paediatrics in thenetherlands: challenges today and tomorrow
TRANSCRIPT

Archives of Disease in Childhood 1993; 69: 251-255
CHALLENGES
Paediatrics in the Netherlands: challenges fortoday and tomorrow
Henk K A Visser
This is the eighth paper ina series showing theproblems facing the medicalservices for children indifferent countries.
Erasmus Universityand Department ofPaediatrics, UniversityHospital, Rotterdam,The Netherlands
Correspondence to:Professor H K A Visser,Sophia Children's Hospital,Gordelweg 160, 3038 GERotterdam, TheNetherlands.
The Dutch Paediatric Society had its 100thanniversary in 1992. Paediatrics in theNetherlands has changed in a remarkable wayparticularly during the last 25 years and thenumber of paediatricians has more thandoubled. Paediatrics is nowadays a popularspecialty for medical students and there are
(too) many applications for specialty training.Many new hospitals - with departments ofpaediatrics - have been constructed. There are
now eight university departments of paediatrics,which include three children's hospitals. Mostof them are in new buildings and the others willfollow within the next few years. A large numberof young paediatricians have been trainedabroad in (clinical) research and have returnedto their home country. The paediatric researchoutput has increased considerably. The healthstatus of Dutch children is good. The countryhas an excellent health care delivery system alsofor children - with universal coverage and so farno serious financial limitations.One may conclude that paediatrics in the
Netherlands is doing well. This is true, but thereare some problems. Costs of health care are ris-ing and there are now political discussionsabout cost and health effectiveness and effi-ciency. The population is aging and an increas-ing proportion of health expenditure will go togeriatric care. For paediatrics the challenge forthe future is to get its adequate share of thenational health budget, while maintaining thequality of care.
There are a number of basic issues in Dutchpaediatrics, which will be mentioned in thisarticle: (i) the integration of health services -
both curative and preventive - with appropriateregionalisation, (ii) paediatric manpower plan-ning, and (iii) quality control of services.Furthermore, I will discuss some problems anddevelopments in perinatal care and deal with theincreasing importance of medical ethical prob-lems in paediatrics. Finally, I will mention thepresent day discussions on non-therapeuticresearch in children that are taking place in the
Dutch parliament.
Table 1 Infant mortality and perinatal mortality in the Netherlands 1 980-91 (data fromCentral Bureau for Statistics)
1980 1985 1989 1990 1991
Infant mortality (per 1000 live births)Perinatal mortality (per 1000 births)Stillbirths (per 1000 births)Neonatal mortality (0-7 days) (per 1000 live births)
8-6 8-011-1 9-86-6 594-5 40
6-89-65-83-8
7-19-65-73.9
6-59-15-33-8
Some general demographic and economicbackground data and selected healthstatus indicatorsThe Netherlands has about 15 million in-habitants, of which about 5% (0-7 million) areof non-Dutch origin. The Netherlands is now amultiracial society with large numbers ofimmigrants from Surinam, Dutch Antilles,Mediterranean countries (mainly Turkey andMorocco), and recently Asian and Africancountries. The immigrants live mainly in thelarge cities (Amsterdam, Rotterdam, TheHague) in the western part of the country (theprovinces of North and South Holland). In theSophia Children's Hospital in Rotterdam about35% of the patients are of non-Dutch origin.
In 1991 nearly 200000 children were born(13.2 per 1000 population) and the birth ratehas been more or less stable for a number ofyears. The average length of life in 1991 was70 9 years for males and 77-1 years for females.Life expectancy at birth was 74 1 years for malesand 80-2 years for females. In 1991 18% of thepopulation was in the age group 0-14 years.
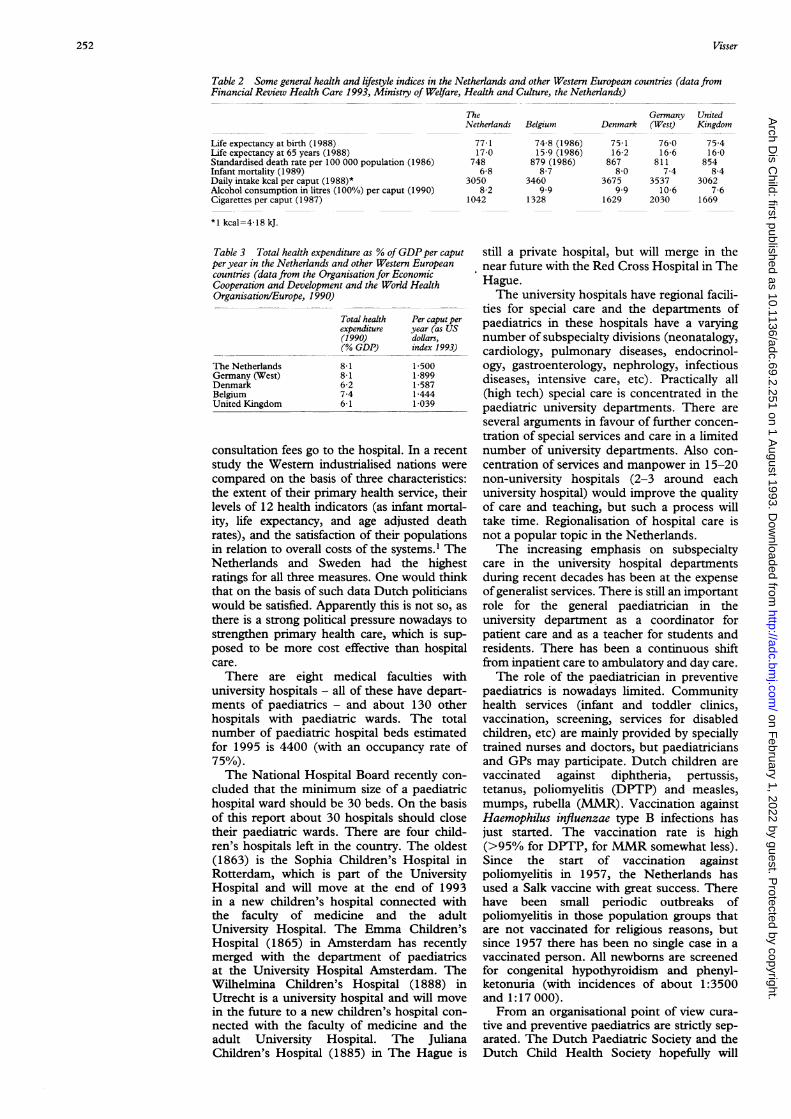
Infant mortality and perinatal mortality arevery low (table 1). Some general health andlifestyle indices for the Netherlands and someWestern European countries are given in table2. Total health expenditure in 1990 was 8- 1% ofgross domestic product (GDP) (table 3).
Health care delivery for childrenThere has always been great emphasis on pri-mary health care in the Netherlands and thegeneral practitioner (GP) is in the centre of thehealth care system. There are now about 6000GPs with an average size of practice of about2500 people. As in the United Kingdom the GPhas a primary responsibility for the care of sickchildren and the paediatrician is a consultantphysician and member of a hospital staff. Thehealth insurance system will pay the GP anannual fee per caput for those families with anannual income of less than about 55 000 Dutchguilders (about £20 750); this includes about70% of the population. The other 30% of thepopulation generally has private health in-surance, which will pay the GP per consulta-tion. The paediatrician is paid by the healthinsurance per consultation but only if thepatient is referred by the GP. More than 750/oof paediatricians are now paid by the hospitaland have a fixed income, in this situation the
251
on February 1, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.2.251 on 1 A
ugust 1993. Dow
nloaded from
Visser
Table 2 Some general health and lifestyle indices in the Netherlands and other Western European countries (data fromFinancial Review Health Care 1993, Ministry of Welfare, Health and Culture, the Netherlands)
TheNetherlands Belgiun
Germany UnitedDenmark (West) Kingdom
Life expectancy at birth (1988)Life expectancy at 65 years (1988)Standardised death rate per 100 000 population (1986)Infant mortality (1989)Daily intake kcal per caput (1988)*Alcohol consumption in litres (100%) per caput (1990)Cigarettes per caput (1987)
*1 kcal=4-18 kJ.
Table 3 Total health expenditure as % of GDPper caputperyear in the Netherlands and other Western Europeancountries (data from the Organisation for EconomicCooperation and Development and the World HealthOrganisation/Europe, 1990)
The NetherlandsGermany (West)DenmarkBelgiumUnited Kingdom
Total healthexpenditure(1990)(% GDP)
8-18-16-27.46 1
Per caput peryear (as USdollars,index 1993)
1 5001-8991-5871-4441-039
consultation fees go to the hospital. In a recentstudy the Western industrialised nations werecompared on the basis of three characteristics:the extent of their primary health service, theirlevels of 12 health indicators (as infant mortal-ity, life expectancy, and age adjusted deathrates), and the satisfaction of their populationsin relation to overall costs of the systems.1 The
Netherlands and Sweden had the highestratings for all three measures. One would thinkthat on the basis of such data Dutch politicianswould be satisfied. Apparently this is not so, as
there is a strong political pressure nowadays tostrengthen primary health care, which is sup-posed to be more cost effective than hospitalcare.
There are eight medical faculties withuniversity hospitals - all of these have depart-ments of paediatrics - and about 130 otherhospitals with paediatric wards. The totalnumber of paediatric hospital beds estimatedfor 1995 is 4400 (with an occupancy rate of75%).The National Hospital Board recently con-
cluded that the minimum size of a paediatrichospital ward should be 30 beds. On the basisof this report about 30 hospitals should closetheir paediatric wards. There are four child-ren's hospitals left in the country. The oldest(1863) is the Sophia Children's Hospital inRotterdam, which is part of the UniversityHospital and will move at the end of 1993in a new children's hospital connected withthe faculty of medicine and the adultUniversity Hospital. The Emma Children'sHospital (1865) in Amsterdam has recentlymerged with the department of paediatricsat the University Hospital Amsterdam. TheWilhelmina Children's Hospital (1888) inUtrecht is a university hospital and will movein the future to a new children's hospital con-
nected with the faculty of medicine and theadult University Hospital. The JulianaChildren's Hospital (1885) in The Hague is
still a private hospital, but will merge in thenear future with the Red Cross Hospital in TheHague.The university hospitals have regional facili-
ties for special care and the departments ofpaediatrics in these hospitals have a varyingnumber of subspecialty divisions (neonatalogy,cardiology, pulmonary diseases, endocrinol-ogy, gastroenterology, nephrology, infectiousdiseases, intensive care, etc). Practically all(high tech) special care is concentrated in thepaediatric university departments. There are
several arguments in favour of further concen-
tration of special services and care in a limitednumber of university departments. Also con-
centration of services and manpower in 15-20non-university hospitals (2-3 around eachuniversity hospital) would improve the qualityof care and teaching, but such a process willtake time. Regionalisation of hospital care isnot a popular topic in the Netherlands.The increasing emphasis on subspecialty
care in the university hospital departmentsduring recent decades has been at the expenseof generalist services. There is still an importantrole for the general paediatrician in theuniversity department as a coordinator forpatient care and as a teacher for students andresidents. There has been a continuous shiftfrom inpatient care to ambulatory and day care.
The role of the paediatrician in preventivepaediatrics is nowadays limited. Communityhealth services (infant and toddler clinics,vaccination, screening, services for disabledchildren, etc) are mainly provided by speciallytrained nurses and doctors, but paediatriciansand GPs may participate. Dutch children are
vaccinated against diphtheria, pertussis,tetanus, poliomyelitis (DPTP) and measles,mumps, rubella (MMR). Vaccination againstHaemophilus influenzae type B infections hasjust started. The vaccination rate is high(>95% for DPTP, for MMR somewhat less).Since the start of vaccination againstpoliomyelitis in 1957, the Netherlands hasused a Salk vaccine with great success. Therehave been small periodic outbreaks ofpoliomyelitis in those population groups thatare not vaccinated for religious reasons, butsince 1957 there has been no single case in avaccinated person. All newborns are screenedfor congenital hypothyroidism and phenyl-ketonuria (with incidences of about 1:3500and 1:17 000).From an organisational point of view cura-
tive and preventive paediatrics are strictly sep-arated. The Dutch Paediatric Society and theDutch Child Health Society hopefully will
77 117-0
7486-8
30508-2
1042
74-8 (1986)15 9 (1986)
879 (1986)8-7
34609.9
1328
75 116 2
8678-0
36759.9
1629
76-016 6
8117 4
353710-6
2030
75-416-0
8548-4
30627-6
1669
252
on February 1, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.2.251 on 1 A
ugust 1993. Dow
nloaded from

Paediatrics in the Netherlands: challenges for today and tomorrow
Table 4 Total number of registered paediatricians ascompared with other specialists and general practitioners(1960-85); this includes paediatricians who are workingpart time
1960 1985
Specialists (total No)PaediatriciansSurgeonsInternistsCardiologistsPulmnonologistsGeneral practitioners
3 73231037348460260
4 343
10 796735925
1 447409345
5 900
(2-9X)(2-4X)(2-5X)(3OX)(6 8X)(1-3X)(1-4X)
Table 5 Paediatricians (per 100 000 <14 years) ascompared with internists including cardiologists andpulmonologists (per 100 000 >14 years) (1960-85)
Population of the Netherlands< 14 years> 14 years
Paediatricians/100 000 < 14 yeaInternists/100 000 > 14 years
cooperate more closelymay lead to a better inhospital and child healtMany children with
now surviving beyoncgroup. An increasing nwith cystic fibrosis, spheart disease, inborn errother long term chroncome under the care of;a great need for regul,clinics of paediatriciacolleagues to facilitate iadolescents from the Itheir comprehensive teahospital centres.
For the coming yearstant to evaluate our pmeasure health outconRegular site visits of pwith quality control bywork.accountable to theMeasuring outcomes mregister what we are doilow up studies. Thereclinical epidemiologicalWe need data on changediseases, the efficacychronic disorders, anddistribution over time.'the pattern of servicescare, ambulatory care,
Table 6 Number ofpaediatritacademic centres (approximate
Paediatricians (total No)Academic centresOther
Table 7 Preliminary estimation of the total number ofpaedia,(fte=fuUl time equivalent consultant positions)
About 90 smaller hospitals with departnents of paediatrics (1st ec.About 16 larger hospitals (1st echelon)
with departments of paediatrics (2nd echelon)Eight academic centres (lst and 2nd echelon)
Regional special careTotal number (approximately)Of these are 300 women in part time (0-5) functionTotal number of paediatricians needed in 2000
care - is changing. In the Netherlands there arenow collaborative working groups on child-hood leukaemia, growth hormone treatment,congenital hypothyroidism, phenylketonuria,and others. The Dutch Paediatric Society hasstarted a working group for registration ofspecific disorders. There are a number ofongoing collaborative follow up studies on(very) low birthweight infants. There is also acomprehensive perinatal and neonatal registra-tion organised by the Dutch Obstetric Societyand Dutch Paediatric Society.
1960 1985 Paediatric education and manpowerplanning
Cmllions) 11-4 14 4 Paediatrics is now one of the important clinical3-5 2-97-9 11-5 disciplines in the curriculum of the medical
us 19 26 schools in the Netherlands. In the six year cur-riculum there are generally paediatric lecturesin the third and fourth year, and a so called
in the future and this junior and senior clerkship in the fifth and/oritegration of paediatric sixth year (three and six weeks of teaching andh community services. experience, respectively).chronic illnesses are Postgraduate training for general practice is
I the paediatric age three years, for paediatrics five years.lumber of adolescents Paediatric residency training is concentrated inina bifida, congenital the eight university departments, but at leastors of metabolism, and one year of the training should be in anlic diseases have now affiliated hospital. There are now about 150adult services. There is paediatric residents in training with an annualar meetings and joint 'output' of about 30 per year.ms and their adult The total number of paediatricians has morethe transition of these than doubled in the last 25 years (table 4), butpaediatric clinics with when calculated per 100 000 children less thanm services to the adult 14 years of age, the total number has alnost
tripled (table 5). About 30°/O of paediatriciansit will be very impor- are now working in the academic centres (table
oaediatric services and 6). There are many vacancies for consultantnes in a critical way. positions these days and it is expected that the)aediatric departnents total number of resident positions will bepeers will make our increased. It is somewhat difficult to make apublic and politicians. prognosis for the total number of paediatriciansieans that we carefully needed in the year 2000. The number ofing and emphasise fol- women paediatricians will increase (in medical
is a great need for schools more than 50°/O of the students are nowstudies in paediatrics. women), and most of them will work in part
!s in prevalence rates of time positions. The number of working hoursof the treatment of per week will decrease. It can be expected thatchanges in birthweight in the future Dutch paediatricians will work inWe want to know how other countries in the European community. A- inpatient care, day- preliminary prognosis for the year 2000 is aboutintensive/medium/low 1000 paediatricians (table 7). Residency train-
ing is typical 'in-service training' with structuralcians working in the eight teaching, which is supervised by a nationalnumbers) board. There is no formal examination. After1960 1985 five years one is registered and is eligible for a
350 735 post as a paediatrician in a hospital, a position70 (220/%) 210 (29%) comparable with a consultant in the United240 525 Kingdom. In all hospitals in the country there is
a total paediatric house staff of about 150-200tricians in the year 2000 young physicians who are not registered as a
resident 'in training'; most of them are waitingfor such a position. The total number of
helon) 90X3 = 270 fte16x3 = 48 fte resident training positions is centrally regulated.16X5 = 808X8 = 648X30= 240
7003001000
fteI fteftefte Perinatal care
There have been great changes in perinatalcare during recent decades. In the Netherlands
253
on February 1, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.2.251 on 1 A
ugust 1993. Dow
nloaded from
254Visser
Table 8 Birth in the Netherlands: place of birth andobstetnc assistance (data from Central Bureau of Statistics)
1980 1985 1989 1990 1991
Obstetric assistance (0/o)PhysicianMidwifeBothOther
Place of birth (%)HomeHospitalOther
59-7 57-839-4 41-705 0404 00
35-4 36-661-3 61-23-3 2-2
54 0 54-145-5 44-805 1-00-0 0-1
33-4 32-164-6 66-22-1 1-6
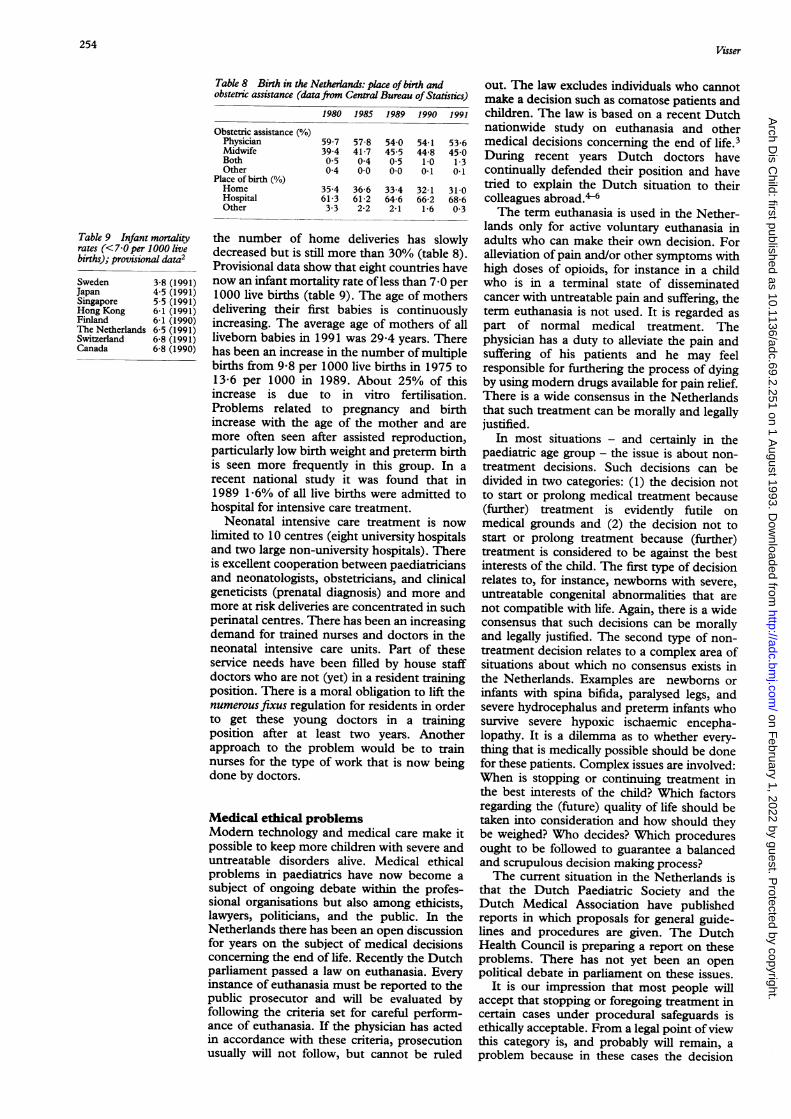
the number of home deliveries has slowlydecreased but is still more than 30% (table 8).Provisional data show that eight countries havenow an infant mortality rate of less than 7 0 per1000 live births (table 9). The age of mothersdelivering their first babies is continuouslyincreasing. The average age of mothers of allliveborn babies in 1991 was 29-4 years. Therehas been an increase in the number of multiplebirths from 9-8 per 1000 live births in 1975 to13-6 per 1000 in 1989. About 25% of thisincrease is due to in vitro fertilisation.Problems related to pregnancy and birthincrease with the age of the mother and aremore often seen after assisted reproduction,particularly low birth weight and preterm birthis seen more frequently in this group. In arecent national study it was found that in1989 1-6% of all live births were admitted tohospital for intensive care treatment.
Neonatal intensive care treatment is nowlimited to 10 centres (eight university hospitalsand two large non-university hospitals). Thereis excellent cooperation between paediatriciansand neonatologists, obstetricians, and clinicalgeneticists (prenatal diagnosis) and more andmore at risk deliveries are concentrated in suchperinatal centres. There has been an increasingdemand for trained nurses and doctors in theneonatal intensive care units. Part of theseservice needs have been filled by house staffdoctors who are not (yet) in a resident trainingposition. There is a moral obligation to lift thenumerous fixus regulation for residents in orderto get these young doctors in a trainingposition after at least two years. Anotherapproach to the problem would be to trainnurses for the type of work that is now beingdone by doctors.
Medical ethical problemsModern technology and medical care make itpossible to keep more children with severe anduntreatable disorders alive. Medical ethicalproblems in paediatrics have now become asubject of ongoing debate within the profes-sional organisations but also among ethicists,lawyers, politicians, and the public. In theNetherlands there has been an open discussionfor years on the subject of medical decisionsconcerning the end of life. Recently the Dutchparliament passed a law on euthanasia. Everyinstance of euthanasia must be reported to thepublic prosecutor and will be evaluated byfollowing the criteria set for careful perform-ance of euthanasia. If the physician has actedin accordance with these criteria, prosecutionusually will not follow, but cannot be ruled
out. The law excludes individuals who cannotmake a decision such as comatose patients andchildren. The law is based on a recent Dutchnationwide study on euthanasia and othermedical decisions concerning the end of life.3During recent years Dutch doctors havecontinually defended their position and havetried to explain the Dutch situation to theircolleagues abroad."The term euthanasia is used in the Nether-
lands only for active voluntary euthanasia inadults who can make their own decision. Foralleviation of pain and/or other symptoms withhigh doses of opioids, for instance in a childwho is in a terminal state of disseminatedcancer with untreatable pain and suffering, theterm euthanasia is not used. It is regarded aspart of normal medical treatment. Thephysician has a duty to alleviate the pain andsuffering of his patients and he may feelresponsible for furthering the process of dyingby using modern drugs available for pain relief.There is a wide consensus in the Netherlandsthat such treatment can be morally and legallyjustified.
In most situations - and certainly in thepaediatric age group - the issue is about non-treatment decisions. Such decisions can bedivided in two categories: (1) the decision notto start or prolong medical treatment because(further) treatment is evidently futile onmedical grounds and (2) the decision not tostart or prolong treatment because (further)treatment is considered to be against the bestinterests of the child. The first type of decisionrelates to, for instance, newborns with severe,untreatable congenital abnormalities that arenot compatible with life. Again, there is a wideconsensus that such decisions can be morallyand legally justified. The second type of non-treatment decision relates to a complex area ofsituations about which no consensus exists inthe Netherlands. Examples are newborns orinfants with spina bifida, paralysed legs, andsevere hydrocephalus and preterm infants whosurvive severe hypoxic ischaemic encepha-lopathy. It is a dilemma as to whether every-thing that is medically possible should be donefor these patients. Complex issues are involved:When is stopping or continuing treatment inthe best interests of the child? Which factorsregarding the (future) quality of life should betaken into consideration and how should theybe weighed? Who decides? Which proceduresought to be followed to guarantee a balancedand scrupulous decision making process?The current situation in the Netherlands is
that the Dutch Paediatric Society and theDutch Medical Association have publishedreports in which proposals for general guide-lines and procedures are given. The DutchHealth Council is preparing a report on theseproblems. There has not yet been an openpolitical debate in parliament on these issues.
It is our impression that most people willaccept that stopping or foregoing treatment incertain cases under procedural safeguards isethically acceptable. From a legal point ofviewthis category is, and probably will remain, aproblem because in these cases the decision
Table 9 Infant mortalityrates (<7-0 per 1000 livebirths); provisional data2
SwedenJapanSingaporeHong KongFinlandThe NetherlandsSwitzerlandCanada
3-8 (1991)4-5 (1991)5-5 (1991)6-1 (1991)6-1 (1990)6-5 (1991)6-8 (1991)6-8 (1990)
on February 1, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.2.251 on 1 A
ugust 1993. Dow
nloaded from

Paediatrics in the Netherlands: challenges for today and tomorrow
not to treat or to stop treatment is guided by acomplex of intentions. Therefore, any decisionto prosecute will depend on the individualcircumstances of each case.
Meanwhile, in the Netherlands, physiciansand parents together make the decision, inconcrete situations, acting in the best interestsof the child. It is our strong impression and ourexperience that in most cases physicians andparents after a scrupulous and careful decisionmaking process, reach a consensus. In the largepaediatric departments and children's hospi-tals in the Netherlands, medical ethical com-mittees evaluate such decisions and thecarefulness of the procedures. The districtpublic prosecutor is also consulted.The prevalence of active euthanasia in child-
ren in the Netherlands is, to our knowledge,extremely low. On active (by definition non-voluntary) euthanasia in children there is noconsensus here. For physicians, this type ofdecision is different from the type of decisionnot to start or to forego medical treatment.From a legal point of view one thing is certain:in such cases death is clearly intended and thatmeans that the cause of death has to bereported as unnatural and will lead to aninvestigation by the public prosecutor.
Paediatricians who are 'euthanasia enthusi-asts' do not exist. The only motivation formaking medical decisions concerning the endof life in children, together with the parents, isthe individual patient's best interests. In thewell funded health care system in theNetherlands there is no incentive to havepatients die soon. All facilities are available forthe care of severely handicapped children.
Non-therapeutic research in childrenRecently the Dutch government has sent a lawproposal to parliament on medical experimentsin humans. Therapeutic and non-therapeuticresearch in children is accepted but understrict guidelines. Non-therapeutic experimentsin children should be controlled by a newcentral medical ethical committee. In the firstdiscussion between government and parlia-ment there was great concern in almost allpolitical parties and it was suggested that non-therapeutic experiments be banned in childrenaltogether. For obvious reasons Dutch paedia-tricians - particularly in academic centres - arealarmed by these developments. A ban onnon-therapeutic research in children would
stop a greater part of paediatric research andwould not be in the interests of children ingeneral.
Both the British Paediatric Association andthe Canadian Paediatric Society have recentlypublished reports on research involving child-ren, and both societies eloquently defend non-therapeutic research in the paediatric agegroup albeit under strict conditions.7 8Arguments on the ethical and legal principlesof research on children have been repeatedlydebated in the medical literature during thelast decades and the greatest majority ofauthors have pointed out that non-therapeuticresearch on children should be acceptable withlimitations.9-15
It is justified to involve children in non-therapeutic research that is judged to be lowrisk or low harm. Such research includes thecollection of data on normal growth and devel-opment in the broadest sense (also bloodvalues) and the assessment of diagnosticmethods. Indeed by prohibiting non-therapeu-tic research in children - and not in adults! -one denies the advantages of such investiga-tions to the paediatric age group as a whole andthis would treat children unjustly.
1 Starfield B. Primary care and health. A cross-national com-parison.3'AMA 1991; 266: 2268-71.
2 Wegman ME. Annual summary of vital statistics 1991.Pediatrics 1992; 90: 835-45.
3 Van der Maas PJ, van Delden JIM, Pijnenburg L, LoomanCWN. Euthanasia and other decisions concerning the endof life. Lancet 1991; ii: 669-74.
4 Rigter H, Borst-Eilers E, Leenen HnJ. Euthanasia across theNorth Sea. BMJ 1988; 297: 1593-4.
5 Sauer PJJ. Ethical decisions in neonatal intensive care units:the Dutch experience. Pediatrics 1992; 90: 729-32.
6 Visser HKA, Aartsen HGM, de Beaufort ID. Medicaldecisions concerning the end of life in children in theNetherlands. Am JDis Child 1992; 146: 1429-3 1.
7 Ethics Advisory Committee. Guidelines for the ethical conductof medical research involving children. London: BritishPaediatric Association, August 1992.
8 Consent Panel Task Force of the National Council onBioethics in Human Research, with the support of theCanadian Paediatric Society. Report on research involvingchildren. Ottawa: Canadian Paediatric Society, May 1992.
9 Curran WJ, Hyg SM, Beecher HK. Experimentation inchildren. A re-examination of legal ethical principles.JAMA 1969; 210: 77-83.
10 The ethics of research involving children as controls[Editorial]. Arch Dis Child 1973; 48: 751-2.
11 Lowe CW, Alexander D, Mishkin B. Non-therapeuticresearch on children: an ethical dilemma. J Pediatr 1974;84: 468-72.
12 McCartney JJ. Research on children. National commission says'yes, if . . . ' Hastings on Hudson, NY; Hastings CentreReport, October 1978: 26-31.
13 Anonymous. Research involving children - ethics, the law,and the climate of opinion [Editorial]. Arch Dis Child1978; 53: 441-2.
14 Dworkin G. Legality of consent to non-therapeuticalmedical research on infants and young children. Arch DisChild 1978; 53: 443-6.
15 Nicholson R, ed. Medical research with children: ethics, lawand practice. Oxford: Oxford University Press, 1986.
255
on February 1, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.69.2.251 on 1 A
ugust 1993. Dow
nloaded from