option b + pmtct strategy in malawi
DESCRIPTION
Loss to follow-up among women in Option B+ PMTCT programme in Lilongwe, Malawi: Understanding outcomes and reasons . Hannock Tweya , Salem Gugsa, Mina Hosseinipour, Colin Speight, Wingston Ng’ambi, Mphatso Bokosi, Janet Chikonda, Annie Chauma, Veena Sampathkumar, Tiwonge Mtande, Sam Phiri. - PowerPoint PPT PresentationTRANSCRIPT
Loss to follow-up among women in Option B+ PMTCT
programme in Lilongwe, Malawi:
Understanding outcomes and reasons
Hannock Tweya, Salem Gugsa, Mina Hosseinipour, Colin Speight, Wingston Ng’ambi, Mphatso Bokosi, Janet Chikonda, Annie Chauma,
Veena Sampathkumar, Tiwonge Mtande, Sam Phiri

Option B+ PMTCT strategy in Malawi• Use of antiretroviral therapy in HIV-infected women
significantly reduces vertical transmission; from 25% to 2%
• In 2011, Malawi embarked on a novel PMTCT programme known as “Option B+”– Lifelong ART for pregnant and breastfeeding women
regardless of WHO clinical stage or CD4 count– NVP syrup for 6 weeks for infants
• Option B+ resulted in a 7-fold increase in the number of women starting ART for PMTCT between the 2nd quarter of 2011 and 3rd quarter 2012
Loss to follow-up in Option B+ PMTCT• Loss to follow-up (LTFU) from care is a considerable
barrier to the effectiveness of PMTCT– 27% are LTFU at 12 month nationally (Malawi HIV Report Dec
2013)
– 24% are LTFU in the first 6 months in facilities with high patient volume (Tenthani et al AIDS 2013)
• Information on LTFU in women starting lifelong ART for PMTCT remains limited

Objectives• To determine factors associated with LTFU among
women starting lifelong ART for PMTCT
• To determine true outcomes of women who are lost to follow-up from PMTCT care
• To describe reasons for LTFU from Option B+ PMTCT programme
Methods: Study design & Setting• We conducted a retrospective cohort study using data from
– A real-time, touch screen-based, electronic Medical Records (EMR)
– A patient tracing programme
• Bwaila Hospital, Lilongwe– Has the busiest ANC and Maternity wings with over 14,000
ANC registrations annually– Provision of PMTCT services is a collaborative effort, led by
the Lilongwe District Health Office and other partners– Starts ~110 women on ART monthly based on Option B+
criteria
Methods: PMTCT services• All pregnant women with unknown HIV status undergo
– A group HIV counselling session– ‘Opt-out’ provider-initiated HIV testing
• “Expert mothers” provide psychosocial and adherence support to HIV-infected women on initial and follow-up visits
• All HIV-infected women are registered in the EMR System and started on a lifelong ART on the day of HIV diagnosis
• At each visit, number of remaining ARV pills and new supply are recorded and next appointment is electronically calculated
Methods: Tracing programme• The patient tracing programme intends to decrease
treatment interruption and prevent LTFU
• Tracing staff generate a list of women that miss an appointment by at least three weeks
• The staff confirms the list by checking in patients files• Women who consent are traced up to three times by
phone call or home visit• The staff complete standard paper forms on tracing
efforts, outcomes and reasons for missing appointment
Methods: Analysis• Tracing outcomes include:
– Dead, uninterrupted therapy, treatment interruptions, self transfer out, stopped ART, never started ART and not traced
• For the purpose of the tracing programme, LTFU was defined as missing a scheduled clinic appointment for at least 3 weeks.
• Multivariable Poisson regression was used investigate factors associated with LTFU
Results: Patients details & LTFU• Between September 2011 and September 2013, 2930 HIV-
infected women started ART for PMTCT Option B+: – 2,458 (84%) were pregnant
• Median age at ART initiation was 26 years (IQR 22-30)• Median follow-up of 8.2 months (IQR 3.1-16.7)• Of 2,930 women, 577 (20%) missed a scheduled clinic
appointment for at least 3 weeks– 272 only collected ARV’s at the time of initiation and did not
return• Overall incidence of LTFU was 23.5 % per year• In terms of retention: 85% at 3 months, 82% at 6 months
79% at 12 months
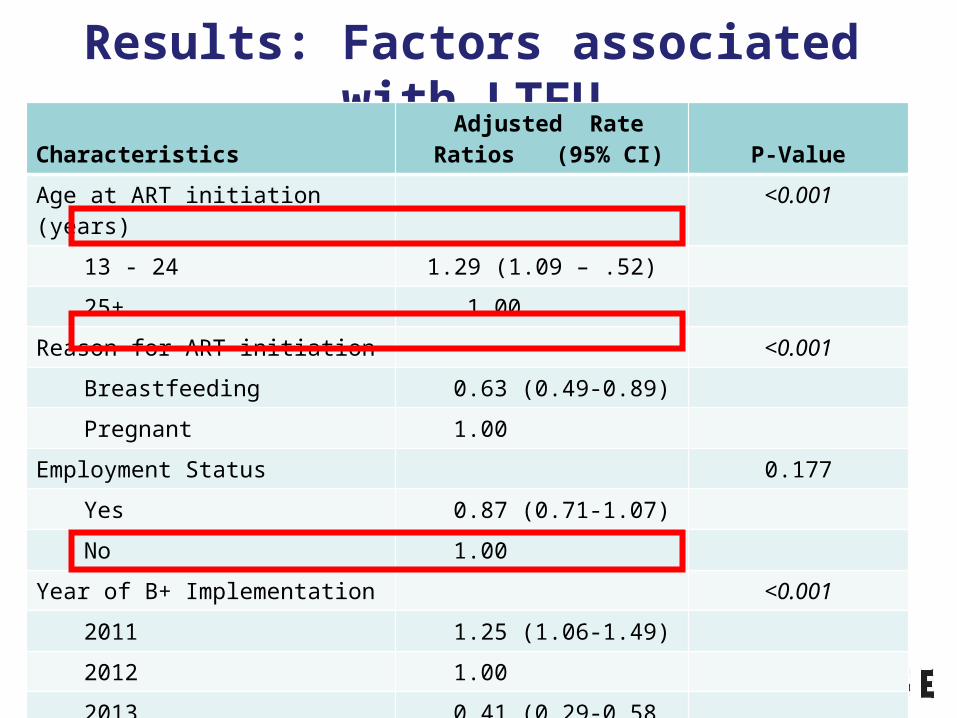
Results: Factors associated with LTFU Characteristics
Adjusted Rate Ratios (95% CI) P-Value
Age at ART initiation (years) <0.00113 - 24 1.29 (1.09 – .52)
25+ 1.00Reason for ART initiation <0.001
Breastfeeding 0.63 (0.49-0.89)
Pregnant 1.00Employment Status 0.177
Yes 0.87 (0.71-1.07)
No 1.00
Year of B+ Implementation <0.0012011 1.25 (1.06-1.49)
2012 1.00
2013 0.41 (0.29-0.58
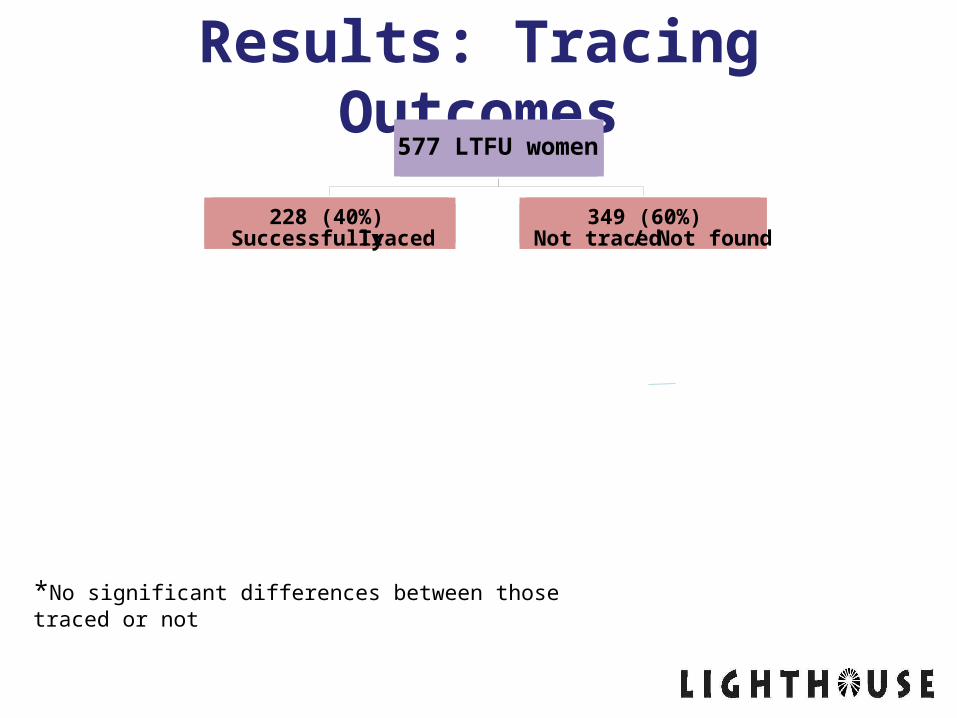
Results: Tracing Outcomes 577 LTFU women
228 (40%) Successfully Traced
349 (60%) Not traced / Not found
*No significant differences between those traced or not

Results: Tracing Outcomes 577 LTFU women
228 (40%) Successfully Traced
349 (60%) Not traced / Not found
67 (30%) Self Transfer
152 (66%) Alive not TO
9 (4%)Died

Results: Tracing Outcomes 577 LTFU women
228 (40%) Successfully Traced
349 (60%) Not traced / Not found
9 (4%) Died
67 (30%) Self Transfer
152 (66%) Alive not TO
9 (6%) ART interruption
7 (5%) Not started ART
5 (3%) Refused interview
Stopped ART118 (77%)
On ART Uninterrupted13 (9%)
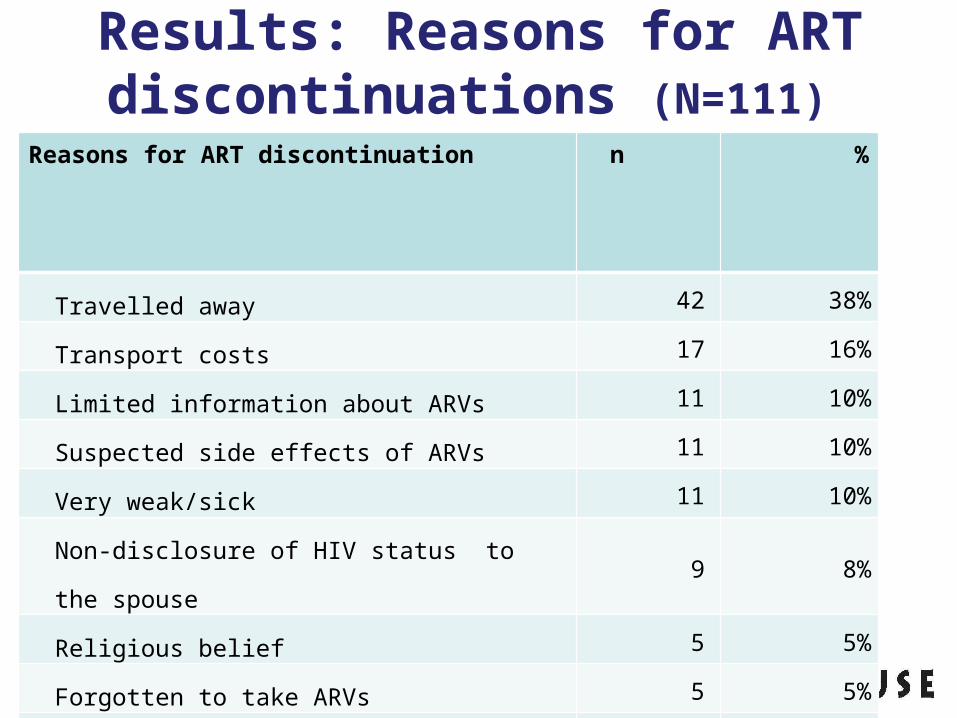
Results: Reasons for ART discontinuations (N=111)
Reasons for ART discontinuation n
%
Travelled away 42 38%
Transport costs 17 16%
Limited information about ARVs 11 10%
Suspected side effects of ARVs 11 10%
Very weak/sick 11 10%
Non-disclosure of HIV status to the spouse 9 8%
Religious belief 5 5%
Forgotten to take ARVs 5 5%
Other reasons 49 44%

Discussion • Overall LTFU was 23.5% per year
– Higher than that reported in the general HIV-infected individuals accessing ART for personal health ( 9.3% per year)
• 47% of women who were lost to follow-up received ARVs once and never returned for their appointment– May suggest that a proportion of these women never started
ART
• Being older ( 25+ years) associated with reduced risk of LTFU– May have settled lifestyles which allow them to better manage ARVs
• Likelihood of LTFU decreased with increasing year of programme implementation between 2011 and 2013 Likely due to the stabilization of the programme
Discussion • A sizeable proportion of women could not be traced due
to incorrect addresses documented in the patient clinic files. – False physical addresses because of fear of stigma and
discrimination
• Among LTFU women that were traced:– Half had stopped ART, leaving their infants at high risk of
HIV– A third self-transferred to another clinic, suggesting
underestimation of national retention in PMTCT programme

Recommendations• ANC/ART clinics should further enhance post-test
counseling by engaging HIV testing counselors and expert mothers for ongoing counseling and psychosocial support.
• Establishing targeted programmes for young women
• ART clinics need to establish data linkages through which information of patients that transfer can be shared.
• Further decentralization of PMTCT services with good ANC/Maternity services

AcknowledgmentsMother2Mother
Baobab Health Trust