oxygen therapy
TRANSCRIPT

Dr SURENDRA
FNB-CCM
RTIICS KOLKATA

Oxygen is a colorless, odorless, tasteless gas that is
essential for the body to function properly and to survive.
Oxygen should be regarded as a drug. It is prescribed
to prevent/treat hypoxaemia, but not hypercapnia or
breathlessness. (Oxygen has not been shown to have
any effect on the sensation of breathlessness in non-
hypoxaemic patients.)
Oxygen saturation is considered as ‘‘the fifth vital
sign’’,
Oxygen therapy is the administration of oxygen
at a concentration greater than room air (
20.946%)
Oxygen may be necessary for life, but it doesn’t
prevent death.
there are no direct measurements of the oxygen
tension in tissues but indirect measures of tissue
oxygenation are used to guide aerobic support
The oxygenation of hemoglobin is evaluated by
the fraction of the hemoglobin in blood that is fully
saturated with O2. This is called the O2 saturation
(SO2) and can be measured using
spectrophotometry
Oxygen therapy is a key treatment in
respiratory care.
Used at cellular level as the final electron
acceptor in the electron transport chain in the
mitochondria of cell
the heart relies on oxygen to pump blood
at the alveolus the PAO2 is 100 mmHg (13.3
kPa).


The transfer of a gas across a membrane relies on
physical principles and is summarized by Fick’s
first law of diffusion:
O2 diffusion = K × A/T × P

Transport of oxygen to the cells can thus be
divided into six simple steps reliant only on the
laws of physics:
(1) convection of oxygen from the environment
into the body (ventilation);
(2) diffusion of oxygen into the blood (oxygen
uptake):
(3) reversible chemical bonding with haemoglobin;
(4) convective transport of oxygen to the tissues
(cardiac output):
(5) diffusion into the cellsand organelles;
(6) the redox state of the cell.
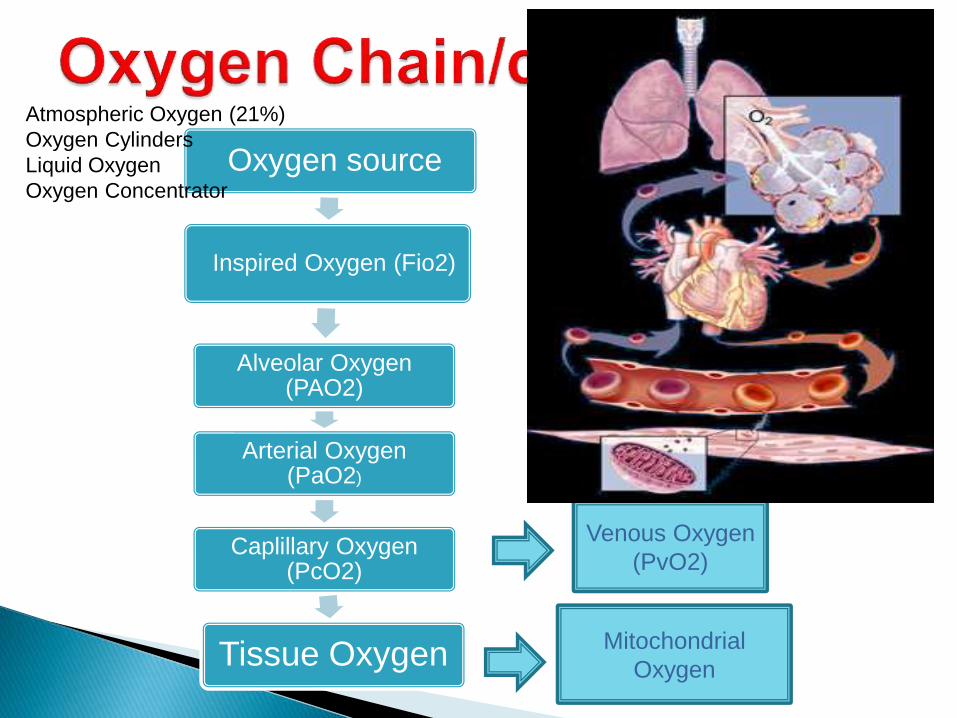
Oxygen source
Inspired Oxygen (Fio2)
Alveolar Oxygen (PAO2)
Arterial Oxygen (PaO2)
Caplillary Oxygen (PcO2)
Tissue Oxygen Mitochondrial
Oxygen
Venous Oxygen
(PvO2)
Atmospheric Oxygen (21%)
Oxygen Cylinders
Liquid Oxygen
Oxygen Concentrator

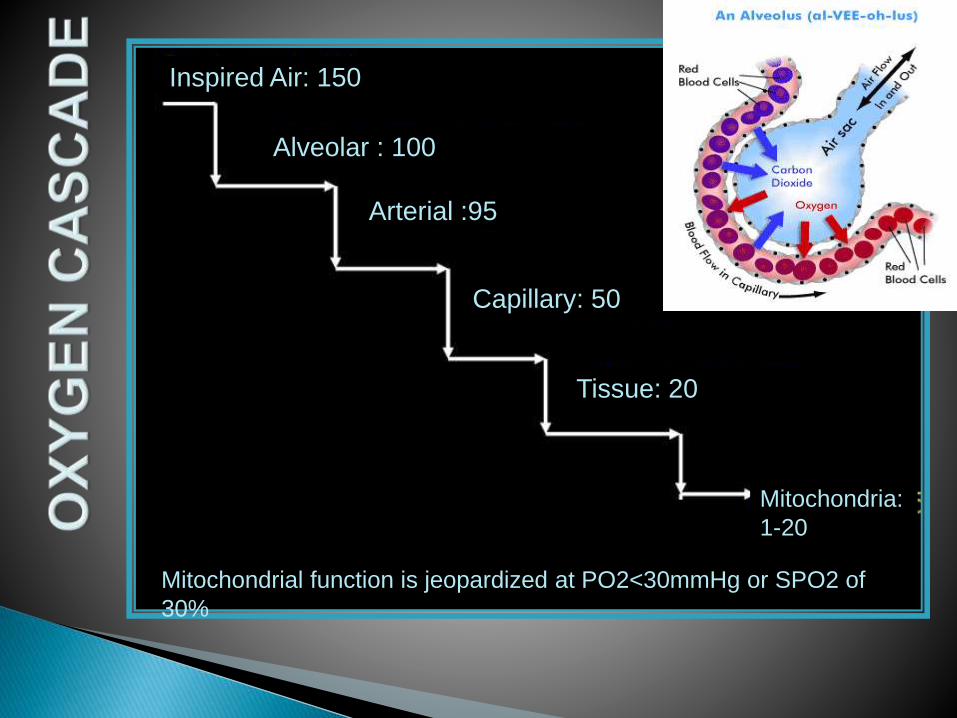
Inspired Air: 150
Alveolar : 100
Arterial :95
Capillary: 50
Tissue: 20
Mitochondria:
1-20
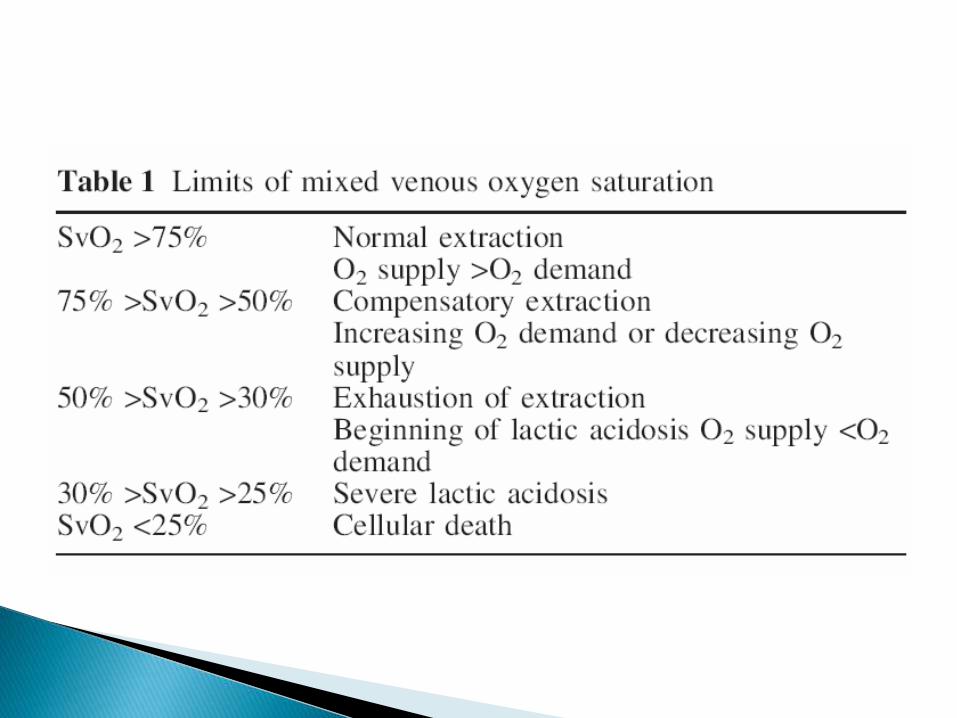
Mitochondrial function is jeopardized at PO2<30mmHg or SPO2 of
30%

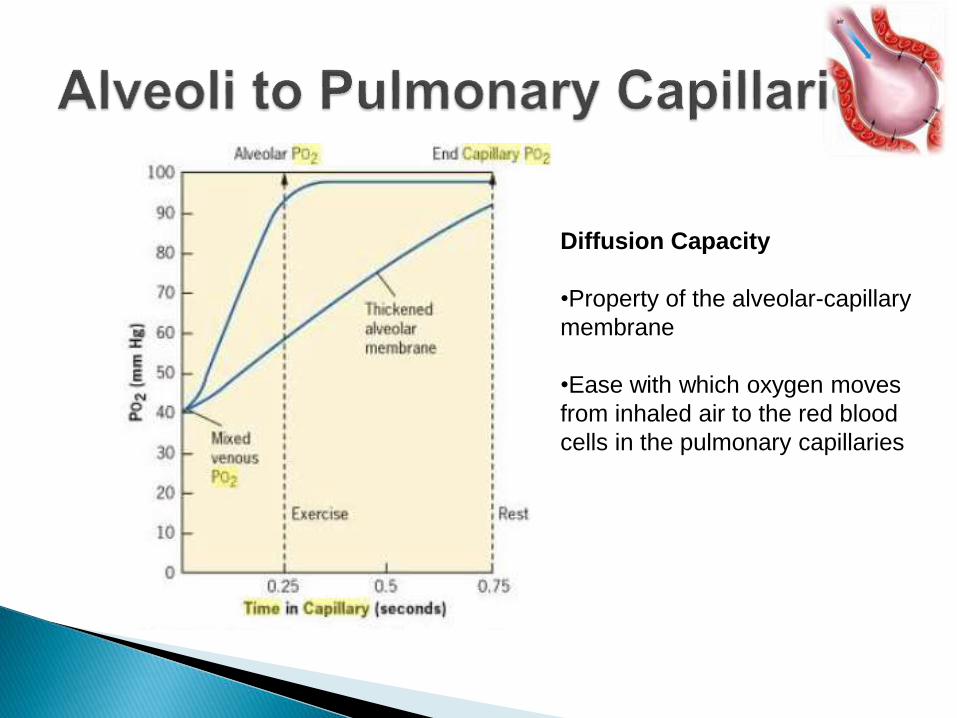
Diffusion Capacity
•Property of the alveolar-capillary
membrane
•Ease with which oxygen moves
from inhaled air to the red blood
cells in the pulmonary capillaries
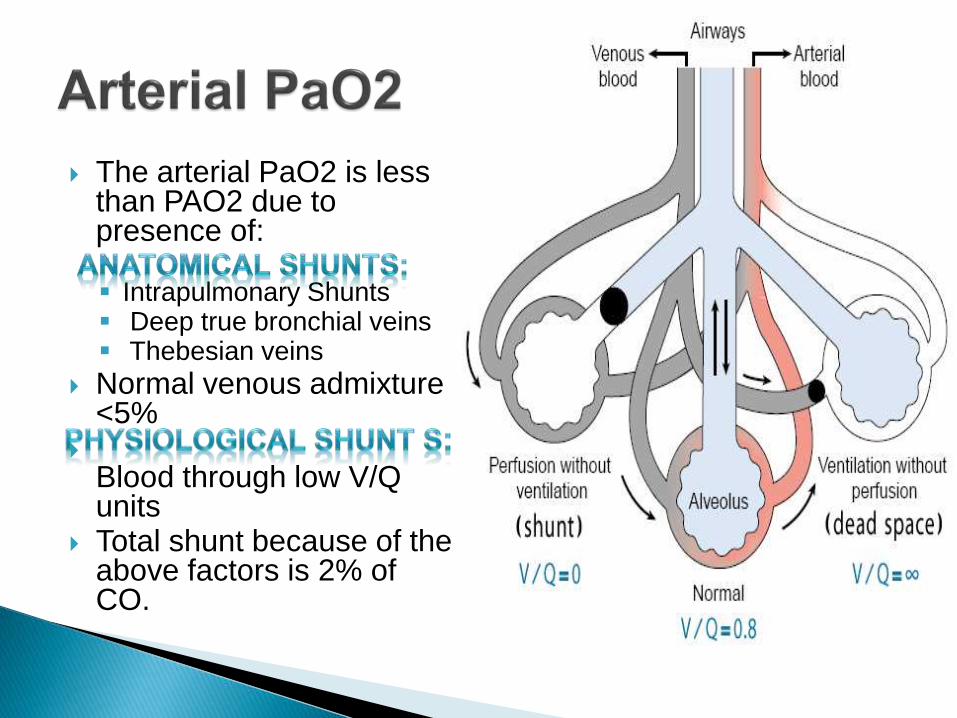
The arterial PaO2 is less than PAO2 due to presence of:
Intrapulmonary Shunts Deep true bronchial veins Thebesian veins
Normal venous admixture <5%
Blood through low V/Q units
Total shunt because of the above factors is 2% of CO.

Focal Hypoventilation
Shunt Effect
Wasted Perfusion
HYPOXEMIA
Hypoxemia without hypercarbia
(Type 1 RF)
Dead Space Effect
Wasted Ventilation
INCREASED WORK OF BREATHING
Minute Ventilation-
PaCO2 Disparity
( Type II RF )
V/Q <1
Low V/Q UnitsV/Q >1
High V/Q Units
V/Q=1.0V/Q=0 V/Q= infinity

Type I or Hypoxemic (PaO2 <60 at sea level): Failure of oxygen
exchange
Increased shunt fraction (Q S /QT )
Due to alveolar flooding
Hypoxemia refractory to supplemental oxygen.
Type II or Hypercapnic (PaCO2 >45): Failure to exchange or remove
CO2
Decreased alveolar minute ventilation (V A )
Often accompanied by hypoxemia that corrects with supplemental
oxygen
Type III Respiratory Failure: Perioperative RF
Type IV Respiratory Failure: Shock
Alveolar arterial oxygen difference P(A-a)O2
Normal is 5-15 mm Hg because oxygenated blood is
mixed with deoxygenated blood.
Affected by:
Age : Increases with age
FiO2: Increases with increasing FiO2.
Indicator of pulmonary parenchymal dysfunction.

Normal P/F > 400; Maximum P/F = 700
Relation between PaO2 and FiO2 is non linear and influenced by:
- Denitrogenation Absorption Atelectesis
-PEEP
Advantage: Simple - bypasses need to calculate PAO2
Disadvantage: Cannot distinguish between Type 1 and Type II RF
S/F = 64+ 0.84 X (P/F)

Thickened interface between air and blood:
Collagen deposition
Cellular infiltration
Reduced surface area for diffusion: Low V/Q due to partially collapsed alveoli
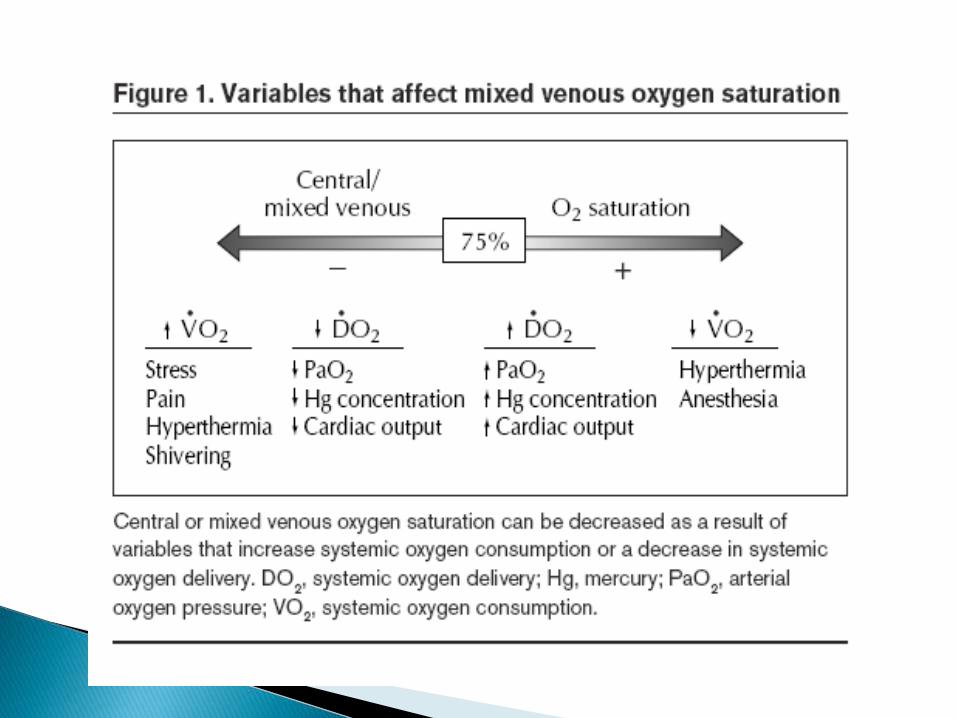
Decreased Delivery with Normal Oxygen Extraction:
Reduced Hb
Reduced SaO2
Reduced Blood Volume
Reduced CO
Normal delivery with increased O2 consumption or extraction

desolved : 0.003 X PaO2 ( Normal is 0.3-0.5ml )
At a normal body temperature (37°C), each increment in PO2 of 1 mm Hg will increase the concentration of dissolved O2 by 0.03 mL/L [0.003ml/dl]
Bound to Hb (19.5 ml) --% of heme binding sites saturated with oxygen is the Hb oxygen saturation %.
CaO2 = (1.34 X Hb X SaO2) + 0.003 X PaO2
Eg at 100% SaO2, Hb 15g%, PaO2 120 mm Hg
CaO2= (1.34 X 15 X 100/100)+(0.003 X 120)
=20.46ml
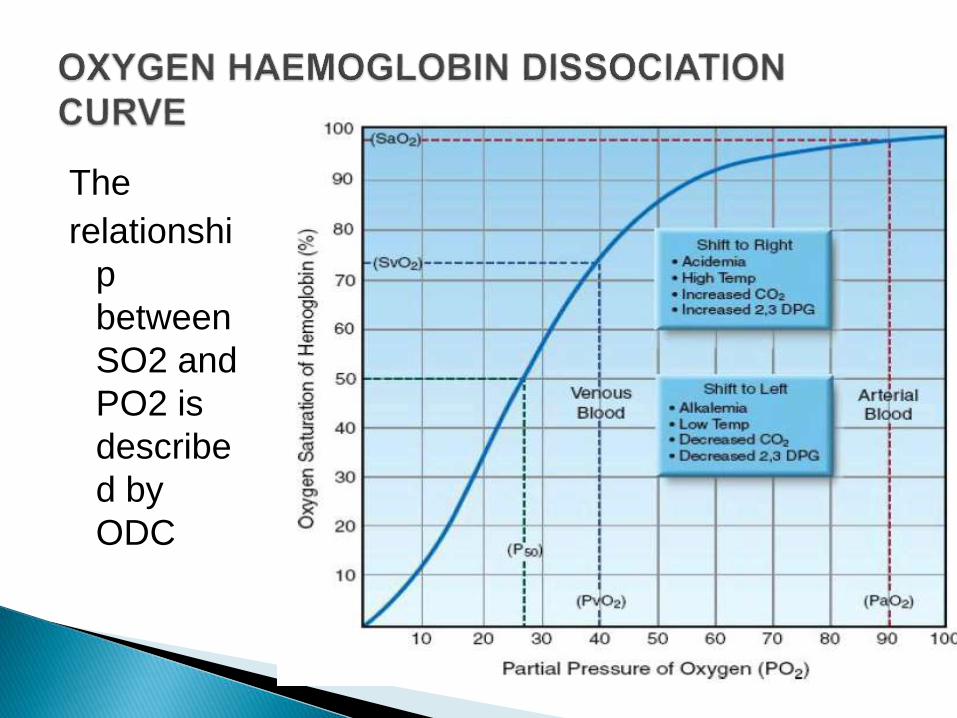
The
relationshi
p
between
SO2 and
PO2 is
describe
d by
ODC

Depends on oxygen content and cardiac output
= CO X CaO2
= 5000 X 20/100
= 1000ml/min
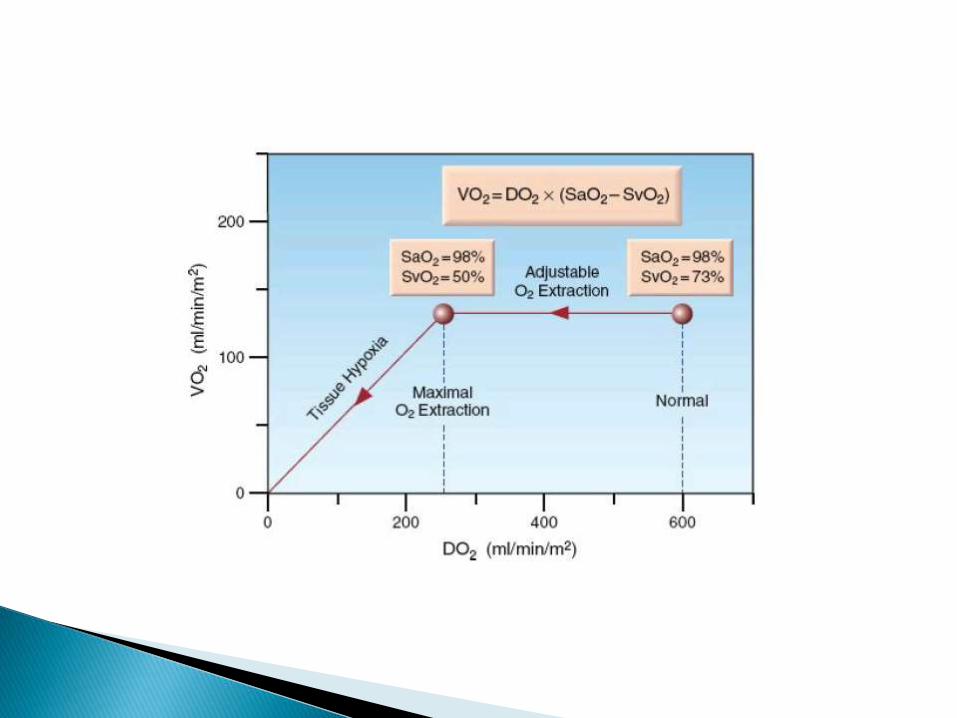
: Oxygen consumption by tissue per min.
250ml/min at rest
: Oxygen Extraction Ratio
VO2/DO2 = 0.25 (Normal range is 0.22-0.32)
Indicates balance b/w delivery and uptake
Low Values: Flow Maldistribution
Metabolic Poison
High Values: Compensatory increase in extraction for reduced
delivery.
Since oxygen is not stored in tissues, the VO2 is also a
global measure of the oxygen consumption of
metabolizing tissues
This equation is a modified version of the Fick equation
for cardiac output (CO = VO2/CaO2 –CvO2); using
this equation to calculate the VO2 is called the
reverse Fick method
the VO2 that is calculated from the modified Fick
equation must change by at least 18% for the change
to be considered significant.
The calculated VO2 from the modified Fick equation is not the whole body VO2 because it does not include the O2 consumption of the lungs. Normally, the VO2 of the lungs accounts for less than 5% of the whole body VO2 , but it can make up 20% of the whole body VO2 when there is inflammation in the lungs (which is common in ICU patients).
The whole body VO2 is measured by monitoring the O2 concentration in inhaled and exhaled gas-- needs an oxygen analyzer
it records the VO2 as the product of minute ventilation (VE) and the fractional concentration of O2 in inhaled and exhaled gas (FIO2 and FEO2).

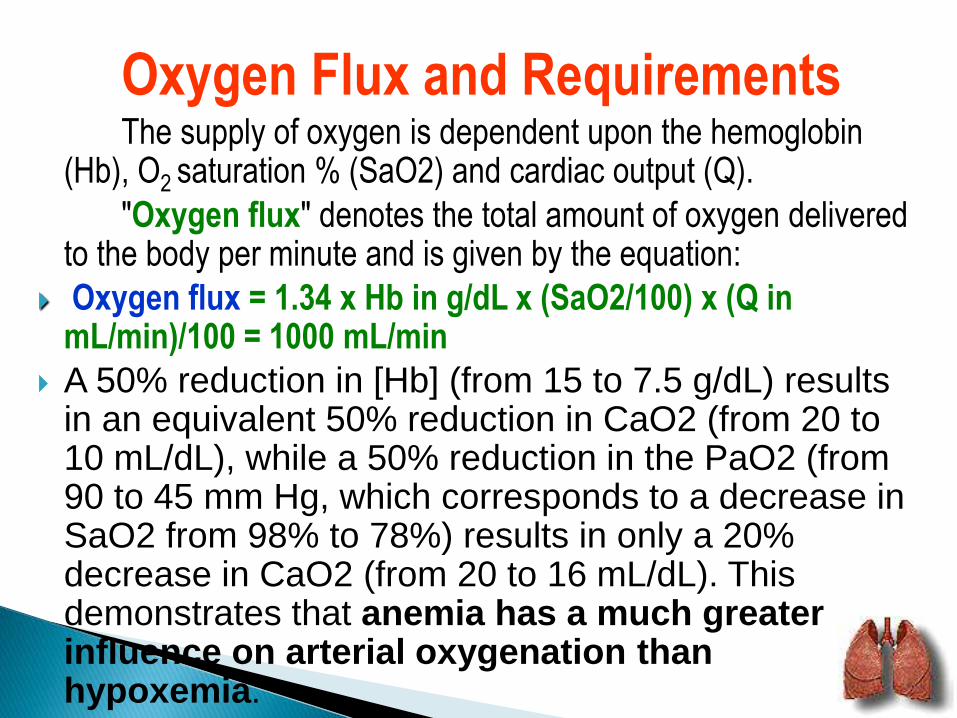
Oxygen Flux and RequirementsThe supply of oxygen is dependent upon the hemoglobin
(Hb), O2 saturation % (SaO2) and cardiac output (Q).
"Oxygen flux" denotes the total amount of oxygen delivered to the body per minute and is given by the equation:
Oxygen flux = 1.34 x Hb in g/dL x (SaO2/100) x (Q in mL/min)/100 = 1000 mL/min
A 50% reduction in [Hb] (from 15 to 7.5 g/dL) results in an equivalent 50% reduction in CaO2 (from 20 to 10 mL/dL), while a 50% reduction in the PaO2 (from 90 to 45 mm Hg, which corresponds to a decrease in SaO2 from 98% to 78%) results in only a 20% decrease in CaO2 (from 20 to 16 mL/dL). This demonstrates that anemia has a much greater influence on arterial oxygenation than hypoxemia.
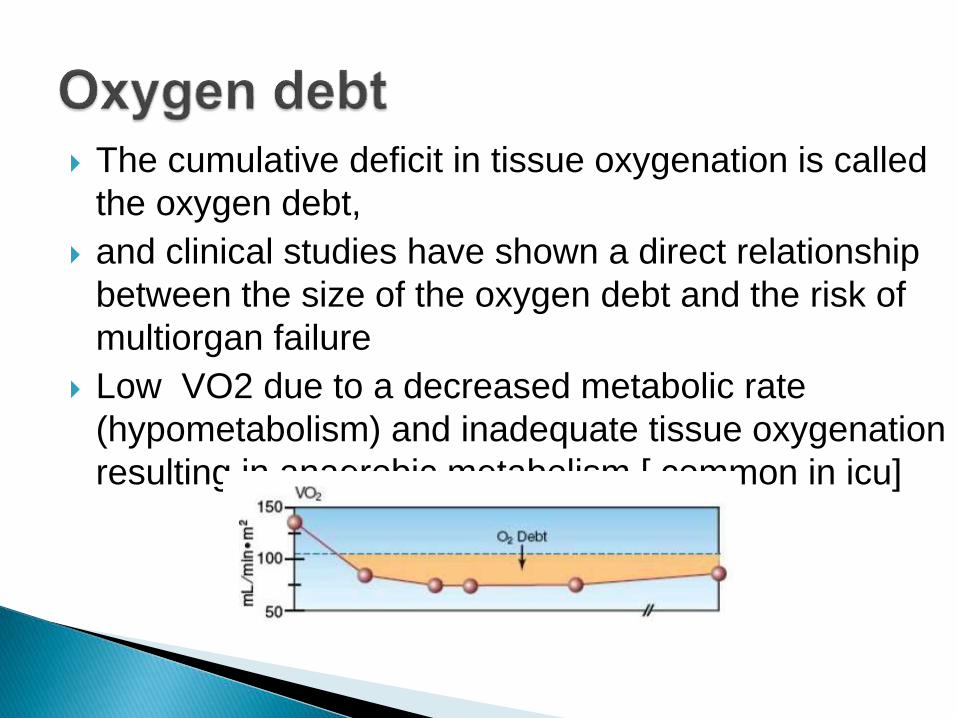
The cumulative deficit in tissue oxygenation is called
the oxygen debt,
and clinical studies have shown a direct relationship
between the size of the oxygen debt and the risk of
multiorgan failure
Low VO2 due to a decreased metabolic rate
(hypometabolism) and inadequate tissue oxygenation
resulting in anaerobic metabolism.[ common in icu]

Breathing pattern regular and at normal
rate.
pink color in nail beds, lips, conjunctiva
of eyes.
No confusion, disorientation, difficulty
with cognition.
Arterial oxygen concentration or
hemoglobin
Oxygen saturation within normal limits.

Date and time oxygen started.
Method of delivery.
Oxygen concentration and flow rate.
Patient observation.
Add oronasal care to the nursing care
plan
Need is determined by measurement of inadequate oxygen
tensions and/or saturations, by invasive or noninvasive
methods, and/or the presence of clinical indicators as
previously described.
Arterial blood gases
Pulse oximetry
Clinical presentation

Documented hypoxemia: Pa02 <60 mm Hg or Sa02 <90%
An acute care situation in which hypoxemia is suspected &
substantiation of hypoxemia is required within an appropriate period
of time following initiation of therapy.
Severe trauma
Acute myocardial infarction
Short-term therapy (e.g., postanesthesia recovery)

Should be determined through evaluation of the patient
(clinical assessment and blood gas result)
In general the indication are:-
1. Hypoxemia/hypoxia
2. Excessive work of breathing
3. Excessive myocardial work
4. Improvement of oxygenation in patient with decreased
O2 carrying capacity ( anaemia)
5. Promotion of absorption of air in the body cavity

Goal directed approach
- post operative (thoracic/abdominal
surgery)
- post extubation
- conscious state/coughing
- redistribution of fluid
- positioning
Three clinical goals of O2 therapy
1. Treat hypoxemia
2. Decrease work of breathing (WOB)
3. Decrease myocardial Work
FACTORS THAT DETERMINE
WHICH SYSTEM TO USE
1. Patient comfort / acceptance by the Pt
2. The level of FiO2 that is needed
3. The requirement that the FiO2 be
controlled within a certain range
4. The level of humidification and /or
nebulization
5. Minimal resistance to breathing
6. Efficient & economical use of oxygen

Low Flow Devices [Patient's inspiratory flow > flow delivered by the
device]
Nasal cannula Nasal catheter
Transtracheal catheter
Reservoir[Reserve volume (flow x time) ≥
patient's tidal volume ,, Fixed flow devices if RV > Inspiratory flow]
Simple mask
Partial rebreathing mask Nonbreathing mask
High Flow Devices[The High-flow system always exceeds
the patient's flow ,Provide fixed FIO2 ]
Air-entrainment mask Air-entrainment nebulizer T-piece with a venturi device
Breathing circuits with reservoir bags
Enclosure
Oxyhood Tent Isolette

EQUIPMENT FLOW FIO2 SPECIAL NOTES
NASAL CANNULA 1 - 6 L/M .24 – 44 6 L/M MAX.
SIMPLE O2 MASK 6 - 10 L/M .35 – 55 USE 5 L/M (WITHOUT BAG) MINIMUM
RESERVOIR MASK 10-15 L/M .60 -80 (MASK WITH BAG) (BAG TO NOT
COLLAPSE)
VENTI MASK 3 L/M .24, 26, 31, READ ENCLOSED6 L/M .35, .40, .50 INSTRUCTIONS
NEBULIZER 8 L/M OR > .28, .30, .35 MIST MUST BE .40, .50, 70 VISIBLE
*** SHOWS THAT FIO2 VARIES WITH DIFFERENTF, VT, INSPIRATORY FLOW RATES.

Partial Rebreathing System Non Rebreathing System

.


Flow: Varies
FiO2: 24%-60%
Advantages: Easy to apply;
disposable,
inexpensive;
stable,
precise Fio2
Disadvantages: Limited to adult use,
Use: Patients in unstable condition who need precise Fio2.

Flow: 10-15 L/min input,
Should provide output flow of atleast 60 lit/min
FiO2: 28%-100%
Advantages: Provide temperature control and humidification
Disadvantage: FiO2<0.28 and >0.40 not ensured
FiO2 varies with back pressure
High infection risk
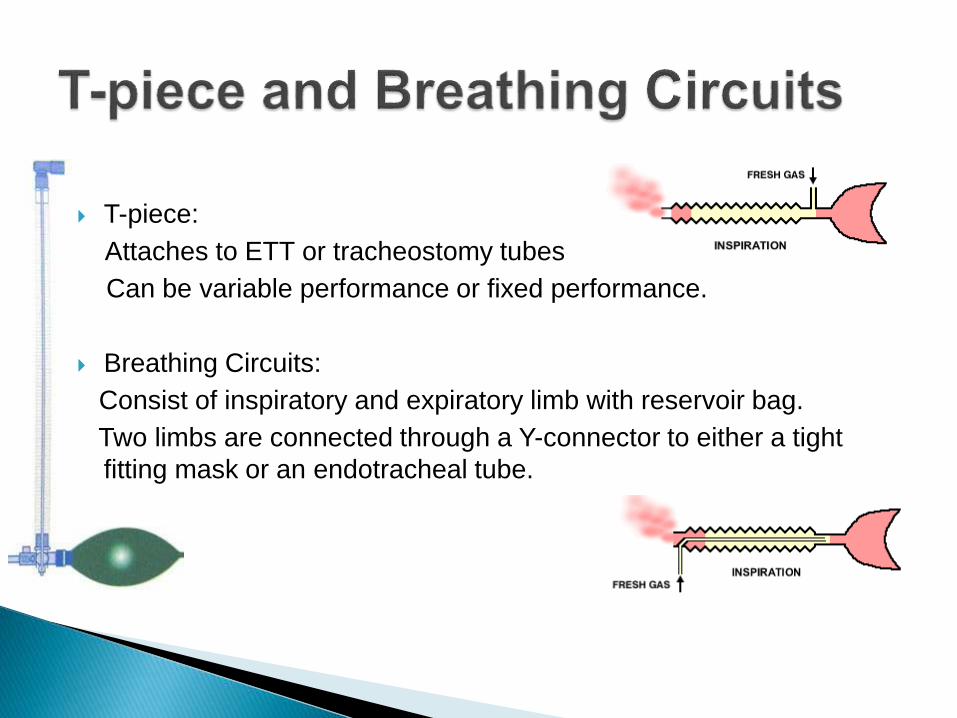
T-piece:
Attaches to ETT or tracheostomy tubes
Can be variable performance or fixed performance.
Breathing Circuits:
Consist of inspiratory and expiratory limb with reservoir bag.
Two limbs are connected through a Y-connector to either a tight
fitting mask or an endotracheal tube.
Weaning should be considered when the patient becomes comfortable, his underlying disease is stabilized, BP, pulse rate, respiratory rate, skin color, and oxymetry are within normal range.
weaning can be gradually attempted by discontinuing oxygen or lowering its concentration for a fixed period for e.g., 30 min. and reevaluating the clinical parameters and SpO2 periodically.
Patients with chronic respiratory disease may require oxygen at lower concentrations for prolonged periods.

Monitoring oxygen therapy Oxygen therapy should be given continuously and should
not be stopped abruptly until the patient has recovered, since sudden discontinuation can wash-out small body stores of oxygen resulting in fall of alveolar oxygen tension.
The dose of oxygen should be calculated carefully.
Partial pressure of oxygen can be measured in the arterial blood.
Complete saturation of hemoglobin in arterial blood should not be attempted.
Arterial PO2 of 60 mmHg can provide 90% saturation of arterial blood, but if acidosis is present, PaO2 more than 80 mmHg is required.

In a patient with respiratory failure, anaemia should be corrected for proper oxygen transport to the tissue.
A small increment in arterial oxygen tension results in a significant rise in the saturation of hemoglobin.
Under normal situations, no additional benefit is secured by raising PaO2 level to greater than 60 to 80 mmHg.
An increase of 1% oxygen concentration elevates oxygen tension by 7 mmHg.
Measurement of arterial blood gases repeatedly is difficult so a simple and non-invasive technique like pulse oximetermay be used to assess oxygen therapy.
Rivers, Emmanual
◦ NEJM 2001; 345: 1368-1377
◦ Early goal-directed therapy in severe sepsis
and septic shock during the first 6 hours after
presentation
◦ Significant reductions in mortality, morbidity in
experimental group that optimized oxygen
delivery and consumption variables



Oxygen toxicity is cellular injury of the lung parenchyma and airway epithelium due to release of cytoxicfree oxygen radicals.
There is no exact threshold at which O2 toxicity occurs, however signs of gas exchange abnormalities occur within 24-48 hours if on 100% oxygen. Atelectasis leading to drop in PO2, decreased lung compliance, infiltrates on x-ray.
Breathing FiO2 up to 50 % for 2-7 days usually does NOT result in toxicity.
12/10/2014 59

Inhibition of Hypoxic pulmonary vasoconstriction
Increased SVR with reduced coronary, cerebral and renal blood flows. [cause vasoconstriction] reducing DO2 when an increase demand, may worsen outcome from CVA and AMI..
Reduced cardiac output & haemodynamic instability.
Increased production of reactive oxygen species.
Paradoxical decrease in O2 consumption due to maldistribution of blood flow due to peripheral shunts which open up to protect the
vital organs from non-physiological effects of hyperoxia.

CO2 Narcosis: In COPD patients, high FiO2 removes the hypoxic drive & causes hypoventilation and narcosis.
Denitrogenation Adsorption AtelectasisFire ( airway fires)
Mucosal damage due to lack of humidity
O2 Toxicity:
Respiratory: ARDS Like syndrome
LUNG TOXICITY (LORRIANE SMITH EFFECT)
Neurological: Seizures (Hyperbaric)
CNS TOXICITY (PAUL BERT EFFECT)
Children: Bronchopulmonary dysplasia
Retrolental fibroplasia
Hypoventilation and Carbon Dioxide
Narcosis
- the increased PO2 decreased and eliminates the
hypoxic drive ( esp. in pt. with chronic CO2 retention
)
- Under this circumstances O2 must be given at low
concentration <30% Ventilatory drive:
Absorption Atelectasis
- Nitrogen a relatively insoluble and exists 80% by
volume of the alveolar gas.N2 assists in maintaining
alveolar stability.O2 therapy replaced N2. Once O2
absorb into the blood the alveolar will collapse esp. in
alveolar distal to the obstruction.
Pulmonary Oxygen Toxicity- The exposure of the high O2 and for prolonged
period
can lead to parenchymal changes
- In general FiO2 > 50% for prolonged period shows increased O2 toxicity
- Pulmonary changes mimic ARDS (Exudativechanges and proliferative changes.)
Sx –cough, burning discomfort, nausea and vomiting,
headache, malaise and etc
Haldane effect: increasing FiO2 decreases the CO2
buffering capacity of haemoglobin, thus potentially
leading to an increase in PaCO2 and acidaemia.
Higher density of oxygen compared with air:
increased viscosity increases the work of breathing in
high conc.
Fire
O2 support combustion
Do not smoke while receiving O2 therapy

Patient on Chemotherapy
Patient on chemotherapy especially
bleomycin will develop pulmonary fibrosis
if get excessive O2 therapy

Carban monoxide
poisoning[100% O2
at 3 atmp]
Tt of cluster
headache, reduction
in oxidative stress in
colonic surgery and
prevention of
desaturation during
Endoscopy.
The use of
hyperoxia to treat
postoperative
nausea and vomiting
and prevent
postoperative
wound infections
lacks high-quality
evidence
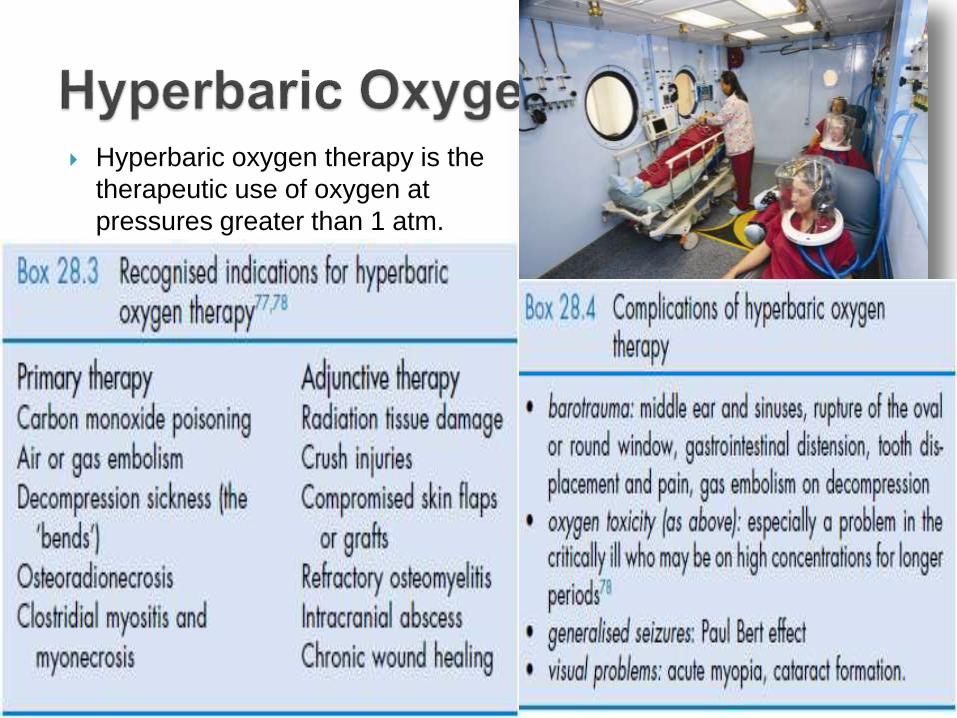
Hyperbaric oxygen therapy is the
therapeutic use of oxygen at
pressures greater than 1 atm.
Indications:
hypoxemia should be verified with pulse oximetry and /or ABG’s when situation more stable.
Oxygen is a drug and should be administered keeping
following things in mind: mode of administration, flow
rate, FiO2 (venturi), treatment goal, monitoring, when to
stop.
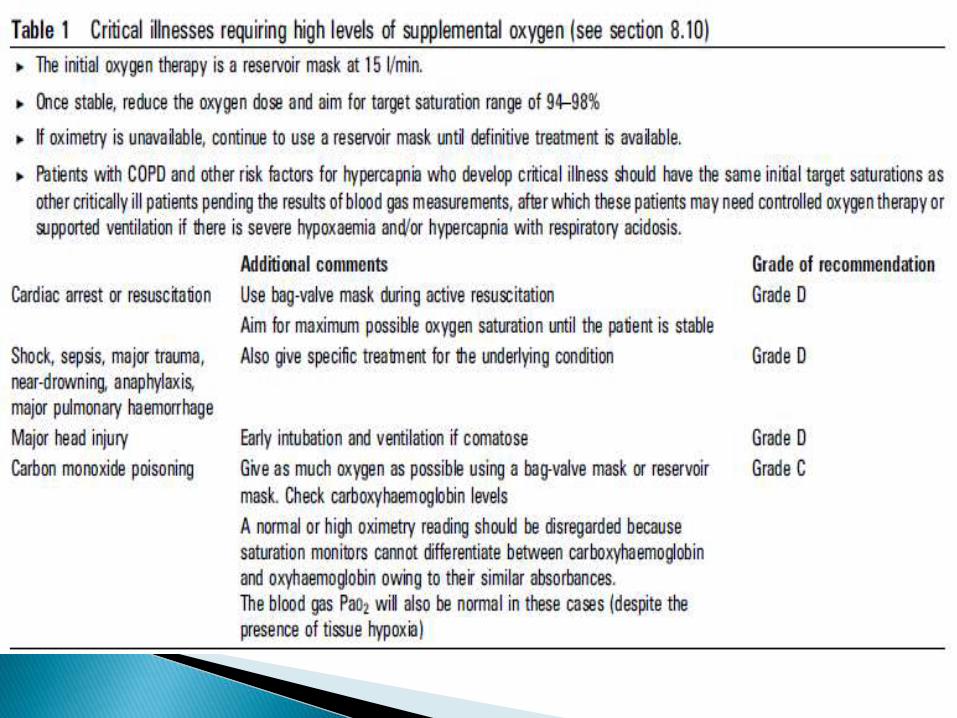
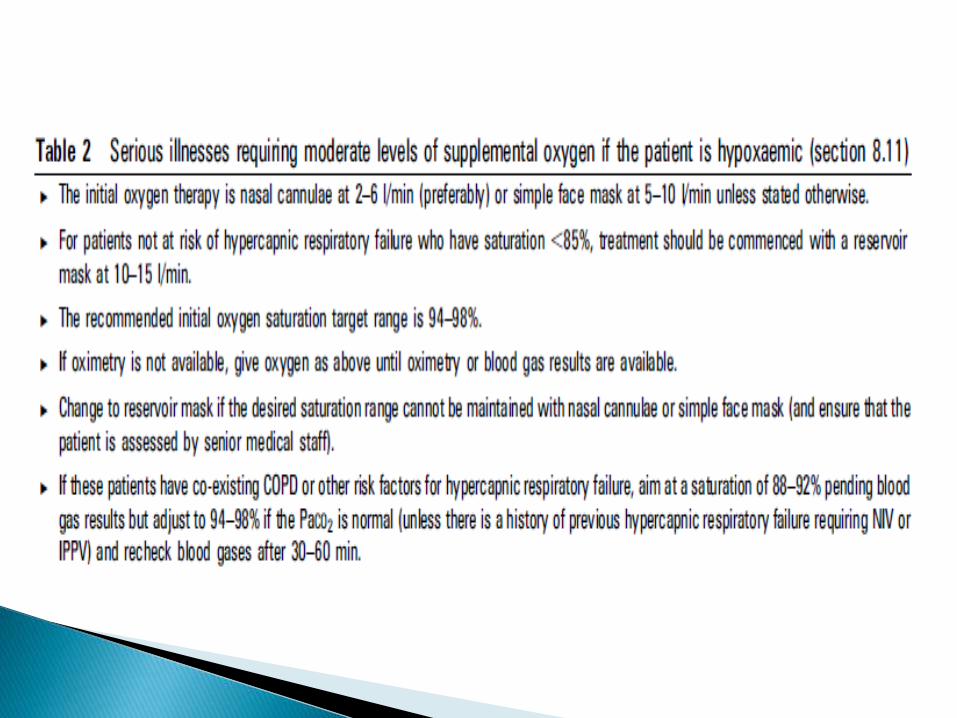
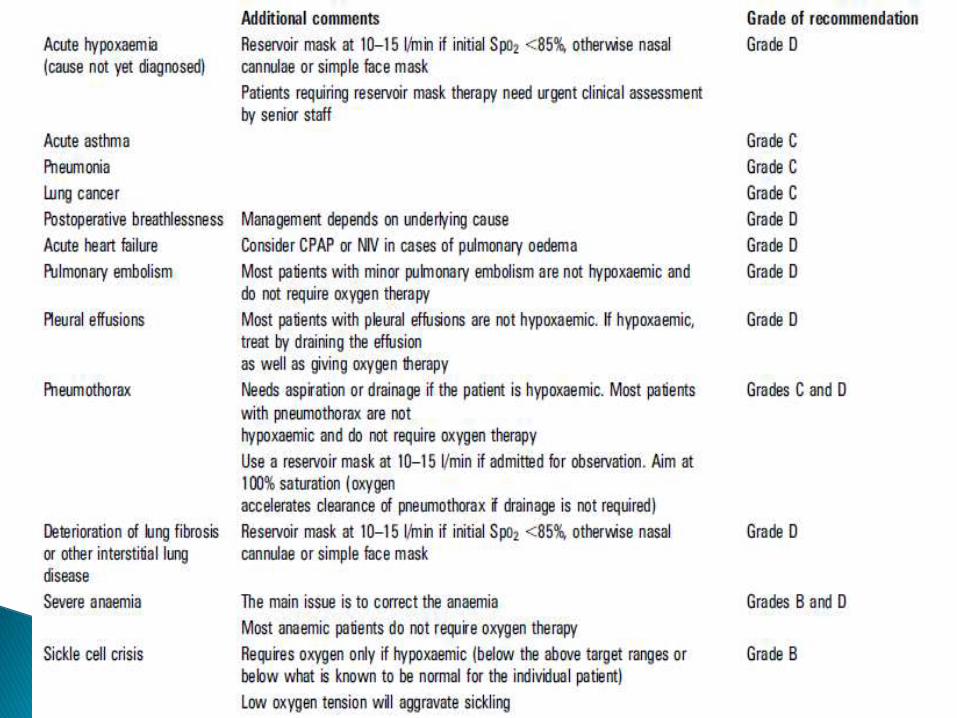
Oxygen should be prescribed to achieve a target
saturation of 94–98% for most acutely ill patients or 88–
92% for those at risk of hypercapnic respiratory failure
as very high levels will not offer any clinical advantage in
most conditions.
The PaO2 measurement is useful for evaluating gas
exchange in the lungs, not for evaluating the
oxygenation of blood.
Nursing Guidelines Oxygen updated Jan 2013Nottingham University Hospitals NHS Trust
Thorax 2008;63(Suppl VI) BTS guideline for emergency oxygen use
in adult patients
Oh,z manual
The icu book
