original research paper ijrrms 2013;3(3) anemia and ... health organisation- definition, diagnosis...
TRANSCRIPT
Anemia and neuropathy in type- 2 diabetes mellitus: A case control study
ABSTRACT
Background:
Aim:Methods:
Results:
Conclusion:
Keywords:
Sinha Babu A, Chakrabarti A, Karmakar RN
Albuminuria and retinopathy, two microvascular complications of diabetes are known to be associated with anemia. Whether diabetic neuropathy, another complication of diabetes, is also associated with anemia is not known.
To find out the association between anemia and diabetic neuropathy in type 2 diabetes mellitus. Fifty patients of type 2 diabetes mellitus with diabetic neuropathy as 'cases' and age sex matched fifty
'controls' were selected from patients attending the diabetic clinic of College of Medicine and JNM hospital. All the cases and controls were free from retinopathy and albuminuria and were investigated for anemia. Appropriate statistical analysis was done to find out any association between anemia and diabetic neuropathy.
Anemia was found to be 68% and 42% among cases and controls respectively and the difference was statistically significant. Both peripheral and autonomic neuropathies were present in 58% cases, only peripheral neuropathy in 30% and pure antonomic neuropathy in 12% cases. No significant association of anemia with any particular type of neuropathy was evident.
Addressing anemia in diabetic individuals may have potential to make a great impact in managing these microvascular problems of diabetes.
anaemia, diabetic neuropathy, case control study
Original Research Paper
1 IJRRMS VOL-3 No.3 JULY - SEP 2013 | | | |
IJRRMS 2013;3(3)
45

1 IJRRMS VOL-3 No.3 JULY - SEP 2013 | | | |
IJRRMS 2013;3(3)Sinha Babu A et al. Anemia and neuropathy in type- 2 diabetes mellitus: A case control study
46

Neuropathy No neuropathy p-value
Age (Years) - 2(4%) 2(4%)
31-45 20(40%) 20(40%)
46-59 20(42%) 20(40%)
60 8(16%) 8(16%)
Male Sex 30(60%) 30(60%)
BMI 25 33(66%) 36(72%) 0.516
HbA1c 7% 36(72%) 28(56%) 0.095
Smoking 21(42%) 26(52%) 0.316
Hypertension 33(66%) 29(58%) 0.409
Total Cholesterol
(200 mg/dl) 29 (58%) 22(44%) 0.161
Triglyceride ( 180 mg/dl) 23(46%) 25(50%) 0.688
LDL-C ( 100mg/dl) 34(68%) 33(66%) 0.831
HDL-C ( 40 mg/dl) 18(36%) 21(42%) 0.538
≥
≥
≥
≥
≥
≥
Most of our study population were between 30 to 60 years of age. Sixty six per cent patients had body mass index above 25. Dyslipidemia was common with mean total cholesterol 288 mg/dl, triglyceride 193 mg/dl, LDL cholesterol 127 mg/dl and HDL cholesterol 42 mg/dl. High BMI (>25), smoking, high
triglyceride(> 180mg/dl) and low HDL-C (≤40 mg/dl) were more among controls than among cases. On the other hand, poor glycemic control
(HbA1C ≥ 7%), hypertension, high total cholesterol
((≥ 200 mg/dl) and high LDL-C (≥100mg/dl) were more among cases. But none of these differences were statistically significant. The cases and controls are therefore comparable with respect to all these variables. Table 2: Relationship between anemia and neuropathy
Neuro No Total P OR/95%CIpathy neuropathy
Anemia 34 21 55 0.009 2.93/1.2-7.25
No anemia 16 29 45
50 50 100
Anemia was more common among cases (68%) than among controls (42%).
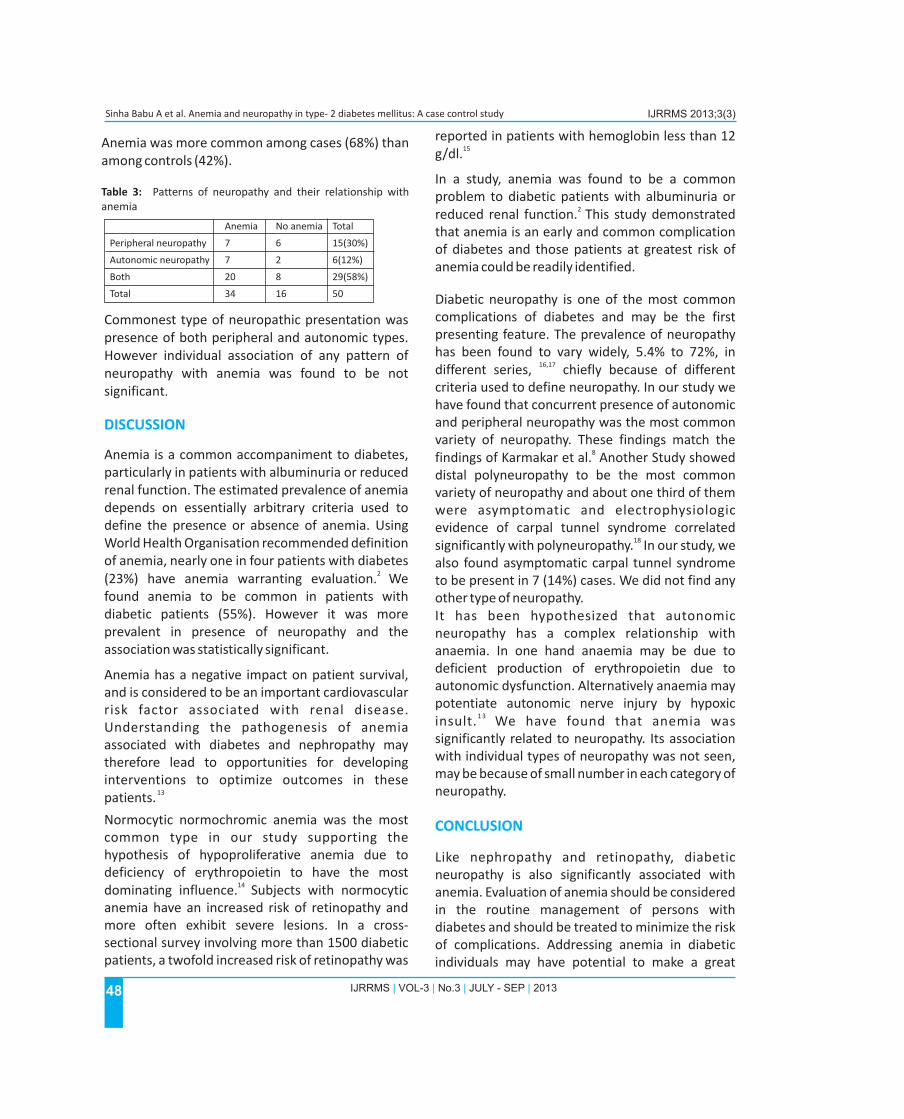
Table 3: Patterns of neuropathy and their relationship with anemia
Anemia No anemia Total
Peripheral neuropathy 7 6 15(30%)
Autonomic neuropathy 7 2 6(12%)
Both 20 8 29(58%)
Total 34 16 50
Commonest type of neuropathic presentation was presence of both peripheral and autonomic types. However individual association of any pattern of neuropathy with anemia was found to be not significant.
Anemia is a common accompaniment to diabetes, particularly in patients with albuminuria or reduced renal function. The estimated prevalence of anemia depends on essentially arbitrary criteria used to define the presence or absence of anemia. Using World Health Organisation recommended definition of anemia, nearly one in four patients with diabetes
2 (23%) have anemia warranting evaluation. We found anemia to be common in patients with diabetic patients (55%). However it was more prevalent in presence of neuropathy and the association was statistically significant.
Anemia has a negative impact on patient survival, and is considered to be an important cardiovascular risk factor associated with renal disease. Understanding the pathogenesis of anemia associated with diabetes and nephropathy may therefore lead to opportunities for developing interventions to optimize outcomes in these
13patients.
Normocytic normochromic anemia was the most common type in our study supporting the hypothesis of hypoproliferative anemia due to deficiency of erythropoietin to have the most
14 dominating influence. Subjects with normocytic anemia have an increased risk of retinopathy and more often exhibit severe lesions. In a cross-sectional survey involving more than 1500 diabetic patients, a twofold increased risk of retinopathy was
DISCUSSION
reported in patients with hemoglobin less than 12 15g/dl.
In a study, anemia was found to be a common problem to diabetic patients with albuminuria or
2 reduced renal function. This study demonstrated that anemia is an early and common complication of diabetes and those patients at greatest risk of anemia could be readily identified.
Diabetic neuropathy is one of the most common complications of diabetes and may be the first presenting feature. The prevalence of neuropathy has been found to vary widely, 5.4% to 72%, in
16,17different series, chiefly because of different criteria used to define neuropathy. In our study we have found that concurrent presence of autonomic and peripheral neuropathy was the most common variety of neuropathy. These findings match the
8findings of Karmakar et al. Another Study showed distal polyneuropathy to be the most common variety of neuropathy and about one third of them were asymptomatic and electrophysiologic evidence of carpal tunnel syndrome correlated
18significantly with polyneuropathy. In our study, we also found asymptomatic carpal tunnel syndrome to be present in 7 (14%) cases. We did not find any other type of neuropathy.It has been hypothesized that autonomic neuropathy has a complex relationship with anaemia. In one hand anaemia may be due to deficient production of erythropoietin due to autonomic dysfunction. Alternatively anaemia may potentiate autonomic nerve injury by hypoxic
1 3 insult. We have found that anemia was significantly related to neuropathy. Its association with individual types of neuropathy was not seen, may be because of small number in each category of neuropathy.
Like nephropathy and retinopathy, diabetic neuropathy is also significantly associated with anemia. Evaluation of anemia should be considered in the routine management of persons with diabetes and should be treated to minimize the risk of complications. Addressing anemia in diabetic individuals may have potential to make a great
CONCLUSION
1 IJRRMS VOL-3 No.3 JULY - SEP 2013 | | | |
IJRRMS 2013;3(3)
48
Sinha Babu A et al. Anemia and neuropathy in type- 2 diabetes mellitus: A case control study

impact in managing these microvascular problems of anemia.
Assistant Professor, Pathology, (Corresponding Author);email: [email protected]
AUTHOR NOTE
Anindita Sinha Babu,
Abhik Chakrabarti, Assistant Professor, MedicineCollege of Medicine and Jawaharlal Nehru
REFERENCES1. G. Deray A. Heurtierb A. Grimaldib V. Launay Vachera C. Isnard Bagnisa. Anemia and Diabetes. Am J Nephrol .2004;24:522–526.2. Thomas MC, MacIsaac RJ, Tsalamandris C, Power D, Jerums G. Unrecognized anemia in patients with diabetes: a cross-
sectional survey. Diabetes Care 2003; 26(4): 1164-9.3. Ranil PK, Raman R, Rachepalli SR, Pal SS, Kulothungan V, Lakshmipathy P.etal,. Anemia and diabetic retinopathy in type 2
diabetes mellitus. J Assoc Physicians India. 2010 Feb;58:91-4.4. Savage S, Estacio RO, Jeffers B, Schrier RW. Urinary albumin excretion as a predictor of diabetic retinopathy, nephropathy
and cardiovascular disease in NIDDM. Diabetes care. 1996;19 (11): 1243-8.5. Alvin C. Powers. Diabetes Mellitus. In: Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo editors. Harrison's
thPrinciples of internal Medicine. 17 edition. McGraw-Hill Medical, 2008: 2275-2304.6. World health organisation- definition, diagnosis and classification of diabetes mellitus: part 1: diagnosis and classification of
diabetes mellitus. Geneva: WHO, 1999.7. World Health Organization. Nutritional anemias: Report of a WHO scientific group. WHO, Geneva. 19688. Karmakar RN, Khandakar MR, Gangopadhyay PK, Ghosh K, Babu AS. Albuminuria and neuropathy in newly detected
diabetics: profile and correlation. J Indian Med Assoc. 2011 Jun;109(6):396-9.9. Veves A, Manes C, Murrey HJ, Young MJ, Boulton AGM. Painful neuropathy and foot ulceration in diabetic patients. Diabetes
Care. 1993; 16(8): 1187-9.10. Wiles PG, Pearce SM, Rice PJ, Mitchell JM. Vibration perception threshold: influence of age, height, sex and smoking and
calculation of accurate centile values. Diabet Med. 1991; 8(2): 157-61.11. Olaleye D, Perkins BA, Bril V. Evaluation of three screening tests and a risk assessment model for diagnosing peripheral
neuropathy in the diabetic clinic. Diabetes Res Clin Pract. 2001; 54(2): 115-28.12. Tentolouris N, Katsilambros N, Papazacos G. Corrected QT interval in relation to the severity of diabetic autonomic
neuropathy. Eur J Clin Invest. 1997; 27(12): 1049-54.13. Kathrine J. Craig, BSc (Hons), RN. et al. Anemia and diabetes in absence of nephropathy. Diabetes Care. 2005;
28(5):1118–1123.14. Winkler AS, Marsden J, Chaudhuri KR, Hambley H, Watkins PJ. Erythropoietin depletion and anemia in diabetes mellitus.
Diabet Med. 1999;16(10):813–9.15. Qiao Q, Keinanen F, Kiukanniemi S, Laara E. The relationship between haemoglobin levels and diabetic retinopathy. J Clin
Epidemiol .1997;50(2):153–8.16. Tontolouris N, Pagoni S, Tzonou A, Katsilambros N Peripheral neuropathy does not invariably coexist with autonomic
neuropathy in diabetes mellitus. Eur J Intern Med. 2001; 12(1): 20-7.17. Ashok S, Ramu M, Deepa R, Mohan V. Prevalence of neuropathy in type 2 diabetes attending a diabetes centre in South
India. J Assoc Physicians India. 2002; 50:546-50.18. Dyck PJ, Kratz KM, Karnes JL et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy and
nephropathy in a population based cohort: the Rochester Diabetic Neuropathy Study. Neurology. 1993; 43: 817-24.
1 IJRRMS VOL-3 No.3 JULY - SEP 2013 | | | |
IJRRMS 2013;3(3)
49
Sinha Babu A et al. Anemia and neuropathy in type- 2 diabetes mellitus: A case control study