oxygen therapy
TRANSCRIPT
OXYGEN THERAPY
Dr. Tejasree
What is oxygen?
Why do we need oxygen?
What is oxygen therapy?
When do we need oxygen therapy?
How to give oxygen therapy?
WHAT IS OXYGEN?
In 1775 by joseph priestley an english
scientist.
Oxygen is a chemical element with
symbol O and atomic number 8.
Highly reactive nonmetallic element
and oxidizing agent that readily
forms compounds.
3rd most abundant element in the universe.
Colorless, odorless, and tasteless
WHY DO WE NEED OXYGEN?
Cellular respiration.
Biochemical energy from nutrients to ATP.
Aerobic respiration.
Anaerobic respiration.

AEROBIC RESPIRATION
Pyruvate from glycolysis.
Kreb’s cycle
Electron transport chain
WHAT IS OXYGEN THERAPY?
Oxygen therapy is administration of oxygen
in concentration more than in ambient air as
a medical intervention.
Thus providing adequate oxygen in the
blood, while decreasing the work of breathing
and reducing the stress on the myocardium.

7
INDICATIONS FOR OXYGEN THERAPY
Hypoxemia
Inadequate amount of oxygen in the blood
SPO2 < 90%
PaO2 < 60 mmHg
Excessive work of breathing
Excessive myocardial workload
FACTORS INFLUENCING OXYGEN
TRANSPORT
Cardiac output
Arterial oxygen content
Concentration of Hb
Metabolic requirements

Hypoxemia
decrease in the arterial oxygen content in
the blood
Hypoxia
decreased oxygen supply to the tissues.

10
CAUSES OF HYPOXEMIA
Shunt
Hypoventilation As carbon dioxide increases oxygen falls
V/Q mismatching (ventilation/perfusion) Pneumonia
Pulmonary edema
ARDS
Increased diffusion gradient asbestosis
Early pulmonary edema
CLINICAL MANIFESTATIONS OF
HYPOXIA Impaired judgment, agitation (restlessness),
disorientation, confusion, lethargy, coma
Dyspnea
Tachypnea
Tachycardia, dysrhythmias
Elevated BP
Diaphoresis
Central cyanosis
CAUSES OF HYPOXIA
Hypoxic hypoxia
Anemic hypoxia
Ischemic or stagnant hypoxia
Histotoxic hypoxia

NEED FOR OXYGEN IS ASSESSED BY
Clinical evaluation
Pulse oximetry
ABG
14
OXYGEN THERAPY
Goal of therapy is an SPO2 of >90% or for documented COPD patients(Spo2 88–92%)-(Pao2=55-60)
As SPO2 normalizes the patients vital signs should improve” Heart rate should return to normal for patient
Respiratory rate should decrease to normal for patient
Blood pressure should normalize for patient

CAUTIONS FOR OXYGEN THERAPY
Oxygen toxicity – can occur with Fio2 > 60% longer than 36 hrs
Fio2>80%longer than 24 hrs Fio2>100%longer than 12hrs
Suppression of ventilation – will lead to increased CO2 and carbon dioxide narcosis
Danger of fire
Absorbtion Atelectasia
Premature retrolental fibroplasia
OXYGEN DELIVERY DEVICES
1. High flow (fixed performance) delivery
systems.
2. Low flow (variable performance) delivery
systems.

Low flow systems
contribute partially to inspired gas client breathes
do not provide constant FIO2
Ex: nasal cannula, simple mask
High flow systems
deliver specific and constant percent of oxygen
independent of client’s breathing
Ex: Venturi mask, non-rebreather mask, trach collar, T-
piece
Low Flow Oxygen Delivery Devices :
These include:
i. Nasal cannula.
ii. Simple mask / Mary Carterall mask.
iii. Oxygen tents.
iv. Non rebreathing mask.
v. Rebreathing mask.
vi. Polymask.
High flow oxygen delivery devices:
i. Venturi mask
ii. Air entertainment nebulizers.
iii. High flow air-oxygen blenders.
iv. Bag & mask ventilation
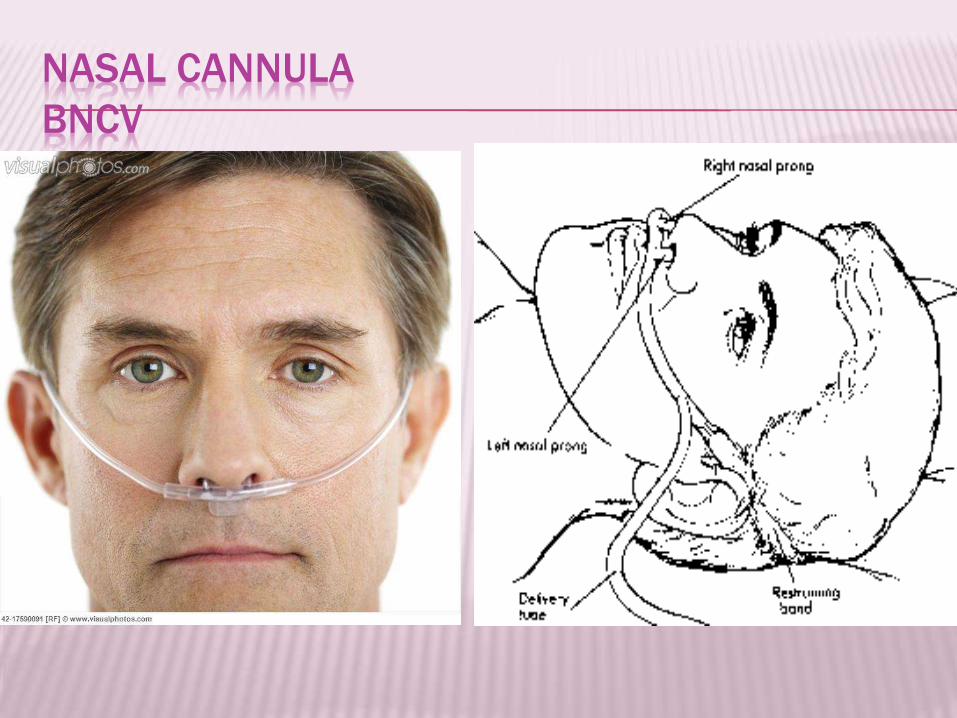
NASAL CANNULA
BNCV
NASAL CANNULA
MERITS DEMERITS Easy to fix
Keeps hands free
Not much interference
with further airway care
Low cost
Compliant
Unstable
Easily dislodged
High flow uncomfortable
Nasal trauma – drying and
crusting
Mucosal irritation
FiO2 can be inaccurate and
inconsistent
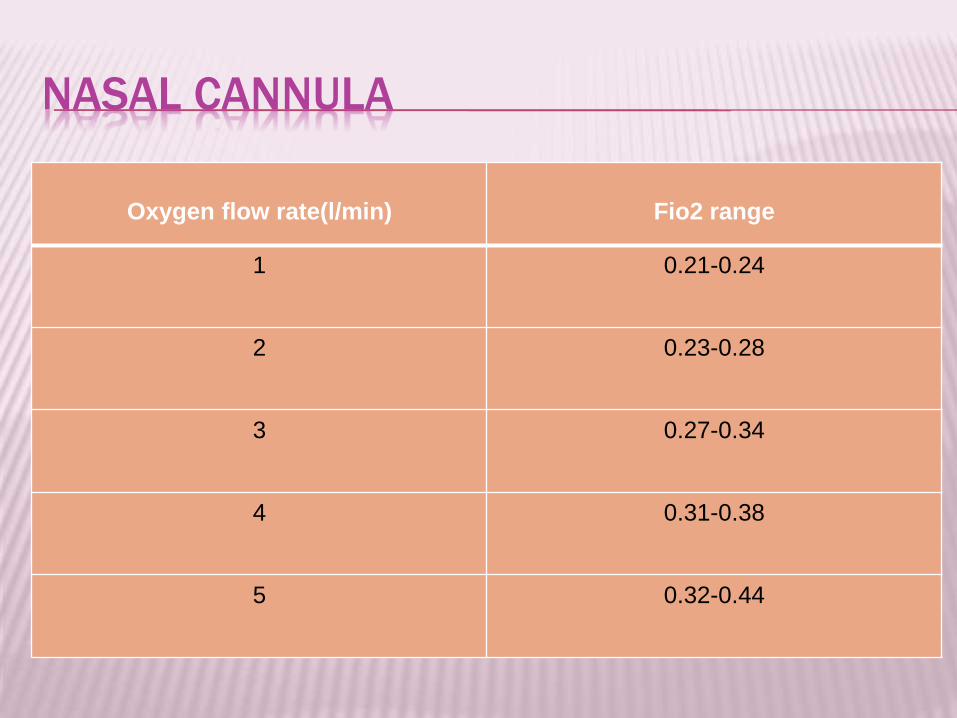
NASAL CANNULA
Oxygen flow rate(l/min) Fio2 range
1 0.21-0.24
2 0.23-0.28
3 0.27-0.34
4 0.31-0.38
5 0.32-0.44

The Inspired percent oxygen increases by
approx. 1-2%(above 21%) per litre of oxygen
flow.



PENDANT RESERVOIR

NASAL RESERVOIR

NASAL CATHETER

NASAL CATHETER
MERITS DEMERITS
Good stability
Disposable
Low cost
Difficult to insert
High flow increases back
pressure
Needs regular changing
May provoke gagging, air
swallowing, aspiration
Nasal polyps, deviated
septum may block insertion

TRANSTRACHEAL CATHETER
A thin
polytetrafluoroethylene
(Teflon) catheter
Inserted surgically with a
guidewire between 2nd and
3rd tracheal rings
FiO2 – 22-35%
Flow – ¼ - 4L/min
Increased anatomic
reservoir
TRANSTRACHEAL CATHETER
MERITS DEMERITS
Lower O2 use and cost
Eliminates nasal and skin
irritation
Better compliance
Increased exercise
tolerance
Increased mobility
High cost
Surgical complications
Infection
Mucus plugging
Lost tract
NASAL MASK
Hybrid of nasal cannula and face mask.
Supplemental oxygen equivalent to nasal
cannula under low flow conditions for adult
patients.
Advantage – patient comfort.
does not produce sores around nares
Dry oxygen is not jetted into nasal cavity.

NASAL MASK

NASAL MASK

NASAL MASK

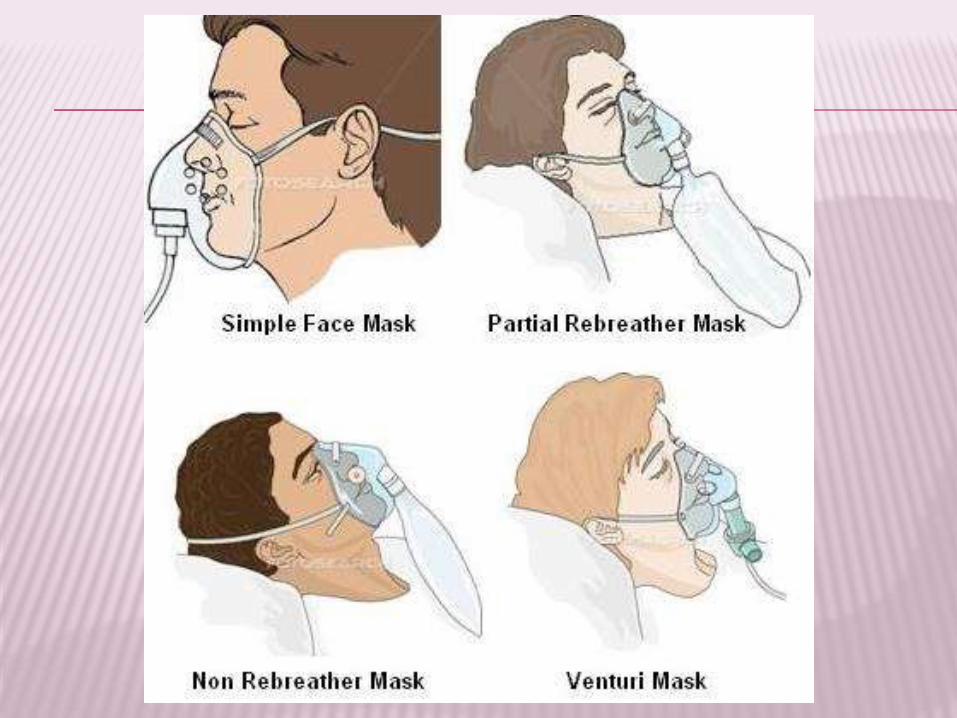
SIMPLE OXYGEN MASK

SIMPLE OXYGEN MASK
MERITS DEMERITS
Disposable
Light weight
Covers both nose and
mouth
Elastic headband
No reservoir bag
Maleable metal nose bridge
Incomplete seal
Inboard leaking
Mixture of oxygen and
entrained room air
Uncomfortable
Speech is muffles
Drinking and eating are
difficult
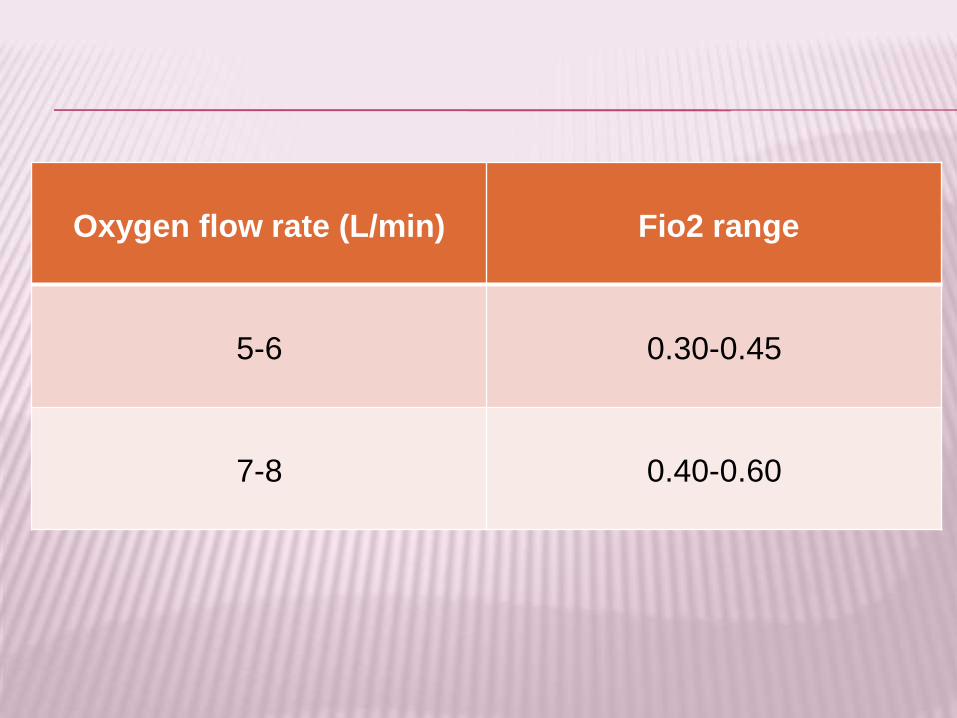
Oxygen flow rate (L/min) Fio2 range
5-6 0.30-0.45
7-8 0.40-0.60

Masks lacking oxygen reservoirs best for
Patients who require concentrations of
oxygen greater than cannulas provide
Need oxygen therapy for fairly short
periods of time
Example: medical transport or therapy,
PACU, ER
not for patients with severe respiratory
disease who are hypoxemic, tachypneic or
unable to protect their airway from
aspiration.

MASK WITH RESERVOIRS
Partial rebreathing mask
Non rebreathing mask

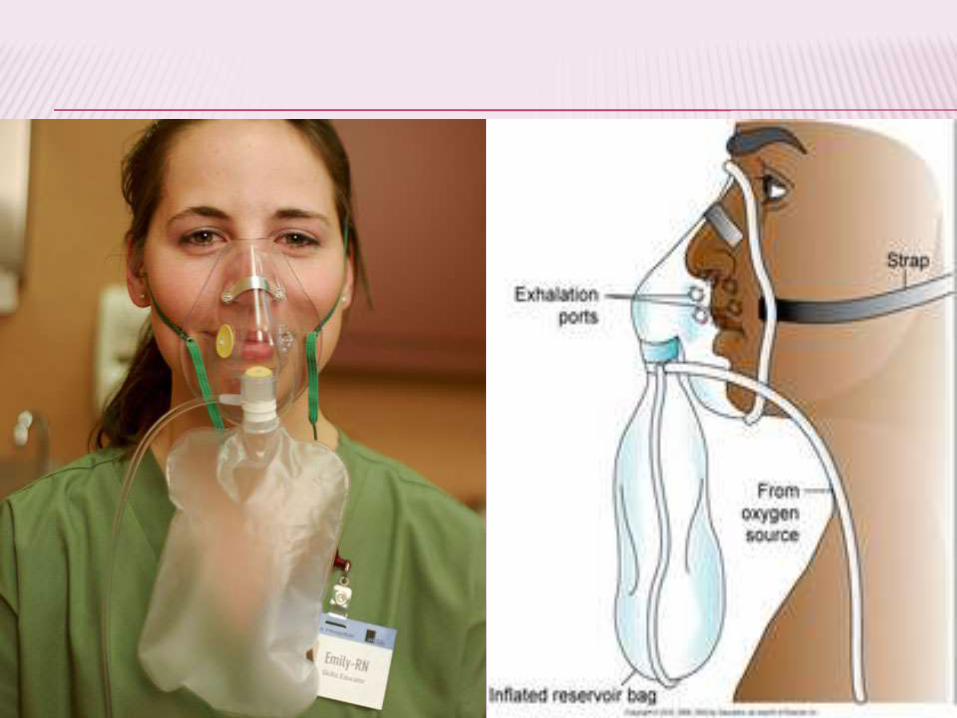
PARTIAL REBREATHING MASK
Consists of mask with exhalation ports and reservoir bag
Reservoir bag must remain inflated
O2 flow rate - 6 to 10L
FIO2=60%-80%
Client can inhale gas from mask, bag, exhalation ports
Poorly fitting; must remove to eat

PARTIAL REBREATHING MASK
No valves
Mechanics –
Exp: O2 + first 1/3 of exhaled gas (anatomic dead space) enters the bag and last 2/3 of exhalation escapes out through ports
Insp: the first exhaled gas and O2 are inhaled
FiO2 - 60-80%
FGF > 8L/min
The bag should remain inflated to ensure the highest FiO2 and to prevent CO2 rebreathing
Exhalation
ports
O2
Reservoir
+


NON-REBREATHING MASK
Consists of mask, reservoir bag, 2 one-way valves at exhalation ports and bag
Client can only inhale from reservoir bag
Bag must remain inflated at all times
O2 flow rate- 10 to 15L
Fio2= 95-100%
Poorly fitting; must remove to eat

NON-REBREATHING MASK
Has 3 unidirectional valves
Expiratory valves prevents air entrainment
Inspiratory valve prevents exhaled gas flow into reservoir bag
FiO2 - 0.80 – 0.90
FGF – 10 – 15L/min
To deliver ~100% O2, bag should remain inflated
Factors affecting FiO2
air leakage and
pt’s breathing pattern
O2
Reservoir
One-way valves

Fixed performance
(High – Flow) equipment


VENTURI MASK
• Most reliable and accurate method for delivering a precise O2 concentration
• Consists of a mask with a jet
• Excess gas leaves by exhalation ports
• O2 flow rate 4 to 15L & Narrowed orifice
• Fio2, 24%-60%
• Can cause skin breakdown; must remove to eat

AIR ENTRAINMENT NEBULIZER
Have a fixed orifice, thus, air-to-O2 ratio
can be altered by varying entrainment port
size.
Fixed performance device
Deliver FiO2 from 28-100%
Max. gas flows – 14-16L/min
Device of choice for delivering O2 to
patients with artificial tracheal airways.
Provides humidity and temperature control

AIR ENTRAINMENT NEBULIZER
Aerosol
mask
Face tentTracheostomy
collar
T tube
HOW TO INCREASE THE FIO2 CAPABILITIES OF
AIR-ENTRAINMENT NEBULIZERS?
1. Adding open reservoir (50-150ml aerosol tube)
2. Provide inspiratory reservoir (a 3-5 L anaesthesia bag) with a one way expiratory valve
3. Connect two or more nebulizers in parallel
4. Set nebulizer to low conc (to generate high flow) and providing supplemental O2 into delivery tube

BAG AND MASK VENTILATION

TRACHEOSTOMY COLLAR/MASK
O2 flow rate 8 to 10L
Provides accurate
FIO2
Provides good
humidity; comfortable

T-PIECE
Used on end of ET tube
when weaning from
ventilator
Provides accurate FIO2
Provides good humidity
FACE TENT
Low flow
O2 wet
O2 flow, 4-8 lit
Fio2=40%

Oxygen tent
Hood
Incubator
ENCLOSURES
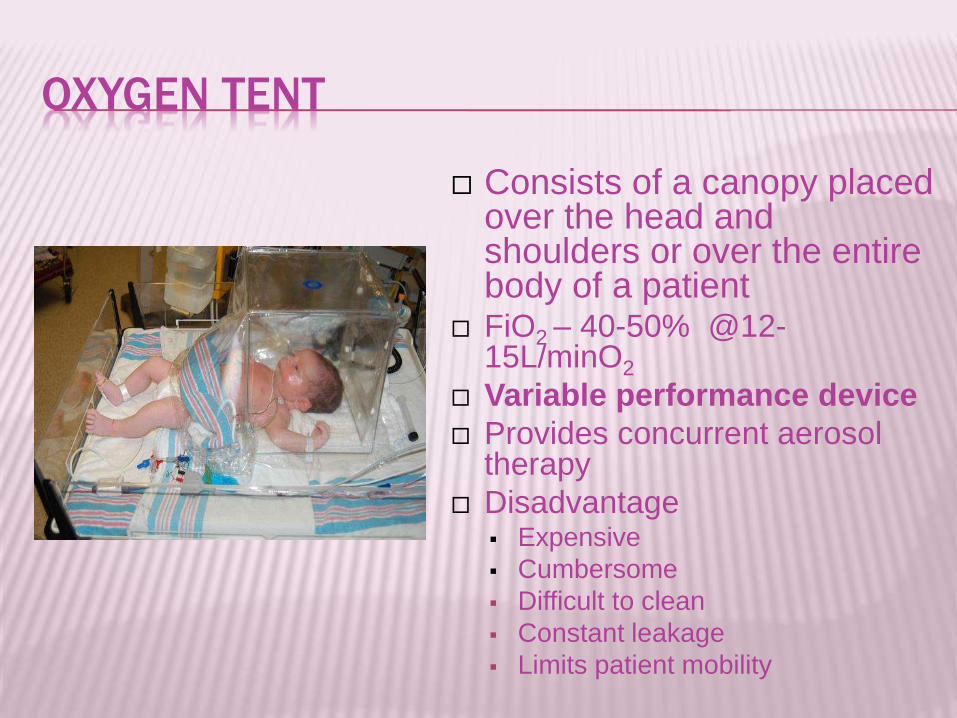
OXYGEN TENT
Consists of a canopy placed over the head and shoulders or over the entire body of a patient
FiO2 – 40-50% @12-15L/minO2
Variable performance device
Provides concurrent aerosol therapy
Disadvantage Expensive
Cumbersome
Difficult to clean
Constant leakage
Limits patient mobility
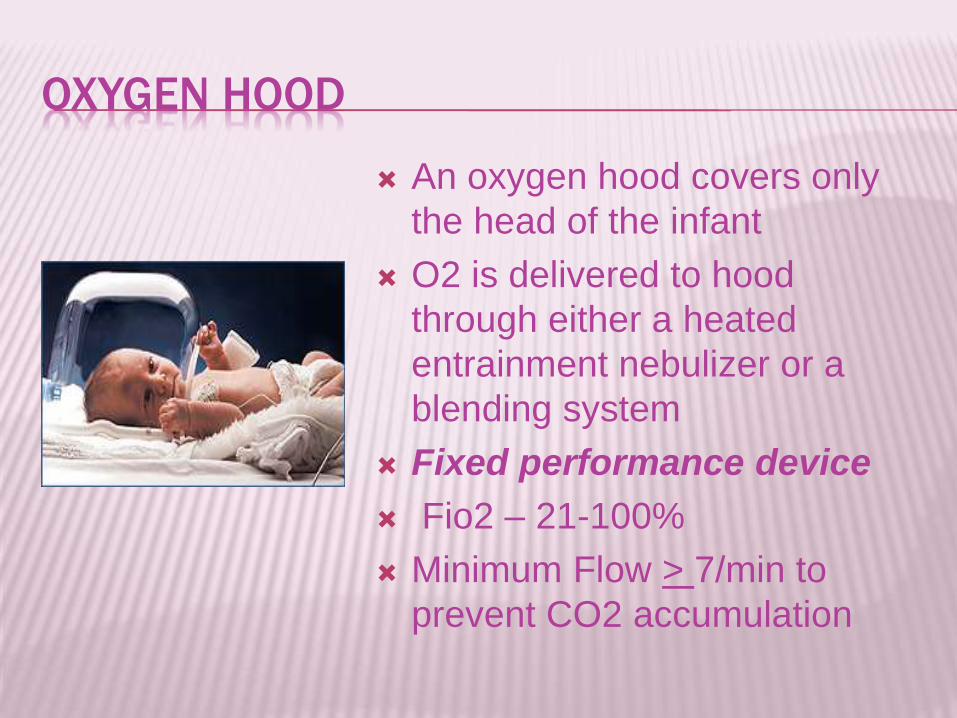
OXYGEN HOOD
An oxygen hood covers only
the head of the infant
O2 is delivered to hood
through either a heated
entrainment nebulizer or a
blending system
Fixed performance device
Fio2 – 21-100%
Minimum Flow > 7/min to
prevent CO2 accumulation
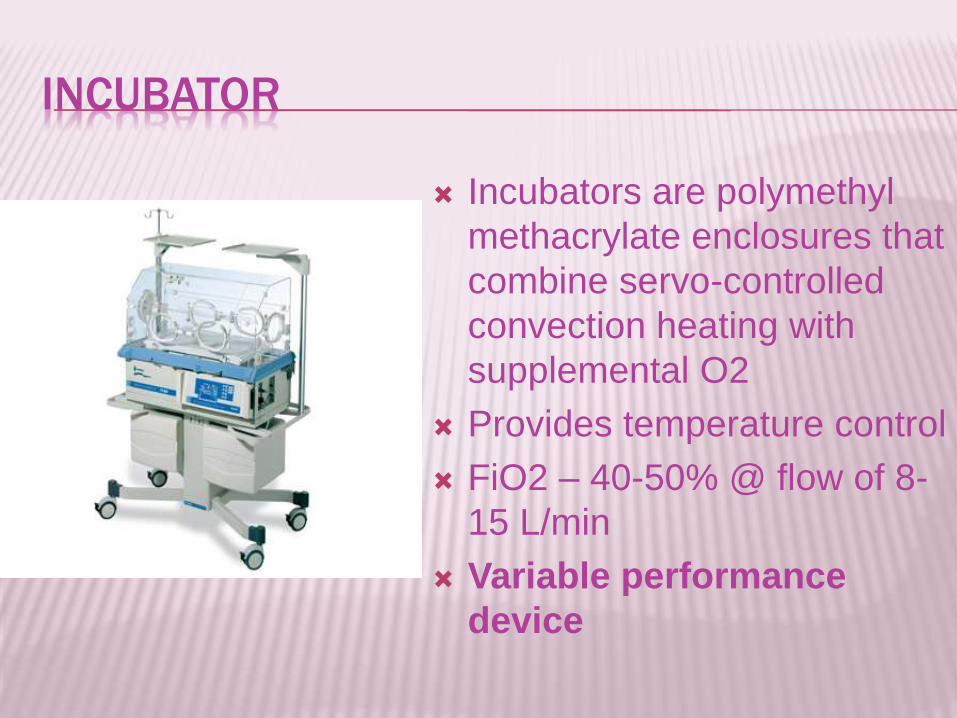
INCUBATOR
Incubators are polymethyl
methacrylate enclosures that
combine servo-controlled
convection heating with
supplemental O2
Provides temperature control
FiO2 – 40-50% @ flow of 8-
15 L/min
Variable performance
device
HYPERBARIC O2 THERAPY (HBOT)
DEFINITION
A mode of medical treatment wherein
the patient breathes 100% oxygen at a
pressure greater than one Atmosphere
Absolute (1 ATA)
1 ATA is equal to 760 mm Hg at sea level
PHYSIOLOGICAL EFFECTS OF HBO
Bubble reduction ( boyle’s law)
Hyperoxia of blood
Enhanced host immune function
Neovascularization
Vasoconstriction
INDICATIONS OF HBOT
ACUTE CONDITIONS CHRONIC CONDITIONS
Decompression sickness
Air embolism
Carbon monoxide
poisoning
Severe crush injuries
Thermal burns
Acute arterial
insufficiency
Clostridial gangrene
Necrotizing soft-tissue
infection
Ischemic skin graft or flap
Radiation necrosis
Diabetic wounds of lower
limbs
Refratory osteomyelitis
Actinomycosis (chronic
systemic abscesses)

METHODS OF ADMINISTRATION OF HBOT
PROBLEMS WITH HBOT
Barotrauma
Ear/ sinus trauma
Tympanic membrane rupture
Pneumothorax
Oxygen toxicity
Fire hazards
Clautrophobia
Sudden decompression

COMPLICATIONS OF OXYGEN
THERAPY

COMPLICATIONS OF OXYGEN THERAPY
1. Oxygen toxicity
2. Depression of ventilation
3. Retinopathy of Prematurity
4. Absorption atelectasis
5. Fire hazard
1. O2 TOXICITY
Primarily affects lung and CNS.
2 factors: PaO2 & exposure time
CNS O2 toxicity (Paul Bert effect)
occurs on breathing O2 at pressure > 1 atm
tremors, twitching, convulsions
PULMONARY OXYGEN TOXICITY
C/F
acute tracheobronchitis
Cough and substernal pain
ARDS like state
PULMONARY O2 TOXICITY (LORRAIN-SMITH
EFFECT)
Mechanism: High pO2 for a prolonged period of time
↓
intracellular generation of free radicals e.g.: superoxide,H2O2 , singlet oxygen
↓
react with cellular DNA, sulphydryl proteins &lipids↓
cytotoxicity↓
damages capillary endothelium,
↓

Interstitial edema
Thickened alveolar capillary membrane.
↓
Pulmonary fibrosis and hypertension

A VICIOUS CYCLE
HOW MUCH O2 IS SAFE?
100% - not more than 12hrs
80% - not more than 24hrs
60% - not more than 36hrs
Goal should be to use lowest possible
FiO2 compatible with adequate tissue
oxygenation
INDICATIONS FOR 70% - 100% OXYGEN
THERAPY
1. Resuscitation
2. Periods of acute cardiopulmonary
instability
3. Patient transport

2. DEPRESSION OF VENTILATION
Seen in COPD patients with chronic hypercapnia Mechanism
↑PaO2
suppresses peripheral V/Q mismatch
chemoreceptors
depresses ventilatory drive ↑ dead space/tidal volume ratio
↑PaCO2

3. RETINOPATHY OF PREMATURITY (ROP)
Premature or low-birth-weight infants who receive supplemental O2
Mechanism↑PaO2
↓retinal vasoconstriction
↓necrosis of blood vessels
↓new vessels formation
↓Hemorrhage → retinal detachment and
blindness
To minimize the risk of ROP - PaO2 below 80 mmHg

4. ABSORPTION ATELECTASIS100% O2
oxygennitrogen
PO2 =673
PCO2 = 40
PH2O = 47
A B
A – UNDERVENTILATED
B – NORMAL VENTILATED
DENITROGENATION ABSORPTION
ATELECTASIS
The “denitrogenation” absorption atelectasis
is because of collapse of underventilated
alveoli (which depends on nitrogen volume to
remain above critical volume )
↓
Increased physiological shunt

5. FIRE HAZARD
High FiO2 increases the risk of fire
Preventive measures
Lowest effective FiO2 should be used
Use of scavenging systems
Avoid use of outdated equipment such as
aluminium gas regulators
Fire prevention protocols should be followed
for hyperbaric O2 therapy