oral appliances for snoring, uars and obstructive sleep apnea bruce w. roman, dds, d. abdsm...
TRANSCRIPT

Oral Appliances for Snoring, Oral Appliances for Snoring, UARS UARS
and Obstructive Sleep Apneaand Obstructive Sleep Apnea
Bruce W. Roman, DDS, D. ABDSMBruce W. Roman, DDS, D. ABDSMDiplomate, American Board of OrthodonticsDiplomate, American Board of Orthodontics
Diplomate, American Board of Dental Sleep MedicineDiplomate, American Board of Dental Sleep Medicine
500 SE Douglas Ave…Roseburg, OR…541.672.5721…[email protected]…www.SmilesByRoman.com500 SE Douglas Ave…Roseburg, OR…541.672.5721…[email protected]…www.SmilesByRoman.com
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
What is SDB (Sleep-Disordered What is SDB (Sleep-Disordered Breathing) and how big a problem Breathing) and how big a problem
is it?is it?SDB includes snoring, Upper Airway Resistance SDB includes snoring, Upper Airway Resistance Syndrome (UARS), sleep apnea and the obesity-Syndrome (UARS), sleep apnea and the obesity-related hypoventilation syndrome.related hypoventilation syndrome.
Young, Young, et alet al, in a 2002 article in , in a 2002 article in AJRCCMAJRCCM, , Epidemiology of OSA: a population health Epidemiology of OSA: a population health perspectiveperspective, concluded: , concluded:
““SDB is being increasingly recognized as a cause of SDB is being increasingly recognized as a cause of substantial morbidity and mortality. Approximately substantial morbidity and mortality. Approximately 9% of women and 24% of men have SDB and a 9% of women and 24% of men have SDB and a majority of those remain undiagnosedmajority of those remain undiagnosed.”.”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Pathophysiology of Snoring Pathophysiology of Snoring and Obstructive Sleep and Obstructive Sleep
ApneaApnea

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
What What is is snoring?snoring?
Snoring is sound waves caused by Snoring is sound waves caused by vibrations, just as our vocal cords vibrations, just as our vocal cords vibrate to form sound waves that we vibrate to form sound waves that we call our voice.call our voice.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Where do the Where do the vibrationsvibrations come come from?from?
As you fall asleep, the soft tissues at the back of the throat, the muscles that line the airway, the soft palate, uvula and the tongue, relax.
The tongue then drops back into the airway, causing it to narrow.
As air passes through this narrower airway, it moves faster and causes the tissues to vibrate.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Is snoring Is snoring reallyreally a a problem?problem?
• Just ask the bed partner…they’ll tell you!!!Just ask the bed partner…they’ll tell you!!!
• 27-31% of all married couples sleep in 27-31% of all married couples sleep in separate separate rooms with snoring being a rooms with snoring being a principal reason.principal reason.
• With loud snoring, even other household With loud snoring, even other household members can be effected. And they don’t members can be effected. And they don’t like it any more than the bed partner.like it any more than the bed partner.
Bed Partners’ and Patients’ Experiences after Bed Partners’ and Patients’ Experiences after Treatment of OSA with an Oral Appliance; Treatment of OSA with an Oral Appliance; Tegelberg, et al., Swed Dent J 2012:Tegelberg, et al., Swed Dent J 2012:
• Both patients and bed partners reported Both patients and bed partners reported improvement in general well-being, improvement in general well-being, physical strength and mental energy (70-physical strength and mental energy (70-80% for patients; 55-68% for bed 80% for patients; 55-68% for bed partners).”partners).”• ConclusionsConclusions: “In all dimensions, the : “In all dimensions, the treatment effect had a great influence, treatment effect had a great influence, not only on patients but on bed partners not only on patients but on bed partners as well.”as well.”
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
What about “heavy” What about “heavy” snoring?snoring?
A study published in the September, 2008 A study published in the September, 2008 issue of issue of SLEEP, Heavy Snoring as a Cause of SLEEP, Heavy Snoring as a Cause of Carotid Artery AtherosclerosisCarotid Artery Atherosclerosis, concluded:, concluded:
“ “Heavy snoring (defined as more than 50% Heavy snoring (defined as more than 50% of the night) of the night) significantlysignificantly increases the risk increases the risk of carotid atherosclerosis (“hardening of the of carotid atherosclerosis (“hardening of the arteries”), and the increase is arteries”), and the increase is independentindependent of other risk factors.”of other risk factors.”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
What is What is UARS?UARS?• Upper Airway Resistance SyndromeUpper Airway Resistance Syndrome (UARS) is a (UARS) is a
sleep condition in which there is airway sleep condition in which there is airway resistanceresistance to breathing. Breathing becomes labored. It is to breathing. Breathing becomes labored. It is similar to trying to breathe through a similar to trying to breathe through a thin thin straw.straw.
• The increased upper airway resistance in UARS The increased upper airway resistance in UARS does not lead to a stoppage of airflow (apnea) or does not lead to a stoppage of airflow (apnea) or decrease in airflow (hypopnea), but instead leads decrease in airflow (hypopnea), but instead leads to an to an arousalarousal due to the increased work of due to the increased work of breathing to overcome the resistance. Repeated breathing to overcome the resistance. Repeated and multiple arousals (which the patient is usually and multiple arousals (which the patient is usually unaware of) result in fragmented and non-unaware of) result in fragmented and non-restorative sleep.restorative sleep.
• The primary UARS symptoms include snoring, The primary UARS symptoms include snoring, daytime sleepiness and excessive fatigue.daytime sleepiness and excessive fatigue.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
What is Sleep Apnea?What is Sleep Apnea?
There are three types of sleep apnea:There are three types of sleep apnea:
1) Central1) Central
2) Obstructive2) Obstructive
3) Complex or Mixed3) Complex or Mixed
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
CentralCentral Sleep Apnea Sleep Apnea
Central sleep apnea occurs when the Central sleep apnea occurs when the brain fails to send the appropriate brain fails to send the appropriate signals to the breathing muscles to signals to the breathing muscles to initiate respirations.initiate respirations.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
ObstructiveObstructive Sleep Apnea Sleep Apnea
Obstructive sleep apnea (OSA) is a sleep-Obstructive sleep apnea (OSA) is a sleep-related breathing disorder that involves a related breathing disorder that involves a RERA (respiratory effort-related arousal), RERA (respiratory effort-related arousal), decrease (hypopnea) or complete halt decrease (hypopnea) or complete halt (apnea) in breathing despite an ongoing (apnea) in breathing despite an ongoing effort to breathe.effort to breathe.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
ComplexComplex or or MixedMixed Sleep Sleep ApneaApnea
Mixed sleep apnea is a combination of Mixed sleep apnea is a combination of bothboth central sleep apnea central sleep apnea andand obstructive sleep apnea.obstructive sleep apnea.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
• If your oxygen level drops low enough—If your oxygen level drops low enough—and if you are experiencing an apnea, it and if you are experiencing an apnea, it will—your brain sends a signal to the will—your brain sends a signal to the muscles in the airway to contract.muscles in the airway to contract.
• The airway opens—usually accompanied The airway opens—usually accompanied by a loud gasp—and air flows again.by a loud gasp—and air flows again.
• Then the cycle starts Then the cycle starts againagain..

Why Be Concerned About Sleep Apnea?
The combination of low oxygen levels and broken
sleep cause one or more of these symptoms:
• 1) Excessive daytime sleepiness
• 2) Snoring
• 3) Cardiovascular disease (“heart attack”)
• 4) Cerebrovascular disease (“stroke”)
• 5) Brain damage
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
In the May, 2009 issue of the In the May, 2009 issue of the Journal of Journal of the American Dental Associationthe American Dental Association, , Simmons & Clark, in an article entitled, Simmons & Clark, in an article entitled, The potentially harmful medical The potentially harmful medical consequences of untreated sleep-consequences of untreated sleep-disordered breathingdisordered breathing, concluded: , concluded:
““The evidence suggests that EH [Episodic The evidence suggests that EH [Episodic Hypoxia], as seen in SDB, causesHypoxia], as seen in SDB, causes damage to the braindamage to the brain…and damage to …and damage to higher cognitive [thinking] functions.” higher cognitive [thinking] functions.”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
6) High blood pressure (hypertension)6) High blood pressure (hypertension)
7) Diabetes7) Diabetes
8) Depression8) Depression
9) Decreased sex drive and impotence9) Decreased sex drive and impotence
10) Morning headaches10) Morning headaches
11) Poor memory and clouded thinking11) Poor memory and clouded thinking
12) Personality changes and irritability12) Personality changes and irritability
13) Restless sleep13) Restless sleep
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
14) Increased health care costs14) Increased health care costs15) GERD (Gastroesophageal Reflux Disease)15) GERD (Gastroesophageal Reflux Disease)16) 10-15X more likely to have a motor16) 10-15X more likely to have a motor vehicle accident:vehicle accident:
– 0 hours of sleep = .195% blood alcohol level reaction time0 hours of sleep = .195% blood alcohol level reaction time– 2 hours of sleep = .102% blood alcohol level reaction time2 hours of sleep = .102% blood alcohol level reaction time– 4 hours of sleep = .095% blood alcohol level reaction time4 hours of sleep = .095% blood alcohol level reaction time– 6 hours of sleep = .045% blood alcohol level reaction time6 hours of sleep = .045% blood alcohol level reaction time
17) Loss of employment17) Loss of employment18) Marital discord18) Marital discord19) Bruxism19) Bruxism
Neurology of Sleep and Sleep-Related Neurology of Sleep and Sleep-Related Breathing Disorders and Their Relationships Breathing Disorders and Their Relationships to Sleep Bruxismto Sleep Bruxism, Simmons, , Simmons, JCDAJCDA; 2012 ; 2012 Feb;40(2):159-167Feb;40(2):159-167
““Recent research by Simmons and Prehn Recent research by Simmons and Prehn has demonstrated that SB or clenching has demonstrated that SB or clenching may occur as a mechanism to prevent may occur as a mechanism to prevent airway collapse. Their studies airway collapse. Their studies demonstrated that during the SB process demonstrated that during the SB process there is a reduction of negative pressures there is a reduction of negative pressures of the upper airway…When the SB process of the upper airway…When the SB process is not present, there is an increase in is not present, there is an increase in airway obstruction.”airway obstruction.”
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC

Effect of an Adjustable Mandibular Effect of an Adjustable Mandibular Advancement Appliance on Sleep Bruxism: Advancement Appliance on Sleep Bruxism: A Crossover Sleep Laboratory StudyA Crossover Sleep Laboratory Study; ; Shönbeck, et al., Shönbeck, et al., Intl J ProsthodonticsIntl J Prosthodontics, May-, May-Jun 2009; 22(3):251-259Jun 2009; 22(3):251-259
ResultsResults: The mean number of SB episodes/hr was : The mean number of SB episodes/hr was reduced by 39% and 47% from baseline with the MAA reduced by 39% and 47% from baseline with the MAA at a protrusion of 25% and 75%, respectively.at a protrusion of 25% and 75%, respectively.
ConclusionConclusion: Short-term use of an MAA is associated : Short-term use of an MAA is associated with a significant reduction in SB motor activity without with a significant reduction in SB motor activity without any appliance breakage. A reinforced MAA design may any appliance breakage. A reinforced MAA design may be an alternative for patients with concomitant tooth be an alternative for patients with concomitant tooth grinding and snoring or apnea during sleep.grinding and snoring or apnea during sleep.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
20) Increased mortality rate, 20) Increased mortality rate, especially especially for for men.men.
Dr. Naresh Punjabi (John Hopkins) and nine other Dr. Naresh Punjabi (John Hopkins) and nine other researchers examined 6,441 men and women. (researchers examined 6,441 men and women. (Sleep-Sleep-Disordered Breathing and Mortality: A Prospective Disordered Breathing and Mortality: A Prospective Cohort StudyCohort Study; ; PLoS MedicinePLoS Medicine, August, 2009). , August, 2009).
FindingsFindings: :
• Participants with severe SDB (an AHI of ≥ 30) were Participants with severe SDB (an AHI of ≥ 30) were about one and a half times as likely to die from any about one and a half times as likely to die from any cause after adjustment for potential confounding cause after adjustment for potential confounding factors.factors.
• In subgroups according to age and sex, men aged 40-In subgroups according to age and sex, men aged 40-70 years with severe SDB had twice the risk of dying 70 years with severe SDB had twice the risk of dying as men of a similar age without SDB.as men of a similar age without SDB.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
21) 21) CANCER!CANCER!
Sleep disordered breathing and cancer Sleep disordered breathing and cancer mortality: results from the Wisconsin mortality: results from the Wisconsin Sleep Cohort Study, Sleep Cohort Study, Nieto, et al, Nieto, et al, AJRCCMAJRCCM, May 20, 2012:, May 20, 2012:
““Compared to normal subjects, the Compared to normal subjects, the adjusted relative hazards of cancer adjusted relative hazards of cancer mortality were 1.1 for mild SDB, 2.0 for mortality were 1.1 for mild SDB, 2.0 for moderate SDB, and 4.8 for severe SDB.”moderate SDB, and 4.8 for severe SDB.”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Measuring Sleep ApneaMeasuring Sleep Apnea
AHI (Apnea-Hypopnea Index)AHI (Apnea-Hypopnea Index): The : The number of apneas and hypopneas that number of apneas and hypopneas that occur per hour.occur per hour.
MildMild: ≥ 5 and < 15 events/hr: ≥ 5 and < 15 events/hr
ModerateModerate: ≥ 15 and ≤ 30 events/hr: ≥ 15 and ≤ 30 events/hr
SevereSevere: > 30 events/hr: > 30 events/hr
Pediatric OSAPediatric OSA
• FrequentlyFrequently overlooked as a problem. overlooked as a problem.• Child often becomes overactive, rather than Child often becomes overactive, rather than
sleepy. Some become hyperactive and are sleepy. Some become hyperactive and are diagnosed ADHD.diagnosed ADHD.
• Symptoms include: 1) Restless sleep; 2) Loud Symptoms include: 1) Restless sleep; 2) Loud snoring; 3) Nightmares; 4) Morning snoring; 3) Nightmares; 4) Morning headaches; 5) Behavioral problems; 6) headaches; 5) Behavioral problems; 6) Bedwetting; 7) Gets tired easily; 8) Wakes up Bedwetting; 7) Gets tired easily; 8) Wakes up tired; 9) Concentration problems; 10) Is tired; 9) Concentration problems; 10) Is irritated.irritated.
• Most common causes: 1) Enlarged tonsils and Most common causes: 1) Enlarged tonsils and adenoids; 2) Narrow maxilla; 3) Obesity.adenoids; 2) Narrow maxilla; 3) Obesity.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
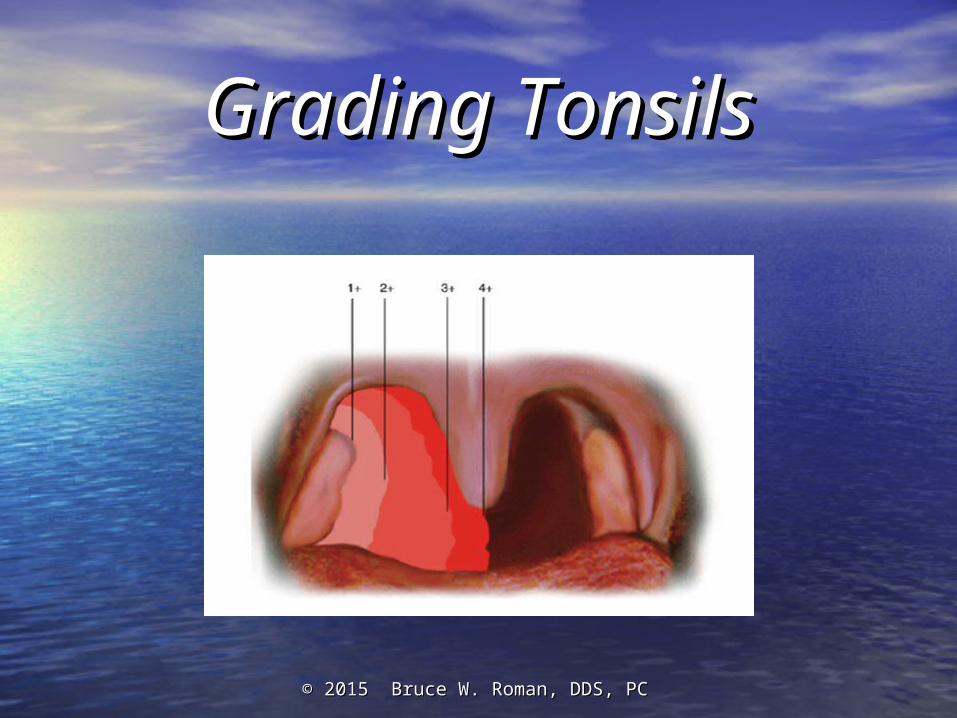
Grading TonsilsGrading Tonsils
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
WhenWhen are Oral Appliances (OA’s) are Oral Appliances (OA’s) indicated?indicated?
In the AASM (American Academy of In the AASM (American Academy of Sleep Medicine) report in the February, Sleep Medicine) report in the February, 2006 issue of 2006 issue of SLEEPSLEEP, , Practice Practice Parameters for the Treatment of Parameters for the Treatment of Snoring and Obstructive Sleep Apnea Snoring and Obstructive Sleep Apnea with Oral Appliances: An Update for with Oral Appliances: An Update for 20052005, it states:, it states:

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
1) OAs are appropriate for use in 1) OAs are appropriate for use in patients with patients with primaryprimary snoring snoring who who do not respond to or are not do not respond to or are not appropriate candidates for treatment appropriate candidates for treatment with behavioral measures such as with behavioral measures such as weight loss or sleep-position change. weight loss or sleep-position change.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
2) 2) Although not as efficacious as Although not as efficacious as CPAP, CPAP, OAs are indicated for use in OAs are indicated for use in patients with patients with mild or moderatemild or moderate OSAOSA who prefer OAs to CPAP, or who prefer OAs to CPAP, or who do not respond to CPAP, are who do not respond to CPAP, are not appropriate candidates for not appropriate candidates for CPAP, or who fail treatment CPAP, or who fail treatment attempts with CPAP or treatment attempts with CPAP or treatment with behavioral measureswith behavioral measures such as such as weight loss or sleep-position weight loss or sleep-position change. change.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
3) Reviewed studies of patients with 3) Reviewed studies of patients with severe OSAsevere OSA demonstrated demonstrated treatment success (variably defined) treatment success (variably defined) with OAs on an average of 34.3% ± with OAs on an average of 34.3% ± 13.5%...CPAP is indicated whenever 13.5%...CPAP is indicated whenever possible for patients with severe possible for patients with severe OSA before considering OAs. OSA before considering OAs.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Journal of Clinical MedicineJournal of Clinical Medicine Special Article of Special Article of March, 2009: March, 2009: Clinical Guide for the Clinical Guide for the
Evaluation, Management and Long-term Evaluation, Management and Long-term Care of OSA in AdultsCare of OSA in Adults
Some key pointsSome key points::
● ● Once the diagnosis is established, the Once the diagnosis is established, the patientpatient should be included should be included in deciding an appropriate treatment strategy that may include in deciding an appropriate treatment strategy that may include PAP devices, OAs, behavioral treatments, surgery, and/or PAP devices, OAs, behavioral treatments, surgery, and/or adjunctive treatments.adjunctive treatments.
● ● CPAP is the treatment of choice for mild, moderate, and severe CPAP is the treatment of choice for mild, moderate, and severe OSA and should be offered as an OSA and should be offered as an optionoption to all patients. to all patients. Alternative therapies may be offered depending upon the Alternative therapies may be offered depending upon the severity of the OSA and the patient’s anatomy, risk factors, and severity of the OSA and the patient’s anatomy, risk factors, and preferencespreferences and should be discussed in detail. and should be discussed in detail.
● ● If CPAP use is considered inadequate based on objective If CPAP use is considered inadequate based on objective monitoring and symptom evaluation, prompt and intensive monitoring and symptom evaluation, prompt and intensive efforts should be implemented to improve PAP use or efforts should be implemented to improve PAP use or consider consider alternative therapiesalternative therapies..
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Appliance Therapy vs. nCPAP Appliance Therapy vs. nCPAP in OSA; Respiration, Oct. 2010in OSA; Respiration, Oct. 2010
The article looked at carefully controlled The article looked at carefully controlled studies in which studies in which bothboth CPAP and OAs were CPAP and OAs were carefully titrated (adjusted).carefully titrated (adjusted).
ConclusionConclusion: There is : There is no clinically no clinically relevant difference between a MAD relevant difference between a MAD [Mandibular Advancement Device][Mandibular Advancement Device] and and nCPAPnCPAP in the treatment of mild/moderate in the treatment of mild/moderate OSA OSA when both treatment modalities when both treatment modalities are titrated [adjusted] objectivelyare titrated [adjusted] objectively..
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
How do you “titrate How do you “titrate objectively”?objectively”?
• After the patient is comfortable with the appliance, After the patient is comfortable with the appliance, additional advancement is slowly introduced.additional advancement is slowly introduced.
• While this is occurring, subjective reports and tests While this is occurring, subjective reports and tests (e.g., Epworth Sleepiness Scale) are used to assess (e.g., Epworth Sleepiness Scale) are used to assess progress.progress.
• Once subjective relief of symptoms is achieved or the Once subjective relief of symptoms is achieved or the limit of what the TMJs and/or musculature will allow is limit of what the TMJs and/or musculature will allow is reached, a sleep test is needed to quantify results.reached, a sleep test is needed to quantify results.
• If indicated, we use the Medibyte portable home If indicated, we use the Medibyte portable home sleep test monitor to quantify results sleep test monitor to quantify results beforebefore referring referring the patient back to their primary care physician or the patient back to their primary care physician or sleep physician for whatever sleep test they deem sleep physician for whatever sleep test they deem necessary.necessary.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
MediByteMediByte®® (Home Sleep Test Portable (Home Sleep Test Portable
Monitor)Monitor)

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
MediByteMediByte® ® HighlightsHighlights
● ● It is the smallest Type 3 recorder in the world It is the smallest Type 3 recorder in the world at 3 x 2.8 x .75 inches. Weighs 3.3 ounces.at 3 x 2.8 x .75 inches. Weighs 3.3 ounces.
● ● It can record up to 12 channels and exceeds It can record up to 12 channels and exceeds the new AASM guidelines.the new AASM guidelines.
● ● On-board pulse oxyimetry, pressure and On-board pulse oxyimetry, pressure and body position sensors eliminate external body position sensors eliminate external transducers.transducers.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Other indications for an OA:Other indications for an OA:1) Use in travel or camping1) Use in travel or camping
2) In 2) In combinationcombination with CPAP: with CPAP:
a) Can advance mandible which allows patient to a) Can advance mandible which allows patient to reducereduce CPAP pressure— CPAP pressure—increasingincreasing compliancecompliance
b) b) No mask or headgear connected to nasal pillowsNo mask or headgear connected to nasal pillows
c) c) Mouth closed so no air will escape (ideal for Mouth closed so no air will escape (ideal for patients who tend to open mouth with CPAP)patients who tend to open mouth with CPAP)

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
What about Medicare? What about Medicare?
• CustomCustom oral appliances are covered under oral appliances are covered under Durable Medical Equipment, Durable Medical Equipment, notnot Medicare Part B. Medicare Part B.
• Most dentists, if they accept Medicare at all, are Most dentists, if they accept Medicare at all, are non-participating DMEPOS suppliers.non-participating DMEPOS suppliers.
● ● Medicare, including supplemental insurance, Medicare, including supplemental insurance, will, on average, reimburse $1321.60. will, on average, reimburse $1321.60. HoweverHowever……
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Medicare issued the following on July 5, Medicare issued the following on July 5, 2012:2012:
Custom fabricated mandibular advancement devices must Custom fabricated mandibular advancement devices must meet all of the criteria below:meet all of the criteria below:
1)1) Have a fixed mechanical hinge (defined as a mechanical Have a fixed mechanical hinge (defined as a mechanical joint containing an inseparable pivot point).joint containing an inseparable pivot point).
2)2) Require no return dental visits beyond the initial 90-day Require no return dental visits beyond the initial 90-day fitting and adjustment period to perform ongoing fitting and adjustment period to perform ongoing modification and adjustments in order to maintain modification and adjustments in order to maintain effectiveness…Items that require adjustments beyond the effectiveness…Items that require adjustments beyond the initial 90-day period are not eligible for classification as initial 90-day period are not eligible for classification as DME. These items are considered as dental therapies, DME. These items are considered as dental therapies, which which are not eligible for reimbursement by Medicareare not eligible for reimbursement by Medicare under the DME benefit. (Effective November 1, 2012?)under the DME benefit. (Effective November 1, 2012?)
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Medicare Limitations of Coverage Medicare Limitations of Coverage and/or Medical Necessity and/or Medical Necessity
The patient must have a Medicare-covered sleep test within The patient must have a Medicare-covered sleep test within the last 3 years that meets either of the following criteria (1 the last 3 years that meets either of the following criteria (1 or 2):or 2):
1) The AHI or RDI is ≥ 15 (moderate or severe sleep apnea) 1) The AHI or RDI is ≥ 15 (moderate or severe sleep apnea) or,or,
2) The AHI or RDI ≥ 5 and ≤ 14 (mild sleep apnea) with a 2) The AHI or RDI ≥ 5 and ≤ 14 (mild sleep apnea) with a minimum of 10 events minimum of 10 events andand documentation of: documentation of:
– a) Excessive daytime sleepiness, impaired cognition, mood a) Excessive daytime sleepiness, impaired cognition, mood disorders, or insomnia, or,disorders, or insomnia, or,
– b) Hypertension, ischemic heart disease, or history of stroke.b) Hypertension, ischemic heart disease, or history of stroke.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Types of Oral Appliances:Types of Oral Appliances:
1) Mandibular advancement or 1) Mandibular advancement or repositioning appliances (or repositioning appliances (or splints or devices)splints or devices)
2) Tongue retaining devices 2) Tongue retaining devices

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
MedicareMedicare Comment Summary of Nov. 11, Comment Summary of Nov. 11, 2010:2010:
CommentComment: There are no randomized, controlled : There are no randomized, controlled crossover trials that show efficacy of any crossover trials that show efficacy of any prefabricated [“boil & bite”] OA. As the literature prefabricated [“boil & bite”] OA. As the literature only supports the use of custom appliances, we only supports the use of custom appliances, we urge the complete removal of the paragraph giving urge the complete removal of the paragraph giving preference to E0485 [prefabricated or “boil & bite” preference to E0485 [prefabricated or “boil & bite” appliances].appliances].
ResponseResponse: Agree. Because of the lack of proven : Agree. Because of the lack of proven efficacy, efficacy, prefabricated appliances will be prefabricated appliances will be denied as not reasonable and necessarydenied as not reasonable and necessary..
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
In an excellent study entitled In an excellent study entitled Comparison of a Comparison of a Custom-made and a Thermoplastic Oral Appliance Custom-made and a Thermoplastic Oral Appliance for the Treatment of Mild Sleep Apneafor the Treatment of Mild Sleep Apnea, ,
Vanderveken, Vanderveken, et alet al concluded concluded: :
““In this study, a custom-made device turned In this study, a custom-made device turned out to be more effective than a out to be more effective than a thermoplastic device in the treatment of thermoplastic device in the treatment of SDB. SDB. Our results suggest that Our results suggest that the the thermoplasticthermoplastic [“boil & bite”][“boil & bite”] device device cannot be recommended as a cannot be recommended as a therapeutic optiontherapeutic option nor can it be used as a nor can it be used as a screening tool to find good candidates for screening tool to find good candidates for mandibular advancement therapy.”mandibular advancement therapy.”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Custom Oral AppliancesCustom Oral AppliancesSomnoDent SomnoDent FusionFusion

Narval Appliance
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
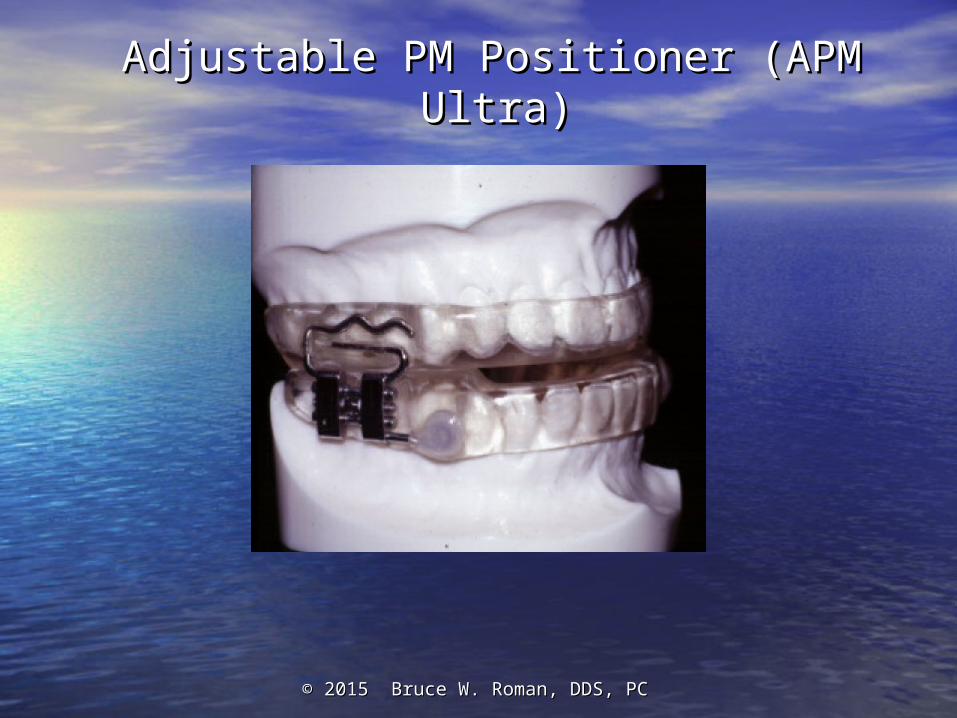
Adjustable PM Positioner (APM Ultra)Adjustable PM Positioner (APM Ultra)

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Elastic Mandibular Advancement Elastic Mandibular Advancement (EMA)(EMA)

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
SUAD DeviceSUAD Device

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
TAP 3TAP 3

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
SomnoDent Herbst SomnoDent Herbst ApplianceAppliance
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
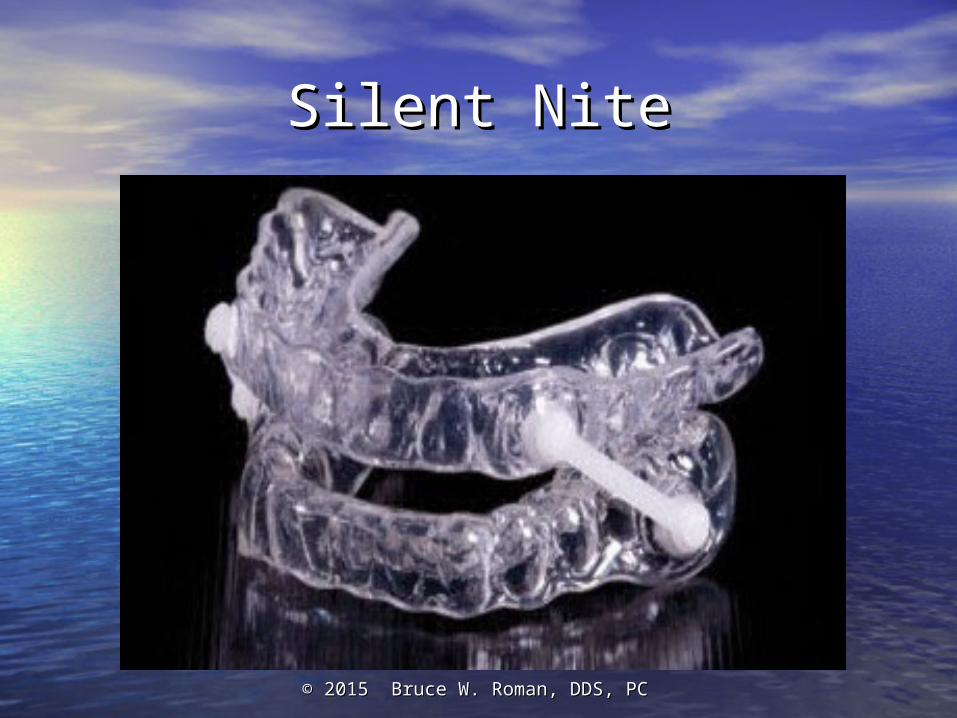
Silent NiteSilent Nite
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
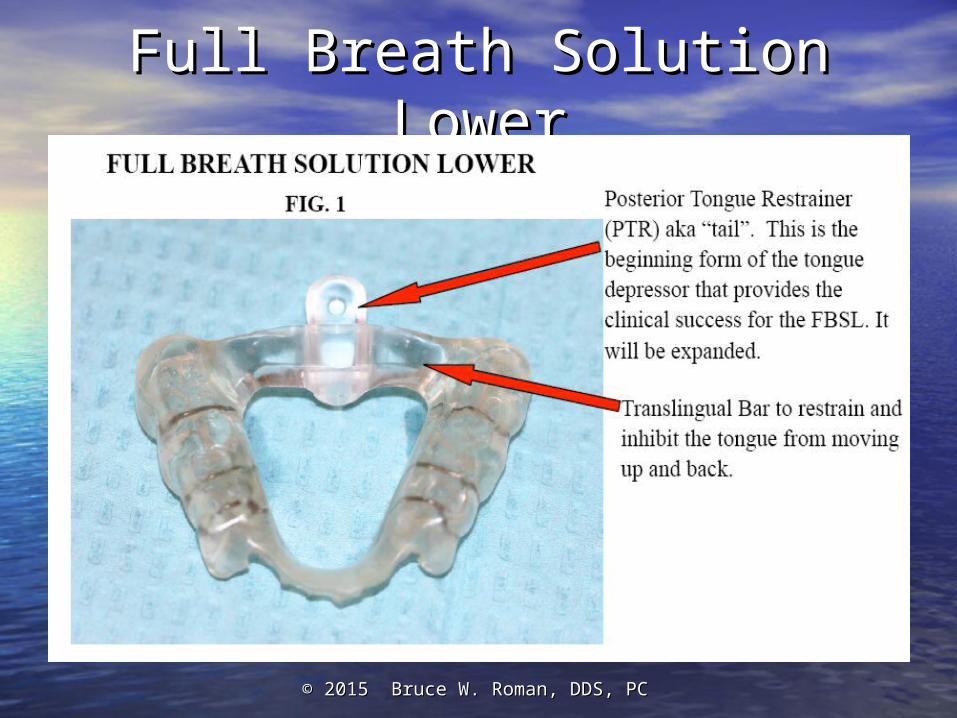
Full Breath Solution LowerFull Breath Solution Lower

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
FBSL with a very small FBSL with a very small “Tail”“Tail”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Mallampati 4 – Closed Mallampati 4 – Closed AirwayAirway

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
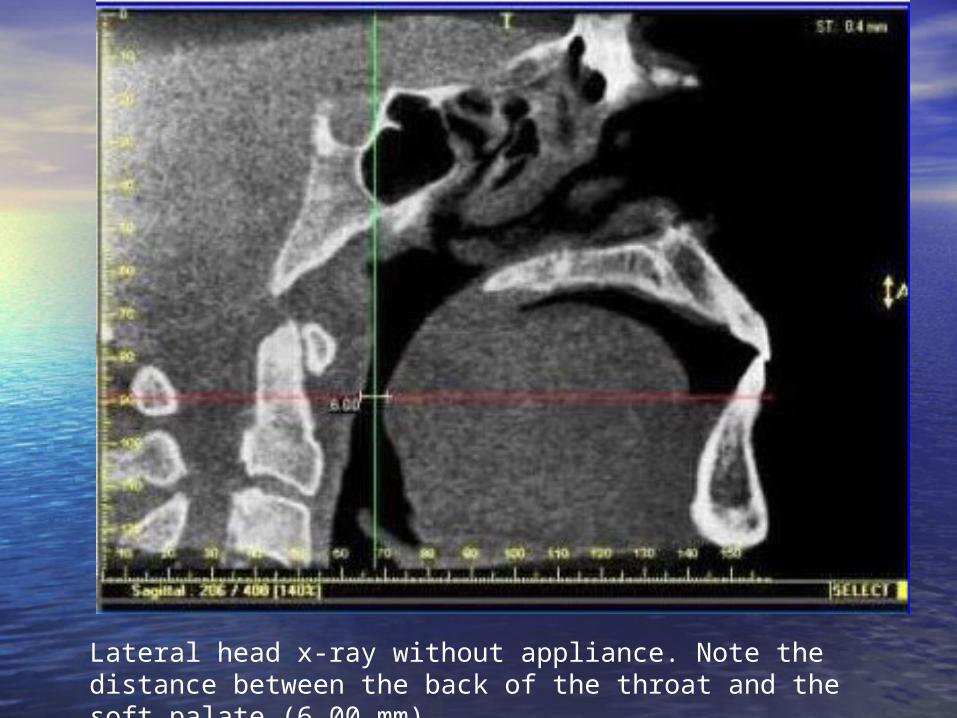
Lateral head x-ray without appliance. Note the distance between the back of the throat and the soft palate (6.00 mm).

Notice the increased distance with the appliance inserted. (The white material you see is the “tail” coated with barium).
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
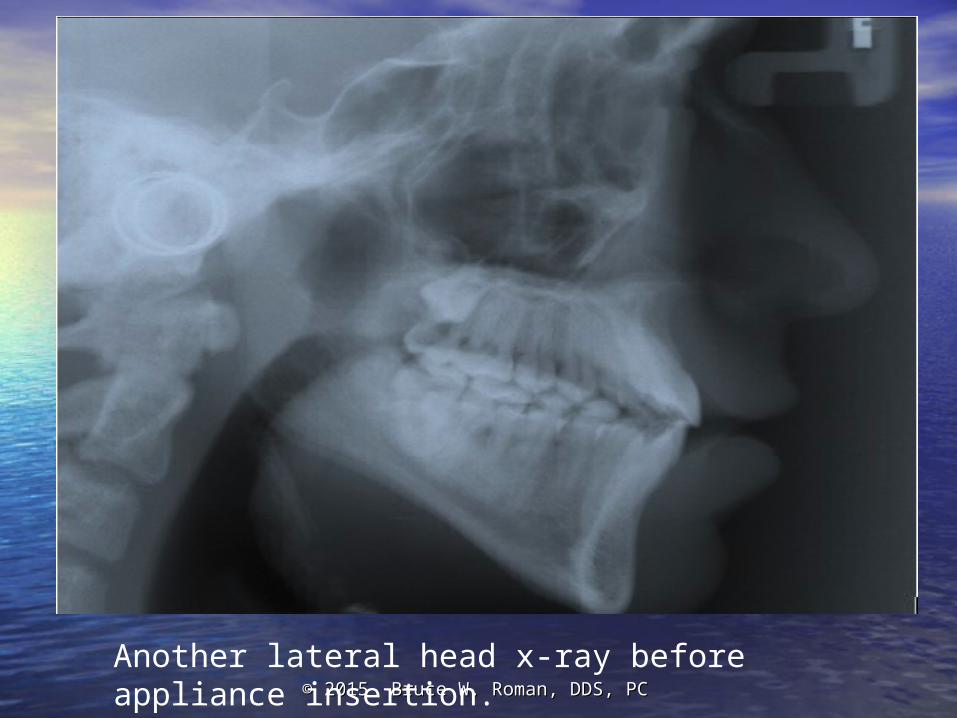
Another lateral head x-ray before appliance insertion.

Same patient with appliance inserted. White squiggly lines are wires in the appliance that help hold it in place.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
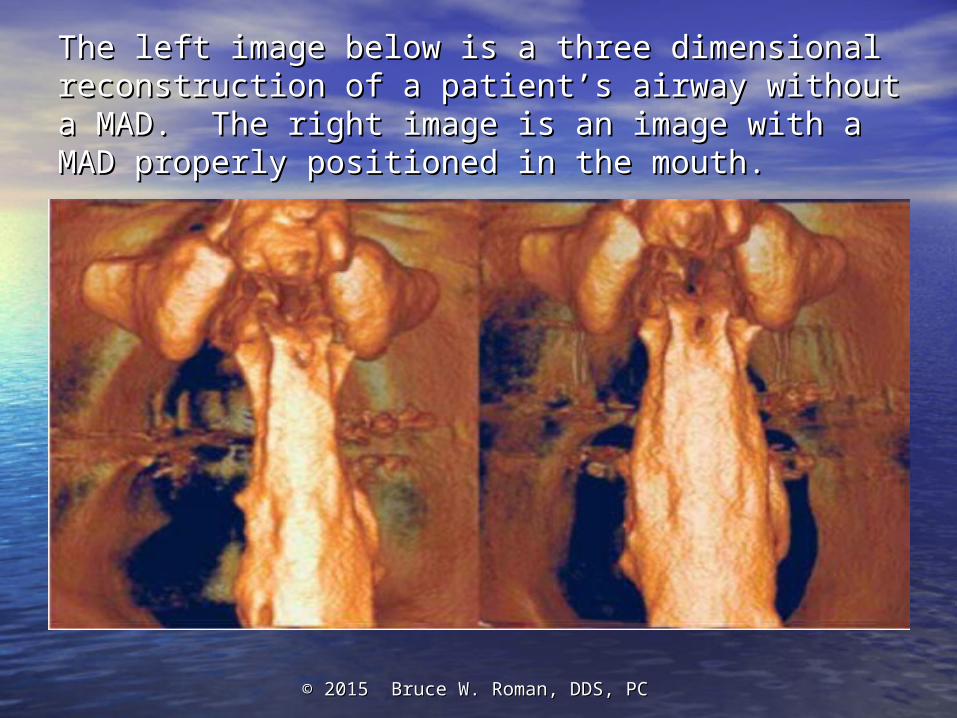
The left image below is a three dimensional The left image below is a three dimensional reconstruction of a patient’s airway without a MAD. reconstruction of a patient’s airway without a MAD. The right image is an image with a MAD properly The right image is an image with a MAD properly positioned in the mouth.positioned in the mouth.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Tongue Retaining Tongue Retaining DevicesDevices
aveoTSD aveoTSD

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
[Original] Tongue Retaining [Original] Tongue Retaining DeviceDevice

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Evaluation for an Oral Evaluation for an Oral Appliance:Appliance:
Sleep Test ReviewSleep Test ReviewThe American Academy of Sleep Medicine The American Academy of Sleep Medicine Clinical Clinical
Guidelines Guidelines states:states:
““The severity of OSA must be established in order to The severity of OSA must be established in order to make an appropriate treatment decision. No clinical make an appropriate treatment decision. No clinical model is recommended to predict severity of model is recommended to predict severity of obstructive sleep apnea, therefore obstructive sleep apnea, therefore objective objective testing is requiredtesting is required. A diagnosis of OSA must be . A diagnosis of OSA must be established by an acceptable method (established by an acceptable method (StandardStandard). ). The two accepted methods of objective testing are The two accepted methods of objective testing are in-laboratory polysomnography (PSG) and home in-laboratory polysomnography (PSG) and home testing with portable monitors (PM).”testing with portable monitors (PM).”

• Chief Complaint addressed and OA Chief Complaint addressed and OA discussion and informationdiscussion and information
• Dental examinationDental examination• Periodontal examinationPeriodontal examination• TMJ examinationTMJ examination
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
After suitability is After suitability is established…established…
1) Diagnostic records: Study models, 1) Diagnostic records: Study models, panoramic or full-mouth x-rays, panoramic or full-mouth x-rays, cephalometric (head) x-ray, cephalometric (head) x-ray, photographs.photographs.
2) Impressions for appliance 2) Impressions for appliance fabrication and a George Gauge bite fabrication and a George Gauge bite registration.registration.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
George Gauge Bite George Gauge Bite RegistrationRegistration
© 2014 Bruce W. Roman, DDS, PC© 2014 Bruce W. Roman, DDS, PC
Delivering the Oral Delivering the Oral ApplianceAppliance
• Once the appliance is received from the Once the appliance is received from the dental lab, it is tried in and adjusted.dental lab, it is tried in and adjusted.
• Directions for its use and care are given. Directions for its use and care are given.
• A normal activation schedule is 1-2 turns A normal activation schedule is 1-2 turns every 3-4 days, while monitoring and every 3-4 days, while monitoring and adjusting that schedule depending upon adjusting that schedule depending upon side effects.side effects.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
How Long Does it Take?How Long Does it Take?
• Usually results are noticed from the next morning Usually results are noticed from the next morning to two weeks. Snoring and excessive daytime to two weeks. Snoring and excessive daytime sleepiness decrease. Bed partners are sleepiness decrease. Bed partners are veryvery happy. happy.
• Over the period of a few months, maximum/ideal Over the period of a few months, maximum/ideal advancement is achieved. However, it can take up advancement is achieved. However, it can take up to 6 months for swelling in the throat tissues to be to 6 months for swelling in the throat tissues to be eliminated. Home sleep tests may be used in the eliminated. Home sleep tests may be used in the interim or even as the final sleep test, depending interim or even as the final sleep test, depending upon the desires of the sleep physician.upon the desires of the sleep physician.
© 2014 Bruce W. Roman, DDS, PC© 2014 Bruce W. Roman, DDS, PC
What is the Dental Team’s What is the Dental Team’s Role?Role?SCREENINGSCREENING----especiallyespecially before: before:
● ● Placing a TMD orthotic.Placing a TMD orthotic.
● ● Removing teeth that would reduce Removing teeth that would reduce tongue space and/or “eliminate” tongue space and/or “eliminate” the possibility of surgery to advance the possibility of surgery to advance the mandible to open up the airway.the mandible to open up the airway.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Aggravation of Respiratory Disturbances by the Use Aggravation of Respiratory Disturbances by the Use of an Occlusal Splint in Apneic Patients: A Pilot of an Occlusal Splint in Apneic Patients: A Pilot StudyStudy (Gagnon, et al., Int J Prosthodont (Gagnon, et al., Int J Prosthodont 2004;17:447-453)2004;17:447-453)
• • ResultsResults: The AHI was increased by more : The AHI was increased by more than 50% in 5 of the 10 patients. The than 50% in 5 of the 10 patients. The percentage of sleeping time with snoring percentage of sleeping time with snoring also increased by 40% with the splint.also increased by 40% with the splint.
• • ConclusionsConclusions: …study suggested that the : …study suggested that the use of an occlusal splint is associated with use of an occlusal splint is associated with the aggravation of respiratory disturbances. the aggravation of respiratory disturbances. It may therefore be relevant for clinicians to It may therefore be relevant for clinicians to question patients about snoring and sleep question patients about snoring and sleep apnea when recommending an occlusal apnea when recommending an occlusal splint.splint.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
How do you “screen”?How do you “screen”?
• • Screening 101Screening 101: Add one sentence to : Add one sentence to your medical history:your medical history:
• • ““Do you snore or have you been told Do you snore or have you been told that you snore?”that you snore?”

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
For the mathematically For the mathematically inclined…inclined…
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Screening 201Screening 201Have patient complete an Have patient complete an Epworth Epworth Sleepiness ScaleSleepiness Scale. If 9 or higher, refer . If 9 or higher, refer to PCP.to PCP.
NoteNote: Males tend to : Males tend to significantlysignificantly under report. Much better to have the under report. Much better to have the bed partner fill it out. bed partner fill it out.

Epworth Sleepiness Epworth Sleepiness ScaleScale• Asks the questionAsks the question: How likely are you to doze off : How likely are you to doze off or fall asleep in the following situations, in contrast or fall asleep in the following situations, in contrast to feeling just tired?to feeling just tired?
This refers to your usual way of life in recent times.This refers to your usual way of life in recent times.
Even if you haven’t done some of these things Even if you haven’t done some of these things recently, try to work out how they would have recently, try to work out how they would have affected you.affected you.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC

Choose the most appropriate number Choose the most appropriate number for each situation:for each situation:
0 = would 0 = would nevernever doze doze
1 = 1 = slight chance slight chance of dozingof dozing
2 = 2 = moderate chance moderate chance of dozingof dozing
3 = 3 = high chance high chance of dozingof dozing
It is important that you answer each It is important that you answer each question as best you can.question as best you can.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
SituationSituation Chance of dozing (0-Chance of dozing (0-
3)3)Sitting and ReadingSitting and Reading ____________________
Watching TVWatching TV ____________________
Sitting, inactive in a public place (e.g., a theatre or a meeting)Sitting, inactive in a public place (e.g., a theatre or a meeting) ____________________
As a passenger in a car for an hour without a breakAs a passenger in a car for an hour without a break ____________________
Lying down to rest in the afternoon when circumstances permitLying down to rest in the afternoon when circumstances permit ____________________
Sitting and talking to someoneSitting and talking to someone ____________________
Sitting quietly after a lunch without alcoholSitting quietly after a lunch without alcohol ____________________
In a car, while stopped for a few minutes in the trafficIn a car, while stopped for a few minutes in the traffic ____________________
TOTALTOTAL ____________________
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC

The Berlin Questionnaire
• While the Epworth Sleepiness Scale is the most widely used questionnaire, it was not specifically designed to identify patients at risk for sleep apnea (it correlates most closely to total sleep time).
• The Berlin Questionnaire was designed to identify patients at risk for sleep apnea but the scoring is a bit more involved. If interested, however, please contact me for more information.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Possible Complications and Side Effects Possible Complications and Side Effects of OA’sof OA’s
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Dental side effects of an oral device to treat Dental side effects of an oral device to treat snoring & OSA, Sleepsnoring & OSA, Sleep, March, 1999, Pantin, , March, 1999, Pantin,
et alet al.:.:
• Excess salivation (30%)Excess salivation (30%)
• TMJ pain (27%)TMJ pain (27%)
• Dental discomfort (27%)Dental discomfort (27%)
• Muscle discomfort (25%)Muscle discomfort (25%)
• Dry mouth (23%)Dry mouth (23%)
• Bite changes (12%)Bite changes (12%)
• TMJ noises (7%)TMJ noises (7%)
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
““Five Years of Sleep Apnea Treatment Five Years of Sleep Apnea Treatment with a MADwith a MAD”, January, 2010, ”, January, 2010, Angle Angle OrthodontistOrthodontist
ConclusionsConclusions::
1) Five-year oral appliance treatment 1) Five-year oral appliance treatment does does not affect TMD [“TMJ”] prevalencenot affect TMD [“TMJ”] prevalence..
2) Is associated with permanent occlusal 2) Is associated with permanent occlusal changes in most sleep apnea patients changes in most sleep apnea patients during the first 2 years. However, this during the first 2 years. However, this tendency reversed 2 years to 5 years.tendency reversed 2 years to 5 years.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Craniofacial Changes After 2 Years Craniofacial Changes After 2 Years of nCPAP Use in Patients with OSA of nCPAP Use in Patients with OSA (Tsuda, et al.; Chest; Oct. 2010)(Tsuda, et al.; Chest; Oct. 2010)
ResultsResults: 1) significant retrusion of the anterior : 1) significant retrusion of the anterior maxilla; 2) setback of the supramentale and chin maxilla; 2) setback of the supramentale and chin positions; 3) retroclination of the maxillary positions; 3) retroclination of the maxillary incisors. (However, none of the patients self-incisors. (However, none of the patients self-reported any permanent change of occlusion or reported any permanent change of occlusion or facial profile).facial profile).
Bottom LineBottom Line: There’s no free lunch with either : There’s no free lunch with either nCPAP or OAs. But treatment of OSA is far more nCPAP or OAs. But treatment of OSA is far more important with either modality than no treatment important with either modality than no treatment in comparison to mostly minor or insignificant in comparison to mostly minor or insignificant changes with both.changes with both.
© 2014 Bruce W. Roman, DDS, PC© 2014 Bruce W. Roman, DDS, PC
What about weight loss?What about weight loss?Effects of dietary weight loss on OSA: a meta-analysisEffects of dietary weight loss on OSA: a meta-analysis, , AnandamAnandam, ,
et al., Sleep Breath, February 29, 2012et al., Sleep Breath, February 29, 2012, concluded: Dietary , concluded: Dietary weight loss programs are effective in reducing the severity of weight loss programs are effective in reducing the severity of OSA but not adequate in relieving all respiratory events. OSA but not adequate in relieving all respiratory events. Weight reduction programs should be considered as adjunct Weight reduction programs should be considered as adjunct rather than curative therapy.rather than curative therapy.
They also found:They also found:
• Patients with mild OSA who gain 10% of body weight are at a Patients with mild OSA who gain 10% of body weight are at a 6X risk of progressing to a higher OSA severity.6X risk of progressing to a higher OSA severity.
• An increase of 10% over time increases the AHI, on average, by An increase of 10% over time increases the AHI, on average, by 30%.30%.
• A 10-15% A 10-15% reductionreduction in body weight can reduce the AHI by 50%. in body weight can reduce the AHI by 50%.

© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Are there any exercises for patients with Are there any exercises for patients with OSA?OSA?
Puhan, Puhan, et alet al., in a ., in a December, 2005 December, 2005 article in the article in the British Medical JournalBritish Medical Journal, , Didgeridoo playing as an alternative Didgeridoo playing as an alternative treatment for OSA, treatment for OSA, showed that regular showed that regular playing (6 days/wk, 25 mins/day for 4 playing (6 days/wk, 25 mins/day for 4 months), reduced the average AHI by months), reduced the average AHI by almost 50% (22.3 to 11.6) and lowered almost 50% (22.3 to 11.6) and lowered the ESS score from 11.8 to 7.4the ESS score from 11.8 to 7.4
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Note: If using for sleep apnea therapy, the headpiece is optional.
© 2015 Bruce W. Roman, DDS, PC© 2015 Bruce W. Roman, DDS, PC
Clinical Asst Professor of MedicineClinical Asst Professor of Medicine, Univ of AZ, , Univ of AZ, Rubin Naiman, Ph. D., saysRubin Naiman, Ph. D., says: : “Learning to play the “Learning to play the didgeridoo is emerging as a surprisingly effective didgeridoo is emerging as a surprisingly effective and practical strategy for managing snoring and and practical strategy for managing snoring and
sleep apnea patients.”sleep apnea patients.”