oral anticoagulation operational guidance for general ... · • set up register of patients on...
TRANSCRIPT

Approved by:
On:
Review Date:
Directorate responsible for Review:
Policy Number:
Signature:
NHS LCR CHS Clinical Quality and Governance Committee
14th June 2010 23 August 2010
Quality
14th June 2011
NP109
.....................................................Liz Rowbotham Director of Quality
Oral Anticoagulation Operational Guidance for General Practice in Leicestershire County & Rutland

Equality Impact Assessment –Policy/ Service Screening Checklist
Policy Title: Oral Operational Guidance for General Practice in Leicestershire County & Rutland
Directorate: Quality
Name of person/s auditing / authoring policy: Mike Passfield
Policy/ Service Content:
• For each of the following checks is this policy sensitive to people of different age, ethnicity, gender, disability, religion or belief, sexual orientation & transgender?
• The checklists below will help you to see any strength and / or highlight improvements required to ensure that the policy / procedure is compliant with equality legislation.
1. Check for DIRECT or INDIRECT discrimination against any minority group of SERVICE USERS:
Response Action required
Resource implication
Question: Does your policy/service contain any issues which may adversely impact people from using the services who otherwise meet the criteria under the grounds of: Yes No Yes No Yes No
1.0 Age X
1.1 Gender (Male, Female and Transsexual) X
1.2 Learning Difficulties / Disability or Cognitive Impairment X
1.3 Mental Health Need X
1.4 Sensory Impairment X
1.5 Physical Disability X
1.6 Race or Ethnicity X
1.7 Religion or Belief (including other belief) X
1.8 Sexual Orientation X
If yes is answered to any of the above items the policy may be considered discriminatory and requires review and further work to ensure compliance with legislation.
2. Check for DIRECT or INDIRECT discrimination against any minority group relating to EMPLOYEES:
Response Action required
Resource implication
Question: Does your policy/ service contain any issues which may adversely impact employees from operating the under the grounds of: Yes No Yes No Yes No
1.9 Age X
2.0 Gender (Male, Female and Transsexual) X
2.1 Learning Difficulties / Disability or Cognitive Impairment X
2.2 Mental Health Need X
2.3 Sensory Impairment X
2.4 Physical Disability X
2.5 Race or Ethnicity X
2.6 Religion or Belief (including other belief) X

2.7 Sexual Orientation X
If yes is answered to any of the above items the policy may be considered discriminatory and requires review and further work to ensure compliance with legislation.
TOTAL NUMBER OF ITEMS ANSWERED ‘YES’ INDICATING DIRECT or INDIRECT DISCRIMINATION =
Number of ‘Yes’ answers for Service users (A) 0
Number of ‘Yes’ answers for Employees. (B) 0
Yes/ No Comments /
Is there any evidence that some groups are affected differently?
No
Is there a need for external or user consultation?
No
If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
No
Is the impact of the policy/guidance likely to be negative?
No
If so can the impact be avoided? N/A
What alternatives are there to achieving the policy/guidance without the impact?
N/A
Can we reduce the impact by taking different action?
N/A
IMPACT (Please Tick)
High Medium Low x
To be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval.
If you have answered “Yes” to any of the above questions, it is likely the policy/ service will need a full assessment. Please complete the full EIA template. If you have identified a potential discriminatory impact of this procedural document, please refer it to policy/service administrator; together with any suggestions as to the action required to avoid/reduce adverse impact.

CONTENTS
SECTION NUMBER
SECTION DESCRIPTION PAGE NUMBER
Introduction • Aim, Objectives, Exceptions
1
1. Setting up in the Practice • Set up register of patients on Warfarin • Using a Patient Specific Direction (PSD) • Establishing a Standard Operating Procedure (SOP) for
INR
2 2 4
2. GP Accepting Stable INR Warfarin Patients from UHL and Community Hospitals
• Process • Flowcharts
5 12
3 Housebound Patients • Pathway for monitoring stable patients • Unstable patients
16 16
4. GP Concern Regarding Patient Stability • 3 step process to access nurse led clinic for advice
19
5. Adjusting Warfarin Dose in General Practice • Dosing • Advice to Patients having Dental Treatment • Pre-Operative Management of Warfarin • Discontinuing Warfarin
19 21 21 21
6. New Patient in General Practice Requiring Warfarin • Warfarin Initiation schedule & prescription chart for slow
initiation treatment
21
7. Practice Clinic Processes • Patient 1st Appointment • Patient follow up
26 27

APPENDICES
1 Staff Competency. Assessment Criteria
28
2 Near Patient Testing and Maintenance of Oral Anti-coagulation Therapy in Primary Care – Standards and Criteria (NPSA Standards)
37
3 Quality Control and Assurance
39
4 Outline of areas to be covered by the SOP
42
5 Side Effects of Warfarin
46
6 Factors That Affect Anti-coagulation Control
48
7 Audit. Minimum Standards NPSA
53
8 Critical Incident / Significant Event Analysis
54
9 Procedure for Obtaining Supplies of Testing Strips and Control Solution
56
10 CoaguCheck Machine – Internal Quality Control Log Sheet
57
11 External Quality Control Check
58
12 External Check: NEQAS: • General Information • NEQAS Registration Form
61
13 UHL Patient Induction Pack 62

NP109 Anticoagulation Operation Policy Page 1 of 70 Status – final, version 1 Approval date; June 2010 Review date; June 2011
ANTICOAGULATION MONITORING
OPERATIONAL GUIDANCE FOR GENERAL PRACTICES AIM To offer therapeutic anticoagulation management to practice patients receiving anticoagulation therapy by means of Near Patient Testing (NPT) and Computer Decision Support.
• To provide best practice • Improved patient safety • Optimise anticoagulant control • Reduce number of INR tests required to maintain good control • Reduce potential for errors in dosing • Improve patient convenience • Improve efficiency in the use of medical time and resources
OBJECTIVES Decrease the risk of thromboembolic events or extension of an existing event by monitoring patients at the optimal level of anticoagulation therapy without producing an unacceptable risk of haemorrhage. Enable optimum care to the patient in terms of accessibility, number of blood tests, waiting times for results, appropriate dosage advice, clear written information and continuity of care. All patients on anticoagulation therapy will be identified on EMIS or other clinical system. Patients will be on anticoagulation therapy only when the clinical benefits outweigh the risks. Safe transfer of information between UHL and practice, within the practice, and between practice and patient is paramount. EXCEPTIONS Patients under 18 yrs Patients with complex pathologies Patients with warfarin intolerance High-risk patients referred back to secondary care after discussion with haematologist This list is not exhaustive and individual cases may be considered by GP for exclusion depending on clinical circumstances

NP109 Anticoagulation Operation Policy Page 2 of 70 Status – final, version 1 Approval date; June 2010 Review date; June 2011
1. SETTING UP IN THE PRACTICE A) Setting up a register of patients who are taking Anticoagulants If the practice has been coding patients on Anticoagulants on EMIS or other clinical system, then they should already have a register. However this should be double checked by performing a drug search of anticoagulation prescriptions. Remember to search for other anticoagulants too such as phenindione (‘Dindevan’) and acenocoumarol (‘Sinthrome’). This list of patients can then be transferred on to INR STAR or other approved CDSS, patient by patient, with full details including indication for anticoagulation therapy, when started and duration of treatment, INR range, minimum last 3 INRs, contraindications, and side effects. This will be laborious but important to set up a good patient base. See separate protocol for INR STAR use. Unfortunately, as INR STAR does not communicate with EMIS/other clinical system, as well as using INR STAR, consider setting up an EMIS/other clinical system code and template. This will keep patient records updated, allow EMIS or other clinical system to provide alerts for contraindicated medication, and provide a back up. B) Using a Patient Specific Direction (PSD) If the practice nurse is going to run the clinic, a PSD has to be set up for each patient. This will support the registered nurse to be able to adjust the warfarin dose. Otherwise the alterations will need to be done by a GP or nurse prescriber.
The Use of a PSD within General Practice (See overleaf for Example PSD) • The PSD must be given to the patient and kept in the patient’s yellow book or
attached to a suitable alternative as long as it contains the relevant information. • A copy of the PSD should be scanned into the patients electronic notes • The PSD needs to be approved and formally agreed by each GP practice. • Each practice must also have a Standard Operating Procedure (SOP) which outlines
roles and responsibilities for INR testing

NP109 Anticoagulation Operation Policy Page 3 of 70 Status – final, version 1 Approval date; June 2010 Review date; June 2011
ORAL ANTICOAGULATION PATIENT SPECIFIC DIRECTION
PATIENT DEMOGRAPHICS Surname
Forename Title
Address
Postcode
Date of Birth
NHS Number
System Number
CLINICAL DETAILS Clinical Indication for Treatment
INR Target
INR Range
Duration of Treatment
Treatment commenced by
Treatment Commenced On
PRESCRIBER DETAILS Surname
Forename Title
Signature
Designation
Date
Aim to keep INR within the above range as guided by INR STAR. Any changes to patient circumstances e.g. drugs, health or alcohol should be highlighted to GP / prescriber. Any INR 5 or above should be highlighted to the GP / Prescriber. Any DNA should be highlighted to the GP / Prescriber

NP109 Anticoagulation Operation Policy Page 4 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
PLEASE REMEMBER • GP’s or Independent/Supplementary Prescribers with specific extended training can
prescribe and carry out dosage adjustments • Registered Nurses are able to carry out dosage adjustment where a Patient Specific
Direction (PSD) exists. • A HCA can undertake testing but cannot make a dosing decision. • All staff must have undertaken appropriate training and be competent in their role.
Nurses must adhere to the guidance issued by the Nursing and Midwifery Council. (Standards for Medicines Management 2008) that recommends that duties such as "patient dosing" should only be undertaken by a Registered Nurse. C) Establishing a Standard Operating Procedure (SOP) in the Practice for INR The PSD needs to be supported by a Standard Operating Procedure. It is not possible to produce a standardised practice template, as each practice will have its own way of delivering the INR service within the Operational Guidance. This needs to be specific for each practice to detail how the service will be run. See appendix 4 for an outline of the areas that need to be covered by the practice's own Standard Operating Procedure (SOP).

NP109 Anticoagulation Operation Policy Page 5 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
2. ACCEPTING ANTICOAGULATED PATIENTS FROM SECONDARY CARE The GP should ensure that the patient has a Yellow Book or suitable alternative (such as a print out) as long as it contains the relevant information. Working Definition of Stability Stability is a difficult area to define but for practical purposes the following is provided:
• Two consecutive INRs in range with the third INR not due for a minimum of one week
• Monitoring reduced to weekly INR checks Any new patients initiated on anticoagulation therapy by UHL or patients already on anticoagulation therapy who are discharged following an inpatient episode, MUST have the following information sent to the practice as a minimum:
Acceptance process The UHL Central Administrator from the Anti-coagulation Team will contact the practice and fax a) Fax Cover Letter b) Acceptance Request Form c) Anticoagulation Information Chart (from clinical system) The GP will indicate on an acceptance form whether the patient will be accepted by the practice, sign the letter and fax the letter back. The fax number to use is 0116 258 7561. Acceptance forms must be returned within 12 hours of receipt. Only when the acceptance form has been faxed back agreeing the transfer of anticoagulation monitoring to the GP, will the patient not be followed up further by the hospital clinic. If the patient is accepted, the practice will transfer the information from the printout to INR STAR and EMIS/other clinical system template in preparation of the patient attending the surgery clinic. The GP surgery will be responsible for informing the patient that they have been accepted by the practice for further monitoring, and arrange their appointment for next INR at the surgery. The hospital gives out patient information on discharge but sending a PIL with the GP letter can reinforce this.
• Clinical indication • When treatment started • Dose • INR range and duration of
treatment
• Last 3 INRs minimum • Next due INR date • Allergies, side effects, contraindications etc • Indication verbal/written pt info given

NP109 Anticoagulation Operation Policy Page 6 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
The PCT has provided a protected GP practice fax number to the UHL Anticoagulation clinic and details of the clinical lead for the practice. If for any reason these details are changed please inform the clinic as soon as possible.
UHL ANTI-COAGULATION TEAM CONTACTS
Central Admin contact number - 0116 2585069
Central Admin Fax Number - 0116 2587561

NP109 Anticoagulation Operation Policy Page 7 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
DISCHARGE FROM SECONDARY TO PRIMARY CARE
GP ACCEPTANCE FORM
LAST 2 CONSECUTIVE INRs IN RANGE AND NEXT NOT DUE FOR 1 WEEK YES/ NO NEXT INR DUE DATE: PATIENT INFORMATION AND YELLOW BOOK ISSUED TO PATIENT YES/ NO ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ This application for anticoagulation monitoring at the Surgery is ACCEPTED
This application for anticoagulation monitoring at the surgery is declined. GP to liaise with hospital please
REASON
Signed…………………………..………………………………..Date: ………………………..………... (PRACTICE GP PARTNER to sign) Surgery administration staff to pass form to the GP for a decision and fax back to hospital the SAME day please GP Surgery only 1. Form faxed back to hospital 0116 258 7561
2. Patient contacted and appointment booked
3. Patient details coded in EMIS/other clinical system and on INR Star
4. Entries double checked by GP
DATE: PATIENT NAME: DOB: ADDRESS:
TEL NO: NHS NUMBER:
CLINIC/ WARD/ HOSPITAL PRACTICE GP NAME & ADDRESS:

NP109 Anticoagulation Operation Policy Page 8 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
UHL COVERING LETTER TO BE SENT TO PRACTICES REQUESTING DISCHARGE -example
Directorate of Cancer and Haematology Integrated Anticoagulation Service Direct Dial: 0116 258 5069 Fax: 0116 258 7561 Date: Dear Re: Patient Name DOB: NHS No: Your patient has been discharged from a UHL ward. The UHL anticoagulation team have been informed of the discharge as the patient is on warfarin. We are faxing you this letter and the warfarin prescription chart for you to review, take a clinical judgement and to make the necessary arrangements for further monitoring. To ensure the smooth transfer of the patient please can you confirm receipt of this fax by completing the acceptance request form within the next 12 hours and let us know whether you will be arranging for the follow up of the patient or if you wish the patient to be seen within UHL for their warfarin monitoring. If you wish UHL to see the patient please indicate the reason for this. Kind regards Stuart Brown Clinical Nurse Specialist Manager

NP109 Anticoagulation Operation Policy Page 9 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
The information contained in this transmission is privileged and confidential. It is intended for the exclusive use of the addressee printed above. If you are not the addressee, any disclosure, reproduction or other dissemination or any other use of this transmission is strictly prohibited. If this transmission has been sent to you in error, please contact us on the above telephone number in order that we can arrange for its safe return.

NP109 Anticoagulation Operation Policy Page 10 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
EXAMPLE OF SURGERY ACCEPTANCE LETTER TO PATIENT

NP109 Anticoagulation Operation Policy Page 11 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
PRIVATE & CONFIDENTIAL Date Dear Re: INR Near-Patient Testing Service (WARFARIN) We are pleased to advise you that you have been accepted to have any further warfarin monitoring blood tests done here at the surgery. The hospital clinic you previously attended has sent us your details and previous results. Tests are carried out using a near patient testing machine, much like the hospital clinics. Your appointment at the surgery has been made for:- DATE: TIME: Warfarin belongs to the group of medicines known as anticoagulants, It is used to prevent and treat the formation of harmful blood clots within the body. Warfarin works by thinning the blood. If you notice any unusual bruising, bleeding, blood in the urine, blackened stools or jaundice (yellowing of the skin and whites of the eyes) contact your doctor or the anticoagulant clinic immediately. Please ensure you bring your yellow anticoagulation book with you to the appointment. Yours Sincerely

NP109 Anticoagulation Operation Policy Page 12 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
SUMMARY OF ENSURING SAFE PATIENT TRANSFER FROM ACUTE AND COMMUNITY HOSPITAL WARDS A. FROM UNIVERSITY HOSPITALS OF LEICESTER FOR COUNTY PRACTICES
Patient ready for discharge from Ward
Warfarin initiation chart/prescription chart to UHL Anticoagulation Administrator
Central Administrator identifies as County patient
Central Admin Contact Telephone number: 0116 258 5069 Central Admin Fax Number ‐ 0116 258 7561
Administrator checks what the GP will accept against the GP list e.g. new
initiations/unstable/stable patients
Chart, covering letter and acceptance form faxed to GP
GP informs patient of their surgery appt
Accepts
Newly initiated or unstable patients
Stable patients
GP faxes back acceptance form Fax: 0116 258 7561
Patient given appointment within UHL Anti‐Coagulation clinic
Declines
Chart, covering letter and acceptance form
faxed to GP
GP faxes back acceptanceFax: 0116 258 7561
Accepts
GP informs patient of their surgery appt
Practice that do not accept unstable
Practice that do accept unstable
Declines
Ref patient to UHL Anticoagulation and complete incident
form

NP109 Anticoagulation Operation Policy Page 13 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
B. FROM COMMUNITY HOSPITALS FOR COUNTY PRACTICES
PROVIDER SERVICES DIRECTORATE
MANAGEMENT OF PATIENT ON WARFARIN THERAPY IN COMMUNITY HOSPITALS
Transfer of care into Community Hospital/Direct admission
Ensure INR monitoring not required more frequently than every 3 days
Patient on warfarin therapy admitted into the community hospital
Patient newly prescribed warfarin as part of their treatment whilst in
Community Hospital
If transfer from Out of County Hospital, Nursing /Residential
home, Home etc Place on CHS Warfarin Chart
Complete ALL sections
Ensure doctor agrees and signs completed chart
Transfer from UHL
GP to transcribe onto CHS Warfarin Chart
Commence on new Warfarin Chart
Complete ALL sections. Ensure doctor agrees and signs the
completed chart
Fit for discharge

NP109 Anticoagulation Operation Policy Page 14 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
EXAMPLE OF COMMUNITY HOSPITAL LETTER ON DISCHARGE
Warfarin Discharge from a Community Hospital to Primary Care
In order to ensure the safe transition of patients on warfarin to primary care it is necessary to complete this referral form. The patient must be stabilised and the form completed and faxed to the GP on the day of discharge (Monday – Friday) from hospital. It is the responsibility of the secondary care team to provide anticoagulation care until the surgery has faxed back confirmation that the patient has been accepted. Forms not filled in fully and correctly will be returned to the secondary care team, and application rejected for near patient testing. Consultant: Patient’s Name: Hospital:
Patient’s Address: Patient’s NHS number:
Hospital Fax Number: Patient’s Telephone Number: Hospital Contact Telephone Number: Patient’s DOB:
Clinical Details: Tick Condition Hospital
Suggestion target INR
Duration treatment
Arterial disease, MI Arterial grafts Atrial fibrillation DVT prophylaxis (high risk) DVT prophylaxis (low risk) DVT, PE recurrent DVT, PE treatment Hypercoaguability states Left Ventricular aneurysm Mural thrombus Prosthetic valves Transient ischaemic episode Other (please state)
Last 3 INR Results Including Loading Dose if Relevant: Date INR Warfarin Dose Next INR check date: Dose of warfarin tablet(s) usually issued: Name of person completing the form: Signed: Date: Position held:

NP109 Anticoagulation Operation Policy Page 15 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
C. FOR CITY PRACTICES
Patient identified as ready for discharge
from Ward
Ward to fax warfarin initiation chart/prescription chart to UHL Anticoagulation Patient can then be discharged without delay:
Administrator identifies as City patient
Patient given an appointment within the UHL clinic (new initiations) or in the
community clinics if an existing patient

NP109 Anticoagulation Operation Policy Page 16 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
3. PATHWAY FOR HOUSEBOUND PATIENTS ON WARFARIN (TO BE SAMPLED BY THE DISTRICT NURSING SERVICE) Housebound patients on warfarin who are stable GP will encourage patients who do go out on trips, hairdressers etc to visit the surgery for their warfarin monitoring. A clinical risk assessment will further clarify which patients should continue with their warfarin monitoring. For those that do require home monitoring, GPs will refer to the district nurses for NPT. The GP retains the role of dosing the patient and informing them of this, and arranging further follow up.
`
Housebound patients who are unstable on warfarin Unstable housebound patients remain under the responsibility if the anticoagulation team, who will arrange ambulance transport to take them to hospital for each INR check. In these circumstances, some GPs may feel that they can offer the above district nurse service and carry out dosing.
GP practice doses patient as per guidance and returns yellow book to patient
Completed DN referral form requesting INR with due date and pt telephone number together with
summary/ INR Star printout
GP identifies patient who requiresanticoagulation monitoring and who is housebound
DN carries out NPT and brings result and yellow book back to surgery
DN advises patient that GP will return yellow book and inform them of their new dose and
follow up
GP re‐refers to DN with new due date for INR and summary printout

NP109 Anticoagulation Operation Policy Page 17 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
4. GP CONCERN REGARDING PATIENT STABILITY If you need advice about a patient, UHL have provided a 3 step plan for how to access further help

NP109 Anticoagulation Operation Policy Page 18 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
FIRST CHECKConcern regarding patient stability:
Check for recent changes in patient’s medication, diet or health Confirm compliance with warfarin regime
SECOND CHECKPatient remains unstable:
Call 0116 258 5069 and speak to anticoagulation specialist nurse for further advice on management
This must be a clinician to clinician discussion
THIRD CHECKIf patient remains unstable:
Referral letter to be sent to the anticoagulation nurse led clinic. The patient will be stabilised at UHL
LRI Anticoagulation Clinic Knighton Street Outpatient Offices
Leicester LE1 5WW
DISCHARGE BACK TO GPOnce patient is stabilised as per UHL/LCRPCT Joint Protocol a fax will be sent to GP Practices
requesting GP to accept patient back
Process for GPs to access UHL for advice

NP109 Anticoagulation Operation Policy Page 19 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
5. ADJUSTING WARFARIN DOSE IN GENERAL PRACTICE Therapeutic recommended uses and International Normalised Ratios (INRs) for those uses (British Society of Haematology) Pulmonary embolus 2.0 ‐ 3.0 Venous Thrombosis (DVT) 2.0 ‐ 3.0 Prophylaxis of postoperative deep vein thrombosis (general surgery) 2.0 ‐ 2.5 Prophylaxis of postoperative deep vein thrombosis in hip surgery and fractures 2.0 – 3.0 Myocardial infarction: prevention of venous thromboembolism 2.0 – 3.0 Transient ischaemic attacks 2.0 – 3.0 Tissue heart valves 2.0 – 3.0 Atrial fibrillation * 2.0 – 3.0 Valvular heart disease 2.0 – 3.0 Recurrent deep vein thrombosis and pulmonary embolism 3.0 – 4.5 Arterial disease including myocardial infarction 3.0 – 4.5 Mechanical prosthetic valves (see table 2) Recurrent systemic embolism 3.0 – 4.5 Intravascular stent 2.5 – 3.5 Table 2 Recommended INR for prosthetic valves Sinus rhythm normal left atrial size (i.e.
most aortic valve replacement patients) Atrial fibrillation enlarged left atrium (i.e. most mitral valve replacement patients)
Low thrombogenicity prosthesis 2.0 – 3.0 2.5 – 3.5 Other prostheses 3.5 – 4.5 3.5 – 4.5
Dosage Regimens The average dose of warfarin required daily is around 5 mg (range 1-9mg) but may vary markedly because of several factors. Warfarin should be given once daily (5-6pm is an ideal time) and is given as a tablet for oral administration. (Tablet strengths are 0.5mg (white),1 mg (brown), 3 mg (blue), 5 mg (pink).) Dosage should always be described in terms of milligrams not numbers of tablets and aim for NO daily dose fluctuations * The British Society of Haematology recommendations for oral anticoagulation for patients with non-rheumatic AF are:
• Patients with no risk factors under the age of 65years should receive 300mg aspirin daily • Patients with risk factors should receive warfarin to achieve a target INR 2.5 • Patients over 65years with additional risk factors should receive warfarin if there are no
serious risk factors The PCT recommendations for oral anticoagulation for patients are:
• 1mg tablets should be prescribed until patients are fully stabilised and familiar with their anticoagulant medication
• As a general rule, patient over the age of 60 shoul dbe prescribed 1mg tablets only, all other strengths including 0.5mg tablets should be used in patients who demonstrate a good understanding of the use of their anticoagulant

NP109 Anticoagulation Operation Policy Page 20 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
ADJUSTING WARFARIN DOSAGE Evidence shows that anticoagulant dosing software helps maintain the INR levels within the therapeutic range, extends the time between INR tests and effectively manages anticoagulant records facilitating audit, and is therefore recommended as first choice when adjusting warfarin doses.
• Aim to achieve the target INR, but keeping within the therapeutic range is acceptable.
• •Any change in warfarin dosage should be checked after one week If INR has been stable for some time; one result outside the therapeutic range (such as 0.5 above or below) may not be enough to require adjustment but check again after one week.
• Try to use constant day dosing and avoid alternate day dosing to aid patient compliance • Try to avoid the use of half tablets. Patients find it difficult to break tablets. 0.5mg warfarin
tablets can be prescribed instead • For maintenance, use the least number of tablets each day • Dose to be expressed in mg NOT number of tablets
If INR is within range • Review in four weeks; can extend to 6-8 weeks if patient has been stable for three
consecutive weeks. If INR is too low
• Ensure compliance - Exclude a change in medication such as phenytoin or factors, which may antagonise Warfarin.
• If INR is at the lower end of range and has been falling, increase dose adjustments in steps of 0.5mg
If INR is too high / haemorrhage
The main adverse effect of all oral anticoagulants is haemorrhage. Checking the INR and omitting doses when appropriate is essential. The following recommendations of the British Society for Haematology apply to patients taking Warfarin.
BSH Guidelines for INR 5.0+ >3.0 and <6.0 Target 2.5 Reduce or stop warfarin restart when INR <5.0
>4.0 and <6.0 Target 3.5 Reduce or stop warfarin restart when INR <5.0
>6.0 and <8.0 No bleeding or minor bleeding stop warfarin, restart when INR <5.0 INR 8.0 No bleeding or minor bleeding Consider admission to hospital for
Vitamin K 0.5mg or to see GP for intravenous vitamin K 0.5mg or oral vitamin K 0.5mg – 2.5mg
Major bleeding Stop warfarin; Admission to hospital for fresh frozen plasma and/or vitamin K
Please refer to BNF for vitamin K recommendations

NP109 Anticoagulation Operation Policy Page 21 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
ADVICE TO PATIENT HAVING DENTAL TREATMENT www.npsa.nhs.uk/health/alerts Leaflet available in a range of languages Patients are advised to continue with warfarin therapy when attending for dental treatment. However they will need to check their INR the day before the appointment to ensure INR is below 3.0 PRE-OPERATIVE MANAGEMENT OF WARFARIN In general:
• For major surgery, stop warfarin 3 days before surgery and introduce heparin pre – op in hospital
• For minor surgery, reduce INR to approx 2.0 on day of surgery In ALL cases liaise with hospital for advice, and this may involve discussion with surgeon and clinician e.g. cardiologist. The Anticoagulation Service offers a Pre operative planning assessment. The dose of warfarin and latest INR on discharge MUST also be made clear and faxed through to the practice on the agreed referral form together with the minimum discharge details, as previously detailed AND entry in patients yellow booklet DISCONTINUING WARFARIN Written confirmation needs to be received from the clinician who commenced warfarin therapy. This should be crosschecked with the original referral form. There is a theoretical hypercoaguable state after stopping warfarin, but the evidence remains conflicting and inconclusive. BCSH guidelines on Oral Anticoagulation (2005) recommend as follows: Oral anticoagulant therapy can be discontinued abruptly when the duration of therapy is completed (grade B, level IIb). However in UHL the anticoagulation department choose a more cautious approach and advise gradual withdrawal of warfarin over a few days to weeks, depending on the dose. They simply ask patients to decrease the dose by 1mg/day over how many ever days their maintenance dose dictates at the time. 6. NEW PATIENT IN GENERAL PRACTICE REQUIRING WARFARIN
Some patients will be found to have a new medical condition, which requires initiation of warfarin e.g. a new diagnosis of A.F. The GP can make a decision to initiate warfarin in the surgery if within his or her clinical competence, but this falls outside the National Enhanced Service. As such, patients can be referred to the hospital anticoagulation clinic. Referral back to the practice will occur in the usual way with a faxed printout of details together with an acceptance form for the GP to fax back, when warfarin stabilised.

NP109 Anticoagulation Operation Policy Page 22 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
If a GP receives a request from another speciality requesting that the patient needs to start warfarin, but initiation falls outside the GP’s competence, please send through a copy of the consultant letter, together with a covering letter to the anticoagulation clinic requesting initiation of anticoagulation. INDICATION FOR WARFARIN USE Short term (up to 12 months) – ACUTE requirement. (HOSPITAL INITIATION) Established DVT Prophylaxis of DVT Xenograft (tissue) heart valve replacements Pulmonary embolism Coronary artery bypass graft Myocardial Infarction
Long term – PREVENTATIVE. Require slower anticoagulation, (GP INITIATION possible) Atrial Fibrillation Recurrent thromboembolism Cardiac prosthetic valve replacement Arterial grafts Embolic complications of Rheumatic heart disease Other conditions for consideration of long-term treatment Lupus-like conditions with risk of clinical thrombosis Congenital antithrombin III deficiency with risk of clinical thrombosis* Congenital protein C or S deficiencies with risk of clinical thrombosis* Transient ischaemic cerebral artery syndrome including basilar artery and vertebral artery syndromes Decisions on anticoagulation relating to these conditions will need haematology expertise
PROCESS
• Counsel patient
Ensure the benefits of anticoagulation outweigh the risks. Ensure the patient has appropriate written information about Warfarin and an INR book.
• Check baseline INR, LFTs, FBCs (baseline INR must be less than <1.3, if baseline is >1.3
patient should be screened for underlying conditions FBC, LFT, clotting screen) If the practice agrees to initiate warfarin for pts with e.g. AF, there are well-established protocols for starting warfarin quickly in hospital – but in primary care there is less of a rush, and the facilities for daily INRs often just aren’t there. The standard 10mg starting dose regimes from the British Society of haematology Guidelines 1999 recommend daily INR for at least 4 days but recent work from Glasgow suggests there is a real alternative.

NP109 Anticoagulation Operation Policy Page 23 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
For patients needing non-immediate anticoagulation to target INR of 2.0-3.0 (e.g. for AF)
• Providing baseline INR ≤ 1.3 AND patient not taking amiodarone • Give 5mg warfarin at 6pm for 4 days then check INR on morning of day 5 • Amend dose for evening of day 5 based on the result and recheck on day 8 • After day 8 test amend dose and recheck in a further 4-7 days, thereafter following
normal practice. Initiation of anticoagulants should only take place with 1mg tablets where possible. Use of other strengths had led to a number of serious incidents For elderly pt 75year + and/or
Abnormal LFTs Cardiac failure Parenteral feeding Less than average bodyweight On oral anticoagulant potentiating drugs
Give 1mg warfarin at 6pm for 4 days then check INR on morning of day 5. Issue new patients with 1mg tablets until stabilised

NP109 Anticoagulation Operation Policy Page 24 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Warfarin Induction Regime for Patients with AF INR on day 5 Dose for days 5-7 INR on day 8 Dose from day 8 < or = 1.7
5mg
< or = 1.7 1.8-2.4 2.5-3.0 >3.0
6mg x 7days 5mg x 7days 4mg x 7days 3mg x 4days
1.8-2.2
4mg
< or = 1.7 1.8-2.4 2.5-3.0 3.1-3.5 >3.5
5mg x 7days 4mg x 7days 3.5mg x 7days 3mg x 4days 2.5mg x 4days
2.3-2.7
3mg
< or = 1.7 1.8-2.4 2.5-3.0 3.1-3.5 >3.5
4mg x 7days 3.5mg x 7days 3mg x 7days 2.5mg x 4 days 2mg x 4days
2.8-3.2
2mg
< or = 1.7 1.8-2.4 2.5-3.0 3.1-3.5 >3.5
3mg x 7days 2.5 mg x 7days 2mg x 7days 1.5mg x 4days 1mg x 4days
3.3-3.7
1mg
< or = 1.7 1.8-2.4 2.5-3.0 3.1-3.5 >3.5
2mg x 7days 1.5mg x 7days 1mg x 7days 0.5mg x 4days omit x 4days
>3.7
0mg
<2.0 2.0-2.9 3.0-3.5
1.5mg x 4days 1mg x 4days 0.5mg x 4 days
This table appears in Tait RC, SefickA. A warfarin induction regimen for out-patient anticoagulation in patients with atrial fibrillation., Br Journal of Haematology 1998; 101:450-454. If uncertain, check with anticoagulant clinic as there are a wide variety of acceptable regimes although the above is the one preferred by UHL.

NP109 Anticoagulation Operation Policy Page 25 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011

NP109 Anticoagulation Operation Policy Page 26 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
7. PRACTICE CLINIC PROCESSES - EXAMPLES
Check on EMIS/other clinical system and ask patient for any changes since last INR: • Medication, diet, alcohol intake • Health • Check side effects • Check compliance • Check risks vs benefits including • Cognitive function • Concurrent condition e.g. risk of falls, • Dexterity
Enter details on EMIS and codeEnter details on INR Star Contact patient with appt
GP to complete Patient Specific Direction
Confirm patient’s knowledge on:
• Side effects • Medication etc
Provide written information and give alert card
Enter on to INR Star and give patient dosing instructions as per PSD
Print off for GP to check and sign as per PSD
Enter dosage in patient’s Yellow Book
PATIENTS 1ST APPOINTMENT WITH PRACTICECLINIC PROCESS
Patient arrives at surgery (clinic)
Check Yellow Anticoagulation Card
Any concerns should be referred to GP
Check INR as per procedure
Ensure Internal Quality Control is carried out prior to first patient, then on a weekly basis or after 50 tests, depending which is first

NP109 Anticoagulation Operation Policy Page 27 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Open EMIS / STARConfirm:
• Name • DOB • NHS Number • 1st Line of Address
Check on EMIS and ask pt for changes in:
• Alcohol intake • Diet • Medication • Health • Check compliance • Check for side effects • Check risks vs benefits
Check Patient ID with:
• Yellow Book • EMIS • STAR
Check INR as per procedure
Any concerns should be referred to G.P
Ensure Quality Control is carried out on analyser for
first patient
Enter on to INR Star and give patient dosing instructions as per PSD
Print off for GP to check and sign as per PSD
Enter dosage in patient’s Yellow Book Complete EMIS template
Follow Up Appointment made
PATIENT FOLLOW UP WITH PRACTICE. CLINIC PROCESS

NP109 Anticoagulation Operation Policy Page 28 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 1 STAFF COMPETENCY Rationale Implementation of this and related competency assessments will enable the Practice to comply with the requirements of the NPSA Risk Assessment of Anticoagulation Therapy (2006) 2 – and should be completed annually Objective On successful completion of this assessment the candidate will be deemed competent to undertake the procedure for the next 12 months. It is recommended that the Practice agree the minimum number of patients to maintain competence Knowledge and Skills Framework (KSF) Link This workforce competence is linked to the following dimensions and levels in the NHS Knowledge and Skills Framework (October 2004) 3 HWB6 Assessment and treatment planning Level 4: Assess physiological and psychological functioning when there are complex and/or undifferentiated abnormalities, diseases and disorders, and develop, monitor and review related treatment plans Suggested evidence
• System of clinical supervision where senior staff oversee and assess work competencies of less experienced staff
• Training records and competence assessment forms annually

NP109 Anticoagulation Operation Policy Page 29 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Anticoagulation Management Clinical Competencies
Name of Delegate
Designation
Date of Assessment
1) An observational assessment must be performed to assess candidate competence (please tick as appropriate)
Performance
Number
Criteria
Pass
Fail
N/a
Comments
Standard 1: The referral contains:
PSC 1
Patient Name and contact details
PSC 2
Date of Birth (D.OB) and gender
PSC 3
NHS No / Hospital No
PSC 4
Hospital No / NHS No
PSC 5
Signature of requesting person and contact details
Standard 2: There is a clear understanding and confidence in using the G.P IT system for patient Management, and evidence that patient information can be accessed and updated
PSC 6
Accesses patient management plan
Can access and update the following:
a) medication
b) diet
c) physical / mental health
PSC7
d) current warfarin therapy and duration of treatment

NP109 Anticoagulation Operation Policy Page 30 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Performance
Number
Criteria
Pass
Fail
N/a
Comments
d) Recent admissions to secondary care /
A&E
PSC8
Can demonstrate safe use of Practice IT systems used in anticoagulation management
Standard 3: There are correct safety checks in place prior Near Patient Testing procedure
PSC9 The patients identity is confirmed correctly:
a) full name
b) date of birth
c) first line of address
PSC10
The patients ‘Yellow Booklet’ confirms identify
PSC11
The patients ‘Yellow Booklet’ is correctly completed
PCS 12
Is aware of G.P practice should patient forget ‘Yellow Booklet’ or have out of date information
PCS13
Is aware of how to access additional ‘Yellow Booklets’
PCS14
Verbal consent is obtained prior to the procedure
PCS15
Consent to carer presence obtained
Patients history / side effects reviewed
a) Verbally
PCS16
b) Electronically
PCS17
If confused carer is used to confirm patients identity
Standard 4: The correct procedure is followed in Near Patient Testing
PCS18
Code Number matches test strip
PCS19
Meter switched on correctly
PCS20
Battery level, date and time checked
PCS21
Patient ID entered (if applicable)
PSC22
Test Strip correctly inserted

NP109 Anticoagulation Operation Policy Page 31 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Performance
Number
Criteria
Pass
Fail
N/a
Comments
PCS23
Waits for hourglass and ‘Bleep’
PCS24
Correctly interprets blood icon and 120 second countdown
PCS25
Patients finger correctly pricked
PCS26
Blood correctly applied to semi-circular, transparent application area within 15 seconds
PCS27
Blood touched against the side of the sample application area
PCS28
Correctly interprets INR result
PCS29
Can identify < > and actions to take if noted
PCS30
Analyser is correctly cleaned and stored
PCS31
Patients results correctly entered on to Practice IT systems and into ‘Yellow Booklet’
PCS32
Patient follow up appointment made
Standard 5: There are robust quality control checks in place
PSC33
There is evidence of quality control checks
PSC34
Control aliquots stored correctly
PSC35
Test strips stored correctly
Standard 6: Practitioners have an understanding of error symbols on the analyser
PSC36
Correctly identifies 5 error messages

NP109 Anticoagulation Operation Policy Page 32 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Assessor Guidance Unless indicated as not applicable (N/A) and a reason provided, all of the above criteria must be achieved to gain competency
• All candidates must also undertake a verbal knowledge assessment
conducted by the assessor
• Where certain aspects of the assessment cannot be observed such as correct responses in the knowledge assessment will suffice as long as the alternative is observed
Competency Agreed
Competency Failed
Name of Assessor
Designation
Signature
Date

NP109 Anticoagulation Operation Policy Page 33 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Knowledge assessment
The candidate will demonstrate an understanding of the importance of the following points (please tick as appropriate)
Criteria
Pass
Fail
N/a
Comments
Actions to take if referral form incomplete
Actions to take if referral incorrect on patient details
Actions to take if the practitioner is unable to access patient management plan or patient information
Actions to take if patient has experienced changes to medication, diet, physical health, admission to A&E / secondary care
Actions to take if ‘Yellow Booklet’ lost
Actions to take if patient does not give verbal consent
Actions to take if patient identity cannot be safely confirmed
Able to manage a minimum of 5 error messages on the analyzer
Understands the term ‘antagonise’
Name of Delegate
Designation
Date of Assessment

NP109 Anticoagulation Operation Policy Page 34 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Criteria
Pass
Fail
N/a
Comments
Can give 2 medicines that ‘antagonise’ Warfarin
Give side effects of Warfarin and actions if noted
Understands the term ‘potentiate’
Can name 2 medicines that ‘potentiate’ Warfarin
Name 2 medicines that must not be prescribed
What advice would you give a patient undergoing surgery or attending a dentist, about his/her warfarin?
Competency Agreed
Competency Failed
Name of Assessor
Designation
Signature
Date

NP109 Anticoagulation Operation Policy Page 35 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Supplementary Questions for use by the Assessor
The following questions should be used to ascertain the candidate understands of the statements in the above knowledge assessment. Q: What would you do if the information on the referral form did not match that on your records, the yellow book or what the patient was saying A: Q: What would you do if you were unable to access the patients IT records if there was a problem with the IT system? A: Q: How would you record your data? A: Q: What actions would you take if you were informed that there had been a change in
a) The patients medication b) Diet c) Physical health d) Admission to secondary care / A&E
A:
Name of Delegate
Designation
Date of Assessment

NP109 Anticoagulation Operation Policy Page 36 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Q: What would you do if the patient lost their yellow booklet? A: Q : What would you do if the patient refused to give consent to blood testing A: Q: What actions would you take if you were unable to safely identify a patient A: Q: What are the side effects of Warfarin therapy? A: Q: State what advice you would give a patient on warfarin undergoing surgery, or attending a dentist appointment A:

NP109 Anticoagulation Operation Policy Page 37 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 2
NEAR PATIENT TESTING AND MAINTENANCE OF ORAL ANTICOAGULATION THERAPY IN PRIMARY CARE
STANDARDS AND CRITERIA (NPSA STANDARDS)
These standards are the minimum required for safe practice and are aimed at reducing error in this part of patient management process. There are 6 standards with performance criteria (PC) Standard S1 There is a clear patient referral system that identifies patient information PCS1 Patient name and contact details PCS2 Patient Date of Birth and gender PCS3 NHS/ Hospital Number PCS4 Any special instructions, investigations (including abnormal blood test results) PCS5 Signature of requesting person and their contact details Standard 2 There is a clear understanding and confidence in using the G.P IT system for patient management, and evidence that patient information can be accessed and updated PCS6 The practitioner can access a patient management plan and identify indications for
warfarin therapy PSC7 The practitioner knows how to access and update the following information:
a) Medication changes b) Changes in diet c) Changes in physical and mental health d) Current warfarin therapy and duration of treatment e) Recent admissions to secondary care / A&E
PSC8 The practitioner can confidently use the Practice IT systems that support patient Anticoagulation management
Standard 3 There are correct safety checks in place prior Near Patient Testing procedure PSC9 The patient’s identity is confirmed using:
a) Full Name b) Date of Birth c) First line of address

NP109 Anticoagulation Operation Policy Page 38 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
PSC10 The patients ‘Yellow Booklet’ is used to confirm the patients correct Identity
PSC11 The patients ‘Yellow Booklet’ is checked for recent INR recordings and dosages PSC12 The practitioner is aware of the system in place should the patient forget their ‘Yellow
Booklet’ or if it is not holding up to date information PSC13 The ‘Yellow Booklet’ can be replaced if lost, damaged or full PSC14 Patient verbal consent is obtained prior to the procedure. PSC15 If there is a carer present during the procedure consent for their presence is obtained PSC16 Patients medical history / side effects are reviewed since last attendance:
a) Verbal b) Using IT systems / electronically
PSC17 If the patient is unable to confirm patient identity details, these care confirmed with their carer
Standard 4 The correct procedure is followed in Near Patient Testing PSC18 Ensures code number matches test strip PSC19 Correctly switches on meter PSC20 Correctly checks battery level, date and time PSC21 Patient ID entered (if applicable) PSC22 Test strip correctly inserted PSC23 Waits until hourglass symbol and ‘bleep’ before progressing PSC24 Correctly interprets the blood drop icon and 120-second countdown PSC25 Patients finger is correctly pricked in line with Infection Control Policies PSC26 Blood correctly applied to cover the semi-circular transparent sample application area
within 15 seconds PCS27 Blood is placed against the side of the sample application area PSC28 Correctly interprets patient test result on display area PSC29 Safely interprets < > signs and actions to be taken if noted PSC30 Analyser is correctly cleaned and stored PSC31 Patient results are correctly entered onto IT system and into patients ‘Yellow Booklet’ PSC32 Patient follow up appointment is arranged according to need Standard 5 There are robust quality control checks in place PSC33 There is a clear audit trail of quality control checks for each analyzer PSC34 The control aliquots are stored safely in correct conditions PSC35 The test strips are stored safely in correct conditions Standard 6
Practitioners have an understanding of error symbols on the analyzer PSC36 Staff can correctly identify a minimum of 5 error signs (to be taken from training manual)

NP109 Anticoagulation Operation Policy Page 39 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 3 (see also appendix 11, 12 and 13) QUALITY CONTROL AND ASSURANCE There are three main methods of ensuring reliability and accuracy of results in the practice setting.
1. INTERNAL QUALITY CONTROL
FOR THE COAGUCHEK S MACHINE
This will be performed at least once a week or prior to testing on the first patient in every clinic:
1. Tap QC tube on tabletop to ensure glass ampoule is at the bottom of the tube. 2. Wrap a cloth around tube and break glass 3. Start the 2 minute timer 4. Tap the QC tube on the table 10 times to ensure solutions are mixed, then place to one side 5. Once the 2 minutes have elapsed, switch on the CoaguChek S using blue button 6. The CoaguChek S will display a code, this should match the code displayed on the foil pouch of
the test strips being used. 7. The CoaguChek S will then display a flashing strip. Unwrap the strip from the foil pouch 8. Insert the strip into the CoaguChek S with the arrows pointing onto the CoaguChek S and the
writing facing upwards 9. A clock will be displayed on the screen, the strip is now at the correct temperature, this takes 45
seconds 10. A drop of blood and 180 seconds will appear on the screen 11. Squeeze the QC tube and discard the first drop of control solution into the lid 12. Apply the second drop of control solution onto the yellow flashing target zone on the test strip 13. Your QC result will be displayed in 1 minute. 14. Document your result on internal quality control log sheet (See Appendix 11)
FOR THE COAGUCHEK XS PLUS MACHINE
This will be performed at least once a week or prior to testing on the first patient in every clinic: Liquid Quality Control 1. Open lid of vial and remove rubber cap. 2. Hold pipette with sealed neck pointing upwards, then cut off the end of the cap with scissors (do
not hold pipette close to your face). 3. Apply gentle pressure to reservoir to transfer entire contents of pipette into vial. 4. Ensure pipette does not come into contact with the dried control plasma. 5. Close container again and ensure you have pipette to hand. 6. Swirl the vial using circular motion to completely dissolve all the control plasma. 7. DO NOT shake the vial or turn it on its side. 8. Select QC Test from the Main Menu Screen. 9. Insert test strip as directed on screen. 10. Select CODE number from the list shown, or select NEW CODE if opening new lot of quality
control solutions.

NP109 Anticoagulation Operation Policy Page 40 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
11. Insert new code chip if required. 12. Apply sample from pipette to test strip as directed on screen. 13. Result is displayed, with the range displayed in brackets below result. 14. Document your result on internal quality control log sheet (See Appendix 11) 2. EXTERNAL QUALITY CONTROL FOR COAGUCHEK S This is no longer deemed necessary for the newer Coagucheck XS plus but continues to apply to the Coagucheck S machines
• Aim to have three patients tested for quality assurance each month (This equates to one test per week)
• Whilst choosing a patient at random for this test, aim to use a wide selection rather than using
the same group on a regular basis
• Record NPT result on appropriate documentation
• Send venepuncture specimen to Pathology Laboratory.
• Mark the normal form with QUALITY CONTROL AND ADD THE ANALYSER MACHINE NUMBER
• When the venepuncture result is received, record in documentation and check against NPT
result previously obtained. Person checking result to initial when checked.
• A difference between UHL lab result and NPT result of +/- 2 standard deviations. For example. a reading of 3.0 acceptable range would be from 2.8 to 3.2.
• A log should be kept recording in columns the date, the near patient test result and the lab
result (See Appendix 12). 3. NATIONAL EXTERNAL QUALITY ASSURANCE SCHEME Uk Neqas For Blood Coagulation: Near Patient Testing Scheme The purpose of the Scheme is to provide external quality assessment (EQA), as a part of the overall quality assurance, for tests of blood coagulation carried out on instrument systems designed for ‘near-patient’ testing at all sites, whether within or remote from hospital laboratories. The aim of the Scheme is to promote high standards of performance and practice, achieved with the UK NEQAS primary aim of education, by provision of independent, objective and impartial information. The British Society for Haematology has published guidelines for the evaluation and use of NPT devices, underlining the importance of EQA of these instruments (Clin. Lab. Haem. 1995, 17, 301-310). The guidelines also promote the importance of a close liaison between the decentralised site and the local Haematology department.

NP109 Anticoagulation Operation Policy Page 41 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Registration The participant registered should be the centre responsible for performing the tests. If the daily testing is carried out by a GP surgery, the surgery should be registered. Data from participants will be treated with strict confidentiality. Each registered participant will be given a unique participation number, which should be quoted in all correspondence. Use of this number will assist in maintaining confidentiality in survey correspondence. Participation Participating centres will be sent four surveys per year, including samples for Prothrombin Time (PT) and/or Activated Partial Thromboplastin Time (APTT). Each participant will receive one or two samples for the tests for which they are registered, per survey. The samples will be appropriate for the system registered. In the case of UK NEQAS supplied samples, this will be lyophilised human plasma which has been screened for hepatitis B surface antigen (HBsAg), and for antibodies to hepatitis C virus and human immunodeficiency virus types 1 and 2 (anti-HIV-1+2). Participants will be provided with instructions on reconstitution and testing of the samples. A closing date for return of results will be given. Results will be analysed, and individual reports sent to participants approximately one week after the closing date. Performance analysis Approval has been granted by the National Quality Assurance Advisory Panel for Haematology for the application of performance criteria. A median result will be calculated for each reagent/instrument group, and the percentage deviation of individual laboratories from this median will be determined. This figure will indicate how close to the 'consensus' result individual results are from other users of the test system, and performance 'outwith consensus' is defined as a result greater than a 15% deviation from the reagent group median. An overall report on the operation of the Scheme will be distributed, initially on an annual basis. UK NEQAS for Blood Coagulation, and the Near Patient Testing EQA Scheme have been awarded full Unconditional Accreditation by Clinical Pathology Accreditation (CPA (UK) Ltd.) in the EQA Scheme Accreditation programme. For further details, please contact the Scheme Manager, UK NEQAS for Blood Coagulation, Rutledge Mews, 3 Southbourne Road, Sheffield S10 2QN U.K.
Tel: 44 (0)114 267 3300 Fax: 44 (0)114 267 3309 E-mail: [email protected]

NP109 Anticoagulation Operation Policy Page 42 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 4 OUTLINE OF AREAS TO BE COVERED BY THE SOP Standard Operating Procedure (SOP) for Oral Anticoagulation with Warfarin (Outline – to be completed and individualised by practice *) This SOP is designed to ensure:
• That the chances of harm to patients are minimised.
• That staff involved in dosing and monitoring patients who are receiving / going to receive anticoagulation treatment are properly trained.
• That equipment used to monitor anticoagulation therapy is fit for purpose and that it is
regularly calibrated and maintained according to manufacturer’s guidelines.
• That dosing / monitoring of anticoagulation therapy is PATIENT specific, agreed with the patients GP, and is sufficiently flexible to accommodate changes in patient circumstances such as co-morbidities, medication and diet.
• That the patient understands the importance of regular monitoring of anticoagulation therapy
and the need to adjust doses.
• That accurate clinical records are kept by the practice for each individual patient with respect to the:
• Therapeutic reason for anticoagulation • Anticipated duration of anticoagulation • INR range expected for the individual patient (depending on the indication) • Dosing regime following the last test • Date the next INR test is due following dosing.
The records may be computerised (with daily backup) or kept manually and all of the above information should also be available in the patients’ yellow anticoagulation booklet (in case the patient is away from the practice area or admitted to hospital).
• That staff are identified to take responsibility for inputting data on to the practice system.
• That all staff involved in anticoagulation therapy understand the course of action to take when the INR is > 5 by referring to a GP.
• That an audit process is set up to ensure that patients are receiving optimal care with respect
to anticoagulation therapy.
• That procedures are in place that ensure that following an INR result the dose of warfarin is adjusted the same day and the patient advised accordingly.

NP109 Anticoagulation Operation Policy Page 43 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Equipment Training and SOP
1. Each practice should ensure that anticoagulation monitoring equipment complies with the required standard ( ) and is regularly maintained and calibrated.
2. That staff engaged in anticoagulation monitoring have appropriate training and updating
according to PCT schedules.
3. That there are clear lines of accountability clinically when action needs to be taken regarding dosing outside the patient specific INR range.
4. That there is due provision to patient / staff safety and adequate precautions are in place for
blood testing The Use of INR Star or other dosing PCT approved software
1. That all staff involved in INR monitoring and warfarin dosing are familiar with INR Star and that training has been undertaken
2. That all staff are aware that only a doctor or nurse prescriber with specific extended training can override INR Star.
3. That a procedure is in place for adjusting patient dosing should INR Star fail. Clinical Records
1. There must be accurate, legible patient records which record either manually or on computer the following fields;
• Clinical indication for anticoagulation.
• Expected INR range for that clinical condition and duration of therapy.
• The INR result immediately on getting a result.
• Recording of the appropriate dose of Warfarin following the last INR result.
• When the next INR test is due.
• That the patient had been informed what the dose of Warfarin to be taken is and when
the next INR is due.
• That the date of the information (above) provided to the patient is recorded.
• Staff must receive appropriate training in the keeping of good clinical records and understand why this is important.
• There must be a policy that permits staff to record clinical information.

NP109 Anticoagulation Operation Policy Page 44 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
• The recording of information must take into account patient confidentiality.
• Responsible staff must be clear on which system data / clinical information is recorded.
• The same information must be recorded in the patients’ yellow book or suitable alternative (such as a print out) as long as it contains the relevant information.
Frequency of INR Testing
1. The frequency of INR testing may have to vary depending on individual patient circumstances.
2. Staff involved in anticoagulation monitoring and treatment must be familiar with the range of factors including other medication / diet / alcohol that can affect INR status.
3. Staff should be in a position to provide information and counsel patients appropriately with
respect to (2) above.
4. Practice systems should be sufficiently flexible to allow daily monitoring of INR if needed (except weekends)
Information Transfer within Practice
1. No patient should be placed in a position of not receiving an INR test on the appropriate day.
2. Patients should not have dosing on a day(s) subsequent to an INR test result. Dosing must be on that day unless the GP or nurse prescriber with specific extended training agrees to an alternative day.
3. There must be systems in the practice, which allow another responsible clinician to inform the
patient of their INR result and subsequent dosing on the same day if the patient cannot initially be contacted and the original member has gone off duty.
Housebound Patients
1. Not all patients can attend surgery for INR testing, so practices must make provision if these patients are to be tested in a timely manner at home (including residential /nursing homes).
2. Dosing must be done by an appropriately qualified member of staff following an INR result
3. See section on clinical records and documentation. The documentation requirements are no
different for housebound patients Patients Coming Out of Hospital / Holiday
1. The practice must make a mutual arrangement with the secondary care trust for the seamless transfer of anticoagulation therapy for patients who are returning home from hospital. UHL should provide proper information and follow the correct procedure in order for the GP to fax back an acceptance otherwise the pt stays under UHL for warfarin monitoring.

NP109 Anticoagulation Operation Policy Page 45 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
2. Patients who have been on a prolonged holiday must have information on the requirements of
monitoring and dosing whilst away and how they will fit into the practice system on return. Who Can Prescribe?
1. Doctors registered with the GMC have the right to prescribe anticoagulation treatment if they feel they have competence in this area and dose the patient.
2. Independent / Supplementary Prescribers with specific extended training can also prescribe
Warfarin
3. Registered nurses are able to carry out patient testing and dosage adjustment where a Patient Specific Direction exists (the PSD must be given to the patient and kept in the patients’ yellow book or suitable alternative (such as a print out) as long as it contains the relevant information.
4. If non-qualified staff such as Health Care Assistants are carrying out patient testing they
cannot decide the dose of Warfarin to be taken by a patient or complete a patients’ yellow book .

NP109 Anticoagulation Operation Policy Page 46 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 5 SIDE EFFECTS OF WARFARIN Bleeding related to warfarin therapy is a drug-induced condition and represents the most frequent complication of anticoagulation therapy. It is caused by relative overdose or increased sensitivity to warfarin and its severity varies from increased bruising to death. Hemorrhagic complications may be manifested by signs of symptoms that do not indicate obvious bleeding – for example, headaches, pains in the chest, abdomen and joints, swellings, shortness of breath and other unexplained symptoms. Almost any organ of the body can be involved. It is important therefore to investigate any unexplained condition for haemorrhage. Bleeding most often occurs in the nasopharynx, gastrointestinal tract, soft tissue and the urinary tract. In a third of these clients, investigation leads to identification of previously unknown lesions, even when the INR is elevated (BSH 1990, Landefeld and Beyth 1993). Intracranial bleeding, although rare, is associated with raised systolic and diastolic blood pressure and increased age (Landefeld and Beyth 1993, Laupacis et al 1994). Risk Factors – Contraindications to Warfarin Contra-indications to warfarin must be considered alongside an individual assessment of each client, his / her medical conditions, home situation and additional support. It is important also to assess the mental condition of the client as mental impairment or lack of cooperation can mean the client is unlikely to maintain the correct dosage. Studies have shown that bleeding is approximately three times more common in intensively treated clients (INR 3.0 – 4.5) than less intensively treated clients. It is not known if the intensity of anticoagulation therapy has decreased in the past 10 years in response to these studies (Kearon and Hirsh 1997, Landefeld and Beyth 1993). There is also a cumulative factor. The risk of bleeding is greatest in the first month of therapy, reducing at year one, but it then continues to increase by approximately 3% per year. The issue of whether the frequency of bleeding increases with age (65 years or more) remains controversial (Landefeld and Beyth 1993, Laupacis et al 1994). Other risk factors for bleeding are poor client compliance, medication errors, drug interactions and co-morbid illness, for example: • Serious cardiac illness / recent myocardial infarction • Liver dysfunction • Renal insufficiency • Poor general condition • Sever anaemia • Atrial fibrillation • History of cerebrovascular accident • History of gastrointestinal bleeding

NP109 Anticoagulation Operation Policy Page 47 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Severity Index It is important to classify the occurrence and severity of bleeding for monitoring and evaluation of the client’s condition. However, definitions in the literature vary widely. Landefeld (1989) devised a 3-PONIT system that identifies the amount of blood loss, the rate of bleeding and the consequence of bleeding. Other methods record bleeding that is major and of no consequence (Landefeld and Beyth 1993). As none of these methods is easy to use in primary care, a simple numerical system has been adopted here (Box 5). Bleeding Severity Index Grade Condition Further Notes Sign/Symptom Action 1 Extended bruising with contact May be simple side effect – Check INR 2 Bruising without contact(s) May be simple side effect – Check INR 3 Prolonged bleeding (such as haemorrhoids,
menorrhagia) INR may be raised - Check INR
4 Haematuria, epistaxis, malena haemoptysis, bleeding gums
Further investigations
5 INR between 6.0 and 8.0 with haemorrhage Admit 6 INR over 8.0 Admit (Emergency) 7 Excess Haemorrhage Admit (Medical Emergency) 8. Death Report

NP109 Anticoagulation Operation Policy Page 48 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 6
FACTORS THAT AFFECT ANTICOAGULATION CONTROL DIET Some foods affect the individual’s response to warfarin. Vitamin K (phytomenadione), for example, may cause INR variability. High concentrations are commonly found in green leafy vegetables, beef liver, rapeseed oil, green tea and some other products. Patients should be advised not to make changes in their level of consumption of these foods, as stopping, starting or changing will affect the INR value. Dietary supplements will potentiate the action of warfarin. In general, a low fat diet is recommended. Common foods that affect anticoagulation control FOODS THAT ANTAGONISE Avocado Broccoli Brussel Sprouts Cabbage (fresh boiled or raw green) Lettuce (dark green / red) Spinach Collards Endive Kale Watercress Ice Cream in large quantities (1 litre) Soya bean products Swiss hard cheese Cranberry juice FOODS THAT POTENTIATE Fish oil supplements Vitamin E supplements NB: This list is not exclusive Alcohol consumption has a variable effect on anticoagulation control. Clients should be advised to take only moderate amounts. Stopping, starting or changing will affect the INR value.
• Moderate intake is not considered to be problematic (2 units daily) • Heavy regular intake may reduce the anticoagulation effect • Acute intake may enhance the anticoagulation effect and result in an inaccurate reading. The
INR should therefore be taken again after one week to re-establish stability. Alternative / Complementary therapy Acupuncture contraindicated in pts on warfarin Aromatherapy Avoid leg massage in pts with a history of DVT Herbal Remedies Avoid in pts on warfarin Homeopathy Avoid if concentration of treatments <12c or <30x

NP109 Anticoagulation Operation Policy Page 49 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Alternative Therapy potential interactions HERBAL MEDICINED
POTENTIAL INTERACTION WITH WARFARIN
Danshen Increased bleeding time
Devils Claw Blood disorders visible on skin- purpura
Dong Quai Increased bleeding time and widespread bruising
Feverfew Inhibition of herbal effects, altered bleeding time
Garlic Altered bleeding time, inhibits platelet aggregation
Gingko Altered bleeding time, inhibits platelet aggregation, hypertension
Ginseng Altered bleeding time, possible addictive effect, manic episodes, headaches, tremor, altered glucose
Glucosamine Altered bleeding time
Papaya Increased bleeding time
St John's Wort
Induces some cytochrome p450 enzymes, so reducing blood concentrations of warfarin
Clinical factors which affect anticoagulation control INTERNAL POTENTIATING FACTORS (INCREASE SENSITIVITY TO WARFARIN) Hyperthyroidism Cardiac failure Renal failure Liver damage Biliary obstruction Fever Infectious disease Cholestasis Malnutrition / weight loss Alteration in intestinal absorption Carcinoma Radiation therapy Menstrual disorders INTERNAL ANTAGONISTIC FACTORS (DECREASE SENSITIVITY TO WARFARIN) Hypothyroidism Diabetes mellitus Oedema Hyperlipidemia Visceral carcinoma NB: This list is not exclusive

NP109 Anticoagulation Operation Policy Page 50 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
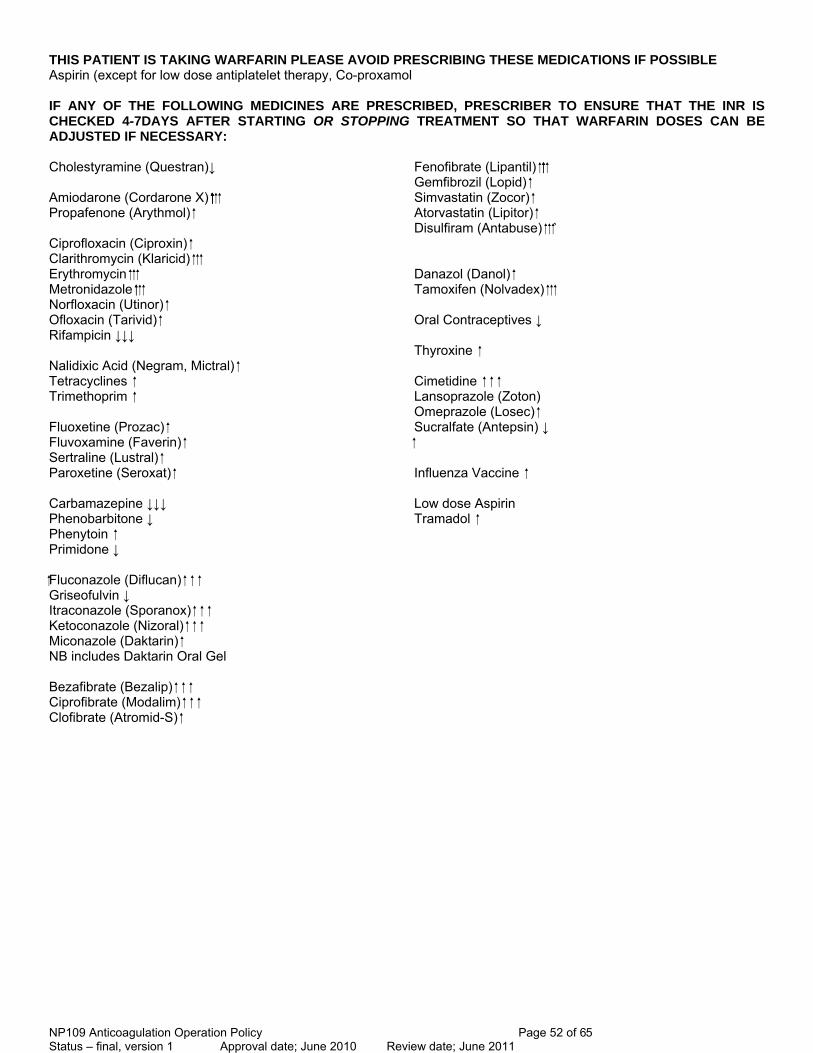
Concomitant drug therapy Giving drugs that interact with warfarin should generally be avoided. Where it is not possible, the client may require more frequent monitoring or changes in anticoagulation management. This is particularly so when a new drug is started, the dose is adjusted or the drug is stopped. Clients should be advised to inform the nurse of any change in their medication. Warfarin and Aspirin Aspirin should only be taken in association with warfarin when prescribed by a cardiologist in accordance with the client’s medical history. Greater care is needed in monitoring these clients, not only because of aspirin’s ability to displace warfarin into the circulation but also because of the irritant effect of aspirin on the gastric mucosa, which increases the incidence of haematemesis. In this situation, the prothrombin time control does not reflect the potential risk of bleeding. DRUGS THAT INTERACT WITH WARFARIN (list not exhaustive. Check EMIS or other clinical system and BNF. Drug Information at UHL if in doubt)
POTENTIATING DRUGS ANTAGONISTIC DRUGS
Gastrointestinal Tract Antacids (magnesium salts) Cholestyramine Cimetidine Colestipol Liquid paraffin and other laxatives Cardiovascular System Amiodarone Spironolactone Clofibrate Diazoxide Dipyridamole Ethacrynic Acid Quinidine Sulphinpyrazone Respiratory System Antihistamines Central Nervous System Carbamazepine Chloral Hydrate and related products Barbiturates Haloperidol Chlorpromazine Phenytoin Dextropropoxyphene Primidone Monoamine oxidase inhibitora Tricyclic antidepressants Triclofos sodium Infections Amino glycosides Griseofulvin Gentamicin Rifampicin Kanamycin Neomycin Streptomycin

NP109 Anticoagulation Operation Policy Page 51 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Tobramycin Endocrine System Anabolic steroids Oral contraceptives Chlorpropamide Corticosteroids Danazol Glucagon Metoclopramide Propylthiouracil Sulphonylureas e.g gliclazide Levothyroxin Tolbutamide Cyclophosphamide Mercaptopurine Methotrexate Tamoxifen Musculoskeletal and joint disease Allopurinol Aspirin and the salicylates Azapropazone Diflunisal Fenclofenac Fenoprofen Flufenamic acid Flurbiprofen Indomethacin Ketoprofen Mefenamic acid Naproxen Malignant disease and immunosuppression Paracetamol (high daily doses, with dextropropoxyphene)
Distalgesic / coproxamol Alternative medicines Gingko biloba St Johns Wort
NP109 Anticoagulation Operation Policy Page 52 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
THIS PATIENT IS TAKING WARFARIN PLEASE AVOID PRESCRIBING THESE MEDICATIONS IF POSSIBLE Aspirin (except for low dose antiplatelet therapy, Co-proxamol IF ANY OF THE FOLLOWING MEDICINES ARE PRESCRIBED, PRESCRIBER TO ENSURE THAT THE INR IS CHECKED 4-7DAYS AFTER STARTING OR STOPPING TREATMENT SO THAT WARFARIN DOSES CAN BE ADJUSTED IF NECESSARY: Cholestyramine (Questran)↓ Fenofibrate (Lipantil) Gemfibrozil (Lopid) Amiodarone (Cordarone X) Simvastatin (Zocor) Propafenone (Arythmol) Atorvastatin (Lipitor) Disulfiram (Antabuse) ` Ciprofloxacin (Ciproxin) Clarithromycin (Klaricid) Erythromycin Danazol (Danol) Metronidazole Tamoxifen (Nolvadex) Norfloxacin (Utinor) Ofloxacin (Tarivid) Oral Contraceptives ↓ Rifampicin ↓↓↓ Thyroxine Nalidixic Acid (Negram, Mictral) Tetracyclines Cimetidine Trimethoprim Lansoprazole (Zoton) Omeprazole (Losec) Fluoxetine (Prozac) Sucralfate (Antepsin) ↓ Fluvoxamine (Faverin) Sertraline (Lustral) Paroxetine (Seroxat) Influenza Vaccine Carbamazepine ↓↓↓ Low dose Aspirin Phenobarbitone ↓ Tramadol Phenytoin Primidone ↓ Fluconazole (Diflucan) Griseofulvin ↓ Itraconazole (Sporanox) Ketoconazole (Nizoral) Miconazole (Daktarin) NB includes Daktarin Oral Gel Bezafibrate (Bezalip) Ciprofibrate (Modalim) Clofibrate (Atromid-S)

NP109 Anticoagulation Operation Policy Page 53 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 7 AUDIT (See ACTIONS THAT CAN MAKE ANTICOAGULANT THERAPY SAFER (NPSA safety alert 18) Full document available at www.npsa.nhs.uk/health/alerts MINIMUM STANDARDS
• All Staff involved in monitoring INRs have the necessary competences
• Written procedure and clinical protocol in place to include guidance on the following • risk assessing benefits ‘v’ risk for individual pts • providing pt information prior to starting warfarin and when necessary (PIL as part of protocol) • How to safely initiate warfarin loading doses in general practice • How to monitor and adjust dosage warfarin to achieve target INR range • Safe systems for documenting results and treatment (computer /written record, responsibility
for updating and informing pt) • Effective communication systems when clinical responsibility for warfarin is being transferred
eg on discharge from hospital • That safe practice is promoted with prescribers and pharmacists to check pt being monitored
regularly and that INR level is safe before issuing or dispensing rpt scripts • Safe practice promoted when co-prescribing and clear arrangement in place for additional
INRs • annual clinical review of pts on warfarin • How pts should discontinue warfarin • All strengths of warfarin should be used to best meet pt needs • Dosage recommendations should use least number tablets, be expressed mg not number of
tablets, use constant daily dosing not alternate day dosing and not require the use of half tablets.
• promotion of written safe practice procedures for housebound/nursing home pts
• Audit of Safety Indicators 1. There is an up to date INR monitoring protocol in place 2. All new patients receive appropriate verbal and written information (INR Book) 3. All patients have at least an annual medication review 4. INR results in terms of number of weeks out of range and point prevalence 5. Percentage of INRs >5.0 6. Percentage of INRs >8.0 7. Percentage of INRs more than 1.0 unit less than their target 8. Percentage of patients suffering adverse events 9. Percentage of patients lost to follow up 10. Number of patients on scheme per quarter

NP109 Anticoagulation Operation Policy Page 54 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 8
CRITICAL INCIDENT / SIGNIFICANT EVENT ANALYSIS In March 2007 the National Patient Safety Agency published a Patient Safety Alert “Actions that can make anticoagulant therapy safer”. It recommends an annual audit of the service provided, however all critical / significant events should be reported to the PCT at the time of the incident. Definitions Serious adverse event
• Bleeding: if admitted to hospital or if surgery was required to stop bleeding and if bleeding led to reduction in Hb of 2g/L or more +/- requiring blood transfusion
• Thrombotic: Transient Ischaemic Attack (with observed neurological deficit), or Stroke, recurrent Deep Vein Thrombosis and Pulmonary Embolism, Systemic embolism
Non-serious event
All cases of bleeding with no significant associated medical consequences eg bruising, small epistaxis, and microscopic haematuria

NP109 Anticoagulation Operation Policy Page 55 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Suggested template for collecting adverse /significant events related to the practice anticoagulation service
Clinical outcome Number of reports
Death
Severe (permanent harm)
Moderate (significant, but not permanent harm, requiring increase in treatment)
Low (temporary harm, requiring extra observation or minor treatment)
No harm
Total
Type of report Number of reports
Prescribing
Dispensing/medicine preparation
Administration
Monitoring
Total
Type of incident Number of reports
Wrong dose
Wrong frequency
Omitted medicine/dose
Wrong drug
Wrong quantity
Mismatching of patient and their medicine
Wrong/transposed/omitted medicine label
Wrong/omitted/passed expiry date
Wrong storage
Wrong route
Contraindication
Patient allergic to treatment
Wrong formulation
Wrong method of preparation/supply
Adverse drug reaction – when used as intended
Wrong or omitted verbal patient directions
Other
Total

NP109 Anticoagulation Operation Policy Page 56 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 9
PROCEDURE FOR OBTAINING SUPPLIES OF TESTING STRIPS AND CONTROL SOLUTION Detailed below is the information practices will need in order to ensure that they have adequate supplies of the strips and control solution for the monitoring of their patients. If you do not currently have an account set up with the supplier Roche Diagnostics, you will need to set one up. The PCT has sent a list of the practices that will be ordering test strips to Roche Diagnostics Ltd and has also negotiated with them the continuation of the discount they gave the PCT. Their contact details are: Roche Diagnostics Limited Charles Avenue Burgess Hill West Sussex RH 15 9RY To order your supplies, please contact Roche Customer Services on: Telephone Number: 0808 100 9998 Fax Number: 0808 100 8060 Email Address: [email protected] If you need to set up an account with Roche then please contact Roche Customer Services using any of the above details. Please be aware that the practice will be responsible for paying the invoices. Failure to do so may jeopardise your supplies.
NP109 Anticoagulation Operation Policy Page 57 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 10
CoaguChek S/XS Internal Quality Control Log Sheet
Date Time Machine
No Person Completing
INR Result Date Time Machine No Person Completing
INR Result
Surgery:

NP109 Anticoagulation Operation Policy Page 58 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
APPENDIX 11 U.K. National External Quality Assessment Programme for Near Patient Testing for Users of Coaguchek & S devices and Coaguchek XS & XS Plus Devices GENERAL INFORMATION 2008/2009 Revised: January 2008 UK NEQAS for Blood Coagulation Rutledge Mews, 3 Southbourne Road, Sheffield S10 2QN U.K. Tel: +44 (0)114 267 3300 Fax: +44 (0)114 267 3309 E-mail: [email protected] Web site: www.ukneqasbc.org
BACKGROUND The purpose of the Near Patient Testing (NPT) programme is to provide external quality assessment (EQA), as a part of the overall quality assurance, for tests of blood coagulation carried out on instrument systems designed for ‘near patient’ or ‘point of care’ testing (POCT) at all sites, whether within or remote from hospital laboratories. The aim of the programme is to promote high standards of performance and practice, achieved with the UK NEQAS primary aim of education, by provision of independent, objective and impartial information. The NPT EQA for Blood Coagulation programme is open to all potential participants, whether government supported, private or commercial concerns. The Scheme is run according to the UK National External Quality Assessment Service Code of Practice. The British Society for Haematology has published guidelines for the evaluation and use of NPT devices, underlining the importance of EQA of these instruments (Clin. Lab. Haem. 1995, 17, 301-310). The guidelines also promote the importance of a close liaison between the decentralised site and the local Haematology department. REGISTRATION The participant registered should be the centre responsible for performing the tests. If the daily testing is carried out by a GP surgery, the surgery should be registered. However, if a laboratory provides a satellite service to GP surgeries, it is suggested that the laboratory should be registered. Results and associated data from participants will be treated with strict confidentiality. Each registered participant will be given a unique participation number, which should be quoted in all correspondence. Use of this number will assist in maintaining confidentiality in survey correspondence.

NP109 Anticoagulation Operation Policy Page 59 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Please Note: The registration at a particular location covers a specific monitor that may be used by a number of different personnel and transported to an alternative location. REGISTERED PARTICIPANTS: Total number of participants 1379 (762 CUC & CUC S users) (594 CUC XS & CUC XS Plus users) UK: 1345 Non-UK 34
PARTICIPATION Participating centres will be sent at least four surveys per year, each comprising two samples for INR determination. The samples will be appropriate for the system registered. In the case of UK NEQAS supplied samples, this will be lyophilised human plasma which has been screened for hepatitis B surface antigen (HBsAg), and for antibodies to hepatitis C virus and human immunodeficiency virus types 1 and 2 (anti-HIV-1+2). Participants will be provided with instructions on reconstitution and testing of the samples. A closing date for return of results will be given. Results will be analysed, and individual reports sent to participants approximately one week after the closing date of a survey. A copy of the report can be sent to another named individual or site if requested in writing.
PERFORMANCE ANALYSIS Approval has been given by the UK National Quality Assurance Advisory Panel (NQAAP) for Haematology for the following performance criteria. A median result will be calculated for each reagent/instrument group, and the percentage deviation of individual laboratories from this median will be determined. This figure will indicate how close to the 'consensus' result individual results are from other users of the test system, and performance 'outwith consensus' is defined as a result greater than a 15% deviation from the reagent group median. An overall report on the operation of the Scheme will be distributed on an annual basis. UK NEQAS for Blood Coagulation and the Near Patient Testing EQA Scheme are fully accredited by Clinical Pathology Accreditation (CPA (UK) Ltd.) in the EQA Scheme Accreditation programme.
ANNUAL SUBSCRIPTION FEES; DISTRIBUTION SCHEDULE The following participation fees will apply for the financial year 1st April 2008 to 31st March 2009. These charges have been approved by the Executive Committee of UK National External Quality Assessment Service:

NP109 Anticoagulation Operation Policy Page 60 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Registration & 1 analyte (PT/INR): £132.00 + VAT where applicable There is no discount for additional registrations in the Near Patient Testing Scheme. Participants joining the Scheme for part of a year will be charged a pro-rata fee: 3 surveys in financial year: 75% of the applicable annual fee 2 surveys in financial year: 50% of the applicable annual fee 1 survey in financial year: 25% of the applicable annual fee Refunds will not be made, for registrations cancelled prior to the end of a financial year. Fees will be subject to review on an annual basis. Invoices will be sent directly to a registered accounts address, to be requested in subsequent documentation. A postal surcharge of £25 per annum will apply for participants located outside member countries of the European Union.
PERSONNEL Organised and Directed by Professor I D Walker, Glasgow Royal Infirmary, Glasgow, UK NEQAS for Blood Coagulation is managed by Mr T A L Woods at Rutledge Mews, 3 Southbourne Road, Sheffield S10 2QN. The Director and Manager receive advice and direction on overall operations from a Steering Committee. Members of staff include: Dr I Jennings, Deputy Scheme Manager Dr S Kitchen Scientific Director Mrs D P Kitchen Senior Biomedical Scientist Ms S Munroe Biomedical Scientist Mrs M Russell PA to Scheme Manager Mrs S L Rowbotham PA to Scheme Director Ms A Cox Medical Laboratory Assistant Mr S Asif Medical Laboratory Assistant Mr P Brown Computing Systems
STEERING COMMITTEE MEMBERS Dr B T Colvin (Chairman), Haematology Dept, The Royal London Hospital, London Mr P Cotton, Haematology Dept., King’s Mill Hospital, Mansfield Road, Sutton Ashfield Dr E Gray (NIBSC), National Institute for Biological Standards & Control, Herts. Dr I Jennings, UK NEQAS for Blood Coagulation, Sheffield Dr D Keeling, Oxford Haemophilia Centre & Thrombosis Unit, Churchill Hospital, Oxford Mrs D P Kitchen, UK NEQAS for Blood Coagulation, Sheffield Dr S Kitchen (Secretary), Coagulation Dept., STH Royal Hallamshire Hospital, Sheffield Dr M Laffan, Haematology, Imperial College School of Med. Hammersmith Hosp. London Dr I Mackie (CEP/MHRA), University College Hospital, London Dr D Perry, Clinical Haematology Dept., Addenbrooke’s Hospital, Cambridge Professor F R Rosendaal (Statistical Advisor), University Hospital, Leiden, The Netherlands Professor I D Walker (Scheme Director), UK NEQAS for Blood Coagulation, Sheffield Mr T A L Woods (Scheme Manager), UK NEQAS for Blood Coagulation, Sheffield

NP109 Anticoagulation Operation Policy Page 61 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
U.K. NATIONAL EXTERNAL QUALITY ASSESSMENT SCHEME FOR BLOOD COAGULATION Rutledge Mews Professor ID Walker (Director) 3 Southbourne Road Mr TAL Woods (Manager) Sheffield S10 2QN Tel: 0114 267 3300 Fax: 0114 267 3309
NEAR PATIENT TESTING EQA SCHEME:
REGISTRATION FORM
Please give name and address details for distribution of survey materials and reports
Please state details of either the Trust/PCT or General Practice responsible for payment of this invoice
Registration required for: Prothrombin Time/INR (YES/NO) ____________________________ Instrument/system used: CoaguChek S (YES/NO) CoaguChek XS/XS Plus (YES/NO) Hemochron Junior Signature with Citrated cuvettes (YES/NO) Hemochron Junior Signature with Non Citrated cuvettes (YES/NO) For other systems please contact UK NEQAS for Blood Coagulation; Tel: (0)114 267 3300 Name/position ____________________________________________________________ Address: ____________________________________________________________
____________________________________________________________
Plea e return form to: Mrs M Russell, UK NEQAS for Blood Coagulation, Rutledge Mews, 3 Southbourne Road, Sheffield S10 2QN.
If you have replaced an existing instrument and wish to change registration from the old to the new device, you do not need to take out a new registration – please record your participant number here: ………………… and your details will be transferred to the relevant programme.

NP109 Anticoagulation Operation Policy Page 62 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
s

NP109 Anticoagulation Operation Policy Page 63 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011

NP109 Anticoagulation Operation Policy Page 64 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011

NP109 Anticoagulation Operation Policy Page 65 of 65 Status – final, version 1 Approval date; June 2010 Review date; June 2011
Telephone 0116 258 5069
Fax 0116 258 7561