osce revision respiratory mark woodhead honorary clinical professor of respiratory medicine
TRANSCRIPT

OSCE Revision
Respiratory
Mark WoodheadHonorary Clinical Professor of Respiratory Medicine

BREATHLESSNESS
• Respiratory

BREATHLESSNESS
• Respiratory• Cardiac• Haematological• Neurological• Psychiatric

BREATHLESSNESS
PatternAge / durationPrecipitants and relieversSeverityAssociated symptomsExacerbations

BREATHLESSNESS
Pattern
Diurnal variation (asthma)Sleep disturbance (asthma)Nocturnal worsening (most causes!)Orthopnoea (LVF, COPD, Obesity…)Paroxysmal nocturnal dyspnoea (LVF)

BREATHLESSNESS
Age / duration
Age < 30 - asthma, bronchiectasis, psychological (COPD unlikely)
Age > 50 - COPD, (asthma), cardiac
Present since childhood asthma (bronchiectasis)
Present only since 40s - COPD
Recent onset – pneumonia, PVTE, pneumothorax
Non-smoker – asthma, Smoker – (asthma) or COPD

BREATHLESSNESS
Precipitants and relievers
Worse in summer – asthmaWorse in winter – most things!
Animals, specific irritants – asthma
Occupation – specific sensitiser (asthma) or just effort?
Risks for PVTE
Effort – most causes

BREATHLESSNESS
Severity
At rest (talking)Effort – how much, distance, stairs ADLsWork
Exacerbations – frequency, times in hospital, ever ICU

BREATHLESSNESS
Associated symptomsSputum > 3/12 of year, in consecutive years – COPD, bronchiectasis, asthmaLarge volume sputum – bronchiectasisHaemoptysis – bronchiectasis, cancer, PVTEAnorexia and weight loss – cancerAnkle swelling – not asthma, cardiac, cor pulmonaleUnilateral leg swelling – PVTEFever, rigors, purulent sputum – pneumoniaPleuritic chest pain – pneumonia, PVTE, pneumothorax

BREATHLESSNESS
Exacerbations
Yes – asthma, COPD, bronchiectasisFrequency and severity…..
CHEST PAIN
• Respiratory

CHEST PAIN
• Respiratory• Cardiac• Musculoskeletal• Gastrointestinal

CHEST PAIN
Site
Central – most thingsLateral – pneumonia, PVTE, pneumothorax, musculoskeletalRadiation – arm – cardiac - back – most things

CHEST PAIN
Type / precipitants
Constant / intermittentEffort related – cardiacPleuritic – pneumonia, PVTE, pneumothorax, musculoskeletalMovement eg arm – musculoskeletalMeals - GI

BRONCHODILATOR THERAPY
Concepts of Prevention and Relief regular vs as required usered/brown inhalers Blue vs
SABALABA, (LABA – formoterol)corticosteroid, anti-muscarinic, combinations

BRONCHODILATOR THERAPY
MDI
Take off capShakeBreathe outDevice to mouthFull breath in and activate as breathingHold breath for few secondsRepeatSteroid – rinse / gargle afterwards

LONG TERM CORTICOSTEROID THERAPY
Benefits – disease control
Harms – dose and duration
Short term – hunger, dyspepsia, insomnia, acne
Long term – weight gain, hypertension, diabetes, pneumonia osteoporosis, skin thinning, cataracts
Balance benefit vs harm, aim for lowest effective dose

EXAMINATION

EXAMINATION - PNEUMONECTOMY
Affected side
Thoracotomy scarReduced movement / expansionDull to percussionVF up or downReduced breath sounds
Mediastinum towards the affected side (trachea, apex beat)
Differential pleural effusion – mediastinum away from affected side

EXAMINATION COPD/ASTHMACyanosis (COPD) Raised respiratory rateTremor – asterixis if CO2 retention (COPD)
- fine - B-agonist
Signs of air trapping due to airway narrowing:reduced cricosternal distanceincreased A-P diameter of chest (‘barrel’)reduced or lost lateral chest expansionparadoxical lower chest movementreduced / absent cardiac dullness on percussionreduced breath sounds (often mainly apical)
Wheeze, insp, exp, but may be absentSputum pot (COPD, bronchiectasis)Inhalers, Peak Flow meter by the bed

EXAMINATION PULMONARY FIBROSIS
Finger clubbing (50%)
Cyanosis (if severe)
Raised respiratory rate
Reduced chest expansion (‘restriction’)
Persistent, bi-basal, fine, late inspiratory crackles

SPIROMETRY
Restriction – FEV1 and FVC reduced in parallelratio normal or increased
FEV1 65% predictedFVC 67%Ratio 80%
Restriction – alveolar disease eg pulmonary fibrosischest wall disease eg kyphoscoliosis, muscle weakness, obesity

SPIROMETRY
Obstruction – FEV1 reduced more than FVC ratio less than 70%
FEV1 65% predictedFVC 80%Ratio 64%
Obstruction – airway diseases eg asthma, COPD, bronchiectasis

BLOOD GASES
Always look at pH first
normal means normal or compensation has occurred
PO2 cannot be interpreted without FiO2

BLOOD GASES
Type I respiratory failure
low PO2 only (PCO2 normal or low and pH normal)
Type II respiratory failure
low PO2 and high PCO2
pH may be normal (compensated – HCO3 will be raised) or reduced

BLOOD GASES
FiO2 0.6
pH 7.37pO2 10.3pCO2 3.1HCO3 25
CO2 + H2O H+ + HCO3

BLOOD GASES
FiO2 0.6
pH 7.47pO2 10.3pCO2 3.1HCO3 25
BLOOD GASES
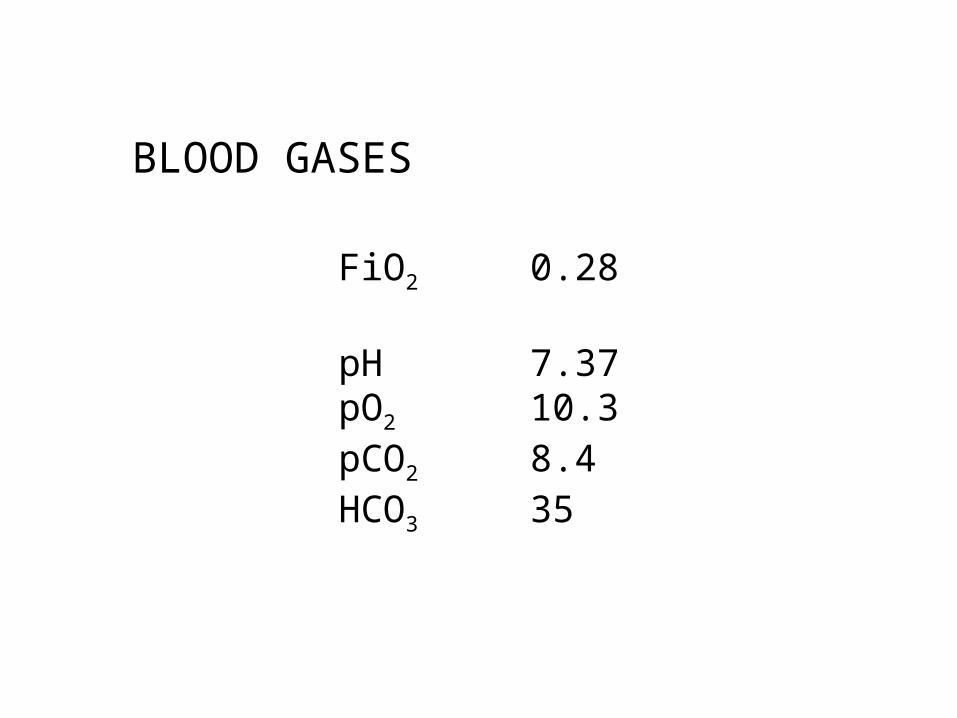
FiO2 0.28
pH 7.37pO2 10.3pCO2 8.4HCO3 35

BLOOD GASES
FiO2 0.6
pH 7.31pO2 10.3pCO2 8.4HCO3 24

BLOOD GASES
FiO2 0.6
pH 7.31pO2 10.3pCO2 8.4HCO3 15