overview: understanding dementia - dartmouth-hitchcock€¦ · understanding dementia bernie...
TRANSCRIPT
November 16, 2009Workshop I
Common Mental Health Concerns In Older AdultsA Series of Four Workshops
1
Understanding Dementia
Bernie Seifert, LICSW
Northern New England Geriatric Education Center
Common Mental Health Concerns In Older Adults
A Series of Four Workshops
Northern New England Geriatric Education Center at Dartmouth Medical School
November 16, 2009 Understanding Dementia
Upcoming workshops:
December 14, 2009 Substance Abuse and Misuse in Older Adults
February 1, 2010 Hoarding Behaviors in Older Adults
March 2, 2010 Understanding Depression in Older Adults
Overview:
Cognitive functioning (“normal aging” vs. dementia) Various types of dementia Screening for /assessment of dementia Helpful interventions when interacting with
individuals who have dementia
Northern New England Geriatric Education Center at Dartmouth Medical School3
Dementia Diagnostic Criteria*
Weakening of the Memory
Deficit in at least one: Aphasia, Apraxia, Agnosia, Executive Functioning
Impairment in social or occupational functioning
Gradual onset and continuing decline
* DSM-IV-TR (Statistical Manual of Mental Disorders)
Northern New England Geriatric Education Center at Dartmouth Medical School4
Dementia
5
Most cases of dementia in older adults are Alzheimer’s Disease (approx. 60% to 80%)
Next most common type is Vascular Dementia (10% to 20%)
The rest form a long list, including (not limited to): AIDS (HIV Infection), Lewey Bodies, Parkinson’s Disease with dementia, Frontotemporal Dementia (Pick’s Disease), etc.
Dementia
Northern New England Geriatric Education Center at Dartmouth Medical School6
3.4 million Americans have dementia2.9 million have Alzheimer’s Disease5% of people 71-79 y.o. have dementia37.4% of people 90 y.o. have dementia1 in 7 of 71 y.o. and older have dementia
Diagnosis of AD
Northern New England Geriatric Education Center at Dartmouth Medical School7
Clinical
Criteria:1. Gradual & progressive decline cognitive function2. Recent memory impairment with eitherLanguage disturbance Skilled motor function decline (without weakness)Visual processingExecutive function decline
3. Not due to psychiatric, neurological, systemic disease4. Not delirium
Early Diagnosis
Northern New England Geriatric Education Center at Dartmouth Medical School8
Only 3% are diagnosed in the early stage
25% are diagnosed in moderate stage
Many are under diagnosed; even more under treated

Normal Aging –vs- Disease
Northern New England Geriatric Education Center at Dartmouth Medical School9
Early DementiaMemory & concentrationMood & Behavior
Late DementiaLanguage and speechMovement and coordinationOther symptoms
Normal Aging –vs- Disease
Northern New England Geriatric Education Center at Dartmouth Medical School10
Alzheimer’s Disease Normal AgingForgets entire experience Forgets part of an experience
Rarely remembers later Often remembers later
Gradually unable to follow written/verbal directions
Usually able to follow written/verbal directions
Gradually unable to use notes as a reminder
Is usually able to use notes as reminders
Gradually unable to care for self Is able to care for self
Typical Aging
Executive Functioning Short-term memory Confrontation Naming
Northern New England Geriatric Education Center at Dartmouth Medical School11
Hey…Don’t blame it all on aging or dementia!
Northern New England Geriatric Education Center at Dartmouth Medical School12
Some behaviors are lifelong May be exaggerated due to stress, depression, etc. Ability to cope and flexibility is characteristic of
person, not aging Personality does not change with age unless
modified by disease

Mild Cognitive Impairment (MCI)
Northern New England Geriatric Education Center at Dartmouth Medical School13
Memory problems and mild impairments,
but able to function quite well in daily life
MCI – Mild Cognitive Impairment
Northern New England Geriatric Education Center at Dartmouth Medical School14
Useful in identifying persons high risk for AD Symptoms may include:
Memory impairment & one of following:disorientation & impaired judgment changes in mood speech disturbance difficulty with task completion
Different types of MCI
Northern New England Geriatric Education Center at Dartmouth Medical School15
Amnestic MCI Multiple domain MCI Single non-memory domain MCI
Risk factors for MCI High Blood Pressure High Cholesterol Diabetes Osteoporosis Obesity COPD Smoking Head Injury
Northern New England Geriatric Education Center at Dartmouth Medical School16

MCI Screening:
Northern New England Geriatric Education Center at Dartmouth Medical School17
Neuropsychological testing Clinical judgment Screening tools such as MMSE, Mini Cog
Vascular Dementia (VaD)
Northern New England Geriatric Education Center at Dartmouth Medical School18
Also known as Multi-infarct Dementia (MID), Vascular Cognitive Impairment (VCI) , & Cognitive Impairment-No Dementia (CIND)
10%-20% of all dementiasCommonly thought of as the 2nd most common
dementia
Vascular Dementia
Northern New England Geriatric Education Center at Dartmouth Medical School19
Increased risk associated with stroke
Differences in presentation: VAD and AD
Northern New England Geriatric Education Center at Dartmouth Medical School20
Executive dysfunction more impaired (abilities include cognitive flexibility, concept formation and self monitoring)
Memory is less impaired (or not impaired)

Treatment for VaD:
Northern New England Geriatric Education Center at Dartmouth Medical School21
Minimize risk factors (What is good for the heart)Lower BPLow blood sugarsAspirin
Possibly use medications (donepezil, galantimine, rivastigmine, memantine) as AD – similar benefits. Need to weigh against cost/side effects.
Other Dementias…
22
Frontotemporal Dementia (focal atrophy of frontal and temporal region of brain)Gradual progressive behavior/language change (highly
inappropriate social interactions)Occurs between 35 – 75 yr olds
Dementia with Parkinsonism & Dementia with Lewey Bodies:Gradual progressive dementiaFluctuations in cognitive functionPersistent visual hallucinationsSpontaneous motor features
Clinical Features of Lewey Bodies Dementia is essential to diagnosis Plus 2 of the following:Cognitive FluctuationsVisual HallucinationsParkinsonism
Northern New England Geriatric Education Center at Dartmouth Medical School23
Northern New England Geriatric Education Center at Dartmouth Medical School24
Frontal lobeParietal lobeTemporal lobeOccipital lobeCerebellumBrain Stem

Reversible Dementia (“pseudo dementia”)
Northern New England Geriatric Education Center at Dartmouth Medical School25
Medication Induced Alcohol related Metabolic disorders Depression
Screening for Dementia:
Northern New England Geriatric Education Center at Dartmouth Medical School26
Mini Mental State Exam (MMSE) Mini-Cog
Case: “Marion”
Northern New England Geriatric Education Center at Dartmouth Medical School27
81 year-old, widowed 15 years ago; lives alone in same home for past 40 years.
Diabetes, hypertension, arthritis, high cholesterol, macular degeneration.
History of depression following her retirement and husband’s death.
Discontinued alcohol use in recent years. Denies current use.
Has involved family living close by.
Family concerned about recent incidences and question recurrence of depression.
Why use the MMSE?
Northern New England Geriatric Education Center at Dartmouth Medical School28
Tests 5 areas of Cognitive Function:OrientationRegistrationAttention & CalculationRecallLanguage
5-10 min. to administerSource: Folstein, 1975

MMSE Limitations:
Northern New England Geriatric Education Center at Dartmouth Medical School29
Cannot diagnose case for change Relies on verbal response, reading and writing
Source: Folstein, 1975
MMSE – 5 Areas:
Northern New England Geriatric Education Center at Dartmouth Medical School30
Orientation Registration Attention & Calculation Recall Language
Source: Folstein, 1975
31
The Mini-Mental State ExamPatient___________________________________ Examiner ____________________________ Date____________Maximum Score
Orientation5 ( ) What is the (year) (season) (date) (day) (month)?5 ( ) Where are we (state) (country) (town) (hospital) (floor)?
Registration3 ( ) Name 3 objects: 1 second to say each. Then ask patient all 3 after you have said them.
Give 1 point for each correct answer. Then repeat them until he/she learns all 3. Count trials and record # trials: ___________
Attention and Calculation5 ( ) Serial 7’s. 1 point for each correct answer. Stop after 5 answers.
Alternatively spell “world” backward.Recall
3 ( ) Ask for the 3 objects repeated above. Give 1 point for each correct answer.Language
2 ( ) Name a pencil and watch.1 ( ) Repeat the following “No ifs, ands, or buts”3 ( ) Follow a 3-stage command:
“Take a paper in your hand, fold it in half, and put it on the floor.”1 ( ) Read and obey the following: CLOSE YOUR EYES1 ( ) Write a sentence.1 ( ) Copy the design shown.
Source: Folstein, 1975
Scoring for the MMSE
Northern New England Geriatric Education Center at Dartmouth Medical School32
24 - 30 “normal” range
20 - 23 mild cognitive impairment
10 - 19 middle stage impairment (moderate)
0 - 9 late stage impairment (severe)Source: Folstein, 1975
Mini-Cog – 3 steps:
Northern New England Geriatric Education Center at Dartmouth Medical School33
1. 3-item - repeat2. Clock-drawing Test (CDT)3. Recall of 3 items
Source: Borson S. The mini-cog: a cognitive “vitals signs” measure for dementia screening in
multi-lingual elderly Int J Geriatr Psychiatry 2000; 15(11):1021.
Why use the Mini-Cog:
Northern New England Geriatric Education Center at Dartmouth Medical School34
Simple, effective and easily administered Relatively uninfluenced by education level Detects cognitive impairment in earliest stages
Source: Borson S. The mini-cog: a cognitive “vitals signs” measure for dementia
screening in multi-lingual elderly, Int J Geriatric Psychiatry 2000;
15(11):1021.
MINI COG – CDT
1) Inside the circle, please draw the hours of a clock as
they normally appear
2) Place the hands of the clock
to represent the time:
“ten minutes after eleven o’clock”
Northern New England Geriatric Education Center at Dartmouth Medical School35
Scoring Mini-Cog
Northern New England Geriatric Education Center at Dartmouth Medical School36
Source: Borson S. The mini-cog: a cognitive “vitals signs” measure for dementia screening inmulti-lingual elderly, Int J Geriatr Psychiatry 2000; 15(11):1021.
Mini-Cog
Recall = 0(+ Dementia)
Recall = 3(- Dementia)Recall = 1-2
Clock Abnormal(+ Dementia)
Clock Normal(- Dementia)

Limitations to Mini-Cog:
Northern New England Geriatric Education Center at Dartmouth Medical School37
Visual impairment Difficulty holding writing implement Tests only executive functioning
Source: Borson S. The mini-cog: a cognitive “vitals signs” measure for dementia screening
in multi-lingual elderly Int J Geriatric Psychiatry 2000; 15(11):1021.
Marion’s Screening Results:
Northern New England Geriatric Education Center at Dartmouth Medical School38
Mini-Cog MMSE
Depression or Dementia?
Northern New England Geriatric Education Center at Dartmouth Medical School39
Feature: Depression: Dementia:
Onset Can be acute or chronic; may coincide with life changes
Chronic, insidious and gradual
Course May have diurnal effects, (worse in AM) situational fluctuations but less than
acute confusion
Long, no diurnal effects, symptoms progressive; relatively stable over time
Duration At least 2 weeks Slow and continuous
Mood/Affect Extreme sadness, may have anxiety / irritability
Depressed or disinterested, easily distracted, inappropriate anxiety, labile
to apathy
Alertness Normal, may be reduced Generally normal
Adapted from: Edwards, N (2003) Differentiating the three D’s: Delirium, dementia and depression, MEDSURG Nursing, 12(6): 347‐357, and Foreman M., Zane D. (1996) Nursing strategies for acute confusion in elders, American Journal of Nursing 96(4): 44‐52
Depression or Dementia? (cont’d)
Northern New England Geriatric Education Center at Dartmouth Medical School40
Feature: Depression: Dementia:
Attention Minimal impairment but poorly motivated Generally normal
Orientation Selective disorientation May be impaired
Memory Selective or patchy impairment – may complain about impairment
Recent & remote impaired, may confabulate to cover-up deficits
Thinking Intact but with themes of hope-lessness, helplessness, or self-deprecation. May
have difficulty concentrating and be slow to speak
Difficulty with abstraction, thoughts impoverished, judgment impaired,
words difficult to find
Hallucinations/Delusions
May have delusions (often paranoid) May have delusions, usually no hallucinations
Adapted from: Edwards, N (2003) Differentiating the three D’s: Delirium, dementia and depression, MEDSURG Nursing, 12(6): 347‐357, and Foreman M., Zane D. (1996) Nursing strategies for acute confusion in elders, American Journal of Nursing 96(4): 44‐52
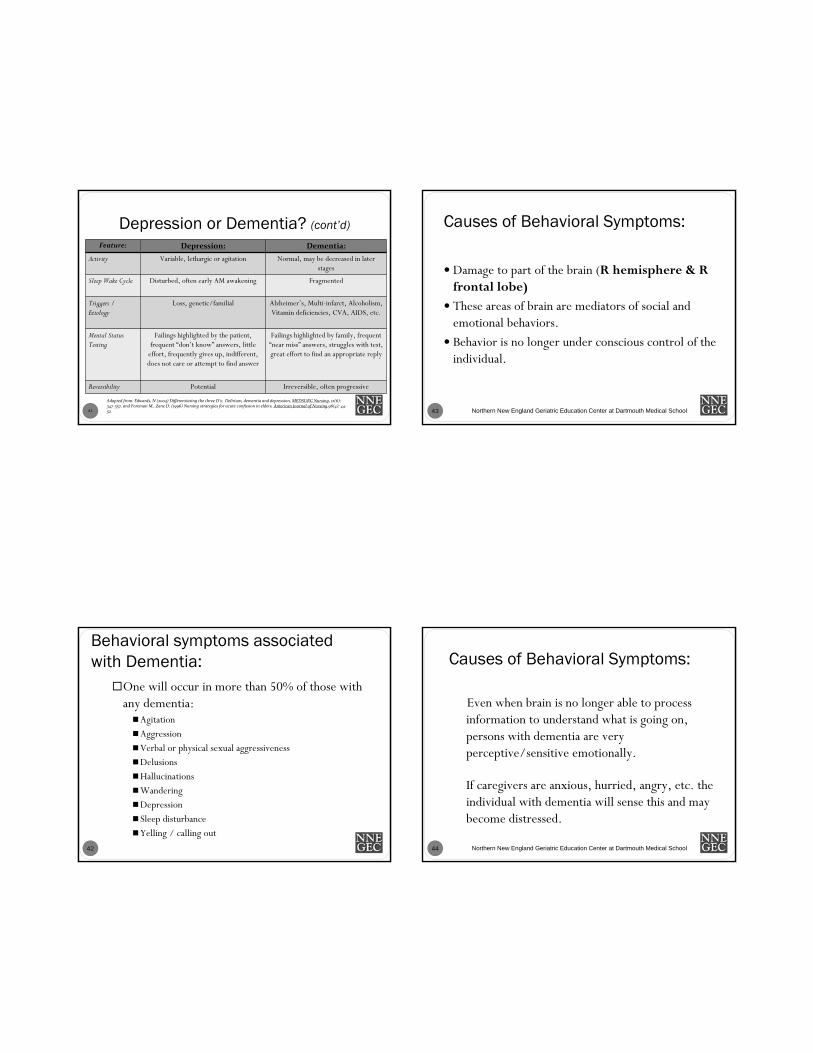
Depression or Dementia? (cont’d)
41
Feature: Depression: Dementia:
Activity Variable, lethargic or agitation Normal, may be decreased in later stages
Sleep Wake Cycle Disturbed, often early AM awakening Fragmented
Triggers / Etiology
Loss, genetic/familial Alzheimer’s, Multi-infarct, Alcoholism, Vitamin deficiencies, CVA, AIDS, etc.
Mental Status Testing
Failings highlighted by the patient, frequent “don’t know” answers, little
effort, frequently gives up, indifferent, does not care or attempt to find answer
Failings highlighted by family, frequent “near miss” answers, struggles with test, great effort to find an appropriate reply
Reversibility Potential Irreversible, often progressive
Adapted from: Edwards, N (2003) Differentiating the three D’s: Delirium, dementia and depression, MEDSURG Nursing, 12(6): 347‐357, and Foreman M., Zane D. (1996) Nursing strategies for acute confusion in elders, American Journal of Nursing 96(4): 44‐52
Behavioral symptoms associated with Dementia:
42
One will occur in more than 50% of those with any dementia:AgitationAggressionVerbal or physical sexual aggressivenessDelusionsHallucinationsWanderingDepression Sleep disturbanceYelling / calling out
Causes of Behavioral Symptoms:
Northern New England Geriatric Education Center at Dartmouth Medical School43
Damage to part of the brain (R hemisphere & R frontal lobe)
These areas of brain are mediators of social and emotional behaviors.
Behavior is no longer under conscious control of the individual.
Causes of Behavioral Symptoms:
Northern New England Geriatric Education Center at Dartmouth Medical School44
Even when brain is no longer able to process information to understand what is going on, persons with dementia are very perceptive/sensitive emotionally.
If caregivers are anxious, hurried, angry, etc. the individual with dementia will sense this and may become distressed.
Non-pharmacological Interventionsin Nursing – (top 10)
Northern New England Geriatric Education Center at Dartmouth Medical School45
Remain flexible
Respond to emotion, not behavior
Don’t argue
Use memory aide
Acknowledge request & respond to them
Look for reasons for behavior
Collaborate with other disciplines
Explore various solutions
Don’t take it personally!
Talk with a colleague
Nursing Interventions: Communication Tips (Top 10 )
Northern New England Geriatric Education Center at Dartmouth Medical School46
Be calm
Focus on feelings, not facts
Pay attention to the tone of the voice
Address by preferred name
Speak slowly using simple words
Ask 1 question at a time
Avoid vague words
Don’t talk about the person as if they aren’t there
Use gestures
Be patient, flexible and understanding
Personal Care with Dignity: (Top 10)
Northern New England Geriatric Education Center at Dartmouth Medical School47
Be flexible – adapt to their preference
Help them stay as independent as possible
Guide by using step-by-step instructions
Communicate as suggested already
Avoid rushing the person
Encourage, reassure, and praise
Watch for unspoken communication
Consider using different products (what do they use at home)
Be patient, kind and understanding
Experiment with new approaches
Response to behavioral symptoms:
Northern New England Geriatric Education Center at Dartmouth Medical School48
Dealing with behaviors are major cause of stress and burnout for care providers
2 strategies:1. Blame the disease not the person2. Interpret behavior according to knowledge of
person’s history

Web Sites:
National Institute of Mental Health www.nimh.nih.gov
National Institute of Neurological Disorders and Stroke (NINDS) www.ninds.nih.gov
Alzheimer’s Association www.alz.org (put in zip code for most local Alzheimer’s Association office)
National Institute on Aging www.nia.nih.gov
Northern New England Geriatric Education Center at Dartmouth Medical School49
Questions / Further Discussion
Northern New England Geriatric Education Center at Dartmouth Medical School50