organizational education for nursing
TRANSCRIPT
1
2011
Organizational Education
for Nursing
This newsletter will help the nursing staff meet the requirements for 2011 Organizational Education for Nursing. The deadline for completion (December 1, 2011) has been communicated through all nursing units and divisions.
It is each nurse’s responsibility to read and understand these topics and apply them as needed.
In order to meet the requirements, the nurse must:
1. Read the newsletter. 2. Follow the instructions based on role in the
organization. 3. Complete the post‐test on Quia (please ask
if you need an explanation for accessing the system).
4. Complete the survey so that the 1.4 contact hours will be added to your education profile the certificate may be awarded.
If you have any additional questions, please contact your supervisor or Pamela Wagner via telephone at extension 35120 or via email at [email protected].
Please keep in mind that this is only a portion of the annual requirements for nursing. Each unit or area may have unit based skills or competencies which need to be completed.

2
Organizational education for Nursing for 2011
The format for Organizational Education for Nurses remains the same as it was this past year. It is being offered through QUIA, a learning management system which will allow you to track your completion and will grade your quizzes without all the worries of making a copy and getting the materials to the right person. All nurses must complete this by the designated time. If you have questions or concerns regarding this process or the content of this newsletter, please contact Pamela Wagner, MSN, RN at telephone number 35120 or via email at [email protected].
Goals and Objectives
Objectives: After reading this newsletter, the nurse should be able to: 1. Verbalize early signs and symptoms of critical illness.2. Discuss the importance of effective communication in caring for the
diverse patient population. 3. Identify the criteria used to determine a hospitals reimbursement for
Value Based Purchasing. 4. Describe the process for obtaining trough levels on patients undergoing
Vancomycin therapy. 5. State the purpose of the Nursing Care Committee.6. Identify appropriate course of action when faced with intimidating or
disruptive behavior. 7. Recall important considerations when administering a blood transfusion.8. Discuss the purpose of the ANA Bill of Rights for Registered Nurses.9. Relate strategies to reduce moral distress in the health care setting.
10. Differentiate performance improvement, research and evidence based practice.
11. Identify the role of the nurse in the management of a patient’s pain.12. Describe the process for obtaining a sterile urine specimen from a patient
with a Urinary Diversion. 13. Identify the nurses’ role in relation to select National Patient Safety Goals.14. Recognize the significance of select medications and a patient’s risk for
falls. 15. 16.
Differentiate truth regarding myths surrounding influenza.Describe Core Measures and their impact on patient outcomes.
Table of Contents
Topic Page Recognition of the Critically Ill 3 ‐ 4 Enhancing Cross‐Cultural Communication in Patient Care 5 ‐ 6 Value Based Purchasing 6IV Vancomycin: Dosing and Monitoring 7Aultman Hospitals Nursing Services Staffing Plan and Nursing Care Committee
8
Conflict Management and Managing Destructive Behavior 9Blood Administration Tips 10 ‐ 11 ANA Bill of Rights for Registered Nurses 11Moral Distress in Healthcare 12 ‐ 13 Understanding the Difference Between PI, EBP, and Research 14Pain: Assessment and Reassessment 15 – 16 Urinary Diversions: Obtaining a Sterile Urine Specimen 17 – 18 National Patient Safety Goals 18 ‐ 21 Influenza Update: Debunking the Myths 21‐23 Medications and Falls 24 – 25 Core Measures 26 ‐ 28

3
Recognition of the Critically Ill Recognizing that a patient is seriously ill is usually not difficult; however, the challenge presented to nurses is recognizing the patient who is in the very early stages of the process. The early identification of patients in trouble allows care providers time to identify the main physiological problem, determine its underlying cause, and implement interventions. The longer the interval between the onset of changes in condition and the appropriate interventions, the more likely it is that the patient’s condition will deteriorate, even to the point of cardiopulmonary arrest. Recognizing the patient at risk Patients seldom deteriorate abruptly, even though care providers may recognize the deterioration suddenly. A number of studies illustrate that early identified abnormal physiological parameters, such as tachypnea, mental status changes, oliguria, or hypotension precede the critical event by more than four hours. Between 50‐84% on in‐hospital cardiac arrests are preceded by unappreciated physiologic instability. Challenges in recognition of the critically ill patient in early stages can be directly related to the patient’s ability to compensate. The young or very fit patient may be much slower to display signs and symptoms of an acute illness than the elderly patient who may have impaired cardiopulmonary function. Additionally, individuals who are immunosuppressed or debilitated may not show an aggressive and clinically obvious inflammatory response. In most patients there exists a balance between the patient’s reserve and the acute disease process. Patients with limited reserve are more likely to experience severe illness and greater degrees of organ‐system failure. Identifying patients at risk of deterioration and planning for potential complications or identifying those patients who are decompensating is crucial in the early intervention process.
Assessing severity “How sick is this patient?” is one of the most important questions a care provider must answer. Measurement of vital signs and other physiologic variables, such as pain, work of breathing, change in mental status, skin tone and color. However, normal vital signs may be early indicators of impending deterioration if they are changed from prior measures. Monitoring your patients vital sign trends allows for early identification that the patient may be deteriorating and directs attention to those aspects of physiology that urgently need treatment. Good clinical skills and a disciplined approach are important in the early recognition of changes in your patient’s status. The framework for assessing the critically ill includes a primary and secondary review and incorporates the patient’s history, assessment, review of vital signs and lab work and implementation of physician orders.

4
Recognition of the Critically Ill (Continued)
Initial primary focus should be on the main physiological problem. Critical illness is often associated with inadequate cardiac output, respiratory compromise, and a depressed level of consciousness. The patient’s history can contribute to the formulation of the diagnosis as you evaluate the circumstances surrounding the patient’s present presentation along with the patient’s past medical/surgical history and current medications.
The initial examination should be brief, focus directed, and concentrate on the basic elements of airway, breathing and oxygenation, circulation, and level of consciousness. Airway and breathing should always be assessed first as tachypnea is the single most important indicator of critical illness and must be accurately measured and documented. Although tachypnea may result from pain or anxiety, it may also reflect pulmonary, systemic, or metabolic abnormalities and should always be fully evaluated. Care providers must be cautious in using the term “anxious.” Patients in respiratory distress will often present early with anxiety or feeling of impending doom. In addition to respiratory rate, evaluation of the patient’s coloring (cyanosis), level of consciousness, work of breathing (use of accessory muscles, rate and depth of respirations), abnormal breath sounds, and oxygen saturation should be evaluated.
Pulse Oximetry is a useful tool; however, this assessment may be unreliable in the presence of hypovolemia, hypotension, or hypothermia. Monitoring trends in oxygen demands (the amount of oxygen the patient is on) in comparison to oxygen saturation can provide early indication of decompensation. For example; the patient who requires increases in FiO2 to maintain a pulse ox of 92% is decompensating.
Inadequate circulation can be a result of abnormalities of the cardiovascular system or secondary abnormalities caused by metabolic disturbances, sepsis, hypoxia, or drugs. A drop in blood pressure may be a late sign of cardiovascular disturbance signaling failure of the compensatory mechanisms. Look for reduced peripheral perfusion, altered level of consciousness, dyspnea, decreased urine output, and JVD in addition to auscultation of abnormal heart sounds.
In low‐flow states or hypotension, the brain and heart will attempt to maintain perfusion by shunting blood to the vital organs. The brain is one of the most sensitive organs to changes in perfusion. As CNS perfusion decreases the patient’s mental status will go through the stages of anxiety, apathy, lethargy, stupor, and eventually coma. Changes in mental status, accompanied by signs of respiratory compromise or hypoperfusion are serious indicators of decompensation.
Translating information into action Failure to recognize changes in a patient’s condition until major complications, including death, have occurred is referred to as failure to rescue. Failure to rescue is based on the premise that although deaths in hospitals are sometimes unavoidable, many can be prevented. Three fundamental problems lead to failure to rescue:
1) Breakdown in communication between caregivers (nurse to nurse, nurse to physician, physician to physician);
2) Failure to recognize early signs of deterioration; 3) Incomplete assessments.
Early identification of patients at risk is the most important solution to improving patient outcomes and the bedside nurse is often the first to detect early signs of possible complications. Judicious attention involves assessing patients frequently, attending to cues, and recognizing complications; documenting your findings is imperative in order to monitor trends. Taking action, when patients have changes in condition, involves quickly instituting appropriate measures and activating a team response.
Nurses at Aultman Hospital are empowered to exert control over the situation to assure such actions are taken. Primary care physicians should be notified early of changes in patient condition and this notification should be documented. The triggers for calling the Rapid Response Team (RRT) are very liberal, with a firm foundation to “Call Early and Call Often.” The concept of RRT focuses on preventing patient crisis by addressing changes in the patient’s status before cardiopulmonary arrest occurs. These team members can efficiently recognize, assess, and stabilize the patient while working with the primary nurse and patient’s physician.

5
Enhancing Cross‐Cultural Communication in Patient Care
Communication is the product of culture, thus the ability for health care professionals to provide culturally competent care strongly depends on the capability to communicate effectively with diverse groups (Rohini Anand, 2006). Addressing the specific needs of diverse groups requires awareness, knowledge and skills necessary for developing enhanced communication skills.
Dr. Micheal S. Woods, M.D. states, “The world is a small place, and the smaller it gets, the more important it becomes that we understand each other.” According to the American Medical Association, the U.S. population is growing older and more diverse. Health care providers are seeing patients from diverse socio‐cultural backgrounds; and patients are seeing more nurses, administrators and doctors from varied cultural backgrounds as well (Ursula Leitzmann, 2011). The white population is older and centered around aging baby‐boomers, while the number of young people is declining. By 2050, America’s three largest minority populations; Hispanic‐Americans, African‐Americans, and Asian‐Americans, will more than likely double in size; an increase in ethnic groups that is largely due to immigration, and higher birth rates among minorities (Cosgrove‐Mather, Washington 2004 ).
Culture, life experiences and traditions can influence and determine characteristics of communication such as the tone of voice; topics that are considered appropriate or inappropriate; how far to stand when participating in a discussion; and more. Consequently, culture shapes responses to illness and treatment. Throughout childhood, people learn how to: 1) Label the experience of illness; 2) Express conditions; 3) Make the distinction between normal and abnormal states.
Diverse health beliefs of patients with a cultural imprint different from that of the providers may affect the diagnosis, treatment and overall health outcome. Caregivers should view each encounter as an opportunity to express mutual empathy and understanding for the patient; reconcile with existing health care practices and provide extended education (Ursala Leitzmann, 2011).
Health care workers and patients with different cultural norms are at risk if managers, co‐workers, or providers have little knowledge of and sensitivity to different communication styles. Developing sensitivity to communicating for
understanding compels providers to make the necessary paradigm shift from the biological focus; something easier said than done considering the pressures, regulations and paperwork required of health care professionals (Rohini Anand, 2006).
It is not surprising to hear that most conflicts and resolutions, in the health care workplace, involve communication. Some of the barriers of effective cross‐cultural communication include assumed similarity, nonverbal communication, language itself, the tendency to evaluate, and preconceptions and stereotypes (Rohini Anand, 2006).
In an attempt to improve communication in health care, Dr. Paul Schyve, M.D., senior vice president, The Joint Commission, stated in an August 4, 2010 press release, “Effective Communication, cultural competence, and patient‐ and family‐centered care are not stand‐alone initiatives. A hospital must embed these practices in the core activities of its system of care delivery to truly meet the needs of the patients, families, and the communities served. According to The Joint Commission, improving communication effectiveness and adapting communication styles will be required for compliance with patient‐centered care.”
Tips for Enhancing Communication Skills and Bridging Cross‐Cultural Communication Barriers (Rohini Anand, 2006)
◦ Self‐Awareness ◦ Establish trust and show concern and empathy
◦ Consciously decide not to act on our own stereotypes and assumptions
◦ Show sensitivity to face‐saving needs
◦ Listen with respect ◦ Have a sense of humor and patience
◦ Increase culture‐specific awareness
◦ Be aware of nonverbal messages
◦ Treat each person uniquely ◦ Listen intently for hidden meanings
◦ Seek out information ◦ Avoid language with questionable connotations
◦ Tolerate ambiguity ◦ Walk in the other person’s shoes

6
Enhancing Cross‐Cultural Communication in Patient Care (Continued)
Helpful Website Links
http://www.diversityRX.org
http://www.jointcommission.org/multimedia/improving‐patient‐provider‐
communication‐‐‐part‐1‐of‐4/
http://gucchd.georgetown.edu/nccc
http://www.fanlight.com/catalog/films/912
http://medethicsfilms.stanford.edu/worldsapart/
Value Based Purchasing
The Health Care Reform Law of 2010 known as the Patient Protection and Affordable Care Act requires the establishment of a Value Based Purchasing (VBP) Program. Although the final rules for this multi pronged program have not yet been released by the Centers for Medicare and Medicaid (CMS), hospitals are gearing up for its implementation by the end of 2011. It is known that hospitals will be reimbursed for services based on Core Measures and Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Scores. Core Measures were introduced in 2005 by CMS and focus on process of care with a concentration in Heart Attack, Heart Failure, Pneumonia and Surgical Care while HCAHPS Hospital Survey, established in 2006, is a measurement of patient perception and patient satisfaction. The outcomes of both Core Measures and HCAHPS are publically reported and available on the HospitalCompare.hhs.gov website.
Ultimately, VBP incentivizes hospitals to improve. Payment will be withheld by CMS if a hospital does not perform at an established level. Please make every effort to comply with the standards for Core Measures and to offer our patients a satisfying experience. More information will be provided as it becomes known.
There’s More in StoreCMS’ Quality‐based Payment Initiatives Will Put 7% of Payment at Risk
2010 2011 2012 2013 2014 2015 2016 2017
Reporting Hospital Quality Data for Annual Payment Update 2% of APU
Meaningful Use 1%
Hospital Acquired Conditions Hospital Acquired Conditions 1%
Value-based Purchasing 2%VBP
Readmissions 3%
Source: Partners JAN/FEB 2011
Projected Look at Value Based Pricing

7
IV Vancomycin: Dosing and Monitoring
Background Vancomycin is one of the few available antibiotics that is effective
against MRSA and other difficult to treat bacteria. Since it may be used against such powerful bacteria, it is important to ensure that it reaches high enough concentrations to completely eliminate the bacteria. If sub‐optimal levels of vancomycin are reached, there is an increased risk of developing vancomycin resistance. Vancomycin is not a benign drug however, as it can cause Red Man’s Syndrome (due to a short infusion time) and renal and ototoxicity if too much is given.
Dosing Vancomycin is dosed based on weight, renal function, and severity of
infection. A typical dose is 15‐20mg/kg of ACTUAL body weight to ensure proper tissue penetration. A current or recent weight is therefore required to initiate therapy in most patients. A patient with normal renal function will require a dosing frequency of 12 hours. Patients with renal insufficiency (whether new or chronic) will require less frequent dosing in order to prevent accumulation and toxicity. Since renal toxicity can be a side effect of receiving vancomycin, it is important for health care professionals to be alert to any signs or symptoms of worsening renal function as this could be an early sign of toxicity and may require vancomycin dose adjustments.
In some patient populations such as in the setting of pregnancy or obesity, more frequent administration may be required to achieve optimal levels and doses of 10mg/kg every 8 hours may be used.
Monitoring Due to its relatively narrow therapeutic window, vancomycin trough
levels are often drawn in patients who will be receiving vancomycin therapy for greater than 72 hours. Peak levels are rarely drawn, despite being popular in the past, as they have not been shown to be clinically useful when compared to trough levels. In order to be a true trough, the blood must be taken 30 minutes or immediately prior to administration of a dose after steady state is reached. Steady state is the point when vancomycin concentrations in the blood are constant. Steady state is a pharmacokinetic term that is calculated to occur
after 5 half‐lives. Since the half‐life of vancomycin is 5‐11 hours in patients with normal renal function, vancomycin steady state occurs after 25‐55 hours. A steady‐state (true) trough can therefore be drawn in most patients before the 3rd (hour 36) or 4th dose (hour 48). A level that is drawn when the levels are not at steady state or taken too early or too late will not be an accurate reflection of the actual trough concentration. Many times that means a second trough level must be drawn to ensure optimal levels. The additional blood draw causes undue stress on the patient, added costs, and potentially a delay in therapy.
Ensuring the proper timing for vancomycin troughs is a multi‐disciplinary responsibility. Physicians need to write the order properly, lab needs to be notified of the correct time for the draw, pharmacy needs to schedule the doses properly to line up with the lab draw, and nursing needs to administer vancomycin doses on time. If a delay occurs, if the dose gets rescheduled, or if a change of dose (increased or decreased) occurs without rescheduling the trough level accordingly, the level may not be accurate or useful when it comes back.
Goal trough levels depend on the treatment indication but are typically in the 10‐20 mg/L range. True troughs that are >20 mg/L can lead to unwanted side effects, accumulation, and toxicity and will require an adjustment in either dose or frequency. True troughs <10 mg/L may put the patient at risk of inadequate drug penetration to the infected site and may lead to treatment failure or the development of drug resistance. Wrap‐up
Nursing, pharmacy, prescribers, and lab all have to work together to ensure proper timing of vancomycin levels to protect the patient from treatment failures or toxicities. Pharmacists are available to assist with dosing and trough level questions with just a phone call to pharmacy.

8
Aultman Hospital Nursing Services Staffing Plan and Nursing Care Committee
The Nursing Care Committee was formed in response to Ohio’s Common Sense Safe Staffing Law (HB 346) that was signed into law in June, 2008. This law affects inpatient areas, including the Operating Room. It requires that the Chief Nursing Officer (CNO) establish a mechanism for obtaining input regarding staffing from all nurses who provide direct care. It also mandates that the hospital must post, in a conspicuous location, a hospital sign informing the public of the staffing plan and how to obtain a copy of it.
Our Nursing Care Committee is comprised of 14 hospital employees: 57 % of them are direct care providers who represent inpatient, Emergency Department and the Operating Room. The remaining members of the Committee are administrative representatives. The Law requires that the committee review the staffing plan at least one time per year and that the plan is consistent with:
1. Centers for Medicare & Medicaid (CMS) Condition of Participation: Nursing Services (482.23) 2. American Nurses’ Association Principles for Nursing Staffing 3. Other standards established by private accreditation organizations or governmental entities to
ensure safe, quality nursing care
The Nursing Services Staffing plan is accessible on the Aultman Health Foundation Intranet via the Knowledge Management tab: http://sharepoint/Aultman/Documents/Nursing%20Policy%20&%20Procedures/General%20Nursing/Nursing%20Services%20‐%20Staffing%20Plan.doc
Additionally, the Committee selects at least two nurse sensitive indicators to monitor related to staffing each year.
A summary of the Committee Activities in 2010 includes:
o Developed Position Statement encouraging RNs to take breaks o Supported staffing based on acuity / Staffing Acronym:
V: Volume (the number of patients requiring nursing care)
A: Acuity (the complexity of care each patient requires)
C: Competency (the level of experience of each nurse)
AULTMAN HOSPITAL NURSING CARE COMMITTEE MEMBERS
Direct Care Nurse Experts Erin Meek, BSN, RN, OCN Med Surg
Jennifer Lindgren, RN Med Surg
Beth Phillips, BSN, RN‐BC Critical Care
Justin Hamilton, RN Critical Care
Dana Kiefer, BSN, RN Step Down
Stacy Ripple, BSN, RN‐BC Step Down
Susan Mayle, RN Heart Services
Amy Good, BSN, R, CNOR Operating Room
Nancy Kane, BSN, RN Perinatal and Pediatrics
Miranda Parker, RN Perinatal and Pediatrics
Stacie Howard‐Carpenter, MHA, RN, CEN
Emergency
Molly Gerber, BSN, RN, CEN Emergency
Diane Limbach, RN LTACH
Nichole Quinn, RN LTACH
Carrie Cassidy, RN Rehabilitation
Pam Tapp, RN, C Psychiatric Nursing
Administrative Representatives
Tina Biasella, MSN, RN, AVPWendy Gotschall, MSN, RN, NE‐BC, VPAnne Gunther, MSN, RN, NE‐BC, CNO
Sue Olivera, MBA, VPSara Reich, BSN, RN, Unit Director
Mark Wright, MBA, CFO
Ex Officio Member: Susan Cutshall, RN, Unit Director: Staffing and Scheduling
Meeting Recorder: Shelley Johnson, MBA, RN, Staffing Office

9
Conflict Management and Managing Disruptive Behavior
Conflict is inevitable; how you manage it can determine if it is beneficial or destructive. There is no one best way to deal with conflict. The Major ways people tend to deal with conflict include:
1. Avoidance: Pretending it is not there or ignoring it. This approach works best when the issue is not important to you but keep in mind that it may make the conflict worse over time.
2. Accommodation: Giving in to others, sometimes to the extent that you compromise yourself. Do not use this technique at the expense of compromising your values.
3. Competition: Working to get your way, rather than clarifying and addressing the issue. 4. Compromise: Giving and taking on both parties parts; helps to get past the issue and move on. 5. Collaboration: Focusing on working together; increases ownership and commitment for both
parties.
Steps to Conflict Resolution
€ Define the Conflict € Express facts and feelings regarding the conflict € List all possible solutions € Decide on a mutual solution € Implement € Evaluate
Managing conflict creates constructive behavior which positively impacts the team… the healthcare team… and the patient.
Behaviors that Undermine a Culture of Safety
• Intimidating and Disruptive Behaviors can: – Foster medical errors – Contribute to poor patient satisfaction – Lead to preventable adverse outcomes – Cause qualified health team members to leave the System
• Safety and Quality of patient care are dependent on: – Teamwork – Communication – Collaboration
Intimidating and Disruptive BehaviorThis is defined as “verbal outburst and physical threats, as well as passive activities such as refusing to perform assigned tasks or quietly exhibiting uncooperative behavior during routine activities.” It can be exhibited by Health Care Professionals in positions of power. Reporting Process within the Foundation Nurses or other hospital employees who observe or are subjected to inappropriate conduct by a practitioner shall do the following: 1. Report the incident to their supervisor. 2. Enter a variance report directly into the
MIDAS system.
Essential Elements of the Health Care Team
€ Communication € Collaboration € Conflict Management € Respect € Zero Tolerance for Disruptive Behavior

10
Blood Administration Tips “Elimination of transfusion errors remains the number one goal on the Joint Commission’s list of National Patient Safety Goals. The College of American Pathology has reported that the most common transfusion safety violations among healthcare systems involve transfusion reaction recognition and annual education in the recognition of transfusion reactions. There is no doubt that nurses must be able to recognize and act on early signs of an adverse event, and that it is dangerous to fail to respond to signs and symptoms of an adverse event. The transfusing nurse is responsible for diligent patient monitoring and assessment throughout the infusion of blood products because transfusion related complications are serious risks of blood administration and major contributors to transfusion associated morbidity and mortality.” 1 Blood administration has the potential to be a hazardous procedure. Existing and emerging evidence compels nurses to recognize and understand that a blood transfusion is a cellular transplant which may cause more harm than good. Blood products should be administered with the same regard and caution as high risk medications. Just as nurses must know the five rights of medication administration, nurses who administer blood products must know the clinical indication, appropriate dose, expected benefit and risks of transfusion therapy for the patient receiving the transfusion. The following tips were written to aid the transfusionist in understanding the importance of all steps within the transfusion process to improve patient outcomes and safety.
• Verify there is an order to transfuse blood products. Physicians may order “type and cross match 2 units of packed red cells” compared to an order to “administer/transfuse 2 units of packed red cells”. The first order is an order for blood bank to prepare two units (should the transfusion be needed in the future). The second order is to actually administer the blood product.
• Evaluate the patient’s need for a blood product. Think “are the lab results and patient symptoms consistent with the need for a transfusion”. If the rationale is unclear, clarify the order with the ordering physician.
• Verify that there is a signed informed consent in the chart prior to administration of the blood products. The ordering physician is required to discuss with the patient the benefits, risks and possible alternatives to a blood transfusion and obtain the patient’s consent for a transfusion.
• Verify the blood sample used for the Type and Screen was drawn within three days of the infusion. The draw date is considered day 0.
• Monitor and record pre‐infusion vital signs including temperature, pulse, respirations and blood pressure within 60 minutes of the start of the infusion.
• Start IV line if not already present using normal saline. Use Y‐type Blood / Solution Set tubing.
• Pre‐transfusion medications are to be administered prior to receiving the blood product:
o Oral medications are to be administered 30‐60 minutes prior to initiation of the infusion
o IV medications are to be administered 10 minutes prior to initiation.
• Retrieve blood product from Blood Bank. A patient identification label is required and the person retrieving the blood is responsible for verifying all information on the Blood Bank unit and sign out log with a Blood Bank staff member. IF THERE IS AN UNEXPECTED DELAY WITH THE INITIATION OF THE TRANSFUSION, THE BLOOD MUST BE RETURNED TO THE BLOOD BANK WITHIN 30 MINUTES OF THE TIME OF ISSUE. Delays in starting a blood transfusion facilitate bacterial growth.
• Visually check the product and perform bedside patient identification with two individuals. Investigate and correct any discrepancies before blood is administered.
• After initiation of the transfusion, the nurse must stay with the patient for the first five minutes of the transfusion to observe the patient for adverse reactions. Adverse reactions most commonly occur within the first 15 minutes of a transfusion.
• Vital signs are to be monitored and documented as follows: o Pre‐transfusion (recommended within 60 minutes of start of
transfusion) o At 15 minutes after initiation of transfusion o At completion of transfusion o One hour after completion of transfusion
Note: Observe for reactions and document in the medical record every 30 minutes during the transfusion until it is completed.

Blood A
• Ta
o o o o o o o
• I
ptu
• Lgc
• Tm
These bloadministprocedur
Au
Administration T
There are many tyadministration of
Fever Lower back pain Tightness in chesChills Neck Vein DistenHypotension Headache
f a transfusion reaphysician and the to follow the procunit to blood bankLate/delayed reacgreater than 48 hochanges in health The Transfusion Cmonitoring.
ood administratiotration. Refer to re details.
ultman North
Tips (continued)
ypes of potential tthe products. Ob
Possible o N
o Rst o A
o Cntion o P
o Uo Do Lo
action is suspecteblood bank at extedure for a Transk along with the IVctions may go undours after the tranto their physicianommittee is respo
on tips are not tothe hospital’s blo
Aultm
transfusion reactioserve the patient
Symptoms of a RNausea and VomitRash Abdominal PainConvulsionsruritis
Urticaria/ HivesDyspneaoss of Consciousn
d, immediately stt. 36314. Complefusion Reaction inV tubing. etected for days, nsfusion. Upon din. onsible for blood a
o be used as a repood administratio
man West
ons that are detecfor symptoms of
eactionting o
oooooo
ness
op the transfusionete the transfusionncluding sending t
weeks or months scharge, instruct t
administration po
placement guide on policy on Share
West Tu 11
cted during the eaa transfusion reac
MalaiseConfusionHematuriaSkill PallorPerspirationOozing from woJaundice
n and notify the n reaction form. Bthe remainder of t
and generally occthe patient to rep
olicy requirements
for blood epoint for compl
usc Dialysis
arly ction:
ound
Be sure the
cur port any
s and
ete
The Regiand concnece The usedand/empcan and
American Nursesistered Nurses is approved by pracerning workplacessary for safe, so
ANA Bill of Rightsd to guide deve/or to guide ployers. Some of thelp address are safety issues such
A
1. Nurses have fulfills their oreceive nursin
2. Nurses have that allow professional scopes of pra
3. Nurses have supports anaccordance wInterpretive S
4. Nurses haveadvocate fowithout fear
5. Nurses have their work, experience an
6. Nurses have is safe for the
7. Nurses have of their emcollectively, i
The ANA Bill o
s Association (ANa document dev
acticing nurses. It ce expectations und professional
s is not a legal docelopment of orgdiscussions betthe issues that thunsafe staffing, m
h as workplace vio
ANA Bill of Rights
the right to practobligations to socieng care. the right to practhem to act istandards and
actice. the right to a wond facilitates ewith the Code of EStatements. e the right to or themselves aof retribution. the right to faconsistent with
nd professional rethe right to a woemselves and for tthe right to nego
mployment, eithen all practice setti
f Rights for Regis
NA) Bill of Rights veloped, deliberatincludes 7 premand environme
nursing practice.
cument, but it mayganizational politween nurses he ANA Bill of Rigmandatory overtiolence.
s
tice in a manner tety and to those w
tice in environmen accordance wlegally authori
ork environment tethical practice, Ethics for Nurses w
freely and opeand their patie
ir compensation h their knowledesponsibilities. ork environment ttheir patients. otiate the conditier as individuals ings.
stered Nurses
for ted, ises ents
y be cies and ghts me,
that who
ents with ized
that in
with
enly nts,
for dge,
that
ions or
12
Moral Distress in Healthcare Being involved in the delivery of patient care can be empowering; we ease pain, heal illness and injury, fight the fight against disease processes, and save lives. There are times when, as direct caregivers, we may be the ones who know what is best for our patients. However, are there times when you feel powerless because what you feel is best is not what is being done?
This feeling of powerlessness is a phenomenon known as moral distress. In 1984, Andrew Jameton defined moral distress as a psychological disequilibrium that occurs when one knows the right action to take, but is constrained from taking it. As a result of internal or external constraints, we may be required to act in a manner contrary to our personal and professional values.
Today’s acute care environment presents us with many difficult situations that may cause moral distress and negatively impact the healthcare environment. Redman (2000) found 1 in 3 nurses experience moral distress and Coreley (2002) found 15% to 26% of nurses will leave the profession due to moral distress. Nearly all health care professions, not just nursing, can experience moral distress including, but not limited to, respiratory therapists, dieticians, social workers and case managers. Important consequences can ensue, including stress, burnout, job dissatisfaction, and departure from the health care field.
Situations that cause moral distress vary among health care providers just as values and obligations are individually interpreted. Sources of moral distress may be personal, interpersonal, and/or environmental. Commonly cited sources include conflicts between the nurse and physician, the feeling of lack of support, lack of competency, work place violence (including bullying), ethical dilemmas and resource constraints (including staffing and lack of equipment). End of life challenges, including futility of care, is often a main source of moral distress for the health care provider.
Recognizing moral distress is an important step towards resolution, however; many health care providers are unaware how it is manifested. Moral distress often involves feelings of frustration and anger, which are easily recognized and may be labeled as emotional distress. However, under the surface, and more difficult to identify, are the feelings that threaten one’s moral integrity; such as feeling belittled, unimportant, or unintelligent. Moral integrity, as described by Hardingham (2004), is a sense of wholeness and self‐worth that comes from having clearly defined values that are congruent with one’s actions and perceptions.
In the health care environment, situations that result in moral distress can result in poor communication, lack of trust, high turnover rates, defensiveness, and lack of collaboration across the disciplines. It can also affect relationships with patients and families and impact the quality and cost of health care.
Moral distress can however lead to a positive change, creating an environment where we can make our optimal contributions to the organization and the patients and families that we serve. However, we must be able to recognize and name the experience of moral distress, affirm our professional obligation to act and commit to addressing moral distress, and be knowledgeable about and use professional and organizational resources to address the issue of moral distress. Many professional organizations, such as American Association of Critical Care Nurses (AACN), American Nurses Association (ANA), and International Council of Nurses, have developed position statements and tools to address moral distress.
Several strategies to reduce moral distress have been published. The AACN (2005) has developed the 4 A’s approach to address and reduce moral distress that is applicable to all disciplines. This change process is cyclic and includes Ask, Affirm, Assess, and Act.

13
Situations of moral distress are inevitable in the day to day setting of the healthcare field. Putting aside and not recognizing or addressing moral distress can result in the lingering of individual symptoms for those experiencing moral distress – a phenomenon described as moral residue.
Moral residue is long‐lasting and powerfully integrated into one’s thoughts and views of self over time. Intervening to address moral distress has several goals: First, it allows us to recognize its existence in the healthcare field. Second, it reduces the threat to our moral integrity. Third, it provides a voice to address the issues, be recognized, valued, and heard. Finally, increasing awareness and addressing moral distress preserves moral sensitivity and integrity among healthcare providers leading to healthy work environment and retention of skilled care providers.
A healthy work environment is everyone’s responsibility. Your unit based council can identify potential causes of moral distress and collaborate to find solutions to these challenges. Unit Managers can provide you with links to debriefing services, ethics committee, grief counseling, and the employee assistance program
ASK: Self awareness of distress
- Am I feeling distressed or am I suffering
- Am I observing distress from any of my peers?
Goal: You become aware that moral distress is
ACT
• Prepare to act: develop a self care plan and look at your Internal and External resources
• Take action: Implement strategies for desired change; Speak up; Be deliberate; Be accountable; Educate!
• Maintain desired change
Goal: Preserve your integrity and authenticity
ASSESS
• Identify sources of your distress: are they personal? Environmental? Both?
• Determine the severity of your distress: 0 = None to 5 = Severe
• Contemplate your readiness to act: Risk versus Benefits; Focus to Decrease risk not to increase benefits
Goal: You are ready to make an action plan
AFFIRM
• Affirm your distress & commitment to take care of yourself & your peers
• Validate feelings and perceptions with others
• Affirm professional obligation to act
Goal: You make a commitment to address
Creation of a healthy work environment where care
providers make their optimal contributions
Adapted from AACN (2005) 4As to Rise Above Moral Distress. Downloaded from www.AACN.org
through our Health Services

PI Performaissue wiimplemeoutcomeimproved
EBP Evidence(EBP) conpractice wgroundedand/or retions fromorganizatproblem/already bavailable journals apolicies a
ResearchResearchgenerateknowledgresearch proposal approvedInstitutioBoard (IRAultman The purphuman re
The CharinteresteAultman.
Und
ance Improvementh poor outcomnted (preferably s are measuredd, deteriorated, or
‐based Practice nsists of which is d in research ecommenda‐m professional tions. The /issue has been researched aby doing a literatand academic resoat Aultman Hospit
h h produces or s new ge. A key to is that the must be d by an onal Review RB) which at is called the Hum
pose of the IRB is tesearch subjects.
t to the right detad in conducting a .
derstanding the
nt (PI) is usually inmes. A process
based on evidd to see if pr stayed the same
and this conclusiveture search of peeources. All nursinal should be evide
an Research Revieto protect the righ
ails the steps to tanursing research
e Difference Bet
nitiated due to anchange is then
dence) and thenperformance has.
e evidence is er‐reviewed ng practice and ence based.
ew Board (HRRB).hts and welfare of
ke if you are study at
tween Perform
Contact the Research Dep
Seek Nursing Research C
Approv
Present to Research Reve
for Appr
14
ance Improvem
Nursing partment
•Comcertif•Com•Makeemai
Quality & Council val
•ContNurs•Atten•ObtaCoundocu
Human eiw Board roval
•Contemai•Mail emai•Onceinitia
ment, Evidence‐
plete the National ficate (http://phrpplete Human Resee an appointment iling NursingResea
tact the Chair of thingResearch@aultnd a Q & R Councilain complete Nursinncil and submit it touments
tact the chair of theiling ClinicalResearor email completeil or by sending to: e approval has beeated and conducted
‐based Practice
Institute of Health.nihtraining.com)arch Revew (HRRBfor assistance or [email protected]
e Nursing Quality aman.com and requ meeting to presenng Scientific Merit o the HRRB along w
e Aultman HRRB [email protected] documents to th Clinical Research n obtained from thd
and Research
h Investigator Tuto
B) formso review complete
m
and Research Counuest to be placed ont research study pReview Form fromwith other complet
o be placed on the comhe HRRB by attachiDepartmenthe HRRB, the resea
rial and submit
d HRRB forms by
ncil via email at on the agenda proposalm the Q & R ted HRRB
agenda by
ng to the above
arch study can be
15
Pain: Assessment and Re‐Assessment
In an effort to move pain to the forefront in the care of patients it has been considered “the fifth vital sign” and has been on the radar of Joint Commission for many years. Pain is physical: disease, injury and infection may cause tissue and nerve damage which is responsible for pain. Pain is emotional: factors such as trauma, stress, anxiety and depression can play a part in a patient’s pain. The pain management standards address the assessment and management of pain. The standards require organizations to:
• Recognize the right of patients to appropriate assessment and management of pain
• Screen patients for pain during their initial assessment and, when clinically required, during ongoing, periodic re‐assessments
• Educate patients suffering from pain and their families about pain management
Both pharmacologic and non‐pharmacologic methods are to be considered for use in the management of pain. Pain is also assessed and reassessed as a component of post procedure monitoring. According to hospital policy, patients should be assessed for pain during their initial assessment, when pain is initially reported, when there is a change in site, or change in type, and there is an intervention for pain. This assessment data documentation should include:
Pain Assessment
Type Aggravating Factors Impact on ADL’s
Intensity Associated Symptoms Patients Acceptable
Goal or intensity
Quality Alleviating Factors
This screening, comprehensive assessment, and documentation are to be performed by authorized personnel. RN’s can screen, assess, and document for the presence of pain while LPN’s can only screen for pain and document. All patients are to be re‐screened for the presence of pain and their intensity documented at a minimum:
• Every eight hours for inpatients • Every ambulatory setting visit • Following a potentially painful procedure which includes operative and invasive procedures and treatments and therapies
Reassessment of pain should be completed 30 minutes after IV medications and one hour after PO or IM medications are administered. If there are more than two consecutive episodes of pain greater than the patient’s goal or acceptable intensity, the healthcare provider needs to call the physician and discuss the patient’s pain management plan. Lastly, but very importantly, the patient education regarding pain manage‐ment must be documented and should include:
• Understanding of pain • Risk for pain • Importance of effective pain management • Methods for pain management

16
Pain: Assessment and Re‐Assessment (Continued) Pain is assessed using a variety of pain scales; samples Include:
FACES: Used with older children and adults
FLACC: Used with infants and children
Numeric Pain Intensity Scale: Used with older children, adolescents, and adults
Behavioral / Non Verbal Scale
Sleeping / calm and Relaxed
Grimacing with
movement
Moaning with
movement
Restless
Fidgety
Clenching
Constant Moaning without stimuli; unable to console
1 to 2 3 to 4 5 to 6 7 to 8 9 to 10
Instructions: Identify behavior and assign pain rating based on appropriate category.
Remember, management of pain is every caregiver’s responsibility.
Act and document!
PAINAD Behavioral Pain Scale (non‐verbal, cognitively impaired individuals)

17
Urinary Diversions: Obtaining a Sterile Urine Specimen Background
Intermittent urinary tract infections are often problematic for patients who have a urinary diversion, such as an ileal conduit. Proper technique in obtaining a urine specimen is imperative to get accurate urine culture results for these patients.
Urinary diversion procedures are performed to treat several illnesses, including; bladder cancer, neuorgenic bladder, congenital abnormalities, trauma, and damage caused by chronic urinary tract infections. Several types of urinary diversions exist including: an incontinent urinary diversion where an external appliance is necessary, a continent urinary diversion where the patient regularly performs self catheterization of the stoma or an orthotopic bladder in which the patient voids via the urethra. One of the most commonly used urinary diversions is the ileal conduit. It is considered an incontinent urinary diversion necessitating an external pouch system to collect the constantly
draining urine. In this procedure a 6 to 8 inch portion of the ileum is converted into a conduit or channel, for urinary drainage. The small portion of bowel is resected, ureters are connected to the conduit and one end of the bowel is brought through the abdominal wall forming a stoma.
A continent urinary diversion, such as the Kock Pouch allows the patient to have an internal reservoir for urine collection freeing the patient from having to wear an external collection bag. However the patient does have to perform stoma catheterization every 4‐6 hours. Ileal Conduit Picture Source: Sudakoff, G. S. et al. Am. J. Roentgenol. 2005;184:131‐138. Knoch Pouch Picture Source: The Urologic Disease Dictionary. National Kidney and Urologic Diseases Information Clearinghouse, NIH Publication No. 10–4376, May 2010.
Obtaining a Urine Culture Sample When a urine culture is ordered for a patient with a urinary diversion, it is imperative that the urine sample be obtained via the stents or via catheterization of the stoma, not taken from the collection bag. Because urinary diversions are created with portion of bowel, bacteria is normally present on the stoma and in the collection bag. Therefore a urine sample taken from the collection bag provides inaccurate information. To obtain a urine sample from a urinary diversion, follow the current hospital policy: “Sterile Urine Specimen
Obtained from Urinary Stoma with/without Stent Placement.” Reminders from the policy:
1. If present, remove the collection pouch off the wafer flange. a. Do not use the pouch contents to obtain the urine specimen. b. Remove gloves and don sterile gloves to complete the procedure.
2. Cleanse the stoma with betadine in a circular motion. a. If stents are present:
i. Secure the stents and cleanse the tips with betadine. ii. Allow urine to drip into the collection container.
3. Lubricate the catheter tip before inserting. 4. Insert the catheter into the stoma approximately 1 ½ inches.
a. It may be necessary to insert the catheter further if the patient has an increased amount of adipose tissue.
b. If resistance is met, angle the catheter medially and down and reattempt insertion.
c. Urine will flow slowly. d. If no urine flows:
i. Encourage the patient to drink a glass of water, if permitted.
ii. Have the patient cough.
Ileal Conduit
18
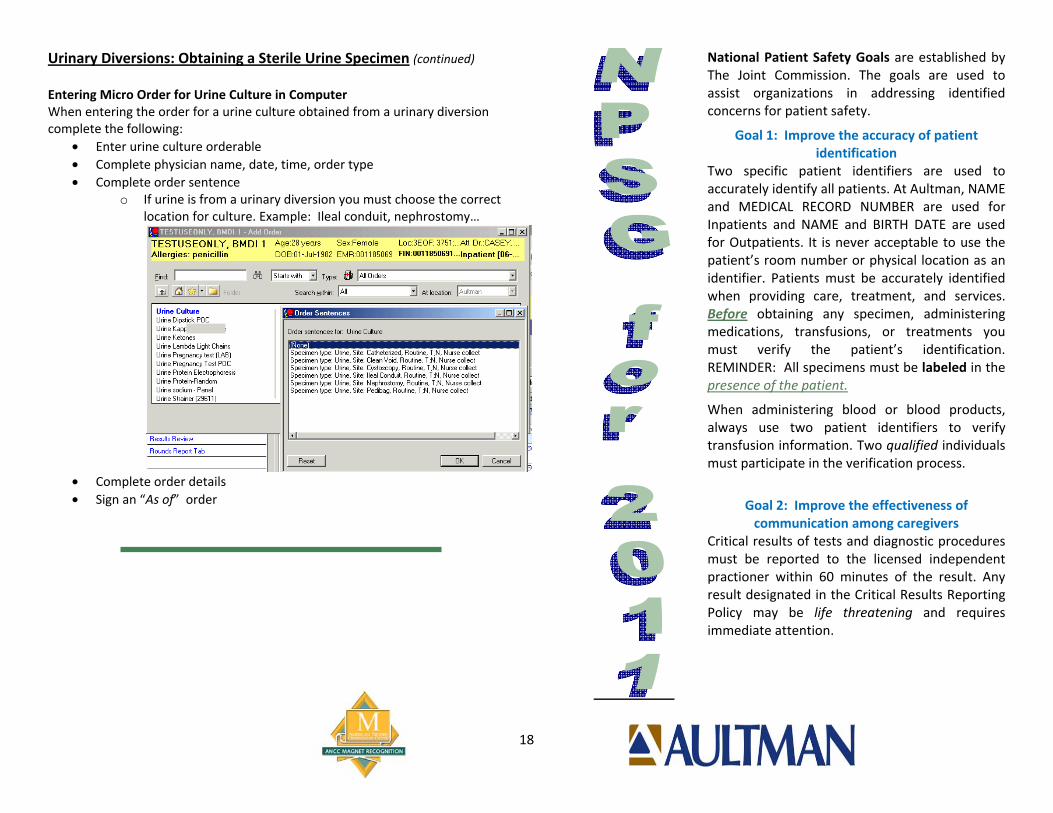
Urinary Diversions: Obtaining a Sterile Urine Specimen (continued) Entering Micro Order for Urine Culture in Computer When entering the order for a urine culture obtained from a urinary diversion complete the following:
• Enter urine culture orderable • Complete physician name, date, time, order type • Complete order sentence
o If urine is from a urinary diversion you must choose the correct location for culture. Example: Ileal conduit, nephrostomy…
• Complete order details • Sign an “As of” order
National Patient Safety Goals are established by The Joint Commission. The goals are used to assist organizations in addressing identified concerns for patient safety.
Goal 1: Improve the accuracy of patient identification
Two specific patient identifiers are used to accurately identify all patients. At Aultman, NAME and MEDICAL RECORD NUMBER are used for Inpatients and NAME and BIRTH DATE are used for Outpatients. It is never acceptable to use the patient’s room number or physical location as an identifier. Patients must be accurately identified when providing care, treatment, and services. Before obtaining any specimen, administering medications, transfusions, or treatments you must verify the patient’s identification. REMINDER: All specimens must be labeled in the presence of the patient.
When administering blood or blood products, always use two patient identifiers to verify transfusion information. Two qualified individuals must participate in the verification process.
Goal 2: Improve the effectiveness of communication among caregivers
Critical results of tests and diagnostic procedures must be reported to the licensed independent practioner within 60 minutes of the result. Any result designated in the Critical Results Reporting Policy may be life threatening and requires immediate attention.

19
National Patient Safety Goals (NPSG) for 2011 (continued)
ALWAYS remember: The licensed caregiver must be notified within 60 minutes of the
completion of the results. 60 minutes: A shared time between Lab or Radiology and Nursing
to Provider Notification. o Results available → Results reported to Nursing →
Results reported to provider Document the receipt of results, communication of the results,
and action if any in PROVIDER NOTIFICATION.
Goal 3: Improve the safety of using medications. Label all medications, medication containers, and other solutions on and off the sterile field in perioperative and other procedural settings. Note: Medication containers include syringes, medicine cups, and basins. ALWAYS LABEL MEDICATIONS WHEN… The person preparing the medication does not administer it. Done
both visually and verbally by two individuals qualified to participate in the procedure.
The medication is not administered IMMEDIATELY upon removal from the original container.
Multiple medications are being administered. All medications and solutions both on and off the sterile field and their labels MUST be reviewed by entering and exiting staff responsible for the management of medications.
One of our most important goals is to reduce the likelihood of patient harm associated with the use of anticoagulant therapy. We provide comprehensive education to our patients with standardized patient/family educational pathways for Warfarin, Heparin, Plavix, and Lovenox as well as video educational materials for Lovenox and Warfarin. For the safety of our patients, INR’s should be done daily on all patients receiving Warfarin. Even patients stabilized on their dose for a long period of time are at risk when they are admitted to the hospital. Many medications given in the hospital may affect the way patients react to Warfarin. Acknowledgement of current INR results is required prior to administration of Warfarin. Standardized orders for warfarin
and heparin are available for use. Our pharmacists review the use of anticoagulant medications. Heparin orders have recently been revised to include current best practice recommendations.
Goal 7: Reduce the risk of health care–associated infections. Hand Hygiene Hand Hygiene is the single most important technique to prevent the spread of infection! A soap/water wash is required when hands are visibly or physically soiled, and after any contact with a patient /environment suspected or known to have spores i.e., Clostridium difficile or Bacillus anthracus.
When hands are not visibly/physically soiled they may be decontaminated by using alcohol‐based hand sanitizer. Remember, the lathering portion of a soap and water wash is to be 15 seconds.
Five Hand Washing Steps: 1. Wet hands under water; 2. Apply soap being sure to
lather all surfaces for 15 seconds
3. Rinse thoroughly 4. Dry thoroughly with
paper towel 5. Use towel to turn faucet off
Note: Following a soap and water wash with alcohol sanitizer decreases the bacterial count.
Prevention of Health Care Associated Infections MDRO (Multidrug‐ Resistant Organisms) Multidrug‐Resistant Organisms are one of the most common causes of healthcare associated infections. MDROs are organisms that have become resistant to many antibiotics commonly used to treat them. Proper hand hygiene, standard and transmission‐driven precautions, are essential in preventing the transmission of MDRO’s. MICU and SICU take special precautions to prevent the transmission of MDRO’s. Patients admitted to MICU and SICU who meet certain criteria are screened for MRSA and Acinetobacter. Screening helps identify patients who may be infected or colonized with such organisms. The patients who are deemed High Risk are preemptively placed in

20
isolation until culture results are available. In addition, any patient in the hospital who is diagnosed with an MDRO will also be placed in isolation.
Aultman uses a method to alert staff of patients who culture positive during a current admission, or who re‐enter the hospital system with a history of an MDRO. These patients are identified by a Two Letter Code. The following codes may be used alone or in combination for patients with more than one organism.
CM: MRSA: Methicillin‐resistant Staphylococcus aureus CV: VRE: Vancomycin‐resistant Enterococcus CD: C. diff: Clostridium difficile CE: ESBL: Extended‐spectrum beta lactamase (Enzyme
produced by certain bacteria that can break down several types of antibiotics, rendering them ineffective)
CA: Acinetobacter baumannii haemolyticus
If your patient has a code on the patient identification materials, place the patient in preemptive isolation precautions and notify the physician. The physician will determine if the patient has cleared the organism. This may be done via clinical correlation and/or testing. The isolation may be discontinued when the physician has determined the patient no longer is infected and/or colonized with the organism. Physicians should order the removal of the code from the hospital information system. Contact lab personnel to remove the code.
NOTE: Regarding codes for C. diff: A Patients’ absence of clinical symptoms (diarrhea) is all that is required to request code removal order from physician. Isolation is not required in this circumstance.
CLABSI (Central Line Associated Blood Stream Infection) Central line‐associated blood stream infections are infections that can occur from the placement and use of a central line. Bacteria can get into the line and cause serious infections for patients. CLABSI rates are monitored by Infection Control. Rates can be found on the Infection Control Surveillance Matrix by contacting your Unit Director. There are several steps that can be taken to prevent the occurrence of a line‐associated blood stream infection. EDUCATE your patients and their families about ways they can
help prevent line associated infections. Always perform HAND HYGIENE prior to manipulation of the
catheter.
DISINFECT the catheter hubs before accessing (“Scrub the Hub”).
EVALUATE the site for infection frequently. REVIEW daily (with physician) the necessity of the line. REMOVAL of nonessential catheters helps prevent infection. CHLORHEXIDINE‐BASED ANTISEPTIC for skin preparation
should be used during insertion and dressing changes (Use for patients over 2 months of age, unless contraindicated).
SSI (Surgical Site Infection) Surgical site infections are among the most common types of health care associated infection. Many things can be done reduce the incidence of surgical site infections. Remember to EDUCATE patients undergoing surgical procedures about ways to prevent SSI. Always follow current SCIP (Surgical Care Improvement Project) Core Measure Guidelines. Education for SCIP can be found in the Core Measure section of this newsletter. Close monitoring of targeted surgical site infection rates by Infection Control helps us to quickly identify any areas of concern for potential problems. These rates can be found on the Infection Control Surveillance Matrix or by contacting your Unit Director.
Aultman Woodlawn

21
**New 2012 National Patient Safety Goal**
CAUTI (Catheter‐Associated Urinary Tract Infection)
Beginning January 1, 2013, hospitals must implement evidenced‐based guide‐ lines to prevent catheter‐associated urinary tract infections (CAUTI). There are several key strategies that can be used to decrease the risk of CAUTI.
1. Evaluate need for the catheter daily. a. Limit catheter use to those necessary for patient care. b. Remove catheter as soon as no longer needed.
1. Proper hand hygiene performed prior to contact with catheters. 2. Use aseptic technique for site preparation/insertion. Maintain sterility
of equipment and supplies. 3. Use catheter securement devices to prevent obstructed urine flow and
drainage. 4. Maintain a closed urine collection system. 5. Replace catheter system when required. 6. Perform Catheter Care with soap and water daily and as needed.
Infection Control conducts surveillance of CAUTI’s monthly. This information is used to evaluate the effectiveness of prevention efforts.
Influenza Update: Debunking the Myths The following are some facts you should consider as a healthcare worker and a member of a family or household. • The CDC tells us the number one way to prevent getting the flu or
spreading the flu is to get the flu vaccine.
• In a typical year, approximately 5 to 20 percent of the population gets the seasonal flu. Flu‐related deaths range from 3,300 to 48,600 (average 23,600).
True or False Question 1 of 10: A flu vaccine can’t give you the flu. Answer: True. The flu vaccine cannot cause flu illness. The viruses in the vaccine are either killed (flu shot) or weakened (nasal spray vaccine), which means they cannot cause infection. Question 2 of 10: The “stomach flu” and influenza are the same thing. Answer: False. “Stomach flu” is a popular term for stomach or intestinal disease, whereas the flu is a respiratory (lung) disease. People who have the flu often feel some or all of the same symptoms: fever, headache, extreme tiredness, dry cough, sore throat and muscle aches. Nausea, vomiting and diarrhea also can occur with flu, but are more common in children than adults.
How much do YOU know about the FLU?
Aultman Hospital

22
Question 3 of 10: Getting a flu vaccine in December or later is not too late. Answer: True. CDC recommends that people get vaccinated as soon as the vaccine becomes available and that vaccination continues into December, January and beyond. Influenza activity usually peaks in February most years, but disease can occur as late as May. Question 4 of 10: Flu viruses change constantly which requires a new vaccine to be produces each year. Answer: True. The viruses in the vaccine change each year based on the worldwide monitoring of influenza viruses. Question 5 of 10: Washing your hands is the best thing you can do to protect against the flu. Answer: False. CDC recommends a flu vaccine as the first and most important step in protecting against the flu. However, preventative actions like covering your cough and washing your hands often are important everyday steps that can help stop the spread of germs. Question 6 of 10: The flu vaccine protects against three strains of the flu. Answer: True. While there are many different flu viruses, the flu vaccine protects against the three viruses that research suggests will be the most common. Question 7 of 10: The flu is typically spread through coughs and sneezes. Answer: True. Flu virus is mainly spread through droplets from coughs and sneezes.
Question 8 of 10: The flu is not a serious illness. Answer: False. Flu is a serious contagious disease that causes illness and related hospitalizations and deaths every year in the United States. Flu seasons can vary in severity. Over a period of 30 years, between 1976 and 2006, estimates of flu‐associated deaths range from a low of about 3,000 to a high of 49,000 people. Question 9 of 10: The flu vaccine is available as a shot or nasal spray. Answer: True. Flu vaccine is also available as a nasal spray (brand name FluMist®). The nasal spray flu vaccine is an option for “healthy” people 2‐49 years of age who are not pregnant. “Healthy” indicates people who do not have an underlying medical condition that predisposes them to influenza complications. Question 10 of 10: You can spread the flu to others before you have symptoms. Answer: True. Most healthy adults may be able to infect others beginning 1 day before symptoms develop and up to 5‐7 days after becoming sick. That means you may be able to pass on the flu to someone else before you know you are sick, as well as while you are sick.

23
Influenza Update (Continued)
Vaccination is the best protection against contracting the flu. Everyone 6 months of age and older should get vaccinated against the flu as soon as the seasonal vaccine is available in your area.
Two types of vaccines are available: shot and nasal mist. The viruses in the flu shot are killed (inactivated), so you cannot get the flu from a flu shot. The viruses in the nasal‐spray vaccine are weakened and do not cause severe symptoms often associated with influenza illness. (In clinical studies, transmission of vaccine viruses to close contacts has occurred only rarely.) The flu shot will be provided free of charge through our Health Services Department as soon as it becomes available. Health Services does not offer the nasal vaccine.
Some MINOR side effects that could occur with the flu vaccine are: o The flu shot:
Soreness, redness, or swelling where the shot was given Fever (low grade) Aches
o The nasal spray (also called LAIV or FluMist®): In children, side effects from LAIV (FluMist®) can include:
runny nose wheezing headache vomiting muscle aches fever
In adults, side effects from LAIV (FluMist®) can include:
runny nose headache sore throat cough
The above content has been directly taken from the CDC website: http://www.flu.gov/
You are a leader, agent of safety, an advocate for your patients! Should you have questions please contact Infection Control & Prevention @ ext. 34815.
to our Contributors for
the 2011 Organizational Education for Nursing Newsletter:
Renee’ Adams, BSN, RN
Sherry Augustine, MT (ASCP)
Brandie Bertleff, BSN, RN
Christina Dewar, Pharm D, BCPS
Laurie Fitzgibbon, MSN, RN, CCNS, CEN
Linda Griggs, MSN, RN‐BC, ACNS‐BC
Deanna Hatfield, MSN, RN, NE‐BC
Ron Manes, BSN, RN, CCRN
Lori Mertes, MD
Colleen Motts, BSN, RN
Angela Ott, MSN, RN, CNE, NE‐BC
Joan Pugnale, BSN, RN, CIC
Kelli J. Scott, MS
Debbie Shaffer, BSN, RN
Tieryn Trissel, MBA, BSN
Pamela T. Wagner, MSN, RN

24
Medications Related to Falls
Background Falls are the leading cause of injury related death in patients over 65 years of age. Elderly patients are at a higher risk of falling due to their age. This risk increases with certain medications that can be found on the Beer’s list. The Beer’s list contains medications that are considered inappropriate for elderly patients for a variety of reasons. This list defines what the concern for the medication is along with alternative therapy options. All medical professionals have a role in fall prevention. Risk Factors Patients who are at an increased risk of falling may have symptoms that include: muscle weakness, balance disorders, visual disturbances, mental status changes, postural hypotension, dizziness, or incontinence. High Risk Medications Certain medications are considered high risk due to their side effect profile that includes sedation, dizziness, confusion, or lack of coordination. Benzodiazepines include alprazolam (Xanax), lorazepam (Ativan), diazepam (Valium), chlordiazepoxide (Librium), clonazepam (Klonopin), and temazepam (Restoril). Hypnotics are also considered high risk and include zolpidem (Ambien) and hydroxyzine (Atarax,Vistaril). Diphenhydramine (Benadryl) can also cause sedation and increase fall risk, especially at higher doses. Elderly patients are more sensitive to these medications and their side effects.
Preventative actionIt is important to be aware of patients that are at a high fall risk. A yellow arm band must be placed on the patient’s wrist and a star must be placed by the patient’s door frame indicating this risk. These patients should be educated on the side effects and risk of falls associated with these medications. Patients should be advised to call for assistance before trying to ambulate. Other suggestions for patient education include sitting on the edge of the bed for a few minutes before standing, turning on the lights before walking, and to walk slowly while steadying themselves as much as possible. The lowest dose of a short acting oral medication is preferred when choosing a patient’s PRN medication for anxiety, sleep, or panic disorders. Please note, patient’s who take benzodiazepines (alprazolam, lorazepam, etc) at home should continue to receive their medications while in the hospital to prevent withdrawal symptoms. They will still require education and actions to prevent falls should still be taken. If given the options of PRN medications, choose the lower risk medication. Preferred formulary options for insomnia treatment in the elderly include temazepam (Restoril) 7.5mg po or zolpidem (Ambien) 5mg po (low dose). Preferred formulary options for anxiety treatment in the elderly are alprazolam (Xanax) 0.25mg po, lorazepam (Ativan) 0.5‐1mg po/IV, and buspirone (Buspar) 5mg‐10mg po. The table below indicates medications that are preferential because they create less of a risk to the patient for falls:
Choose This Avoid this Restoril 7.5mg po prn insomnia Ambien 10mg po prn insomnia Xanax 0.25mg po prn anxiety Ativan 2mg po prn anxiety Ambien 5mg po prn insomnia Diphenhydramine 50mg po prn insomnia Ativan 1mg po prn anxiety Ativan 1mg IV prn anxiety

25
Additional Resources
Lexi‐Comp, available on the intranet and as a link in Powerchart, identifies Beers Criteria medications in the drug monograph under either the “Dosing: Geriatric”, the “Geriatric Considerations”, or the “Medication Safety Issues” categories. Pulling up a drug monograph and using the internet explorer “Find” function (type Ctl + F at the same time) to search for “Beers” or “Geriatric” is an easy way to determine if a medication poses a fall risk. Pharmacists are also able to help answer questions
regarding the Beers List medications.
MEDICATIONS & FALLS
The Beers Criteria is a list of medications considered potentially inappropriate for the elderly
The elderly, due to advanced age, are already at a higher risk of falling, and Beer’s Criteria medications further increase this risk
Lexi‐Comp includes “Geriatric Considerations” and “Beer’s List Medication” categories in high risk drug monographs
Beers Criteria list of High‐risk anxiolytics and hypnotics for the elderly
• Benzodiazepines: clorazepate, chlordiazepoxide, diazepam, alprazolam, lorazepam, oxazepam, temazepam, triazolam, flurazepam
• Meprobamate • Barbiturates: primidone and phenobarbital (excluded if used to control seizures) • Anti‐histamines: Diphenhydramine, Hydroxyzine
Benzodiazepines
• Class of medications commonly used for short term treatment of insomnia, anxiety and panic disorders
• Side effects associated with benzodiazepines include o Sedation o Dizziness o Confusion o Lack of coordination
• The elderly tend to experience increased sensitivity to the effects of benzodiazepines
Preventative Action
• Use the lowest effective dose of prn medications • Review medications in Lexi‐Comp for elderly‐related cautions or to determine if a
medication may increase patient risk of falls • Patient education –
o Inform patient of side effects and risk of falls associated with these medications
o Remind patient that nursing assistance is available for ambulation o Inform patient of the importance of sitting upright at the bedside for 1‐2
minutes before standing
26
Core Measures
What are Core Measures? Core Measures are evidence‐based indicators used to measure quality in a consistent way. This enables everyone to compare quality between hospitals. Comparisons can be found on www.hospitalcompare.hhs.gov. Core Measures reflect best practice for the patient. Why are Core/Performance Measures important?
• Core/Performance measures are proven patient care practices demonstrated through research. Research indicates that adherence to these measures improves patient outcomes.
• Hospital Medicare reimbursement is affected by participation and adherence to these measures.
• These measures are publicly reported and a hospital’s performance and adherence to these measures may influence where a person chooses to seek care.
How can the nurse make a difference in Core/Performance measures? • Documentation is the Key to successful reporting of these measures! • When there is a deviation from a core/performance measure
recommendation, there must be supporting documentation as to why there was a deviation.
• Use the task list to chart and always clear task lists at the end of your shift.
These measures include the following: The Surgical Care Improvement Project (SCIP), Heart Failure (HF), Pneumonia (PN), and Acute Myocardial Infarction (AMI). Each of these measures has several components that have to be met on selected patients in order to be compliant.
Nurses are patient advocates and need to provide the best care possible. Adherence to the Core/Performance measures can help contribute to this.
ACUTE MYOCARDIAL INFARCTION (AMI)The AMI Core Measures focus on providing the best care for the patient with Acute Myocardial Infarction. Aultman must achieve 100% compliance to be counted in the 90th percentile.
The required measures include: o ASA administered within 24 hours
before or after hospital arrival or contraindication documented.
o ASA prescribed upon discharge or contraindication documented.
o Smoking cessation advice/ counseling provided before discharge.
o ACE Inhibitor or ARB prescribed at discharge for LVSD (left ventricular systolic dysfunction) or contraindication documented.
o Beta blocker prescribed at discharge or contraindication documented.
o Median time to primary PCI (Percutaneous Coronary Intervention). (Time, in minutes, from hospital arrival to primary PCI in patients with ST‐segment elevation or LBBB on the ECG performed closest to hospital arrival).
o Primary PCI rendered within 90 minutes of hospital arrival. (% within 90 min).
o Inpatient mortality. o Statin prescribed at discharge or contraindication documented.
For any questions regarding the AMI Core Measures contact Ron Mane, BSN, RN, CCRN, via email at [email protected] or at extension 30785.
27
PNEUMONIA Pneumonia is the sixth leading cause of death in the United States. Patients are included in the Pneumonia core measure when they are assigned a pneumonia DRG upon discharge, which is determined by the coding department. Please note that even if a patient is not admitted with a primary diagnosis of pneumonia, this may end up as the assigned DRG. The requirements of this measure include:
o Blood cultures drawn within 24 hours of arrival: • Make sure cultures are drawn prior to hanging antibiotics
o Antibiotic selection ICU/Non ICU patients. o Antibiotics hung within 6 hours of patient arrival time:
• Verify Antibiotic time from ED green sheet (410D) if patient is admitted from ED
o Smoking Cessation: • If patient has smoked within last year, smoking
cessation information must be offered and documented as such
o Pneumococcal Vaccine Assessment/ Administration. o Influenza Vaccine Assessment/Administration:
• October 1st‐March 31st
For more details or any questions regarding pneumonia contact Renee Adams, BSN, RN, via email at [email protected] or at ext 35247.
Surgical Care Improvement Project (SCIP) SCIP focuses on providing the best care for the surgical patient. The surgeries included in this core measure are:
SCIP SurgeriesTotal Hip Replacement Certain Other General SurgeriesTotal Knee Replacement Hysterectomy
Colon Surgery Vascular SurgeriesExploratory Laparotomy CABG
The requirements of this measure include:
o Prophylactic antibiotic received within 1 hour prior to surgical incision, 2 hours for vancomycin
o Appropriate prophylactic antibiotic selection o Prophylactic antibiotic discontinued:
• Within 24 hours after anesthesia end time • 48 hours for Cardiac Surgery only (If antibiotics are ordered beyond the 24 or 48 hours, a specific reason should be documented)
o Hair removal using clippers o Post‐operative normothermia
(36oC) in all surgical patients o Controlled 6 am post‐op serum
glucose, day 1 & 2, for cardiac surgery patients
o Patients maintained on beta blocker peri‐operatively if on beta blocker therapy prior to admission
o Recommended Venous Thromboembolism or VTE prophylaxis ordered and initiated within 24 hours prior to surgery to 24 hours after surgery
o Foley catheter removal on POD#1 or POD#2, or documented reason for continuing
For more details or any questions regarding SCIP contact Tieryn Trissel, MBA, RN, via email at [email protected] or at ext 37353.

28
HEART FAILURE Heart Failure is followed by both the Joint Commission and the American Heart Association. An asterisk designates the Core Measure. No asterisk designates the additional AHA Get with the Guidelines Quality Measures. Heart Failure Core Measures focus on providing the best care for the HF patient. The Heart Failure Core Measures include:
o HF DC Instructions * include activity level, diet, DC medications, follow up appointment, weight monitoring, what to do if symptoms worsen.
o Documented Left Ventricular Function* o ACEI/ARB for LV Systolic Dysfunction or documented contraindication* o Smoking Cessation Counseling* o Warfarin for Chronic or Recurrent A‐fib or documented
contraindication o Aldosterone Antagonist for LVSD or documented contraindication o CRT‐D or CRT‐P placed or prescribed for patients with EF< or = to 35%
and QRSD of 120ms or above, or documented contraindication o DVT prophylaxis o Evidence‐based Specific Beta‐blockers o Hydralazine/Nitrate prescribed at discharge o ICD place or prescribed at discharge o Influenza vaccination during flu season o Pneumococcal vaccination
For more details or any questions regarding HF Core Measures contact Colleen Motts, BSN, RN via email at [email protected] or pager 430‐8777.

29
References Recognition of the Critically Ill
Barco, A.., Putnam, J., Riggs, J., Bayne, A.(2011). A historical look at CPR and the concept of failure to rescue. The Kansas Nurse, 86(1), 15‐16.
Clarke, S., Aiken, L. (2003). Failure to rescue. American Journal of Nursing, 103(1), 42‐47.
Society of Critical Care Medicine (2007). Fundamentals of Critical Care Support. Author: Mount Prospect, IL.
Society of Critical Care Medicine (2009). Designing, Implementing, and Enhancing a Rapid Response System. F. Sebat (ed). Author: Mount Prospect, IL.
Thomas, K., Force, M., Rasmussen, D., Dodd, D. & Whildin, S. (2007). Rapid response team: Challenges, solutions, benefits. Critical Care Nurse, 27(1), 20‐27.
Enhancing Cross‐Cultural Communication in Patient Care Cosgrove‐Mather, B. (Washington 2004 ). America's Face is Changing. AP . Rohini Anand, P. (2006). Cultural Competency in Health Care. Washington, DC: National MultiCultural Institute ‐ NMCI Publications. Ursula Leitzmann, M. M. (2011, April 28). Cultural Competence in Health Care . Retrieved October 12, 2010, from IOR Global Services: http://www.IORWorld.com
IV Vancomycin: Dosing and Monitoring
Rybak M, Lomaestro B, Rotschafer JC, Moellering Jr. R, Craig W, Billeter M, Dalovisio JR, Levine DP. Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American society of health‐system pharmacists, the infectious diseases society of America, and the society of infectious diseases pharmacists. Am J Health‐Syst Pharm. 2009 Jan 1; 66: 82‐98.
Vancomycin Hydrochloride. Lexi‐Comp Onilne. Accessed May 27, 2011
Blood Administration Tips
1Nursing: The Art and Science of Safe Transfusion. Feature article for The Bleeding Edge. May 2011, Vol. 3, Issue 5. Urinary Diversions: Obtaining a Sterile Urine Specimen
Content was reviewed by Dr. G. Kmetz, Canton Urology Associates.
Smith, S.F., Duell, D.J. & Martin, B.C. (2008). Clinical nursing skills: Basic to advanced skills. (7th ed). Upper Saddle River, NJ: Prentice Hall Lewis, S.L., Heitkemper, M.M., Dirksen, S. R., O’Brien, P.R. & Bucher, L. (2007). Medical‐Surgical nursing: Assessment and management of clinical problems. (7th ed). St. Louis, Missouri: Mosby Elsevier Medications and Falls Beers MH, Ouslander JG, Rollingher I, Reuben DB, Brooks J, Beck JC. Explicit criteria for determining inappropriate medication use in nursing home residents. Arch Intern Med 1991;151:1825‐32. Beers MH. Explicit criteria for determining potentially inappropriate medication use by the elderly: an update. Arch Intern Med 1997;157:1531‐6. Potentially harmful drugs in the elderly: Beers list and more. Pharmacist’s Letter/Prescriber’s Letter 2007; 23(9): 230907.