ophthalmology panre review - ncapancapa.org/wp-content/uploads/2017/02/eye-review_pt.-1.pdf ·...
TRANSCRIPT
Ophthalmology
PANRE Review Brock Phillips, PA-C
I am not an ophthalmologist, optometrist or
certified eye guy of any sort - I am a
practicing UC/EM PA-C who frequently
evaluates eye/vision complaints, consults
Ophtho regularly and has taken an interest
in the topic. Eyes are fascinating!
Thanks to Joshua F. Smith, PA-C - who
originally created this lecture and
graciously allowed me to adapt it
Review A&P of the eye and topics covered
on PANRE Blueprint – buzzwords & key points
are noted in red
Score 100% on the ophthalmology questions!
Augment your clinical practice with a few
ophtho pearls, tips and tricks
Blepharitis
Blowout fracture
Cataract
Chalazion
Conjunctivitis
Corneal abrasion
Corneal ulcer
Dacryoadenitis
Ectropion
Entropion
Foreign body
Glaucoma
Hordeolum
Hyphema
Macular degeneration
Nystagmus
Optic neuritis
Orbital cellulitis
Papilledema
Pterygium
Retinal detachment
Retinal vascular occlusion
Retinopathy
Strabismus
Work from the outside inward…
Gross exam - photophobia, asymmetry,
doorknob DXs
Visual acuity
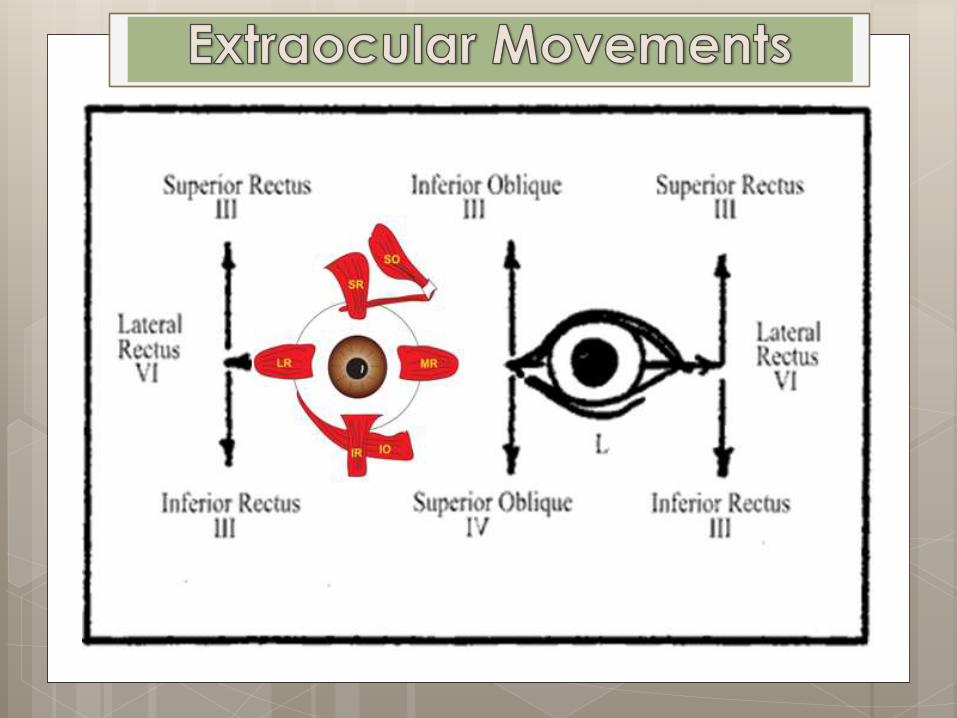
EOMs and visual fields
Periorbital eye, lids, lashes, glands & ducts
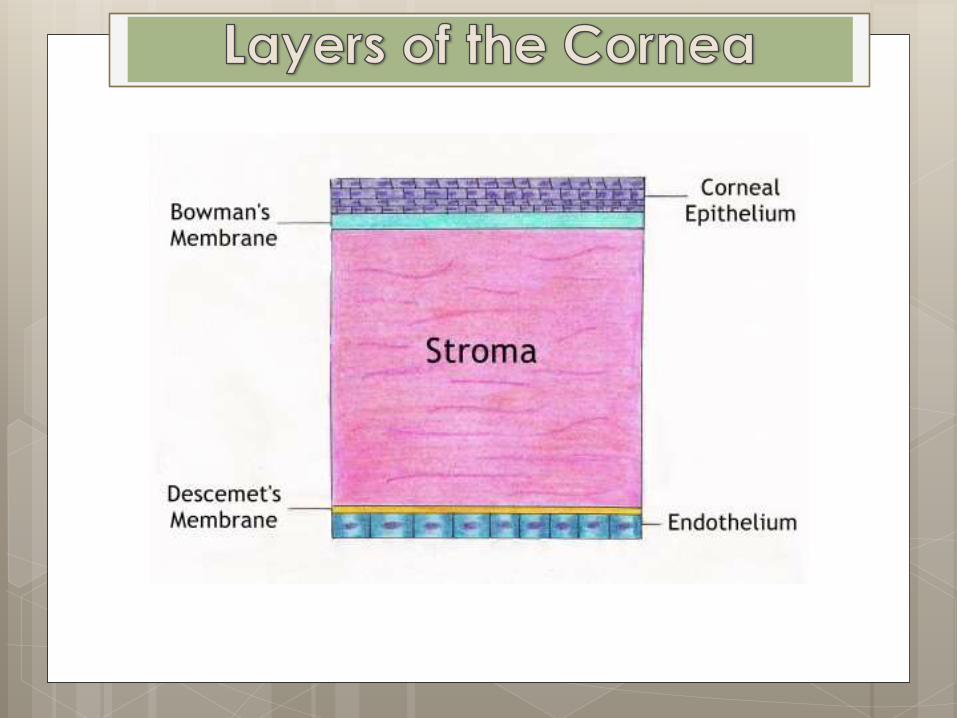
Conjunctiva, sclera & cornea
Iris & limbus
Pupillary size & response
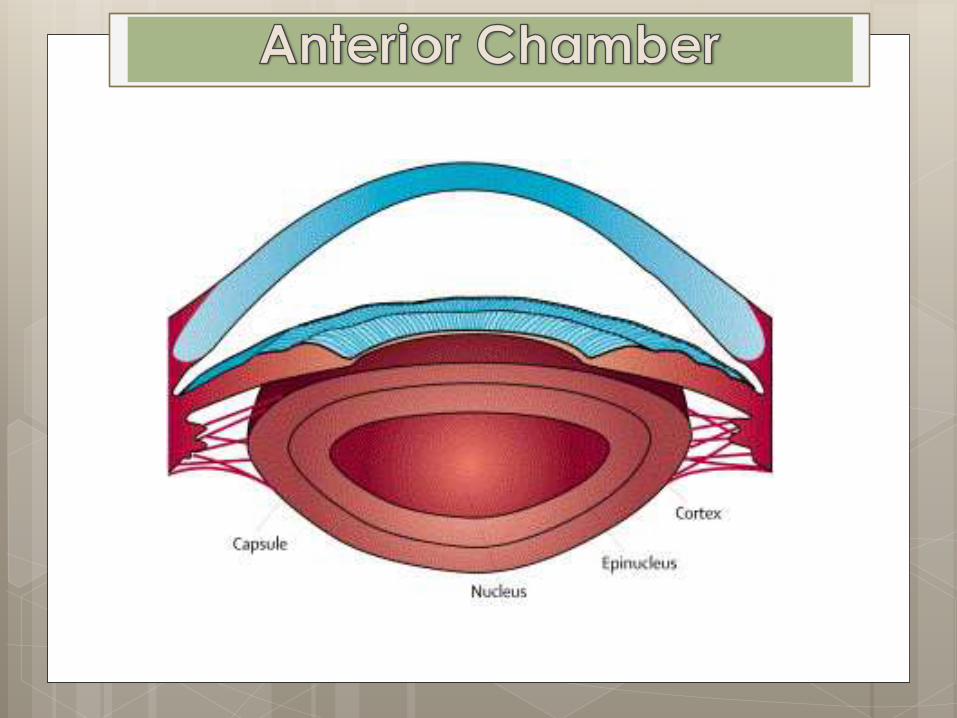
Anterior chamber
Posterior chamber
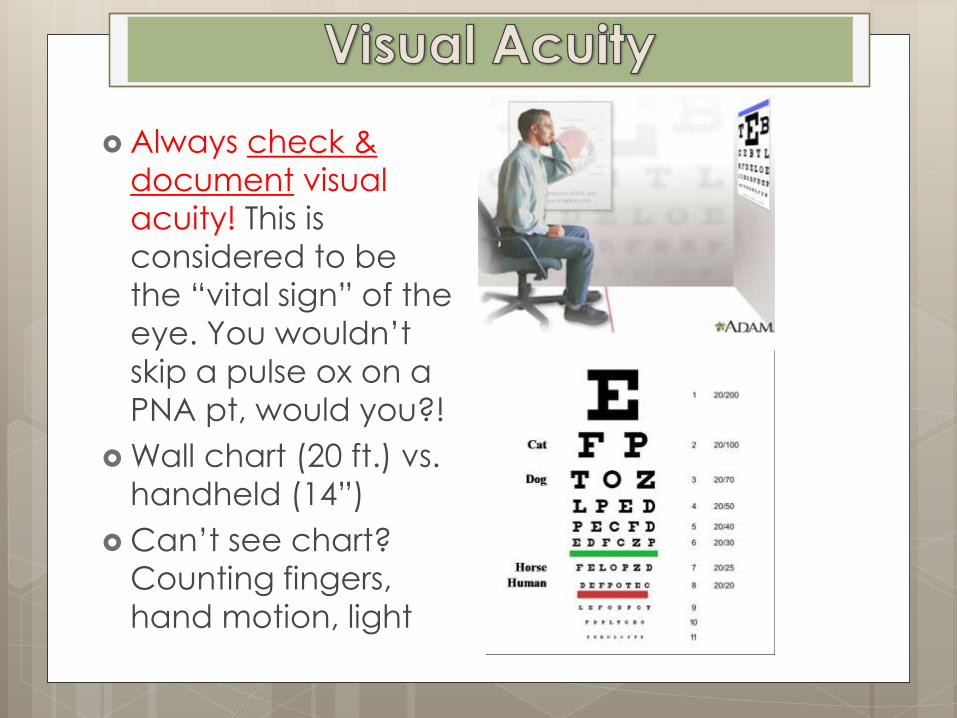
Always check &
document visual
acuity! This is
considered to be
the “vital sign” of the
eye. You wouldn’t
skip a pulse ox on a
PNA pt, would you?!
Wall chart (20 ft.) vs.
handheld (14”)
Can’t see chart?
Counting fingers,
hand motion, light
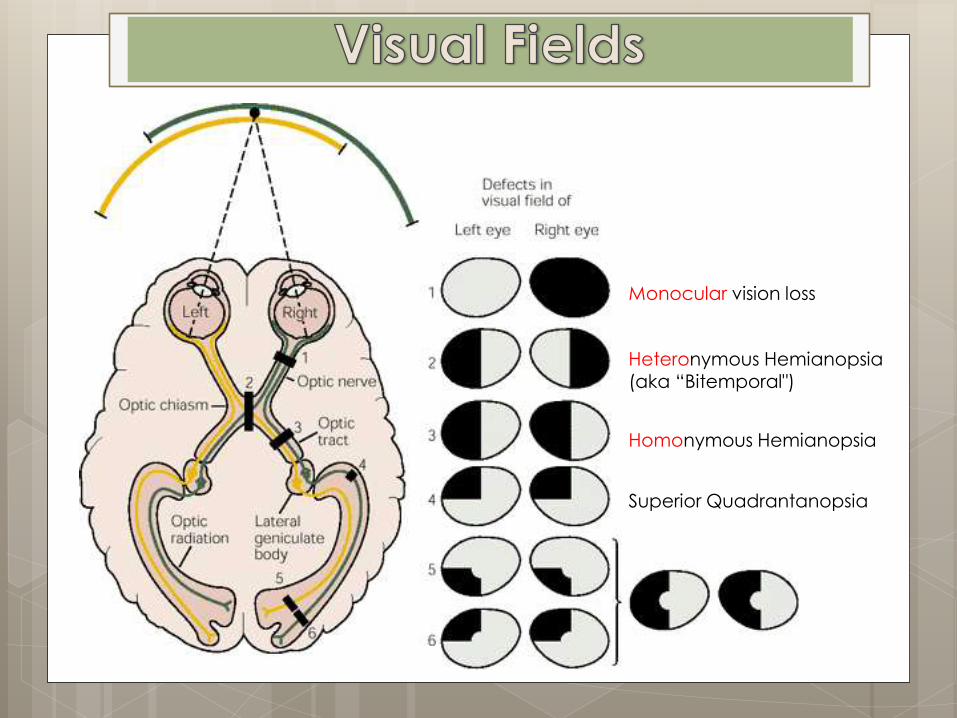
Homonymous Hemianopsia
Heteronymous Hemianopsia (aka “Bitemporal")
Superior Quadrantanopsia
Monocular vision loss
http://openi.nlm.nih.gov/imgs/rescaled512/3223174_pone.0027095.g001.png
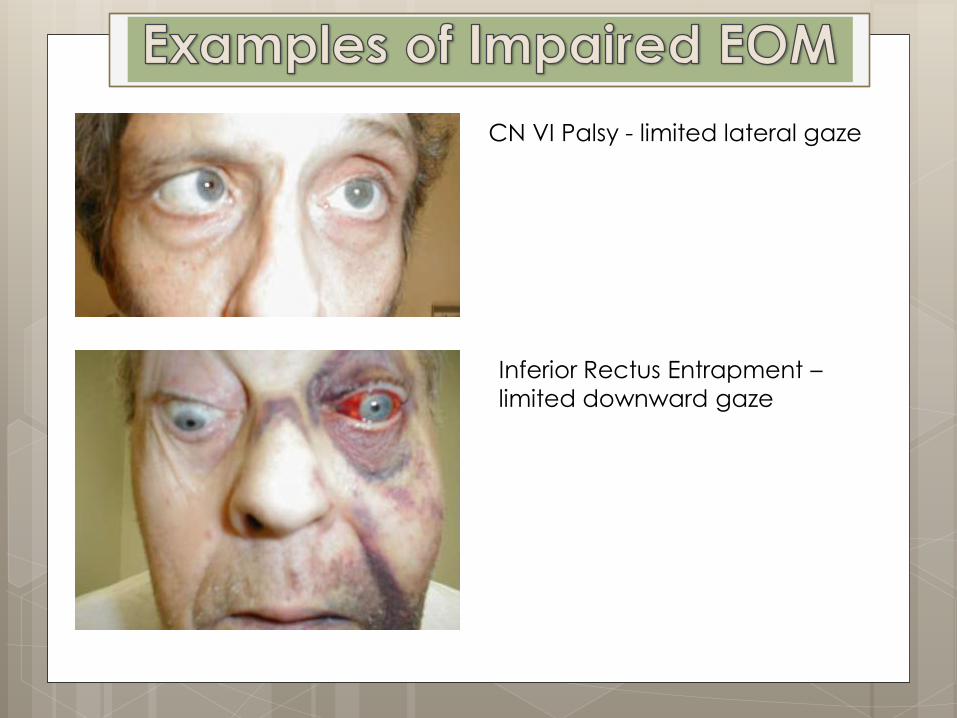
CN VI Palsy - limited lateral gaze
Inferior Rectus Entrapment –
limited downward gaze
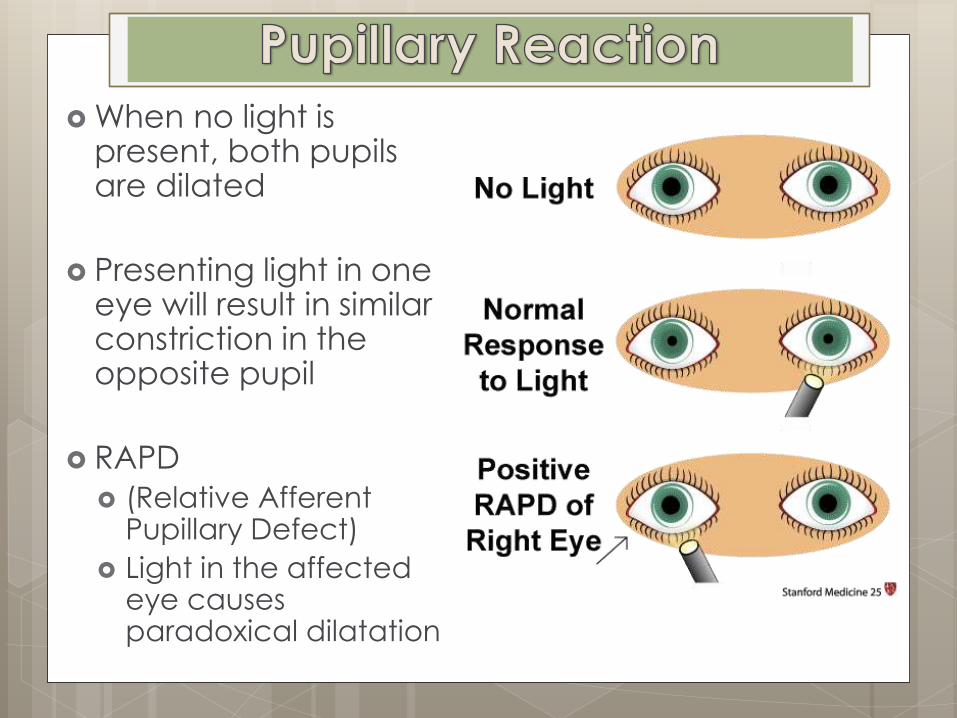
When no light is present, both pupils are dilated
Presenting light in one eye will result in similar constriction in the opposite pupil
RAPD
(Relative Afferent Pupillary Defect)
Light in the affected eye causes paradoxical dilatation
Lids and
Conjunctiva Blepharitis
Ectropion/Entropion
Chalazion
Hordeolum
Dacryocystitis
Conjunctivitis
Pterygium
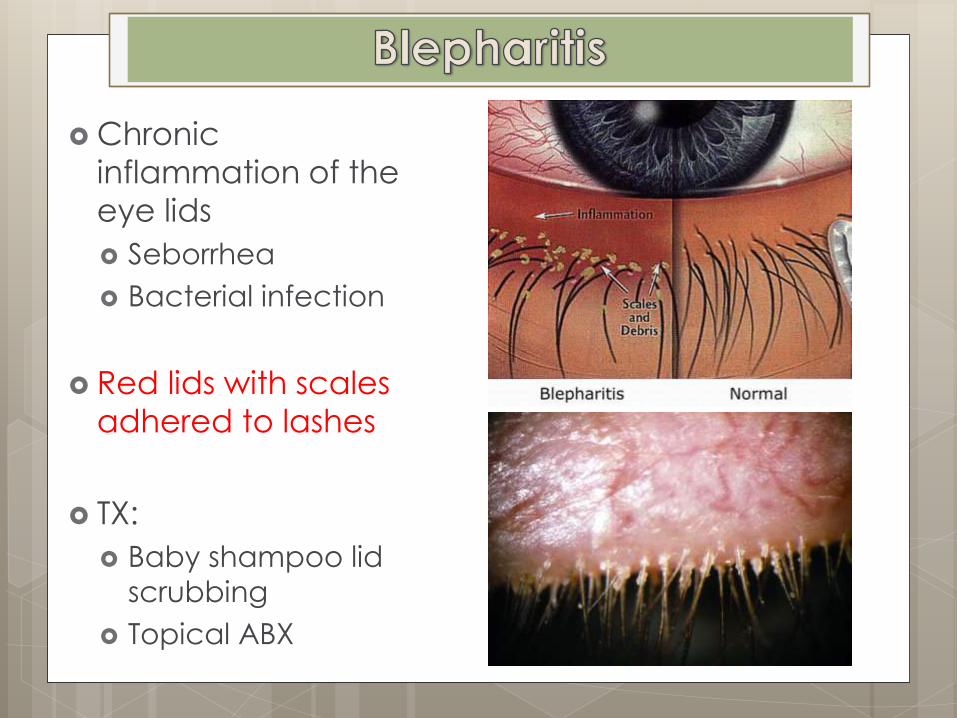
Chronic
inflammation of the
eye lids
Seborrhea
Bacterial infection
Red lids with scales
adhered to lashes
TX:
Baby shampoo lid
scrubbing
Topical ABX
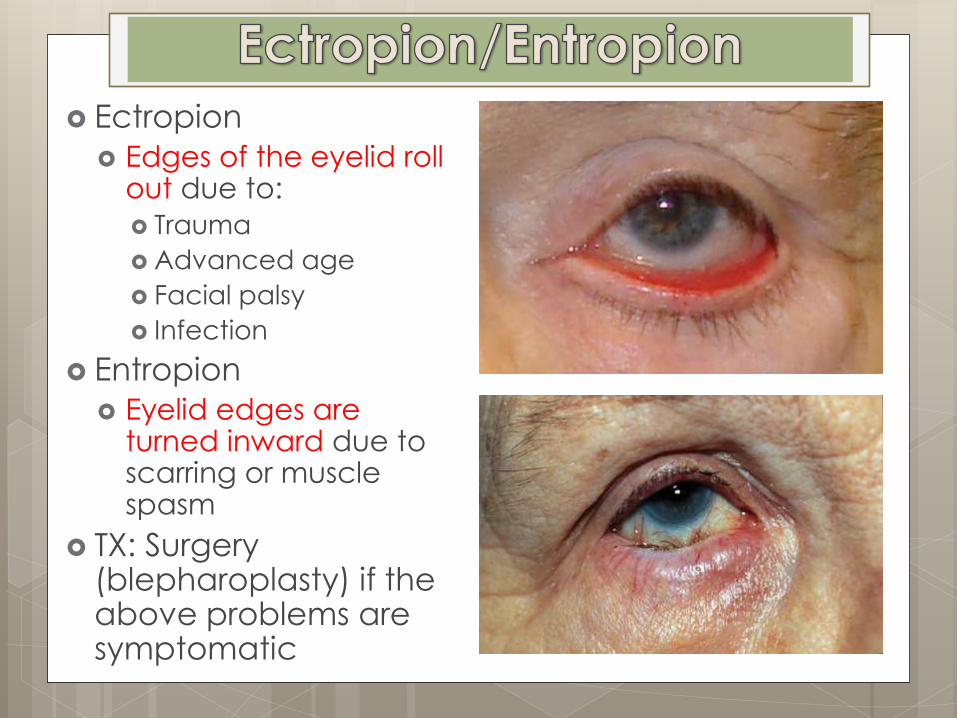
Ectropion
Edges of the eyelid roll out due to:
Trauma
Advanced age
Facial palsy
Infection
Entropion
Eyelid edges are turned inward due to scarring or muscle spasm
TX: Surgery (blepharoplasty) if the above problems are symptomatic
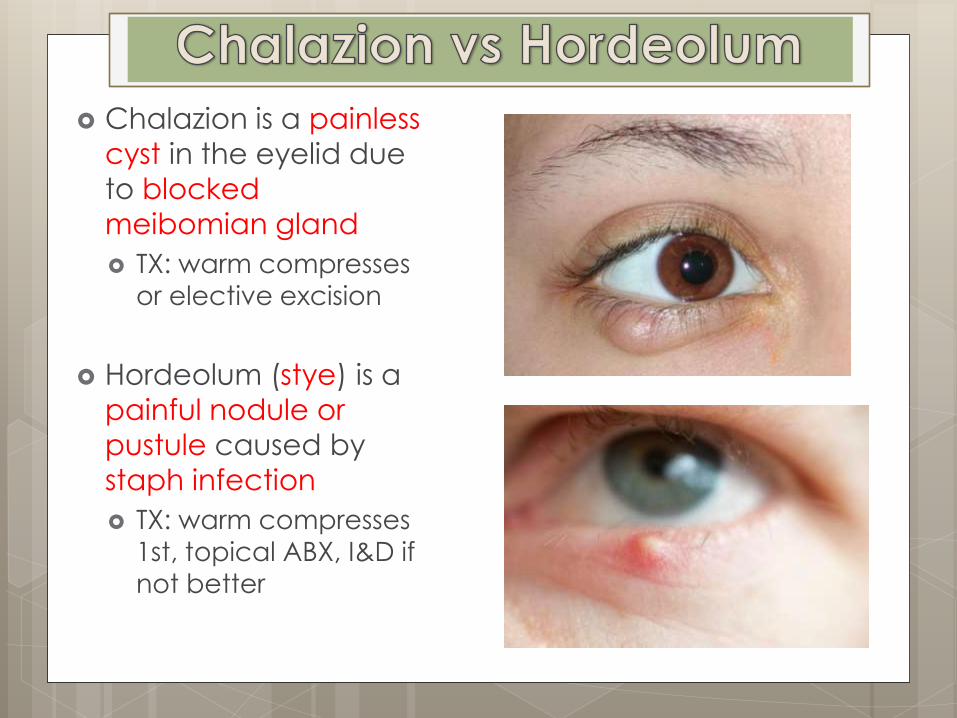
Chalazion is a painless
cyst in the eyelid due
to blocked
meibomian gland
TX: warm compresses
or elective excision
Hordeolum (stye) is a
painful nodule or
pustule caused by
staph infection
TX: warm compresses
1st, topical ABX, I&D if
not better
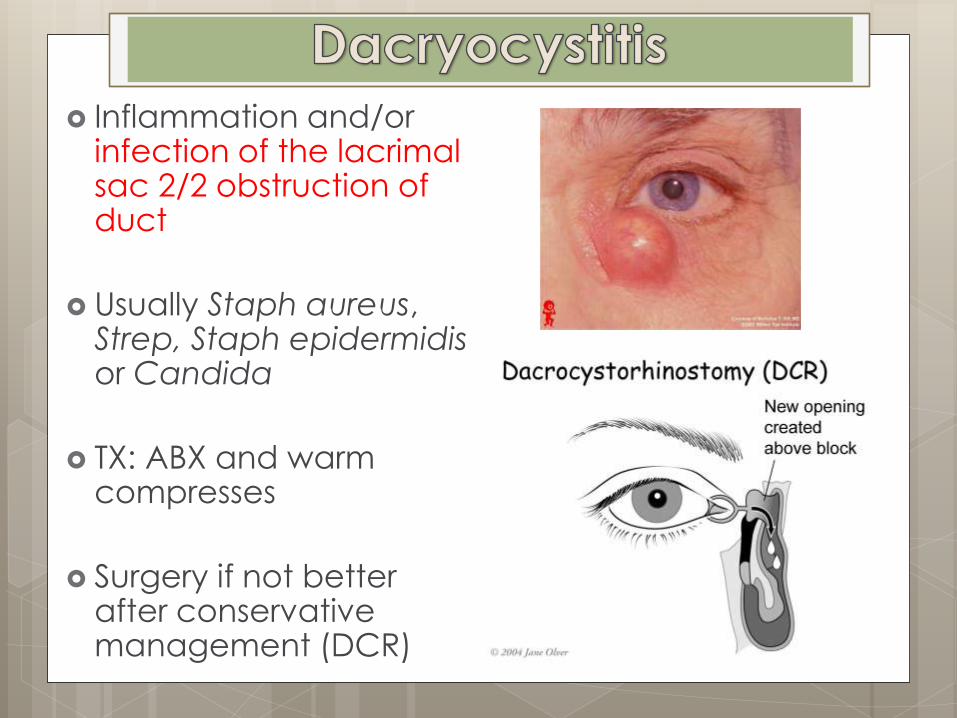
Inflammation and/or infection of the lacrimal sac 2/2 obstruction of duct
Usually Staph aureus, Strep, Staph epidermidis or Candida
TX: ABX and warm compresses
Surgery if not better after conservative management (DCR)
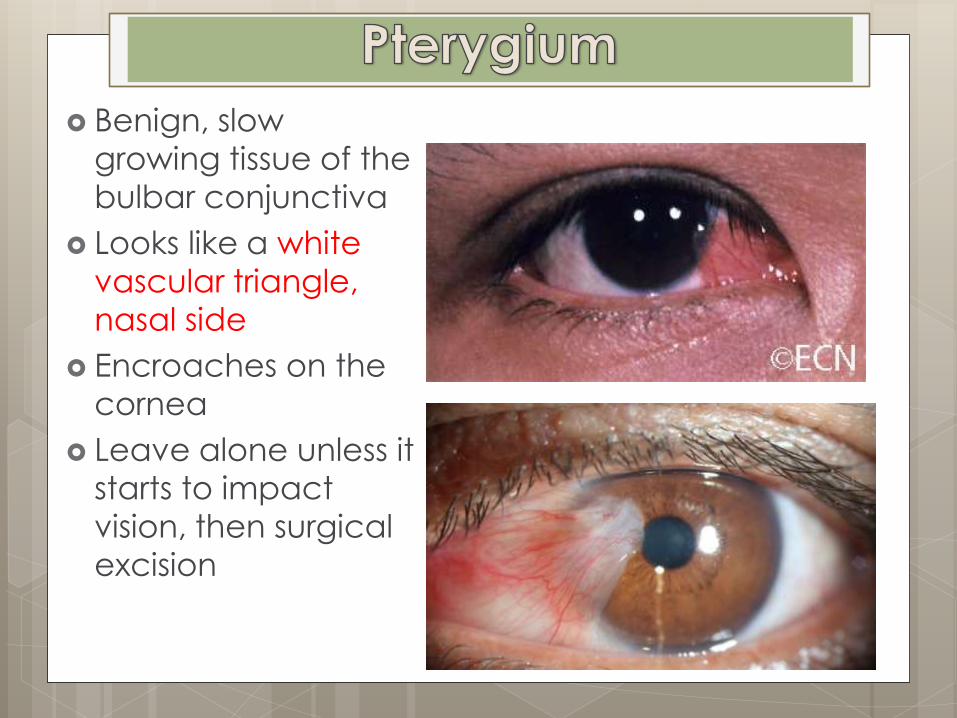
Benign, slow
growing tissue of the
bulbar conjunctiva
Looks like a white
vascular triangle,
nasal side
Encroaches on the
cornea
Leave alone unless it
starts to impact
vision, then surgical
excision
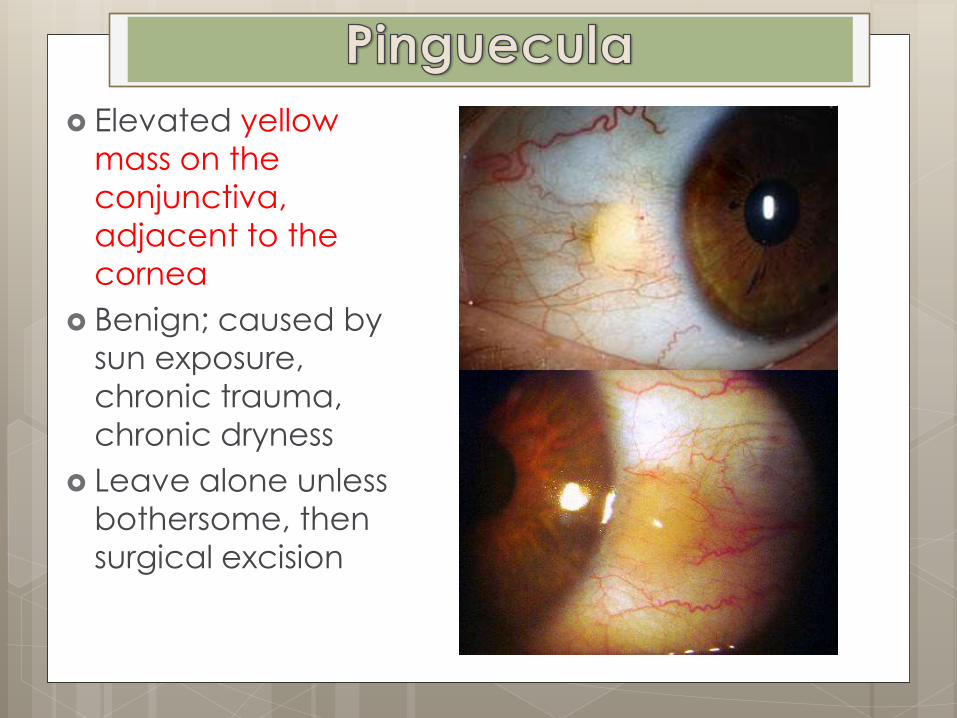
Elevated yellow
mass on the
conjunctiva,
adjacent to the
cornea
Benign; caused by
sun exposure,
chronic trauma,
chronic dryness
Leave alone unless
bothersome, then
surgical excision
Conjunctivitis Allergic
Viral
Bacterial
HSV/Zoster
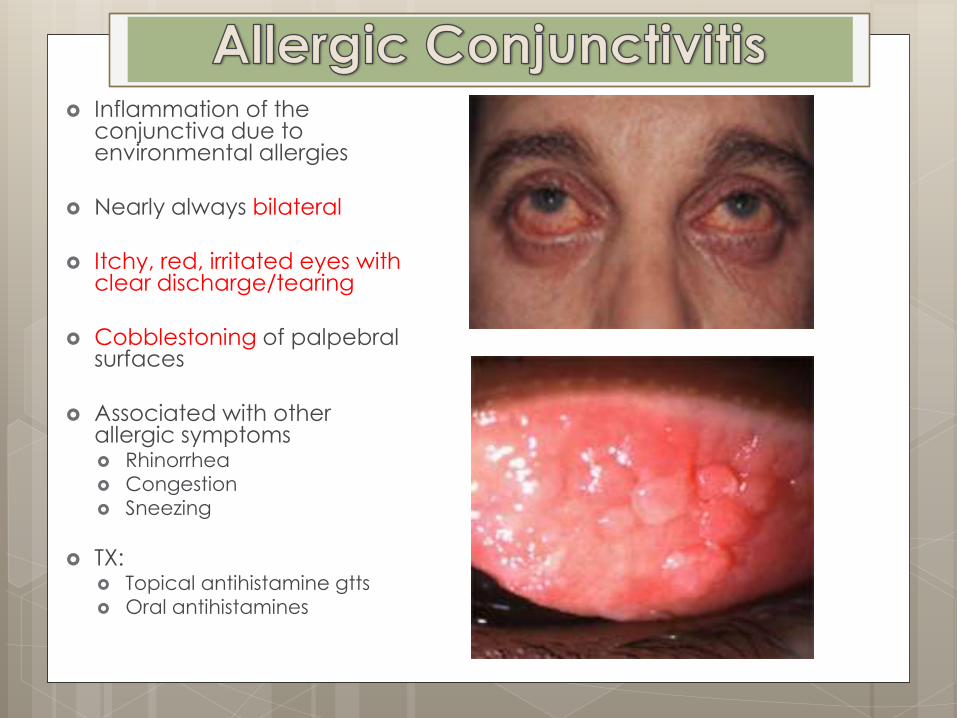
Inflammation of the conjunctiva due to environmental allergies
Nearly always bilateral
Itchy, red, irritated eyes with clear discharge/tearing
Cobblestoning of palpebral surfaces
Associated with other allergic symptoms Rhinorrhea
Congestion
Sneezing
TX: Topical antihistamine gtts
Oral antihistamines
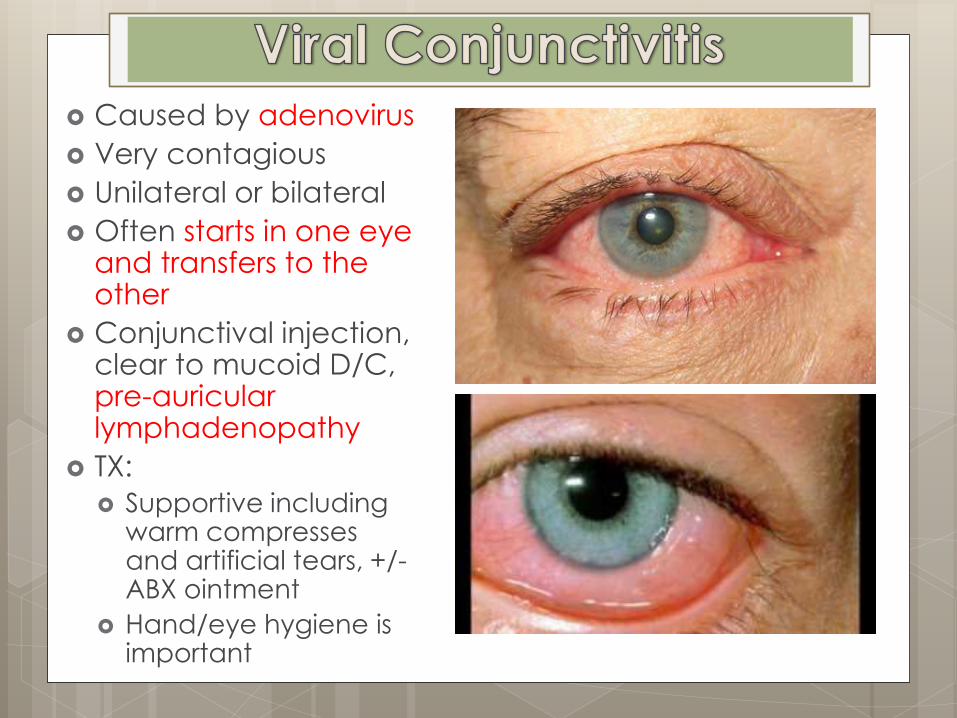
Caused by adenovirus
Very contagious
Unilateral or bilateral
Often starts in one eye and transfers to the other
Conjunctival injection, clear to mucoid D/C, pre-auricular lymphadenopathy
TX:
Supportive including warm compresses and artificial tears, +/- ABX ointment
Hand/eye hygiene is important
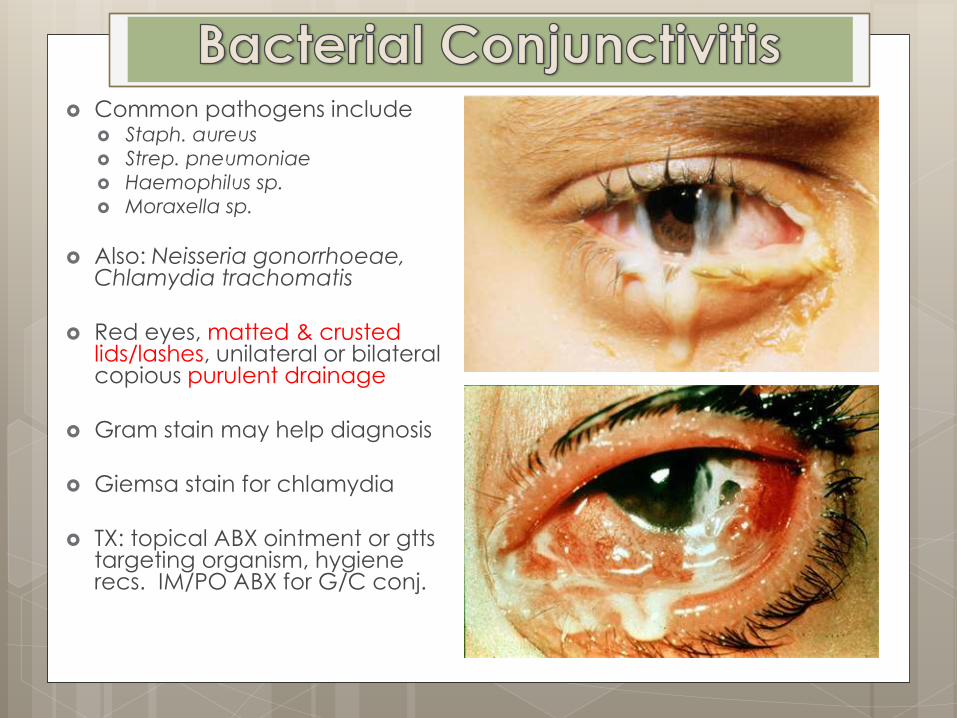
Common pathogens include Staph. aureus
Strep. pneumoniae
Haemophilus sp.
Moraxella sp.
Also: Neisseria gonorrhoeae, Chlamydia trachomatis
Red eyes, matted & crusted lids/lashes, unilateral or bilateral copious purulent drainage
Gram stain may help diagnosis
Giemsa stain for chlamydia
TX: topical ABX ointment or gtts targeting organism, hygiene recs. IM/PO ABX for G/C conj.
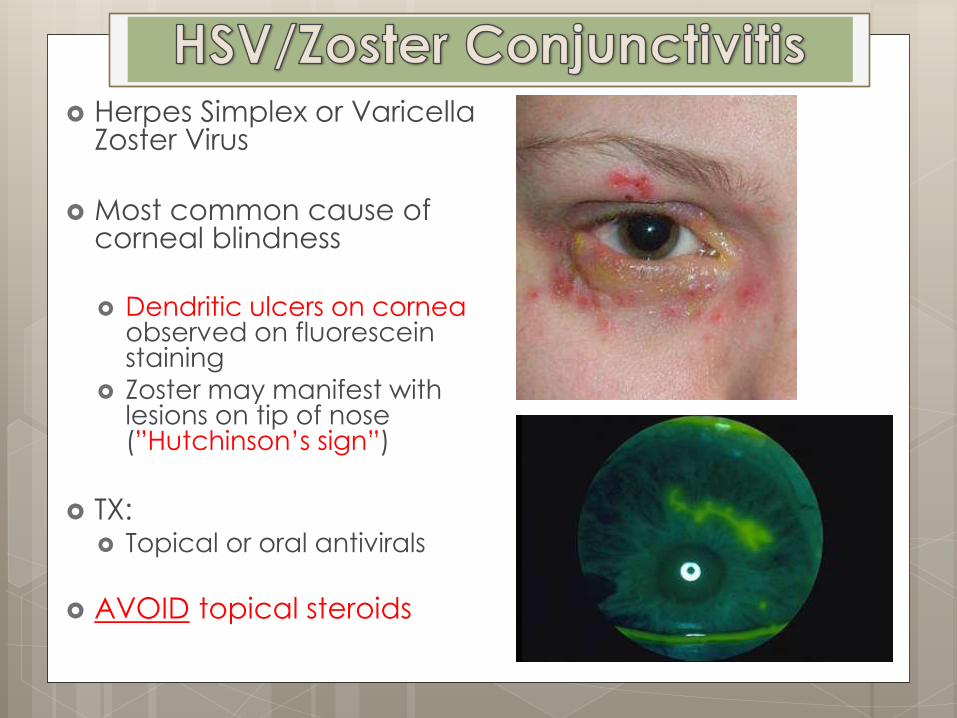
Herpes Simplex or Varicella Zoster Virus
Most common cause of corneal blindness
Dendritic ulcers on cornea
observed on fluorescein staining
Zoster may manifest with lesions on tip of nose (”Hutchinson’s sign”)
TX: Topical or oral antivirals
AVOID topical steroids
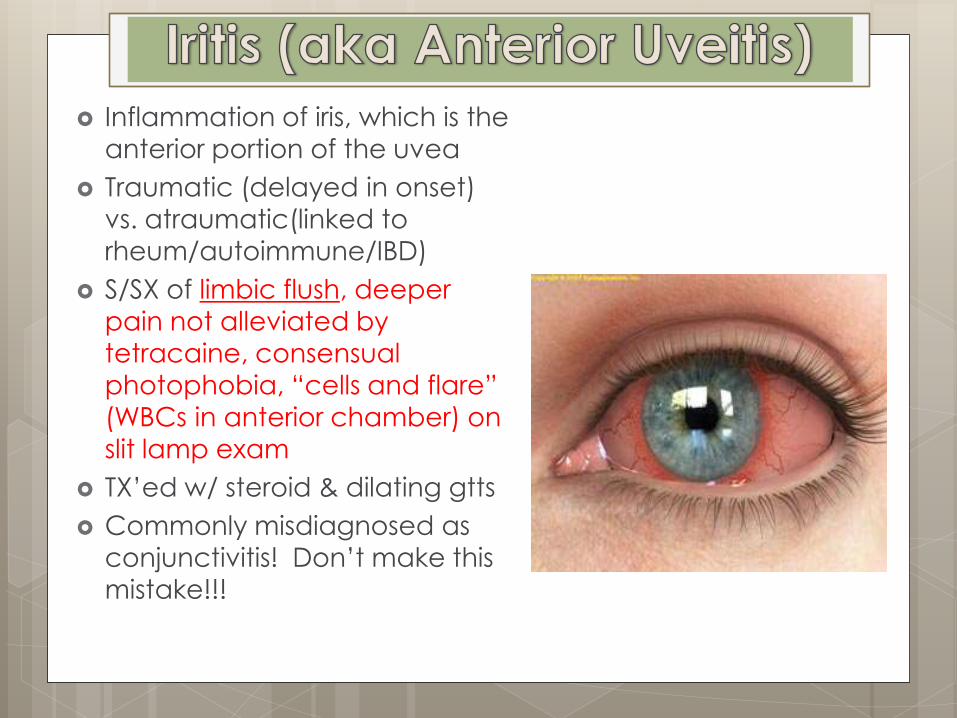
Inflammation of iris, which is the
anterior portion of the uvea
Traumatic (delayed in onset)
vs. atraumatic(linked to
rheum/autoimmune/IBD)
S/SX of limbic flush, deeper
pain not alleviated by
tetracaine, consensual
photophobia, “cells and flare”
(WBCs in anterior chamber) on
slit lamp exam
TX’ed w/ steroid & dilating gtts
Commonly misdiagnosed as conjunctivitis! Don’t make this mistake!!!
Anterior
Chamber/Lens Corneal Abrasion
Corneal Ulcer
Cataract
Glaucoma
Hyphema
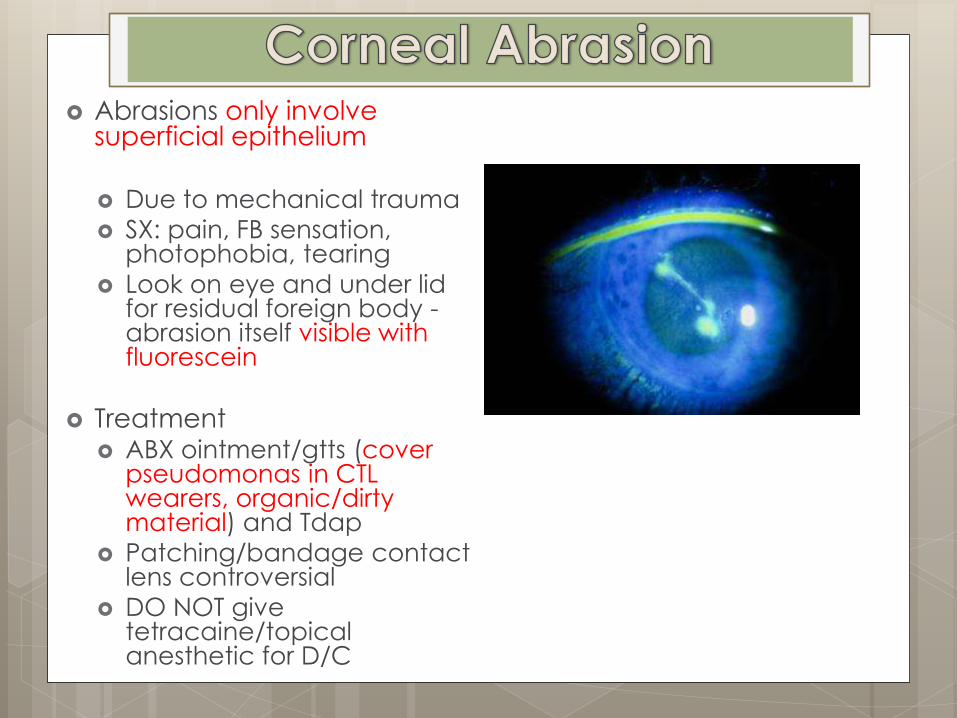
Abrasions only involve superficial epithelium Due to mechanical trauma
SX: pain, FB sensation, photophobia, tearing
Look on eye and under lid for residual foreign body - abrasion itself visible with fluorescein
Treatment ABX ointment/gtts (cover
pseudomonas in CTL wearers, organic/dirty material) and Tdap
Patching/bandage contact lens controversial
DO NOT give tetracaine/topical anesthetic for D/C
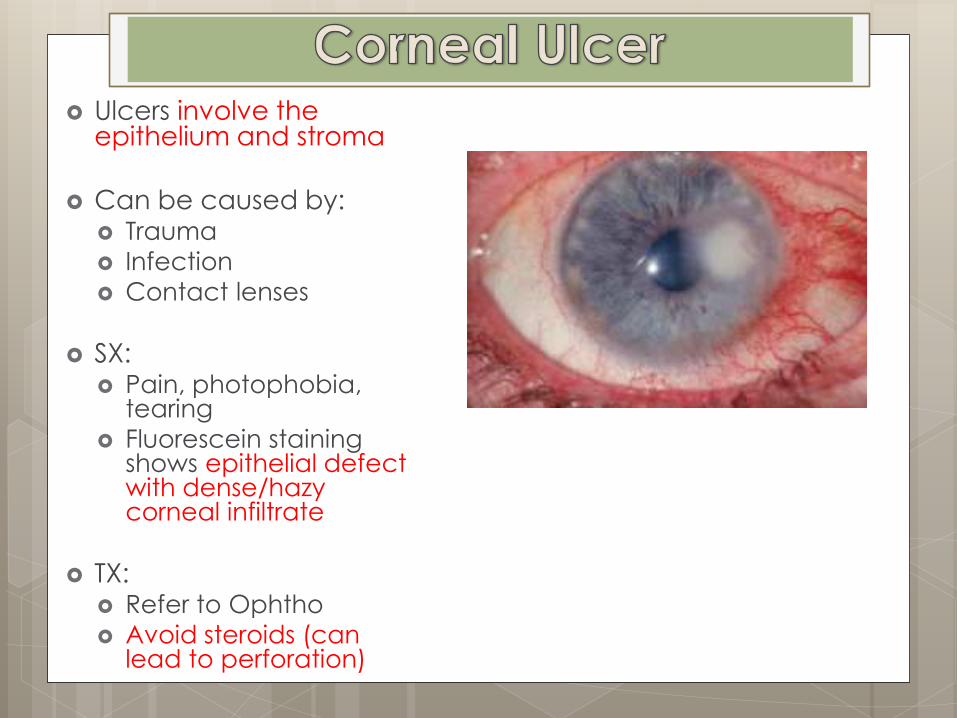
Ulcers involve the epithelium and stroma
Can be caused by: Trauma
Infection
Contact lenses
SX: Pain, photophobia,
tearing
Fluorescein staining shows epithelial defect with dense/hazy corneal infiltrate
TX: Refer to Ophtho
Avoid steroids (can lead to perforation)
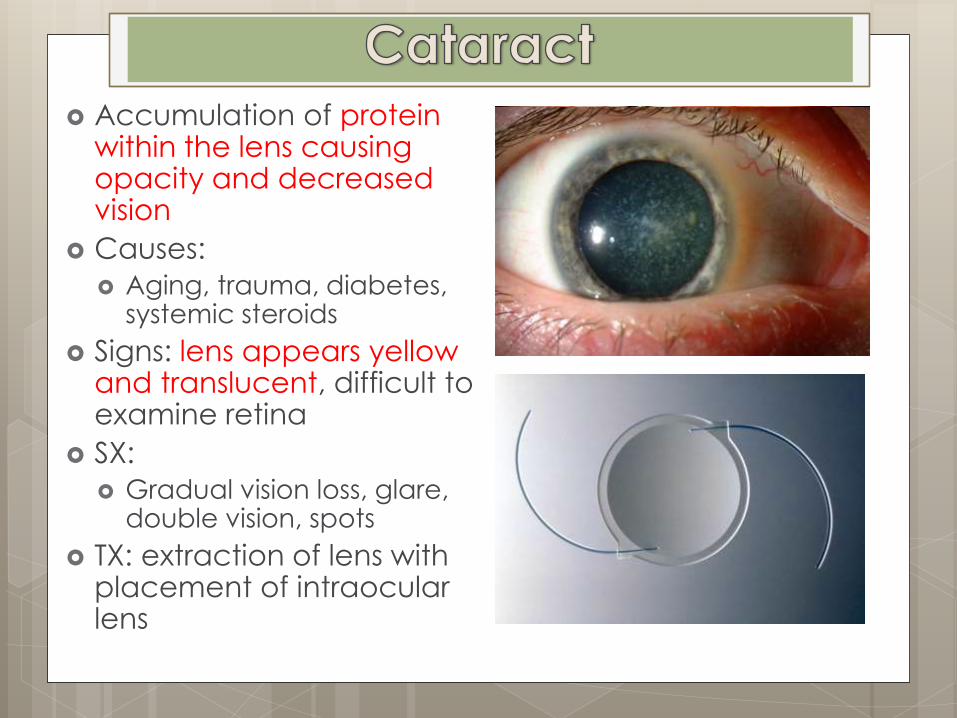
Accumulation of protein within the lens causing opacity and decreased vision
Causes:
Aging, trauma, diabetes, systemic steroids
Signs: lens appears yellow and translucent, difficult to examine retina
SX:
Gradual vision loss, glare, double vision, spots
TX: extraction of lens with placement of intraocular lens
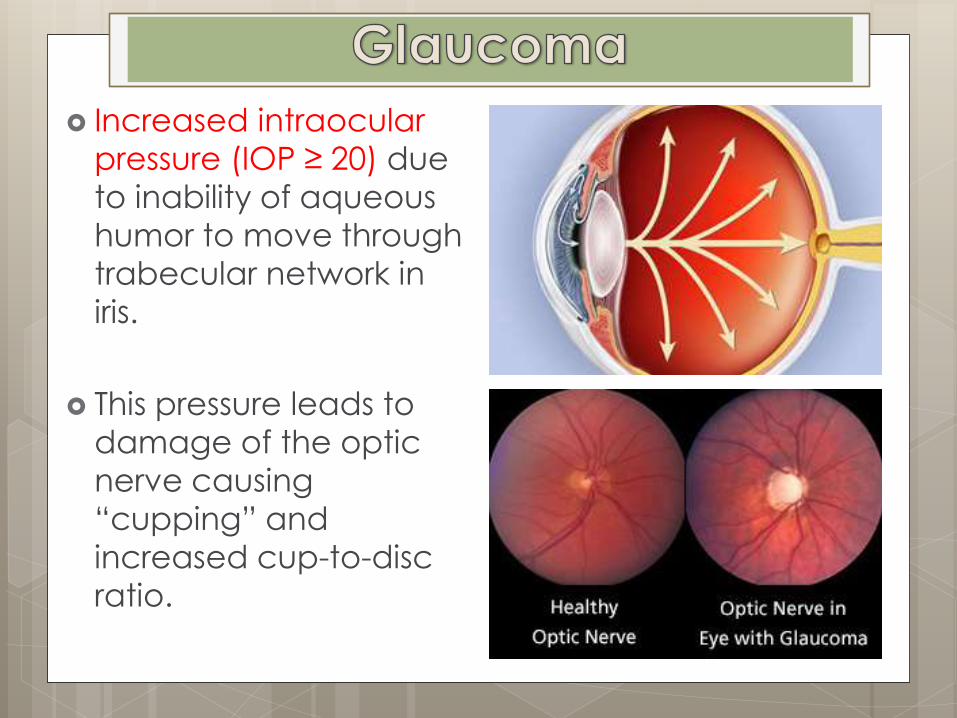
Increased intraocular
pressure (IOP ≥ 20) due
to inability of aqueous
humor to move through
trabecular network in
iris.
This pressure leads to
damage of the optic
nerve causing
“cupping” and
increased cup-to-disc
ratio.
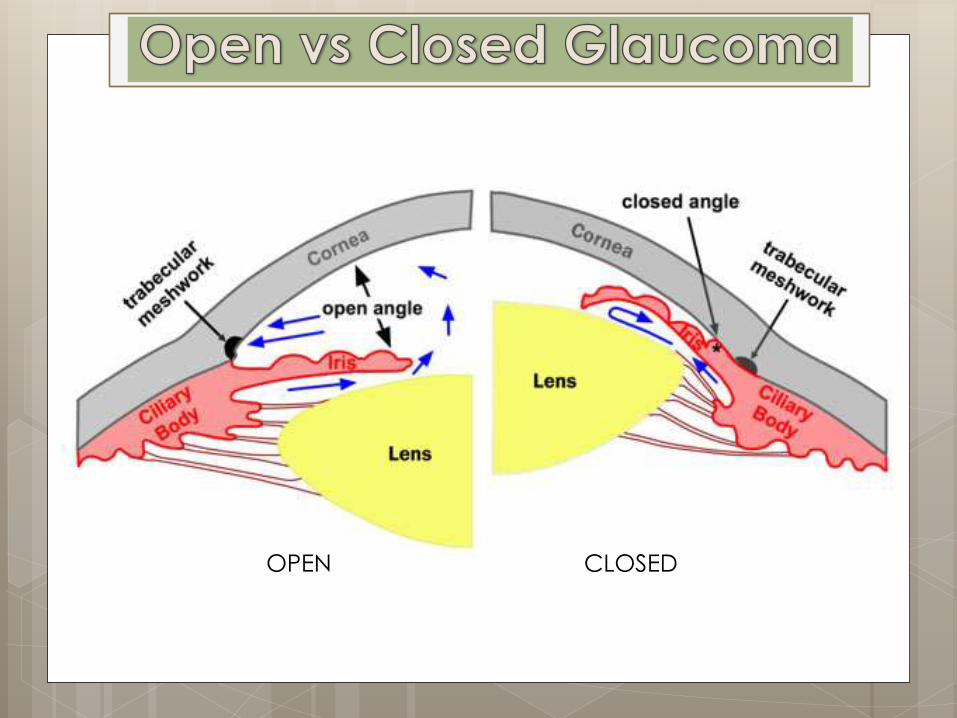
OPEN CLOSED
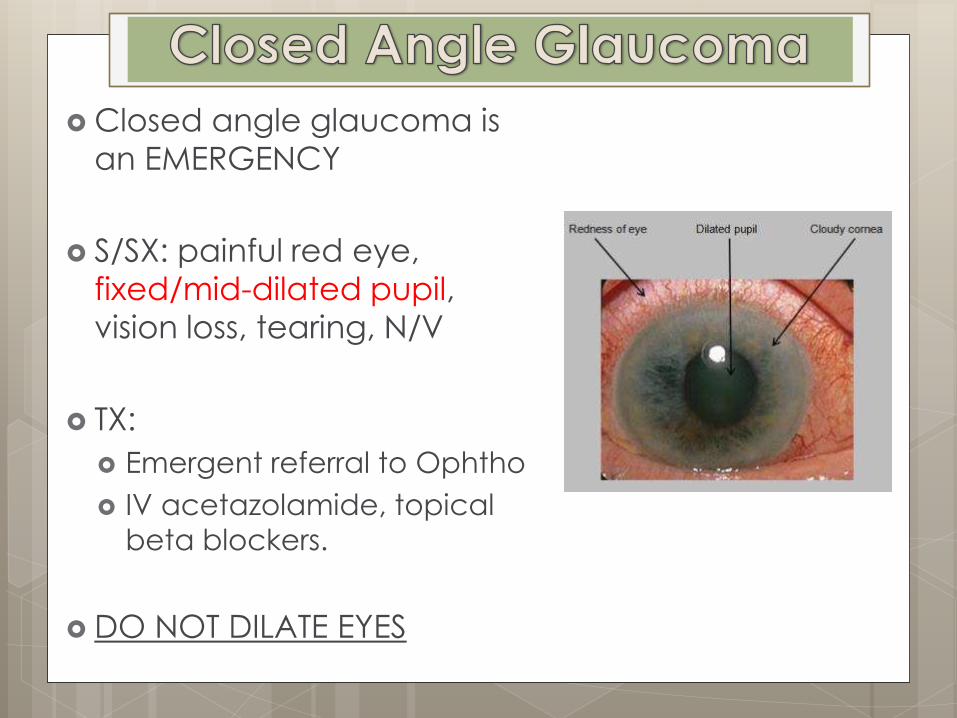
Closed angle glaucoma is
an EMERGENCY
S/SX: painful red eye,
fixed/mid-dilated pupil,
vision loss, tearing, N/V
TX:
Emergent referral to Ophtho
IV acetazolamide, topical
beta blockers.
DO NOT DILATE EYES
Open angle glaucoma is chronic compared to
closed
SX: can cause gradual loss of vision progressing to
blindness. Usually asymptomatic at first. First SX is loss
of peripheral vision.
TX - topical drops including:
Prostaglandins (first line)
Beta blockers (timolol)
Alpha agonists (brimonidine)
Carbonic anhydrase inhibitors