palliative care in patients with heart failure and cancer
TRANSCRIPT

Palliative Care in Patients with Heart Failure and Cancer
HFA, Gothenburg 2011
Mary Ryder MSc Nursing, ANP, RNP, NFESC

Palliative Care
The term ‘palliative care’ was introduced in the 1970’s by Balfour Mount to describe care of patients living with a life-limiting illness that focused on maximising quality of life. Unlike hospice care palliative care was not limited by prognosis or setting of care
Lynch et al J of Hosp & Pall Nurs. 2011

Palliative Care and Cancer
• Palliative care is delivered in conjunction with Cancer treatment from diagnosis
• Delivered by a specialist working with the Cancer team
• Supportive care managing quality of life issues
• Palliative care addresses the emotional, physical, emotional, practical, and spiritual issues of cancer.
National Cancer Institute 2011

Palliative Care and Heart Failure
• Unpredictable disease trajectory causing problems for identifying need for palliative care
• Many co-morbidities
• Complex medication regimes frequently changing
Anderson et al 2001, Murray et al 2002, Exley et al 2005 Selman et al 2007, Gott et al 2007

Symptom Management
• Dyspnoea – Cancer patients with or without lung involvement
– 3rd most common reported symptom of HF patients along with fatigue and dry mouth
– Dyspnoea increases with • Depression
• Anxiety
– Most patients who report dyspnoea also report fatigue and pain: regardless of underlying diagnosis
Brennan et al May/June 2011

Outline of experiences of patients Lung Cancer
• Initially feel well but told you are ill
• "How long have I got?“
• Swinging between hope and despair
• Lung cancer takes over life and becomes overriding concern
• Treatment calendar dominates life, more contact with services and professionals
• Specialist services often available in the community
• Care prioritised early as "cancer" and later as "terminally ill"
Cardiac Failure • Feel ill but told you are well
• "I know it won't get better, but I hope it
won't get any worse“
• Daily grind of hopelessness
• Much co-morbidity to cope with; heart often not seen as main issue
• Shrinking social world dominates life, little contact with health and social services
• Specialist services rarely available in
the community • Less priority as a "chronic disease" and
less priority later as uncertain if yet "terminally ill"
Murray et al BMJ 2002
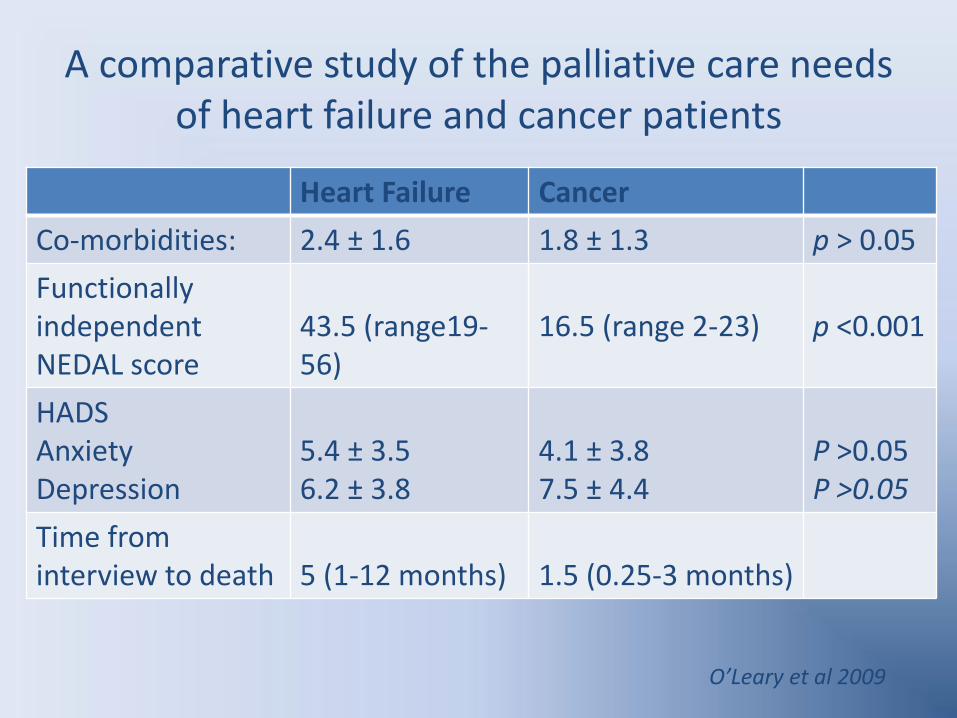
A comparative study of the palliative care needs of heart failure and cancer patients
Heart Failure Cancer
Co-morbidities: 2.4 ± 1.6 1.8 ± 1.3 p > 0.05
Functionally independent NEDAL score
43.5 (range19-56)
16.5 (range 2-23)
p <0.001
HADS Anxiety Depression
5.4 ± 3.5 6.2 ± 3.8
4.1 ± 3.8 7.5 ± 4.4
P >0.05 P >0.05
Time from interview to death
5 (1-12 months)
1.5 (0.25-3 months)
O’Leary et al 2009

Edmonton Symptom Assessment Scale symptoms (prevalence and score intensity) Symptoms Prevalence (%) Mean intensity Heart Cancer Heart Cancer failure failure
Reduced wellbeing 100 90 5.1 5.2 Dyspnoea 92 60 5.3 3.1* Tiredness 92 82 5.6 5.5 Reduced appetite 82 90 3.7 4.9* Drowsiness 6 22 3.6 3.2 Anxiety 68 48 3.2 2.4 Depression 66 22 3.0 2.3 Pain 60 66 2.8 3.3 * Nausea 28 28 1.0 1.1 *Statistically significant difference, significance level P , 0.05
O’Leary et al 2009

Mean SF36 domain scores Heart failure Cancer Mean (SD) Mean (SD) Physical functioning 22.96 (12.11) 17.88 (18.75) Role physical 37.62 (23.87) 30.69 (24.59) Bodily pain 69.28 (28.8) 73.02 (29.24) General health 44 (20.31) 42.0 (24.36) Vitality 42.75 (19.1) 38.05 (18.88) Social functioning 58.75 (32.65) 43.61 (26.19)* Role emotional 69.16 (30.36) 68.7 (30.05) Mental health 71.8 (19.99) 68.55 (17.47) Physical summary measure 31.61 (6.86) 30.31 (8.51) Mental summary measure 48.83 (13.03) 46.28 (11.67) *Statistically significant difference using independent t-test, P ¼ 0.01.
O’Leary et al 2009
Quality of Life in heart failure and cancer patients

Meeting patients palliative care needs within HF services
• Physical: High Symptom Burden
• Emotional: Good Support
• Quality of Life: Social Isolation
• Communication: Unmet needs
• Where comprehensive heart failure services are available the majority of patients palliative care needs can be addresses within the HF team
• Many patients needs are being met O’Leary et al 2009
Themes from interviews
• A proportion of the population felt that they had some unanswered questions pertaining to their diagnosis
• Patients identified a preference with the continuity of care in HFU
‘the nurse knows me very well’
O’Leary et al 2009

Specialist Palliative Care
• Pharmacological & non-pharmacological management of symptoms
• Dyspnoea: – Use of opioids – Use of practical aids
• Anxiety and Depression – Use of Benzodiazepines
• Pain – Use of long acting opioids
• Mobility – Greater access to aids

Recommendations
• Many needs are being met
• Extension of cardiology multidisciplinary approach into community – outreach nurses
• Palliative care – education
• Close liaison/cross fertilisation of ideas
• Inform the public of role of palliative care
O’Leary et al 2009

Palliative Care
• Since Sept 2009
• 15 Heart Failure patients referred for Home Heart Failure Management for end-of –life
• GP central communicator
• HF service referred patients to Specialist Palliative Care
• 10 died at home to date
Ryder SVUH data 2010

Summary
• Palliative care for both Cancer and Heart Failure have same goals
– Optimising symptoms
• Specialist palliative services are more skilled at symptom management at end-of-life
• Sharing skills between specialist disciplines is the target to achieve goals at end-of-life for all patients irrespective of diagnosis