ortho ‘bad stuff’ robert v. cantu, md · ortho ‘bad stuff’ robert v. cantu, md. ... with...
TRANSCRIPT

ORTHO ORTHO ‘‘BAD BAD STUFFSTUFF’’
Robert V. Cantu, MDRobert V. Cantu, MDAssistant Professor of Assistant Professor of OrthopaedicOrthopaedic
SurgerySurgery
DartmouthDartmouth--Hitchcock Medical CenterHitchcock Medical Center

OutlineOutline
Open FracturesOpen Fractures
Compartment SyndromeCompartment Syndrome
Pelvic FracturesPelvic Fractures
Hip DislocationHip Dislocation
Knee DislocationKnee Dislocation
Vascular Injury with Extremity FractureVascular Injury with Extremity Fracture
Spine InjurySpine Injury
ScapulothoracicScapulothoracic DissociationDissociation
Survey results and questionsSurvey results and questions

EpidemiologyEpidemiology
Accidental injury is #1 Accidental injury is #1 cause of death for people cause of death for people age 1age 1--44 years44 years
Typical day sees 170,000 Typical day sees 170,000 people injured with 400 people injured with 400 deathsdeaths
Overall annual cost over Overall annual cost over 200 billion200 billion

PolytraumaPolytrauma
PatientPatient
Syndrome of injuries with Syndrome of injuries with ISS>17 ISS>17
PolytraumaPolytrauma patients susceptible patients susceptible to systemic reaction to injuries to systemic reaction to injuries that can lead to that can lead to dysfunction/failure of uninjured dysfunction/failure of uninjured organsorgans
““TrimodalTrimodal mortalitymortality””-- scene, scene, within 24 hrs, 2within 24 hrs, 2ndnd--33rdrd weekweek

Open FracturesOpen Fractures
First step is identificationFirst step is identification
ER treatment includes ER treatment includes tetanus booster and IV tetanus booster and IV antibioticsantibiotics
Wrap wound with sterile Wrap wound with sterile gauze and gauze and splint splint extremityextremity

GustilloGustillo
and Andersonand Anderson
Grade 1Grade 1-- skin opening of 1cm or less, minimal muscle skin opening of 1cm or less, minimal muscle contusion, usually inside out mechanismcontusion, usually inside out mechanism
Grade 2Grade 2-- skin laceration 1skin laceration 1--10cm, extensive soft tissue damage10cm, extensive soft tissue damage
Grade 3aGrade 3a-- extensive soft tissue laceration(10cm) but adequate extensive soft tissue laceration(10cm) but adequate bone coveragebone coverage
Grade 3bGrade 3b-- extensive soft tissue injury with extensive soft tissue injury with periostealperiosteal stripping stripping requiring flap advancement or free flaprequiring flap advancement or free flap
Grade 3cGrade 3c-- vascular injury requiring repairvascular injury requiring repair

Type 1Type 1
Wound less than 1cmWound less than 1cm
Usually an Usually an ‘‘in to in to outout’’woundwound
Tetanus booster plus Tetanus booster plus 1gm IV 1gm IV ancefancef

Type 2Type 2
Wound between 1Wound between 1--10 cm10 cm
Tetanus booster and Tetanus booster and 1gm IV 1gm IV AncefAncef

Type 3Type 3
IIIaIIIa: wound greater than : wound greater than 10cm, significant 10cm, significant periostealperiosteal lossloss
Tetanus booster, 1gm IV Tetanus booster, 1gm IV AncefAncef, single dose IV , single dose IV gentamycingentamycin

III BIII B
Wound greater than 10cm, Wound greater than 10cm, significant wound contamination, significant wound contamination, barnyard injury, barnyard injury, wound requires wound requires soft tissue flap coveragesoft tissue flap coverage
Tetanus booster, IV Tetanus booster, IV AncefAncef, IV , IV Gent, IV PenicillinGent, IV Penicillin

III CIII C
Open fracture with Open fracture with vascular injury requiring vascular injury requiring repairrepair
True emergencyTrue emergency
If vascular repair not If vascular repair not performed within 6 performed within 6 hours, amputation rate hours, amputation rate >90%>90%

Timing of I+D For Open FracturesTiming of I+D For Open Fractures
““There is There is universal agreementuniversal agreement that open that open fractures require emergency treatmentfractures require emergency treatment”” ((GustilloGustillo and and Anderson JBJS 1976)Anderson JBJS 1976)
One study 1102 patients no difference in One study 1102 patients no difference in infection rate <12 hrs infection rate <12 hrs vsvs>12 hrs >12 hrs ((PatzakisPatzakis CORR 1989)CORR 1989)
104 open tibia fractures in children no 104 open tibia fractures in children no difference <6 hrs difference <6 hrs vsvs >7 hrs >7 hrs ((KrederKreder J J pedped OrthopOrthop 195)195)
554 open fractures in children, no difference 554 open fractures in children, no difference <6hrs vs. >7 hrs <6hrs vs. >7 hrs (Skaggs JBJS 2005)(Skaggs JBJS 2005)

Timing of Wound ClosureTiming of Wound Closure
119 open fractures immediate vs. delayed closure119 open fractures immediate vs. delayed closure-- no difference no difference in infection rate (Delong J Trauma 1999)in infection rate (Delong J Trauma 1999)
532 patients requiring microsurgical flap coverage open fracture532 patients requiring microsurgical flap coverage open fracture--flap <72 hrs had 6% flap <72 hrs had 6% infxninfxn rate, flap >72 hrs had 30% rate, flap >72 hrs had 30% infxninfxn rate rate ((GopalGopal JBJS[Br] 2000)JBJS[Br] 2000)
Only 18% of infections due to organism cultured at initial Only 18% of infections due to organism cultured at initial surgery (surgery (PatzakisPatzakis JOT 2000)JOT 2000)


Compartment SyndromeCompartment Syndrome
Rise in pressure within a Rise in pressure within a fascialfascial compartment compartment which if untreated leads to decreased perfusion which if untreated leads to decreased perfusion and eventual muscle necrosisand eventual muscle necrosis

CausesCauses
Limb fracture (45%)Limb fracture (45%)Soft tissue traumaSoft tissue traumaProlonged compression limbProlonged compression limbBurnsBurnsPostPost--ischemic swellingischemic swellingIV infiltrationIV infiltrationOtherOther

Acute vs. ChronicAcute vs. Chronic
Acute seen after injury or Acute seen after injury or ischemiaischemia
Chronic seen in athletes Chronic seen in athletes (leg most commonly). (leg most commonly). Elevated pressures with Elevated pressures with exercise, resolve with exercise, resolve with rest.rest.
DiagnosisDiagnosis
Hallmark is pain out of Hallmark is pain out of proportion to injuryproportion to injury

DiagnosisDiagnosis
5 P5 P’’s: s: PPain, ain, PPallor, allor, PParesthesiasaresthesias, , PParalysis, aralysis, PPulselessnessulselessness

DiagnosisDiagnosis
Swollen/tense Swollen/tense muscle muscle compartmentscompartments
May or may not have May or may not have decreased sensation in decreased sensation in extremityextremity
Serial exams importantSerial exams important
PainPain
Typically pain increased Typically pain increased on passive stretch of on passive stretch of involved muscle involved muscle compartment(s)compartment(s)

LabsLabs
Elevated Elevated CPKCPK’’ss indicative of indicative of muscle damagemuscle damage
Renal function (BUN, Renal function (BUN, creatininecreatinine) may be impaired ) may be impaired if if rhabdomyolysisrhabdomyolysis
Acidosis secondary to muscle Acidosis secondary to muscle ischemiaischemia

TimingTiming
Muscle shows functional Muscle shows functional changes after 2changes after 2--4 hours 4 hours ischemic time, with cell ischemic time, with cell death occurring after 4death occurring after 4--12 hours*12 hours*
**WhitesidesWhitesides 19751975

MeasurementMeasurement
Required if diagnosis in Required if diagnosis in questionquestion
Multiple devices availableMultiple devices available

Slit CatheterSlit Catheter
Hand held monitoring Hand held monitoring devicedevice

Where to MeasureWhere to Measure
Pressures highest at level Pressures highest at level of fractureof fracture
MeasurementMeasurement--
WhatWhat’’s too Highs too High
> 30 mm Hg (> 30 mm Hg (RorabeckRorabecket al.)et al.)
>45 mm Hg (>45 mm Hg (MatsenMatsen et et al.)al.)
Within 30 mm Hg of Within 30 mm Hg of diastolic pressure diastolic pressure ((WhitesidesWhitesides et al.)et al.)

TreatmentTreatment
Immediate surgical Immediate surgical decompression of decompression of involved compartmentsinvolved compartments

24 24 yoyo
Male Snowboarding Male Snowboarding AccidentAccident


Acute Quadriceps Compartment Acute Quadriceps Compartment SydromeSydrome
24 24 yoyo male weight lifter male weight lifter using highusing high--dose dose creatinecreatinefollowing 3 hour lower following 3 hour lower extremity work outextremity work out

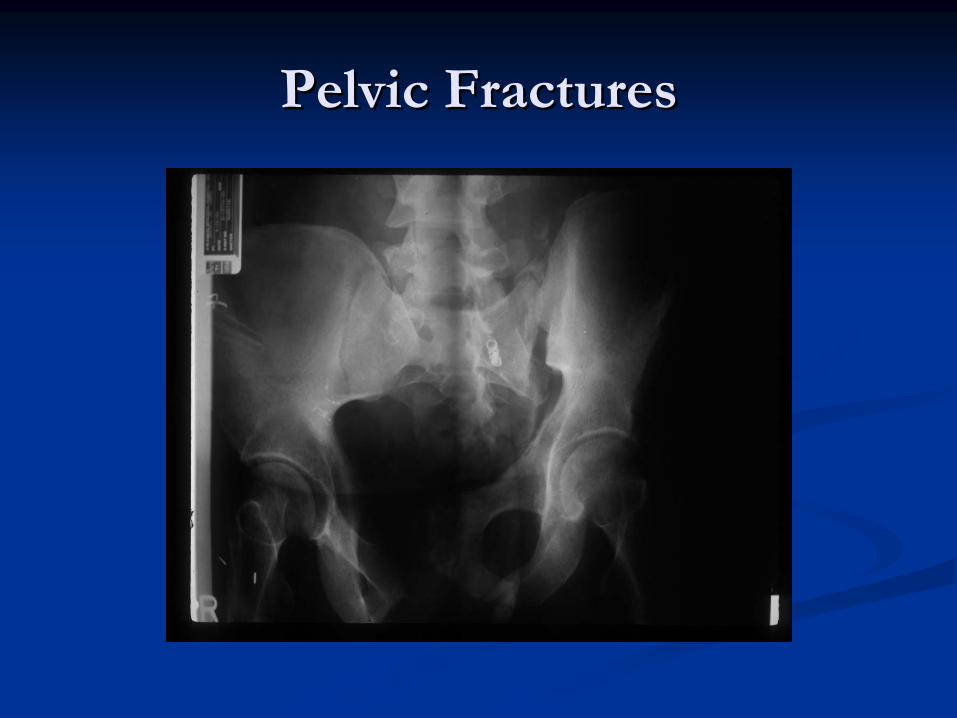
Pelvic FracturesPelvic Fractures

LigamentousLigamentous
AnatomyAnatomy

Patients with pelvic Patients with pelvic fractures who present fractures who present
hypotensivehypotensive . . . . . . Mortality increased from 3% to 38%Mortality increased from 3% to 38%
((NaamNaam
et al. Arch Sur. 1983)et al. Arch Sur. 1983)
Acute Mortality Pelvic FracturesAcute Mortality Pelvic Fractures
Early external fixation and patient mobilization Early external fixation and patient mobilization shown to decrease mortalityshown to decrease mortality
One study showed mortality decreased from One study showed mortality decreased from 41% to 21% in patients with admission SBP < 41% to 21% in patients with admission SBP < 100mm Hg100mm Hg
RiemerRiemer
et al. J. of Trauma 1993et al. J. of Trauma 1993

Associated InjuriesAssociated Injuries

Burgess and Young ClassificationBurgess and Young Classification
Lateral CompressionLateral Compression
AnteroposteriorAnteroposterior compressioncompression
Vertical ShearVertical Shear
CombinedCombined

Acute pelvic stabilizationAcute pelvic stabilization
MAST/PASG deviceMAST/PASG deviceclassic transport deviceclassic transport device
SheetsSheetsExternal FixationExternal FixationNewer devicesNewer devices
pelvic binderspelvic binders

Pelvic BinderPelvic Binder
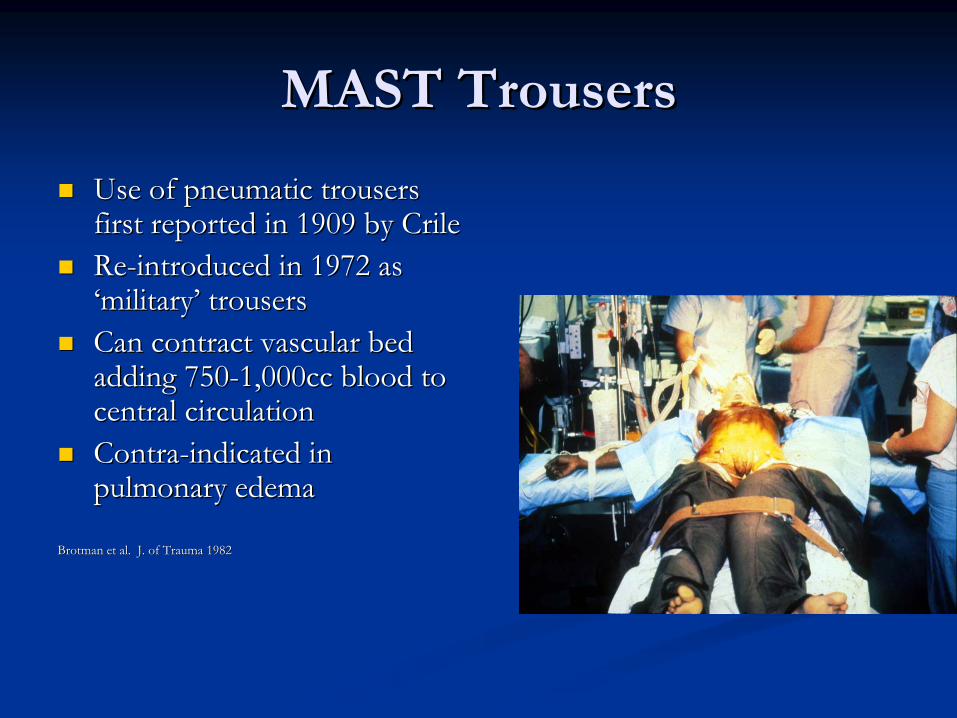
MAST TrousersMAST Trousers
Use of pneumatic trousers Use of pneumatic trousers first reported in 1909 by Crile first reported in 1909 by Crile ReRe--introduced in 1972 as introduced in 1972 as ‘‘militarymilitary’’ trouserstrousersCan contract vascular bed Can contract vascular bed adding 750adding 750--1,000cc blood to 1,000cc blood to central circulationcentral circulationContraContra--indicated in indicated in pulmonary edemapulmonary edema
BrotmanBrotman
et al. J. of Trauma 1982et al. J. of Trauma 1982

Pelvic FixationPelvic Fixation
External fixationExternal fixation
delayed reconstructiondelayed reconstruction


Hip DislocationHip Dislocation

DiagnosisDiagnosis
Typically high energy injuryTypically high energy injury
With posterior dislocation, With posterior dislocation, leg shortened and internally leg shortened and internally rotatedrotated
With anterior dislocation leg With anterior dislocation leg may be shortened and may be shortened and externally rotatedexternally rotated

TreatmentTreatment
Urgent reductionUrgent reduction
Proper pain Proper pain medication/relaxation medication/relaxation necessary for reductionnecessary for reduction
Avoid repeated attempts Avoid repeated attempts in ED in ED

Reduction Posterior DislocationReduction Posterior Dislocation
Stabilize pelvisStabilize pelvis
Flex hip, adduction, Flex hip, adduction, traction with gentle traction with gentle internal/external rotationinternal/external rotation
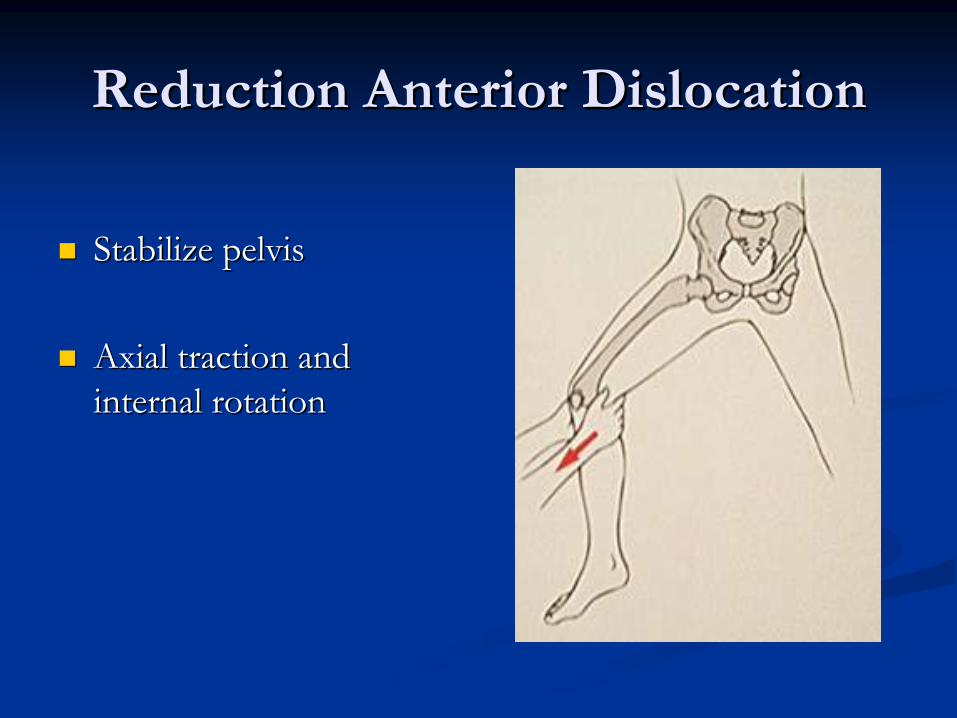
Reduction Anterior DislocationReduction Anterior Dislocation
Stabilize pelvisStabilize pelvis
Axial traction and Axial traction and internal rotationinternal rotation

Irreducible DislocationIrreducible Dislocation

Long Term ComplicationsLong Term Complications
AVN most debilitatingAVN most debilitating

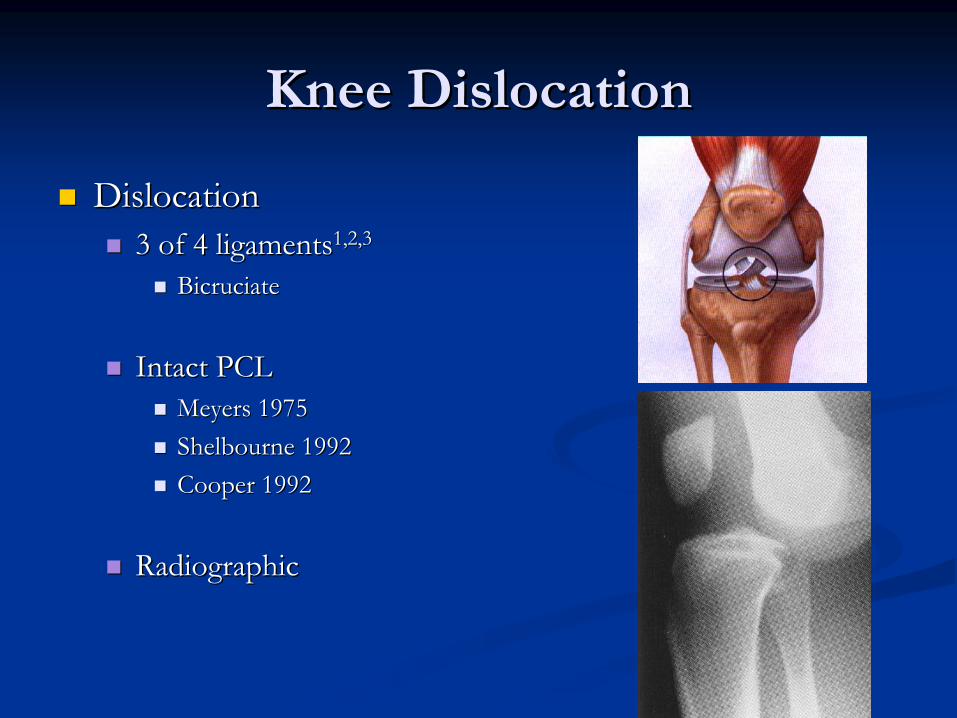
Knee DislocationKnee Dislocation
DislocationDislocation3 of 4 ligaments3 of 4 ligaments1,2,31,2,3
BicruciateBicruciate
Intact PCLIntact PCLMeyers 1975Meyers 1975ShelbourneShelbourne 19921992Cooper 1992Cooper 1992
RadiographicRadiographic

Kennedy 1963
Position Classification ofPosition Classification of Knee DislocationsKnee Dislocations
AnteriorAnteriorPosteriorPosteriorLateralLateralMedialMedialRotatoryRotatory
PosterolateralPosterolateral

Schenck 1994
Mechanism of Knee DislocationMechanism of Knee Dislocation
AnteriorAnteriorMost commonMost commonFrequent vascular injury (traction)Frequent vascular injury (traction)
PosteriorPosteriorHighest incidence vascular injury Highest incidence vascular injury (complete tear)(complete tear)Highest incidence extensor Highest incidence extensor mechanism disruptionmechanism disruption
PosterolateralPosterolateralIrreducibleIrreducibleHighest incidence Common Highest incidence Common Peroneal Nerve injuryPeroneal Nerve injury

1 - Siliski 1998, 2 - Green 1975, 3 -Fanelli 1999, 4 - Meyers 1975
Associated InjuriesAssociated Injuries
Meniscus Meniscus ((≈≈100)100)11
Vascular Vascular (32%)(32%)22
Nerve Nerve (20(20--30%)30%)33
Fractures Fractures ((≈≈60%)60%)44

1 - Green 1977
Popliteal Artery InjuryPopliteal Artery Injury
Overall Incidence: 32%Overall Incidence: 32%11
MechanismMechanismStretching / RuptureStretching / Rupture
HyperextensionHyperextensionAnterior dislocationAnterior dislocationTethered arteryTethered artery
Intimal DamageIntimal DamageDirect contusionDirect contusionPosterior dislocationPosterior dislocation
Delayed ThrombusDelayed ThrombusNever Blame SpasmNever Blame Spasm

Initial Evaluation / ManagementInitial Evaluation / Management
HistoryHistoryMechanismMechanism
Physical ExamPhysical ExamGross deformityGross deformityCompare to opposite kneeCompare to opposite kneeClue!Clue!
Coexist Varus/Valgus Coexist Varus/Valgus instability in full extensioninstability in full extension
ACL/PCL injuryACL/PCL injury
NeurovascularNeurovascular

Cole & Harner 1999
Diagnosis ofDiagnosis of Popliteal Artery InjuryPopliteal Artery Injury
HistoricalHistoricalAA--gram for everyonegram for everyone
RecentRecentSymmetrical distal pulsesSymmetrical distal pulsesABI > 0.85ABI > 0.85Serial Exam by Vascular Serial Exam by Vascular SurgeonSurgeon

Cole & Harner 1999
Technique of Closed ReductionTechnique of Closed Reduction
AnteriorAnteriorTraction & elevation distal femurTraction & elevation distal femur
PosteriorPosteriorTraction & extension of prox tibiaTraction & extension of prox tibia
Lateral/MedialLateral/MedialTraction & translationTraction & translation
RotationalRotationalTraction & derotationTraction & derotation


Vascular Injury with Extremity Vascular Injury with Extremity FractureFracture

DiagnosisDiagnosis
Always consider with penetrating traumaAlways consider with penetrating trauma
With blunt trauma typically high energy injuryWith blunt trauma typically high energy injury
Physical exam: palpate distal pulsesPhysical exam: palpate distal pulses

Ankle Brachial IndexAnkle Brachial Index
Measurement systolic pressure of injured Measurement systolic pressure of injured extremity compared to uninjuredextremity compared to uninjured
If ratio<0.9 then consider vascular consult and If ratio<0.9 then consider vascular consult and angiogramangiogram

TreatmentTreatment
Vascular injury first priorityVascular injury first priority
Can perform temporary Can perform temporary skeletal stabilization prior to skeletal stabilization prior to vascular repairvascular repair
Alternative is vascular shunt, Alternative is vascular shunt, then orthopedic repair, then orthopedic repair, followed by definitive followed by definitive vascular repairvascular repair

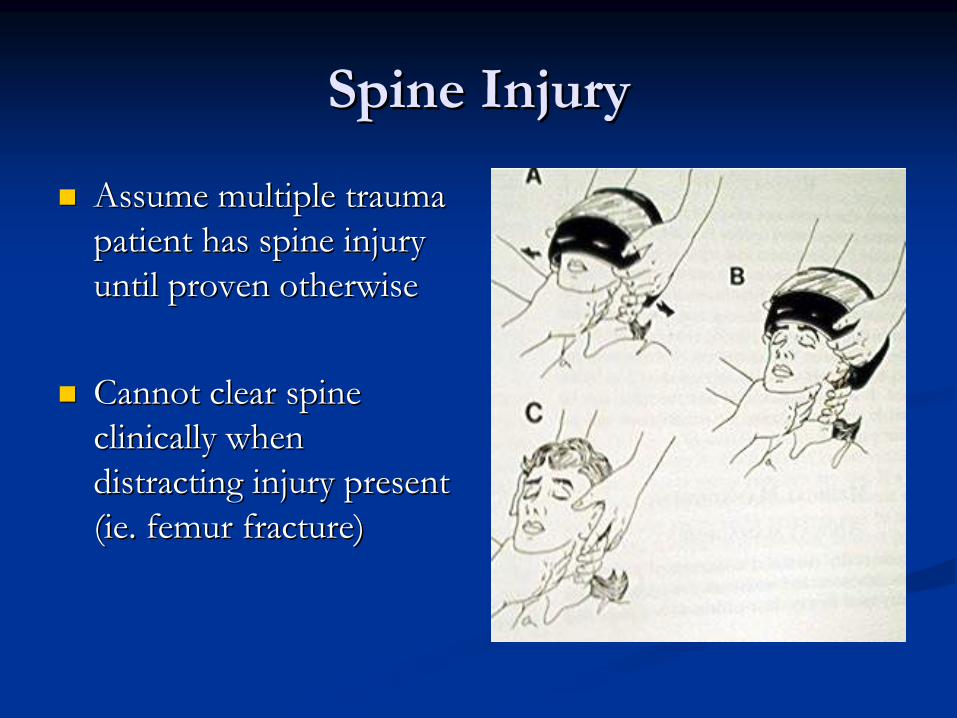
Spine InjurySpine Injury
Assume multiple trauma Assume multiple trauma patient has spine injury patient has spine injury until proven otherwiseuntil proven otherwise
Cannot clear spine Cannot clear spine clinically when clinically when distracting injury present distracting injury present ((ieie. femur fracture). femur fracture)

Epidemiology of Epidemiology of Spine InjuriesSpine Injuries
Vehicular trauma, falls, Vehicular trauma, falls, gunshot/knife wounds, gunshot/knife wounds, sports/recreation account for sports/recreation account for most injuriesmost injuries
Bimodal distribution: highest Bimodal distribution: highest prevalence between 15prevalence between 15--24 24 yrs, second peak after 55 yrs, second peak after 55 yearsyears

Spine ImagingSpine Imaging
If any question image If any question image entire spineentire spine
CT scan more sensitive CT scan more sensitive than plain filmsthan plain films
MRI for neurologic MRI for neurologic injuryinjury

Spine InjurySpine Injury
Incidence of nonIncidence of non--contiguous spine fracture contiguous spine fracture about 10%about 10%

Spinal Cord InjurySpinal Cord Injury
Aggressive resuscitation Aggressive resuscitation to prevent hypoxia, to prevent hypoxia, hypovolemiahypovolemia
Document detailed examDocument detailed exam
Serial examsSerial exams-- by same by same person if possibleperson if possible

Spinal Cord InjurySpinal Cord Injury
Consider steroid Consider steroid protocolprotocol--methylprednisolonemethylprednisolone20mg/kg loading dose 20mg/kg loading dose then 5.4mg/kg per hr x then 5.4mg/kg per hr x 24 hours24 hours

LigamentousLigamentous
InjuryInjury
11° 3.5mm

Related PointsRelated Points
Of unconscious trauma patients, 5Of unconscious trauma patients, 5--10% have 10% have significant csignificant c--spine injuryspine injury
If patientIf patient’’s car requires towing, 1 in 300 chance s car requires towing, 1 in 300 chance serious cserious c--spine injuryspine injury
If patient ejected from car 1 in 8 riskIf patient ejected from car 1 in 8 risk

Related PointsRelated Points
Aspiration of gastric contents and shock are two Aspiration of gastric contents and shock are two most common causes of premost common causes of pre--hospital death in hospital death in SCI patients SCI patients
In spinal cord injured patients 35% incidence of In spinal cord injured patients 35% incidence of concomitant fractures (11% missed)concomitant fractures (11% missed)
((VaccaroVaccaro, , ICLICL--1997)1997)


ScapulothoracicScapulothoracic
DissociationDissociation

ScapulothoracicScapulothoracic
DissociationDissociation

Scapulothoracic Dissociation Scapulothoracic Dissociation
Traumatic disruption of Traumatic disruption of scapula from posterior chest scapula from posterior chest wallwall
Referred to as Referred to as ““closed closed traumatic forequarter traumatic forequarter amputationamputation””
Neurovascular injury Neurovascular injury commoncommon

ScapulothoracicScapulothoracic
DissociationDissociation
Left Left scapulothoracicscapulothoracicdissociation with dissociation with subclaviansubclavian artery artery disruptiondisruption

Scapulothoracic Dissociation Scapulothoracic Dissociation ContinuedContinued
Treatment focused on care of neurovascular Treatment focused on care of neurovascular injuryinjury
If vascular injury then emergency arteriogram If vascular injury then emergency arteriogram followed by repair. Brachial plexus explored at followed by repair. Brachial plexus explored at same time.same time.
A Few More PointsA Few More Points

Results of ED SurveyResults of ED Survey
0.64
0.28
0.08
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Alw
ays
have
cove
rge
Som
etim
esha
veco
vera
ge
Nev
er h
ave
cove
rage
Per
cent
of t
ime
Orthopaedic oncall coverage

Is your coverage adequate?
0.64
0.520.48
00.10.20.30.40.50.60.7
Day timecoverage
Nighttimecoverage
Weekendcoverage
Per
cent
of t
ime
Orthopaedic oncall coverage

SurveySurvey
““Do you think orthopedists are reluctant to Do you think orthopedists are reluctant to come in when you feel they should?come in when you feel they should?””
YesYes--55%55%
““How often does your onHow often does your on--call orthopedist come call orthopedist come in when you ask to have a patient evaluated?in when you ask to have a patient evaluated?””
AlwaysAlways--29%29%
SurveySurvey
““Has ease of arranging a patient transfer for Has ease of arranging a patient transfer for orthopedic injury to DHMC changed over the orthopedic injury to DHMC changed over the past 5 years?past 5 years?””A. Much betterA. Much betterB. No changeB. No changeC. Much worseC. Much worse

OITE 2008OITE 2008
74.74.
Which of the following has been most closely Which of the following has been most closely associated with nonunion after femoral nailing?associated with nonunion after femoral nailing?
1.1.
Use of Use of NSAIDsNSAIDs2.2.
Comminuted fracturesComminuted fractures3.3.
Early Early weightbearingweightbearing4.4.
SmokingSmoking5.5.
Static interlocked nailStatic interlocked nail
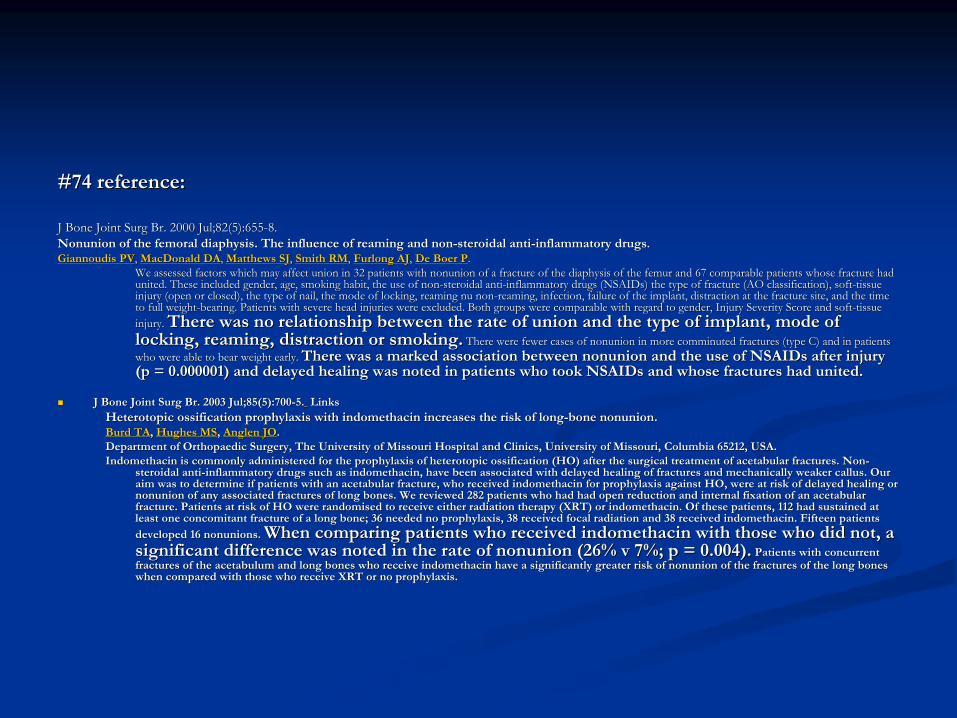
#74 reference:#74 reference:
J Bone Joint J Bone Joint SurgSurg
Br.Br.
2000 Jul;82(5):6552000 Jul;82(5):655--8.8.Nonunion of the femoral Nonunion of the femoral diaphysisdiaphysis. The influence of reaming and non. The influence of reaming and non--steroidal antisteroidal anti--inflammatory drugsinflammatory drugs..GiannoudisGiannoudis
PVPV, , MacDonald DAMacDonald DA, , Matthews SJMatthews SJ, , Smith RMSmith RM, , Furlong AJFurlong AJ, , De Boer PDe Boer P..We assessed factors which may affect union in 32 patients with nWe assessed factors which may affect union in 32 patients with nonunion of a fracture of the onunion of a fracture of the diaphysisdiaphysis
of the femur and 67 comparable patients whose fracture had of the femur and 67 comparable patients whose fracture had united. These included gender, age, smoking habit, the use of nounited. These included gender, age, smoking habit, the use of nonn--steroidal antisteroidal anti--inflammatory drugs (inflammatory drugs (NSAIDsNSAIDs) the type of fracture (AO classification), soft) the type of fracture (AO classification), soft--tissue tissue injury (open or closed), the type of nail, the mode of locking, injury (open or closed), the type of nail, the mode of locking, reaming nu nonreaming nu non--reaming, infection, failure of the implant, distraction at the freaming, infection, failure of the implant, distraction at the fracture site, and the time racture site, and the time to full weightto full weight--bearing. Patients with severe head injuries were excluded. Both bearing. Patients with severe head injuries were excluded. Both groups were comparable with regard to gender, Injury Severity Scgroups were comparable with regard to gender, Injury Severity Score and softore and soft--tissue tissue injury. injury. There was no relationship between the rate of union and the typeThere was no relationship between the rate of union and the type
of implant, mode of of implant, mode of locking, reaming, distraction or smoking.locking, reaming, distraction or smoking.
There were fewer cases of nonunion in more comminuted fracturesThere were fewer cases of nonunion in more comminuted fractures
(type C) and in patients (type C) and in patients who were able to bear weight early. who were able to bear weight early. There was a marked association between nonunion and the use of There was a marked association between nonunion and the use of NSAIDsNSAIDs
after injury after injury (p = 0.000001) and delayed healing was noted in patients who too(p = 0.000001) and delayed healing was noted in patients who took k NSAIDsNSAIDs
and whose fractures had united.and whose fractures had united.
J Bone Joint J Bone Joint SurgSurg Br.Br. 2003 Jul;85(5):7002003 Jul;85(5):700--5.5. LinksLinksHeterotopicHeterotopic
ossification prophylaxis with ossification prophylaxis with indomethacinindomethacin
increases the risk of longincreases the risk of long--bone nonunion.bone nonunion.BurdBurd
TATA, , Hughes MSHughes MS, , AnglenAnglen
JOJO..Department of Department of OrthopaedicOrthopaedic
Surgery, The University of Missouri Hospital and Clinics, UniveSurgery, The University of Missouri Hospital and Clinics, University of Missouri, Columbia 65212, USA.rsity of Missouri, Columbia 65212, USA.IndomethacinIndomethacin
is commonly administered for the prophylaxis of is commonly administered for the prophylaxis of heterotopicheterotopic
ossification (HO) after the surgical treatment of ossification (HO) after the surgical treatment of acetabularacetabular
fractures. Nonfractures. Non--
steroidal antisteroidal anti--inflammatory drugs such as inflammatory drugs such as indomethacinindomethacin, have been associated with delayed healing of fractures and mec, have been associated with delayed healing of fractures and mechanically weaker callus. Our hanically weaker callus. Our aim was to determine if patients with an aim was to determine if patients with an acetabularacetabular
fracture, who received fracture, who received indomethacinindomethacin
for prophylaxis against HO, were at risk of delayed healing or for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. We reviewed nonunion of any associated fractures of long bones. We reviewed 282 patients who had had open reduction and internal fixation of282 patients who had had open reduction and internal fixation of
an an acetabularacetabular
fracture. Patients at risk of HO were fracture. Patients at risk of HO were randomisedrandomised
to receive either radiation therapy (XRT) or to receive either radiation therapy (XRT) or indomethacinindomethacin. Of these patients, 112 had sustained at . Of these patients, 112 had sustained at least one concomitant fracture of a long bone; 36 needed no propleast one concomitant fracture of a long bone; 36 needed no prophylaxis, 38 received focal radiation and 38 received hylaxis, 38 received focal radiation and 38 received indomethacinindomethacin. Fifteen patients . Fifteen patients
developed 16 developed 16 nonunionsnonunions. . When comparing patients who received When comparing patients who received indomethacinindomethacin
with those who did not, a with those who did not, a significant difference was noted in the rate of nonunion (26% v significant difference was noted in the rate of nonunion (26% v 7%; p = 0.004).7%; p = 0.004).
Patients with concurrent Patients with concurrent fractures of the fractures of the acetabulumacetabulum
and long bones who receive and long bones who receive indomethacinindomethacin
have a significantly greater risk of nonunion of the fractures have a significantly greater risk of nonunion of the fractures of the long bones of the long bones when compared with those who receive XRT or no prophylaxis.when compared with those who receive XRT or no prophylaxis.

Thank YouThank You