organizing care for patients with chronic diseases darren a. dewalt, md, mph associate professor...
TRANSCRIPT

Organizing Care for Patients with Chronic Diseases
Darren A. DeWalt, MD, MPHAssociate Professor
University of North Carolina

Living with chronic illness is like piloting a small plane
icic.org

To get safely to their destination, pilots need
Self-Management Support
Effective Clinical Management
Treatment Plan
Close Follow-up
Flight instruction
Preventive Maintenance
Safe Flight Plan
Air Traffic Control Surveillance
icic.org
Usual care works well if your plane is about to crash
icic.org

Essential Element of Good Chronic Illness Care
Informed,ActivatedPatient
ProductiveInteractions
PreparedPractice Team
icic.org

What characterizes a “prepared” practice team?
PreparedPractice Team
At the time of the visit, they have the patient information, decision support, people,
equipment, and time required to deliver evidence-based clinical management and
self-management support
icic.org

What characterizes a “informed, activated” patient?
Patient understands the disease process, and realizes his/her role as the daily self manager. Family and caregivers are engaged in the patient’s
self-management. The provider is viewed as a guide on the side, not the sage on the stage!
Informed,ActivatedPatient
icic.org

Assessment of self-management skills and confidence as well as clinical statusTailoring of clinical management by stepped protocolCollaborative goal-setting and problem-solving resulting in a shared care planActive, sustained follow-up
Informed,ActivatedPatient
ProductiveInteractions
PreparedPractice Team
How would I recognize aproductive interaction?
icic.org

Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
DeliverySystemDesign
DecisionSupport
ClinicalInformation
Systems
Self-Management
Support
Health System
Resources and Policies
Community
Health Care Organization
Chronic Care Model
Improved Outcomesicic.org
Self-management Support
• Emphasize the patient's central role.• Use effective self-management support
strategies that include assessment, goal-setting, action planning, problem-solving and follow-up.
• Organize resources to provide support
icic.org

Delivery System Design
• Define roles and distribute tasks amongst team members.
• Use planned interactions to support evidence-based care.
• Provide clinical case management services.• Ensure regular follow-up.• Give care that patients understand and that fits their
culture
icic.org

Features of case management
• Regularly assess disease control, adherence, and self-management status
• Either adjust treatment or communicate need to primary care immediately
• Provide self-management support• Provide more intense follow-up • Provide navigation through the health care process
icic.org

Decision Support
• Embed evidence-based guidelines into daily clinical practice.
• Integrate specialist expertise and primary care.• Use proven provider education methods.• Share guidelines and information with patients.
icic.org

Clinical Information System
• Provide reminders for providers and patients. • Identify relevant patient subpopulations for
proactive care.• Facilitate individual patient care planning.• Share information with providers and patients.• Monitor performance of team and system.
icic.org
Health Care Organization
• Visibly support improvement at all levels, starting with senior leaders.
• Promote effective improvement strategies aimed at comprehensive system change.
• Encourage open and systematic handling of problems.• Provide incentives based on quality of care.• Develop agreements for care coordination.
icic.org

Community Resources and Policies
• Encourage patients to participate in effective programs.• Form partnerships with community organizations to
support or develop programs.• Advocate for policies to improve care.
icic.org
Let’s Look at Examples
• Diabetes (Kirkman will discuss)• Heart Failure• Depression• Hypertension• Prevention• Arthritis (Hawker and Allen will discuss)

Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes:Reduced Hospitalizations
Improved health-related quality of life
DeliverySystemDesign:
PCP, pharmacist, educator work
together to manage patient in
office and on phone
Decision Support:
Guidelines embedded
in care system (visit
planner)
ClinicalInformation
SystemsRegistry to track
patients and ensure receiving
core quality
Self-Management
Support:Literacy appropriate
educational materials, reminder
calls/education, clearly distilled plans
Health System:4 Academic Health CentersCommunity
Heart Failure Management
DeWalt et al. Circulation. 2012 Jun 12;125(23):2854-62.DeWalt et al. BMC Health Serv Res. 2006 13;6:30. McAlister et al. J Am Coll Cardiol. 2004 18;44(4):810-9.

Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes:Incr. Use of antidepressants
Incr. Use of counseling80% remission in 2 yrs (40% for usual care)
Higher role functioning
DeliverySystemDesign:
PCP, nurse and office staff all
involved.Monthly contact
with pts by phone via nurse
Decision Support:AHCPR
guidelinesPsychia-
trist review and advice
on tx adjust
ClinicalInformation
SystemsPt roster with tx
summaries, feedback to care
team
Self-Management
Support:office nurse provided
info on treatment options, readiness
intervention, tx effectiveness assessment
Health System:12 PCPs in US metro and non-metro)Community
Depression
Rost et al BMJ 2002;325:934
icic.org
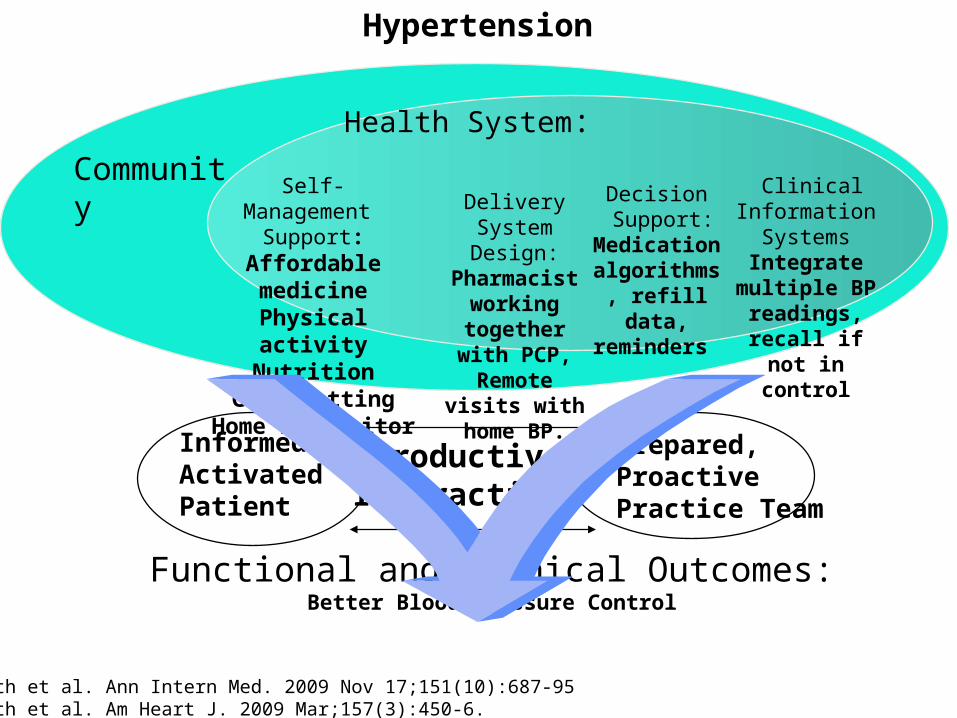
Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes:Better Blood Pressure Control
DeliverySystemDesign:
Pharmacist working together
with PCP,Remote visits with home BP.
Decision Support:
Medication algorithms, refill data, reminders
ClinicalInformation
SystemsIntegrate
multiple BP readings, recall if not in control
Self-Management
Support:Affordable medicine
Physical activityNutrition
Goal settingHome BP monitor
Health System:
Community
Hypertension
Bosworth et al. Ann Intern Med. 2009 Nov 17;151(10):687-95Bosworth et al. Am Heart J. 2009 Mar;157(3):450-6.

Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes:Better functional status, better nutrition, higher screening rates,
DeliverySystemDesign:
Easy scheduling, pre-visit decision
aids, health educator, access
to facilities (gym)
Decision Support:
Reminders to clinical team, information for patients
ClinicalInformation
SystemsRegistry to
monitor appropriate
screening and counseling
Self-Management
Support:Physical activity
NutritionGoal setting
Navigation for screening
Health System: Commitment to prevention
CommunityAccess to walking,
healthy foods, mindfulness, social
capital
Prevention

Multiple Chronic Illnesses is the Rule, not the Exception

Planning Productive Interactions for Chronic Conditions
Additional Diagnoses* 45%
Functional Limits** 50%
> 2 Symptoms*** 35%
Not Good Health Habits 30%
*Arthritis (34%), obesity (28%), hypertension (23%),cardiovascular (20%), lung 17%)** Physical (31%), pain (28%), emotional (16%), daily activities (16%)*** Eating/weight (39%), joint pain (32%), sleep (25%), dizzy/fatigue(23%), foot (21%), backache (20%)
For Example: Diabetic Needs
icic.org

Number of Chronic Conditions per Medicare Beneficiary
Number of Conditions
Percent of Beneficiaries
Percent of Expenditures
0 18 1
1 19 4
2 21 11
3 18 18
4 12 21
5 7 18
6 3 13
7+ 2 14
63% 95%
icic.org

Guidelines are Essential, but not Sufficient
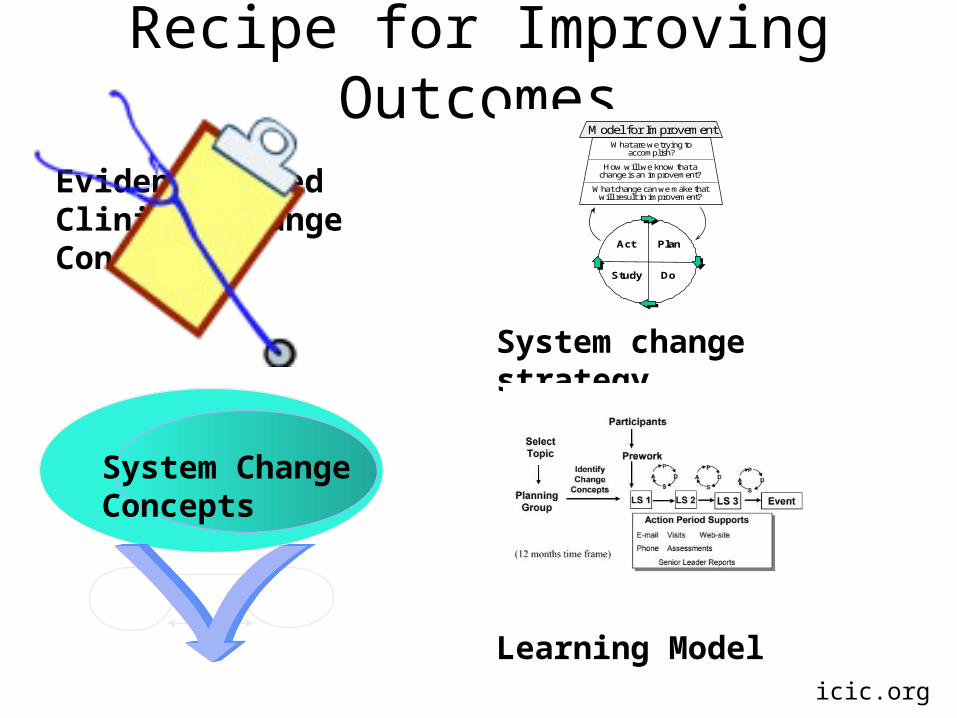
Recipe for Improving Outcomes
Evidence-basedClinical ChangeConcepts
Learning Model
System ChangeConcepts
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
System change strategy
icic.org

Drivers for Changing Models of Care
• Accountable leadership• Partnerships that promote quality of care• Attractive motivators and incentives• Transparent performance measurement• Organized quality improvement effort• Consumer engagement• Plans for sustainability
Margolis et al. J Contin Educ Health Prof. 2010;30(3):187-96.
How are these levers getting pulled?
• Motivators and incentives– pay for performance– Payment for Patient Centered Medical Home
• Transparent performance reporting– NCQA– Public reporting in some markets
• Organized Quality Improvement– Collaboratives and practice facilitation increasingly available
• Consumer engagement– Patients like me– Patient associations (Crohn’s and Colitis Foundation)

Summary
• CCM identifies the key aspects of care for the future
• Successful implementation of CCM improves outcomes across a variety of conditions/prevention
• Changing the system of care is required to successfully implement the CCM
• Several levers can influence the pace and success of large-scale system transformation