paediatric antiretroviral formulations – present and future
TRANSCRIPT
SEPTEMBER 2021 I 1
Leader in digital CPD for Southern African healthcare professionals
HIV and AIDSEarn 3 free CEUs
© 2021 deNovo Medica
Dr Leon Levin Senior Paediatric AdvisorRight to Care Johannesburg
Clinical update
Paediatric antiretroviral formulations – present and future
Learning objectivesYou will learn:
• The benefits and limitations of currently available paediatric antiretroviral formulations
• The benefits and limitations of pipeline paediatric formulations that will be considered for future use.
Acronyms and abbreviationsABC: abacavir3TC: lamivudineLPV: lopinavirr: ritonavir used as booster doseRTV: ritonavirATV: atazanavir DRV: darunavirTAF: tenofovir alafenamide
TDF: tenofovir disoproxil fumarate COBI: cobicistatFTC: emtricitabineDTG: dolutegravirRPV: rilpivirineAZT: zidovudineNRTI: nucleoside reverse transcriptase inhibitorPI: protease inhibitor
IntroductionRapid and dramatic change is currently occurring in the treatment of HIV in children. In 2021, the National Department of Health (NDoH) and the Southern African HIV Clinicians Society updated their antiretroviral (ARV) drug dosing chart for children in order to accommodate newly available paediatric ARV formulations. Yet other new ARV formulations will soon be available and the paediatric ARV drug dosing chart will therefore be updated again for 2022. The current 2021 dosing chart can be accessed at https://sahivsoc.org/Files/PaedDosingChart_2021.pdf.1 Dr Leon Levin discusses the benefits and limitations of the currently available new paediatric ARV formulations, as well as the pipeline formulations that will be considered for future use.
This report was made possible by an unrestricted educational grant from Cipla. The content of the report is independent of the sponsor.
© s
hutt
erst
ock/
1428
3777
20
Reviewed by:
2 I SEPTEMBER 2021
Clinical update: Paediatric antiretroviral formulations – present and future
The ABC/3TC dispersible tablet can be swallowed whole or dissolved in 10ml of water
The ABC/3TC combination may improve adherence due to a lower pill burden, i.e. a fewer number of tablets that need to be swallowed
Currently available new paediatric ARV formulations
Abacavir (ABC)/lamivudine (3TC) 120/60mg dispersible scored tabletsThis is a new formulation of older well-known drugs that have been used as the backbone of first-line paediatric ARV regi-mens, from young babies to teenagers. The ABC/3TC dispersible tablet can be swallowed whole or dissolved in 10ml of water. If dis-solved, the container should be rinsed out with another 10ml of water that is given to the child. It can be used in children weighing from 3kg to 24.9kg (Table 1) and at 25kg, the adult ABC/3TC (600/300mg) combination is then given. If the child weighing ≥25kg is not able to swallow tablets whole, the ABC/3TC 600/300mg tablet can be crushed, although it is not dispersible. Alternatively, four of the ABC/3TC 120/60mg dispersible tablets can be given.
As part of the first-line ARV regimen for chil-dren, the ABC/3TC 120/60mg combination could replace the need for:• ABC 20mg/ml oral solution• ABC 60mg dispersible tablets• ABC 300mg tablets• 3TC 10mg/ml oral solution (there may be a
small role for this formulation in neonates)• 3TC 150mg tablets.
Further benefits of this formulation are that the patients (and carers) do not need to transport and store as many bottles of oral solution or tablets; the ABC/3TC combina-tion may also improve adherence due to a
lower pill burden, i.e. a fewer number of tablets that need to be swallowed, and the fact that it is given once daily. Also of importance, this dispersible combination tablet negates the need for drawing oral solutions out with a syringe, which some patients and/or carers struggle to do.
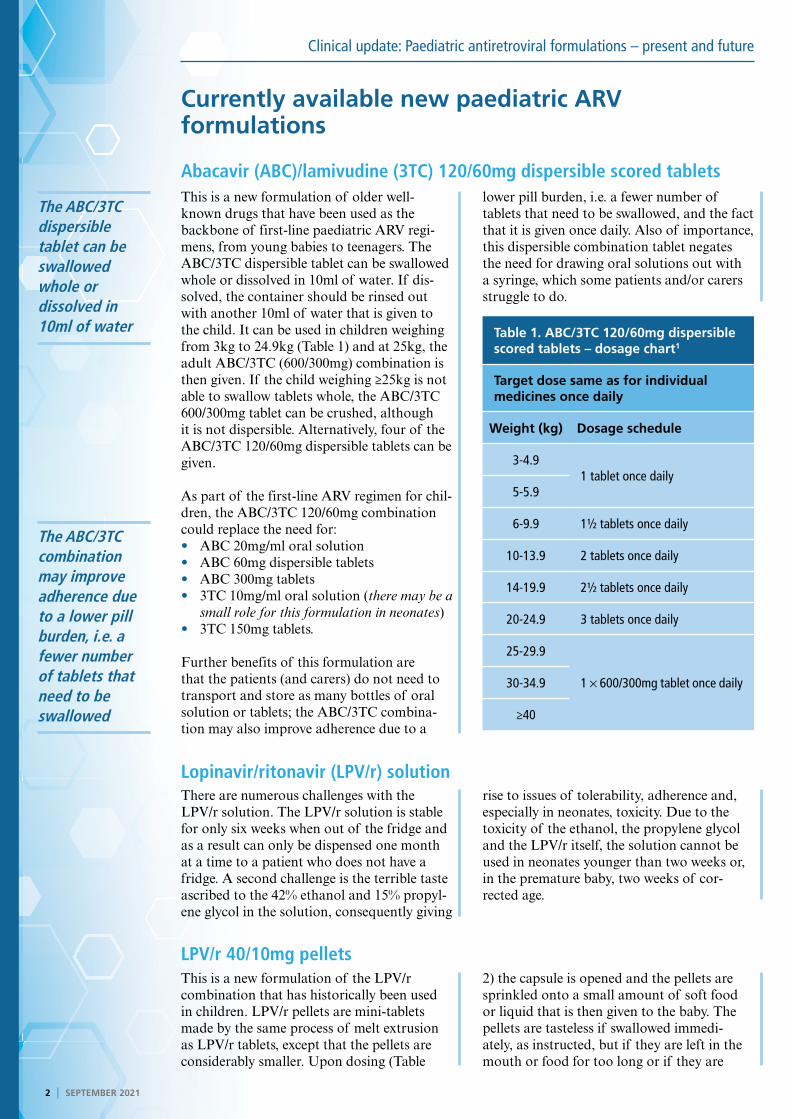
Table 1. ABC/3TC 120/60mg dispersible scored tablets – dosage chart1
Target dose same as for individual medicines once daily
Weight (kg) Dosage schedule
3-4.91 tablet once daily
5-5.9
6-9.9 1½ tablets once daily
10-13.9 2 tablets once daily
14-19.9 2½ tablets once daily
20-24.9 3 tablets once daily
25-29.9
1 × 600/300mg tablet once daily30-34.9
≥40
Lopinavir/ritonavir (LPV/r) solutionThere are numerous challenges with the LPV/r solution. The LPV/r solution is stable for only six weeks when out of the fridge and as a result can only be dispensed one month at a time to a patient who does not have a fridge. A second challenge is the terrible taste ascribed to the 42% ethanol and 15% propyl-ene glycol in the solution, consequently giving
rise to issues of tolerability, adherence and, especially in neonates, toxicity. Due to the toxicity of the ethanol, the propylene glycol and the LPV/r itself, the solution cannot be used in neonates younger than two weeks or, in the premature baby, two weeks of cor-rected age.
LPV/r 40/10mg pelletsThis is a new formulation of the LPV/r combination that has historically been used in children. LPV/r pellets are mini-tablets made by the same process of melt extrusion as LPV/r tablets, except that the pellets are considerably smaller. Upon dosing (Table
2) the capsule is opened and the pellets are sprinkled onto a small amount of soft food or liquid that is then given to the baby. The pellets are tasteless if swallowed immedi-ately, as instructed, but if they are left in the mouth or food for too long or if they are
SEPTEMBER 2021 I 3
Clinical update: Paediatric antiretroviral formulations – present and future
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
LPV/r pellets are slightly better tolerated than the LPV/r solution
The child with a high viral load while taking the LPV/r solution is also invariably not tolerating the solution and therefore LPV/r pellets should also be offered to this child
chewed, the unpleasant taste starts to emerge. LPV/r pellets are slightly better tolerated than the LPV/r solution, but this is depend-ent on technique; a step-wise method of administration is explained in Figure 1 and an excellent video can be accessed at https://we.tl/t-bpxoKeTHte. In infants younger than six months, the pellets need to be sprinkled onto a spoon of milk or placed on the tongue before drinking, which makes administration a challenge. There is also a theoretical risk of aspirating. Therefore in the state sector, LPV/r pellets are recommended for infants older than six months who cannot tolerate the LPV/r solution. Those who qualify as not tolerating the LPV/r solution include the patient who spits out the medicine or refuses it and those who are vomiting. Dr Levin is of the view that the child with a high viral load while taking the LPV/r solution is also invariably not tolerating the solution and that LPV/r pellets should therefore also be offered to this child. LPV/r has a high resistance bar-rier and the viral load should be adequately suppressed; if this is not the case, it is invari-ably due to lack of adherence.
Table 2. LPV/r 40/10mg oral pellets – dosage chart1
Target dose 300/75mg/m2/dose LPV/r twice daily
Weight (kg) Dosage schedule
3-4.92 capsules twice daily
5-5.9
6-9.9 3 capsules twice daily
10-13.9 4 capsules twice daily
14-19.9 5 capsules twice daily
20-24.9 6 capsules twice daily
25-29.9 7 capsules twice daily
≥30 10 capsules twice daily
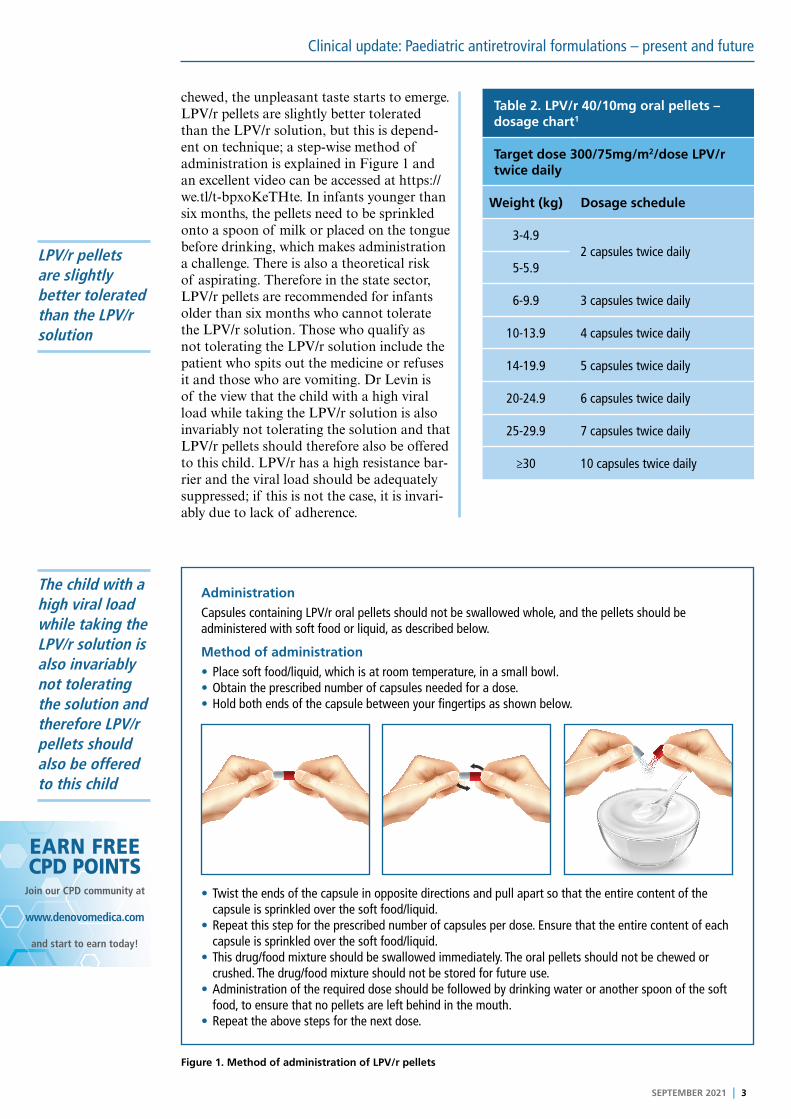
Figure 1. Method of administration of LPV/r pellets
Administration
Capsules containing LPV/r oral pellets should not be swallowed whole, and the pellets should be administered with soft food or liquid, as described below.
Method of administration
• Place soft food/liquid, which is at room temperature, in a small bowl.• Obtain the prescribed number of capsules needed for a dose.• Hold both ends of the capsule between your fingertips as shown below.
• Twist the ends of the capsule in opposite directions and pull apart so that the entire content of the capsule is sprinkled over the soft food/liquid.
• Repeat this step for the prescribed number of capsules per dose. Ensure that the entire content of each capsule is sprinkled over the soft food/liquid.
• This drug/food mixture should be swallowed immediately. The oral pellets should not be chewed or crushed. The drug/food mixture should not be stored for future use.
• Administration of the required dose should be followed by drinking water or another spoon of the soft food, to ensure that no pellets are left behind in the mouth.
• Repeat the above steps for the next dose.
4 I SEPTEMBER 2021
Clinical update: Paediatric antiretroviral formulations – present and future
The RTV solution has now been discontinued and only the RTV heat-stable powder is available
Barriers to uptake of LPV/r pellets in the state sectorBarriers to the uptake of LPV/r pellets in the state sector include:• Lack of awareness• Difficulty of use• Technique• Previously they needed to be prescribed by
a doctor, but now this has changed• In some provinces, a motivation has to be
signed by a doctor as a prerequisite for access• Cost.
In mitigation of these barriers, a publicity and education campaign has been undertaken and nurses are now allowed to prescribe LPV/r pellets. However, the motivation forms are still problematic in some areas.
Ritonavir (RTV) 100mg heat-stable powderPaediatric use of RTV solution has tradition-ally been in the context of super-boosting LPV/r when used with rifampicin for the treatment of tuberculosis, as well as being used as a booster with atazanavir (ATV) and darunavir (DRV). Problems with the RTV solution are the taste, which Dr Levin indi-cates is even worse than that of the LPV/r solution, and that it has a shelf life of only six months. The six-month shelf life has proved most problematic; often the solution will have expired by the time it reaches the clinic and so clinics do not order it; instead they prefer to double the LPV/r dose for patients using rifampicin. In this case, low levels of LPV may occur due to drug interactions with the rifampicin, further to which LPV resistance emerges rapidly. The RTV solution has now been discontinued and only the RTV heat-stable powder is available.
Advantages of RTV heat-stable powder are the shelf life of 36 months and that there are no cold chain storage requirements. Each sachet contains 100mg of RTV, which is the standard dose for boosting protease inhibi-tors (PIs) in adults. A full sachet of powder (100mg) can be sprinkled over soft food or mixed with liquid. However, if quantities less than 100mg are required, there is a compli-cated 11-step process involving adding one sachet to 9.4ml of liquid to give a 10mg/ml solution. For this reason it is preferable to only use multiples of 100mg as a dose (Table 3). The RTV powder does not contain alcohol or propylene glycol. Disadvantages of the
RTV powder are the bitter aftertaste, which may be lessened if peanut butter, chocolate spread or blackcurrant syrup are taken imme-diately after administration. The RTV powder must be used within two hours of mixing with food or liquid.
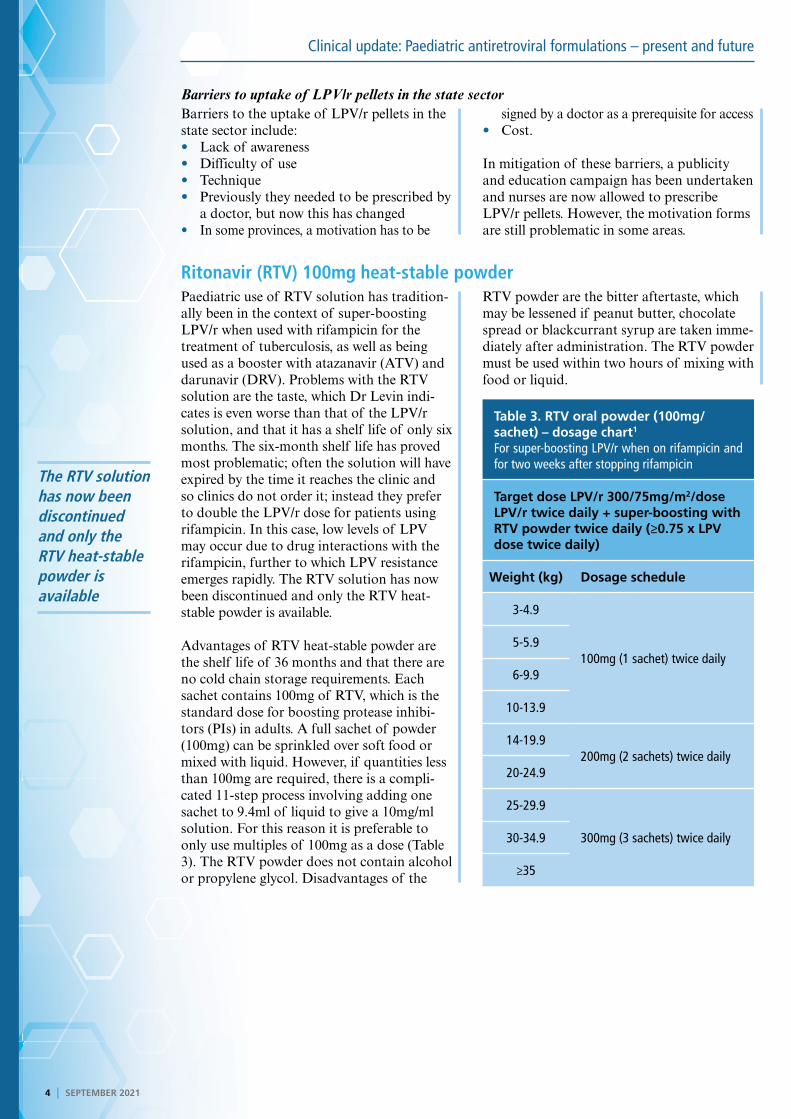
Table 3. RTV oral powder (100mg/sachet) – dosage chart1
For super-boosting LPV/r when on rifampicin and for two weeks after stopping rifampicin
Target dose LPV/r 300/75mg/m2/dose LPV/r twice daily + super-boosting with RTV powder twice daily (≥0.75 x LPV dose twice daily)
Weight (kg) Dosage schedule
3-4.9
100mg (1 sachet) twice daily5-5.9
6-9.9
10-13.9
14-19.9200mg (2 sachets) twice daily
20-24.9
25-29.9
300mg (3 sachets) twice daily30-34.9
≥35
SEPTEMBER 2021 I 5
Clinical update: Paediatric antiretroviral formulations – present and future
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
TAF is a prodrug of tenofovir, but has markedly lower adverse effects on the kidneys and bones
Some confusion can easily arise between the two types of DTG formulation; the film-coated DTG tablets and the dispersible DTG tablets are not bioequivalent
The future – new agents and new formulations not yet available
LPV/r 40/10mg granulesLPV/r granules apparently dissolve well in soft food or liquids; unfortunately, unlike the pellets, the granules do have a bad taste.
LPV/r 40/10mg granules are not yet registered with SAHPRA.
ABC/3TC/LPV/r (30/15/40/10mg) powderThis four-in-one powder is not yet registered with the US Food and Drug Administration or SAHPRA. The powder is contained in a capsule; this is opened up to be sprinkled on
food or mixed into liquid. The powder has a pleasant ‘strawberry ice cream’ taste. “It is truly delicious,” Dr Levin reflects.
Tenofovir alafenamide (TAF) TAF is a prodrug of tenofovir, but has mark-edly lower adverse effects on the kidneys and bones, making it better suited for both renal and paediatric patients than tenofovir diso-proxil fumarate (TDF). It is a very small for-mulation; a 10mg dose is used together with CYP450 inhibitors such as RTV or cobicistat
(COBI) whereas in the absence of CYP450 inhibitors, a 25mg dose is used. TAF can be given from six years of age and ≥25kg. There is a suspicion that it may be associated with weight gain but this does seem to be less of a problem in children.
TAF/emtricitabine (FTC)/dolutegravir (DTG) (25/200/50mg) tabletA single, tiny TAF/FTC/DTG tablet requires once-daily dosing in children older than six years and weighing 25kg or more. Renal func-tion should be monitored, as should weight gain. When the child’s weight reaches 35kg,
they can switch to TDF/3TC/DTG (also known as TLD). There are currently at least two generics of TAF/FTC/DTG, and one has already been registered by SAHPRA.
TAF/FTC/rilpivirine (RPV) 25/200/25mg tabletThis tiny tablet can only be used from 12 years of age and with weight ≥35kg because it contains RPV, which can only be used from 12 years and 35kg. The actual dose of RPV that is used is 25mg because the standard dose of 75mg is quite toxic, with QT prolon-gation. The 25mg dose of RPV used in the
TAF/FTC/RPV formulation is safe but the lower dose consequently has a low genetic barrier to resistance and can only be used with viral loads <100 000 copies/ml. Renal function and weight gain should be moni-tored. TAF/FTC/RPV has been registered by SAHPRA but is not yet available.
DTG paediatric formulationsSome confusion can easily arise between the two types of DTG paediatric formulation; the film-coated DTG tablets and the dis-persible DTG tablets are not bioequivalent. The film-coated tablet, such as the 50mg DTG currently used, can be crushed but is not dispersible. There are 10mg and 25mg formulations currently awaiting SAHPRA registration, having originally been developed for treating paediatric patients from 30-40kg
with a 35mg once-daily dose; however, the safety of the 50mg dose in children who weigh ≥20kg has since been established and so the need for the 35mg dose has fallen away. To have the same effect as the dispersible DTG tablets, a 1.6-fold greater dose of the film-coated DTG is required - 40mg of film-coated DTG tablets are equivalent to 25mg of dispersible DTG tablets, causing potential confusion.
6 I SEPTEMBER 2021
Clinical update: Paediatric antiretroviral formulations – present and future
Dr Levin is of the view that the ABC/3TC/LPV/r powder is a preferred candidate for second-line regimens after failing DTG-based paediatric first-line therapy
The dispersible DTG tablets are dispersible in water; formulations that will be available are 5mg and 10mg tablets. Since there are 10mg tablets in both formulations and because they are not bioequivalent this has great poten-tial to create confusion; it is important to note that the generic 10mg dispersible DTG tablet is scored, which will be an easy way of distinguishing it from the unscored 10mg
film-coated tablet. The DTG dispersible tablets can be used from four weeks of age and ≥3kg. An application for registration is currently lodged with SAHPRA. Availability of the dispersible DTG tablet will likely result in LPV/r no longer being used as a first-line ARV in paediatrics. The recommended dos-age of the two DTG formulations are sum-marised in Tables 4 and 5.
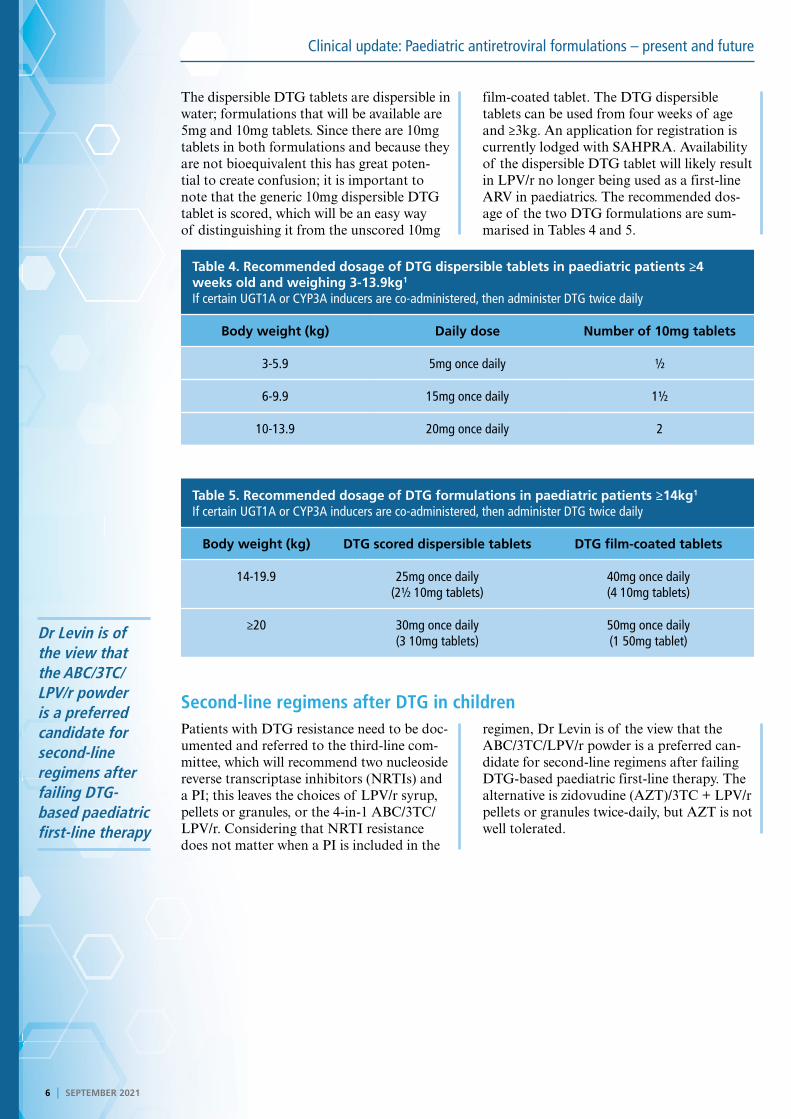
Table 4. Recommended dosage of DTG dispersible tablets in paediatric patients ≥4 weeks old and weighing 3-13.9kg1
If certain UGT1A or CYP3A inducers are co-administered, then administer DTG twice daily
Body weight (kg) Daily dose Number of 10mg tablets
3-5.9 5mg once daily ½
6-9.9 15mg once daily 1½
10-13.9 20mg once daily 2
Table 5. Recommended dosage of DTG formulations in paediatric patients ≥14kg1 If certain UGT1A or CYP3A inducers are co-administered, then administer DTG twice daily
Body weight (kg) DTG scored dispersible tablets DTG film-coated tablets
14-19.9 25mg once daily(2½ 10mg tablets)
40mg once daily(4 10mg tablets)
≥20 30mg once daily(3 10mg tablets)
50mg once daily(1 50mg tablet)
Second-line regimens after DTG in childrenPatients with DTG resistance need to be doc-umented and referred to the third-line com-mittee, which will recommend two nucleoside reverse transcriptase inhibitors (NRTIs) and a PI; this leaves the choices of LPV/r syrup, pellets or granules, or the 4-in-1 ABC/3TC/LPV/r. Considering that NRTI resistance does not matter when a PI is included in the
regimen, Dr Levin is of the view that the ABC/3TC/LPV/r powder is a preferred can-didate for second-line regimens after failing DTG-based paediatric first-line therapy. The alternative is zidovudine (AZT)/3TC + LPV/r pellets or granules twice-daily, but AZT is not well tolerated.
DisclaimerThe views and opinions expressed in the article are those of the presenters and do not necessarily reflect those of the publisher or its sponsor. In all clinical instances, medical practitioners are referred to the product insert documentation as approved by relevant control authorities.
Clinical update: Paediatric antiretroviral formulations – present and future
EARN FREECPD POINTS
Are you a member of Southern Africa’s leading
digital Continuing Professional Development
website earning FREE CPD points with access to
best practice content?
Only a few clicks and you can register to start
earning today
Visit
For all Southern African healthcare professionals
www.denovomedica.com
DeNovo Medica
@deNovoMedica
deNovo Medica
Find us at
Published by
70 Arlington Street, Everglen, Cape Town, 7550Tel: (021) 976 0485 I [email protected]
© 2021 deNovo MedicaReg: 2012/216456/07
This CPD-accredited programme was written for deNovo Medica byGlenda Hardy, BSc(Hons) Medical Cell Biology and reviewed by Dr Leon Levin
SEPTEMBER 2021 I 7
Key learnings
Of currently available paediatric ARV formulations:
• The ABC/3TC scored and dispersible tablet has many benefits with few disadvantages
• The LPV/r solution is not well tolerated; LPV/r pellets are slightly better tolerated dependent on administration technique but the NDoH recommends them for infants only from the age of six months and not tolerating LPV/r solution
• The RTV heat-stable powder has many advantages over the RTV solution, which has now been discontinued
Of paediatric ARV formulations that will be available in the near future:
• LPV/r granules dissolve well in soft foods or liquids but still have a bad taste
• ABC/3TC/LPV/r powder has a pleasant taste and is likely to be the preferred second-line regimen after DTG-based paediatric first-line failure
• TAF formulations have markedly lower adverse effects on the kidneys and bones, although renal function and weight gain should be monitored, and can be used from the age of six years and ≥25kg
• Dosing confusion can easily arise between the 10mg formulations of DTG film-coated tablets and DTG dispersible tablets, which are not bioequivalent.
NOW EARN FREE CPD POINTS
Click here to access and submit deNovo Medica’s CPD modules
ReferencesClick on reference to access the scientific article1. South African National Department of Health, Southern African HIV Clinicians Society. Antiretroviral drug dosing chart for children, 2021.