pancreatic trauma: march 1 lessons learned · •aast grade iii-v managed with nom •86 patients...
TRANSCRIPT

Pancreatic Trauma:Lessons Learned
Bindi Naik-Mathuria, MD, MPH
Associate Professor of Surgery and Pediatrics
Trauma Medical Director
Texas Children’s Hospital
Baylor College of Medicine
Houston, TX, USA
March 1st, 20192019

Page 1
xxx00.#####.ppt 12/26/2019 10:45:31 AMSurgical ServicesTrauma Services
• I have no disclosures

Page 2
xxx00.#####.ppt 12/26/2019 10:45:32 AMSurgical ServicesTrauma Services
Acute grade III pancreatic injury

Page 3
xxx00.#####.ppt 12/26/2019 10:45:32 AMSurgical ServicesTrauma Services
• Which management strategy do you prefer for this injury?
- Operative (distal pancreatectomy)
- Non-operative (observation)
- ERCP and stent placement
- Undecided

Page 4
xxx00.#####.ppt 12/26/2019 10:45:32 AMSurgical ServicesTrauma Services
Serum Lipase Level
Post-injury Day 1: 121
Post-injury Day 2: 5,800

Page 5
xxx00.#####.ppt 12/26/2019 10:45:33 AMSurgical ServicesTrauma Services
Post-Injury Day 3

Page 6
xxx00.#####.ppt 12/26/2019 10:45:33 AMSurgical ServicesTrauma Services
Background
• Pancreatic injury in children is relatively rare
• Blunt epigastric force causes the pancreas
to fracture, most commonly in the body overlying the spine

Page 7
xxx00.#####.ppt 12/26/2019 10:45:33 AMSurgical ServicesTrauma Services
AAST CT Grading Scale for Pancreatic TraumaGrade Type of Injury Description of Injury
I Hematoma Minor contusion without duct injury
Laceration Superficial laceration without duct injury
II Hematoma Major contusion without duct injury or tissue loss
Laceration Major laceration without duct injury or tissue loss
III Laceration Distal transection or parenchymal injury with duct injury
IV Laceration Proximal transection or parenchymal injury involvingampulla
V Laceration Massive disruption of pancreatic head
Observation? Distal Pancreatectomy?
Observation vs. Complex Operative Management
Observation

Page 8
xxx00.#####.ppt 12/26/2019 10:45:34 AMSurgical ServicesTrauma Services
Controversy Regarding Management
• Adult recommendations*:
• Grade III/IV injuries should be managed with resection and drainage as non-operative management leads to morbidity
• Pediatric recommendations: UNCLEAR
• Lack of high-quality evidence
• Retrospective
• Lack of standardization
* EAST PMG J Trauma Jan 2017 82(1):185-99.

Page 9
xxx00.#####.ppt 12/26/2019 10:45:34 AMSurgical ServicesTrauma Services

Page 10
xxx00.#####.ppt 12/26/2019 10:45:34 AMSurgical ServicesTrauma Services
Most Common Reported Outcomes
• % Pseudocyst
• % Fistula
• % Other complications
• Hospital Length of Stay
• ICU Length of Stay
• Use of TPN
• Time to oral feeds
• Number of additional interventionsVARIABILITY
When to feed?How to feed?
How long to observe in hospital?
Pseudocyst management?Role of ERCP?

Page 11
xxx00.#####.ppt 12/26/2019 10:45:35 AMSurgical ServicesTrauma Services
• 19 pediatric trauma centers
• 12/19 (63%) used both approaches
• Lack of standardization in NOM clinical management51%
OM
49% NOM
21% were laparoscopic

Page 12
xxx00.#####.ppt 12/26/2019 10:45:36 AMSurgical ServicesTrauma Services
#GOALS
1. We need to standardize NOM management
2. We need a prospective trial to compare outcomes of OM vs NOM

Page 13
xxx00.#####.ppt 12/26/2019 10:45:36 AMSurgical ServicesTrauma Services
Creating a Standard NOM Clinical Pathway
• 20 Pediatric Trauma Centers
• Retrospective study of children ≤ 18
• AAST Grade III-V managed with NOM
• 86 patients
• Median age 9
• 73% grade III, 27% grade IV/V
Naik-Mathuria et al, Proposed clinical pathway for NOM of high-grade pediatric pancreatic injuries, multicenter. J Trauma Acute Care Surg 2017 83(4):589-596

Page 14
xxx00.#####.ppt 12/26/2019 10:45:36 AMSurgical ServicesTrauma Services
Pancreatic Enzymes
100
200
300
400
500
Am
yla
se
0 2 4 6 8Day
200
400
600
800
1000
1200
Lip
ase
0 2 4 6 8Day
Amylase Lipase

Page 15
xxx00.#####.ppt 12/26/2019 10:45:37 AMSurgical ServicesTrauma Services
Are Serial Pancreatic Enzymes Useful?
Pseudocyst No Pseudocyst p
Amylase at Presentation (median)
421 (n=38) 423 (n=28) 0.97
Lipase at Presentation(median)
1163 (n=38) 778 (n=27) 0.29
Peak Amylase (median) 697 (n=15) 715 (n=12) 0.73
Peak Lipase (median) 3177 (n=39) 1685 (n=27) 0.23
Grade III Grade IV/V p
Amylase at Presentation (median)
399 (n=55) 392 (n=20) 0.95
Lipase at Presentation(median)
1050 (n=55) 713.5 (n=22) 0.70
Peak Amylase (median) 538 (n=23) 1325 (n=7) 0.29
Peak Lipase (median) 2130 (n=55) 1755 (n=21) 0.65

Page 16
xxx00.#####.ppt 12/26/2019 10:45:37 AMSurgical ServicesTrauma Services
Feeding Practices
• Diet advancement• 46 (66%) advanced diet based on
symptom improvement• 24 (34%) advanced diet based on
symptom improvement + down-trending labs
• Jejunal feeds 31%• TPN 68%

Page 17
xxx00.#####.ppt 12/26/2019 10:45:37 AMSurgical ServicesTrauma Services
Feeding Practices
020
40
60
80
10
0
Days
Feeding Management
Days on TPN Days to Clear Liquids
Days to Regular Diet
020
40
60
80
10
0
Days
Feeding Management for Grade III (Pancreatic Body Inj)
Days on TPN Days to Clear Liquids
Days to Regular Diet0
20
40
60
80
10
0
Days
Feeding Management for Grade IV/V (Pancreatic Head Inj)
Days on TPN Days to Clear Liquids
Days to Regular Diet

Page 18
xxx00.#####.ppt 12/26/2019 10:45:38 AMSurgical ServicesTrauma Services
Hospital LOS
020
40
60
Days
Hospital LOS for Grades III & IV/V
Grade III Grade IV/V

Page 19
xxx00.#####.ppt 12/26/2019 10:45:38 AMSurgical ServicesTrauma Services
Development of a Standard Clinical Pathway
0
10
20
30
40
50
60
70
80
90
100
% P
atie
nts
50%
Naik-Mathuria et al, Proposed clinical pathway for NOM of high-grade pediatric pancreatic injuries, multicenter. J Trauma Acute Care Surg 2017 83(4):589-596

Page 20
xxx00.#####.ppt 12/26/2019 10:45:38 AMSurgical ServicesTrauma Services
Peri-Pancreatic Fluid Collection Management
• 42/100 (42%) patients• APFC (1-4 wk): 27%• Pseudocyst (4 wk): 15%
• 11/42 (27%) needed CG/resection
• Cysts > 7cm had longer recoveryObservation
64%ERCP/stent10%
Percutaneous Drain
Placement, 24%
Needle Aspiration2%
75
25
79
27
TPN USE NEED FOR DEFINITIVE
PROCEDURE
Intervention Observation
11
25
1215
TIME TO REGULAR DIET
HOSPITAL LOS Rosenfeld EH, Naik-Mathuria B et al. Pediatr Surg Int 2019 Aug 35(8):861-7

Page 21
xxx00.#####.ppt 12/26/2019 10:45:39 AMSurgical ServicesTrauma Services
ERCP Use
• ERCP was used at 14/22 (64%) centers
• 20 patients with NOM, 6 with OM
0
1
2
3
4
5
6
7
8
9
1 2 3 4 5 6 7 8 9 10 11 12 13+
Days from Injury to ERCP
Rosenfeld EH, Naik-Mathuria B et al. J Pediatr Surg 2018;53(1):146-151

Page 22
xxx00.#####.ppt 12/26/2019 10:45:39 AMSurgical ServicesTrauma Services
Did ERCP Alter Management or Improve Outcome?
• 4/4 (100%) YES
• 3/3 (100%) YES
• 2/3 (67%) YES
• 3/11 (37%) YES
• 0/3 (0%) NO
• 2/2 UNCLEAR if outcome altered
• Evaluation of duct integrity (diagnostic only)
• Stricture
• Fistula control
• Early attempt at duct leak control
• Symptomatic pseudocyst
• Delayed attempt at duct leak control
82
1211
1714
DAYS TO REGULAR DIET DAYS ON TPN* LENGTH OF STAY
Observation Interventional ERCP

Page 23
xxx00.#####.ppt 12/26/2019 10:45:40 AMSurgical ServicesTrauma Services
Is MRCP Superior to CT?Rosenfeld EH, Naik-Mathuria B et al. Ped Surg Int 2018 Sept 34(9):961-6

Page 24
xxx00.#####.ppt 12/26/2019 10:45:40 AMSurgical ServicesTrauma Services
Avoid serial labs
Early oral feeding Avoid re-imaging until at least one
week
Initial observation
of pseudocyst
Discharge based on
symptoms, not labs
Naik-Mathuria et al. J Trauma Acute Care Surg 2017 83(4):589-596
“LESS IS MORE”

Page 25
xxx00.#####.ppt 12/26/2019 10:45:41 AMSurgical ServicesTrauma Services
Prospective, Multicenter Trial OM vs NOM
• Observational longitudinal cohort study
• 25 PTS pediatric trauma centers
• Acute grade III injuries
• Surgeon chooses OM vs NOM
• Standard clinical pathways
• Outcomes:
• Early and delayed complications
• Return to school
• Quality of life
• Readmissions
• Hospital costs

Page 26
xxx00.#####.ppt 12/26/2019 10:45:41 AMSurgical ServicesTrauma Services
Page 27
xxx00.#####.ppt 12/26/2019 10:45:41 AMSurgical ServicesTrauma Services
PRELIMINARY DATA
• 18 patients: 7 OM, 11 NOM
• Avg Time to Oral diet 2.4 days
• 1 day OM vs 3 days NOM
• Avg Length of Stay 8.8 days
• 7 days OM vs 10 days NOM

Page 28
xxx00.#####.ppt 12/26/2019 10:45:42 AMSurgical ServicesTrauma Services
MRCP performed
Mechanism ERCP performed

Page 29
xxx00.#####.ppt 12/26/2019 10:45:42 AMSurgical ServicesTrauma Services
Jejunal Feeds UseTPN Use
Peripancreatic fluid collection > 7 days after injury
Fistula development
NOYES
2 OM (28%) 2 NOM (18%)
1 PT WITH NOM HAD PANCREATIC INSUFFICIENCY 10 MONTHS AFTER INJURY
Page 30
xxx00.#####.ppt 12/26/2019 10:45:42 AMSurgical ServicesTrauma Services
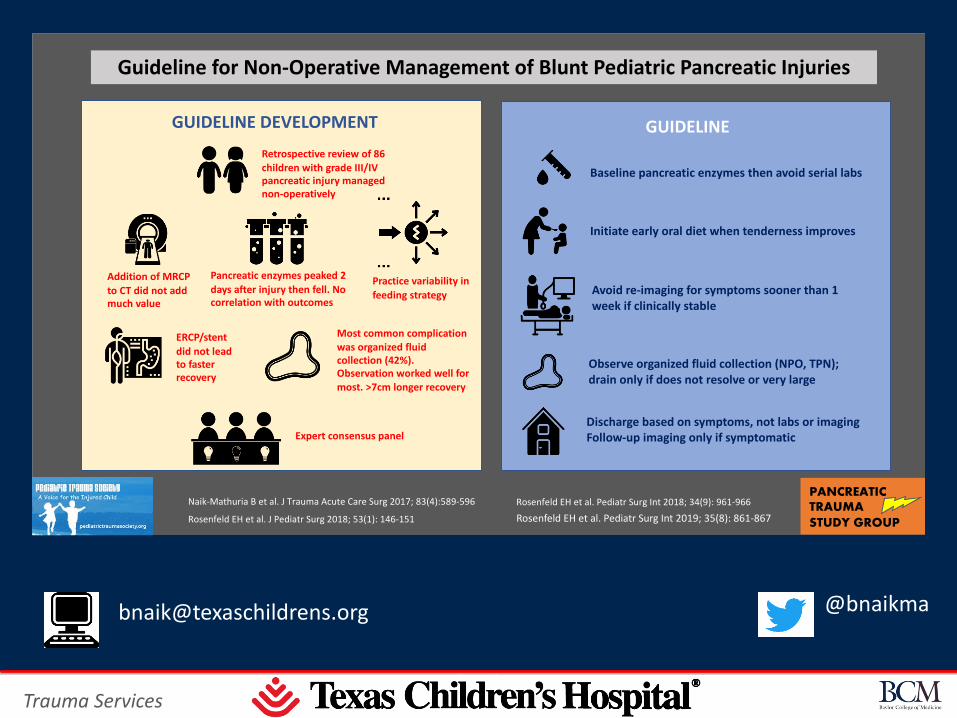
Guideline for Non-Operative Management of Blunt Pediatric Pancreatic Injuries
Retrospective review of 86 children with grade III/IV pancreatic injury managed non-operatively
Pancreatic enzymes peaked 2
days after injury then fell. No correlation with outcomes
Practice variability in
feeding strategy
Most common complication was organized fluid collection (42%). Observation worked well for most. >7cm longer recovery
ERCP/stent
did not lead to faster recovery
Expert consensus panel
GUIDELINE DEVELOPMENT
Baseline pancreatic enzymes then avoid serial labs
Initiate early oral diet when tenderness improves
Avoid re-imaging for symptoms sooner than 1 week if clinically stable
Observe organized fluid collection (NPO, TPN); drain only if does not resolve or very large
Discharge based on symptoms, not labs or imagingFollow-up imaging only if symptomatic
GUIDELINE
Naik-Mathuria B et al. J Trauma Acute Care Surg 2017; 83(4):589-596
Rosenfeld EH et al. J Pediatr Surg 2018; 53(1): 146-151 Rosenfeld EH et al. Pediatr Surg Int 2019; 35(8): 861-867
PANCREATIC TRAUMA STUDY GROUP
Rosenfeld EH et al. Pediatr Surg Int 2018; 34(9): 961-966
Addition of MRCP
to CT did not add much value