our vision as the leading global provider of fitness and wellness education, canfitpro empowers...
TRANSCRIPT
Our Vision
• As the leading global provider of fitness and wellness education, canfitpro empowers people to lead passionate and fulfilling lives through safe, fun, and effective physical activity.

Our Mission
• United as members, canfitpro delivers the world's best, accessible, affordable, and attainable fitness education and experiences.

Making Professionalism Easy!
canfitpro INTERACTIVE
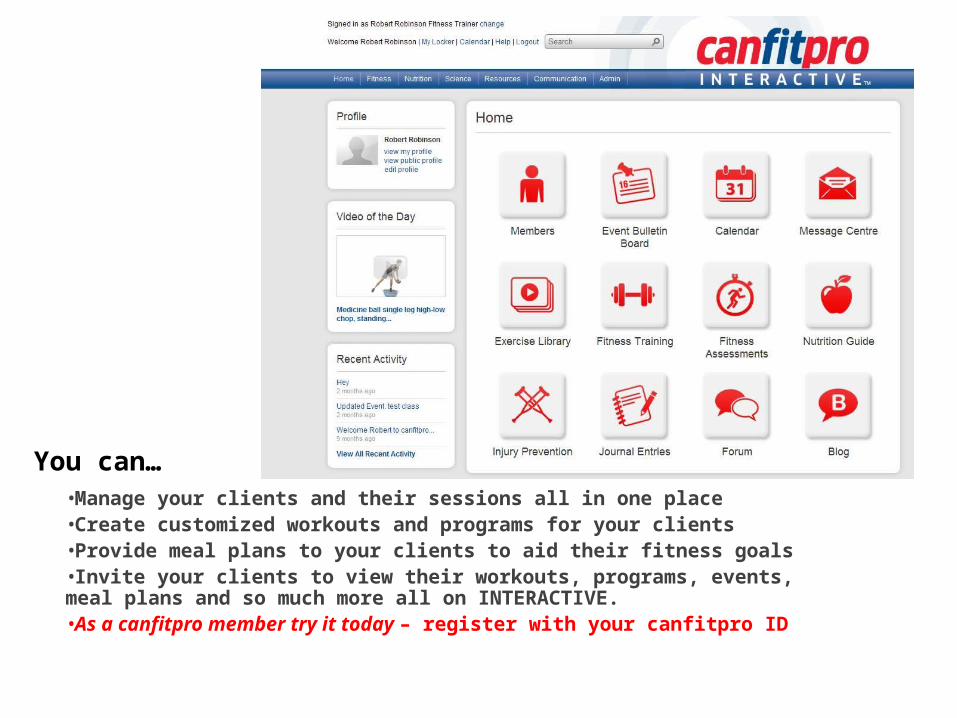
You can…
•Manage your clients and their sessions all in one place•Create customized workouts and programs for your clients•Provide meal plans to your clients to aid their fitness goals •Invite your clients to view their workouts, programs, events, meal plans and so much more all on INTERACTIVE.•As a canfitpro member try it today – register with your canfitpro ID

To see thousands of exercise demonstrationsVisit us at www.canfitprointeractive.com
canfitpro INTERACTIVE
Your credentials matter
Why be part of the register?
Mission Statement The mission of repscanada is to increase
the credibility of the fitness profession by providing a centralized location where consumers and employers can identify and verify fitness certifications and standards.
www.repscanada.com

Acknowledgments
• Human Kinetics (USA and Canada)• Primal Pictures Ltd. (UK)
Principles of Fitness, Health and Wellness
Foundations of Professional Personal TrainingChapter 1
Components of Fitness
Primary Components– Cardiorespiratory capacity– Muscular capacity– Flexibility– Body composition
Secondary Components– Balance– Coordination– Agility– Reaction time– Speed– Power– Mental capability
Health and Wellness

Benefits of Physical Activity
• What are they?

canfitpro’s Recommendations on Physical Activity, Nutrition, and Mindset for Optimal Health
Aerobic Activity Accumulate up to 300 minutes of moderate-intensity aerobic or 150 minutes of vigorous-intensity per week.
Muscle Strengthening Major muscle groups worked 3 or more days per week.
Flexibility Enjoy flexibility exercises 4 or more days per week.
Nutrition Implement health promoting nutrition and hydration.
Mindset Adopt strategies for a positivemindset.
Components of Fitness
Primary Components
• Cardiorespiratory Capacity• Muscular Capacity• Flexibility• Body Composition
Secondary Components
• Balance• Coordination• Agility• Reaction Time• Speed • Power• Mental Capacity
canfitpro Training Principles
• FITT• Individualization• Specificity• Progressive overload
• Recovery• Structural tolerance• All-around development• Reversibility• Maintenance
Nutrition Concepts for Personal Trainers
Foundations of Professional Personal TrainingChapter 2

Nutrition
Nutrition is the study of food and how the body uses it. Nutrients are chemical components of
foods that are essential for energy, growth, cellular repair and regulation of metabolic
functions.
Scope of Practice - Defined
• Scope of Practice → is a term used to set boundaries for various professions that define the procedures, actions, and processes they are permitted to practice
• The Scope of Practice is limited to that which the individual has received education and experience, and in which he/she has demonstrated competency
Scope of Practice and Personal Training
• With regard to nutritional counseling– Personal trainers should develop a referral system
(dietician, naturopathic, medical doctor)– Gain additional education (Nutrition & Wellness
Specialist)– Only offer general nutritional advice and
information based on Canada’s Food Guide
Scope of Practice and Personal Training con’t
• Personal Trainer’s are not permitted to:– Prescribe or recommend supplements of any kind– Perform a client diet analysis
Essential Nutrients
• Carbohydrates• Fat• Protein• Vitamins• Minerals
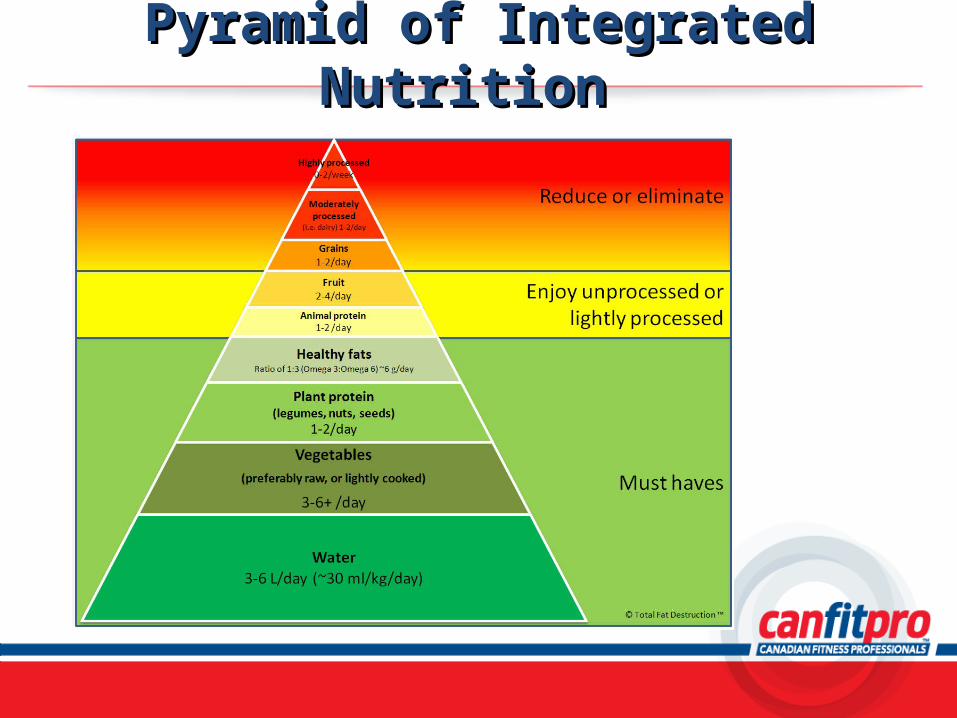
Pyramid of Integrated Nutrition Pyramid of Integrated Nutrition
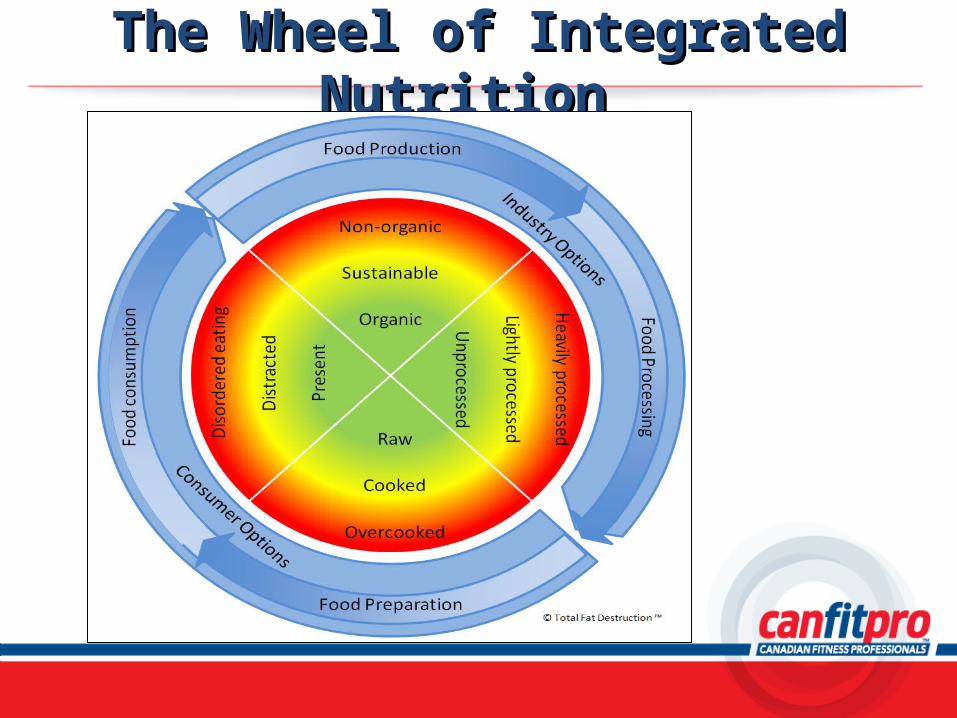
The Wheel of Integrated Nutrition The Wheel of Integrated Nutrition
Nutrition
•Pyramid of Integrated Nutrition
•The Wheel of Integrated Nutrition
•Hydration
Carbohydrates
• What is a carbohydrate and it’s function?• 2 categories of carbohydrate
– Simple (sugars → jam, syrup, honey, fruit)– Complex (bread, pasta, cereal, potatoes,
vegetables)– What are the best sources of carbohydrate?
Carbohydratesand Calories
• One gram of carbohydrate = 4 calories– One granola bar contains 23 g of carbohydrate.
What is the total amount of calories from carbohydrate for one bar?
– One cup of Cheerios breakfast cereal contains a total of 80 calories from carbohydrate. How many grams of carbohydrate are in one cup of cereal?
» 45% to 65% of total caloric intake» No more than 25% from simple sugars
Carbohydrates and Exercise
• The higher the intensity of exercise, the greater the reliance on carbohydrate – Relates to anaerobic metabolism which uses only glucose
as fuel• Even lower intensity exercise uses carbohydrate but to a
lesser extent because fat can also be used• Ideally, active people should consume complex and simple
carbohydrates during and immediately after exercise.
Fat• What is fat and it’s function?• 3 types of lipids in food
– Triglycerides (represents 95% of fat we eat)• Chain length determines digestion, absorption and function
– Phospholipids– Sterols– What are the best sources of fat?
Fat and Calories
• One gram of fat = 9 calories– One granola bar contains 3 g of fat. What is the
total amount of calories from fat for one bar?– One cup of Cheerios breakfast cereal contains a
total of 18 calories from fat. How many grams of fat are in one cup of cereal?
» 20% to 35% of total caloric intake
Fat and Exercise
• How are lipids used in exercise?– The lower the intensity of exercise, the greater the proportion of fat
burned to satisfy energy needs– As exercise intensity increases the proportion of fat burned
decreases and the proportion of carbohydrates increases– As exercise intensity increases the total number of calories burned
increases– Although the proportion of fat burned decreases to satisfy the
energy needs of the higher intensity activity, the total energy requirement increases and therefore the total volume of fat burned is greater
Protein
• What is protein and it’s function?• Made up of amino acids
– Complete protein– Incomplete protein– What are the best sources of protein?
Protein and Calories
• One gram of protein = 4 calories– One granola bar has 2 g of protein. What is the
total amount of calories from protein for one bar? – One cup of Cheerios breakfast cereal contains a
total of 12 calories from protein. How many grams of protein are in one cup of cereal?
» 10% to 35% of total caloric intake» 0.8 g / kg of body weight
Protein and Exercise
• If protein is being used to fuel exercise then not enough carbohydrate has been consumed
• It’s best suited for other body functions• It takes longer to digest and therefore not
recommended immediately before or during exercise.
Vitamins
• What are vitamins and their function?• 2 categories of vitamins
– Water soluble• Vitamin B complex, vitamin C
– Fat soluble• Vitamins A, D, E, K
– How can you maximize your vitamin intake?
Minerals
• What are minerals and their function?• Examples:
– Sodium, potassium → regulate body fluid– Calcium, phosphorus → bone health– Iron → carries hemoglobin which transports oxygen– Iodine → regulates metabolism
Water
• How important is water intake?• What is the function of water?• Water and exercise
– Consume 8-16 ounces one hour before– 8 ounces 20 minutes before– 4-8 ounces every 10 to 15 min. during– 16 ounces for every pound of weight lost after exercise
Ergogenic Aids
• As a personal trainer– Respect the scope of your abilities and refer clients
to a nutritionist– Your responsibility is to help clients by offering
general nutritional advice and info– You should not recommend any sport supplements
or ergogenic aids and refer clients to appropriate professional
Designed to improve physiological or psychological functions.
A Plan for Good Nutrition
How can we help clients to eat better?
What are 4 guidelines for developing a healthy
diet?
Nutrition Mix and Match
Nutrient
A) CarbohydrateB) WaterC) MineralsD) ProteinE) VitaminsF) Fat
Function
1. Needed for healthy body functions; individual needs and requirements
2. Major fuel source; essential for hormone production, healthy skin, transport some vitamins
3. Growth and repair of tissue4. Makes up 60% of body; used
for all body functions5. Water and fat soluble6. Fuel for brain and nervous
system
Bioenergetics
Foundations of Professional Personal TrainingChapter 3
Bioenergetics Bioenergetics ConceptsConcepts
Chapter 2Chapter 2
DefinitionsDefinitions
Bioenergetics
Energy
Homeostasis
Metabolism
Bioenergetics
Bioenergetics is the study of how energy flows in the human body.
Bioenergetics• Key terms
– Energy– Homeostasis– Metabolism
Adenosine Triphosphate (ATP)
• What is ATP?– Adenosine - P ~ P ~ P
• How is ATP created?– Anaerobic metabolism
• ATP-CP phosphagen system• Glycolytic or lactic acid system
– Aerobic metabolism• Aerobic or oxidative energy system
ATP-CP Phosphagen System
• ATP-CP Phase 1– Uses stored ATP (1-2 seconds at maximal effort)– ATP (splits) → ADP + P + energy
• ATP-CP Phase 2– Split of CP to create more ATP (10 seconds of intense
effort)– ADP + CP → ATP + creatine
↑ creatine kinase
Glycolytic System• Provides fuel for up to 2 min. at maximal intensity• Breakdown of carbohydrate in the form of glycogen stored in
the muscle cell– Glycogen → 3ATP
• Breakdown of carbohydrate in the form of glucose stored in the blood– Glucose → 2ATP + 2LA (lactic acid) + heat
• As more glucose is metabolized, more lactic acid is produced• ↑ lactic acid in the cell = ↑ cell acidity = ↓ muscle contraction speed and strength
Aerobic Glycolysis
• Provides fuel for more than 2 min. at moderate intensity• Breakdown of glucose or glycogen (with oxygen present)
– Glucose + O2 → 38ATP + CO2 + H2O + heat
• Mitochondria is the site of aerobic metabolism• System is limited by ability of cardiorespiratory system to
deliver O2
Fatty Acid Oxidation
• Provides fuel for over 2 min. during low-intensity exercise• Breakdown of fatty acids (with oxygen present)
– Fatty acid + O2 → 100ATP + CO2 + H2O + heat
• Fatty acids are high energy fuel but they require large amounts of oxygen for reaction to take place
• System is virtually unlimited, but few people exercise for extreme durations; those that do use up a great deal of body fat
Lactate Threshold
• One concept that is important to understand regarding strenuous exercise is the lactate threshold (LT)
• The LT is the point at which the aerobic system cannot supply enough ATP for the needs of the body, forcing the anaerobic systems to increase their contribution of ATP.
Lactate Threshold con’t
• When does this occur?• What is the resulting by-product?• What does this mean for more
conditioned/fitter clients?
Interaction of the Systems
• At rest• At the beginning of exercise• During steady-state exercise• During strenuous exercise• During recovery
Oxygen Demands
• Oxygen deficit– The volume of oxygen missing in the first few minutes of
exercise
• Oxygen debt– When we stop exercising we still have an elevated oxygen
delivery and this extra oxygen is used to rebuild needed supplies of CP and ATP as well as to assist the liver in the breakdown of left over lactic acid
Developing the Energy Systemswith Interval Training
• Program variables– Work-to-rest ratio– Type of relief
• ATP-CP, glycolytic, oxidative
– Level of intensity– Arranging work and rest times
• Important considerations
Cardiorespiratory Concepts
Foundations of Professional Personal TrainingChapter 4
Cardiovascular System
• Heart• Arteries• Veins
Cardiovascular System Functions
• Transportation of nutrients, oxygen, carbon dioxide, metabolic waste and hormones
• Maintaining core temperature of the body
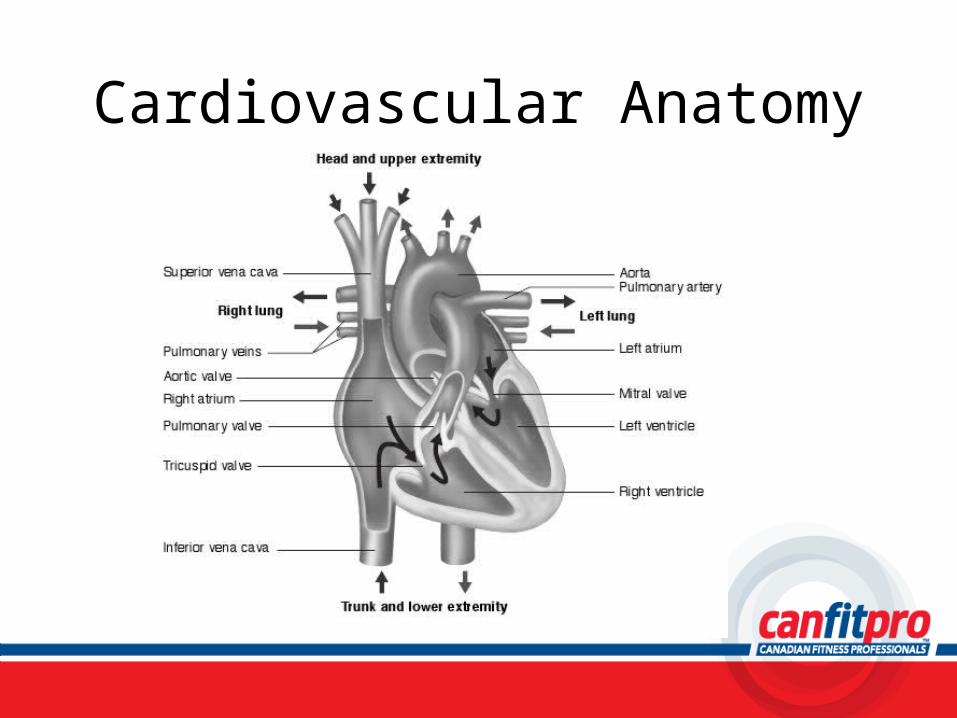
Cardiovascular Anatomy
Circulation of Blood Through the Body
• Veins carry blood towards the heart• Arteries carry blood away from the heart• Right side before left• Atrium before ventricle
Blood Pressure
• Systolic pressure• Diastolic pressure• Average resting BP is 120/80
What happens to blood pressure during exercise?
Heart Rate• Resting HR = approximately 72 bpm• Pulse - felt at arteries close to the skin
– Carotid artery– Brachial artery– Radial artery
• Max HR = 220 – age• ↑ in oxygen demands ↑ in HR
Stroke Volume
• Amount of blood that the left ventricle ejects in one beat
• Typical male has a SV of around 70 ml/beat• As client becomes fitter = SV increases
Cardiac Output
• Q = SV x HR
How does Cardiac Output change during exercise?

Respiratory System
• Made up of left and right lungs and air passage way
• Allows gas exchange between blood and the environment
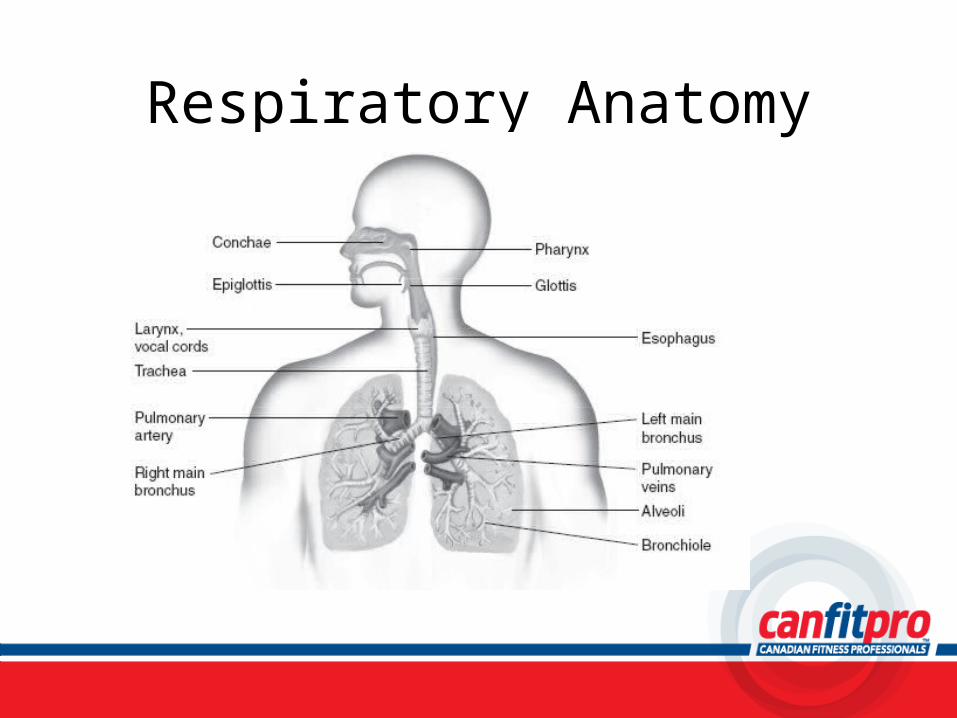
Respiratory Anatomy
Exercise Response
• Cardiovascular system– ↑ in HR, SV, Q – Vasoconstriction,
Vasodilation– BP
• ↑ in systolic pressure• Diastolic remains same or
slightly decreses
• Respiratory System– ↑ Rate of respiration
• Pulmonary ventilation – at rest = 10 L/min– First few minutes of
exercise it can ↑ to 45 L/min
– After 2 min, once client has reached homeostasis it can ↑ to 60 L/min
Physiological Benefits
• Summary– ↑ SV– ↑ blood delivery– ↑ red blood cells– ↑ capillary density– ↑size and number of mitochondria– ↑aerobic enzymes
System Integration
• Efficiency of the cardiovascular, respiratory and muscular systems
• Measured as aerobic capacity = VO2max– Maximum amount of O2 the body can extract and
use in the process of energy production
Aerobic fitness
Cardiorespiratory Recovery
• After exercise stops, O2 consumption remains elevated (EPOC)
• Light activity = recovery period that is short and unnoticeable
• Intense activity = recovery period lasting many hours, even days
• Active recovery
How can a personal trainer assist their clients with cardiorespiratory recovery?

Benefits of Cardiorespiratory Training
• What are they?

Exercise Prescription
• Cardiorespiratory Training– FITT– Considerations
• Number of sessions client is able to commit to• Clients current fitness level• Clients goals for cardiorespiratory training
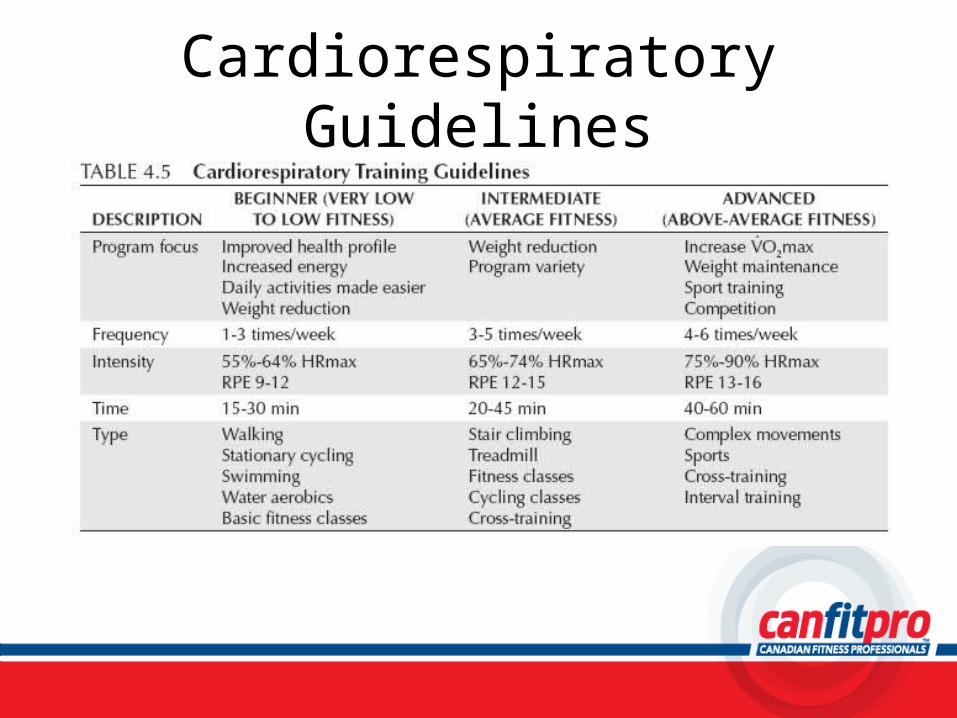
Cardiorespiratory Guidelines
Monitoring Intensity• HR• Rate of Perceived Exertion (RPE)• Talk test
Target HR Zone Calculation
Maya is a 25 year old beginner with a resting HR of 75.
Calculate her training zone.
AnswersLower target heart rate
= (220 – 25) x .55= 195 x .55= 107 bpm
Upper target heart rate = (220 – 25) x .64= 195 x .64= 125 bpm
Heart Rate Reserve Calculation
Nolan is a 30 year old intermediate with a resting HR of 70 bpm.
Calculate his training zone.
AnswersLower target heart rate
= {[(220 – 30) – 70] x .65} + 70= [(190 – 70) x .65] + 70= (120 x .65) + 70= 78 + 70= 148 bpm
AnswersUpper target heart rate
= {[(220 – 30) – 70] x .74} + 70= [(190 – 70) x .74] + 70= (120 x .74) + 70= 88.8 + 70= 159 bpm
Rate of Perceived Exertion
• Borg Scale• Modified Borg Scale
Case Study
Howard is a 35 year old investment advisor who wants to increase his lean muscle mass, improve his VO2 max as well as drop the 20 pounds he has gained from too many business lunches. Howard plays golf in the summer and hockey in the winter. He worked out in university but has not be in a gym in 5 years. His resting HR is 78 bpm and his resting BP is 122/84. He is 6 feet tall and weighs 210 pounds. Howard is able to work out for 1 hour 5 days a week.
Skeletal Anatomy and Flexibility
Foundations of Professional Personal TrainingChapter 5
Skeletal Overview
• Human adult skeleton has 206 bones• Born with 270 bones
– fuse to 206 by age 20 25‑
• Minor differences between men & women– Men → generally larger and heavier– Women → larger pelvic capacity for childbirth
Skeletal Overview con’t
• Four essential functions of skeleton– Protect vital organs and soft tissue– Factory where red blood cells are produced – Serve as reservoir for minerals– Provides attachment for muscles to produce
movement
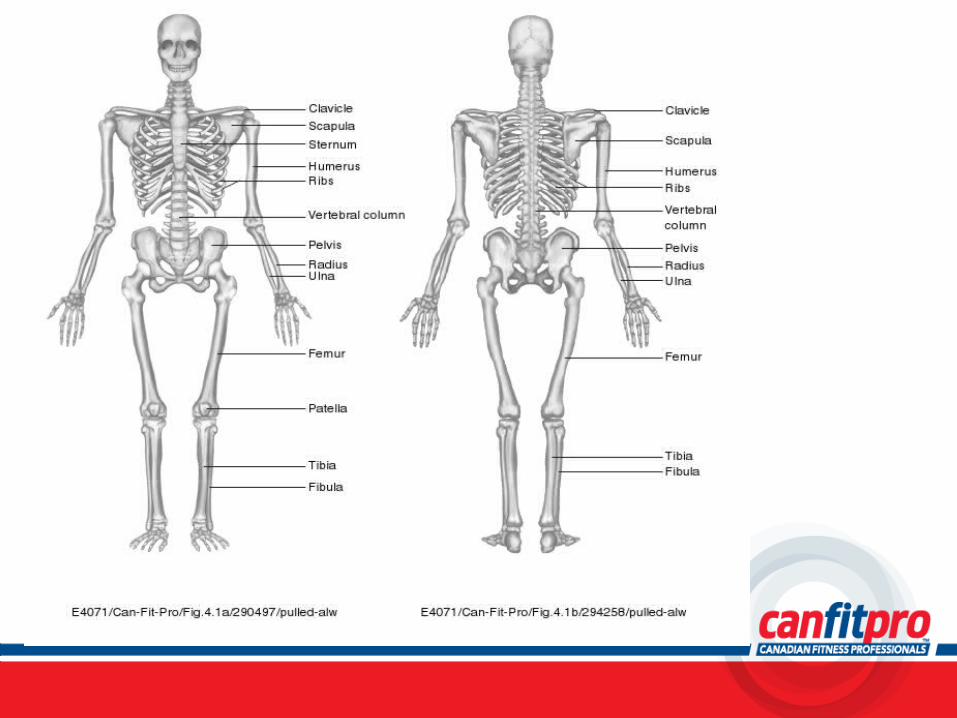
The Human Skeleton
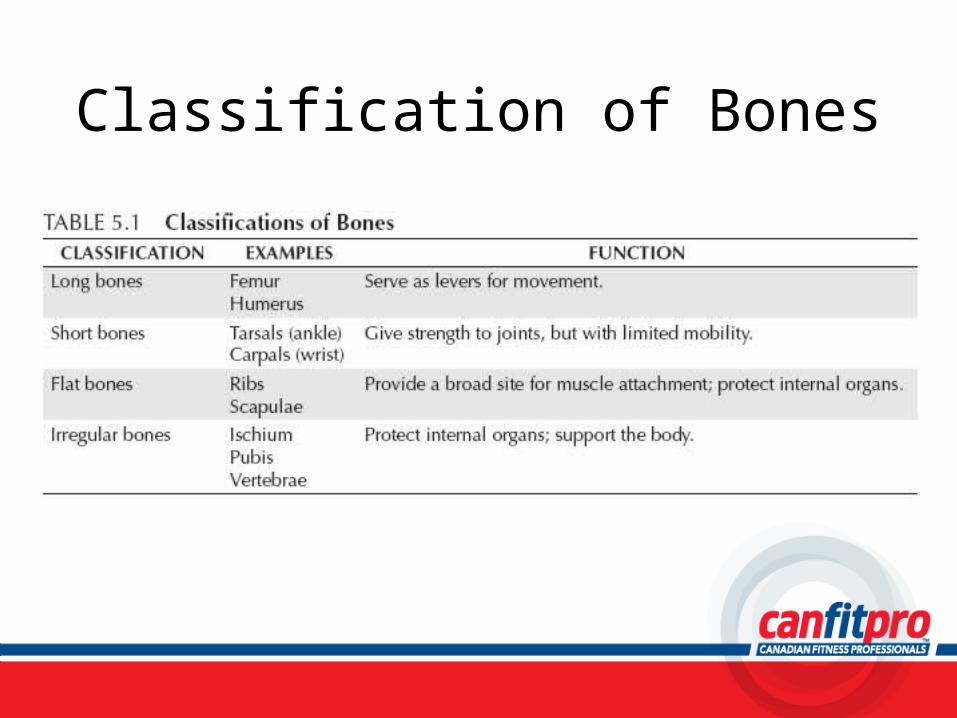
Classification of Bones
Parts of the Skeleton
• Axial Skeleton– Includes 80 bones
• Skull• Spine• Ribs• sternum
• Appendicular Skeleton– Includes 126 bones
• Shoulders• Pelvis• Bones in limbs
Anatomical Position
What is anatomical position?
Anatomical Terminology• Anterior/Posterior• Medial/Lateral• Superior/Inferior• Supine/Prone• Dorsal/Plantar• Proximal/Distal
Joint Movement Terminology
• Joint = place where bones meet– Flexion / Extension– Hyperextension– Abduction (protraction) / Adduction (retraction)– Circumduction
Joint Movement Terminology con’t
– Medial Rotation / Lateral Rotation– Supination / Pronation– Inversion / Eversion – Elevation / Depression
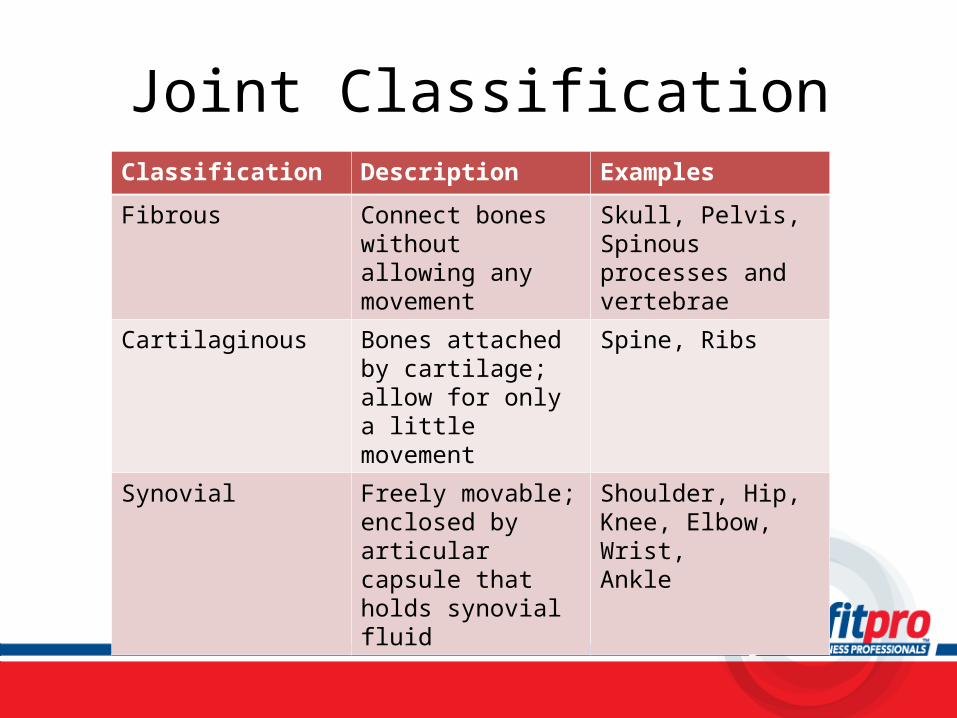
Joint ClassificationClassification Description Examples
Fibrous Connect bones without allowing any movement
Skull, Pelvis, Spinous processes and vertebrae
Cartilaginous Bones attached by cartilage; allow for only a little movement
Spine, Ribs
Synovial Freely movable; enclosed by articular capsule that holds synovial fluid
Shoulder, Hip, Knee, Elbow, Wrist, Ankle
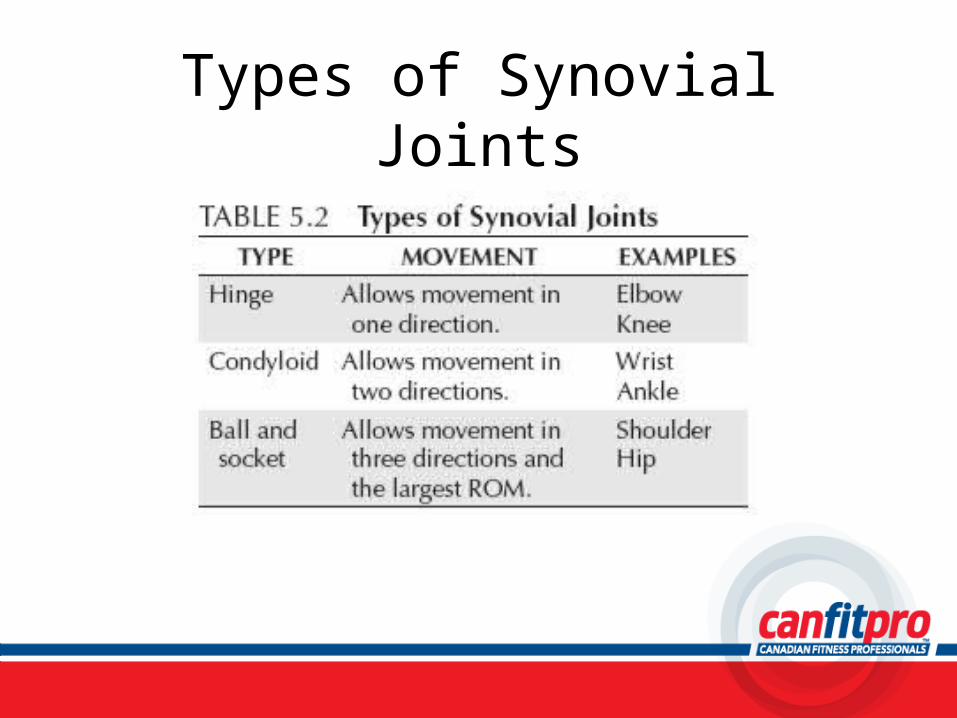
Types of Synovial Joints
Flexibility• FITT
– Frequency– Intensity– Time– Type
Flexibility Techniques
Static Stretching• What is it?
– Goal– Example– Advantage/Disadvantage
Dynamic Stretching• What is it?
– Goal– Example– Advantage/Disadvantage
Flexibility Guidelines
• What are they?
Stretches for all Major Muscle Groups
• Refer to Appendix B, page 253 - 264

Muscular Concepts
Foundations of Professional Personal TrainingChapter 6
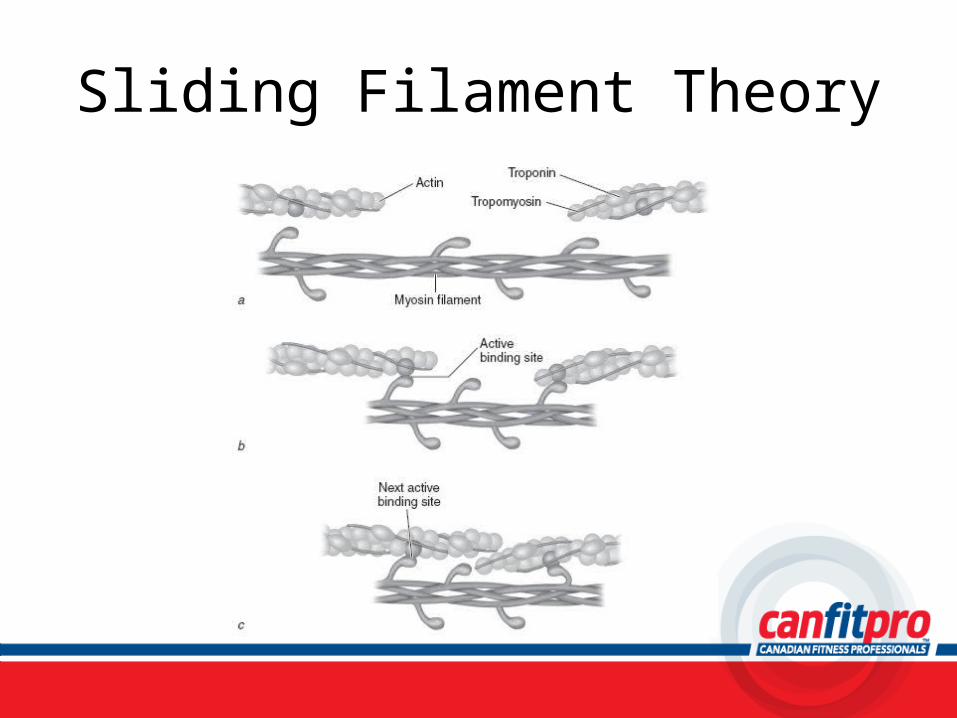
Sliding Filament Theory
Types of Muscle Contractions
• Isotonic → concentric• Isotonic → eccentric• Isometric
Nervous System
• Basic Organization– To perform coordinated and skilled movements,
you must have coordination between the muscular & nervous system
– 2 parts to the nervous system• Central Nervous System (CNS)• Peripheral Nervous System (PNS)
Organization of the Nervous System
CNS• Composed of the brain
and spinal cord• Control centre
PNS• Composed of nerves that
connect the extremities to the brain
• Delivers information about all body parts to the brain (CNS) for processing
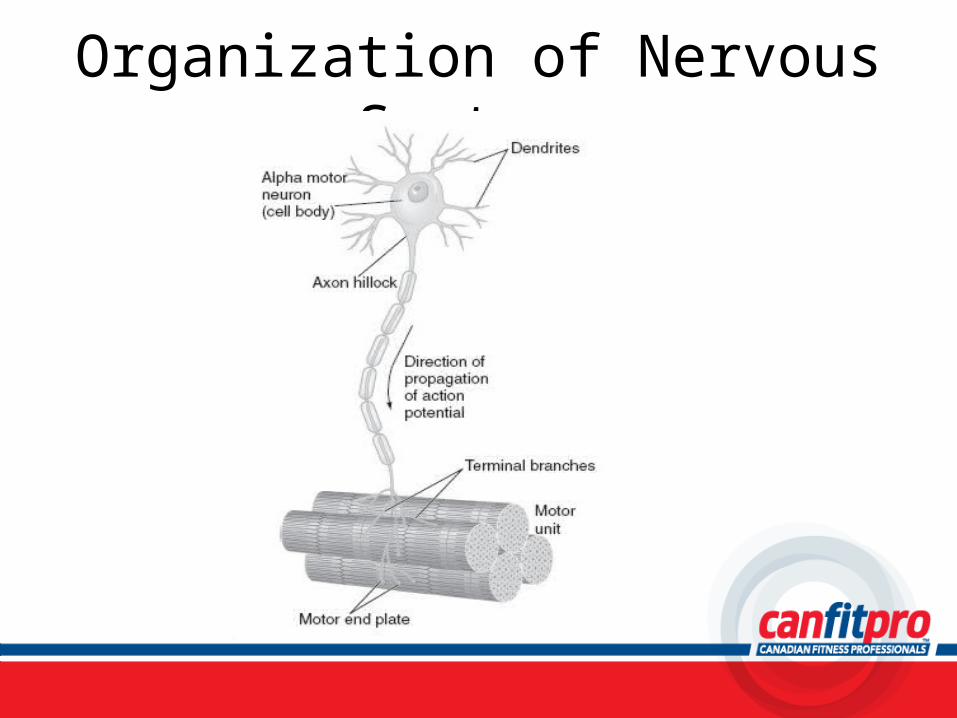
Organization of Nervous System
Muscle Fibre Types
• Slow twitch• Fast twitch
Muscle Anatomy and Action
• Muscles pull on bones to create movement at a joint
• Prime movers/agonists• Antagonists• Synergists
Major Muscles of the Body
• More than 600 muscles in the human body • Skeletal muscles produce movement by exerting
force on tendons which pull on bones• Most muscles cross a joint and attach to the
articulating bone that forms that joint
Major Muscles of the Body con’t
• Origin → where a muscle begins (proximal)• Insertion → where a muscle ends (distal)• When a muscle contracts it pulls the insertion
towards the origin
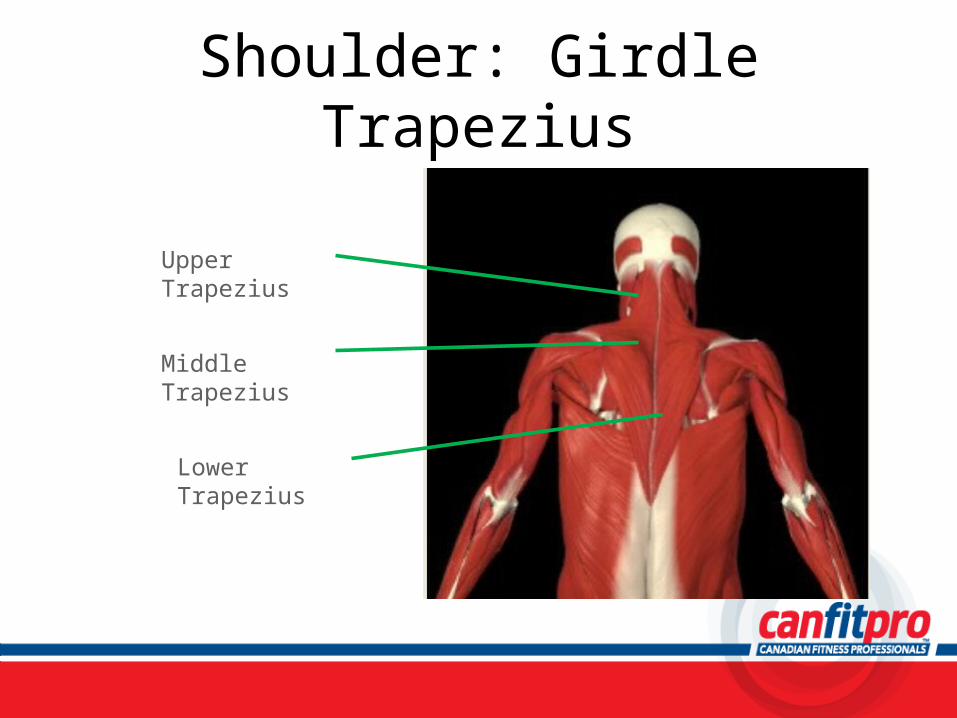
Shoulder: Girdle Trapezius
Upper Trapezius
Middle Trapezius
Lower Trapezius
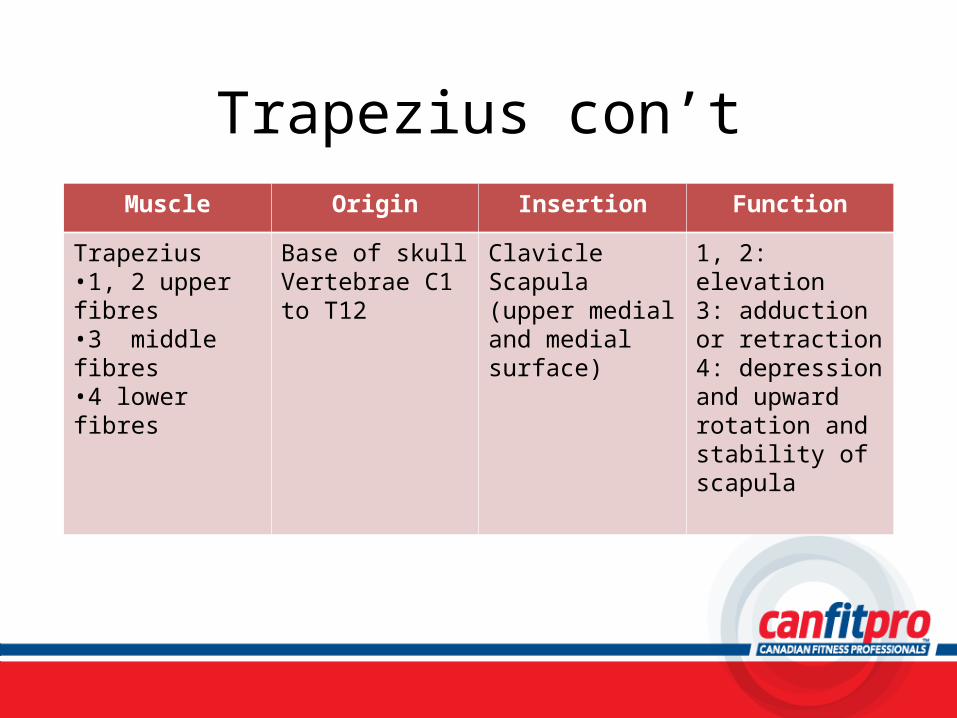
Trapezius con’tMuscle Origin Insertion Function
Trapezius•1, 2 upper fibres•3 middle fibres•4 lower fibres
Base of skullVertebrae C1 to T12
ClavicleScapula (upper medial and medial surface)
1, 2: elevation3: adduction or retraction4: depression and upward rotation and stability of scapula
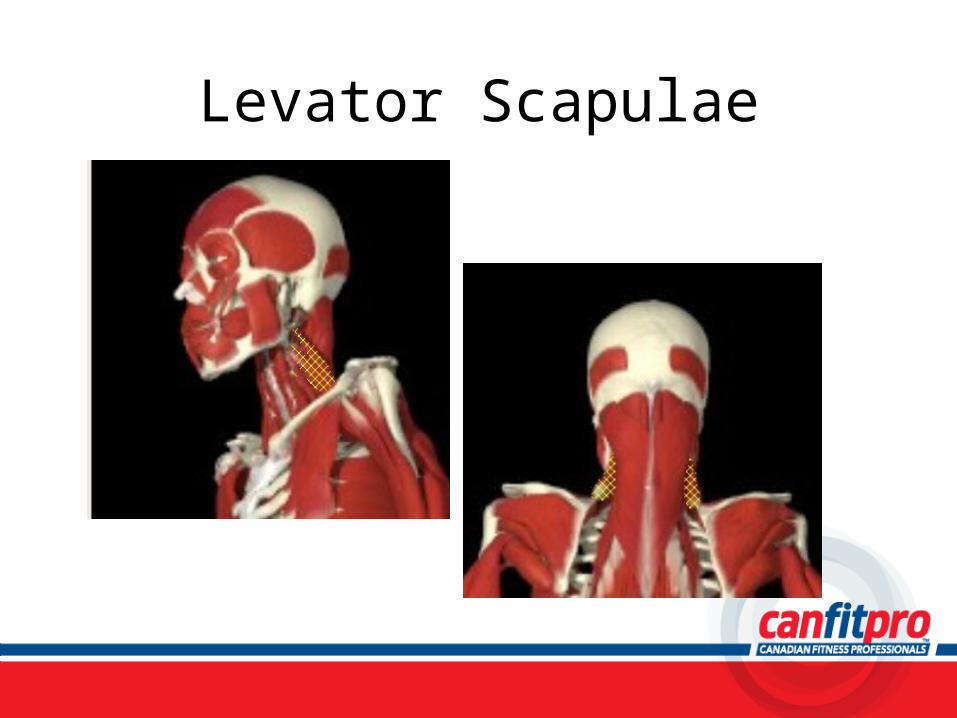
Levator Scapulae
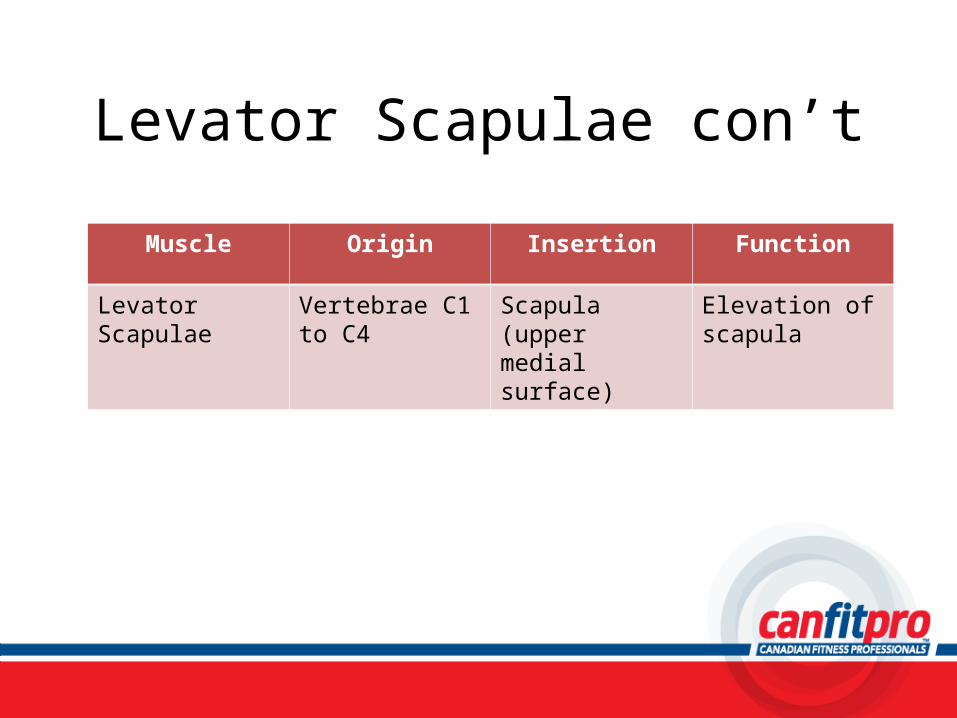
Levator Scapulae con’t
Muscle Origin Insertion Function
Levator Scapulae Vertebrae C1 to C4
Scapula (upper medial surface)
Elevation of scapula
Exercises:Trapezius and Levator Scapulae
• Dumbbell Trap Shrug (seated)– Page 209
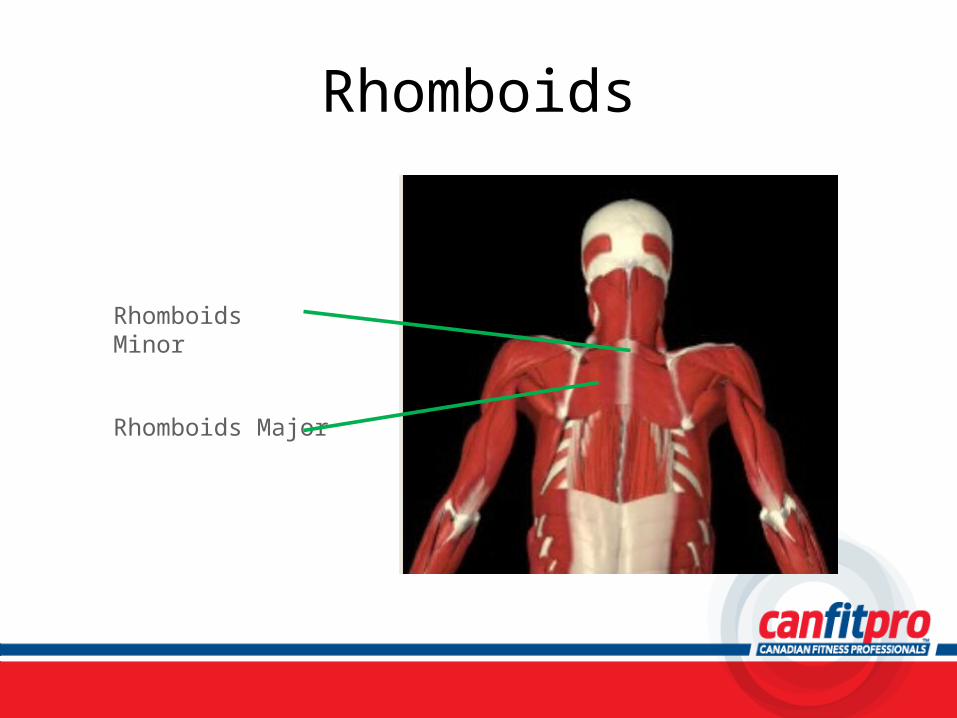
Rhomboids
Rhomboids Minor
Rhomboids Major
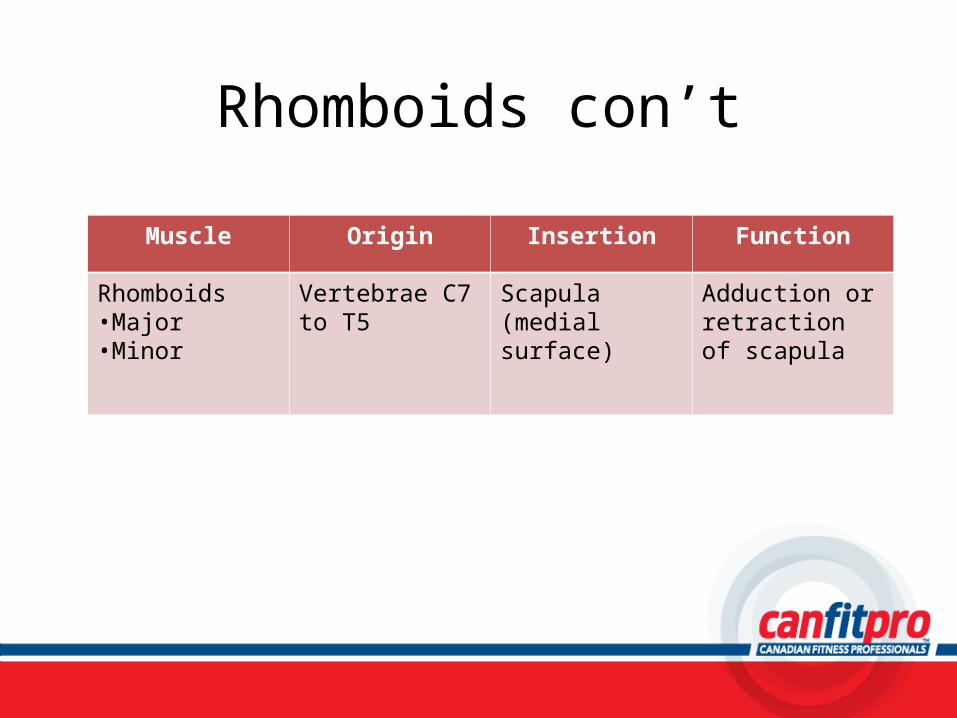
Rhomboids con’t
Muscle Origin Insertion Function
Rhomboids•Major•Minor
Vertebrae C7 to T5
Scapula (medial surface)
Adduction or retraction of scapula
Exercise: Rhomboids
• Cable Lat Row (seated with V-bar)– Page 205
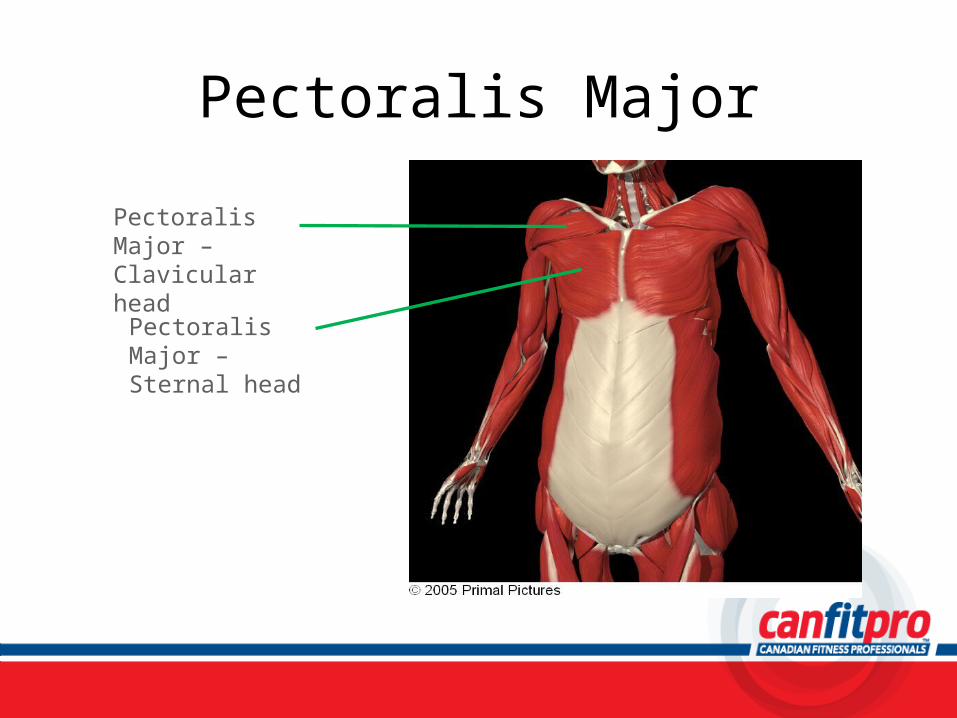
Pectoralis Major
Pectoralis Major – Clavicular head
Pectoralis Major – Sternal head
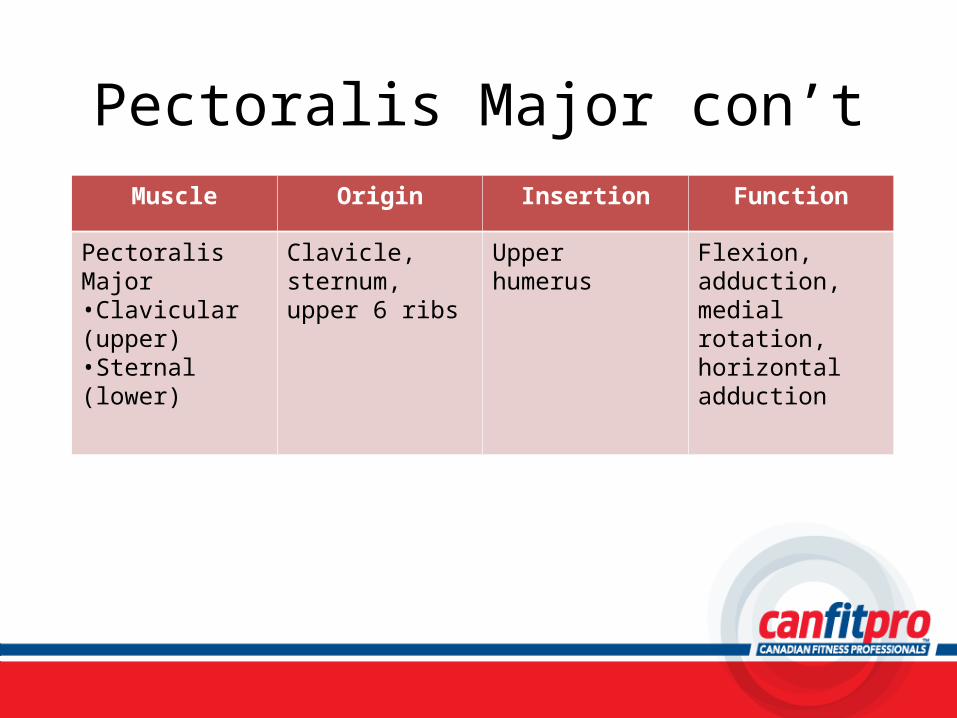
Pectoralis Major con’tMuscle Origin Insertion Function
Pectoralis Major•Clavicular (upper)•Sternal (lower)
Clavicle, sternum, upper 6 ribs
Upper humerus Flexion, adduction, medial rotation, horizontal adduction
Exercise: Pectoralis Major
• Barbell Chest Press– Page 197
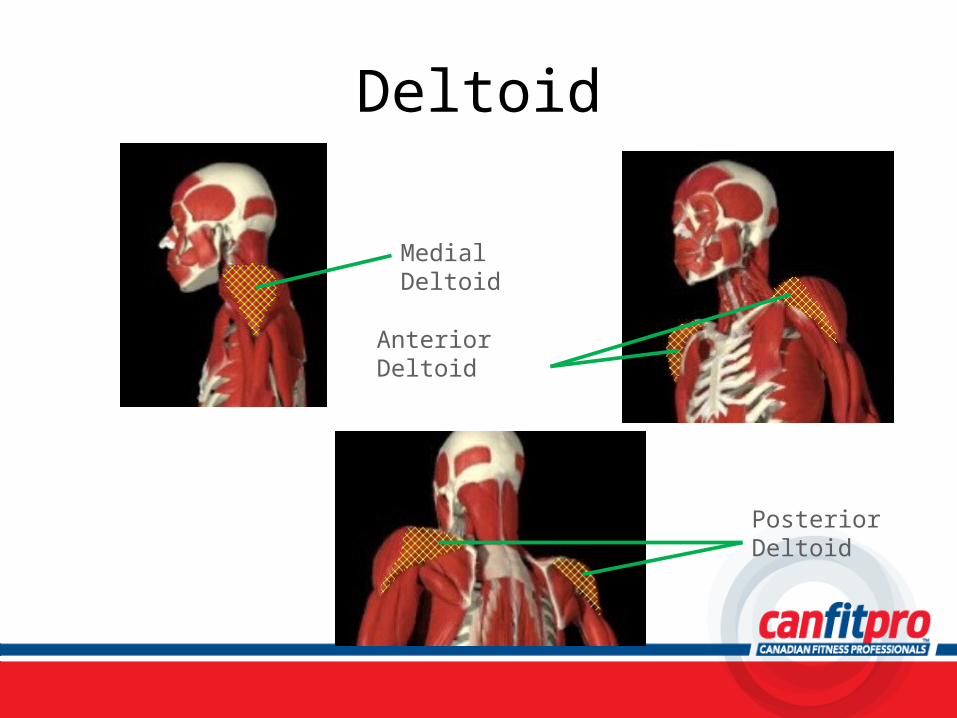
Deltoid
Medial Deltoid
Anterior Deltoid
Posterior Deltoid
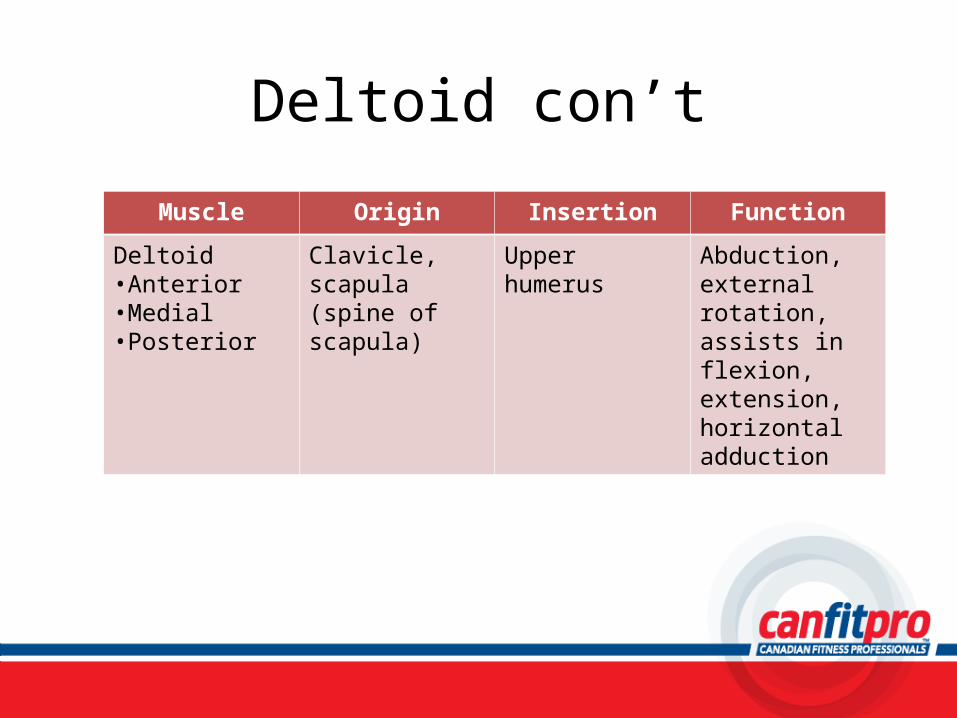
Deltoid con’t
Muscle Origin Insertion Function
Deltoid•Anterior•Medial•Posterior
Clavicle, scapula (spine of scapula)
Upper humerus Abduction, external rotation, assists in flexion, extension, horizontal adduction
Exercise: Deltoid
• Dumbbell Shoulder Press (seated)– Page 211
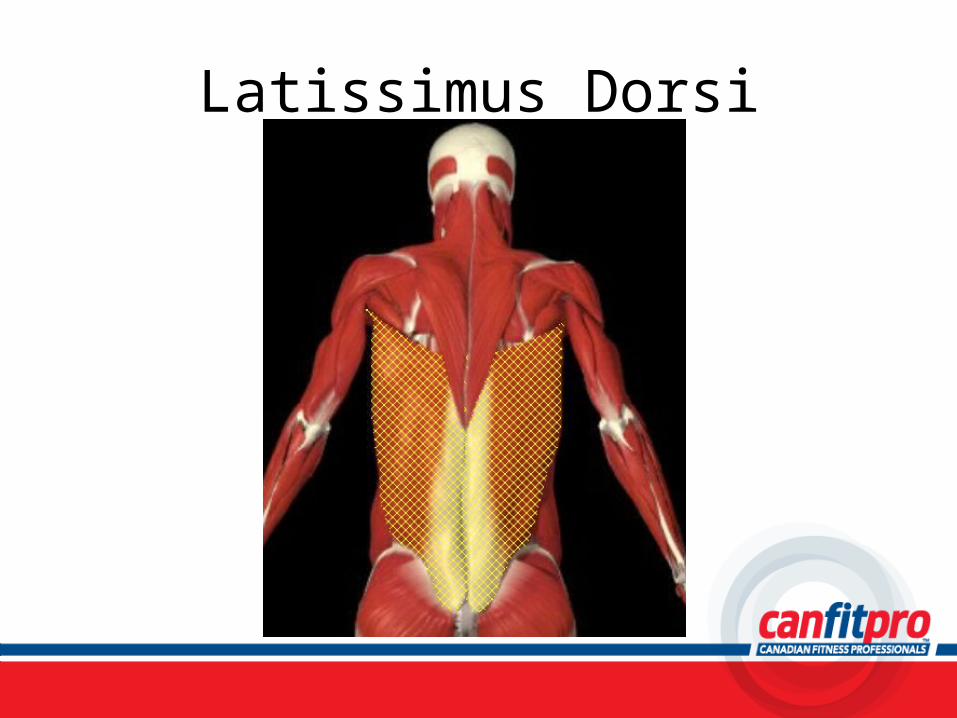
Latissimus Dorsi
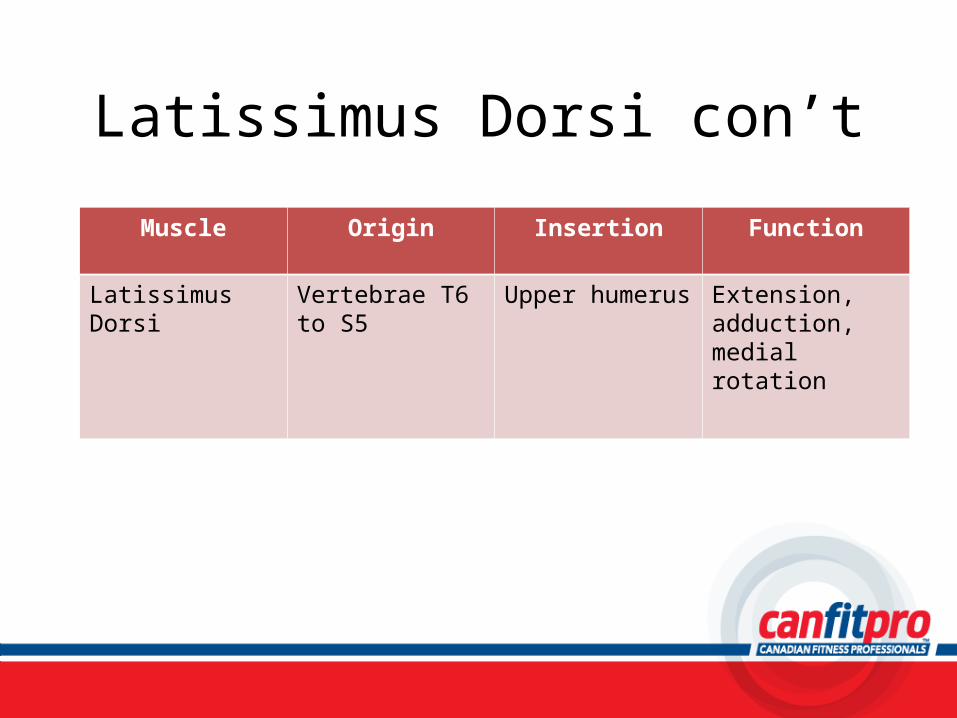
Latissimus Dorsi con’t
Muscle Origin Insertion Function
Latissimus Dorsi Vertebrae T6 to S5 Upper humerus Extension, adduction, medial rotation
Exercise: Latissimus Dorsi
• Cable Lat Pulldown (wide grip)– Page 203
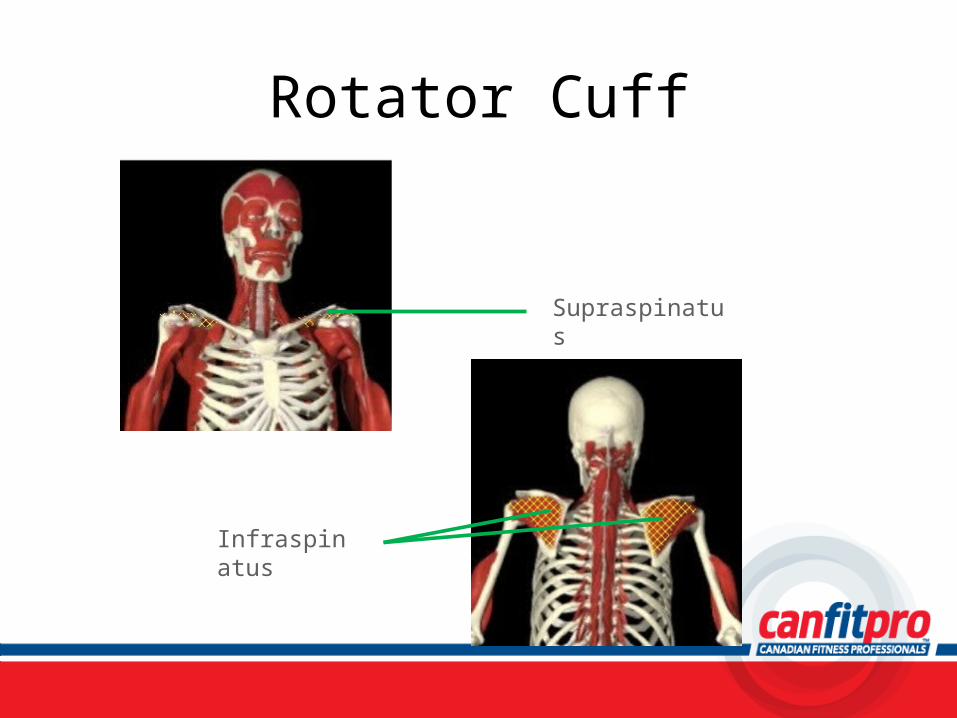
Rotator Cuff
Supraspinatus
Infraspinatus
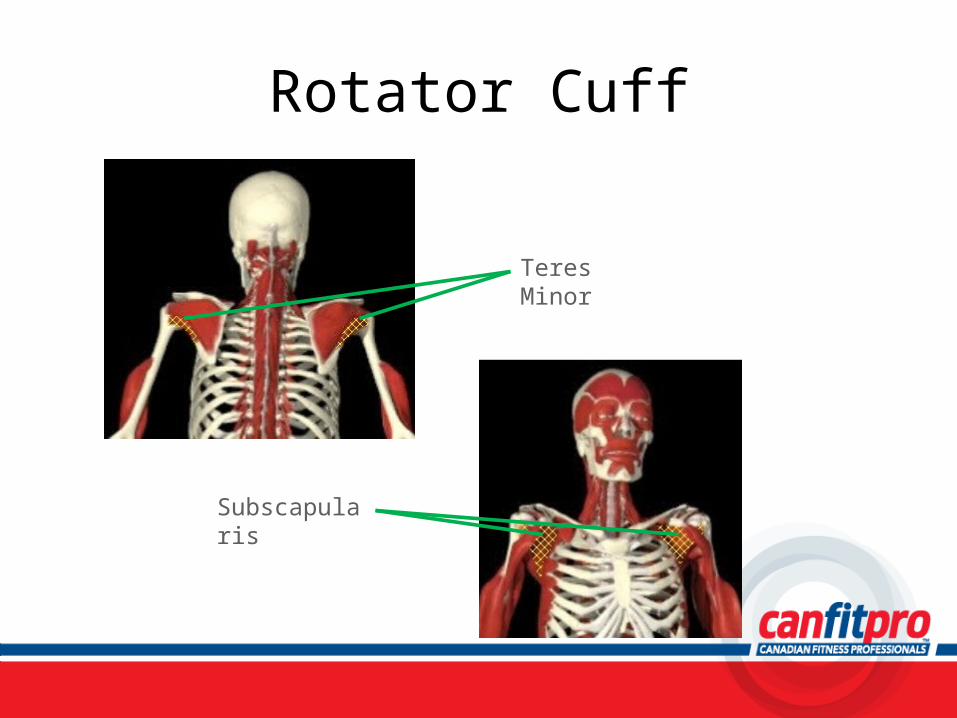
Rotator Cuff
Teres Minor
Subscapularis
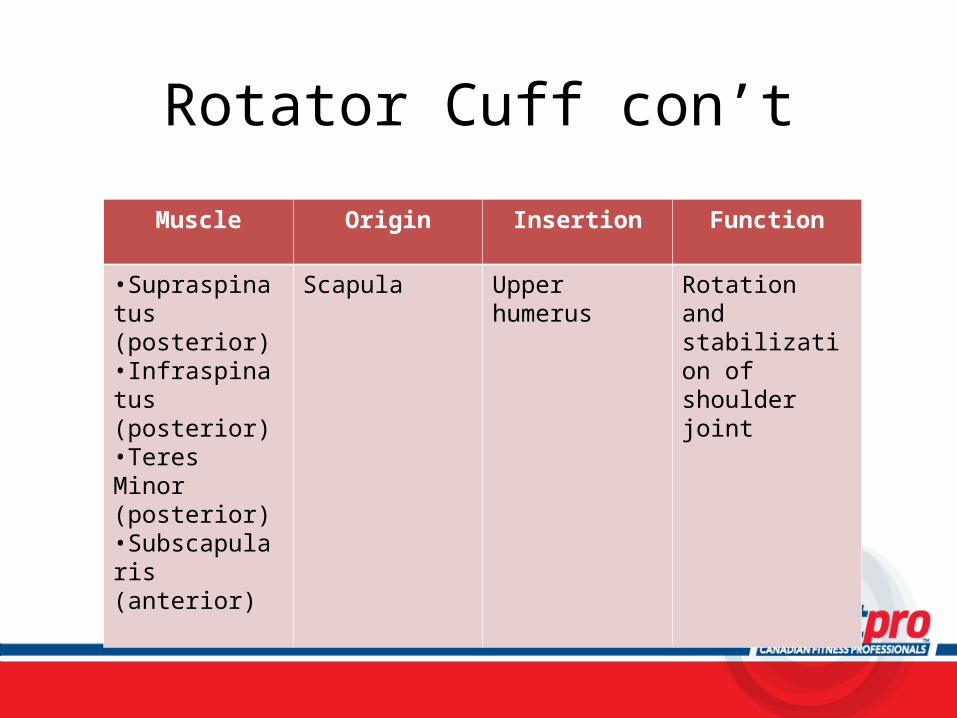
Rotator Cuff con’t
Muscle Origin Insertion Function
•Supraspinatus (posterior)•Infraspinatus (posterior)•Teres Minor (posterior)•Subscapularis (anterior)
Scapula Upper humerus Rotation and stabilization of shoulder joint
Exercise: Rotator Cuff
• Tubing Rotator Cuff External Rotation (standing)– Page 215
• Tubing Rotator Cuff Internal Rotation (standing)– Page 217
Elbow: Biceps Brachii
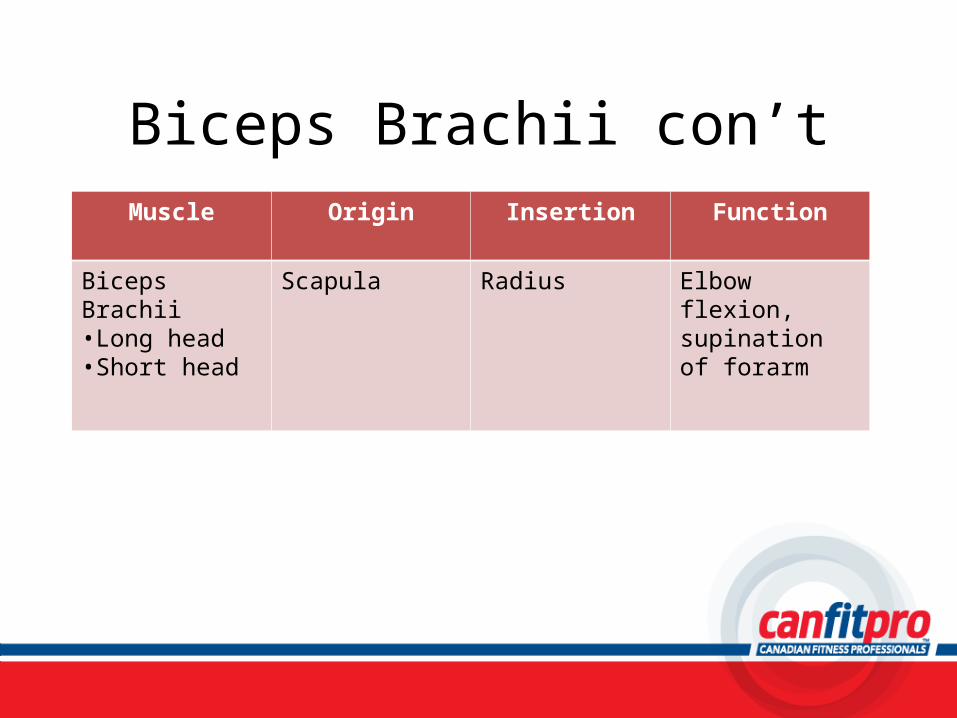
Biceps Brachii con’tMuscle Origin Insertion Function
Biceps Brachii•Long head•Short head
Scapula Radius Elbow flexion, supination of forarm
Exercise: Biceps Brachii
• Dumbbell Biceps Curl (seated, with supination)– Page 221
Brachioradialis

Brachioradialis con’t
Muscle Origin Insertion Function
Brachioradialis Humerus Radius Flexion
Exercise: Brachioradialis• Dumbbell Biceps Curl (seated, hammer grip)
– Page 223
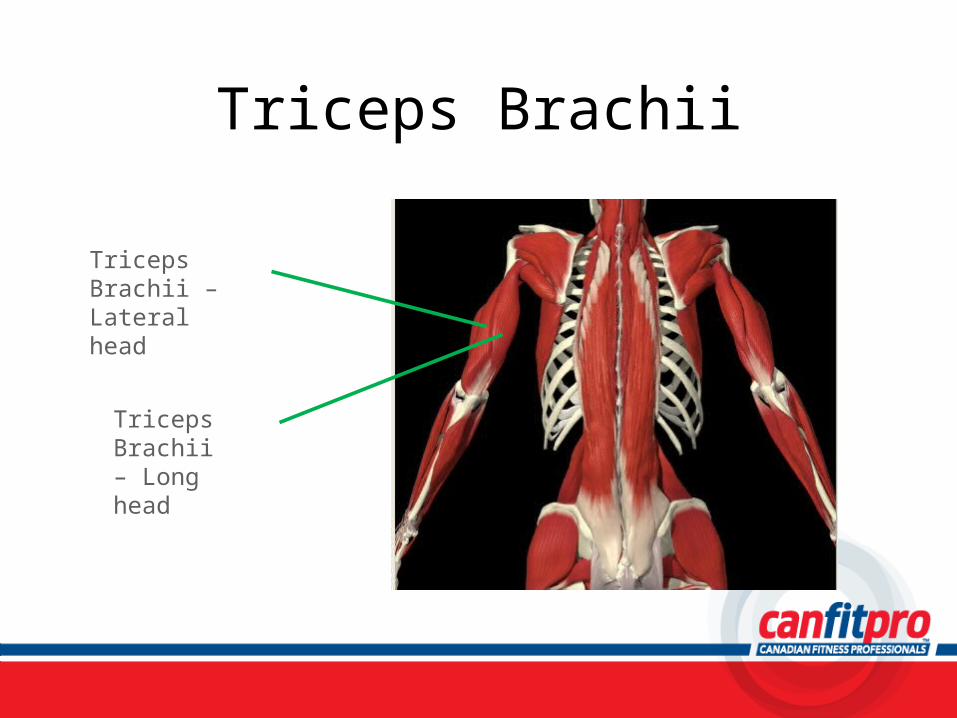
Triceps Brachii
Triceps Brachii – Lateral head
Triceps Brachii – Long head
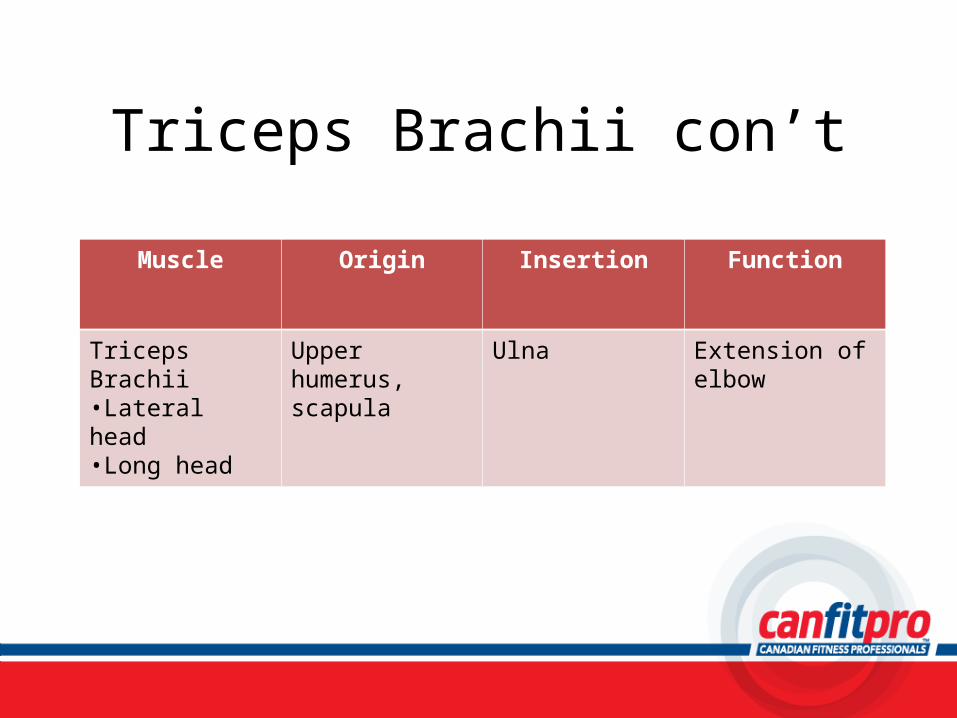
Triceps Brachii con’t
Muscle Origin Insertion Function
Triceps Brachii•Lateral head•Long head
Upper humerus, scapula
Ulna Extension of elbow
Exercise: Triceps Brachii
• Cable Triceps Extension (standing, V-bar)
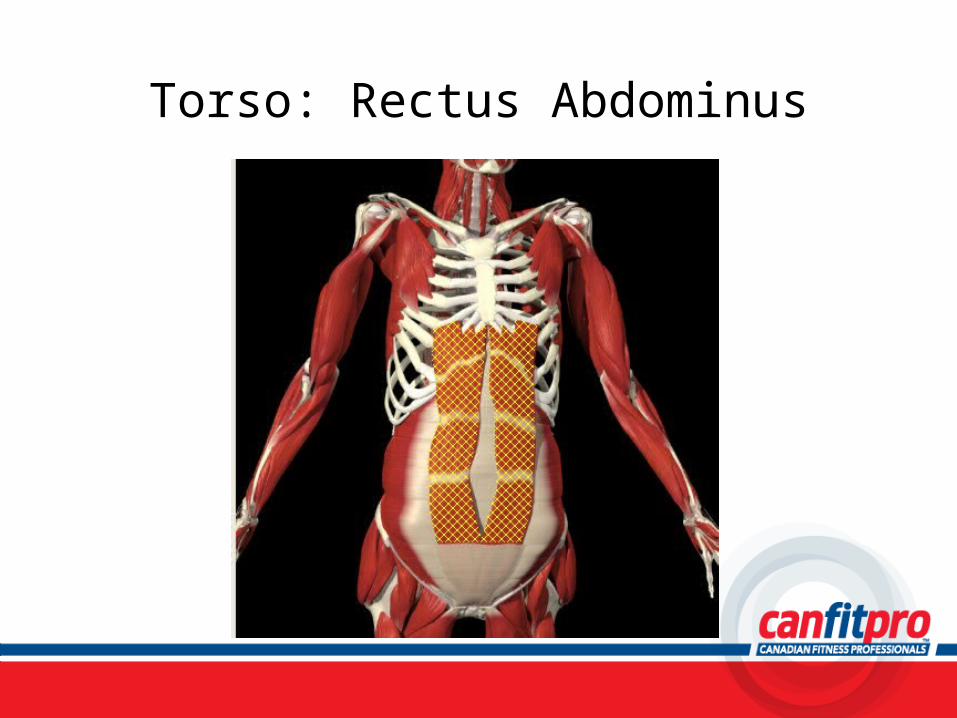
Torso: Rectus Abdominus
Rectus Abdominus con’t
Muscle Origin Insertion Function
Rectus Abdominus Pubis Ribs 5 to 7, sternum
Spinal flexion, posterior pelvic tilt
Exercise: Rectus Abdominus
• Partial Abdominal Curl-up– Page 249
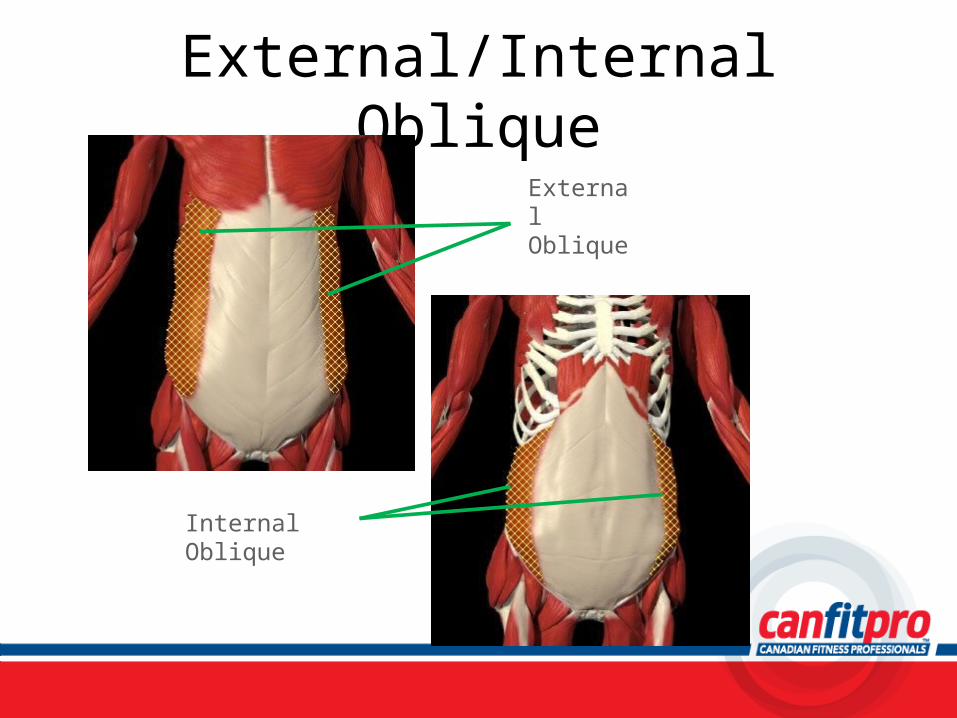
External/Internal ObliqueExternal Oblique
Internal Oblique
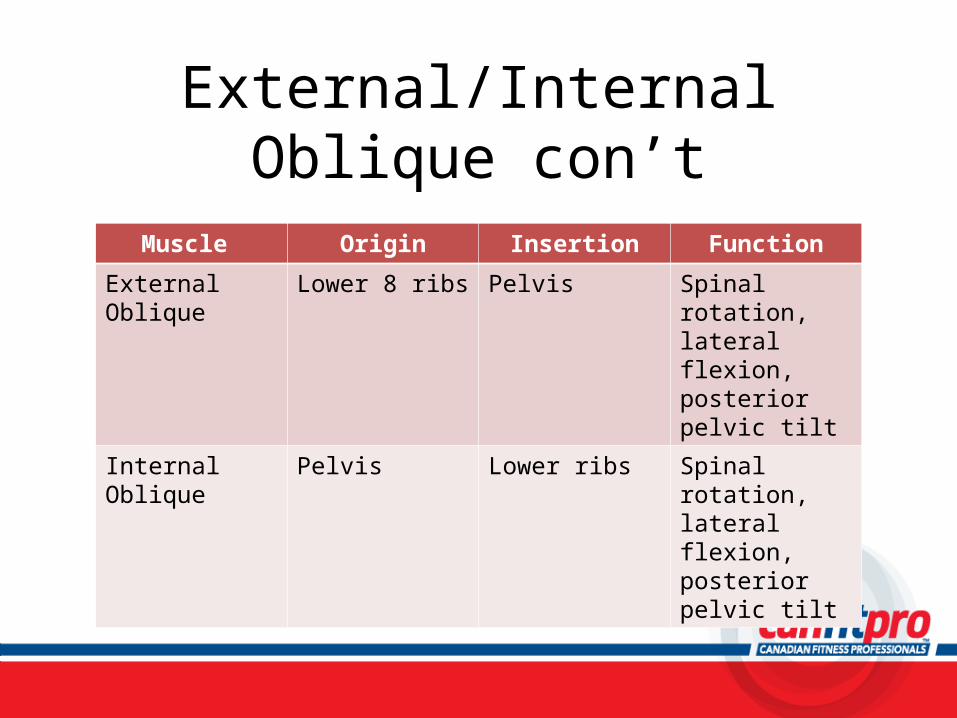
External/Internal Oblique con’t
Muscle Origin Insertion Function
External Oblique Lower 8 ribs Pelvis Spinal rotation, lateral flexion, posterior pelvic tilt
Internal Oblique Pelvis Lower ribs Spinal rotation, lateral flexion, posterior pelvic tilt
Exercise: External/Internal Oblique
• Shoulder To Knee Curl-up– Page 247
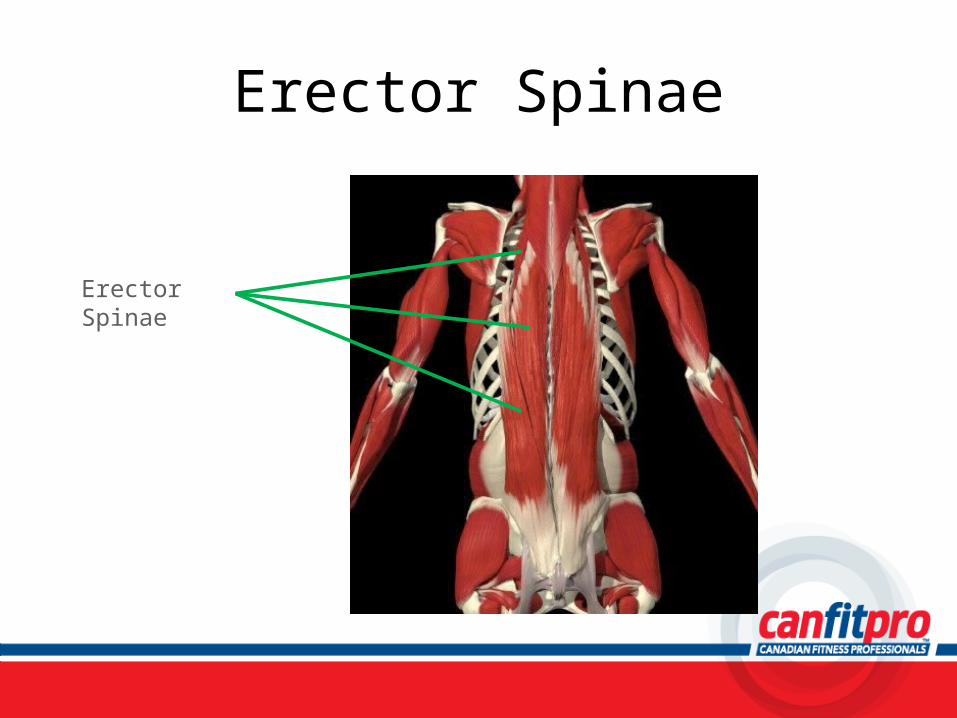
Erector Spinae
Erector Spinae
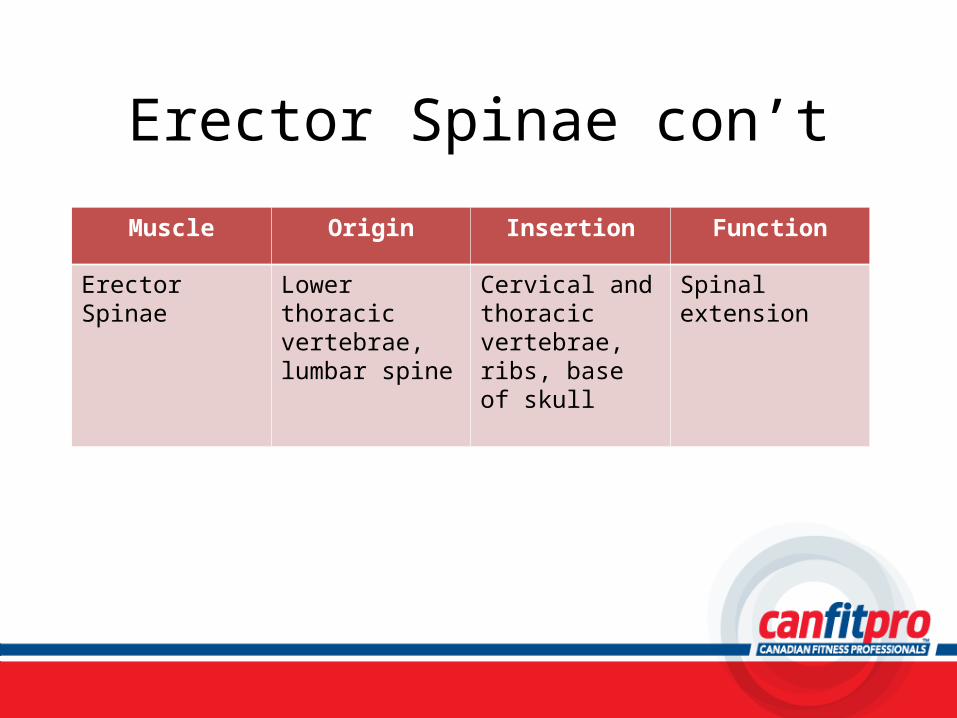
Erector Spinae con’t
Muscle Origin Insertion Function
Erector Spinae Lower thoracic vertebrae, lumbar spine
Cervical and thoracic vertebrae, ribs, base of skull
Spinal extension
Exercise: Erector Spinae
• Back Extension (prone, upper body)– Page 245
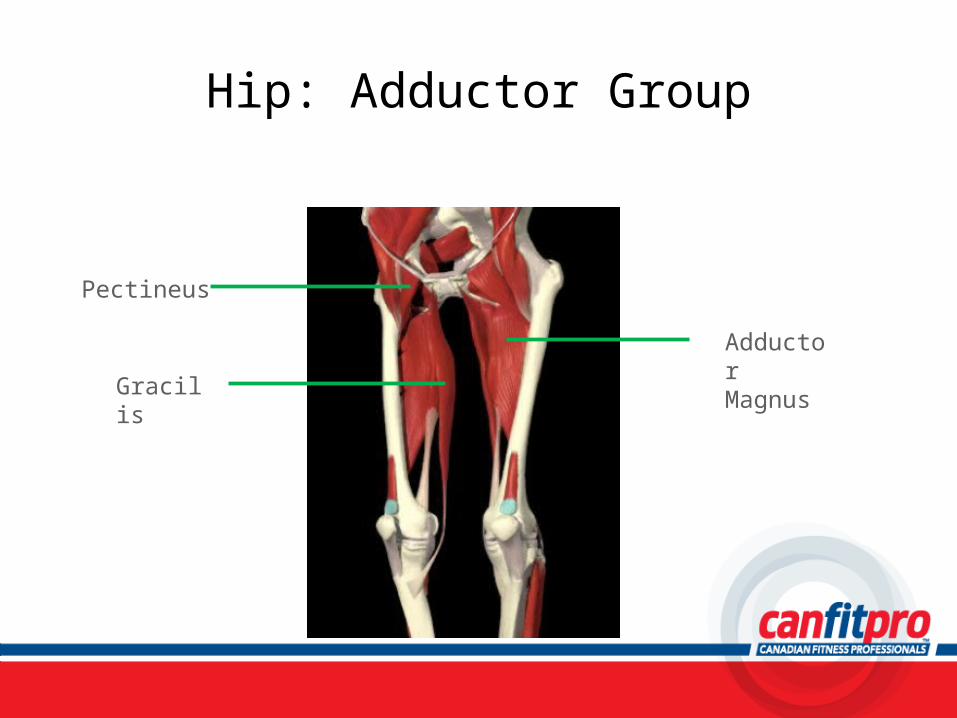
Hip: Adductor Group
Pectineus
Adductor Magnus
Gracilis
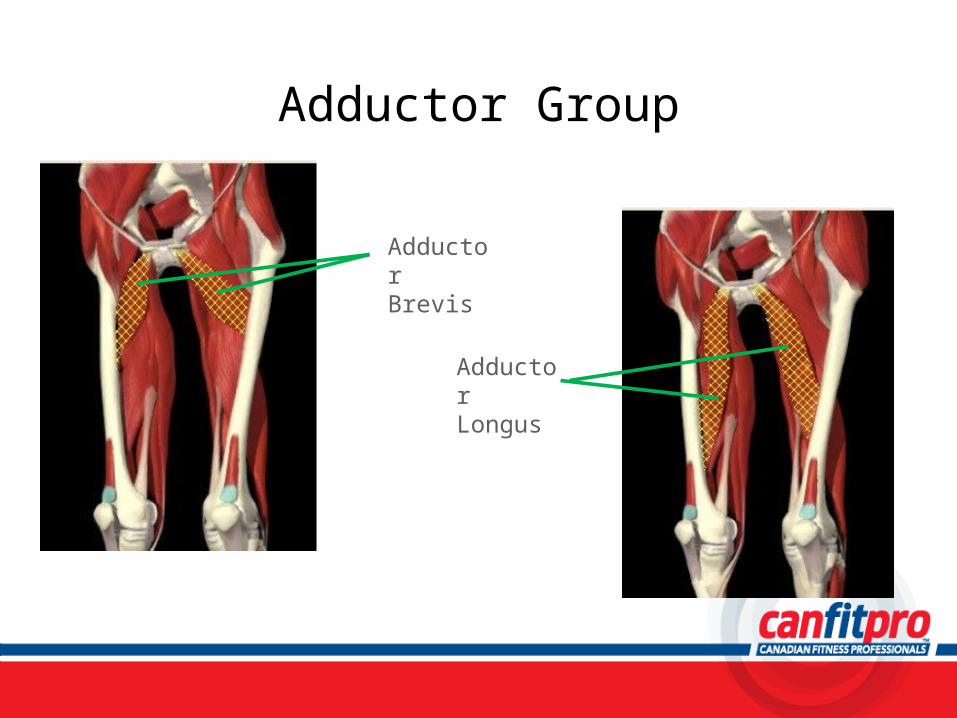
Adductor Group
Adductor Brevis
Adductor Longus
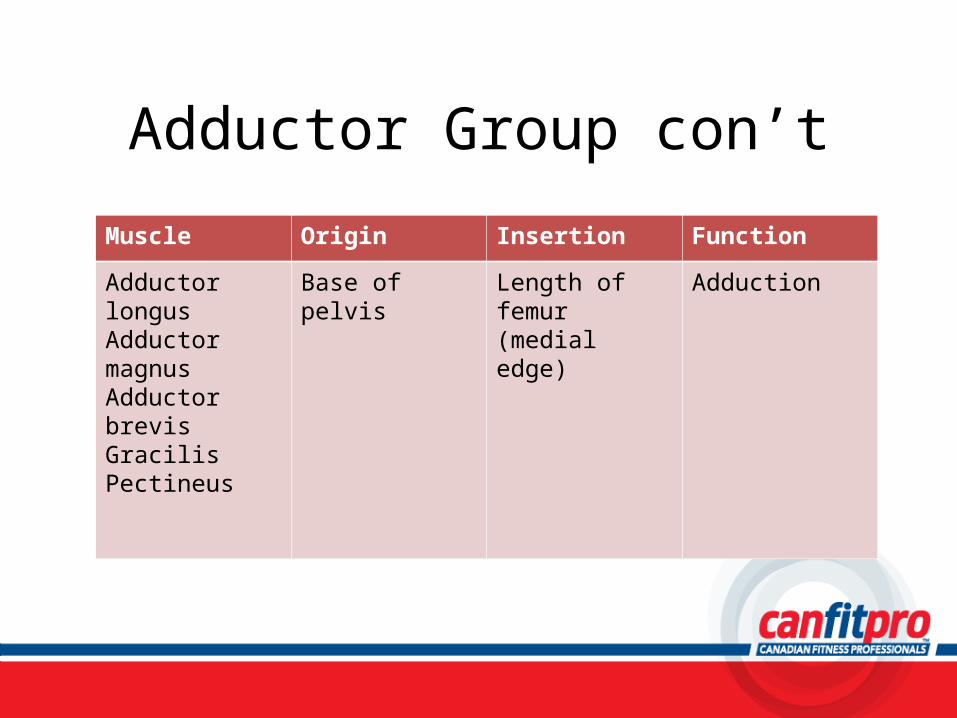
Adductor Group con’t
Muscle Origin Insertion Function
Adductor longus Adductor magnus Adductor brevis GracilisPectineus
Base of pelvis Length of femur (medial edge)
Adduction
Exercise: Adductor Group
• Cable Hip Adduction (standing)– Page 239
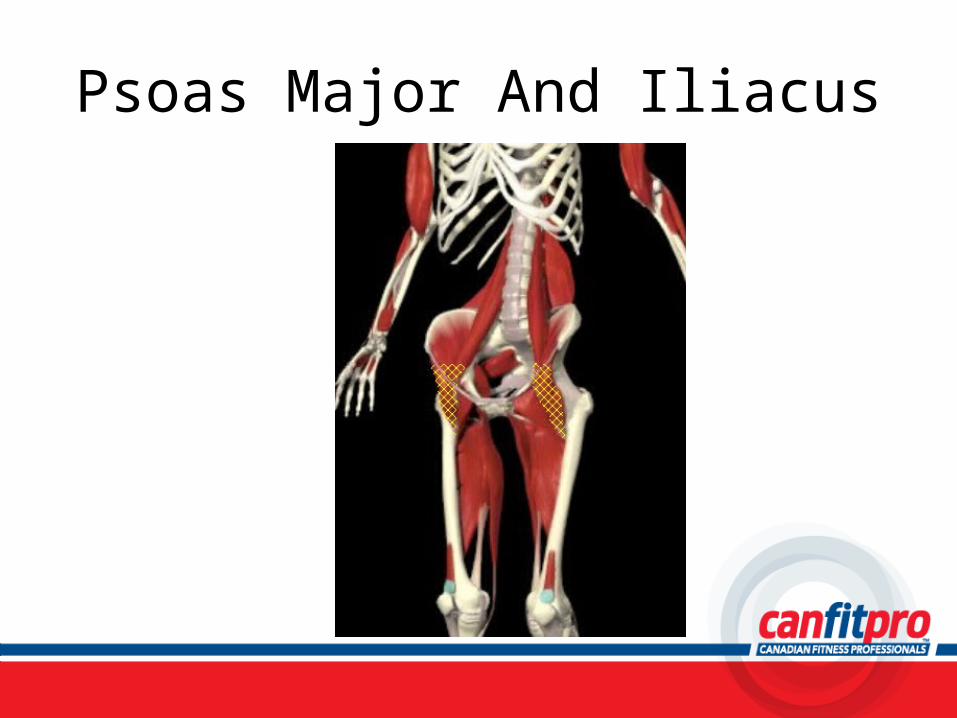
Psoas Major And Iliacus
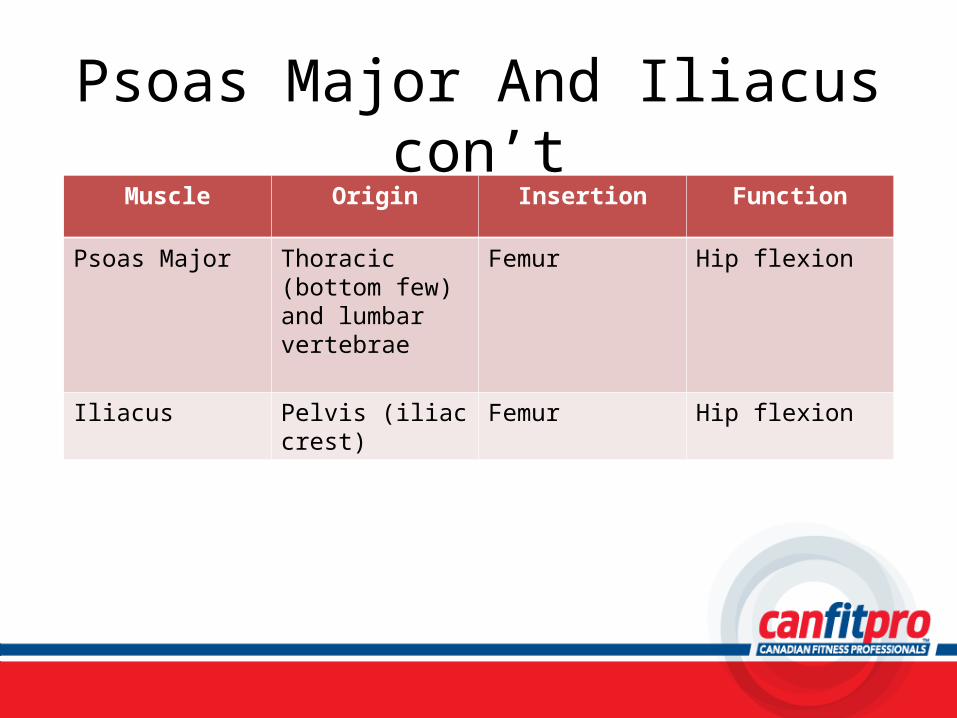
Psoas Major And Iliacus con’tMuscle Origin Insertion Function
Psoas Major Thoracic (bottom few) and lumbar vertebrae
Femur Hip flexion
Iliacus Pelvis (iliac crest) Femur Hip flexion
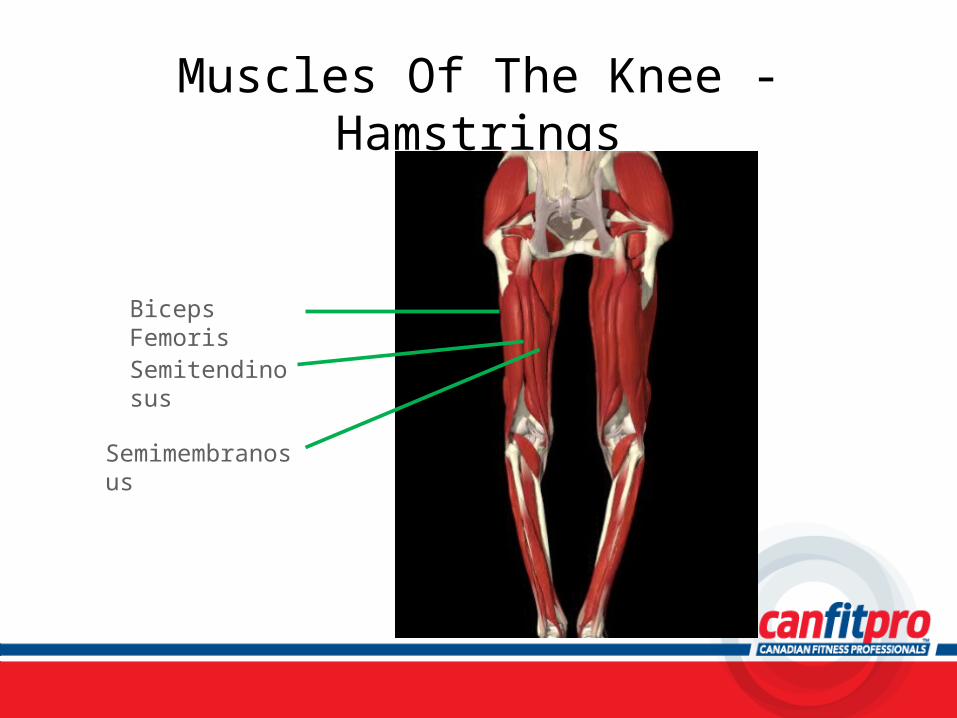
Muscles Of The Knee - Hamstrings
Biceps Femoris
Semitendinosus
Semimembranosus
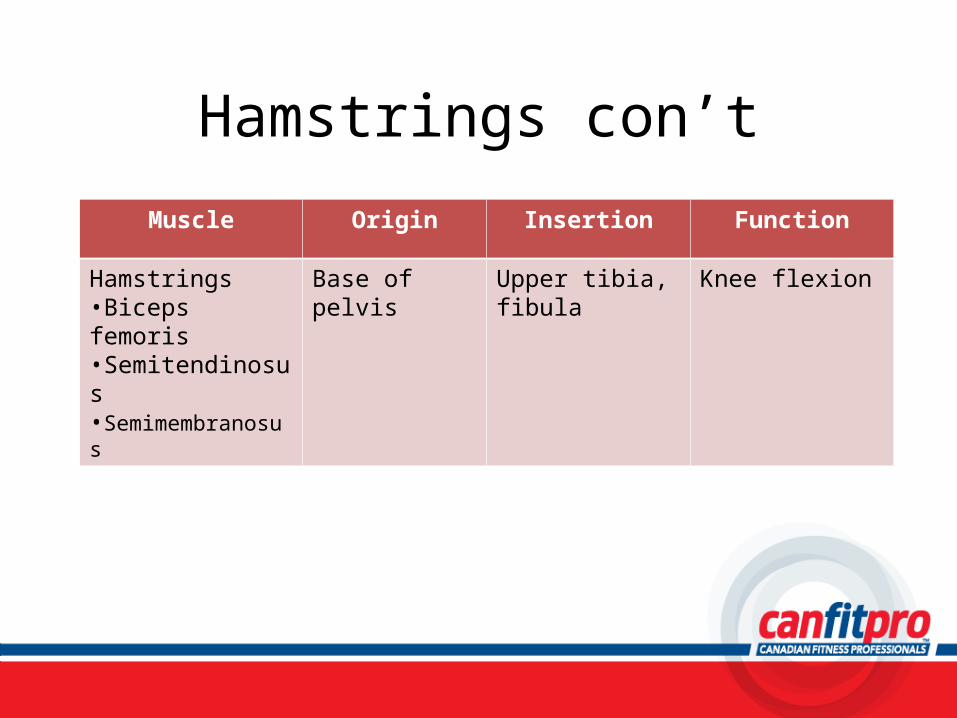
Hamstrings con’t
Muscle Origin Insertion Function
Hamstrings•Biceps femoris•Semitendinosus•Semimembranosus
Base of pelvis Upper tibia, fibula Knee flexion
Exercise: Hamstrings
• Machine Leg Curl (prone)– Page 237
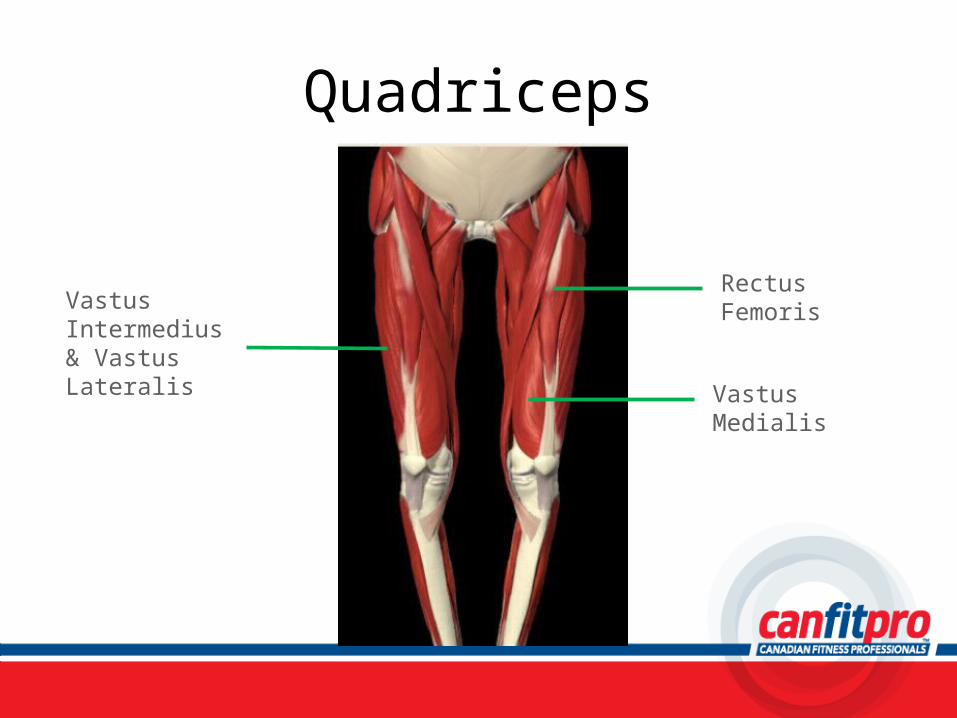
Quadriceps
Vastus Intermedius & Vastus Lateralis
Rectus Femoris
Vastus Medialis
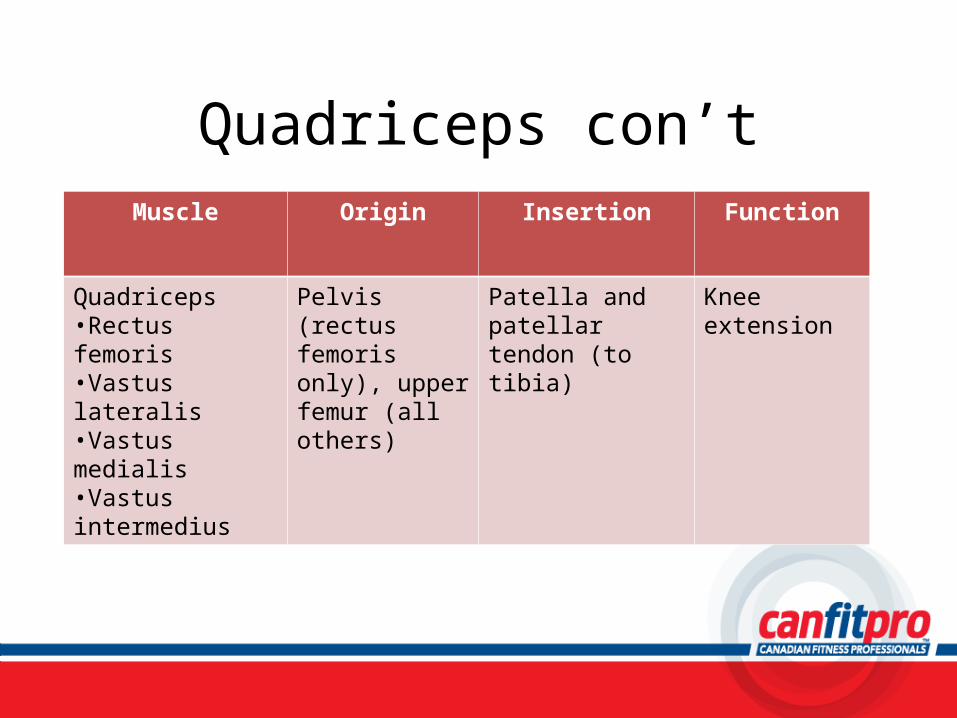
Quadriceps con’tMuscle Origin Insertion Function
Quadriceps•Rectus femoris•Vastus lateralis•Vastus medialis•Vastus intermedius
Pelvis (rectus femoris only), upper femur (all others)
Patella and patellar tendon (to tibia)
Knee extension
Exercise: Quadriceps
• Machine Leg Extension– Page 235
Exercise: Hamstrings, Quads, Adductors
• Barbell Squat– Page 233
• Dumbbell Lunge– Page 234
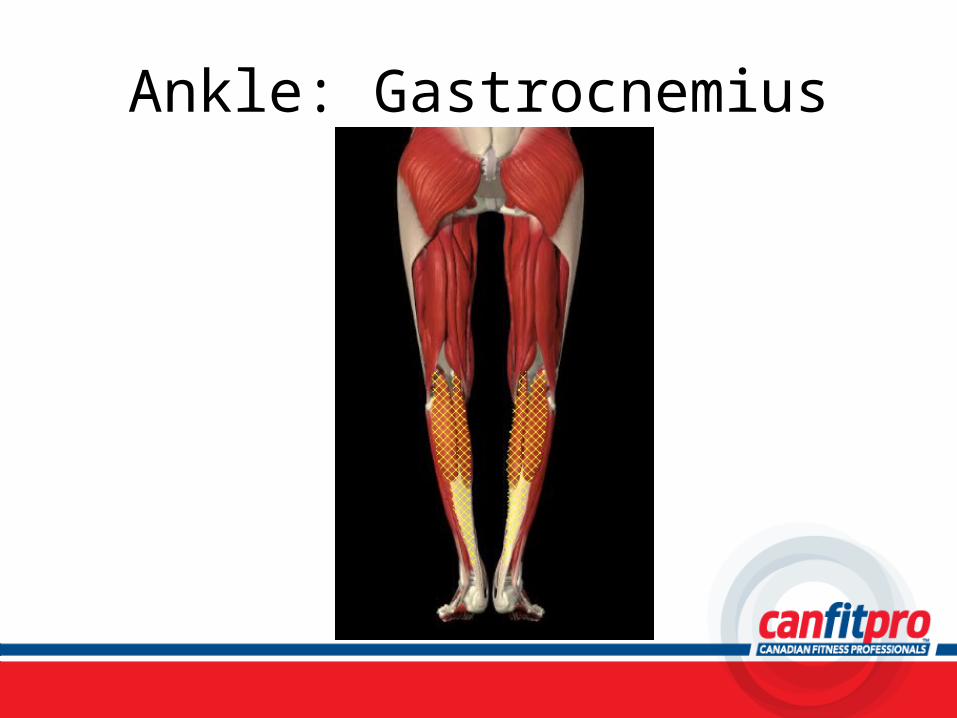
Ankle: Gastrocnemius
Gastrocnemius con’t
Muscle Origin Insertion Function
Gastrocnemius Base of femur Heel (Achilles tendon)
Knee flexion, plantar flexion
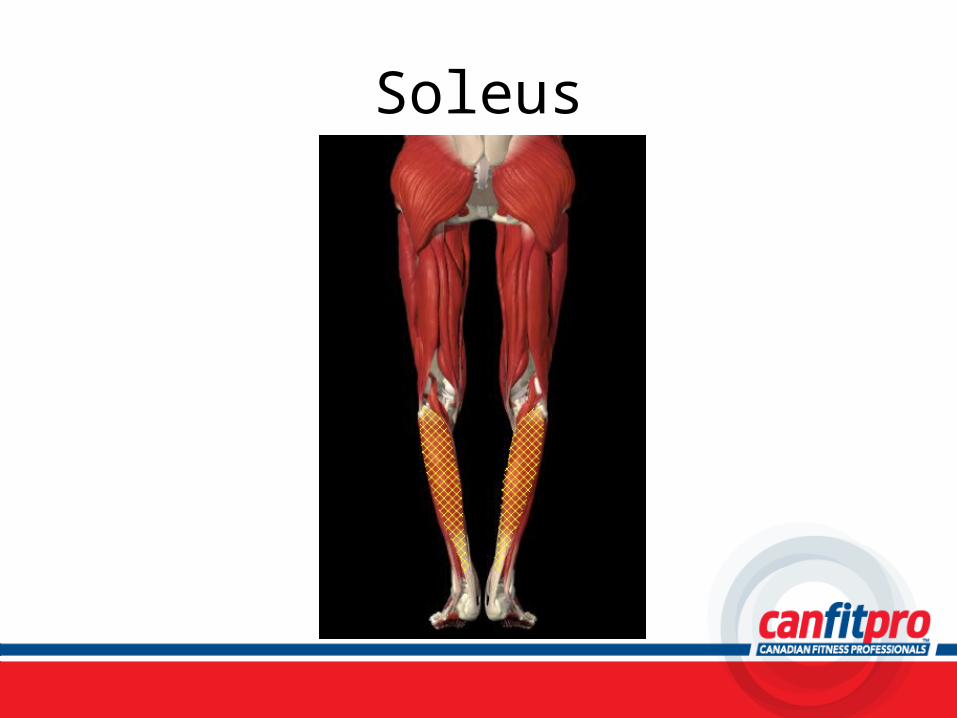
Soleus
Soleus con’t
Muscle Origin Insertion Function
Soleus Top of tibia and fibula
Heel (Achilles tendon)
Plantar flexion
Exercise: Gastrocnemius and Soleus
• Dumbbell Heel Raise (standing)– Page 243
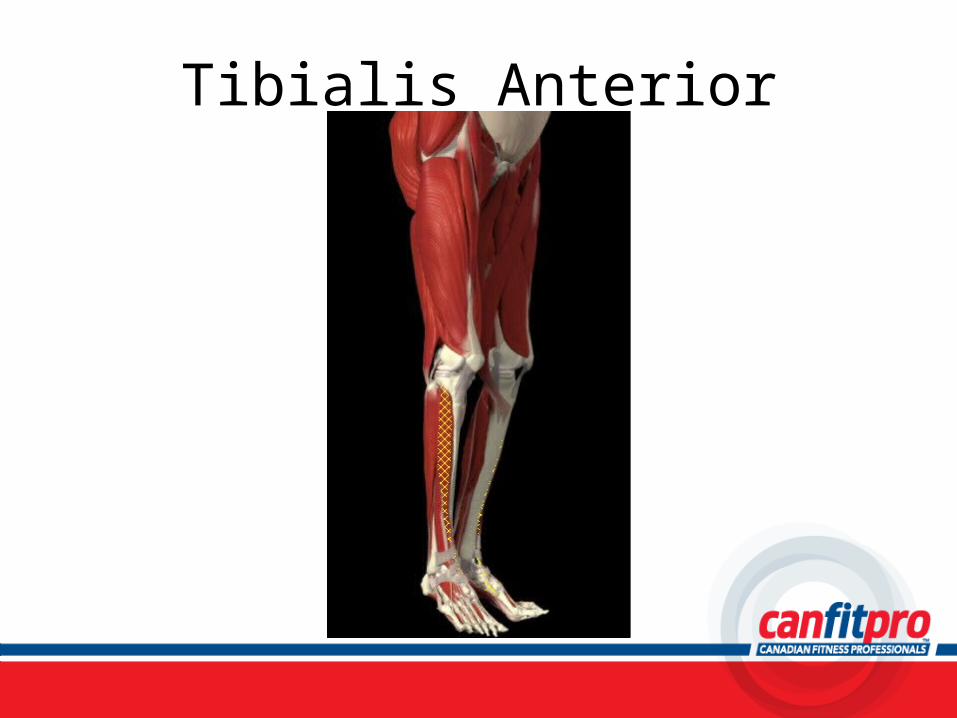
Tibialis Anterior
Tibialis Anterior con’t
Muscle Origin Insertion Function
Tibialis Anterior Top 2/3 of tibia Metatarsal Dorsiflexion, inversion

Benefits of Resistance Training
• What are they?
What to Train for?
• Muscular strength• Muscular power• Muscular endurance
Exercise Prescription• Resistance Training
– FITT– Considerations
• Number of sessions client is able to commit to• Clients current fitness level• Clients goals for resistance training
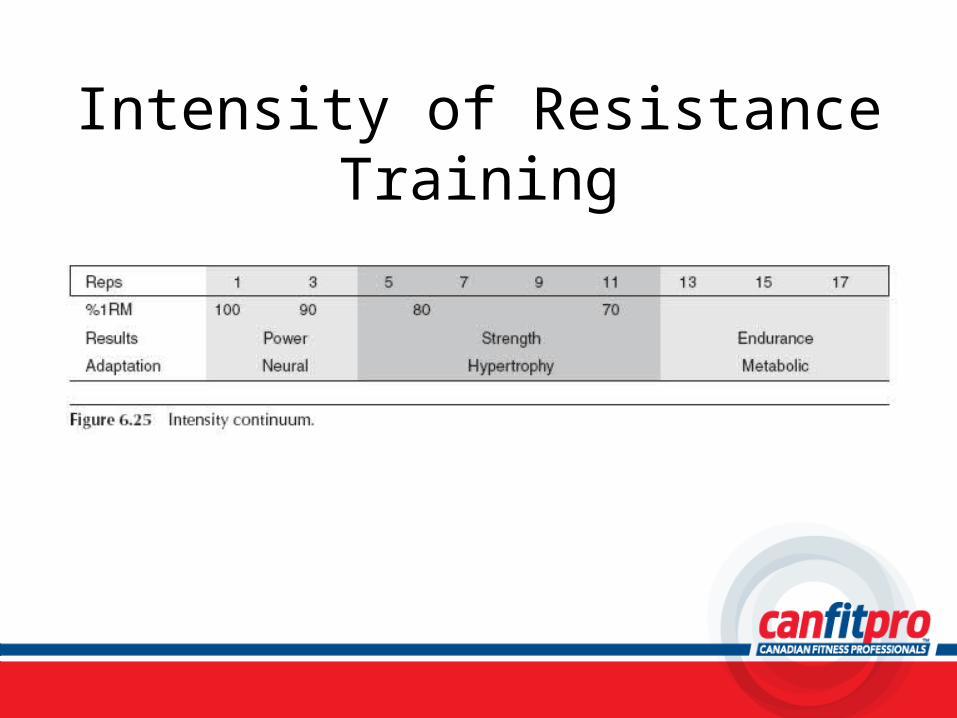
Intensity of Resistance Training
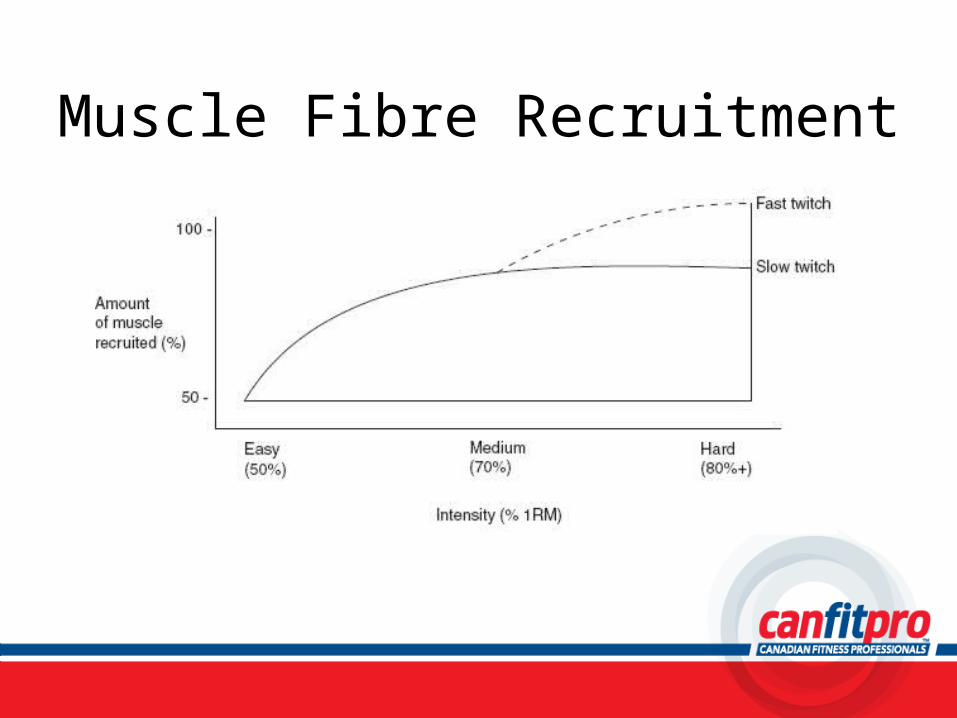
Muscle Fibre Recruitment
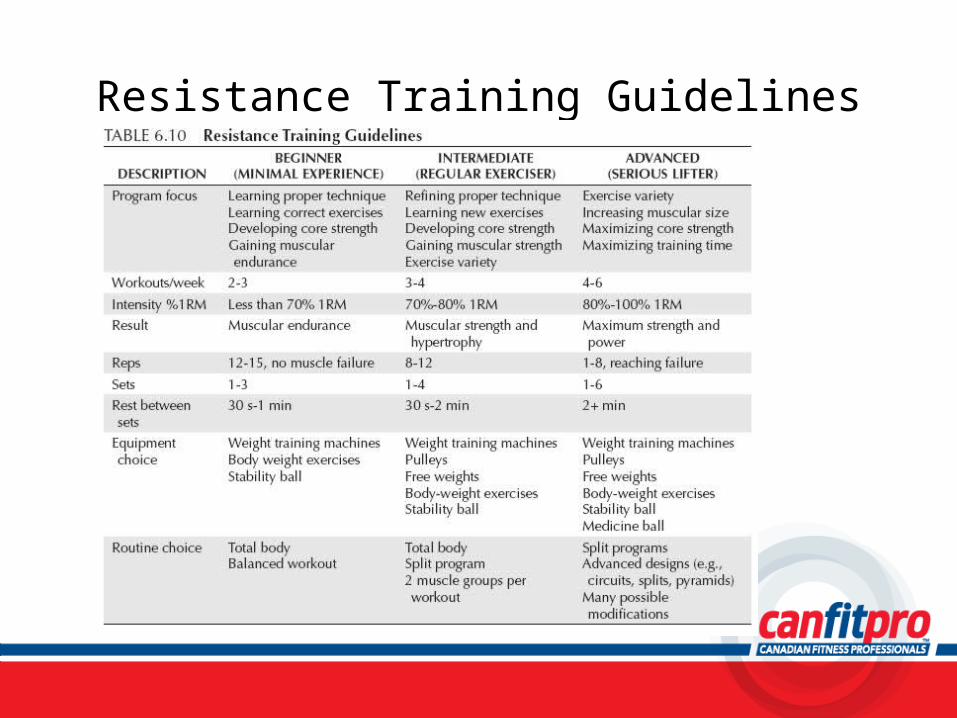
Resistance Training Guidelines

Types of Resistance Training
• Isotonic Training• Isometric Training• Isokinetic Training
Isotonic Training
– Concentric and eccentric muscle contractions– Constant resistance → arm curl with DB– Variable resistance → Nautilus equipment (cams),
Universal equipment (leverage)
Isometric Training– Static muscle contraction– Muscle length does not change when force is
applied against a fixed resistance– Limbs are not required to move– Strength gains limited to the joint angle at which
the exercise takes place
Isokinetic Training
– Needs specialized equipment that controls speed of movement through ROM
– Accommodating resistance → resistance matches strength of muscle and accommodates changes in mechanical advantage
Injury Recognition
Foundations of Professional Personal TrainingChapter 7
Pre-Exercise Screening cont...Pre-Exercise Screening cont...
Why screen?• It allows for facility professionalism and fulfillment
of legal responsibilities (duty of care).• The ability to identify a possible need to refer the
individual to a more qualified exercise professional or additional health professionals.PAR-Q+ is available on the canfitpro website under ‘Downloads and Forms’ or can be completed online at www.eparmedex.com
Scope of Practice and Personal Training
Personal trainers are:• NOT permitted to diagnose injury or illness• NOT permitted to diagnose source pain• NOT permitted to suggest therapies in the absence of direct
communication with an appropriate health care practitioner (ie. physician, physiotherapist)
• To refer to an appropriate health care practitioner
Common Scenarios for Personal Trainers
• What do I do if my client comes to me…– With undiagnosed pain– With diagnosed pain– Asking for my opinion about treatment they are getting
from a health professional– Wanting to start training while being treated for an injury– Suggesting we ignore their health professionals advice on
resuming exercise

Pain
Pain is there for a reason and indicates a lack of normal tissue function or homeostasis in
the body.
Two Types of PainMechanical Pain
• Result of damage to musculoskeletal system by mechanical action or motion – Example → falling, tripping
Systemic Pain• Result of a disease,
infection, or medical condition – Example → rheumatoid
arthritis, heart disease
Two Types of Musculoskeletal InjuryAcute Injuries
• Result from single force application creating tissue damage and immediate pain and dysfunction – Example → broken bone,
sprain, contusion
Overuse Injuries• Result from repeated stress
resulting in gradual onset of pain and dysfunction over days or weeks – Example → stress fracture,
ITB, bursa inflammation
Injury Signs and Symptoms
• Symptom is usually described by the client as what they feel
• Sign is the result of what they were feeling– Therefore a client may say: “I feel a tightness in
my hamstring.” (symptom) Then they run and the hamstring tears and swells (sign).
Immediate Management of Acute Injuries
• Goals → minimize tissue damage and the inflammatory response– First 72 hrs very important– Undiagnosed pain should be referred to a health
professional– RICE principle applies
• Rest, Ice, Compression, Elevation
Prevention of Acute Injuries
Intrinsic Factors• Psychological and physical
characteristic status of your client– Examples → muscle
weakness, muscle imbalances, joint laxity, cognitive function
Extrinsic Factors• External factors your client
must deal with– Examples → environmental
factors such as temperature, humidity, fitness apparel, exercise equipement
Steps to Preventing Acute Injuries
• Intake interview• Par Q & Assessment• Start with lighter loads and lower intensity• Perform warm-up and cool down• Educate on proper technique and equipment set-up• Ensure maintenance of equipment and safe training
area
Immediate Management of Overuse Injuries
• Don’t downplay chronic pain• First 72 hrs is very important (RICE)• Decrease or limit volume and intensity• Pain lasting longer than 3 days or undiagnosed
pain should be refer to a health professional
Steps to Preventing Overuse Injuries
• Identify intrinsic and extrinsic risk factors• Ensure proper biomechanics are followed• Par Q & Assessment• Follow the FITT principle at safe levels• Develop a balanced training approach• Education about rest and cross training benefits
Pre-exercise Screening
Foundations of Professional Personal TrainingChapter 8
Pre-exercise Screening
– Be professional and fulfill legal responsibilities– Identify a possible need to refer client to other health
professionals– Understand client better and establish good
communication– Identify areas of strength or weakness based on previous
injury– Develop a precise, individualized exercise program– Determine safe and effective exercises
To identify clients who have medical conditions that leave them at risk for injury or death when performing moderate to vigorous physical activity the following should be done
Pre-exercise Screening• Key Terms
– Duty of Care– Known Disease– Signs and Symptoms– Cardiac Risk– Health Risk Stratification
Duty Of Care
• Obligation of personal trainer and fitness facility to ensure client is reasonably safe
• Any breach of Duty of Care may result in negligence• Negligence may leave trainer and/or facility liable for
damages• Therefore, every personal trainer and fitness facility must
screen clients first.
Signs And Symptoms• May be well established prior to diagnosis by a medical practitioner• Act as early warning signals• Examples that should prompt medical referral include:
– Pain and discomfort in chest, lower jaw, or left shoulder– Ankle swelling– Feelings of rapid, throbbing HR– Severe pain in leg muscles when walking– Unusual fatigue and general feelings of lethargy– Difficulty breathing when standing or at night– Shortness of breath at rest or during light activity– Feelings of dizziness or fainting
Client Risk Stratification
• Use the answers on the PAR-Q+ and health history questionnaire
• Determine the risk that clients will put themselves in when starting a new exercise program
• Determine what precautions should be taken– Place client in 1 of 3 categories:
• Apparently healthy• Increased risk• Known disease
Pre-Exercise ScreeningPre-Exercise Screening
• As Fitness Professionals we have ‘duty of care’ to our participants ; i.e. We are legally responsible to ensure the safety of our participants.
• Any breach thereof could result in a potential negligence claim
Pre-Exercise Screening cont’d…Pre-Exercise Screening cont’d…
• All members/participants must fill out a Physical Activities Readiness Questionnaire for Everyone (PAR – Q+) to identify any health risks. This serves to identify risks, and assists in protecting the centre and instructor against potential negligence.
• The PAR-Q+ includes seven questions designed to identify people who will be required to answer follow up questions about their medical conditions.
Pre-Exercise Screening cont...Pre-Exercise Screening cont...
Why screen?• It allows for facility professionalism and fulfillment
of legal responsibilities (duty of care).• The ability to identify a possible need to refer the
individual to a more qualified exercise professional or additional health professionals.PAR-Q+ is available on the canfitpro website under ‘Downloads and Forms’ or can be completed online at www.eparmedex.com
Fitness Assessment
Foundations of Professional Personal TrainingChapter 9
Why do Fitness Assessments?
• Gives Personal Trainer a clear indication of client’s current health status and actual fitness level (using resting HR and BP)
• Fine-tuning exercise prescription• Start with baseline information to help improve
client’s health and wellness, and to measure future progress
• Determining lifestyle factors that may be counterproductive
Why do Fitness Assessments? Con’t
• Goal setting and counseling• Isolating injuries or risk factors• Help develop a unique, individualized and accurate exercise
prescription• Motivating clients, thus increasing adherence and compliance
Testing Procedures• Pretesting must always precede tests and measures:
– Client must be told what to wear– When and where?– Not to exercise or drink caffeine or alcohol for 12
hours prior to the test– Complete PAR-Q+– Explain testing session– Sign informed consent document– Begin tests and measures
Testing Procedures con’t
– Follow logical and consistent order• Prescreening• Body composition• Light warm-Up• Cardiorespiratory fitness testing• Muscular strength and endurance testing• Flexibility testing
Prescreening
• Resting HR (RHR)– Must be < 100 bpm to continue testing– Normal 70 bpm for men; 75 bpm for women– As CV fitness ↑ RHR should ↓
Procedure for Resting HR
Equipment– Wrist watch– HR monitor (optional)
Procedure1. Have client sit quietly.2. Place index and middle finger on
carotid or radial artery.3. Begin counting first beat as zero and
keep counting beats for 30 seconds.4. Multiply number by 2 to determine
bpm.
Prescreening
• Resting BP – Must be less then 140/100 mmHg to continue
testing– Normal BP is 120/80 mmHg– As CV fitness ↑ elevated BP should decrease
Procedure for Resting BP
Equipment– Stethoscope and
sphygmomanometer– Chair and table
Procedure1. Have client sit with left arm
supported on table or by you.2. Place BP cuff on upper left arm
approximately 1” above the antecubital space.
3. Pump the cuff to over 200 mmHg and place the stethoscope over the brachial artery.
4. Slowly release pressure (2 mmHg/sec) and listen for the first tapping sounds – systolic pressure.
5. Continue to let air out until you no longer hear noise – diastolic pressure.
Evaluating Body Composition• Skin folds and girths• Bioelectrical Impedance Analysis (BIA)• Waist girth measurements• Body Mass Index (BMI)
Procedure for Waist Girth Measurements
Equipment– Flexible tape measure
Procedure1. Have client stand with feet shoulder
width apart and even weight on each foot.
2. Place tape measure around circumference of the waist, at the level of greatest narrowing. Do not indent skin by pulling to tight.
3. If noticeable narrowing is not apparent, take waist girth at midpoint between lowest floating rib and top of hip bone.
4. Normative data is measured in cm.
Procedure for BMI
Equipment– Pen and paper– Calculator
Procedure1. Obtain client’s body weight in
kilograms.2. Obtain client’s height in metres.3. Use the equation (BMI = kg/m2)4. BMI < 19 or > 25 puts client at risk5. BMI > 30 often indicates obesity
(exception : those with a large amount of muscle mass will fall above 30, so be careful in your interpretations)
Evaluating Cardiorespiratory Fitness
• Submaximal graded tests– Use steps, treadmill, stationary bike etc.
• Rockport Walking Fitness Test– Measurement of VO2max
Procedure for Rockport Walking Fitness Test
Equipment– Wrist watch– Stop watch– HR monitor (optional)– 400 m track (inside lane) or pre-
measured 1 mile loop
Procedure1. Have client warm-up and actively
stretch 5-10 minutes before the test.
2. Instruct client to walk 1 mile (4 laps on 400m track) as quickly as possible.
3. Record time in minutes it took client to finish.
4. Record client’s radial pulse immediately at end of test for a 15 second count and convert to bpm.
5. Use the equation on the following slide.
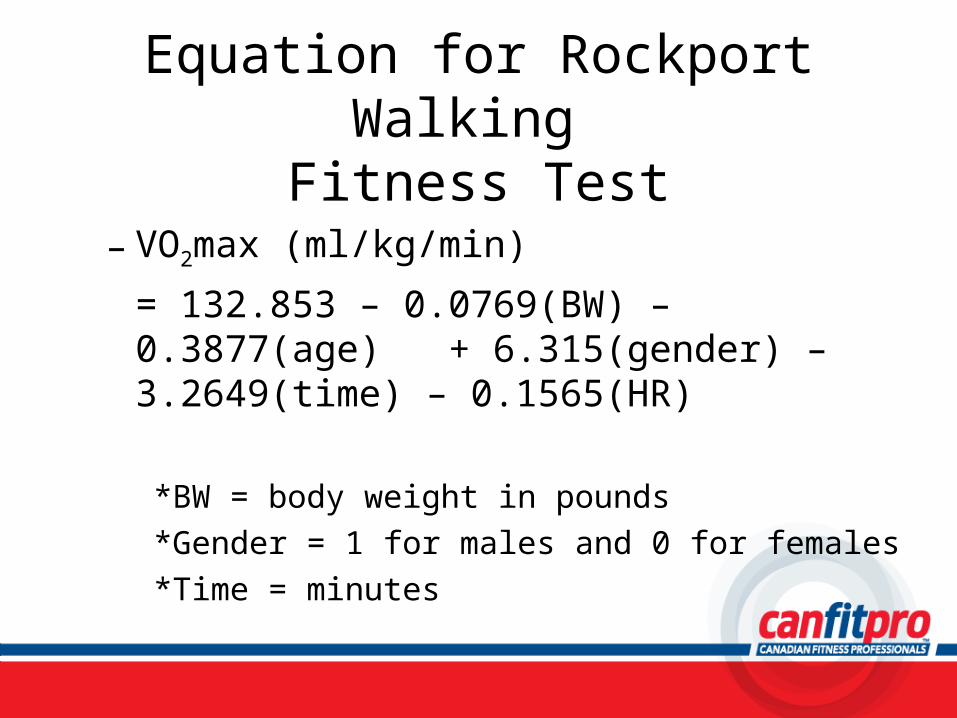
Equation for Rockport Walking Fitness Test
– VO2max (ml/kg/min)
= 132.853 – 0.0769(BW) – 0.3877(age) + 6.315(gender) – 3.2649(time) – 0.1565(HR)
*BW = body weight in pounds*Gender = 1 for males and 0 for females*Time = minutes
Evaluating Muscular Strength
• Normative strength tests– Grip strength– 10 repetition maximum
• Non-normative strength tests– Percent improvement
Procedure for 10 Repetition Maximum
Equipment– May use any exercise that
involves major muscle group– (i.e. bench press, leg press,
squat, lat pull-down)
Procedure1. Have client warm up for 5-10 min.2. Instruct client to perform 5-10
repetitions at 50% of perceived 10RM.
3. After 1 min. rest and light stretching, the client performs 5 repetitions at 75% of perceived 10 RM.
4. Increase the weight to the client’s perceived 10 RM.
5. To calculate 1RM, divide the weight the client did for 10RM by 0.75.
Evaluating Muscular Endurance
• Push-up • Abdominal Curl-up
Procedure for Push-upEquipment
– Exercise mat or towelProcedure
1. Instruct client to perform a couple of push-ups to observe proper form.
2. Hands are pointing forward and under shoulders.
3. Have client push up from mat and fully straighten elbows using toes as pivot and upper body in straight line
4. Return to start position and let chin touch mat. Stomach and legs should not touch mat.
5. If a full push-up can not be performed have client pivot from knees with tops of feet on floor.
6. Perform as many reps as possible until technique breaks over 2 reps or client is straining.
Evaluating Flexibility
• Sit and reach test• Shoulder flexibility test
Procedure for Modified Sit and Reach Test
Equipment– Tape measure or metre stick– Masking tape (to hold
measuring device in place)
Procedure1. Have client warm up for 5-10 min.
and perform 2 modified hurdler stretches for 20 sec. on each leg.
2. Have client remove shoes and place heels at the top of the measuring device with inner soles within 2 cm of the measuring device.
3. Client reaches forward with both hands as far as possible, holding for 2 sec. Hands should be even.
4. Score the most distant point reached with the fingertips.
Sources of Error in Testing
• The validity and reliability can be affected by:– Client factors– Equipment– Personal trainer’s skill– Environment
Program Design
Foundations of Professional Personal TrainingChapter 10
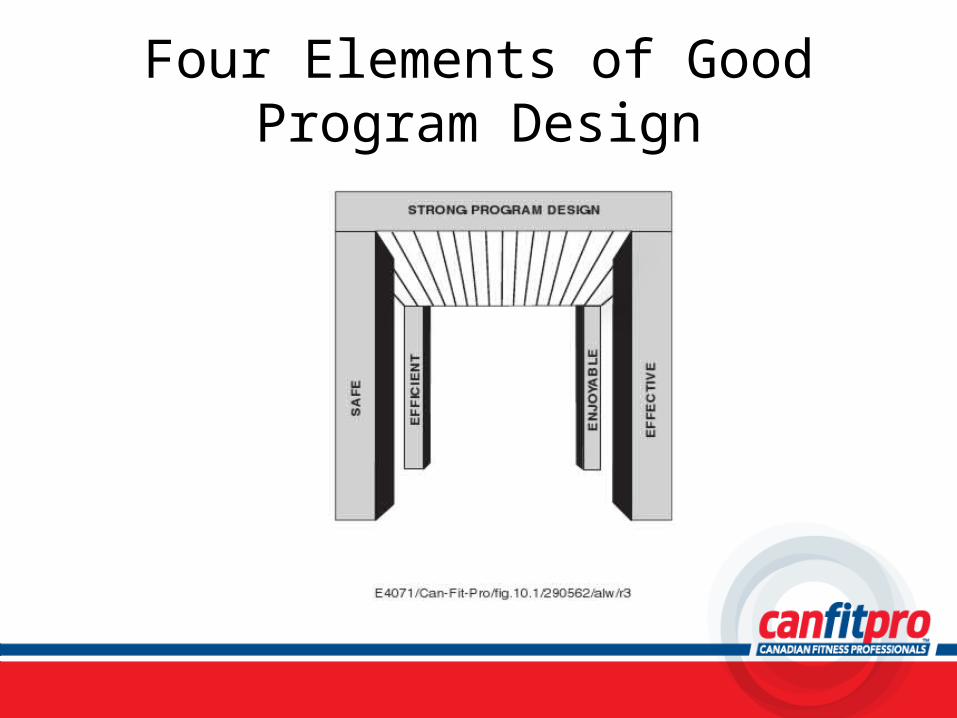
Four Elements of Good Program Design
PeriodizationPeriodization is a planned systematic approach to
training that involves progressive cycling of various aspects of a training program during a
specific period of time.
Periodization as it Applies to Personal Training
• The goal of periodizing an exercise program is to optimize training during both short (i.e. weeks, months) and long periods of time (i.e. years).
• Using periodization, a competitive athlete is able to peak physical performance at a particular point in time. The same concept works if your goal is overall health and fitness.
• The bottom line is…periodization will help maximize results in a minimal amount of time!
Components of Periodization
• Macrocycle– Largest component of
periodization program– Usually consisting of
several months to years (i.e. Olympic athlete’s 4 year program)
Components of Periodization con’t
• Mesocycle– This is the intermediate
component of the periodized program
– Usually consisting of 1 to several months
Components of Periodization con’t
• Microcycle– This is the smallest
component of the periodization program
– Usually consisting of 1 to several weeks, but not normally shorter than 1-2 weeks
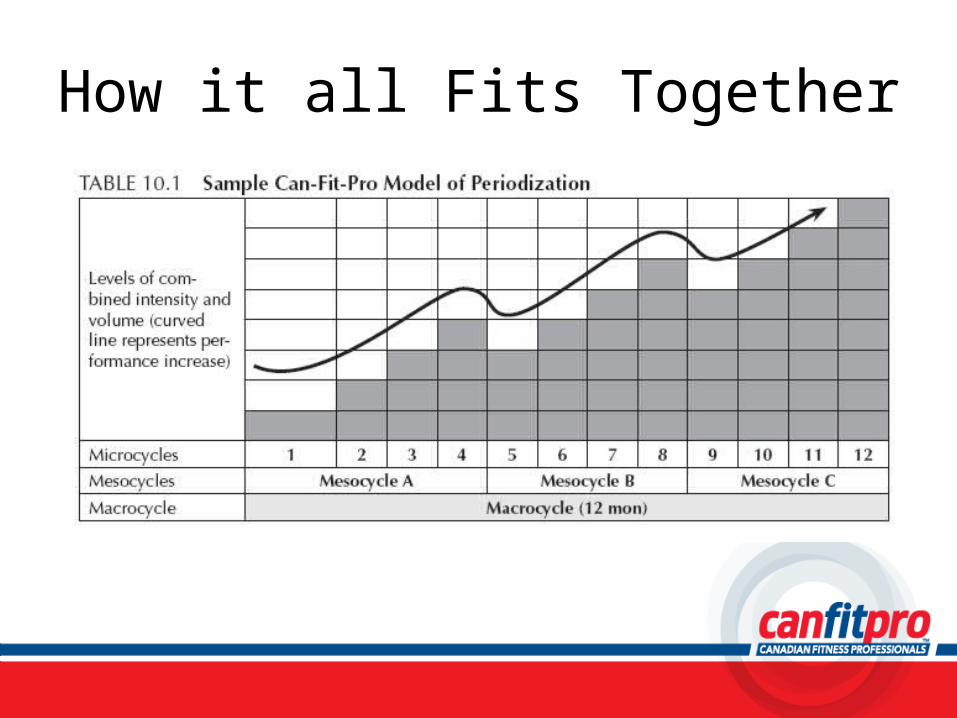
How it all Fits Together
Elite Athlete vs. Fitness Client Differences in Periodization Models
Elite Athlete– Periodization based on
preparing for major competition peak
– While fitness is a focus so are: mental prep, technical skills, specific training, competition and peaking phases, etc.
Fitness Client– Periodization focused mostly
on fitness as developed through:
• Strength training• Cardiorespiratory training• Flexibility training
– Goals are more focused to long-term health and wellness rather than competitive readiness
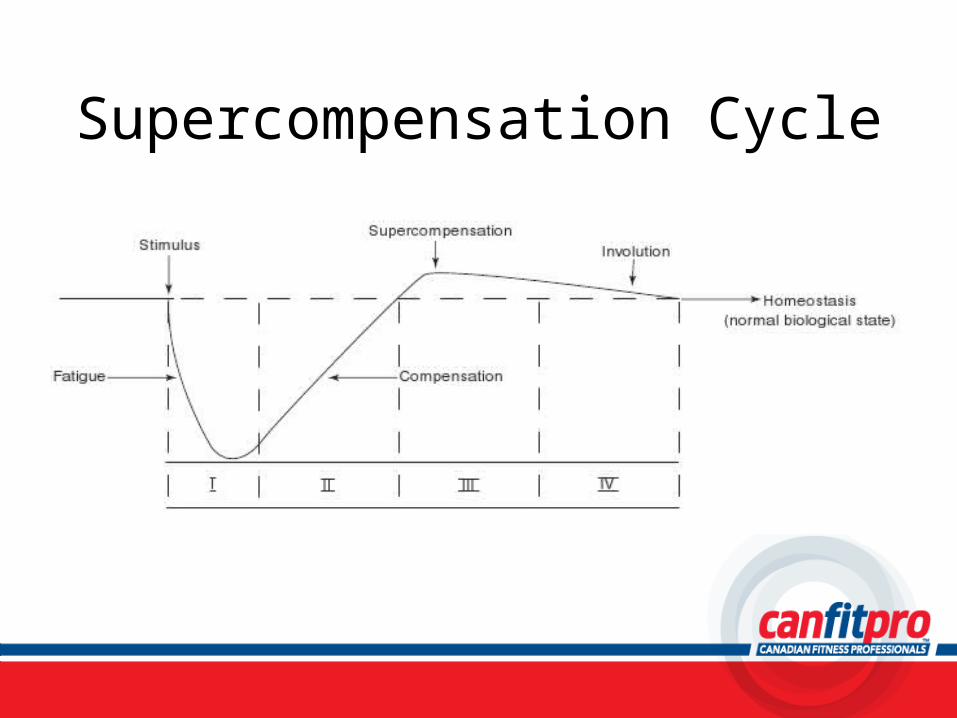
Supercompensation Cycle
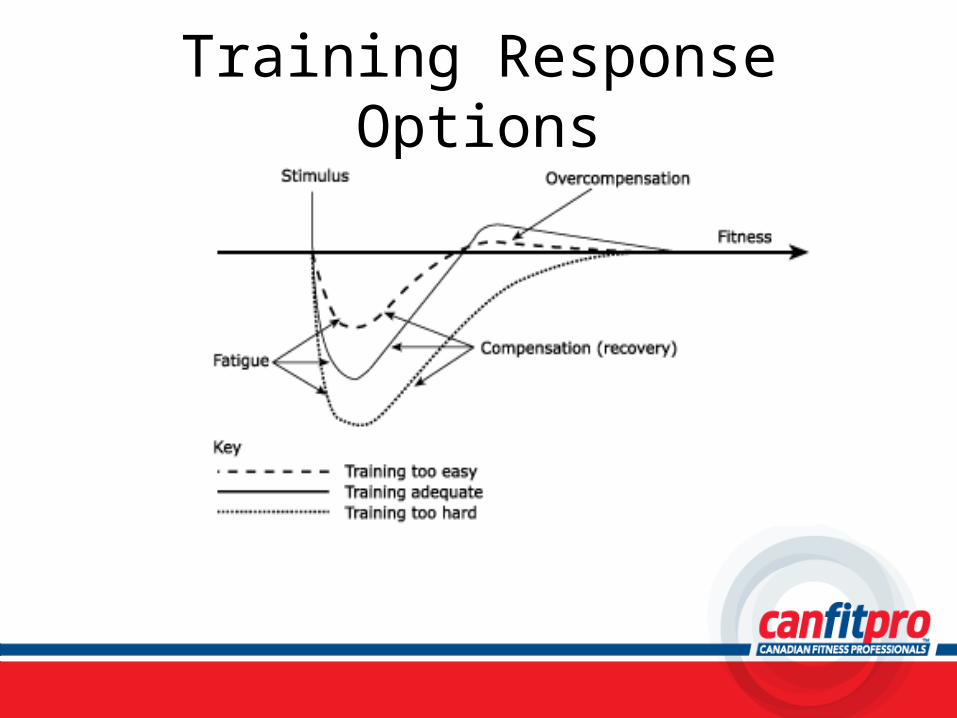
Training Response Options
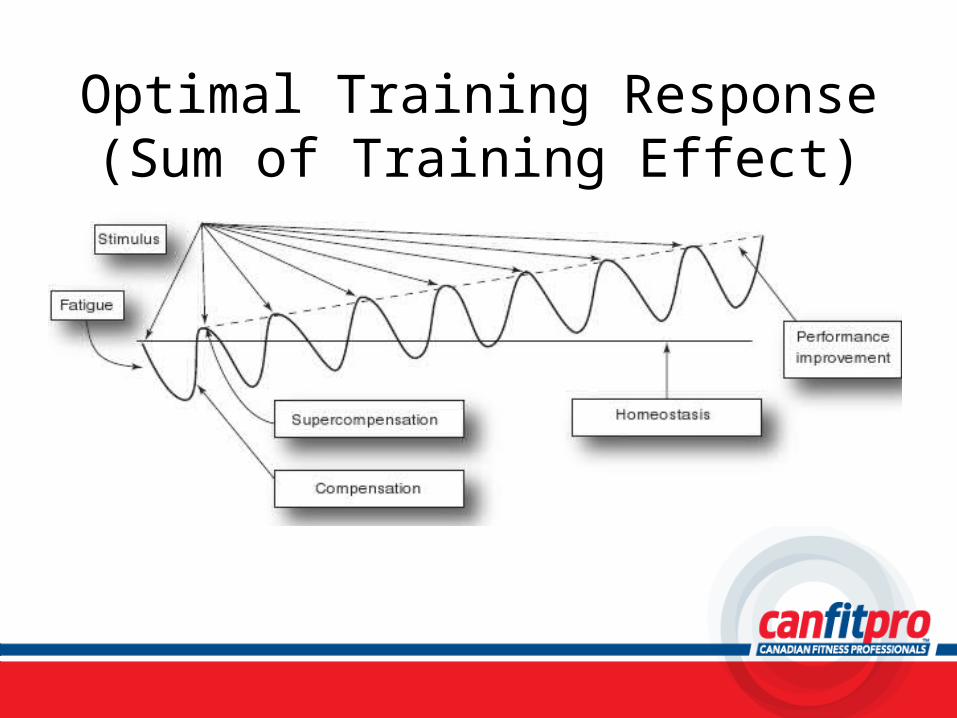
Optimal Training Response(Sum of Training Effect)
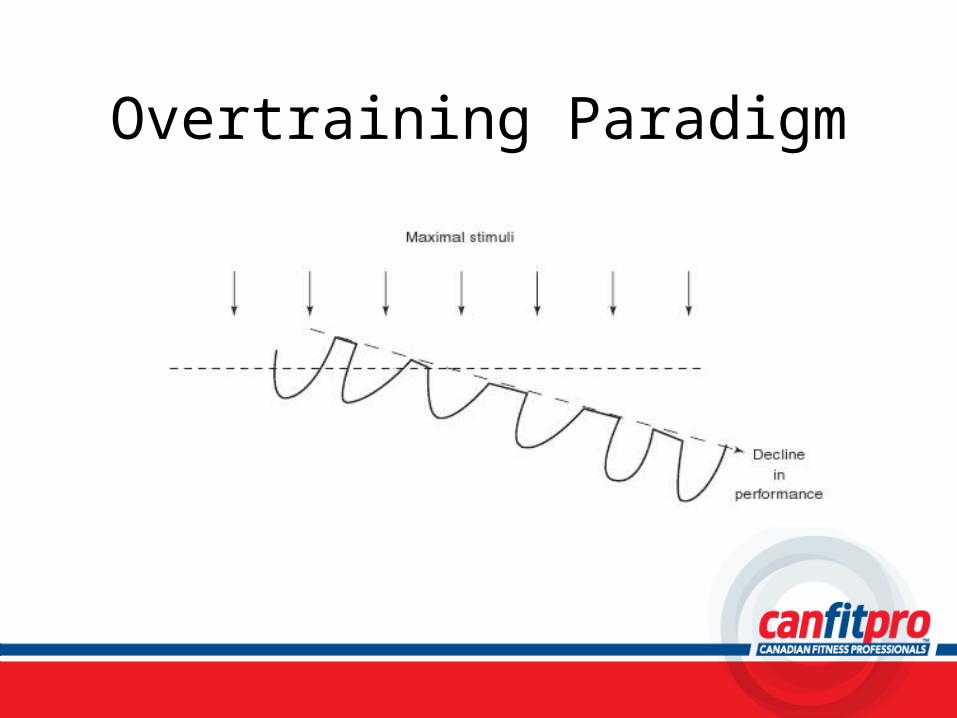
Overtraining Paradigm

canfitpro’s Training Principles• FITT• Individualization• Specificity• Progressive Overload• Recovery• Structural Tolerance• All-around Development• Reversibility• Maintenance
Program Design
• While there are volumes of scientific research with regards to the “best” way to train, personal training is still an art as much as it is a science.
• Your challenge is to take the science, meld it into your philosophy and apply it to an individualized program for your client that fits their goals!
Five Steps to Successful Program Design
• Step 1 → Information gathering• Step 2 → Prioritization of program goals• Step 3 → Creation and evaluation of
program• Step 4 → Delivery of the program• Step 5 → Re-assessment

Step 3: Creation and Evaluation
• In creating a program, consider:– Why am I including this exercise?– Is this a balanced program?– Does it meet the SMART goals for the client?– Is it safe, effective, efficient and enjoyable?– Does it have strength, cardio and flexibility?
Step 3: con’t• Include:
– Basic components of a program– Use of proper terminology
• Consider:– Strength training options
• Type of equipment• Approaches to set performance• Common split training combinations
Step 3: con’t• Consider:
– Cardiorespiratory training options• Type of equipment
– Flexibility training options• Equipment vs no equipment

Developing Your Spiel• Demonstrations of new movements or
equipment use must be delivered with confidence and clarity
• Your knowledge and expertise are demonstrated by incorporating alternative cues or explanations
Typical Personal Training Programs
Foundations of Professional Personal TrainingChapter 11
Critical Questions to Answer
• Designing an effective personalized program requires understanding the client’s– Goals, health status and exercise history– Assessment results and fitness level– Workout location and equipment options– Number of session per week– Time allotted for each session
Putting the Program Together(Other Considerations)
• Beginner, intermediate, advanced• Body building vs. performance athlete• Aesthetics vs. functional training• Machine vs. free weight• Balanced vs. unbalanced• Weight loss vs. weight gain• Strength vs. endurance
All these will significantly influence the type of program you develop and exercise you
select.
For example…
Balanced vs. Unbalanced Training
• Unbalanced training (i.e. training the back more than the chest) is an appropriate strategy for clients whom are dominant in one area and not another, especially when time is a factor
• This is the same case for stretching where you should focus on the areas requiring increased mobility rather than having the client stretch all muscle groups
Modifications to Program Designs
• Modification = small manipulation of sets, reps, load, tempo, exercise
• The body adapts (in 2-6 weeks) to the stimulus it is given (principle of adaptation) resulting in increased performance (overcompensation cycle)
• If the stimulus is not changed further adaptation is inhibited• An entirely new program is not required to continue to
improve and should probably be avoided in the case of a beginner who is just learning the exercise.
As a personal trainer you need to have several different ways to change an exercise in order to challenge the body to continue
to improve.Practice, practice, practice and continuing
education are vital to increasing your knowledge and skill set.
Recording The Program
• The program card should include– The client name– Exercises to be performed– Sets and set performance– Reps and tempo– Amount of rest between sets– Cues/comments/reminders on how to perform exercises
Psychology of Personal Training
Foundations of Professional Personal TrainingChapter 12
What qualities do effective personal trainer’s exhibit?

Qualities Of Effective Personal Trainers
– Knowledgeable– Supportive– Model healthy behaviour– Trustworthy– Enthusiastic– Innovative– Patient– Sensitive– Flexible
– Self Aware– Ability to access resources
and services– Ability to generate
expectations of success– Able to provide timely and
specific feedback– Able to provide clear and
reasonable instructions and plans
Behaviour Change• Stages of change
– Pre-contemplation– Contemplation– Preparation– Action– Maintenance
What Stage is your Client at?
• The Physical Activity Stages of Change Questionnaire is used to determine what stage of change a client is at
Intervention Strategies
• How would you change your approach?1. Client who has been a regular exerciser for
the past 6 months.2. Client who has never exercised and was just
told by their doctor that they need to start.3. Client who has failed at exercise in the past
but is aware of the benefits.
Motivational Strategies
• How can personal trainer’s motivate their client’s toward success?
What Determines Exercise Adherence?
• Demographics• Cognitive and personality variables• Behaviours• Environmental factors
– Social– Physical
• Physical Activity Characteristics– Intensity and duration– Perceived effort– Group Programming– Leader Qualities
SMART Goals
• Client that wants to lose weight.
• Client that wants to increase energy levels.

Treatment Strategies for Different Personalities
• Technical• Sociable• Assertive
Client Fears and Perceptions
• Lack of experience or negative experiences can lead clients to be fearful
• Try to understand and address their experiences and perceptions toward exercise– Successful programming can only begin once
this has been done!
Business of Personal Training
Foundations of Professional Personal TrainingChapter 13

Career Opportunities
• Working within – A fitness centre– A personal training studio– As a freelance/contract personal trainer

Marketing your Services
• Product• Price• Promotion• Place

Product
• Differentiation• Development • Positioning
Price
• High price/low price or mid level pricing• What makes the best sense for you?• Different ways of pricing personal training
sessions• Alternatives to traditional package pricing

Promotions• Direct mail• Print or space ads• Electronic media• Networking• Guerilla marketing• Media outreach• Referrals
It is important to track your marketing efforts.
Why?
Place
• Importance of location

Selling your Services
• Focus on the clients needs and wants• Show how you can help• Develop action plan• Ask for feedback• Present prices• Overcome objections• Follow up
What should your professional image be?

Client-Trainer Agreement

Terminating the Relationship
Risk Management
• Adhere to guidelines
• Insurance
• Litigious situations
• Policies and procedures
Policies and Procedures• canfitpro recommends that personal
trainers follow these policies– Establish a fixed pricing policy and stick to it– Implement a 24 hour cancellation policy– Offer a money back guarantee

The PTS Certification Path
Where do I go from here?
Steps to PTS Certification• 25 hour PTS course• Obtain adult CPR certification/renewal
– Mandatory in order to obtain PTS certification certificate
• PTS theory exam – Usually scheduled within 3-4 weeks from course
end date
• PTS practical exam– Must complete within 6 months of successful
theory exam completion
PTS Theory Exam Details
• Theory exam (3-4 weeks after course)– 100 multiple choice questions and a client case
study– Must obtain 80% average between the two
components– Exam is scheduled for 3 hours– Exam marks will be given to individual candidates
within one week of exam date by the PRO Trainer
PTS Practical Exam Details• Practical exam (complete within 6 months of
successful theory exam)– Upon scheduling practical exam date with PRO
Trainer , candidate will be emailed a detailed hypothetical client and exam package
– Candidate prepares a one hour program for client and comes prepared to show all required skills
– Candidate is required to bring in their own test client
– Practical mark will be given to individual candidates immediately following the examination
Liability Insurancecanfitpro’s preferred insurance provider:
Annual premiums starting as low as $158!
www.sthunt.com/canfitpro 1-877-734-8776