original article influence of gender and economic status
TRANSCRIPT

1634
This is an open access article distributed in accordance with the Creative Commons Attribution (CC BY 4.0) license: https://creativecommons.org/licenses/by/4.0/) which permits any use, Share — copyOPEN ACCESS
OPEN ACCESSOPEN ACCESS
and redistribute the material in any medium or format, Adapt — remix, transform, and build upon the material for any purpose, as long as the authors and the original source are properly cited. © Copyright: Author(s)
International Journal of Medicine in Developing Countries
Influence of gender and economic status on the level of Saudi awareness towards coronary artery diseases risk factors and its positive modificationsFaisal S. Alahmari1, Fras W. Alhijli1, Mohammed A. Alfadhel1, Khaled A. Alkhudhairi1, Sultan A. Aljohani1, Mohammad R. Alshammri2*
ABSTRACT
Background: Coronary artery disease (CAD) has been a significant cause of mortality in Saudi Arabia in recent years. The objective of the present study is to evaluate the influence of gender and economic status on Saudi awareness of CAD risk factors and their positive modifications.
Methods: A cross-sectional study was conducted distributing an online digital questionnaire at Imam Mohamed-Ibn-Saud University in Riyadh, Saudi Arabia. The sample size was estimated to assume that 50% is the expected prevalence, 95% confidence level, and 5% margin of error resulting in 384 individuals.
Results: The study included 406 participants, 274 (67.5%) were males, and 132 (32.5%) were females aged 17-35 years with a mean age of 21 years. Around 83.3% (84% males and 82% females) believed that tobacco smoking was a risk for CAD. About 90.4% (60.6% males and 91.7% females) believed that physical inactivity was a risk for CAD. About 87% (89% males and 83% females) believed that regular fast-food intake was a risk for CAD. About 67% (69% males and 63% females) believed that regular soft drink intake was a risk for CAD.
Conclusion: The awareness levels toward CAD modifiable risk factors were relatively low among people in Imam Mohammad Ibn Saud Islamic University. Gender difference had an insignificant role in the level of aware-ness. There were somewhat higher CAD modifiable risk factors rates among the studied population, increasing with a decrease in monthly income. The population had a strong welling to modify their risk status.
Keywords: Heart disease, coronary artery disease, heart attack, obesity, hypertension, diabetes.
Introduction
Coronary artery disease (CAD), which is also known as ischemic heart disease, and atherosclerotic cardiovascular disease, is the third leading cause of death worldwide and is linked to 17.8 million global deaths. Patients with CAD usually present with myocardial infarction and ischemic cardiomyopathy [1,2]. CAD represents around 55% of heart failure causes in the middle east compared to around 70% in the western world [3]. However, there is a paucity of data regarding the epidemiology of CAD from Saudi Arabia. Previous reports showing that the overall prevalence of CAD was 5.5% in Saudi Arabia [4]. In Saudi Arabia, CAD is more frequent among men (74.8%) compared to women (25.2%) and predominantly among adults >50 years (72%) [5]. Most CAD patients present with ST-elevation myocardial infarction associated with
diverse risk factors [6]. The most common reported CAD risk factors in Saudi Arabia are diabetes mellitus (DM), hypertension, tobacco smoking, obesity, hyperlipidemia, and former heart disease [7,8]. Therefore, the present study was aimed to assess the influence of gender and economic status on Saudi awareness towards CAD risk factors and their positive modifications.
Correspondence to: Mohammad R. Alshammri*Department of Internal Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia.Email: [email protected] list of author information is available at the end of the article.Received: 26 July 2021 | Accepted: 12 September 2021
Faisal S. Alahmari et al, 2021;5(9):1634–1640.https://doi.org/10.24911/IJMDC.51-1627327523
ORIGINAL ARTICLE

Influence of gender and economic status on the level of Saudi awareness toward CAD
1635
Subjects and Methods
This was a cross-sectional survey that involved distributing an online digital questionnaire, conducted in the capital of Saudi Arabia, “Riyadh”, with a target population specifically in Imam Mohamed-Ibn-Saud University. The questionnaire was handed out to participants in an online fashion using a convenient sampling technique. The data thus obtained from the survey were used to evaluate the knowledge of established risk factors of CAD among the participants. All students and faculty members from all ethnicities aged above 18 years were included in the study. Those diagnosed with CAD and pregnant women were excluded. The sample size was estimated to assume that 50% is the expected prevalence, 95% confidence level, and 5% margin of error resulting in 384 individuals. After obtaining the university’s IRB approval, those who agreed to participate were handed over an electronic survey tool to fill out the questionnaire. The questionnaire included three dimensions of knowledge, attitude, and practice toward CAD risk factors and intentions to modify them. In addition to the demographic and general information, it consisted of 26 questions (demographic and general info = 7, knowledge = 14, attitude = 1, practice = 11). The questions were multiple choices, varying on the nature of the question, while some of them included yes/no while others required specific answers with or without explanation. The members of the research group developed the questionnaire; therefore, it is yet to be validated. The awareness of CAD was arbitrarily defined as positive if a given respondent recognized six or more risk factors in the response questionnaire. Descriptive analysis was performed to describe the demographics of participants. The inferential analysis was utilized to assess the association between participants’ demographics and the prevalence of risk factors knowledge of CAD and modify them. Significance of association was tested using the Chi-Square test or Fisher’s Exact test, wherever applicable.
Results
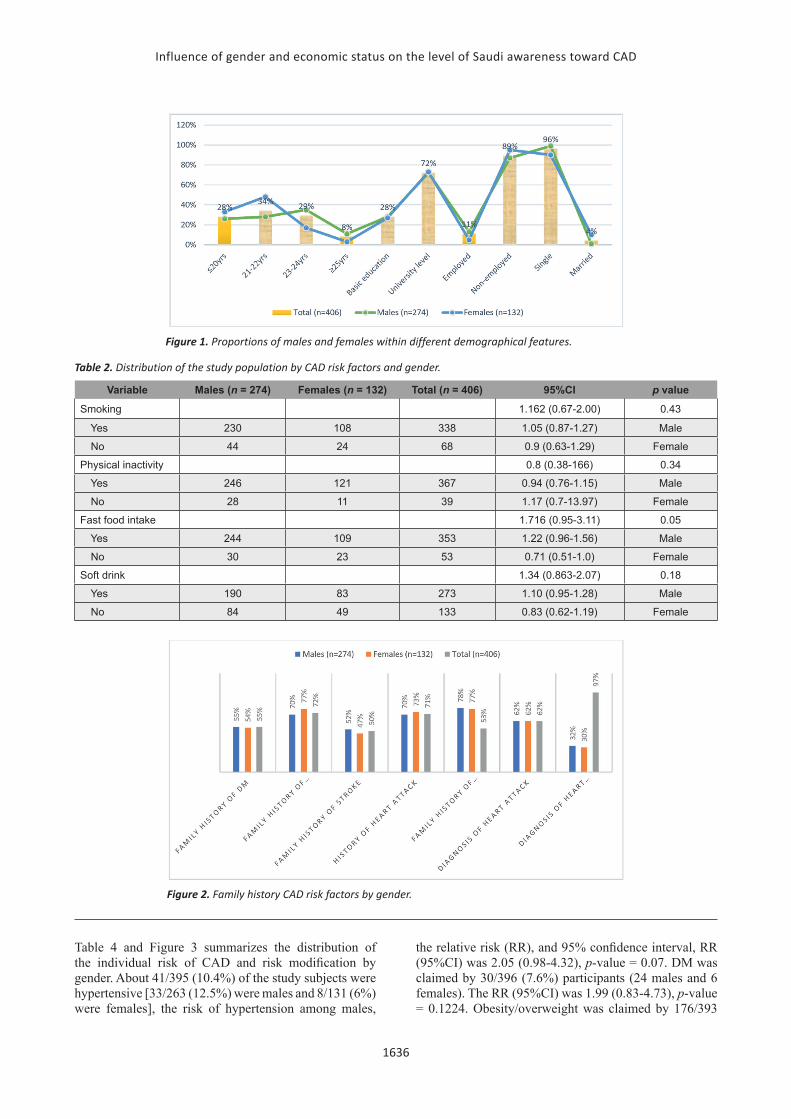
Out of the 406 respondents, 274 (67.5%) were males, and 132 (32.5%) were females aged 17-35 years with a mean age of 21 years. About 292/406 (72%) were university students, and the remaining 114/406 (28%) were with basic education levels. Out of 114 persons, 43/114 (38%) were employed in the university. Most of the participants were single-marital status 389/406 (96%), as described in Table 1. The distribution of the males and females revealing different proportions within different demographical features, as indicated in Figure 1.
Table 2 and Figure 2 summarizes the distribution of the study population by CAD risk factors and gender. Around 338/406 (83.3%) [230/274 (84%) males and 108/132 (82%)] females participants believed that tobacco smoking was a risk for CAD. The positive association and 95% confidence interval was 1.162 (0.67-2.00). About 367/406 (90.4%) [246/274 (60.6%) males and 121/132 (91.7%) females] participants believed that physical inactivity was a risk for CAD. About 353/406 (87%) [244/274 (89%) males and 109/132 (83%) females] participants believed that regular fast-food intake was a risk for CAD. About 273/406 (67%) [190/274 (69%) males and 83/132 (63%) females] participants believed that regular soft drink intake was a risk for CAD.
As summarized in Table 3 and Figure 2, about 223, 294, 205, 288, and 317 participants believed that family history of DM, hypertension, stroke, history of heart attack, and family history of hyperlipidemia, in that order. The proportions were comparative between males and females, as shown in Figure 2. About 253 participants (171 males & 82 females) agreed that diagnosis of heart attack was a strong risk factor. About 128 participants (88 males & 40 females) agreed that heart disease diagnosis was a strong risk factor, as indicated in Table 3 and Figure 2.
Table 1. Distribution of the study population by demographical characteristics.
Variable Males (n = 274) Females (n = 132) Total (n = 406)Age ≤20 years 71 43 114
21-22 77 63 140
23-24 96 22 118
≥25 30 4 34
Education Basic education 78 36 114
University level 196 96 292
Employment status Employed 36 7 43
Non-employed 238 125 363
Marital status Single 270 119 389
Married 4 13 17
Influence of gender and economic status on the level of Saudi awareness toward CAD
1636
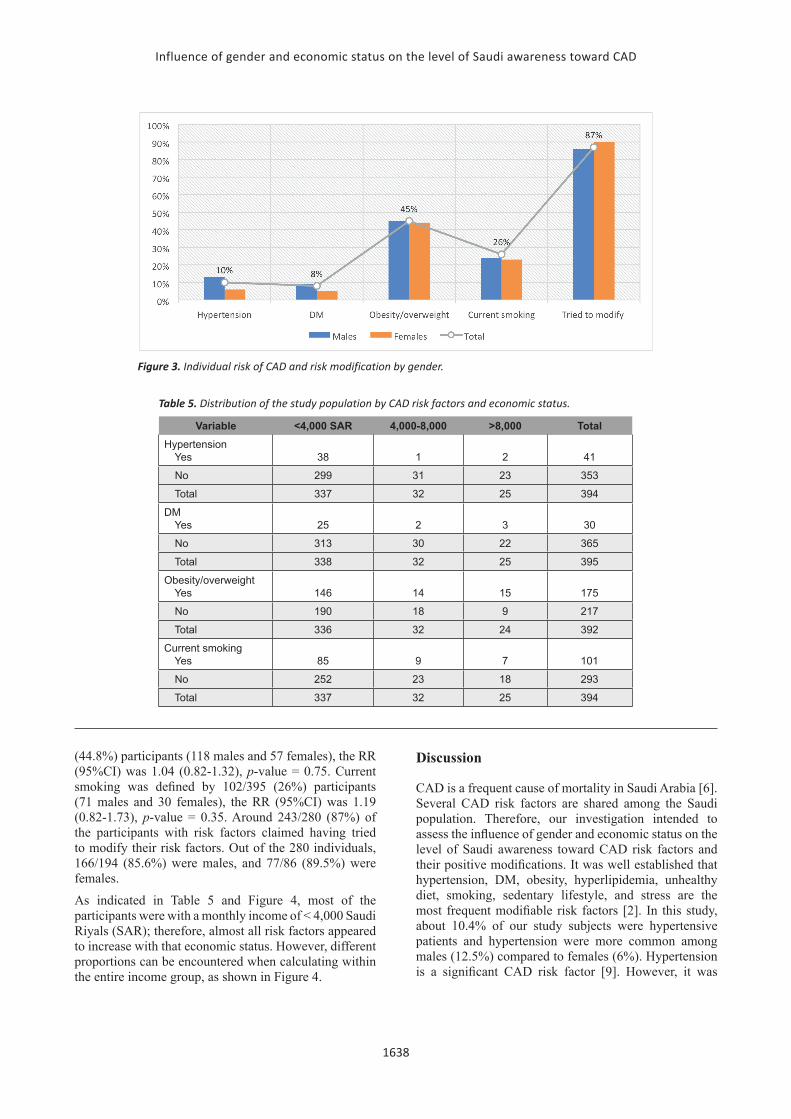
Table 4 and Figure 3 summarizes the distribution of the individual risk of CAD and risk modification by gender. About 41/395 (10.4%) of the study subjects were hypertensive [33/263 (12.5%) were males and 8/131 (6%) were females], the risk of hypertension among males,
the relative risk (RR), and 95% confidence interval, RR (95%CI) was 2.05 (0.98-4.32), p-value = 0.07. DM was claimed by 30/396 (7.6%) participants (24 males and 6 females). The RR (95%CI) was 1.99 (0.83-4.73), p-value = 0.1224. Obesity/overweight was claimed by 176/393
Figure 1. Proportions of males and females within different demographical features.
Table 2. Distribution of the study population by CAD risk factors and gender.
Variable Males (n = 274) Females (n = 132) Total (n = 406) 95%CI p value
Smoking 1.162 (0.67-2.00) 0.43
Yes 230 108 338 1.05 (0.87-1.27) Male
No 44 24 68 0.9 (0.63-1.29) Female
Physical inactivity 0.8 (0.38-166) 0.34
Yes 246 121 367 0.94 (0.76-1.15) Male
No 28 11 39 1.17 (0.7-13.97) Female
Fast food intake 1.716 (0.95-3.11) 0.05
Yes 244 109 353 1.22 (0.96-1.56) Male
No 30 23 53 0.71 (0.51-1.0) Female
Soft drink 1.34 (0.863-2.07) 0.18
Yes 190 83 273 1.10 (0.95-1.28) Male
No 84 49 133 0.83 (0.62-1.19) Female
Figure 2. Family history CAD risk factors by gender.

Influence of gender and economic status on the level of Saudi awareness toward CAD
1637
Table 4. Distribution of the individual risk of CAD and risk modification by gender.
Variable Males (n = 274) Females (n = 132) Total (n = 406) RR (95%CI), p-valueHypertension Male versus Females (M vs. F)
Yes 33 8 41 2.05 (0.98-4.32), 0.07
No 230 123 354
DM M versus F
Yes 24 6 30 1.99 (0.83-4.73), 0.1224
No 240 125 366
Obesity/overweight M versus F
Yes 118 57 176 1.04 (0.82-1.32), 0.75
No 143 74 217
Current smoking M versus F
Yes 71 30 102 1.19 (0.82-1.73), 0.35
No 191 102 293
Risk modification
No risk 80 46 126
Tried to modify the risk 106 77 243
Not tried 28 9 37
Table 3. Distribution of the study population by family history CAD risk factors and gender.
Variable Males (n = 274) Females (n = 132) Total (n = 406)
Family history of DM
Yes 152 71 223
No 122 61 183
Family history of hypertension
Yes 192 102 294
No 82 30 112
Family history of stroke
Yes 143 62 205
No 131 70 201
History of heart attack
Yes 191 97 288
No 83 35 118
Family history of hyperlipidemia
Yes 215 102 317
No 59 30 89
Diagnosis of heart attack
Yes 171 82 253
No 103 50 153
Diagnosis of heart disease
Yes 88 40 128
No 186 92 278
Influence of gender and economic status on the level of Saudi awareness toward CAD
1638
(44.8%) participants (118 males and 57 females), the RR (95%CI) was 1.04 (0.82-1.32), p-value = 0.75. Current smoking was defined by 102/395 (26%) participants (71 males and 30 females), the RR (95%CI) was 1.19 (0.82-1.73), p-value = 0.35. Around 243/280 (87%) of the participants with risk factors claimed having tried to modify their risk factors. Out of the 280 individuals, 166/194 (85.6%) were males, and 77/86 (89.5%) were females.
As indicated in Table 5 and Figure 4, most of the participants were with a monthly income of < 4,000 Saudi Riyals (SAR); therefore, almost all risk factors appeared to increase with that economic status. However, different proportions can be encountered when calculating within the entire income group, as shown in Figure 4.
Discussion
CAD is a frequent cause of mortality in Saudi Arabia [6]. Several CAD risk factors are shared among the Saudi population. Therefore, our investigation intended to assess the influence of gender and economic status on the level of Saudi awareness toward CAD risk factors and their positive modifications. It was well established that hypertension, DM, obesity, hyperlipidemia, unhealthy diet, smoking, sedentary lifestyle, and stress are the most frequent modifiable risk factors [2]. In this study, about 10.4% of our study subjects were hypertensive patients and hypertension were more common among males (12.5%) compared to females (6%). Hypertension is a significant CAD risk factor [9]. However, it was
Figure 3. Individual risk of CAD and risk modification by gender.
Table 5. Distribution of the study population by CAD risk factors and economic status.
Variable <4,000 SAR 4,000-8,000 >8,000 TotalHypertension Yes 38 1 2 41
No 299 31 23 353
Total 337 32 25 394
DM Yes 25 2 3 30
No 313 30 22 365
Total 338 32 25 395
Obesity/overweight Yes 146 14 15 175
No 190 18 9 217
Total 336 32 24 392
Current smoking Yes 85 9 7 101
No 252 23 18 293
Total 337 32 25 394

Influence of gender and economic status on the level of Saudi awareness toward CAD
1639
reported that the hypertension is higher among males in some studies, others showing reverse findings which might be attributed to the specific sociodemographic characteristics [10,11]. Other risk factors including DM, obesity/overweight, and tobacco smoking represented 7.6% (8.8% in males and 4.5% in females), 44.8% (43% males vs. 43% females), and 26% (26% males vs. 23% females), in that order. Obesity/overweight and smoking are relatively similar for both genders; hence, hypertension and DM showing elevations among males.
The present investigation’s findings show a statistically insignificant association between smoking, physical inactivity, and soft drink intake awareness as modifiable CAD risks. Also, there was no gender difference. However, most participants believed that regular fast-food intake could be a modifiable risk for CAD, which was statistically significant. Moreover, males were more aware than females. In this context, a study from Saudi Arabia has shown that the Saudi population has a low level of awareness regarding the like between CAD and modifiable risks, such as tobacco smoking, physical inactivity, soft drink, and fast food [12]. Nevertheless, low awareness levels among both (males and females) were determined for family history of DM, family history of hypertension, family history of stroke, heart attack history, and hyperlipidemia. Such findings were recently reported from Saudi Arabia. The study showed a significantly low level of awareness towards CAD risk factors and a high prevalence of CAD modifiable risk factors [13]. The present study’s findings revealed that a reasonable number of participants with risk factors has tried to modify their risk with females more than males. Such results may necessitate the introduction of sustainable health awareness programs.
Conclusion
The awareness levels toward CAD modifiable risk factors are relatively low among Imam Mohammad Ibn Saud Islamic University. Gender difference had an
insignificant role in the level of awareness. There were somewhat higher CAD modifiable risk factors rates among the studied population, increasing with a decrease in monthly income. The population had a strong welling to modify their risk status.
List of AbbreviationsCAD Coronary artery disease DM Diabetes mellitus IMSIU Imam Mohammad Ibn Saud Islamic University
Conflict of interestsThe authors declare that there is no conflict of interest regarding the publication of this paper.
FundingNone.
Consent to participateInformed consent was obtained from all the participants.
Ethical approvalEthical approval was obtained from the Institutional Review Board at Imam Mohammad Ibn Saud Islamic University, Riyadh via reference number 59-2020 dated: 09-07-2020
Author detailsFaisal S. Alahmari 1, Fras W. Alhijli1, Mohammed A. Alfadhel1, Khaled A. Alkhudhairi1, Sultan A. Aljohani1, Mohammad R. Alshammri2
1. College of Medicine, Imam Muhammad ibn Saud Islamic University, Riyadh, Saudi Arabia
2. Department of Internal Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia
References
1. Khan MAB, Hashim M, Mustafa H, Baniyas MY, Al Suwaidi SK, AlKatheeri R, et al. Global epidemiology of ischemic heart disease: results from the global burden of disease study. Cureus. 2020;12(7): e9349. https://doi.org/10.7759/cureus.9349
Figure 4. Study population by CAD risk factors within the entire economic status.

Influence of gender and economic status on the level of Saudi awareness toward CAD
1640
2. Brown JC, Gerhardt TE, Kwon E. Risk factors for coronary artery disease [Internet]. StatPearls [Internet]. U.S. National Library of Medicine; 2021 [cited 2020 Jun 6]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554410/
3. Elasfar AA, Alhabeeb W, Elasfar S. Heart failure in the Middle East Arab countries: current and future perspectives. J Saudi Heart Assoc. 2020;32(2):236241. https://doi.org/10.37616/2212-5043.1040
4. Al-Nozha MM, Arafah MR, Al-Mazrou YY, Al-Maatouq MA, Khan NB, Khalil MZ, et al. Coronary artery disease in Saudi Arabia. Saudi Med J. 2004;25(9):1165–71.
5. Aldosari KH, Alkhathlan KM, Al-Ghamdi S, Abdelhamid Elshaer FE, Karrar MH, Aldawsari AM. Pattern of coronary arterial lesions amongst Saudi Arabians: a cross-sectional coronary fluoroscopic angiography study. Pan Afr Med J. 2020;18;36:21. https://doi.org/10.11604/pamj.2020.36.21.21423
6. Khaled S, Almalki M, Shalaby G, Niazi AK, Ahmed S, Alsilami A, et al. Epidemiological variation of acute myocardial infarction relevant to in-hospital outcomes-tertiary center experience-Saudi Arabia. J Saudi Heart Assoc. 2020;32(3):340–9. https://doi.org/10.37616/2212-5043.1139
7. Kinsara AJ, Alsaleh A, Taher ZA, Alshamiri M, Elshaer F Sr. The primary management strategies for ST-elevation myocardial infarction patients in Saudi Arabia: a sub-study of the Saudi acute myocardial infarction registry. Cureus. 2020;12(11):e11783. https://doi.org/10.7759/cureus.11783
8. Sheikh MSA. Role of plasma soluble lectin-like oxidized low-density lipoprotein receptor-1 and microRNA-98
in severity and risk of coronary artery disease. Balkan Med J. 2021;38(1):13–22. https://doi.org/10.5152/balkanmedj.2021.20243
9. Weber T, Lang I, Zweiker R, Horn S, Wenzel RR, Watschinger B, et al. Hypertension and coronary artery disease: epidemiology, physiology, effects of treatment, and recommendations: a joint scientific statement from the Austrian Society of Cardiology and the Austrian Society of Hypertension. Wien Klin Wochenschr. 2016;128(13-14):467–79. https://doi.org/10.1007/s00508-016-0998-5
10. Rai RK, Kumar C, Singh PK, Singh L, Barik A, Chowdhury A. Incidence of prehypertension and hypertension in rural India, 2012-2018: a sex-stratified population-based prospective cohort study. Am J Hypertens. 2020;33(6):552–62. https://doi.org/10.1093/ajh/hpaa034
11. Cao YJ, Qi SF, Yin HS, Zhang F, Shi WW, Gao JC, et al. Prevalence, awareness, treatment and control of hypertension in elderly residents in Hebei province. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(3):296–300.
12. Almalki MA, AlJishi MN, Khayat MA, Bokhari HF, Subki AH, Alzahrani AM, et al. Population awareness of coronary artery disease risk factors in Jeddah, Saudi Arabia: a cross-sectional study. Int J Gen Med. 2019;12:63–70. https://doi.org/10.2147/IJGM.S184732
13. Alruways AFH, Alotaibi NA, Rashikh MA, Alnufeie AA, Alshammari YJD, Alharthy MR, et al. Awareness and prevalence of coronary artery disease risk factors among Saudi adults in Dawadmi, Riyadh province: a cross-sectional study. J Family Med Prim Care. 2020;9(11):5629–37. https://doi.org/10.4103/jfmpc.jfmpc_934_20