transcranial stimulationwith a needle or surface electrode. Continuous or so-calledfree-running electromyogram recording of upper extremitymuscle groups helps to monitor cervical nerve roots duringthe operation142.
Somatosensory evoked potentials can vary in response tothe dose of inhalational anesthetic agents, and the rate of false-positive recordings is high. In one study, sixty (86%) of seventypatients with an amplitude decrease of >50% had no neuro-logical deficit postoperatively143. False-negative somatosensoryevoked potentials are rare with proper technique and appropri-ate threshold selection144. Motor evoked potentials are more spe-cific but are blunted by neuromuscular blocking agents and inmore severe cases of myelopathy. Motor evoked potentialsshould not be used in children or in patients with metallic an-eurysmal clips, cardiac pacemakers, or epilepsy.
At our institution, baseline recordings are obtained forthe patient after the induction of anesthesia but before final po-sitioning. A change in spinal cord function is indicated whensomatosensory evoked potentials decrease in amplitude by 50%and increase in latency by 10% or when the stimulation thresh-old for motor evoked potentials is exceeded by 100 mV.
OverviewOperative management is indicated for most patients with clin-ically evident cervical spondylotic myelopathy. Patients withvery early or mild clinical findings are clinically and radio-graphically assessed with regard to their level of disability,the duration of symptoms, the degree of stenosis, and evi-dence of progression, and a decision regarding treatment ismade by weighing these factors against the risks of operative

1637
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
intervention. The objective of operative treatment is to ade-quately decompress the spinal cord and to maintain the stabil-ity of the spinal column.
A choice of operative techniques is available for thesurgical treatment of cervical spondylotic myelopathy, andthe specific procedure that is chosen is based on multiplefactors, including the location of the compressive pathology,the longitudinal extent of disease, the alignment of the spinalcolumn, and the dimensions of the spinal canal. Appropriateoperative surgical treatment of cervical spondylotic myelop-athy will result in satisfactory recovery from myelopathy inmost cases, with improvement being higher in younger pa-tients, patients in whom operative treatment is performedearlier in the course of the disease, and patients with lesscomorbidity.
Raj D. Rao, MDKrishnaj Gourab, MDKenny S. David, MDDepartment of Orthopaedic Surgery, Medical College of Wisconsin, Mil-waukee, WI 53226
The authors did not receive grants or outside funding in support of their research for or preparation of this manuscript. They did not receive pay-ments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, educational institution, or other charitable or nonprofit organization with which the authors are affiliated or associated.
doi:10.2106/JBJS.F.00014
References
1. Bertalanffy H, Eggert HR. Complications of anterior cervical discectomy without fusion in 450 consecutive patients. Acta Neurochir (Wien). 1989;99:41-50.
2. Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: patho-physiology, natural history, and clinical evaluation. J Bone Joint Surg Am. 2002;84:1872-81.
3. Clarke E, Robinson PK. Cervical myelopathy: a complication of cervical spondy-losis. Brain. 1956;79:483-510.
4. Sampath P, Bendebba M, Davis JD, Ducker TB. Outcome of patients treated for cervical myelopathy. A prospective, multicenter study with independent clinical re-view. Spine. 2000;25:670-6.
5. Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med. 1934;211:210-5.
6. Hirabayashi K, Miyakawa J, Satomi K, Maruyama T, Wakano K. Operative re-sults and postoperative progression of ossification among patients with ossifica-tion of cervical posterior longitudinal ligament. Spine. 1981;6:354-64.
7. Tsuji H. Laminoplasty for patients with compressive myelopathy due to so-called spinal canal stenosis in cervical and thoracic regions. Spine. 1982;7:28-34.
8. Robinson RA, Smith GW. Anterolateral cervical disc removal and interbody fusion for cervical disc syndrome. Bull Johns Hopkins Hosp. 1955;96:223-4.
9. Cloward RB. The anterior approach for removal of ruptured cervical disks. J Neurosurg. 1958;15:602-17.
10. Simmons EH, Bhalla SK. Anterior cervical discectomy and fusion. A clinical and biomechanical study with eight-year follow-up. J Bone Joint Surg Br. 1969;51:225-37.
11. Kadanka Z, Mares M, Bednanik J, Smrcka V, Krbec M, Stejskal L, Chaloupka R, Surelova D, Novotny O, Urbanek I, Dusek L. Approaches to spondylotic cervical myelopathy: conservative versus surgical results in a 3-year follow-up study. Spine. 2002;27:2205-11.
12. Kadanka Z, Mares M, Bednarik J, Smrcka V, Krbec M, Chaloupka R, Dusek L. Predictive factors for spondylotic cervical myelopathy treated conservatively or surgically. Eur J Neurol. 2005;12:55-63.
13. Matsumoto M, Chiba K, Ishikawa M, Maruiwa H, Fujimura Y, Toyama Y. Rela-tionships between outcomes of conservative treatment and magnetic resonance imaging findings in patients with mild cervical myelopathy caused by soft disc her-niations. Spine. 2001;26:1592-8.
14. Emery SE, Bohlman HH, Bolesta MJ, Jones PK. Anterior cervical decompres-sion and arthrodesis for the treatment of cervical spondylotic myelopathy. Two to seventeen-year follow-up. J Bone Joint Surg Am. 1998;80:941-51.
15. Suri A, Chabbra RP, Mehta VS, Gaikwad S, Pandey RM. Effect of intramedul-lary signal changes on the surgical outcome of patients with cervical spondylotic myelopathy. Spine J. 2003;3:33-45.
16. Wada E, Suzuki S, Kanazawa A, Matsuoka T, Miyamoto S, Yonenobu K. Subto-tal corpectomy versus laminoplasty for multilevel cervical spondylotic myelopathy: a long-term follow-up study over 10 years. Spine. 2001;26:1443-8.
17. Bohlman HH. Cervical spondylosis with moderate to severe myelopathy. A re-port of seventeen cases treated by Robinson anterior cervical discectomy and fu-sion. Spine. 1977;2:151-62.
18. Okada K, Shirasaki N, Hayashi H, Oka S, Hosoya T. Treatment of cervical spondylotic myelopathy by enlargement of the spinal canal anteriorly, followed by arthrodesis. J Bone Joint Surg Am. 1991;73:352-64.
19. al-Mefty O, Harkey HL, Marawi I, Haines DE, Peeler DF, Wilner HI, Smith RR, Holaday HR, Haining JL, Russell WF, Harrison B, Middleton TH. Experimental chronic compressive cervical myelopathy. J Neurosurg. 1993;79:550-61.
20. Tanaka J, Seki N, Tokimura F, Doi K, Inoue S. Operative results of canal-expansive laminoplasty for cervical spondylotic myelopathy in elderly patients. Spine. 1999;24:2308-12.
21. Lee TT, Manzano GR, Green BA. Modified open-door cervical expansive lami-noplasty for spondylotic myelopathy: operative technique, outcome, and predic-tors for gait improvement. J Neurosurg. 1997;86:64-8.
22. Arnasson O, Carlsson CA, Pellettieri L. Surgical and conservative treatment of cervical spondylotic radiculopathy and myelopathy. Acta Neurochir (Wien). 1987;84:48-53.
23. Fujiwara K, Yonenobu K, Ebara S, Yamashita K, Ono K. The prognosis of surgery for cervical compression myelopathy. An analysis of the factors involved. J Bone Joint Surg Br. 1989;71:393-8.
24. Morio Y, Teshima R, Nagashima H, Nawata K, Yamasaki D, Nanjo Y. Correla-tion between operative outcomes of cervical compression myelopathy and mri of the spinal cord. Spine. 2001;26:1238-45.
25. Matsuda Y, Miyazaki K, Tada K, Yasuda A, Nakayama T, Murakami H, Matsuo M. Increased MR signal intensity due to cervical myelopathy. Analysis of 29 surgi-cal cases. J Neurosurg. 1991;74:887-92.
26. Mehalic TF, Pezzuti RT, Applebaum BI. Magnetic resonance imaging and cervi-cal spondylotic myelopathy. Neurosurgery. 1990;26:217-27.
27. Kawaguchi Y, Kanamori M, Ishihara H, Ohmori K, Abe Y, Kimura T. Pathomech-anism of myelopathy and surgical results of laminoplasty in elderly patients with cervical spondylosis. Spine. 2003;28:2209-14.
28. Matsuda Y, Shibata T, Oki S, Kawatani Y, Mashima N, Oishi H. Outcomes of surgical treatment for cervical myelopathy in patients more than 75 years of age. Spine. 1999;24:529-34.
29. Kawaguchi Y, Kanamori M, Ishihara H, Ohmori K, Nakamura H, Kimura T. Mini-mum 10-year followup after en bloc cervical laminoplasty. Clin Orthop Relat Res. 2003;411:129-39.
30. Bucciero A, Vizioli L, Carangelo B, Tedeschi G. MR signal enhancement in cer-vical spondylotic myelopathy. Correlation with surgical results in 35 cases. J Neu-rosurg Sci. 1993;37:217-22.
31. Sodeyama T, Goto S, Mochizuki M, Takahashi J, Moriya H. Effect of decom-pression enlargement laminoplasty for posterior shifting of the spinal cord. Spine. 1999;24:1527-32.
32. Suda K, Abumi K, Ito M, Shono Y, Kaneda K, Fujiya M. Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine. 2003;28:1258-62.
33. Kawakami M, Tamaki T, Iwasaki H, Yoshida M, Ando M, Yamada H. A compar-ative study of surgical approaches for cervical compressive myelopathy. Clin Or-thop Relat Res. 2000;381:129-36.

1638
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
34. Chiba K, Toyama Y, Watanabe M, Maruiwa H, Matsumoto M, Hirabayashi K. Impact of longitudinal distance of the cervical spine on the results of expansive open-door laminoplasty. Spine. 2000;25:2893-8.
35. Yonenobu K, Fuji T, Ono K, Okada K, Yamamoto T, Harada N. Choice of surgical treatment for multisegmental cervical spondylotic myelopathy. Spine. 1985;10:710-6.
36. Kadoya S, Nakamura T, Kwak R. A microsurgical anterior osteophytectomy for cervical spondylotic myelopathy. Spine. 1984;9:437-41.
37. Herkowitz HN, Kurz LT, Overholt DP. Surgical management of cervical soft disc herniation. A comparison between the anterior and posterior approach. Spine. 1990;15:1026-30.
38. Ratliff JK, Cooper PR. Cervical laminoplasty: a critical review. J Neurosurg. 2003;98(3 Suppl):230-8.
39. An HS, Evanich CJ, Nowicki BH, Haughton VM. Ideal thickness of Smith-Robinson graft for anterior cervical fusion. A cadaveric study with computed tomo-graphic correlation. Spine. 1993;18:2043-7.
40. Vaccaro AR, Ring D, Scuderi G, Garfin SR. Vertebral artery location in relation to the vertebral body as determined by two-dimensional computed tomography evaluation. Spine. 1994;19:2637-41.
41. Smith MD, Emery SE, Dudley A, Murray KJ, Leventhal M. Vertebral artery in-jury during anterior decompression of the cervical spine. A retrospective review of ten patients. J Bone Joint Surg Br. 1993;75:410-5.
42. Goto S, Mochizuki M, Kita T, Kobayashi Y, Sodeyama T, Watanabe T, Kitahara H, Moriya H. Anterior surgery in four consecutive technical phases for cervical spondylotic myelopathy. Spine. 1993;18:1968-73.
43. Raynor RB. Intraoperative ultrasound for immediate evaluation of anterior cer-vical decompression and discectomy. Spine. 1997;22:389-95.
44. Groff MW, Sriharan S, Lee SM, Maiman DJ. Partial corpectomy for cervical spondylosis. Spine. 2003;28:14-20.
45. Yonenobu K, Okada K, Fuji T, Fujiwara K, Yamashita K, Ono K. Causes of neurologic deterioration following surgical treatment of cervical myelopathy. Spine. 1986;11:818-23.
46. Connolly ES, Seymour RJ, Adams JE. Clinical evaluation of anterior cervical fusion for degenerative cervical disc disease. J Neurosurg, 1965;23:431-7.
47. Robinson RA, Walker AE, Ferlic DC, Wiecking DK. The results of anterior interbody fusion of the cervical spine. J Bone Joint Surg Am. 1962;44:1569-87.
48. Stevens JM, Clifton AG, Whitear P. Appearances of posterior osteophytes after sound anterior interbody fusion in the cervical spine: a high-definition computed myelographic study. Neuroradiology. 1993;35:227-8.
49. Yamamoto I, Ikeda A, Shibuya N, Tsugane R, Sato O. Clinical long-term re-sults of anterior discectomy without interbody fusion for cervical disc disease. Spine. 1991;16:272-9.
50. Shoda E, Sumi M, Kataoka O, Mukai H, Kurosaka M. Developmental and dy-namic canal stenosis as radiologic factors affecting surgical results of anterior cervical fusion for myelopathy. Spine. 1999;24:1421-4.
51. Tani T, Ishida K, Ushida T, Yamamato H. Intraoperative electroneurography in the assessment of the level of operation for cervical spondylotic myelopathy in the elderly. J Bone Joint Surg Br. 2000;82:269-74.
52. Zdeblick TA, Ducker TB. The use of freeze-dried allograft bone for anterior cer-vical fusions. Spine. 1991;16:726-9.
53. Samartzis D, Shen FH, Matthews DK, Yoon ST, Goldberg EJ, An HS. Compari-son of allograft to autograft in multilevel anterior cervical discectomy and fusion with rigid plate fixation. Spine J. 2003;3:451-9.
54. Wittenberg RH, Moeller J, Shea M, White AA 3rd, Hayes WC. Compressive strength of autologous and allogenous bone grafts for thoracolumbar and cervical spine fusion. Spine. 1990;15:1073-8.
55. Buck BE, Malinin TI. Human bone and tissue allografts. Preparation and safety. Clin Orthop Relat Res. 1994;303:8-17.
56. Shapiro S. Banked fibula and the locking anterior cervical plate in an-terior cervical fusions following cervical discectomy. J Neurosurg, 1996;84:161-5.
57. Brown MD, Malinin TI, Davis PB. A roentgenographic evaluation of frozen al-lografts versus autografts in anterior cervical spine fusions. Clin Orthop Relat Res. 1976;119:231-6.
58. Wang JC, Hart RA, Emery SE, Bohlman HH. Graft migration or displace-ment after multilevel cervical corpectomy and strut grafting. Spine. 2003;28:1016-22.
59. Vaccaro AR, Falatyn SP, Scuderi GJ, Eismont FJ, McGuire RA, Singh K, Garfin SR. Early failure of long segment anterior cervical plate fixation. J Spinal Disord. 1998;11:410-5.
60. Sasso RC, Ruggiero RA Jr, Reilly TM, Hall PV. Early reconstruction failures af-ter multilevel cervical corpectomy. Spine. 2003;28:140-2.
61. Connolly PJ, Esses SI, Kostuik JP. Anterior cervical fusion: outcome analysis of patients fused with and without anterior cervical plates. J Spinal Disord. 1996;9:202-6.
62. Kaiser MG, Haid RW Jr, Subach BR, Barnes B, Rodts GE Jr. Anterior cervical plating enhances arthrodesis after discectomy and fusion with cortical allograft. Neurosurgery. 2002;50:229-38.
63. Wang JC, McDonough PW, Endow KK, Delamarter RB. Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion. Spine. 2000;25:41-5.
64. Park JB, Cho YS, Riew KD. Development of adjacent-level ossification in pa-tients with an anterior cervical plate. J Bone Joint Surg Am. 2005;87:558-63.
65. Samartzis D, Shen FH, Lyon C, Phillips M, Goldberg EJ, An HS. Does rigid in-strumentation increase the fusion rate in one-level anterior cervical discectomy and fusion? Spine J. 2004;4:636-43.
66. Wang JC, McDonough PW, Endow K, Kanim LE, Delamarter RB. The effect of cervical plating on single-level anterior cervical discectomy and fusion. J Spinal Disord. 1999;12:467-71.
67. Herrmann AM, Geisler FH. Geometric results of anterior cervical plate stabili-zation in degenerative disease. Spine. 2004;29:1226-34.
68. Epstein NE. The management of one-level anterior cervical corpectomy with fusion using Atlantis hybrid plates: preliminary experience. J Spinal Disord. 2000;13:324-8.
69. Bohlman HH, Emery SE, Goodfellow DB, Jones PK. Robinson anterior cervical discectomy and arthrodesis for cervical radiculopathy. Long-term follow-up of one hundred and twenty-two patients. J Bone Joint Surg Am. 1993;75:1298-307.
70. Cauthen JC, Kinard RE, Vogler JB, Jackson DE, DePaz OB, Hunter OL, Wasser-burger LB, Williams VM. Outcome analysis of noninstrumented anterior cervical discectomy and interbody fusion in 348 patients. Spine. 1998;23:188-92.
71. Martin GJ Jr, Haid RW Jr, MacMillan M, Rodts GE Jr, Berkman R. Anterior cer-vical discectomy with freeze-dried fibula allograft. Overview of 317 cases and lit-erature review. Spine. 1999;24:852-9.
72. Mikawa Y, Shikata J, Yamamuro T. Spinal deformity and instability after multi-level cervical laminectomy. Spine. 1987;12:6-11.
73. Ishida Y, Suzuki K, Ohmori K, Kikata Y, Hattori Y. Critical analysis of extensive cervical laminectomy. Neurosurgery. 1989;24:215-22.
74. Hirabayashi K, Satomi K. Operative procedure and results of expansive open-door laminoplasty. Spine. 1988;13:870-6.
75. Naito M, Ogata K, Kurose S, Oyama M. Canal-expansive laminoplasty in 83 patients with cervical myelopathy. A comparative study of three different proce-dures. Int Orthop. 1994;18:347-51.
76. Yue WM, Tan CT, Tan SB, Tan SK, Tay BK. Results of cervical laminoplasty and a comparison between single and double trap-door techniques. J Spinal Disord. 2000;13:329-35.
77. Deutsch H, Mummaneni PV, Rodts GE, Haid RW. Posterior cervical lamino-plasty using a new plating system: technical note. J Spinal Disord Tech. 2004;17:317-20.
78. O’Brien MF, Peterson D, Casey AT, Crockard HA. A novel technique for lamino-plasty augmentation of spinal canal area using titanium miniplate stabilization. A computerized morphometric analysis. Spine. 1996;21:474-84.
79. Goto T, Ohata K, Takami T, Nishikawa M, Tsuyuguchi N, Morino M, Matusaka Y, Nishio A, Inoue Y, Hara M. Hydroxyapatite laminar spacers and titanium mini-plates in cervical laminoplasty. J Neurosurg. 2002;97(3 Suppl):323-9.
80. Benzel EC, Lancon J, Kesterson L, Hadden T. Cervical laminectomy and dentate ligament section for cervical spondylotic myelopathy. J Spinal Disord. 1991;4:286-95.
81. Nowinski GP, Visarius H, Nolte LP, Herkowitz HN. A biomechanical comparison of cervical laminaplasty and cervical laminectomy with progressive facetectomy. Spine. 1993;18:1995-2004.
82. Guigui P, Benoist M, Deburge A. Spinal deformity and instability after multi-level cervical laminectomy for spondylotic myelopathy. Spine. 1998;23:440-7.
83. Kaptain GJ, Simmons NE, Replogle RE, Pobereskin L. Incidence and outcome of kyphotic deformity following laminectomy for cervical spondylotic myelopathy. J Neurosurg. 2000;93(2 Suppl):199-204.

1639
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
84. Yasuoka S, Peterson HA, MacCarty CS. Incidence of spinal column defor-mity after multilevel laminectomy in children and adults. J Neurosurg. 1982;57:441-5.
85. Kato Y, Iwasaki M, Fuji T, Yonenobu K, Ochi T. Long-term follow-up results of laminectomy for cervical myelopathy caused by ossification of the posterior longi-tudinal ligament. J Neurosurg. 1998;89:217-23.
86. Itoh T, Tsuji H. Technical improvements and results of laminoplasty for com-pressive myelopathy in the cervical spine. Spine. 1985;10:729-36.
87. Hirabayashi K, Toyama Y, Chiba K. Expansive laminoplasty for myelopathy in ossification of the longitudinal ligament. Clin Orthop Relat Res. 1999;359:35-48.
88. Kohno K, Kumon Y, Oka Y, Matsui S, Ohue S, Sakaki S. Evaluation of prognos-tic factors following expansive laminoplasty for cervical spinal stenotic myelopa-thy. Surg Neurol. 1997;48:237-45.
89. Callahan RA, Johnson RM, Margolis RN, Keggi KJ, Albright JA, Southwick WO. Cervical facet fusion for control of instability following laminectomy. J Bone Joint Surg Am. 1977;59:991-1002.
90. Kumar VG, Rea GL, Mervis LJ, McGregor JM. Cervical spondylotic myelopathy: functional and radiographic long-term outcome after laminectomy and posterior fusion. Neurosurgery. 1999;44:771-8.
91. Maurer PK, Ellenbogen RG, Ecklund J, Simonds GR, van Dam B, Ondra SL. Cervical spondylotic myelopathy: treatment with posterior decompression and Lu-que rectangle bone fusion. Neurosurgery. 1991;28:680-4.
92. Houten JK, Cooper PR. Laminectomy and posterior cervical plating for multi-level cervical spondylotic myelopathy and ossification of the posterior longitudinal ligament: effects on cervical alignment, spinal cord compression, and neurologi-cal outcome. Neurosurgery. 2003;52:1081-8.
93. Epstein NE. Laminectomy with posterior wiring and fusion for cervical ossifi-cation of the posterior longitudinal ligament, spondylosis, ossification of the yel-low ligament, stenosis, and instability: a study of 5 patients. J Spinal Disord. 1999;12:461-6.
94. Heller JG, Edwards CC 2nd, Murakami H, Rodts GE. Laminoplasty versus laminectomy and fusion for multilevel cervical myelopathy: an independent matched cohort analysis. Spine. 2001;26:1330-6.
95. Abumi K, Kaneda K, Shono Y, Fujiya M. One-stage posterior decompression and reconstruction of the cervical spine by using pedicle screw fixation systems. J Neurosurg. 1999;90(1 Suppl):19-26.
96. Heller JG, Silcox DH 3rd, Sutterlin CE 3rd. Complications of posterior cervical plating. Spine. 1995;20:2442-8.
97. Graham AW, Swank ML, Kinard RE, Lowery GL, Dials BE. Posterior cervical ar-throdesis and stabilization with a lateral mass plate. Clinical and computed tomo-graphic evaluation of lateral mass screw placement and associated complications. Spine. 1996;21:323-9.
98. Jones EL, Heller JG, Silcox DH, Hutton WC. Cervical pedicle screws versus lateral mass screws. Anatomic feasibility and biomechanical comparison. Spine. 1997;22:977-82.
99. Miyazaki K, Tada K, Matsuda Y, Okuno M, Yasuda T, Murakami H. Posterior ex-tensive simultaneous multisegment decompression with posterolateral fusion for cervical myelopathy with cervical instability and kyphotic and/or S-shaped defor-mities. Spine. 1989;14:1160-70.
100. Hamanishi C, Tanaka S. Bilateral multilevel laminectomy with or without posterolateral fusion for cervical spondylotic myelopathy: relationship to type of onset and time until operation. J Neurosurg. 1996;85:447-51.
101. Kawaguchi Y, Kanamori M, Ishiara H, Nobukiyo M, Seki S, Kimura T. Preven-tive measures for axial symptoms following cervical laminoplasty. J Spinal Disord Tech. 2003;16:497-501.
102. Baba H, Furusawa N, Chen Q, Imura S. Cervical laminoplasty in patients with ossification of the posterior longitudinal ligaments. Paraplegia. 1995;33:25-9.
103. Nurick S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain. 1972;95:87-100.
104. Hukuda S, Mochizuki T, Ogata M, Shichikawa K, Shimomura Y. Operations for cervical spondylotic myelopathy. A comparison of the results of anterior and posterior procedures. J Bone Joint Surg Br. 1985;67:609-15.
105. Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper PR. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999;44:762-70.
106. Batzdorf U, Batzdorff A. Analysis of cervical spine curvature in patients with cervical spondylosis. Neurosurgery. 1988;22:827-36.
107. Fukushima T, Ikata T, Taoka Y, Takata S. Magnetic resonance imaging study on spinal cord plasticity in patients with cervical compression myelopathy. Spine. 1991;16(10 Suppl):S534-8.
108. Wang MY, Shah S, Green BA. Clinical outcomes following cervical lamino-plasty for 204 patients with cervical spondylotic myelopathy. Surg Neurol. 2004;62:487-93.
109. Good DC, Couch JR, Wacaser L. “Numb, clumsy hands” and high cervical spondylosis. Surg Neurol. 1984;22:285-91.
110. Voskuhl RR, Hinton RC. Sensory impairment in the hands secondary to spondylotic compression of the cervical spinal cord. Arch Neurol. 1990;47:309-11. Erratum in: Arch Neurol. 1990;47:653.
111. Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K. Myelopathy hand. New clinical signs of cervical cord damage. J Bone Joint Surg Br. 1987;69:215-9.
112. Stark RJ, Kennard C, Swash M. Hand wasting in spondylotic high cord com-pression: an electromyographic study. Ann Neurol. 1981;9:58-62.
113. Prabhu K, Babu KS, Samuel S, Chacko AG. Rapid opening and closing of the hand as a measure of early neurologic recovery in the upper extremity after surgery for cervical spondylotic myelopathy. Arch Phys Med Rehabil. 2005;86:105-8.
114. Bertalanffy H, Eggert HR. Clinical long-term results of anterior discectomy without fusion for treatment of cervical radiculopathy and myelopathy. A follow-up of 164 cases. Acta Neurochir (Wien).1988;90:127-35.
115. Edwards CC 2nd, Heller JG, Murakami H. Corpectomy versus laminoplasty for multilevel cervical myelopathy: an independent matched-cohort analysis. Spine. 2002;27:1168-75.
116. Sakaura H, Hosono N, Mukai Y, Ishii T, Iwasaki M, Yoshikawa H. Long-term outcome of laminoplasty for cervical myelopathy due to disc herniation: a compar-ative study of laminoplasty and anterior spinal fusion. Spine. 2005;30:756-9.
117. Yonenobu K, Hosono N, Iwasaki M, Asano M, Ono K. Laminoplasty versus subtotal corpectomy. A comparative study of results in multisegmental cervical spondylotic myelopathy. Spine. 1992;17:1281-4.
118. Yonenobu K, Yamamoto T, Ono K. Laminoplasty for myelopathy: indications, results, outcomes, and complications. In: Clark CR, editor. The cervical spine. 3rd ed. Philadelphia: Lippincott-Raven; 1998. p 849-64.
119. Hosono N, Yonenobu K, Ono K. Neck and shoulder pain after laminoplasty. A noticeable complication. Spine. 1996;21:1969-73.
120. Yoshida M, Tamaki T, Kawakami M, Nakatani N, Ando M, Yamada H, Ha-yashi N. Does reconstruction of posterior ligamentous complex with extensor musculature decrease axial symptoms after cervical laminoplasty? Spine. 2002;27:1414-8.
121. Shiraishi T. Skip laminectomy—a new treatment for cervical spondylotic my-elopathy, preserving bilateral muscular attachments to the spinous processes: a preliminary report. Spine J. 2002;2:108-15.
122. Yoshida M, Otani K, Shibasaki K, Ueda S. Expansive laminoplasty with reat-tachment of spinous process and extensor musculature for cervical myelopathy. Spine. 1992;17:491-7.
123. Shiraishi T, Fukuda K, Yato Y, Nakamura M, Ikegami T. Results of skip lami-nectomy-minimum 2-year follow-up study compared with open-door laminoplasty. Spine. 2003;28:2667-72.
124. Kawai S, Sunago K, Doi K, Saika M, Taguchi T. Cervical laminoplasty (Hat-tori's method). Procedure and follow-up results. Spine. 1988;13:1245-50.
125. Kimura I, Shingu H, Nasu Y. Long-term follow-up of cervical spondylotic myelopathy treated by canal-expansive laminoplasty. J Bone Joint Surg Br. 1995;77:956-61.
126. Hilibrand A, Berta S, Daffner S. The impact of anterior cervical fusion upon overall range of motion and neck flexibility. In: Proceedings of the Annual Meeting of the North American Spine Society; 2003 Oct 21-25; San Diego, CA.
127. Hanai K, Fujiyoshi F, Kamei K. Subtotal vertebrectomy and spinal fusion for cervical spondylotic myelopathy. Spine. 1986;11:310-5.
128. Sasai K, Saito T, Akagi S, Kato I, Ogawa R. Cervical curvature after lamino-plasty for spondylotic myelopathy—involvement of yellow ligament, semispinalis cervicis muscle, and nuchal ligament. J Spinal Disord. 2000;13:26-30.
129. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopa-thy and myelopathy at segments adjacent to the site of a previous anterior cervi-cal arthrodesis. J Bone Joint Surg Am. 1999;81:519-28.
130. Rao RD, Wang M, McGrady LM, Perlewitz TJ, David KS. Does anterior plating of the cervical spine predispose to adjacent segment changes? Spine. 2005;30:2788-93.

1640
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 88-A · NU M B E R 7 · JU LY 2006OP E R AT IVE TREA T M EN T OF CER V ICA L SP O NDY L O T I C MYE LOPA THY
131. Flynn TB. Neurologic complications of anterior cervical interbody fusion. Spine. 1982;7:536-9.
132. Yonenobu K, Hosono N, Iwasaki M, Asano M, Ono K. Neurologic complica-tions of surgery for cervical compression myelopathy. Spine. 1991;16:1277-82.
133. Satomi K, Ogawa J, Ishii Y, Hirabayashi K. Short-term complications and long-term results of expansive open-door laminoplasty for cervical stenotic myel-opathy. Spine J. 2001;1:26-30.
134. Komagata M, Nishiyama M, Endo K, Ikegami H, Tanaka S, Imakiire A. Pro-phylaxis of C5 palsy after cervical expansive laminoplasty by bilateral partial foraminotomy. Spine J. 2004;4:650-5.
135. Apfelbaum RI, Kriskovich MD, Haller JR. On the incidence, cause, and pre-vention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine. 2000;25:2906-12.
136. Heeneman H. Vocal cord paralysis following approaches to the anterior cer-vical spine. Laryngoscope. 1973;83:17-21.
137. Bazaz R, Lee MJ, Yoo JU. Incidence of dysphagia after anterior cervical spine surgery: a prospective study. Spine. 2002;27:2453-8.
138. Pompili A, Canitano S, Caroli F, Caterino M, Crecco M, Raus L, Occhipinti
E. Asymptomatic esophageal perforation caused by late screw migration after anterior cervical plating: report of a case and review of relevant literature. Spine. 2002;27:E499-502.
139. Shenoy SN, Raja A. Delayed pharyngo-esophageal perforation: rare compli-cation of anterior cervical spine surgery. Neurol India. 2003;51:534-6.
140. Curylo LJ, Mason HC, Bohlman HH, Yoo JU. Tortuous course of the vertebral artery and anterior cervical decompression: a cadaveric and clinical case study. Spine. 2000;25:2860-4.
141. Eleraky MA, Llanos C, Sonntag VK. Cervical corpectomy: report of 185 cases and review of the literature. J Neurosurg. 1999;90(1 Suppl):35-41.
142. Jimenez JC, Sani S, Braverman B, Deutsch H, Ratliff JK. Palsies of the fifth cervical nerve root after cervical decompression: prevention using continuous in-traoperative electromyography monitoring. J Neurosurg Spine. 2005;3:92-7.
143. Papastefanou SL, Henderson LM, Smith NJ, Hamilton A, Webb JK. Surface electrode somatosensory-evoked potentials in spinal surgery: implications for in-dications and practice. Spine. 2000;25:2467-72.
144. Epstein NE, Danto J, Nardi D. Evaluation of intraoperative somatosensory-evoked potential monitoring during 100 cervical operations. Spine. 1993;18:737-47.