osteochondritis dissecans jamie flint. patient presentation 16 year old male highly active ...
TRANSCRIPT
Osteochondritis DissecansJamie Flint

Patient Presentation 16 year old male Highly active Crutches training pre-surgery Decreased ROM in L knee Locking Pain Several months
Patient Presentation L knee Osteochondritis Dissecans
s/p ORIF L lateral femoral condyle OCD lesion
Evaluate and treat Non weight-bearing CPM Brace on at all times ROM, quad sets, and SLR
http://www.breg.com/products/knee-bracing/functional-ligament/fusion-xt-knee-brace

Clinical Decision Making Physician (Direct)
Adolescent bone growth Salvageable unstable lesion
Quadriceps not firing (Direct) Electrical stimulation or AROM
Father is a doctor, Mother is a nurse (Indirect) Both highly involved in POC
Appointment time (2:30pm Tue, Thur) Potential PTA referral (Refer)

Disease Taxonomy ICF Model
What he could/couldn’t do Easily transferred to patient
Health Condition L Osteochondritis Dissecans
Body Functions and Structures Decreased strength, A/PROM, pain,
balance
Disease Taxonomy (ICF) Activities
Sitting – difficult due to ROM Standing – non weight-bearing Walking – crutches Running – nope
Participation Sitting – watch television, classroom Unable to participate in sports Bathing and dressing difficult

Disease Taxonomy The classroom
Sitting difficult Elevation and icing Swelling – non compliance with icing Increased stiffness and pain Leave early for next class Limited participation Medications Grades – no complaints
Rigor (assessment tool) Reliability of knee joint range of motion and
circumference measurements after total knee arthroplasty: does tester experience matter? 19 outpatients (10 female) 1 inexperienced PT, 1 experienced PT 2 hour training session Blinded – curtain hanging over upper body Patient verbally stated “stop” at end ROM Goniometry and tape measure Relaxed knee, fully extended Pen mark 1cm proximal to patella
Rigor (assessment tool) Conclusions
Intra-rater reliability - .99 for both Inter-rater reliability - .98 to .99 Repeated knee goniometric and
circumferential measurements should be recorded by the same PT.
Tester experience appears not to influence the degree of reliability.
Jakobsen T, Christensen M, Christensen S, Olsen M, Bandholm T. Reliability of knee joint range of motion and circumference measurements after total knee arthroplasty: does tester experience matter?. Physiotherapy Research International [serial online]. September 2010;15(3):126-134. Available from: CINAHL with Full Text, Ipswich, MA. Accessed March 29, 2015.
Rigor (assessment tool) Circumferential measurements post
ACL reconstructive surgery 18 lower extremities 6 measurements around knee and thigh “specially made device” Velcro straps
around lateral leg Intra-rater reliability – (0.82-1.0) Inter-rater reliability – (0.72 – 0.97)
Soderberg, G. L., Ballantyne, B. T. and Kestel, L. L. (1996), Reliability of lower extremity girth measurements after anterior cruciate ligament reconstruction. Physiother. Res. Int., 1: 7–16. doi: 10.1002/pri.43

Rigor (intervention) Randomized Controlled Trial of the
Effectiveness of Continuous Passive Motion After Total Knee Replacement
141 adults post TKA Initial knee flexion <75 degrees 1 group 3 hours therapy 1 group 3 hours therapy + 2 hours CPM ROM, Length of stay, FIM, TUG, girth
measurements, self-reported index scores
Rigor (intervention) All subjects improved No statistical difference in discharge
outcome measures between groups Do the benefits outweigh the costs?
5 other studies had positive results 9 other studies found little value of CPM Systematic reviews, Meta-analysis, and
Cochrane study agree with findings
Herbold J, et. al. Randomized Controlled Trial of the Effectiveness of Continuous Passive Motion After Total Knee Replacement, 2014-07-01Z, 95: 7(1240-1245) American Congress of Rehabilitation Medicine. Accessed March 29th, 2015

Patient Education Learning style
Active experimentation Adolescent
Activity limitations (MD) Crutches training
Learned quickly, stair training Barriers
Parents MD and weight bearing status
PWB - 25 lbs every other day Using the scale
Cost Benefit Analysis Total # of visits – 20 (1 no charge) Insurance – Hospital health plan
(parents)
PT Evaluation $75.09 Therapeutic Exercises $32.36 Manual Therapy $30.08 Gait Training $28.64

Cost Benefit Analysis Total Cost - $1315.17 Out of pocket cost (25% of total) - $328.80 Benefits
Improve mobility Decrease pain Long-term effects Improve QOL Increase independence Get back to school and sports
Yes, satisfying quality of care
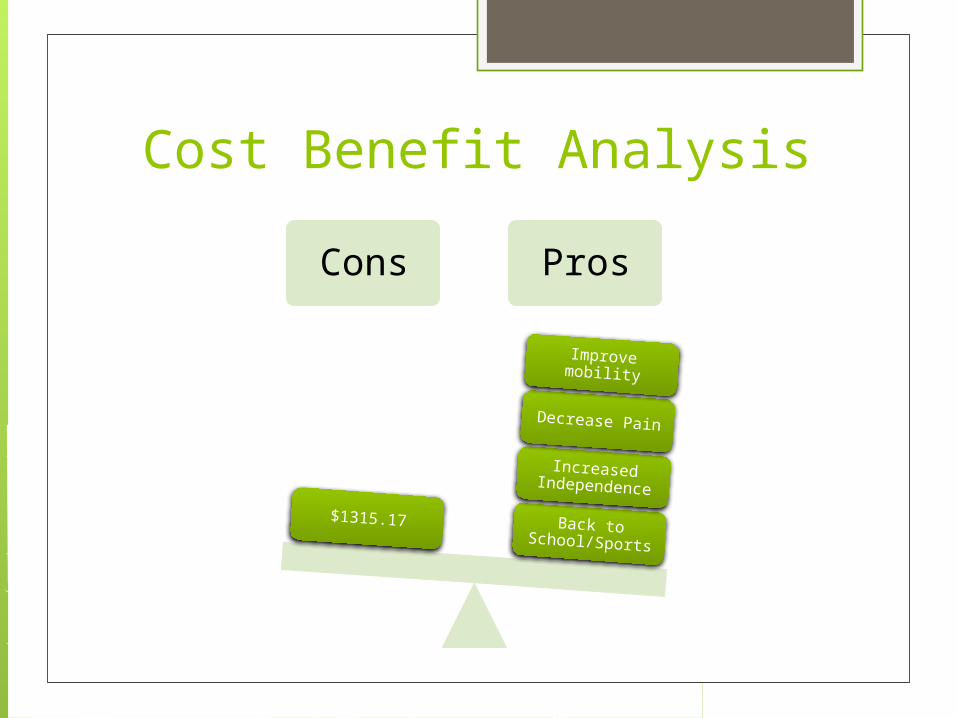
Cost Benefit Analysis
Cons Pros
Back to School/Sports
Increased Independence
Decrease Pain
Improve mobility
$1315.17
Evaluating Clinical Change Continue PT 1-2x/week for 8-12 weeks
or longer depending on length of non weight-bearing status.
Patient to assess need for further therapy scheduling for 1 visit/week or 1 visit every other week until his next appointment with MD.

Evaluating Clinical Change After PT intervention, patient will ambulate
100 ft independently without antalgic gait bilaterally in order to progress towards running/jogging for recreational sports(to be met within 6-8 weeks).
Following PT intervention, patient will demonstrate L knee AROM of 0-130 degrees without pain in order to perform all functional activities at home, in the school and the community. (to be met within 4-6 weeks)
Quality of Life Knee Injury and Osteoarthritis Outcome
Score (KOOS) Pain Symptoms Activities of daily living Sport and recreation function Knee-related quality of life
file:///Users/flint06/Downloads/Knee%20Injury%20and%20Osteoarthritis%20Outcome%20Score%20(KOOS).pdf

Values
MotivatedFamily
OrientedSports
OptimisticRespectfulEfficient
TimelinessGenuine
ProductiveProfessional
Patient Shared Physical Therapist
Patient Goals* He looked forward to:
Being stretched by PT (PROM) Riding on the recumbent bike
Pushing a weighted sled Improved push off during gait
His immediate first-time goals were unrealistic
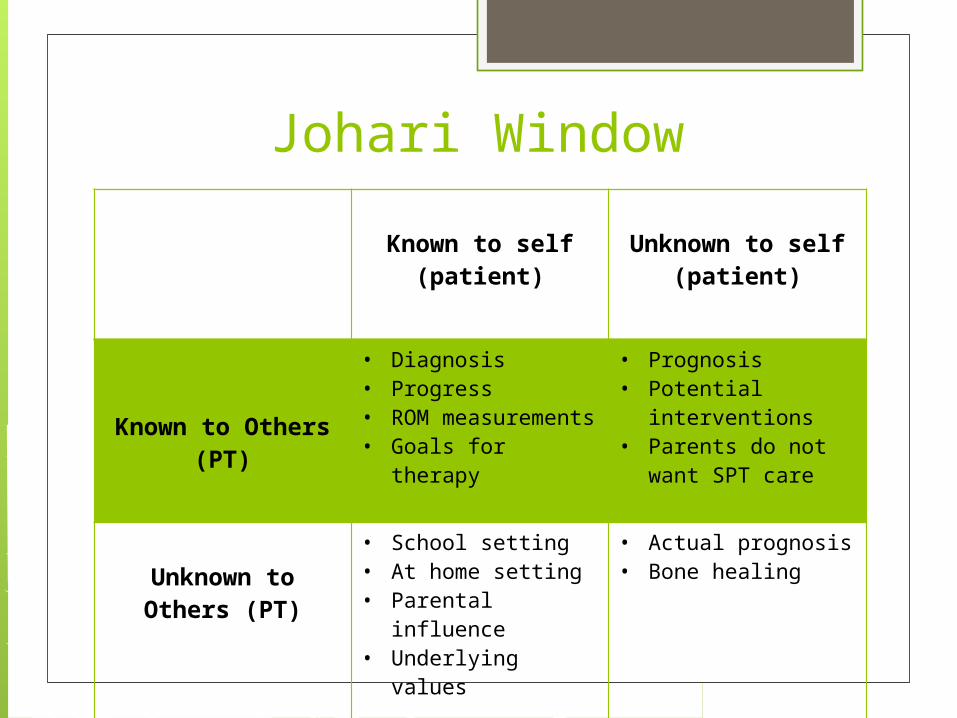
Johari Window
Known to self (patient)
Unknown to self (patient)
Known to Others (PT)
• Diagnosis• Progress• ROM
measurements• Goals for therapy
• Prognosis• Potential
interventions• Parents do not
want SPT care
Unknown to Others (PT)
• School setting• At home setting• Parental influence• Underlying values
• Actual prognosis• Bone healing
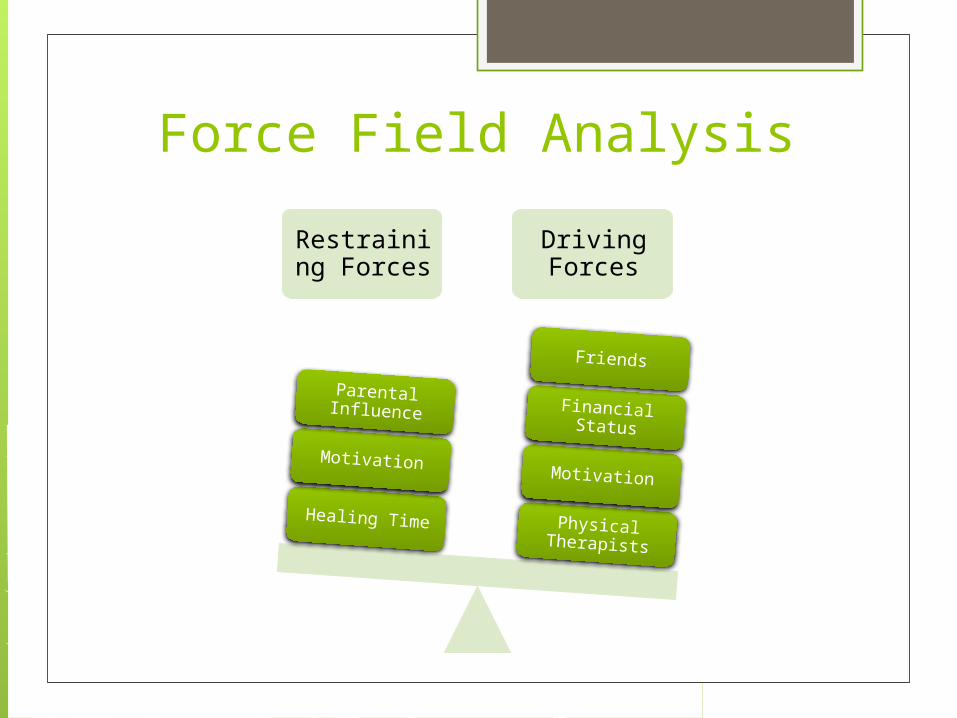
Force Field Analysis
Restraining Forces
Driving Forces
Physical Therapists
Motivation
Financial Status
Friends
Healing Time
Motivation
Parental Influence
Good to Know! Juvenile OCD has a better prognosis
than does adult OCD, with higher rates of spontaneous healing with conservative treatment
MRI remains to be the gold standard for diagnosing OCD lesions
Shock wave therapy to improve healing rate, bone and cartilage growth.
Ethical Issues Parental issues (Father is doctor) Student PT treatment
His normal PT was gone one day SPT (Me) performed interventions Still overseen by another PT 1 treatment no charge
2 Therapeutic Exercise ($65.00)
Evidence Based Practice Physical Therapy Management of
Patients with Osteochondritis Dissecans Initial Phase
Weight bearing restrictions Immobilization Decrease pain/swelling Normal mobility, ROM Improve muscle activation Retain muscle strength Enhance L/E neuromuscular control
Evidence Based Practice Intermediate Phase
Increased weight bearing Residual strength and muscle activation Both open and closed kinetic chain Initiate sports-specific maneuvers Balance/proprioception Minimum 4+/5 LE muscle strength
Evidence Based Practice Advanced Stage
Dynamic movement patterns Neuromuscular control of the athlete Encourage symmetry Higher volume activity Goal: return to sport
References Jakobsen T, Christensen M, Christensen S, Olsen M, Bandholm T. Reliability of
knee joint range of motion and circumference measurements after total knee arthroplasty: does tester experience matter?. Physiotherapy Research International [serial online]. September 2010;15(3):126-134. Available from: CINAHL with Full Text, Ipswich, MA. Accessed March 29, 2015. http://web.b.ebscohost.com.ezproxy.undmedlibrary.org/ehost/pdfviewer/
pdfviewer?vid=3&sid=61a96d2e-3d44-4f74-9edd-8630b55b35af%40sessionmgr198&hid=110
Soderberg, G. L., Ballantyne, B. T. and Kestel, L. L. (1996), Reliability of lower extremity girth measurements after anterior cruciate ligament reconstruction. Physiother. Res. Int., 1: 7–16. doi: 10.1002/pri.43 http://onlinelibrary.wiley.com.ezproxy.undmedlibrary.org/doi/10.1002/pri.43/abstract
Medicare Physician Fee Schedule http://www.apta.org/apta/advocacy/feecalculator.aspx?navID=10737423156
Pascual-Garrido C, Moran CJ, Green DW, Cole BJ. Osteochondritis dissecans of the knee in children and adolescents. Curr Opin Pediatr. February 2013;25(1):46-51. http://ezproxy.undmedlibrary.org/login?url=http://search.ebscohost.com.ezproxy .undmedlibrary.org/login.aspx?direct=true&AuthType=ip,url,uid,cookie&db=c8h&AN=2011896384&site=ehost-live. doi: 10.1097/MOP.0b013e32835adbf5.

References Phillips M, Pomeranz S. Imaging of Osteochondritis Dissecans of the Knee. Operative
Techniques in Sports Medicine. 2008; 16(2). Published 2008. Accessed December 2014. https://www-clinicalkey-com.ezproxy.undmedlibrary.org/#!/content/playContent/1-s2.0-S1060187208000336
Lyon R, Cheng Liu X, Kubin M, Schwab J. Does Extracorporeal Shock Wave Therapy Enchance Healing of Osteochondritis Dissecans of the Rabbit Knee? Clinical Orthopaedics and Related Research. 2012 471(4): 1159-1165. Available from PubMed. Accessed December 2014. http://link.springer.com.ezproxy.undmedlibrary.org/article/10.1007%2Fs11999-012-2410-8
Herbold J, et. al. Randomized Controlled Trial of the Effectiveness of Continuous Passive Motion After Total Knee Replacement, 2014-07-01Z, 95: 7(1240-1245) American Congress of Rehabilitation Medicine. Accessed March 29th, 2015 https://www-clinicalkey-com.ezproxy.undmedlibrary.org/#!/content/playContent/1-s2.0-
S0003999314002196 Paterno M, Prokop T, Schmitt L. Physical Therapy Management of Patients with
Osteochondritis Dissecans. Clinics in Sports Medicine. 2014 33 (2): 353-374. Available from PubMed. Accessed December 2014. https://www-clinicalkey-com.ezproxy.undmedlibrary.org/#!/content/playContent/1-s2.0-S0278591914000027