original article open access -...
TRANSCRIPT

Evaluation of Femoral Neck Anteversion using Digital RadiographyOriginal Article
Recent Advances in Arthroplasty© All rights are reserved by Vipin Sharma et al.
ISSN 2576-6716
*Address for Correspondence: Dr. Vipin Sharma, Department of Orthopedics, Dr Rajendra Prasad Government Medical College, HP, INDIA. E-mail: [email protected]
Received: September 20, 2017; Accepted: October 25, 2017; Published: October 26, 2017.
Vipin Sharma1*, Krishna Kumar2 and Pawan K Soni3 1, 2Department of Orthopedics, Dr. Rajendra Prasad Govt. Medical College, Himachal Pradesh, India.3Department of Radio diagnosis, Dr. Rajendra Prasad Govt. Medical College, Himachal Pradesh, India.
AbstractBackground: Femoral neck anteversion is an important parameter of proximal femoral geometry. Not only it has an anthropologi-cal value but also it gives an insight into possible underlying hip pathology.Aims of the study: The present study was conducted with an aim to measure femoral neck anteversion values in Sub Himalyan population of North West India using digital radiography.Materials and Methods: This was a prospective hospital based study carried out to study the average femoral neck anteversion in Sub Himalyan population of North West India. Digital radiography was used to measure anteversion in 89 femora. The results obtained were statistically analysed. Results: The mean femoral neck anteversion by digital radiography method was 14.70±2.26. Males had higher anteversion values when compared to females in both groups which was statistically nonsignificant.Conclusion: The data from this study would help establish values of femoral neck anteversion for Sub Himalayan population of North West India and help in planning orthopaedic surgeries like osteotomies about the hip and total hip replacement.Keywords: Femur, Hip Joint; Radiography; Torsion Abnormality.
Introduction The anteversion angle (declination) of the femur neck is the angle
formed by the femoral condylar plane (bicondylar plane) and a plane passing through the center of the neck and femoral head [1]. The orientation of bicondylar plane to femoral neck axis differentiates between anteversion and retroversion. This bicondylar plane passing posterior to femoral neck axis indicates anteversion while this plane passing anterior to neck axis indicates retroversion [2]. Femoral neck anteversion is highest at birth (36° ) and progressively decreases with age to an adult value of about 16 degree; the value of regression being about 1.5(0.2-3.1) degree / year [3]. It is important to know the true value of these anthropometric parameters of proximal femur in our population and its relationship to values obtained by various other methods in different studies [4]. Anteversion values are important from clinical point of view as well as these give us an insight into various possible pathologies like hip and knee osteoarthritis and labral hip pathology [4]. Many methods are available for measuring femoral neck anteversion which include clinical examination, fluoroscopy, radiography, Ultrasonography, CT and MRI [1, 5]. Because of the wide variation in health infrastructure in our country, it may not always be possible to measure femoral neck anteversion by CT and MRI. Hence in the present study femoral neck anteversion of subhi-malayan population of North West India was measured using digital radiography.
Aims and Objectives
The present study aimed to evaluate femoral neck anteversion of proximal femur in patients using digital Radiography and any variations of these measurements attributable to age and gender.
Material and Methods
This prospective hospital-based study was conducted at a tertiary care institute after due ethical approval, over a period of one year. Patients in age group 20-60 years presenting to department of orthopaedics who gave written consent to participate in the study were included, while patients with age less than 20 years, fracture proximal shaft of femur, fracture of neck/ head of femur, old operated patients with above mentioned fractures, patients with deformity in the hip and osteo arthritis of hip and knee were excluded.
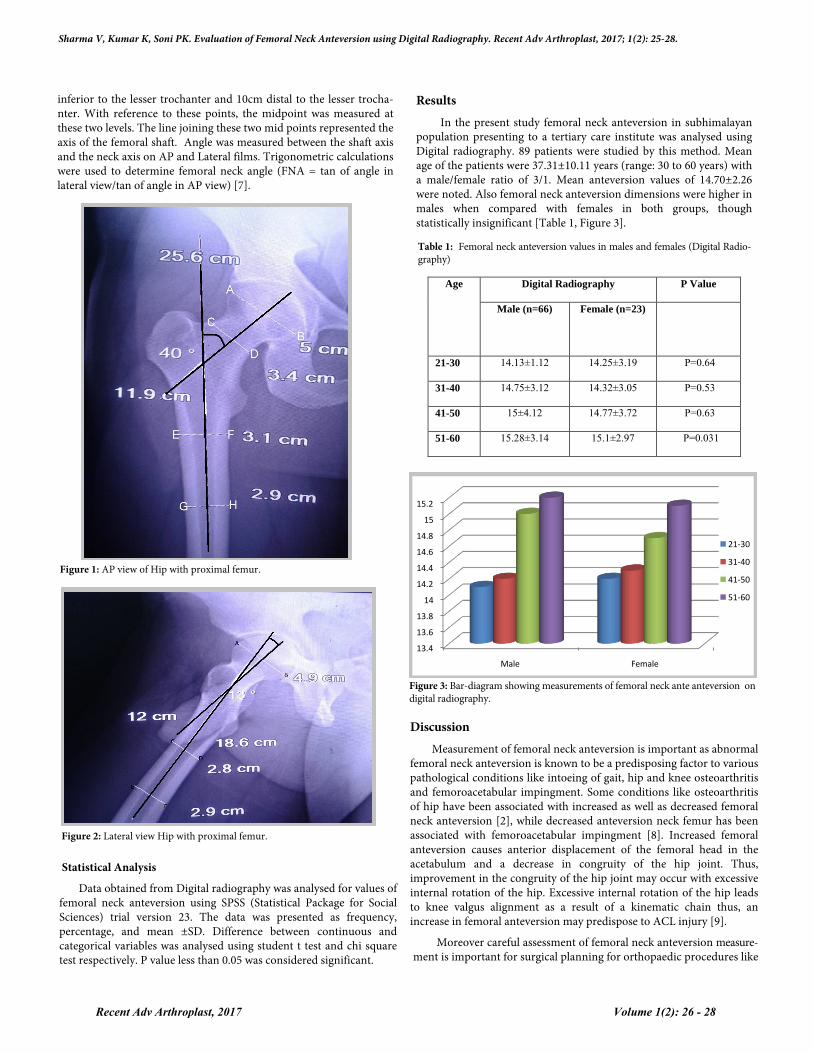
89 consecutive patients were analysed for femoral neck anteve-rsion on digital radiographs. Patients were enrolled and subjected to detailed history and clinical examination. Biplanar X-ray method described by Ogata et al. was used to calculate the femoral neck anteversion [6]. Femoral condylar axis was made parallel to the table by placing the patient supine with the knees flexed to 90° over the edge of the table and the legs suspended down. X-ray tube was centred over femoral neck and an AP film was taken with beam perpendicular to table [Figure 1]. Subsequently hip was flexed to 90 degree and rotated externally till the entire lateral aspect of the leg touched the table and lateral view of femoral neck taken. This position rotated the femur to 90°on its long axis and the condylar axis became perpendicular to the table [Figure 2]. Neck axis was defined by marking two points each at widest diameter of head and base of neck; and their mid points marked .The central axis of the neck was located on each film by a line connecting these two mid points .Two points were taken at outer cortex of shaft femur on both sides; just
Recent Adv Arthroplast, 2017 Volume 1(2): 25 - 28
but another meta-analysis found that while the posterior minimal incision THR results in a significant decrease in surgical duration, blood loss and hospital stay, it is not clear whether mini incision THR in general is superior to standard incision THR [39].
MIS approachesApart from the skin incision, the damage caused in other soft
tissues (fascia, muscles, tendons) and the risk of complications from nerves and vessels also determines the invasiveness of the procedure.
Sharma V, Kumar K, Soni PK. Evaluation of Femoral Neck Anteversion using Digital Radiography. Recent Adv Arthroplast, 2017; 1(2): 25-28.
Results In the present study femoral neck anteversion in subhimalayan
population presenting to a tertiary care institute was analysed using Digital radiography. 89 patients were studied by this method. Mean age of the patients were 37.31±10.11 years (range: 30 to 60 years) with a male/female ratio of 3/1. Mean anteversion values of 14.70±2.26 were noted. Also femoral neck anteversion dimensions were higher in males when compared with females in both groups, though statistically insignificant [Table 1, Figure 3].
inferior to the lesser trochanter and 10cm distal to the lesser trocha-nter. With reference to these points, the midpoint was measured at these two levels. The line joining these two mid points represented the axis of the femoral shaft. Angle was measured between the shaft axis and the neck axis on AP and Lateral films. Trigonometric calculations were used to determine femoral neck angle (FNA = tan of angle in lateral view/tan of angle in AP view) [7].
Figure 1: AP view of Hip with proximal femur.
Figure 2: Lateral view Hip with proximal femur.
Statistical Analysis
Data obtained from Digital radiography was analysed for values of femoral neck anteversion using SPSS (Statistical Package for Social Sciences) trial version 23. The data was presented as frequency, percentage, and mean ±SD. Difference between continuous and categorical variables was analysed using student t test and chi square test respectively. P value less than 0.05 was considered significant.
13.4
13.6
13.8
14
14.2
14.4
14.6
14.8
15
15.2
Male Female
21-30
31-40
41-50
51-60
Age Digital Radiography P Value
Male (n=66) Female (n=23)
21-30 14.13±1.12 14.25±3.19 P=0.64
31-40 14.75±3.12 14.32±3.05 P=0.53
41-50 15±4.12 14.77±3.72 P=0.63
51-60 15.28±3.14 15.1±2.97 P=0.031
Table 1: Femoral neck anteversion values in males and females (Digital Radio-graphy)
Discussion Measurement of femoral neck anteversion is important as abnormal femoral neck anteversion is known to be a predisposing factor to various pathological conditions like intoeing of gait, hip and knee osteoarthritis and femoroacetabular impingment. Some conditions like osteoarthritis of hip have been associated with increased as well as decreased femoral neck anteversion [2], while decreased anteversion neck femur has been associated with femoroacetabular impingment [8]. Increased femoral anteversion causes anterior displacement of the femoral head in the acetabulum and a decrease in congruity of the hip joint. Thus, improvement in the congruity of the hip joint may occur with excessive internal rotation of the hip. Excessive internal rotation of the hip leads to knee valgus alignment as a result of a kinematic chain thus, an increase in femoral anteversion may predispose to ACL injury [9].
Moreover careful assessment of femoral neck anteversion measure-ment is important for surgical planning for orthopaedic procedures like
Figure 3: Bar-diagram showing measurements of femoral neck ante anteversion on digital radiography.
Recent Adv Arthroplast, 2017 Volume 1(2): 26 - 28

Citation: Swerdlow RH, Lyons KE, Khosla SK, Nashatizadeh M, Pahwa R. A Pilot Study of Oxaloacetate 100 mg Capsules in Parkinson ’sdisease Patients. J Parkinsons Dis Alzheimer Dis. 2016;3(2): 4.
*Address for Correspondence:Leandro Bueno Bergantin,Rua Pedro de Toledo, 669 – Vila Clementino, São Paulo– SP, Brazil, CEP: 04039-032. Fax: 1-913-588-0681;E-mail: [email protected]
Sharma V, Kumar K, Soni PK. Evaluation of Femoral Neck Anteversion using Digital Radiography. Recent Adv Arthroplast, 2017; 1(2): 25-28.
derotation osteotomy of femur and total hip replacement [10]. Failure to recognize the abnormally anteverted or retroverted hip during total hip replacement may lead to abnormal range of motion and an unstable hip [11].
Variations in the values of femoral neck anteversion measureme-nts have been reported in literature from across the globe. Therefore analysis of anteversion femoral neck in a population assumes impo-rtance. A multitude of methods like Physical examination, Radiology, CT, MRI, Ultrasound and Dry bone measurements are available to measure femoral neck anteversion. Measurements by physical exami-nation are dependent on various parameters like musculoskeletal condition, dorsal/ventral decubitus attitude of patient (dorsal or ventral decubitus) and position of knee during examination of patient ( extension or flexion) [12].
Hence instead of measurements by physical examination, greater reliability in measurements has been reported with alternative methods [13].
CT and MRI have greater accuracy in determination of femoral neck anteversion with MRI having advantage of no radiation exposure and being able to provide greater insight into underlying pathology [14].
In the present study digital radiography was used to assess femoral neck anteversion, the values being 14.70±2.26.
Similarly the dimensions of femoral neck anteversion were higher in males when compared with females, but statistically non significa-nt. Femoral neck anteversion with values of 13.68°+-7.92° and 13°have been reported by some studies from Indian subcontinent [15, 16]. While other studies have reported mean anteversion values of 11.5 0±5.9 0 (Males) and 11.4°±4.7 (Females) using radiography and 20.4° using CT [7, 17].
Similarly variable values for femoral neck anteversion ranging from 7° to 14° have been reported from western literature also [18, 19]. The higher values of femoral neck anteversion in present study could be due to `geographical factors like living on hilly terrain and socio cultural factors that actively involve squatting and working in fields in day to day activities.
Some authors have noted variations in femoral neck anteversion based on right and left side. Significantly greater FNA was noted on left side in some studies [7, 15, 16] while others reported a higher value on right side [20].
This variability in values of femoral neck anteversion both in Indian and western studies could be due to different races, different methods of measurement and use of different anatomical landmarks while doing the measurements e.g. using transepicondylar axis rather than retrocondylar axis. The higher anteversion values can be due to persistent version due to abnormal postnatal sitting and sleeping postures [21].
In our study digital radiography was used instead of conventional radiography and measurements were done using PACS software provided with digital radiography, thereby increasing accuracy of measurements.
Femoral neck anteversion is important in reconstructive surgery such as total hip arthroplasty and many researches have been underta-ken in order to develop the optimal orientation of the hip prosthesis. In a reconstructive surgery of the hip, especially the femoral stem
replacement in hemiarthroplasty surgery, femoral neck anteversion is adjusted to a value of 15-17 degree which is the normal value for anteversion. Sometimes contra lateral side anteversion values may be required if anteversion can not be evaluated on affected side.
Limitation
A limitation of this study is its relatively small sample size and much larger studies, preferably multicenter ones, would be required to expand the database for studied population.
Conclusion
The study provides a baseline value of femoral neck anteversion in Subhimalayan population from North West India population and compares it with anteversion values from rest of the world. The data from this study will be helpful in planning of osteotomies about the hip and procedures like total hip replacement.
References1. Kim JS, Park TS, Park SB, Kim JS, Kim IY, Kim SI, et al. Measurement of
femoral neck anteversion in 3D. Part 1:3D imaging method. Med Biol EngComput. 2000; 38:603-609. [Cossref]
2. Tonnis D and Skamel HJ. Computerized tomography in evaluation of decreasedacetabular and femoral anteversion. Radiologe. 2003; 43:735-739. [Cossref]
3. Gulan G, Matovinovic D, Nemec B, Rubini D and Ravli J. Femoral NeckAnteversion. Coll Antropol. 2000; 2: 521-527. [Cossref]
4. Ejnisman L, Philippon M, Lertwanich P, Pennock A, Herzog M, Briggs K, et al. Relationship Between Femoral Anteversion and Findings in Hips withFemoroacetabular Impingement.Orthopedics. 2013; 36: 293-300. [Cossref]
5. Ryder CT and Crane L. Measuring femoral anteversion: the problem and amethod. J Bone Joint Surg Am. 1953; 35:321-328. [Cossref]
6. Ogata K, Goldsand EM. A simple biplanar method of measuring femoralanteversion and neck-shaft angle. J Bone Joint Surg Am. 1979; 61:846-851. [Cossref]
7. Jain AK, Maheshwari AV, Singh MP, Nath S and Bhargav SK. Femoral neckanteversion: A comprehensive Indian study. Indian J Orthop. 2005; 39: 137-144.
8. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA, et al.Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003; 417:112-120. [Cossref]
9. Kaneko M and Sakuraba K. Association between Femoral Anteversion andLower Extremity Posture upon Single-leg Landing: Implications for AnteriorCruciate Ligament Injury. J Phys Ther Sci. 2013; 25:1213-1217. [Cossref]
10. Srimathi T, Muthukumar T, Anandarani V.S, Umapathy S and Rameshkumar S.A study on femoral neck anteversion and its clinical correlation. Journal ofClinical and Diagnostic Research. 2012; 6:155-158. [Cossref]
11. Kudrna JC. Femoral version: definition, diagnosis, and intraoperative correctionwith modular femoral components. Orthopedics. 2005; 28:1045-1047. [Cossref]
12. Maud PJ and Foster C. Physiological assessment of human fitness. Illinois:Human Kinetics; 2006. [Cossref]
13. Grunert S, Bruckl R and Rosemeyer B. Rippstein and Müller. Roentgenologicdetermination of the actual femoral neck-shaft and antetorsion angle 1:Correction of the conversion table and study of the effects of positioning errors.Radiologe. 1986; 26:293-304. [Cossref]
14. Shindle MK, Voos JE, Nho SJ, Heyworth BE and Kelly BT. Arthroscopicmanagement of labral tears in the hip. J Bone Joint Surg Am. 2008; 90:2-19. [Cossref]
15. Siwach RC and Dahiya S. Anthropometric study of proximal femur geometryand its clinical application. Indian J Orthop. 2003; 37:247-251. [Cossref]
16. Maheshwari AV, Zlowodzki MP, Siram G and Jain AK. Femoral neckanteversion acetabular anteversion and combined anteversion in the normalIndian adult population: A computed tomographic study. Indian J Orthop. 2010;44:277-282. [Cossref]
17. Saikia KC, Bhuyan S and Rongphar R. Anthropometric study of the hip joint inNortheastern region population with computed topography scan. Indian JOrthop. 2008; 42:260-266. [Cossref]
Recent Adv Arthroplast, 2017 Volume 1(2): 27 - 28

Sharma V, Kumar K, Soni PK. Evaluation of Femoral Neck Anteversion using Digital Radiography. Recent Adv Arthroplast, 2017; 1(2): 25-28.
18. Noble PC, Alexander JW, Lindahl LJ, Yew DT, Granberry WM, Tullos HS, et al.The anatomic basis of femoral component design. Clin Orthop Relat Res.198x8:148-165. [Cossref]
19. Bargar WL, Jamali AA and Nejad AH. Femoral anteversionin THA and its lack ofcorrelation with native acetabular anteversion. The anatomic basis of femoralcomponent design. Clin Orthop Relat Res. 2010; 468:527-532. [Cossref]
20. Jiang N, Peng L, Al-Qwbani M, Xie GP, Yang QM, Chai Y, et al. Femoralversion, neck-shaft angle and acetabular anteversion in Chinese Han population:a retrospective analysis of 466 healthy adults. Medicine (Baltimore). 2015;94:e891. [Cossref]
21. Weinstein SL and Buckwaster JA. Turek’s orthopaedics in the paediatricfoot.6th edi. Philadelphea: Lippincott Williams and Wilkins. 2005. [Crossref]
Recent Adv Arthroplast, 2017 Volume 1(2): 28 - 28