overview of leprosy sara atkinson. world-wide distribution of leprosy significance of the disease...
TRANSCRIPT
Overview of leprosySara Atkinson
• world-wide distribution of leprosy• significance of the disease• understand some immunology behind the
clinical spectrum• be aware of some of the existing treatment
and immunological tests and their shortcomings
• potential importance of understanding the M. leprae genome and current genetics
Kaufman MH, MacLennan. Robert the Bruce and leprosy.Proc R Coll Physicians Edinb 2000; 30: 75-80
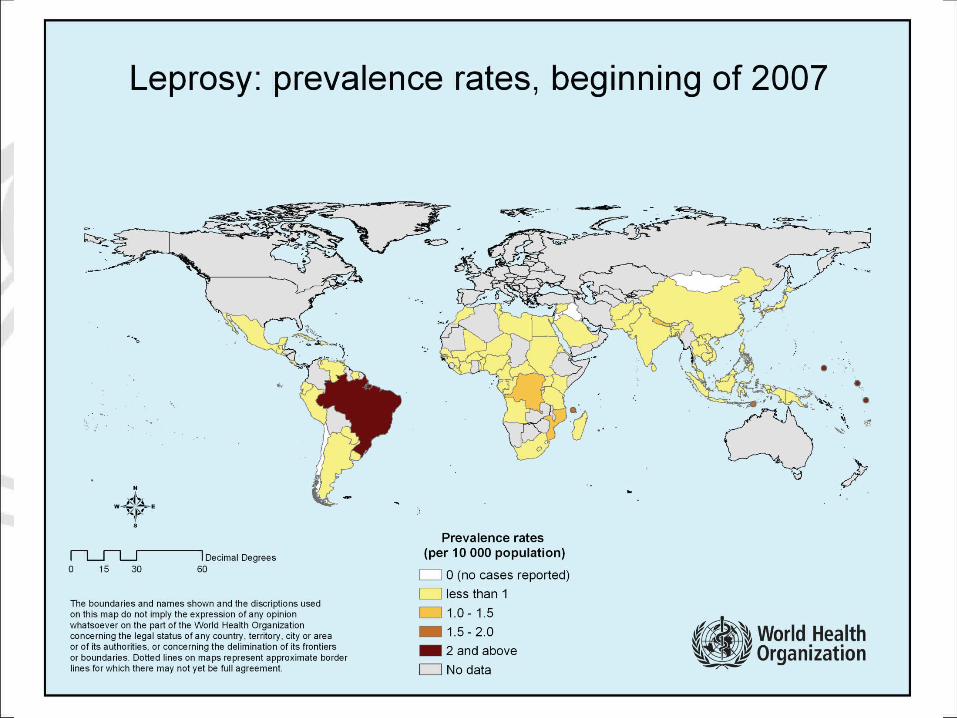
Leprosy - today
• affects 12-15 million people worldwide
• infection relates to overcrowding and lack of hygiene
• stigma
• transmission
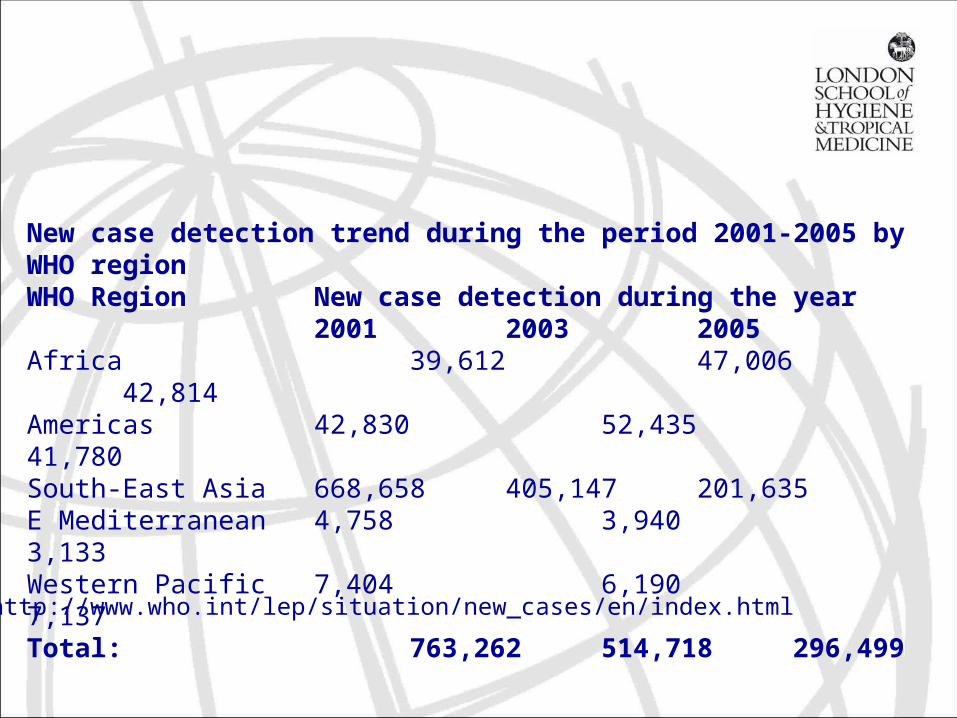
New case detection trend during the period 2001-2005 by WHO region
WHO Region New case detection during the year 2001 2003 2005
Africa 39,612 47,006 42,814 Americas 42,830 52,435 41,780 South-East Asia 668,658 405,147 201,635 E Mediterranean 4,758 3,940 3,133 Western Pacific 7,404 6,190 7,137 Total: 763,262 514,718 296,499
http://www.who.int/lep/situation/new_cases/en/index.html
Leprosy - the infection
• infectious agent Mycobacteria leprae, acid fast, rod shaped bacillus
• structure of M. leprae and M. tuberculosis are very similar although disease very different
• affects skin, peripheral nerves, mucosa of upper respiratory tract, eyes
• intracellular infection
• BCG vaccination confers some protection
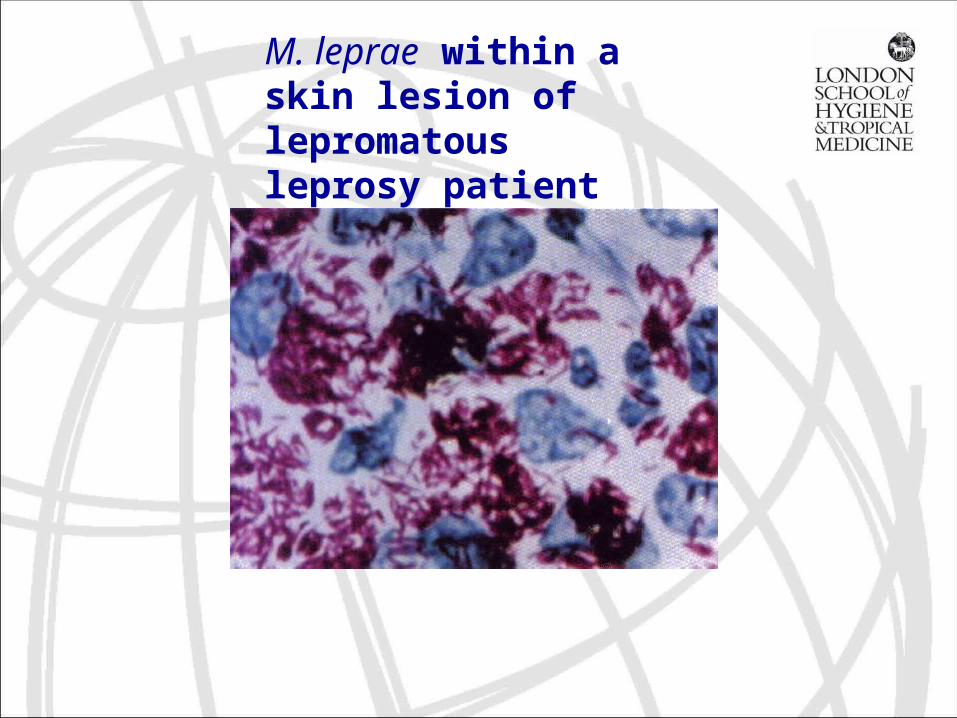
M. leprae within a skin lesion of lepromatous leprosy patient
Leprosy - the infection
only host is the human, except?

Diagnosis
• clinical signs and symptoms
• skin lesion with sensory loss, with or without thickened nerves and/or
• positive skin slit smears
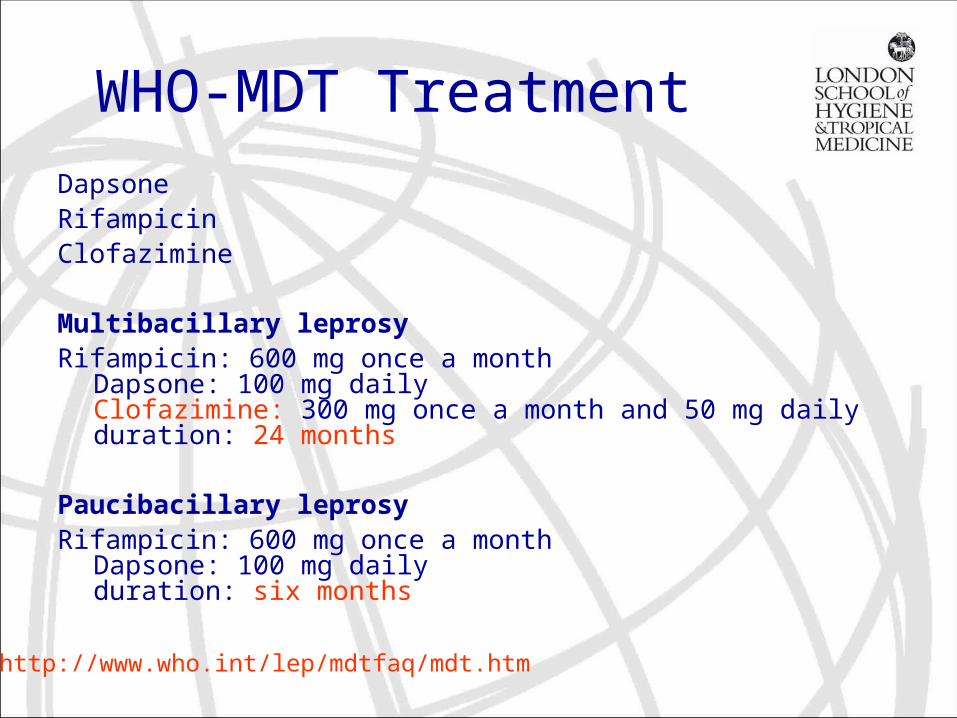
WHO-MDT TreatmentDapsoneRifampicin Clofazimine
Multibacillary leprosyRifampicin: 600 mg once a month
Dapsone: 100 mg dailyClofazimine: 300 mg once a month and 50 mg dailyduration: 24 months
Paucibacillary leprosyRifampicin: 600 mg once a month
Dapsone: 100 mg dailyduration: six months
http://www.who.int/lep/mdtfaq/mdt.htm

Multi-Drug Therapy
MDT cures most patients in 6 months (the more infectious patients within 1 year).
Early treatment prevents deformities and disabilities and therefore social stigmatisation avoided.
Picture courtesy of WHO
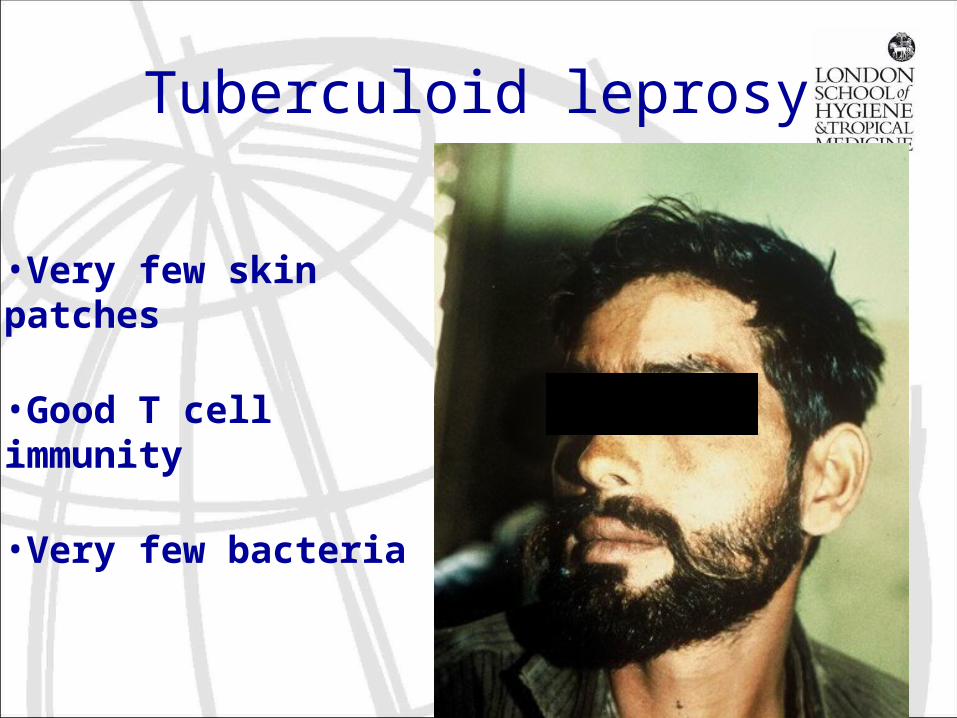
Tuberculoid leprosy
•Very few skin patches
•Good T cell immunity
•Very few bacteria
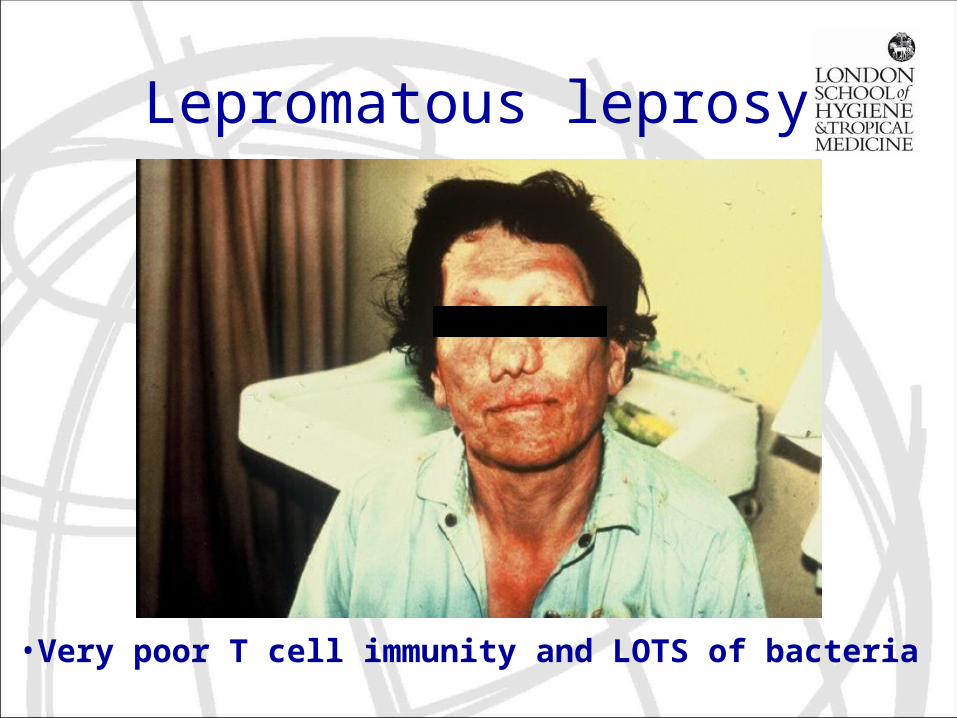
Lepromatous leprosy
•Very poor T cell immunity and LOTS of bacteria
Why is there a spectrum of host response to the same bacteria?
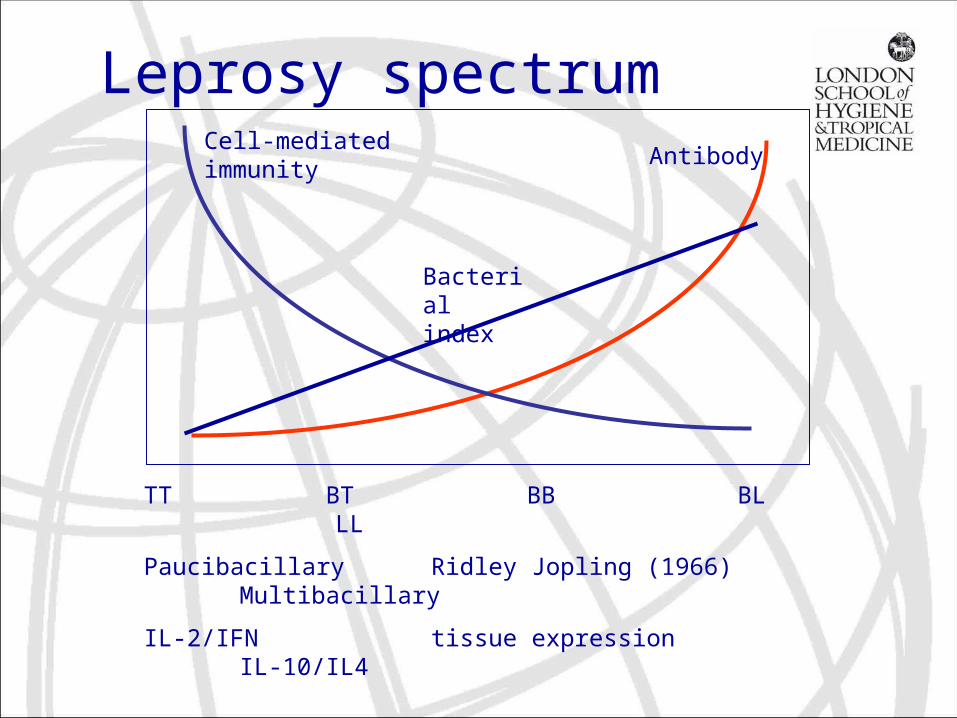
TT BT BB BL LL
Paucibacillary Ridley Jopling (1966) Multibacillary
IL-2/IFN tissue expression IL-10/IL4
Bacterial index
AntibodyCell-mediated immunity
Leprosy spectrum
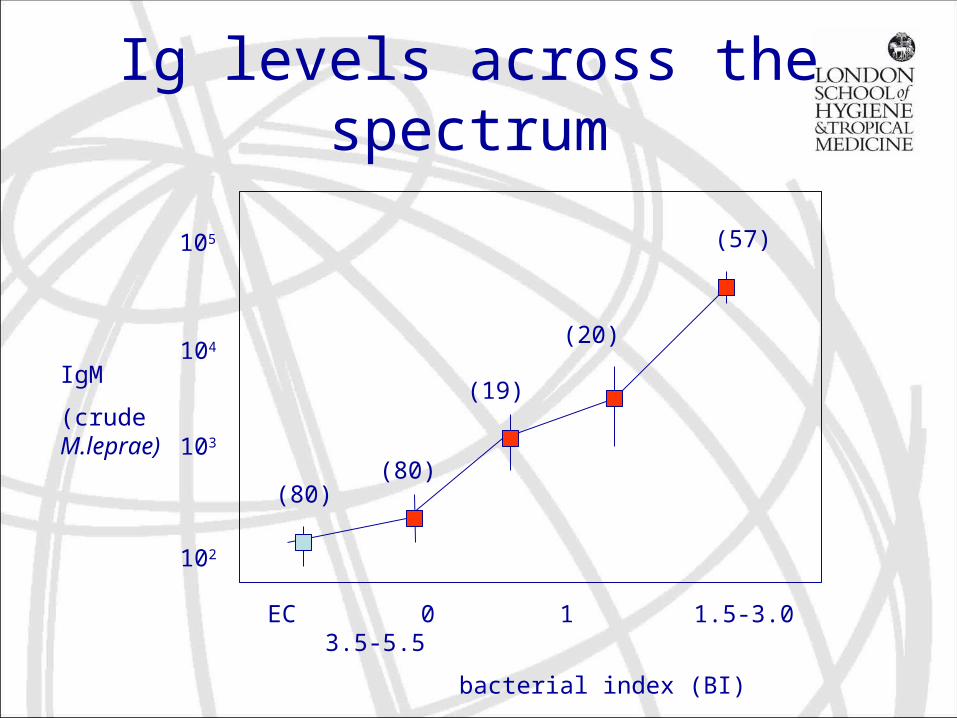
Ig levels across the spectrum
105
104
103
102
EC 0 1 1.5-3.0 3.5-5.5
bacterial index (BI)
IgM
(crude M.leprae)
(80)(80)
(19)
(20)
(57)
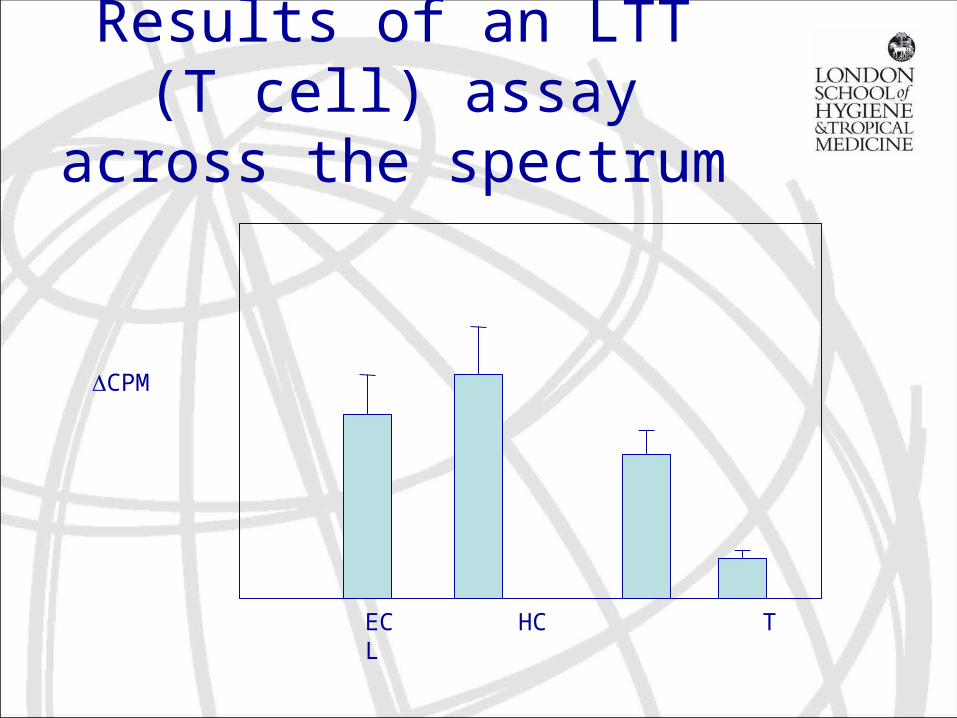
Results of an LTT (T cell) assay across the
spectrum
ΔCPM
EC HC T L
how does the host respond to infection?
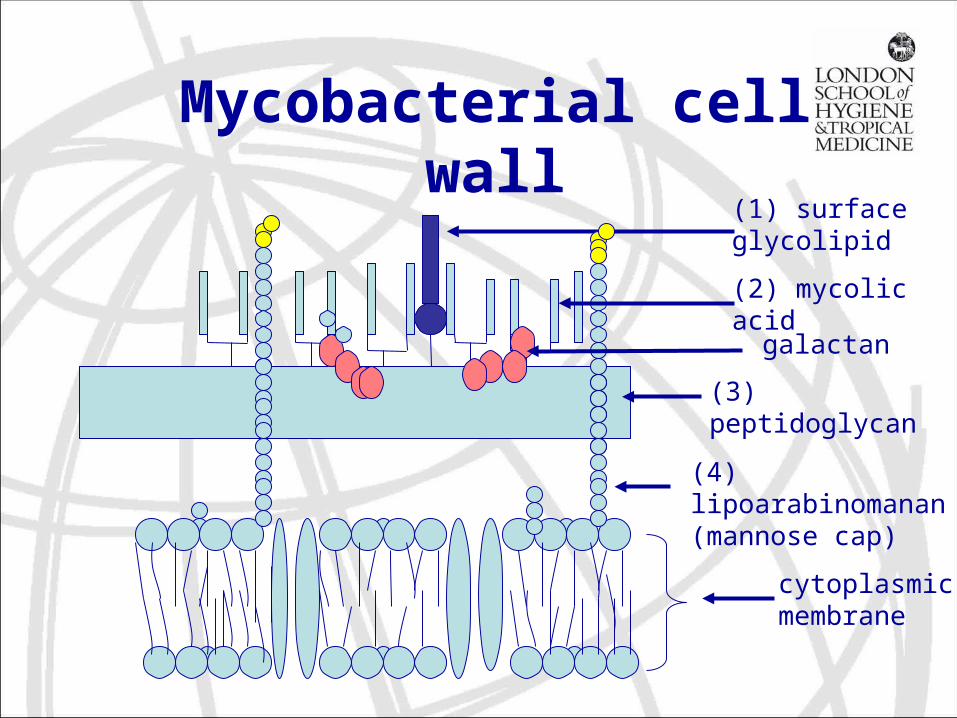
(2) mycolic acid
(3) peptidoglycan
cytoplasmic membrane
galactan
Mycobacterial cell wall
(1) surface glycolipid
(4) lipoarabinomanan (mannose cap)
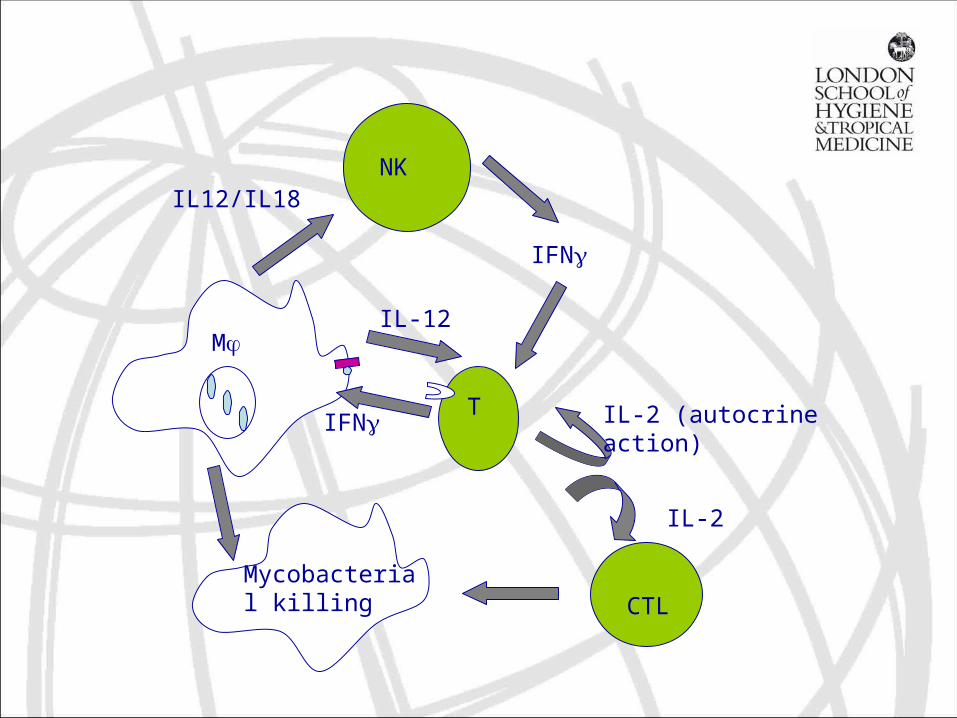
NK
T
CTL
IFNγ
IL-12
Mycobacterial killing
IL-2 (autocrine action)IFNγ
IL12/IL18
Mφ
IL-2
Immunology of M. leprae
• Resides in macrophages, monocytes and Shwann cells
• receptor mediated phagocytosis and thereby avoiding oxidative burst
• PGL-1 binds CR1 and CR4, LAM binds MMR and CD14
• vesicle resists fusion with lysosomes to maintain neutral pH
• M. leprae interfere with intracellular signalling
• LAM and PGL-1 interfere with Ag processing and presentation mechanisms
Reactions
• occurs often within the first 6 months of treatment
• complex clinical manifestations• eg. swelling, redness, tenderness of skin
lesions, pain and tenderness of nerves sometimes with loss of function, irirtis
Two types of reactionRR and ENL
Type1 (RR)
Borderline
Alteration in CMI
prednisolone
Type 2 (ENL)
Lepromatous
Immune complexes
Systemic, iritis
Prednisolone (or thalidomide)
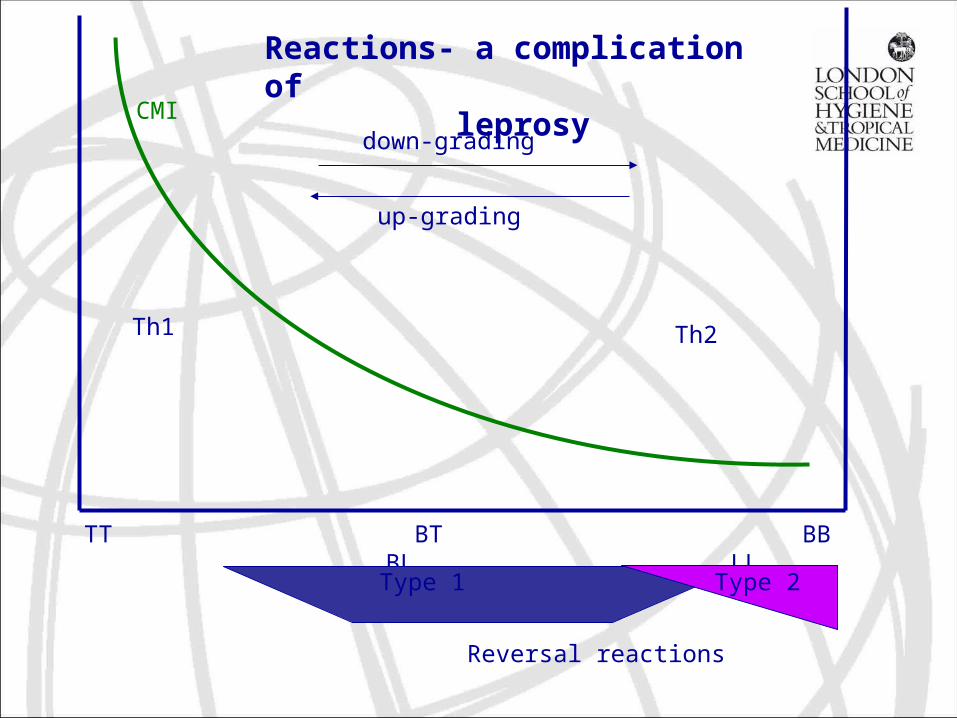
TT BT BB BL LL
CMI
Type 1 Type 2
Reversal reactions
Th1 Th2
down-grading
up-grading
Reactions- a complication of leprosy
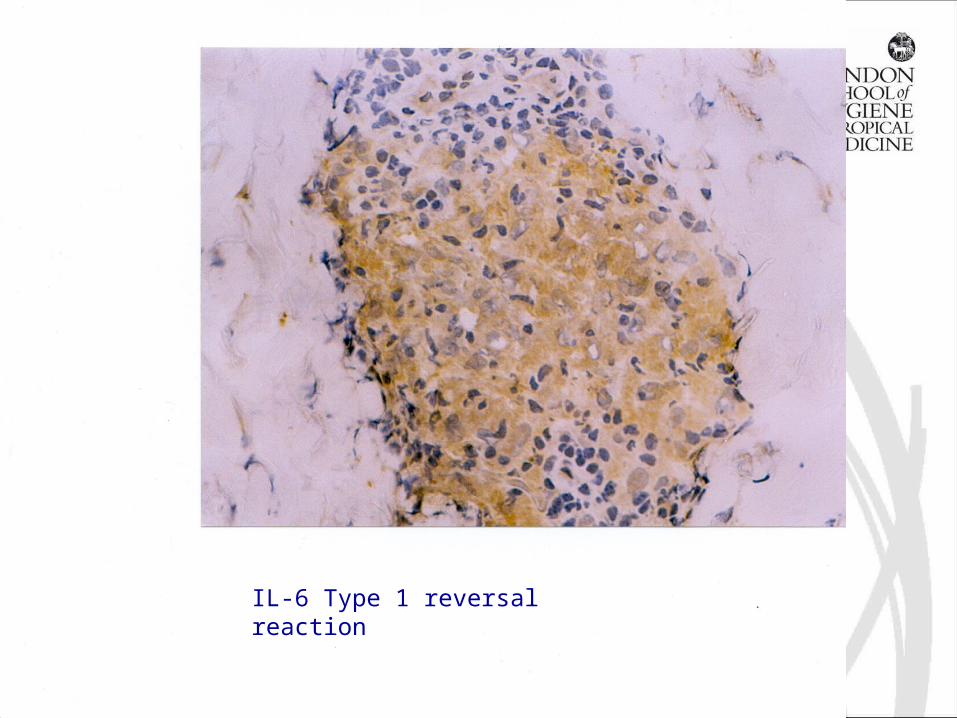
IL-6 Type 1 reversal reaction
why are most people resistant to disease?
Has this women infected her daughter?
Why is it rare for people working with leprosy patients to catch leprosy
Dr Thomas Chiang, MALC
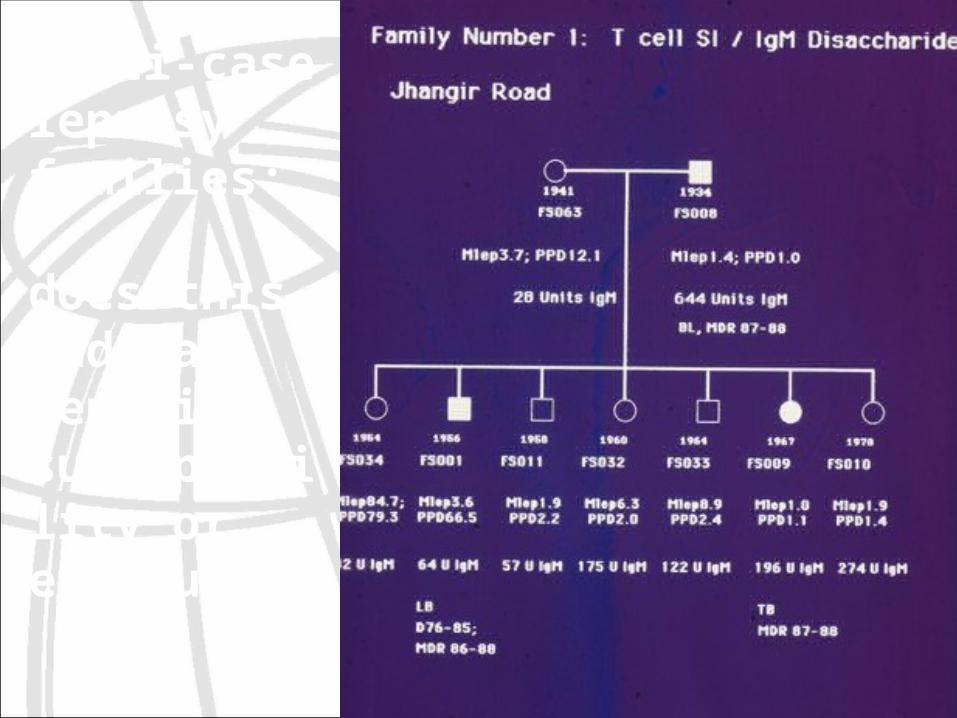
Multi-case leprosy families:
does this indicate genetic susceptibility or exposure?
Genetic susceptibility to leprosy….
•Clustering of cases in families and higher concordance in monozygotic than dizygotic twins
•Associations of HLA-DR2 alleles with susceptibility to leprosy
•Major susceptibility locus mapped to chromosome 10p13 using sib pairs and parents from South India (mannose receptor?)
•Polymorphisms in toll-like receptor 2, and cytokine gene promoters (TNF2, IL-10) also associated with MB or PB leprosy
•Polymorphisms within the IL-12 receptor β2 gene
Siddiqui et al 2001 Nature Genetics 27:439; Fitness et al 2002 Genes Immun 3:441; Ohyama et al 2005 J Clin Path 58:740.
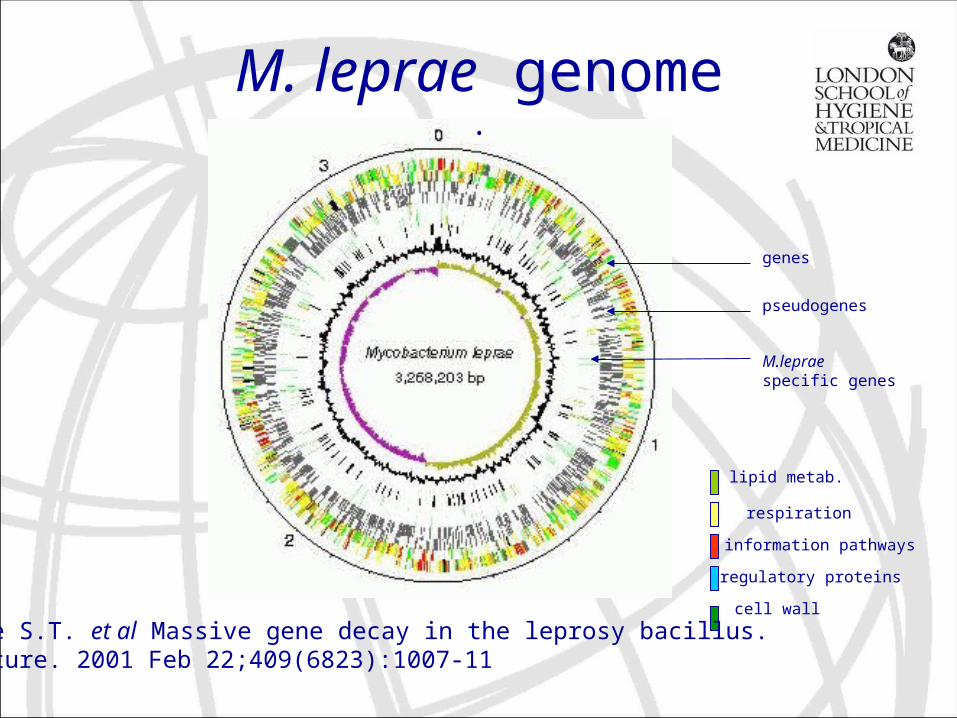
genes
pseudogenes
M.leprae specific genes
lipid metab.
respiration
information pathways
regulatory proteins
cell wall
Cole S.T. et al Massive gene decay in the leprosy bacillus. Nature. 2001 Feb 22;409(6823):1007-11
M. leprae genome.
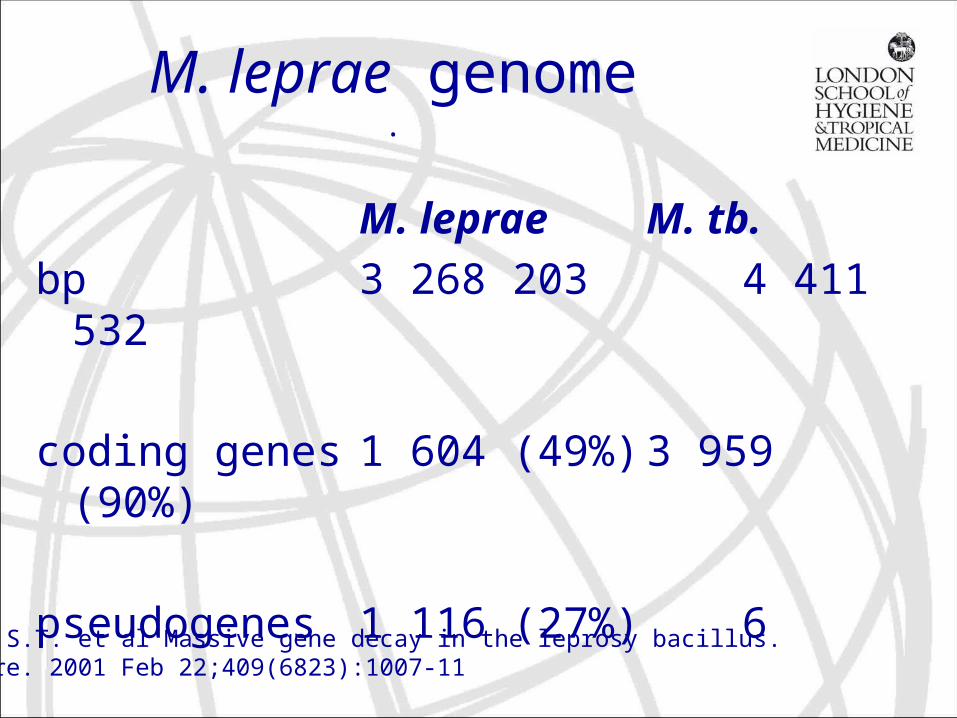
M. leprae genome.
M. leprae M. tb.
bp 3 268 203 4 411 532
coding genes 1 604 (49%) 3 959 (90%)
pseudogenes 1 116 (27%) 6
Cole S.T. et al Massive gene decay in the leprosy bacillus.Nature. 2001 Feb 22;409(6823):1007-11
Use of genome research
• Vaccine • M. leprae-specific human T-cell epitopes, • new drugs• in vitro systems
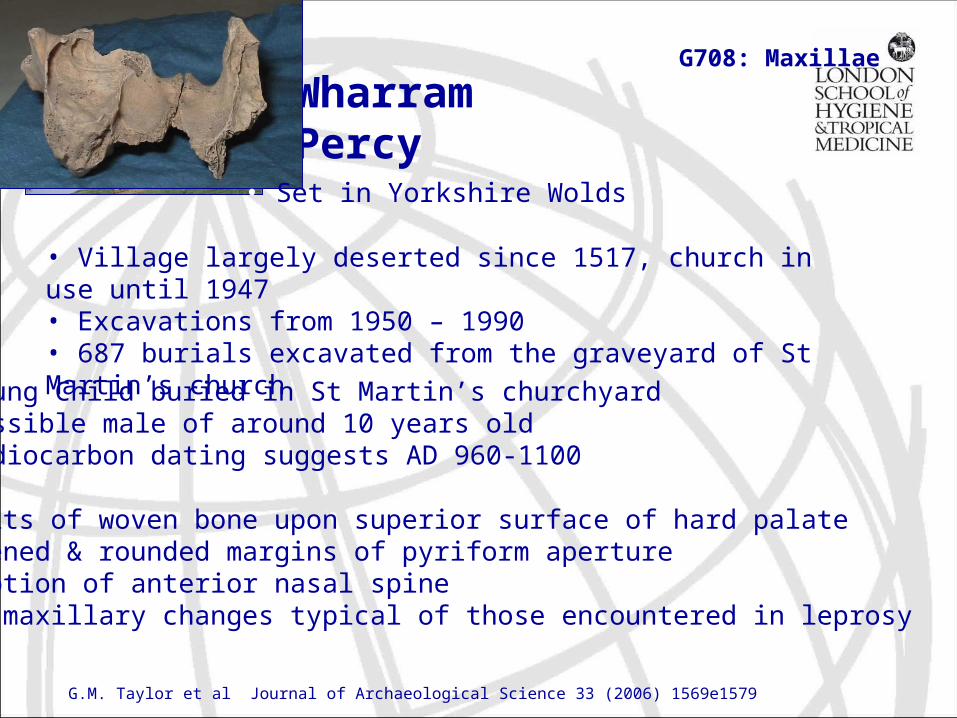
Wharram Percy
• Village largely deserted since 1517, church in use until 1947• Excavations from 1950 – 1990• 687 burials excavated from the graveyard of St Martin’s church
G708: Maxillae
• Set in Yorkshire Wolds
• Young Child buried in St Martin’s churchyard• Possible male of around 10 years old• Radiocarbon dating suggests AD 960-1100
• Deposits of woven bone upon superior surface of hard palate• Thickened & rounded margins of pyriform aperture • Resorption of anterior nasal spine• Rhino-maxillary changes typical of those encountered in leprosy
G.M. Taylor et al Journal of Archaeological Science 33 (2006) 1569e1579
Conclusions
• complex disease, M. leprae resides in macrophages, monocytes and Shwann cells causing many clinical manifestations
• MDT treatment generally effective
• spectrum of disease demonstrates CMI is protective (tuberculoid), Ab not protective (lepromatous)
• immunological/clinical complications…reactions “upgrading” of CMI can lead to tissue damage
• host genetic factors
• need for good diagnostic test
• no simple diagnostic test for leprosy
• BCG confers some protection against leprosy