original article - blood transfusionbloodtransfusion.it/articoli/000033/en/000105.pdf · perdite di...
TRANSCRIPT

296 Blood Transfus 2006; 4: 296-310
Correspondence:Dr. Massimo FranchiniServizio di Immunoematologia e Trasfusione,Ospedale Civile Maggiore, Piazzale Stefani, 137126 Verona, Italiae-mail: [email protected]
Original article
Use of platelet gel and bone from tissue bankin reconstructive orthopaedic surgery:the regenerative medicine as a multidisciplinary modelMassimoFranchini1,GuidoRocca2,AdeliaBosinelli1,MaurizioGoverna3,DanielaOlzer1,Silvia Fiorini1, ChiaraAloisi1,Andrea Scalvi2, GiorgioGandini1, DinoBarisoni3,MassimoMarcer2,GiuseppeAprili1
1Servizio di Immunoematologia e Trasfusione � Banca dei Tessuti della regione Veneto, Verona;2Divisione di Ortopedia e Traumatologia, Azienda Ospedaliera di Verona;31a Divisione di Chirurgia Plastica e Centro Ustioni, Azienda Ospedaliera di Verona, Italia
Introduzione
Il grande, tumultuoso, affascinante progresso dellaMedicina, che abbiamo vissuto e stiamo vivendo negliultimi anni, ha portato a un enorme sviluppo anche nelcampodei trapianti di organi e tessuti. La trapiantologia,intesaormaicomeunabrancaautonomaconlapeculiaritàdipoggiarenecessariamente sucoordinamentoesinergiedimolte altre discipline del panorama sanitario, è oggisnodo strategico delle strutture sanitarie più avanzate.Nell'ambito della trapiantologia, a fianco del trapiantod'organi, sta acquisendoun ruolo sempre più rilevante iltrapianto/innestodi tessuti, sia dal puntodi vista tecnico-scientifico, sia per quanto riguarda l'allargamento delleindicazioni terapeutichee ladiffusionediutilizzo.Il rapidosviluppodelle tecnichedi trapianto/innestodi
tessutihaviaviaposto rilevanti interrogativiedha,quindi,aperto importantiproblemi, che riguardano,daun lato,gliaspetti etici, normativi eorganizzativi e, dall'altro, quelli ipiù strettamente tecnici e specialistici (sicurezza econservazionedei tessutiutilizzati).Per dare una chiara e concreta risposta a queste
problematichedifondo,sonostateistituite intuttoilmondo(dapprimanegliStatiUnitiesuccessivamenteinEuropa)leBanche deiTessuti, in grado di raccogliere,manipolare,qualificare, distribuire tessuti con caratteristiche di altolivello qualitativo. Il tessuto diBanca costituisce oggi ilsupportobiologicopiù importantenellemoderne tecnichedi ricostruzione chirurgica. Grazie ai tessuti messi adisposizione dalleBanche, infatti, lamoderna chirurgiaricostruttiva ha potuto compiere importanti progressi el'innesto tissutale si pone pertanto oggi come unaimportante opzione chirurgica destinata a consentireimportanti recuperi anatomici, funzionali ed estetici,restituendo salute, benessere e qualità di vita a tanti
Abstract
Background. The aim of regenerative medicine, ayoung area of medicine, is not only to repair damagedtissues but also to regenerate them in order to restoretheir original function.Patients. In this study we evaluated the efficacy of
platelet gel, a blood component fornon-transfusional use,and homologous bone chips from a tissue bank in 25consecutive patients undergoing various types ofreconstructive orthopaedic surgery in theDepartment ofOrthopaedics and Trauma of the Ospedale CivileMaggiore, Verona, for severe bone disorders such aspseudoarthrosis, osteomyelitis, andbone defects.Results. The laboratory, instrumental and clinico-
functional resultsweregoodor satisfactory inall patients.This combined strategy was, therefore, shown to beextremely efficient in the regenerative treatment ofcomplexbonedisorders.Conclusions. It should be underlined that these
excellent results were obtained only through the closecollaboration of different specialists, including thoseworking in orthopaedic surgery, plastic surgery andtransfusionmedicine.
Key words: platelet gel, bone chips, orthopaedic surgery,regenerativemedicine.

297
pazienti1. È, infatti, sorto di recente una nuova branca,altamentespecialistica,dellamedicina,denominatamedicinarigenerativa, ilcuicompitononèsoltantoquellodiripararei tessutidanneggiatimaanche, e soprattutto,di rigenerarlifisiologicamente, ripristinandonela funzionalitàperduta.Tra i settori chirurgici, dove lamedicina rigenerativa
trova importanti applicazioni, quello della chirurgiaortopedica ricostruttiva è sicuramente il più interessante.Infatti,quandol'ossoperde lepropriecapacità riparative inpresenzadiuncalloosseopatologico,oppuredi importantiperdite di sostanza per cause traumatiche o post-chirurgiche,oaseguitodibonificheincasodiosteomieliti,è indispensabile affiancare auna sintesi stabile unvalidosupportobiologicoperpoter raggiungere l'obiettivodellaconsolidazioneossea.Inquesticasi, tutt'altrocherari, l'ossodi banca rappresenta una valida e sicura alternativa agliinnesti ossei autoplastici, avendo sia capacitàosteoconduttive (l'innesto osseo funge da strutturatridimensionalepassivachefavorisce l'inserimentodivasisanguigni e la formazione di nuovo osso) cheosteoinduttive (la sintesidinuovoossoavvieneattraversol'attivazione dal tessuto circostante, da parte di fattori dicrescita presenti nell'innesto, di cellule mesenchimalidell'ospite e successiva trasformazione in osteoblasti).Inoltre, l'ossodi banca, prelevatodadonatore cadavereovivente (epifisi femorali),garantisce l'apportodi tuttoquelsubstrato biologico necessario al chirurgo e spesso nonfacilmente reperibile nel paziente stesso.Allo scopo diaumentare la capacità osteoinduttiva e per stimolarel'osteogenesi (sintesidinuovoossonellasededell'innesto),al tessuto osseo di banca può essere associato il gelpiastrinico. Ilgelpiastrinicoèunemocomponenteperusotopico prodotto dal sangue intero dopo opportunecentrifugazioni e costituito da plasma ricco di piastrineattivateedegranulatedopocontattocontrombinaautologae rappresenta una fonte autologa di fattori di crescita diderivazionepiastrinicaingradodistimolarelarigenerazioneosseaedi incrementare lamaturazionedegli innestiossei2.Pertanto, il gel piastrinico ed il tessutoosseodi banca
utilizzati in associazione rappresentano un prodottobiologicocompleto, estremamenteefficacenel riparare erigenerare il tessutoosseodanneggiato inalcunepatologieortopediche, quali le pseudoartrosi e i difetti ossei3-13.Scopodiquestostudioèquellodianalizzare,attraverso
una valutazione laboratoristica e clinica, l'efficacia e lasicurezzadell'associazionedi tessutoosseomorcellizzatodi banca con gel piastrinico autologo in 25 pazienticonsecutivi, sottopostiadinterventidichirurgiaortopedicaricostruttiva.Questostudioèfruttodellacollaborazionedi
Introduction
The fascinating and great progress inMedicine thatwearewitnessingandexperiencing inrecentyearshas ledtomajor developments in the field of organ and tissuetransplantation.Transplantology,nowabranchofmedicinein itsownrightalthoughwith thepeculiarityofnecessarilyrelying on co-ordination and synergismbetweenmanyhealthcaredisciplines, iscurrentlyastrategicpivotofmoreadvanced health care facilities. Within the field oftransplantology, alongside organ transplants, tissuetransplantation/grafting isgaininganevermore importantrole, both froma technico-scientific point of viewandasfar asconcerns itsbroadening therapeutic indicationsandits spreadinguse.The rapid development of tissue transplant/grafting
techniques has raised important questions and led toproblems related, on the one hand, to ethical, regulatoryandorganisational issues and, on theother hand, tomorestrictly technicalandspecialist aspects (safetyandstorageof the tissues used).Inorder to resolve theseproblems,TissueBankswere
set up throughout theworld (first in theUnitedStates andtheninEurope).TissueBankscollect,process,qualifyanddistribute high quality tissues, which nowadays are themost important biological support inmodern techniquesof reconstructive surgery. In fact, thanks to the tissuesmadeavailablebytheseBanks, reconstructivesurgeryhasprogressedgreatlyand tissuegrafting isnowanimportantsurgicaloptionenablingsubstantialanatomical, functionaland aesthetic recovery, restoring health,well-being andquality of life tomany patients1. Indeed, a new, highlyspecialised branch of medicine, called regenerativemedicine, has recently come into being. This branch ofmedicineaimsnotonly to repairdamagedtissuesbutalso,and above all, to regenerate it physiologically, thusrestoring lost function.Among the areas of surgery in which regenerative
medicine has important applications, reconstructiveorthopaedic surgery is undoubtedly one of the mostinteresting. In fact,whenbone loses its capacity for self-repair, because of the presence of a pathological bonecallus or the loss of large amount of substance followingtrauma,surgery,ordebridementinthecaseofosteomyelitis,it is essential that a stable synthesis is accompanied by avalid biological support in order that bone consolidationcantakeplace. In thesecases,whicharefar fromrare,bonefromaTissueBankrepresents avalidandsafealternativeto autologous bone grafts, since it has both
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

298
MFranchini et al
3diverse strutturedell'AziendaOspedalieradiVerona: ilServiziodiImmunoematologiaeTrasfusione, laDivisionediOrtopediaeTraumatologiadell'OspedaleCivileMaggioree la IDivisionediChirurgiaPlasticaeCentroUstioni.
Materiali e metodi
Pazienti
Dal1gennaio2002al30giugno2005,pressolaDivisionediOrtopediaeTraumatologiadell'OspedaleCivileMaggioredell'AziendaOspedalieradiVerona,25pazienticonsecutivi,affetti da pseudoartrosi, osteomielite odifetti ossei, sonostati sottoposti a trattamento ricostruttivoutilizzandogelpiastrinicoautologoetessutoosseomorcellizzatoomologo.L'etàmedia dei pazienti era di 41,8 anni (range20-86). Imaschierano19,lefemmine6,ilrapportomaschi/femmineeradi3,2.L'etàmediadeimaschi eradi37,8anni,mentrequelladellefemmineeradi52,4anni).Lecaratteristichedeipazientielepatologiedibasesono
riportatenella tabella I.Criteriodiesclusionedall'applicazionedigelpiastrinico
e ossomorcellizzato era rappresentato dalla presenza disepsi inatto.Tutti i pazienti arruolatinello studioavevanosubitoprecedentementealmenoun interventoortopediconella sede interessata (totale 35 interventi, media 1,4interventi,range1-5).Mediamente,dalmomentodeltraumaall'interventocongelpiastrinicoeossomorcellizzato,eranotrascorsi17,3mesi(range2-96mesi).
osteoconductive properties (the bone graft acts as apassive three-dimensional structurewhich favours theentranceofbloodvessels and the formationofnewbone)andosteoinductiveproperties (the synthesis of newboneoccurs through the activationof hostmesenchymal cellsin the surrounding tissue and their subsequenttransformation intoosteoblasts, botheffectspromotedbygrowth factors present in the graft). Furthermore,homologous bone (femoral epiphyses), taken from acadaveric or living donor, guarantees the presence of allthebiological substrate necessary for the surgeon,whichis often not easily obtained from the patient. In order toincrease its osteoinductive capacity and stimulateosteogenesis (the synthesis of newbone at the site of thegraft), homologous bone tissue can be combinedwithplatelet gel. Platelet gel is a blood component for topicaluse produced from whole blood after appropriatecentrifugation. It is formedofplasma rich inplatelets thathave been activated and degranulated after contactwithautologous thrombin and is an autologous source ofplatelet-derivedgrowthfactorscapableofstimulatingboneregenerationandimprovingthematurationofbonegrafts2.For this reason, the combination of platelet gel and
homologous bone from a Tissue Bank represents abiologicallycompleteproduct that isextremelyeffectiveatrepairing and regeneratingdamagedbone tissue in someorthopaedic pathologies, such as pseudoarthrosis andbonedefects3-13.Theaimofthisstudywastoanalyse, throughlaboratory
and clinical parameters, the efficacy and safety of the
Table I � The characteristics of the patients enrolled in the study
Number of patients 25Males 19Females 6Male/female ratio 3.2Mean age (range) 41.8 (20-76)Pathologies:- Pseudoarthrosis
Tibia 11Radius 1Femur 2Humerus 2Clavicle 1
- OsteomyelitisTibia 2Femur 2
- Bone defectsTibia 3Femur 1
Blood Transfus 2006; 4: 296-310

299
Gel piastrinico
Il gel piastrinico era fornito dal Servizio diImmunoematologiaeTrasfusionedell'AziendaOspedalieradiVerona. Il giornoprecedente l'intervento chirurgico, ilpaziente, previo consenso informato, veniva sottopostopresso il Servizio Trasfusionale a prelievo di 450mLdisangue intero,utilizzandounasaccaquadruplasenzafiltro(conSAG-M).Successivamente, la sacca veniva sottoposta ad una
primacentrifugazione(2.400gpmper5minutiSORVALLInstrumentsRC3C) che consentiva di separare il sangueintero inemazieconcentrate, chevenivanosubito reinfuseal paziente, e in plasma riccodi piastrine (PRP). Il PRPècostituitoapprossimativamentedel10percentodelvolumedel sangue totale prelevato e ha una conta piastrinica di500.000�3.000.000/µL.Attraversounasecondacentrifugazione(3.900gpmper
7minuti), il PRP veniva separato in plasma povero dipiastrine (PPP), che veniva conservato a �40 °C per 42giorni, e in concentrato piastrinico (CP), che venivaconservato in agitatore continuo a +22 °C per 24 ore. Ilvolume finale del concentrato piastrinco era variabile(usualmentecompresotra20e35mL),inrelazioneall'entitàdel volume finale richiesto. Su ciascun concentratopiastrinicovenivacontrollatoilnumerodei leucocitiedellepiastrinechevenivaconfrontato con idati pre-donazionedelpaziente(TabellaII).La trombina autologa veniva preparata secondo due
modalitàdifferenti.Nellaprimametodica (invigoredal1gennaio2002),venivanoprelevate2provette inACD,chevenivanocentrifugatea3.000gpmper5minuti.Al plasma così ottenuto veniva aggiunto sterilmente
(sotto cappa)Cagluconato secondo laproporzionedi0,2mLperognimLdiplasma.Ilvolumefinalevenivaincubato
combination of homologous bone chips and autologousplatelet gel in 25 consecutive patients undergoingreconstructiveorthopaedic surgery.This study is the result of collaborationbetween three
different structures inVeronaHealthCareAuthority: theService of Immunohaematology and Transfusion, theOrthopaedicsandTraumaDivisionof theOspedaleCivileMaggiore and the First Division of Plastic Surgery andBurnsCentre.
Materials andmethods
Patients
Between January 1st, 2002 and June 30th, 2005, 25consecutivepatientswithpseudoarthrosis, osteomyelitisorbonedefectsunderwent reconstructive treatmentusingautologousplateletgel andhomologousbonechips in theOrthopaedicsandTraumaDivisionof theOspedaleCivileMaggioreofVerona.Themeanageofthepatientswas41.8years(range,20-86).Therewere19males and6 females for amale/female
ratio of 3.2. Themean age of themaleswas 37.8 years,while that of the femaleswas 52.4 years). The patients'characteristics andorthopaedic pathologies are reportedin table I.Acriterion for exclusion from treatmentwithplatelet gel and bone chips was active sepsis. All thepatients enrolled in the studyhadundergone at least oneprevious orthopaedic intervention to the site concernedfor a total of35 interventions (mean1.4 interventionsperpatient; range,1-5).Themean period between the trauma and treatment
withplateletgelandbonechipswas17.3months(range,2-96months).
Table II � Characteristics of the platelet gel
Parameter Mean Standard Rangedeviation
Volume of platelet gel (mL) 28.2 ± 6.1 22-44
Patients' baseline values- Platelet count (x 103/µL) 265 ± 62.5 205-378- White cell count (x 103/µL) 6.7 ± 2.1 4-10.6
Platelet concentrate- Platelet count (x 106/µL) 3.6 ± 0.8 2.2-5.1- White cell count (x 103/µL) 18.5 ± 12.9 1.2-42.4
Platelet recovery (%) 88.1
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

300
MFranchini et al
a37°Cper15-30minuti.Dopoavertolto,sempresterilmente,il coagulo formatosi, veniva eseguita un nuovacentrifugazionea4.000gpmper5minuti e, infine,venivarecuperato il surnatante, riccodiprecursoridella trombina.Il surnatantevenivacosì stoccato incuvette sterili di 1mLciascuna e congelato a �40 °C. Dall'1 gennaio 2004 latrombinaautologavenivapreparatausandounaappositaprovettacontente trombina (S-Monovette®,SarstedtAG,Verona, Italia).Tale provetta è dotata di stantuffo che varimossoappenaconclusoilprelievo(9mLdisangue).Dopocentrifugazionea4.000gpmper5minuti, laprovettavenivastoccata a temperatura inferiore a �40 °C.Almomentodell'utilizzo la provetta era scongelata a temperaturaambientepercirca30-60minutie,dopoaversvitatoil tappoavite,venivaprelevatoconunasiringailsierosopranatantericcodi trombina.Ilgiornosuccessivoalprelievo, insalaoperatoria, ilgel
piastrinico veniva prodotto in contenitori sterili,aggiungendoaogni7mLdiCP,1mLdi trombinaautologaed1mLdiCagluconatofinoadottenereilvolumerichiesto.Sfruttando la proporzione 7:1:1, si ottiene il volumedesideratocheè, ingenere, di20-30mLtotali.La figura1riporta le fasidellaproduzionedelgelpiastrinico.
Osso morcellizzato
LaBanca dei Tessuti della RegioneVeneto, sede diVerona (inserita nel Servizio di Immunoematologia eTrasfusionedell'AziendaOspedalieradiVeronaecertificataUNIENISO9001:2000dall'aprile2003)hasviluppatounprotocollo per la donazione, la validazione e l'utilizzo ditessutomuscolo-scheletrico osseo da donatore vivente(epifisi femorali). Il protocollodellaBancadeiTessuti diVeronaè suddivisonelle seguenti 3 fasi successive.
Fase pre-operatoriaValutazione dell'idoneità alla donazione da parte del
medicoortopedico, comprendente il consenso informatoalla donazione, il questionario anamnestico, ladocumentazioneclinica, laboratoristica(emocromo, indicidi flogosi, funzionalitàepaticae renale,proteine totali conelettroforesi proteica, sierologia della lue e markerssierologicidiHBV,HCV,HIV)estrumentale(radiografiadeltorace)delpaziente/donatore.Ilgiornodelprelievovengonoinviati alla Banca dei Tessuti campioni di sangue deldonatore per l'esecuzione di:ALT; gruppo sanguigno;screeningsierologicoemolecolareper ivirusHBV,HCV,HIV;sierologiadellalue;ricercadianticorpiperHTLV1/2eperCMV.
Platelet gel
The platelet gel was supplied by the Service ofImmunohaematology andTransfusion (SIT) ofVeronaHospital.Thedaybefore theplannedsurgery, a sampleof450mLofwholebloodwaswithdrawnfromthepatientonceheor shehadgiven informedconsent.Thebloodwascollected intoaquadruplebagwithout
afilter(withSAG-M).Thebagwasthencentrifugedforthefirst time(2,400rpmfor5minutesSORVALLInstrumentsRC3C) in order to separate thewhole blood into red cellconcentrate,whichwas immediately re-infused into thepatient,andplatelet-richplasma(PRP).ThePRPconstitutedapproximately 10 percent of the total of whole bloodwithdrawnandhadaplateletcountof500,000�3,000,000/µL.Bymeans of a second centrifugation (3,900 rpm for 7minutes), thePRPwasseparated intoplatelet-poorplasma(PPP),whichwas stored at �40 °C for up to 42days, andplatelet concentrate (PC),whichwasmaintained undercontinuousagitationat+22°Cfor the following24hours.Thefinalvolumeof thePCvaried(usuallybetween20and35mL) in relation to the final volume required for theintervention.Thenumbersof leucocytesandplateletsweremeasuredineachPCandthesevalueswerecomparedwiththepatient's pre-donationvalues (Table II).Theautologousthrombinwaspreparedintwodifferent
ways. In the firstmethod (used since January 1st, 2002),twosampleswerecollectedintotest-tubescontainingACD,whichwerecentrifugedat3,000rpmfor5minutes.Calciumgluconatewasaddedundersterileconditions
(underahood) to theplasma thusobtained inaproportionof0.2mLforevery1mLofplasma.Thefinalvolumewasincubatedat37°Cfor15-30minutes.Afterhavingremoved,again under sterile conditions, the clot that forms, theproductwascentrifugedagainat4,000rpmfor5minutes.Finally, the supernatant, rich in thrombinprecursors,wasrecovered. The supernatant was stored in 1mL sterilecuvettes and frozenat�40°C.FromJanuary 1st, 2004 the autologous thrombinwas
prepared using a specific test-tube containing thrombin(S-Monovette®,SarstedtAG,Verona, Italy).This test-tubehas a plunger that is removed from the needle once thebloodwithdrawalhasbeencompleted(9mLof blood).Aftercentrifugationat4,000rpmfor5minutes, thetest-tubewasstoredata temperaturebelow�40°C.At the timeofuse, itwas thawedat roomtemperature forabout30-60minutesand,afterhavingunscrewedthescrewcap, thesupernatantserumrich in thrombinwascollectedwithasyringe.Theday after the collectionof thePC, theplatelet gel
Blood Transfus 2006; 4: 296-310

301
Fase intra-operatoriaL'epifisi femorale viene prelevata sterilmente in sala
operatoriae,dopoavereseguitountamponedellasuperficieossea e della spongiosa e una biopsia ossea per esamecolturale,vieneposizionatain4contenitorisuccessivi(primadoppiosacchettodimaterialeplasticosterile,quindidoppiocontenitore in plastica rigida con chiusura ermetica);
Figure 1 - Preparation and use of the platelet gel
wasproduced insterile containers in theoperating theatrebyadding1mLofautologousthrombinand1mLofcalciumgluconatetoevery7mLofPCtoreachtherequiredvolume.Thefinalvolumenecessary,whichisusually20-30mL,wasachieved maintaining this 1:1:7 proportion. Figure 1illustrates the stages of productionof platelet gel.
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

302
MFranchini et al
all'esternodell'ultimocontenitorevienepostaun'etichettaidentificativa.L'epifisi femoraleviene,quindi, inviataallaBancadeiTessuti,unitamenteallabiopsia,altamponeosseoealladocumentazionediaccompagnamento(comprendenteconsenso informato, questionario anamnestico,documentazioneclinica,esamidi laboratorioestrumentalibasali,idoneitàalladonazione,verbalediprelievoincuivienedatal'idoneitàanatomicadell'epifisifemorale).L'epifisi,dopoesserestataidentificataconunappositocodice,vienequindiposta inuncongelatorededicato(contenente tessutoosseoinattesadivalidazione)a�80°C.
Validazione del tessuto osseoLaBancadeiTessuti, sullabasedelladocumentazione
consegnatadalmedicoortopedicoedell'esitodegli esamilaboratoristiciecolturali,pone ilgiudiziofinaledi idoneitàdell'epifisi femorale.Vieneeseguito, inoltre,unoscreeningmolecolareperivirusHBV,HCVeHIVadalmeno15giornididistanzadalprelievo.Unavoltavalidato, il tessutovienetrasferito inunappositocongelatorea�80°C,contenentetessutomuscolo-scheletricovalidatoprontoper l'evasione.La morcellizzazione del tessuto osseo avviene
utilizzandounappositomorcellizzatoremeccanico(Howex100,BoneMill,Gävle,Svezia)con3tipidilamedautilizzarein base alle dimensioni delle chips di spongiosa che sivoglionoottenere.Unavoltadecorticata l'epifisi femorale,questavienetrituratamediante ilmorcellizzatore. Il tessutomorcellizzatoottenutoviene lavatoabbondantementeconfisiologica sterile (sacca riscaldata a 37 °C), inmododaeliminarecelluleematicheeadiposeresidue.Siottengonocosì dellechipsdi tessutocortico-spongiosodeldiametrodi 2-3mm.Si creanoaliquotedi 10-20-30gchevengonoimbustate sterilmente in triplabusta sottovuotomedianteuna sigillatrice.Daogni lotto processato vienepreparataun'aliquotadimorcellizzatoper ilcontrollomicrobiologico(germiaerobi,anaerobiemiceti)post-irradiazione.Lebustedi morcellizzato vengono quindi stoccate a �80 °C esuccessivamente inviate alladittaGammaraddiBolognaperl'irraggiamentoaraggigamma(25kGy).Comecontrollodell'avvenuto irradiamento si utilizzano sia indicatoribiologici (spore di Bacillus pumilus) che indicatoricolorimetrici (bollino).Almomento dell'utilizzo in salaoperatoria, il tessuto morcellizzato viene scongelatorapidamenteconsoluzionefisiologicaa37°Ce,unavoltaaperti i3 involucri,vienepostosterilmente inunabacinellacontenente una soluzione antibiotica. Si esegue, inoltre,un prelievo bioptico per il controllo microbiologico.Successivamente, almorcellizzato viene aggiunto il gelpiastrinico e si forma, così, un prodotto di consistenza
Bone chips
TheTissueBank of theRegion ofVeneto, located atVerona (within theService of Immunohaematology andTransfusionofVeronaHospital;UNIENISO9001:2000certificationfromApril2003)hasdevelopedaprotocol forthedonation,validationanduseofmusculo-skeletalbonetissuefromlivingdonors(femoralepiphyses).Theprotocolof the Verona Tissue Bank covers the following threestages.
Pre-operative stageThepatient/donor suitability fordonation is evaluated
by theorthopaedic surgeonbasedon informedconsent tothe donation, assessment of the patient's history, clinicalrecords, laboratory tests (full blood count, markers ofinflammation, liverfunctiontests, renal functiontests, totalproteins with electrophoresis, syphilis serology andserologicalmarkersofHBV,HCVandHIVinfection)andinstrumental investigations (chestX-rays).Thedayof thebone donation, samples of the donor's blood are sent tothe Tissue Bank for the following tests: ALT; bloodgrouping; serological andmolecular screening forHBV,HCV, and HIV; syphilis serology, and searches forantibodiestoHTLV1/2andCMV.
Intra-operative stageThe femoral epiphysis is removed under sterile
conditions in theoperating theatreand,afterhaving takenswabsof the surfaceof theboneand the spongiosumandtaken abonebiopsy for culture, is put into a four-layeredcontainer (first a double sterile plastic bag, then ahermetically sealeddouble container of rigid plastic); anidentifyinglabelisplacedontheoutsideofthemostexternalcontainer.The femoral epiphysis is thensent to theTissueBank, togetherwith the biopsy, the bone swabs and theaccompanying documentation (including the informedconsent, clinical history questionnaire, clinicaldocumentation, baseline laboratory and instrumentalinvestigations, suitability for donation, and report of thecollectionof thebone inwhich the anatomical suitabilityof the femoralepiphysis is stated).Theepiphysis, labelledwith a specific code, is then placed in a specific freezer(containingbone tissueawaitingvalidation)at�80°C.
Validation of the bone tissueOn the basis of the documentation provided by the
orthopaedic surgeon and the outcome of the laboratoryandmicrobiologicalexaminations, theTissueBankissues
Blood Transfus 2006; 4: 296-310
303
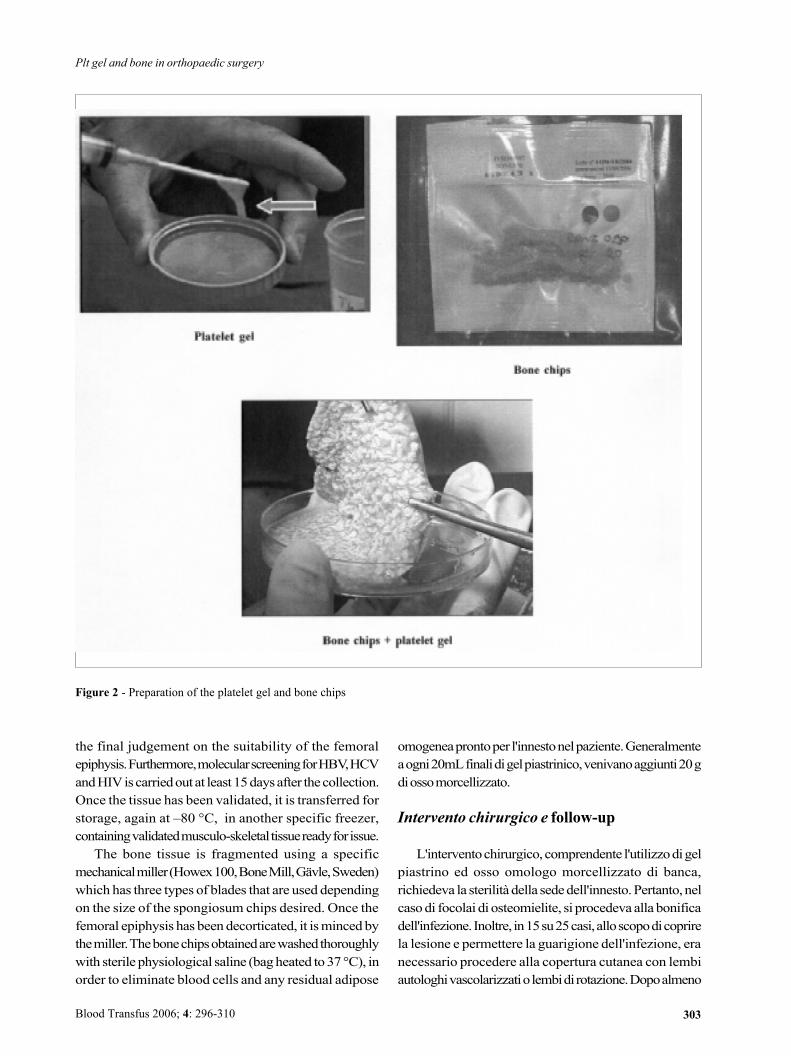
omogeneaprontoper l'innestonelpaziente.Generalmenteaogni20mLfinalidigelpiastrinico,venivanoaggiunti20gdiossomorcellizzato.
Intervento chirurgico e follow-up
L'interventochirurgico, comprendente l'utilizzodigelpiastrino ed osso omologo morcellizzato di banca,richiedeva la sterilitàdella sededell'innesto.Pertanto, nelcasodi focolai di osteomielite, si procedeva alla bonificadell'infezione. Inoltre, in15su25casi,alloscopodicoprirela lesione e permettere la guarigione dell'infezione, eranecessario procedere alla copertura cutanea con lembiautologhivascolarizzatiolembidirotazione.Dopoalmeno
Figure 2 - Preparation of the platelet gel and bone chips
the final judgement on the suitability of the femoralepiphysis.Furthermore,molecularscreeningforHBV,HCVandHIViscarriedout at least15daysafter thecollection.Once the tissue has been validated, it is transferred forstorage, again at �80 °C, in another specific freezer,containingvalidatedmusculo-skeletaltissuereadyforissue.The bone tissue is fragmented using a specific
mechanicalmiller(Howex100,BoneMill,Gävle,Sweden)which has three types of blades that are used dependingon the size of the spongiosum chips desired. Once thefemoral epiphysis has beendecorticated, it ismincedbythemiller.Thebonechipsobtainedarewashedthoroughlywith sterile physiological saline (bagheated to37 °C), inorder to eliminate blood cells and any residual adipose
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

304
MFranchini et al
Figure 3 - Filling of a post-traumatic bone defect
Blood Transfus 2006; 4: 296-310
305
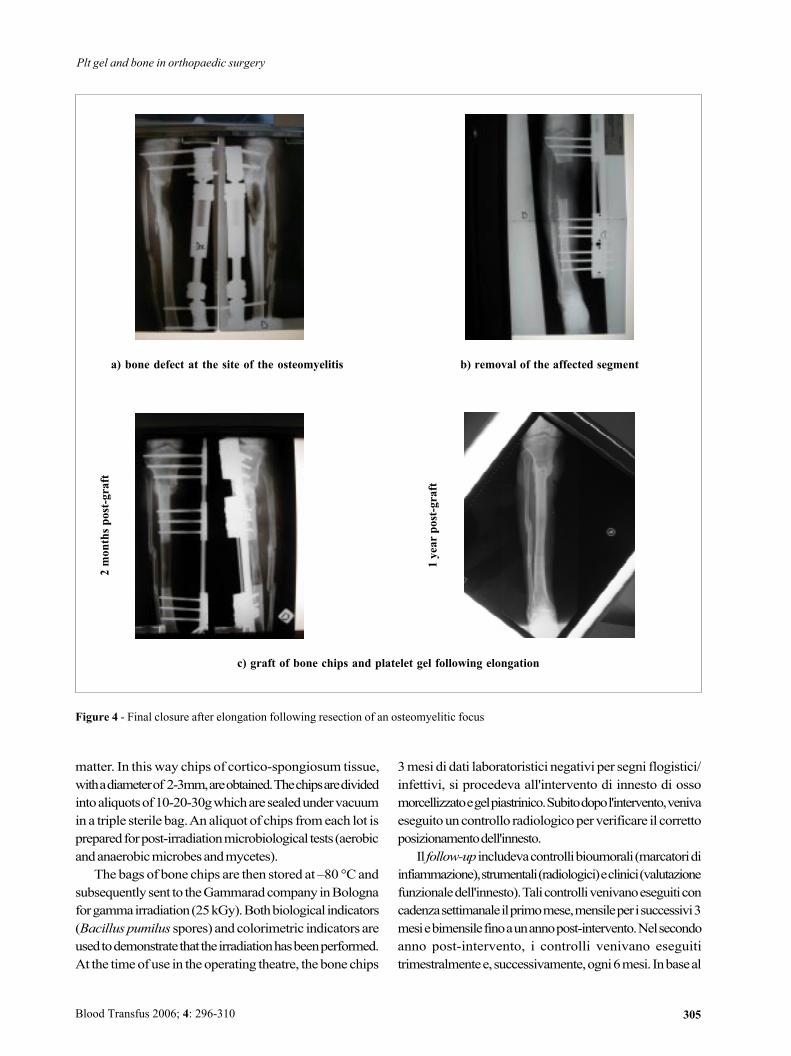
a) bone defect at the site of the osteomyelitis b) removal of the affected segment
c) graft of bone chips and platelet gel following elongation
2monthspost-graft
1yearpost-graft
Figure 4 - Final closure after elongation following resection of an osteomyelitic focus
3mesi di dati laboratoristici negativi per segni flogistici/infettivi, si procedeva all'intervento di innesto di ossomorcellizzatoegelpiastrinico.Subitodopol'intervento,venivaeseguitouncontrollo radiologicoperverificare il correttoposizionamentodell'innesto.Il follow-up includevacontrollibioumorali(marcatoridi
infiammazione),strumentali(radiologici)eclinici(valutazionefunzionaledell'innesto).Talicontrollivenivanoeseguiticoncadenzasettimanaleilprimomese,mensileperisuccessivi3mesiebimensilefinoaunannopost-intervento.Nelsecondoanno post-intervento, i controlli venivano eseguititrimestralmentee,successivamente,ogni6mesi. Inbaseal
matter. In thisway chips of cortico-spongiosum tissue,withadiameterof 2-3mm,areobtained.Thechipsaredividedintoaliquotsof10-20-30gwhicharesealedundervacuumin a triple sterile bag.Analiquot of chips fromeach lot ispreparedforpost-irradiationmicrobiological tests (aerobicandanaerobicmicrobesandmycetes).The bags of bone chips are then stored at �80 °Cand
subsequently sent to theGammaradcompany inBolognaforgammairradiation(25kGy).Bothbiological indicators(Bacilluspumilus spores) andcolorimetric indicators areusedtodemonstratethattheirradiationhasbeenperformed.At the timeofuse in theoperating theatre, thebonechips
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

306
MFranchini et al
risultatodeicontrolli, l'esitodell'innestovenivagiudicato:buono(totaleripristinodideambulazionee/omotilitàarticolare,assenzadisegnidiinfezione/flogosi,dimostrazioneradiologicadiunacompletaintegrazionedell'innestoconiltessutoosseocircostante),soddisfacente(ripristinodelladeambulazioneconparzialedeficitarticolare,cheperònoninficiavalanormalevita di relazione, assenza di segni di infezione/flogosi,documentazioneradiologicadiunacompleta integrazionedell'innesto con il tessuto osseo circostante) o negativo(mancatoripristinofunzionale,presenzadiinfezioni,mancataintegrazioneradiologicadell'innesto).
Risultati
I valori medi riguardanti il volume dei concentratipiastrinici raccolti, e la relativa conta piastrinica eleucocitariasonoriportatinella tabellaI.Laconcentrazionemedia piastrinica pre-donazione nei pazienti era di265x103/µL,mentre la concentrazionepiastrinicanelCPottenutoeradi3,6x106/µL,conunaresafinaledell'88,1%.Itipi di intervento cui erano stati sottoposti i 25 pazientierano i seguenti: chiusura finale (end-point) dopoallungamentopost-resezionedi focolai osteomielitici (4casi), riempimentodidifetti osseipost-traumatici (4casi),riempimentodidifetti osseidopo toilettedipseudoartrosi(17 casi). Il follow-upmedio post-intervento era di 16,9mesi (range 3-42 mesi). In 15/25 casi (60%), l'esitodell'intervento era considerato buono: infatti, in questipazienti, al terminedelperiododi follow-up, persistevanol'assenzadisegnilaboratoristicidiinfezione/infiammazioneeilcompletoripristinodelladeambulazionee/odellamotilitàarticolare. Parallelamente, a livello radiologico,l'osteointegrazione dell'innesto era documentata dallaprogressiva dissoluzione della trama granulare e dallagradualeriduzionedellaradio-opacitàchediventavasimileaquelladell'ossocircostante.In10/25casi(40%)ilrisultatodell'innesto si poteva considerare soddisfacente, dalmomentochealterminedelperiododifollow-uppersisteva,inassenzadi segnidi infiammazione/flogosie inpresenzadi una buona osteointegrazione dell'innesto, un parzialedeficit di deambulazionee/odellamotilità articolare, chenoncomprometteva,comunque,lanormalevitadirelazione.In un caso di intervento di chiusura dell'end-point, dopoallungamento post-resezione di focolaio osteomieliticotibialepost-traumatico,sièdovutoricorrereall'amputazionedellagambaperlaricomparsadell'osteomielite,8mesidopol'innesto.Va, tuttavia, sottolineato che il nuovo focolaioosteomieliticosiera formato inunazonadiversadaquella
are thawedrapidlywithphysiological salineat37°Cand,once the threecovershavebeenopened,areplaced,understerile conditions, in a bowl containing an antibioticsolution.Furthermore,asampleistakenformicrobiologicaltests.Subsequently thebonechipsareaddedto theplateletgel formingaproductofhomogeneousconsistencyreadyforgrafting into thepatient.Usually20gofbonechipsareadded toevery20mLof the finalplateletgel.
The surgical intervention and follow-up
The site into which the graft of platelet gel andhomologousbonechips is placedmust be sterile.Thus, in thecaseof fociofosteomyelitis, thesiteof the
infectionwasthoroughlycleaned.Furthermore, in15of25cases, in order to cover the lesion and enable healing ofthe infection, it was necessary to cover the defect withautologous vascularised skin flaps or flaps placed byrotation.Theboneallograftwithplateletgelwasperformedat least 3 months after laboratory test for markers ofinflammationor infectionwerenegative.Immediatelyafter theoperationa radiological control
was performed to check the correct position of the graft.The follow-up included biohumoral (markers ofinflammation), instrumental (radiological) and clinical(functionalevaluationof thegraft)controls.Thesecontrolswerecarriedoutweekly in thefirstmonth,monthlyfor thenext 3months and then every2months up to ayear aftertheoperation. In thesecondyearafter surgery thecontrolswere carried out every 3months and then, subsequently,every6months.Depending on the results of these controls, the
outcomeof thegraftwas judged: good (total recoveryofambulation and/or jointmobility, no signs of infection/inflammation, radiological demonstration of completeintegration of the graft with the surrounding bone),satisfactory (recovery of ambulationwith a partial jointdeficit, not affecting normal life behaviours, no signs ofinfection/inflammation, radiological documentationof acompleteintegrationofthegraftwiththesurroundingbone)or negative (lack of functional recovery, presence ofinfections, lackof radiologicallydemonstrated integrationof thegraft).
Results
Themeanvolumeof thePCcollectedandtheirplateletandwhitecellcountsarereported in table I.Themeanpre-
Blood Transfus 2006; 4: 296-310

307
dell'innesto di ossomorcellizzato e gel piastrinico, che,invece,mostravanounabuonaosteointegrazione.Pertanto,tale complicanza era da attribuirsi allamalattia primitivapiuttosto che all'innesto stesso. La figura 3 mostra ilriempimentocongelpiastrinicoedossomorcellizzatodiundifettoosseopost-traumatico.Lafigura4mostralachiusurafinale (end-point) dopo allungamento post-resezione difocolaiosteomielitici.
Discussione e conclusioni
Il gel piastrinico, emocomponente ad uso nontrasfusionale,èentrato,ormaidaqualcheanno,nell'attivitàroutinaria dimolti Servizi Trasfusionali.Grazie alle sueproprietàrigenerativeeriparativetessutali,essoèutilizzatocon frequenza sempremaggiore inchirurgia ricostruttivaortopedica,maxillo-faccialeeodontostomatologicaenelleulcerecronichedivarianatura.Lecaratteristichebiologichedelgelpiastrinico sonoessenzialmentedovuteall'elevataconcentrazionedi fattoridicrescita (Tabella III), contenutinegliα-granulipiastrinicieliberatiunavoltachelepiastrinevanno incontro ad attivazione edegranulazione14-21. Talifattoridicrescita,capacidistimolarelareplicazionedicelluledi originemesenchimale come fibroblasti, osteoblasti ecellule endoteliali sono: platelet derived growth factor(PDGF), transforminggrowthfactor-beta(TGF-β),epitelialgrowthfactor(EGF), fibroblastgrowthfactor(FGF),insulingrowthfactorIeII(IGFI-II)eplateletderivedangiogenesisfactor (PDAF)14. Inoltre, un ruolo importante nellariparazione e rigenerazione ossea è svolto dalle bonemorphogenetic proteins (BMP), costituite da peptidiosteoinduttivi di derivazione piastrinica, appartenenti algruppodelTGF-β.Daunpuntodivistafisiologico,siritienechenelsitodella lesionecisiaunrilascio inizialediPDGF,TGF-β e IGF I e II, per effettodella degranulazionedellepiastrine presenti in loco. Il PDGFstimola, da un lato, lamitosidellecellulestaminalimesenchimalipresentinell'osso
donation platelet concentration in the patients was265x103/µL,while theplateletconcentrationinthePCwas3.6x106/µL,withafinalyieldof88.1%.The25patients underwent the followingoperations:
final closure after elongation following resection ofosteomyelitic foci (4cases), fillingofpost-traumaticbonedefects (4 cases), and filling of bone defects followingtoilette of pseudoarthrosis (17cases).Themeandurationof thepost-operativefollow-upwas
16.9months (range, 3-42months). In15/25cases (60%),theoutcomeof theoperationwasconsideredgood: in fact,in these patients, at the end of the period of follow-uptherewerestillnolaboratorysignsofinfection/inflammationandtherewascompleterecoveryofambulationand/orjointmobility. In parallel, osteointegration of the graft wasradiologicallydemonstratedbytheprogressivedissolutionof thegranularweaveandby thegradual reductionof theradio-opacity, which became similar to that of thesurroundingbone. In 10/25 cases (40%) the result of thegraft could be considered satisfactory, given that, at theendof the follow-upperiod,apartialdeficit inambulationand/or joint mobility persisted, although this did notcompromisenormal lifebehaviours,while therewerenosignsof infection/inflammationandgoodosteointegrationof the graft.Amputation of a leg was necessary in onepatientbecauseoftherecurrenceofosteomyelitis8monthsafter thegraft.This patient had undergone a final closure after
elongation following the resection of a post-traumaticosteomyelitic focus in the tibia. It should, however, benoted that the new osteomyelitic focus developed in adifferentareafromthatofthegraftofbonechipsandplateletgel,which, in contrast, showedgood integration.Thus, this complicationwas attributed to theprimary
disease rather than to thegraft. Figure3 shows the fillingof apost-traumaticbonedefectwithplatelet gel andbonechips. Figure 4 shows the final closure after elongationfollowingresectionofosteomyelitic foci.
Table III � Growth factors present in platelet gel and their functions
- PDGF (platelet-derived growth factor): stimulates mitosis and angiogenesis � regulates the activity of other growth factors forfibroblasts and osteoblasts.
- TGF-β (transforming growth factor-beta): stimulates fibroblasts and preosteoblasts and inhibits endothelial cells, epithelial eellsand osteoclasts.
- EGF (epithelial growth factor): stimulates mesenchymal and epidermal cells.- FGF (fibroblast growth factor): angiogenic factor.- IGF I � II (insulin growth factors I and II): increase osteoblasts and the deposition of bone.- PDAF (platelet-derived angiogenesis factor): angiogenic factor.
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

308
MFranchini et al
e, dall'altro, ha un effetto angiogenetico, inducendo epotenziandolaformazionedinuovivasinellesedidilesione.Contemporaneamente,pereffettodelTGF-β , siassiste
alla proliferazione di fibroblasti, in grado di depositarematrice collagene per sostenere la crescita vasale, e pro-osteoblasti,che,a lorovolta, sidifferenzianoinosteoblasti,responsabili della produzione di matrice ossea.Successivamente, il rilascio di IGF I e II agisce sugliosteoblasti dell'endostio, che iniziano così a riempire letrabecoledell'ossospugnoso. Inoltre, laneoformazionedivasi sanguigni è in grado di veicolare altre piastrineprovenienti dal torrente circolatorio, automantenendo, intalmodo, il processodi rifornimentodei fattori di crescitanecessari21. Tuttavia, la rigenerazione del tessuto osseonecessita,oltrechedicelluleosteoprogenitrici (fibroblasti,osteoblasti e condrociti) e di fattori di crescita, anche diunamatriceosteoinduttiva, laquale, andando incontroadunlentoprocessodidissoluzioneadoperadegliosteoclasti,regolailrilasciocontrollatodeifattoridicrescitaincorporatiinessa.Talematricepuòessere sintetica (idrossiapatite)ocostituitada tessutoosseoumano(autologoodomologo).Inparticolare, inquestiultimianni, l'ossoomologodibancaè stato utilizzato con successo in chirurgia ortopedica emaxillo-facciale ricostruttiva.Anche nel nostro studio,l'ossoomologomorcellizzatosièrivelatomoltoefficacenelpromuovererapidamenteiprocessi riparativierigenerativiossei.Esso inoltre, pur essendoomologo, si è dimostratodotato di una scarsissima antigenicità a causa sia delprocesso di congelamento (�80 °C) che del processo diirraggiamento (25 kGy) cui è stato sottoposto primadell'innesto.Questo trattamentosiè rivelatofondamentaleneldeterminare l'ottimaosteointegrazionedell'innestoneltessutoosseodel ricevente22,23. Per quanto riguarda il gelpiastrinico,confrontandoinostridaticonquelli riportati inletteratura, laconcentrazionepiastrinicanelprodottofinaleè risultata particolarmente elevata. Questa evidenza hasicuramente contribuito all'efficacia dellametodica, dalmomentochelaconcentrazionefinaledeifattoridicrescitaè direttamente proporzionale alla quantità di piastrinedegranulate nel gel stesso. Inoltre, da un punto di vistachirurgico, il gel piastrinico ha conferito una notevolecompattezzaeplasticitàall'ossomorcellizzatodainnestare,accrescendo così lamaneggevolezza intraoperatoria delmaterialebiologicodainnestareefavorendone,intalmodo,il suocorrettoposizionamentoall'internodeldeficitosseo.L'esitodegli innesti, cheèstatobuonoosoddisfacente
nella totalità dei casi, documenta l'efficacia dellaassociazione tra gel piastrinico e osso di banca, sia interminiclinici/funzionali chedi integrazionecon il tessuto
Discussion and conclusions
Supplyingplatelet gel, a bloodcomponent for topicalrather thantransfusionaluse,hasnowbeenroutinepracticeforseveralyears inmanyTransfusionServices.Thanks toitspropertiesof regeneratingandrepairing tissues,plateletgel is beingusedeverymore frequently in reconstructiveorthopaedic surgery,maxillo-facial surgery,dentistryandthe treatment of chronic ulcers of various causes. Thebiologicalpropertiesofplateletgelarebasicallydue to thehighconcentrationsofgrowthfactors(TableIII),containedin the plateletα-granules, which are released once theplateletsareactivatedanddegranulated14-21.Thesegrowthfactors, able to stimulate the replication of cells ofmesenchymal origin such as fibroblasts, osteoblasts andendothelialcells,are:plateletderivedgrowthfactor(PDGF),transforminggrowthfactor-beta(TGF-β),epithelialgrowthfactor(EGF),fibroblastgrowthfactor(FGF),insulingrowthfactors I and II (IGF I and II) and platelet-derivedangiogenesis factor (PDAF)14. Furthermore, bonemorphogeneticproteins(BMP),whichareplatelet-derivedosteoinductivepeptidesbelonging to thegroupofTGF-β,playanimportantroleinbonerepairandregeneration.Fromaphysiological point of view, it is thought that there is aninitialreleaseofPDGF,TGF-β andIGFIandIIatthesiteofthe lesion, through theeffect ofdegranulationofplateletspresent in loco.PDGFstimulatesmitosisofmesenchymalstemcells in the bone and also has an angiogenic effect,inducingandpotentiating the formationofnewvessels inthe site of the lesion.At the same time, TGF-β inducesproliferation of fibroblasts (which deposit the collagenmatrixable to supportvesselgrowth)andpro-osteoblasts(which differentiate into osteoblasts responsible for theproductionofbonematrix).Subsequently, thereleasedIGFI and II act on the osteoblasts of the endostium, whichstarts to fill the trabeculae of the spongy bone.Furthermore, thenewly formedbloodvessels enable thedeliveryofotherplatelets fromthebloodstream, thusself-maintaining thenecessary supplyofgrowth factors21.However, regenerationofbonetissuerequiresnotonly
progenitorcells (fibroblasts,osteoblastsandchondrocytes)andgrowth factors, but alsoanosteoinductivematrix.Byundergoinga slowprocessofdissolutionunder theeffectof osteoclasts, thematrix regulates the controlled releaseofgrowthfactors incorporatedwithinit.Thismatrixcanbyartificial (hydroxyapatite) or formed of human bone(autologousorhomologous). In recentyearshomologousbone fromTissueBanks has been usedwith success inorthopaedic surgery and reconstructivemaxillo-facial
Blood Transfus 2006; 4: 296-310

309
osseo ospite. Tuttavia, la dimostrazione di un realevantaggio osteogenico del gel piastrinico richiede unostudio randomizzatocontrollato.Pertanto, ulteriori studi,possibilmente sucasistichepiùampie, sononecessari perconfermare i nostri positivi risultati. Il fatto, comunque,che i pazienti inclusi in questo studio fossero affetti dagravi patologie ossee e fossero già stati sottoposti anumerosi interventi senza successo, testimoniaulteriormente l'efficaciadiquestametodica.Inconclusione, ilnostrostudiorappresentaunesempio
di sinergismopluridisciplinare,nelquale specializzazionidiverse(chirurgiaortopedica,chirurgiaplasticaemedicinatrasfusionale) cooperano tradi loro.Solamenteattraversouna stretta ed armonica collaborazione si possonocrearequellepremesseche,daunlato,portanoallacrescitaumanae culturale del personale sanitario coinvolto e, dall'altro,permettonodiraggiungereinmodoottimalequellocheèloscopodellamedicina rigenerativa: ilmiglioramentodellaqualitàdivitadeipazienti.
Riassunto
Premessa. La medicina rigenerativa è un settore dellamedicina sorto recentemente, il cui obiettivo non è solo quellodi riparare tessuti danneggiati ma anche quello di rigenerarliin modo da ripristinare la loro funzionalità originaria.Pazienti. Inquestostudioabbiamovalutato l'efficacia
del gel piastrinico, emocomponente per uso nontrasfusionale, e tessuto osseomorcellizzato omologo dibanca in 25 pazienti consecutivi, sottoposti a variinterventi di chirurgia ortopedica ricostruttiva, pressolaDivisionediOrtopediaeTraumatologiadell'OspedaleCivileMaggioredell'AziendaOspedalieradiVerona,pergravi patologie ossee quali pseudoartrosi, osteomieliti,difetti ossei.Risultati.Nella totalitàdeicasi trattati si sonoottenuti
risultati buoni o soddisfacenti, sia da un punto di vistalaboratoristico-strumentale che clinico-funzionale.Pertanto, tale metodica combinata si è dimostrataestremamente efficace nel trattamento rigenerante diqueste complessepatologieossee.Conclusioni.Questi risultati eccellenti si sonopotuti
ottenere solamente grazie ad un sinergismo tra diversespecializzazioni, quali la chirurgia ortopedica, lachirurgia plastica e lamedicina trasfusionale.
Parole chiave: gel piastrinico, ossomorcelizzato,chirurgiaortopedica,medicinarigenerativa.
surgery. Inour study,homologousbonechipswere foundtobevery efficient in rapidlypromoting theprocesses ofbone repair and regeneration.Furthermore, despitebeinghomologous, bone chips appear to be extremelyweaklyantigenic because of both the freezing (�80 °C) andirradiation (25 kGy), that they undergo before grafting.These treatmentswere found to be fundamental for theexcellent integrationof thegraftwith the recipient's bonetissue22,23.As far as regards the platelet gel, the platelet
concentrations in the final products we used wereparticularly high compared to those reported in theliterature.Thisundoubtedlycontributed to theefficacyoftheprocedure,given that the finalconcentrationofgrowthfactors is directly proportional to the amount ofdegranulatedplatelets in thegel.Fromasurgicalpointofview, theplateletgelconferred
notable compactness and plasticity to the bone chips,increasingtheintra-operativemanageabilityofthebiologicalmaterial to graft and, in thisway, facilitating the correctplacementof thegraftwithin thebonedefect.Theoutcomeof thegrafts,whichwasconsidered tobe
goodorsatisfactory inall cases,documents theefficacyofthe combination of platelet gel and bone chips in bothclinical and functional terms and with regards to theintegrationof thegraftwithhostbonetissue.Nevertheless,a randomisedcontrolled trial is necessary todemonstratethe real osteogenic advantage of the platelet gel. For thisreason, further studies, possibly on larger numbers ofpatients, are needed to confirmour positive results. Thefact, however, that thepatients included in this studyhadsevere bone disorders and had already undergonenumerous operations without success, bears furtherwitness to the efficacy of the combination of bone chipsandplateletgel.In conclusion, our study is an example of
multidisciplinarysynergism, inwhichdifferentspecialties(orthopaedic surgery, plastic surgery and transfusionmedicine)co-operatetogether.Onlyclosecollaborationcanlay thebases forprofessional andpersonal enrichmentofthehealthcarestaff involvedaswellas theachievementoftheaimof regenerativemedicine: the improvementof thepatients' qualityof life.
Plt gel and bone in orthopaedic surgery
Blood Transfus 2006; 4: 296-310

310
1) Franchini M, Gandini G,Aprili G. La donazione e il prelievodi tessuti. In: Condividere la Vita. Donazione e Trapianti diOrgani e Tessuti.Conoscenze, Opinioni, Vissuti Psicologici.Edizioni Libreria Cortina Verona, 2005 pag, 149-55.
2) Borzini P, Mazzucco L, Cattana E. Platelet gel: clinical useand unanswered questions. Blood Transf 2004; 2: 10-4.
3) Franchini M, Dupplicato P, Ferro I, et al. Efficacy of plateletgel in reconstructive bone surgery. Orthopedics 2004; 28:161-3.
4) Caloprisco G, Borean A, Mele A. Il gel piastrinico: come equando. In: Progressi in Emaferesi. Lezioni del VII corsonazionale di aggiornamento in emaferesi. Cortona 8-9April2002. Pag. 39-51.
5) Autori Vari. Il gel piastrinico e la colla di fibrina: unaconfermata competenza della Medicina Trasfusionale. IlSevizio Trasfusionale, 31, September � October 2002.
6) Rocca G, Savonitto P, Franchini M, et al. L'utilizzo del gelpiastrinico nelle pseudoartrosi, difetti ossei e nell'allungamentodegli arti. Abstract. 89° Congresso Società Italiana diOrtopedia e Traumatologia. Naples, 24-28 October 2004.
7) Biggi F, CalopriscoG, ScorranoA. L'utilizzo di gel piastrinicoautologo in ortopedia e traumatologia (3 anni di esperienze).Abstract. 89° Congresso Società Italiana di Ortopedia eTraumatologia. Naples, 24-28 October 2004.
8) Vecchio S, Oliverio F, Sirianni G, GeremiccaW. Esperienzanell'utilizzo del gel piastrinico nel trattamento dellapseudoartrosi.Abstract. Convegno Interregionale dei ServiziTrasfusionali del Centro-Sud. Catania, 23-25 October 2003.
9) Tremiterra E, Bovenzi D, LoffredoA, et al.Applicazione delgel piastrinico in chirurgia ortopedica. Abstract. ConvegnoInterregionale dei Servizi Trasfusionali del Centro-Sud.Catania, 23-25 ottobre 2003.
10) Vecchio S, D'Ettoris A, Leonardo P, et al. Il gel piastriniconella pratica clinica. Abstract. Convegno Interregionale deiServizi Trasfusionali del Centro-Sud. Rome, 5-7May 2005.
11) Vitello P, Di Gregorio P. Emocomponenti per uso nontrasfusionale: il gel piastrinico. Abstract. ConvegnoInterregionale dei Servizi Trasfusionali delCentro-Sud.Rome,5-7 May 2005.
12) Rughetti A, Flamini S, Colafarina O, et al. Closed surgery:
autologous platelet gel for the treatment of pseudoarthosis.Blood Transf 2004; 2: 37-43.
13) Turrini A, Gandini AR, Olzer D, et al. Studio preliminaredell'utilizzo del gel piastrinico autologo in chirurgia ortopedicae maxillo-facciale. Convegno Interregionale dei ServiziTrasfusionali del Nord, Trento, 22-24 May 2003.
14) Slater M, Patava J, Kingham K, Mason R. Involvement ofplatelets in stimulating osteogenic activity. J Orthop Res1995; 13: 655-63.
15) Zimmermann R, Jakubietz R, Jakubietz M, et al. Differentpreparation methods to obtain platelet components as asource of growth factors for local application. Transfusion2001; 41: 1217-24.
16) Aldegheri R, Dupplicato P,Agostini S, et al. Ruolo dei fattoridi crescita autologhi nella chirurgia ossea ricostruttiva. GiorIt Ort Traumatol 2002; 28: 157-65.
17) Cametti S, Causero A, Corso L, et al. Ruolo dei fattori dicrescita nella rigenerazione ossea: nostra esperienza.Abstract.89° Congresso Società Italiana di Ortopedia e Traumatologia.Naples, 24-28 October 2004.
18) Lieberman IR, Daluiski A, Einhorn TA. The role of growthfactors in the repair of bone. Biology and clinical applications.J Bone Joint SurgAm 2002; 84-A: 1032-44.
19) Slater M, Patava J, Kingham K, Mason RS. Involvement ofplatelets in stimulating osteogenic activity. J Orthop Res1995; 13: 655-63.
20) Burnouf T, Radosevich M, Goubran HA. Local hemostaticblood products: fibrin sealant and platelet gel. TreatHemophilia 2004; 36: 1-7.
21) DiMaggioN, Lucarelli E, BeccheroniA, et al. Il plasma riccodi piastrine promuove la neoangiogenesi in vivo. Abstract.89° Congresso Società Italiana di Ortopedia e Traumatologia.Naples, 24-28 October 2004.
22) Mizutani A, Fujita T, Watanabe S, et al. Experiments onantigenicity and osteogenicity in allotransplanted cancellousbone. Int Orthop. 1990; 14: 243-8.
23) ShashaN,Krywulak S, BacksteinD, et al. Long-term follow-up of fresh tibial osteochondral allografts for failed tibialplateau fractures. J Bone Joint SurgAm 2003; 85-A Suppl 2:33-9.
References
Blood Transfus 2006; 4: 296-310
MFranchini et al