parenteral fish oil as a pharmacological agent to modulate post ... · of these effects as well as...
TRANSCRIPT
Parenteral fish oil as a pharmacological agent to modulate post-operative immune response: A randomized, double-blind,
and controlled clinical trial in patients with gastrointestinal cancer
Raquel Susana Matos de Miranda Torrinhas, Raquel Santana, Thaís Garcia, Maria Fernanda Cury-Boaventura,
Maria Mirtes Sales, Rui Curi,�Dan Linetzky Waitzberga
Clinical Nutrition 32 (2013) 503-510

Introduction
! Parenteral Nutrition (PN) ! An intravenous mixture containing multiple nutrients:
fluids, proteins, carbohydrates, fats, vitamins, and minerals. It may be used to provide full or partial nutrition to people who are not able to sustain their nutrition via the gastrointestinal tract.
! Fish Oil Lipid Emulsion (FOLE) ! Long-chain omega-3 polyunsaturated fatty acids (n-3
PUFA) consisting primarily of eicosapentanoic (EPA) and docosahexanoic (DHA) acids.

Introduction
! Benefits of PN-FOLE ! Avoids digestive and absorptive losses of n-3 PUFA’s ! Incorporates into plasma and blood cells at a faster
rate than enteral nutrition (EN) ! Induces an improved post-operative balance of
inflammatory mediators with a decrease in post-operative infection rates

Rationale
! Aim/Hypothesis ! To assess post-operative immune response after short-
term pre-operative parenteral infusion of isolated FOLE in gastrointestinal cancer patients
! Additional goals ! To assess post-operative duration of stay in ICU after
short-term pre-operative parenteral infusion of isolated FOLE in gastrointestinal cancer patients
! To assess patients with an additional risk of having complications ! Elderly age 60+ and/or malnourished patients

Methods
! Patients ! Adults ages 18-75 admitted for elective resection of
gastric or colon cancer ! 2 blocks of patients, 50 in each block ! Exclusions include
! Allergy to any ingredient of FOLE, infection (i.e. AIDS), inflammatory disease (i.e. arthritis), immunologic disease (i.e. lupus), metabolic disease (i.e. diabetes mellitus), dementia, and implanted electromagnetic instruments

Methods
! Lipid Treatment ! FOLE – Omegaven 10% ! Control Group – MCT/LCT – Lipovenos MCT 10% ! 3 days before surgery, 0.2g fat/kg of total body weight
of lipid emulsions (LEs) was continuously infused for 6h per day. Location of the exclusive peripheral venous access was changed daily.

Methods
! Inflammatory mediators ! IL-6 and IL-10 by ELISA ! CRP by imunoturbidimetric method ! prostaglandin E2 (PGE2) by Biotrack enzyme immune
assay system via spectrophotometer reader

Results
and hospital stay.10 The primary clinical endpoint was to assesspost-operative clinical outcome in all patients, but we also laterseparately assessed patients with an additional risk of havingcomplications, namely the elderly (age ! 60-years-old) and/ormalnourished patients [scored patient-generated-subjective globalassessment (PG-SGA)].11,12
2.6. Sample size and statistical analysis
The sample size (minimum of 28 patients per treatment) wascalculated by considering post-operative complications as themain clinical endpoint, a significance level of a ¼ 0.05, testpower of 80%, standard deviation of 30% of the arithmetic meanfor samples, and a difference of group means of 20% as thehighest average value. Statistical discussion was guided bya previous statistical plan supervised by a senior statistician(J.P.). For all statistical analyses, the significance level was set at5%. Demographic/descriptive data were compared betweentreatments by the Wilcoxon test for continuous variables andthe chi-squared test for categorical variables. Values andchanges in immunological data between the time of assessmentand type of treatment were evaluated by the Wilcoxon test.For leukocyte function, we grouped the different variablesprovided by each flow cytometry kit to describe an individualfunction (i.e., phagocytosis ¼ percentage of phagocytingmonocytes þ intensity of phagocyting monocytes þ percentageof phagocyting neutrophils þ intensity of phagocyting neutro-phils) and tested their compliance by using Cronbach’s alphatest. When leukocyte functions had compliances !50%, theywere treated as their respective Cronbach’s alpha scores, whichwere calculated from the arithmetic average of their standard-ized component variables, obtained by subtracting the meandivided by the standard deviation. Clinical data were comparedbetween treatments by the chi-squared and binomial tests. Forelderly and/or malnourished subgroup of patients we analyzedthe frequency of infectious complications and length of ICU andHospital stay by using Exact Binomial and F tests, respectively.Statistical analyses were conducted with SPSS 18.0 for Windows(SPSS, Chicago, IL, USA).
3. Results
3.1. Patients
Of the patients who met the inclusion criteria, 84 agreed toparticipate in the study. From these patients, 21 were excludedfrom the protocol for various reasons [voluntary withdraw notassociated with any discomfort or side effect of LE infusion (FO:n ¼ 3; MCT/LCT: n ¼ 4), voluntary withdrawal after reference ofabdominal pain and tachycardia (MCT/LCT: n ¼ 2), change ofsurgery date (FO: n ¼ 5; MCT/LCT: n ¼ 2), incomplete infusion of LE(FO: n ¼ 1; MCT/LCT: n ¼ 4)], and 63 patients completed theinfusion protocol [FO (n ¼ 31) and MCT/LCT (n ¼ 32)]. However, 2patients who completed the MCT/LCT infusion protocol died post-operatively after a) septic shock during the immediate post-oper-ative period as a result of anastomotic dehiscence; and b) infectionand septic shock, caused by self-inflicted lesion at the surgicalwound. These patients were not assessed for clinical variables,except patient b, whose duration of ICU stay was assessed becausehe experienced the complication during his stay in the ward. ACONSORT diagram shows the flow of participant’s assignment andanalysis (Fig. 1). The study groups were adequately matched fordescriptive characteristics of demography, tumor site, and type ofsurgery (Table 1). For the patients where immunological markerswere assessed, there was no significant difference in baselinevalues, except for IL-6, which was higher in FO patients than inMCT/LCT patients, and IL-10, which was higher in MCT/LCT patientsthan in FO patients (Table 2).
3.2. Immune response markers
Changes in immunological measurements that occurred withinthe same group of patients in relation to their baseline values areshown in Fig. 2. In addition, Table 3 shows changes and p valuesthat occurred in immunological measurements during the studyperiod between FO andMCT/LCT patients. After infusion and beforethe surgery (T1), FO patients exhibited a decrease in IL-6 levels(p ¼ 0.018) and MCT/LCT patients demonstrated an increase in IL-6(p ¼ 0.003) and IL-10 (p ¼ 0.053) levels compared to baseline
Fig. 1. CONSORT diagram of gastrointestinal cancer patient’s randomization to receive 3 days of pre-operative peripheral infusion of a fish oil parenteral lipid emulsion (FO) that wasrich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chain triglycerides.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 505

Results
immune response.18 The effect of fish oil LE supplementation insurgical patients under PN is often compared to LEs based onsoybean oil as a control. However, soybean oil LEs are rich in n-6PUFA, and therefore they are potentially inflammatory and immu-nosuppressive. In surgical patients, MCT/LCT has been shown toprevent abdominal abscesses and improve or maintain immuneresponse markers compared to soybean oil LE.19e21
Changes in immune response to the surgical trauma are markedby increased production of both pro-inflammatory and anti-inflammatory mediators. Therefore, we evaluated key mediatorsof these effects as well as leukocyte functions and surface mole-cules that may be influenced by their imbalance in order to identifytargets of post-operative immune response that could be modu-lated by fish oil LE.
We found that the post-operative plasma concentration of IL-6 was decreased in patients treated with fish oil LE compared topatients treated with control LE. In agreement with this finding,previous studies have shown that surgical patients under
standard PN also presented decreased post-operative levels ofserum IL-6 after the supplementation with LE containing fish oilcompared to pure soybean oil LE.22,23 However, it was hypothe-sized that the post-operative decrease of IL-6 levels observed inthese studies may be a consequence of the n-6 PUFA infusion,which is present in large amounts in the LE soybean oil used asa control. Omega-6 PUFAs are precursors of the pro-inflammatory leukotriene (LT) B4, which has been experimen-tally associated with a dose-dependent accumulation of IL-6mRNA and cytokine release, while omega-3 PUFAs competewith the same enzymatic pathways for the less inflammatoryLTB5 synthesis.24
The control LE used in our study contains 50% less omega-6PUFA than soybean oil LE, and therefore we suggest that thedecreased post-operative levels of IL-6 found may be due to thehigh content of n-3 PUFA provided by fish oil LE rather than thedecrease of omega-6 PUFAs. In addition, our findings supportrecent studies that have also shown decreased IL-6 levels in surgical
Fig. 2. Intra-group changes (mean ! standard error) of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3 days witha peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chaintriglycerides. Wilcoxon test, Up < 0.05 vs. T0, for FO patients; *p < 0.05 vs. T0, for MCT/LCT patients.
Table 3Inter-group changes in the mean of the difference in variation of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3days with a peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich inmedium-chain triglycerides. Data are expressed as mean ! standard deviation and analyzed by the Wilcoxon test.
Immunological marker Group T1eT0 P value T2eT0 P value T3eT0 P value
Interleukin-6 FO "0.05 ! 0.30 <0.0001* 0.09 ! 0.52 0.029* 0.22 ! 0.60 0.202MCT/LCT 0.15 ! 0.26 1.29 ! 1.18 0.60 ! 0.99
Interleukin-10 FO "0.005 ! 0.05 0.019* 0.76 ! 0.32 <0.0001* "0.07 ! 0.13 <0.0001*MCT/LCT 0.01 ! 0.03 "0.10 ! 0.03 0.20 ! 0.04
Oxidative burst FO "0.08 ! 0.65 0.632 "0.96 ! 0.70 0.028* e e
MCT/LCT 0.11 ! 0.78 "1.16 ! 0.73 e
Percentage HLA-DR (Mf) FO 2.67 ! 15.94 0.464 "2.31 ! 7.83 0.046* e e
MCT/LCT "8.11 ! 31.20 "15.86 ! 18.92 e
Percentage CD32 (Mf) FO 1.17 ! 12.98 0.253 0.19 ! 12.48 0.025* e e
MCT/LCT "4.96 ! 7.84 "15.11 ! 16.72 e
Intensity CD32 (Nf) FO "0.14 ! 99.87 0.200 65.00 ! 138.84 0.010* e e
MCT/LCT "1.23 ! 35.68 20.26 ! 91.61 e
Mf ¼ Monocytes; Nf ¼ Neutrophils.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 507
immune response.18 The effect of fish oil LE supplementation insurgical patients under PN is often compared to LEs based onsoybean oil as a control. However, soybean oil LEs are rich in n-6PUFA, and therefore they are potentially inflammatory and immu-nosuppressive. In surgical patients, MCT/LCT has been shown toprevent abdominal abscesses and improve or maintain immuneresponse markers compared to soybean oil LE.19e21
Changes in immune response to the surgical trauma are markedby increased production of both pro-inflammatory and anti-inflammatory mediators. Therefore, we evaluated key mediatorsof these effects as well as leukocyte functions and surface mole-cules that may be influenced by their imbalance in order to identifytargets of post-operative immune response that could be modu-lated by fish oil LE.
We found that the post-operative plasma concentration of IL-6 was decreased in patients treated with fish oil LE compared topatients treated with control LE. In agreement with this finding,previous studies have shown that surgical patients under
standard PN also presented decreased post-operative levels ofserum IL-6 after the supplementation with LE containing fish oilcompared to pure soybean oil LE.22,23 However, it was hypothe-sized that the post-operative decrease of IL-6 levels observed inthese studies may be a consequence of the n-6 PUFA infusion,which is present in large amounts in the LE soybean oil used asa control. Omega-6 PUFAs are precursors of the pro-inflammatory leukotriene (LT) B4, which has been experimen-tally associated with a dose-dependent accumulation of IL-6mRNA and cytokine release, while omega-3 PUFAs competewith the same enzymatic pathways for the less inflammatoryLTB5 synthesis.24
The control LE used in our study contains 50% less omega-6PUFA than soybean oil LE, and therefore we suggest that thedecreased post-operative levels of IL-6 found may be due to thehigh content of n-3 PUFA provided by fish oil LE rather than thedecrease of omega-6 PUFAs. In addition, our findings supportrecent studies that have also shown decreased IL-6 levels in surgical
Fig. 2. Intra-group changes (mean ! standard error) of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3 days witha peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chaintriglycerides. Wilcoxon test, Up < 0.05 vs. T0, for FO patients; *p < 0.05 vs. T0, for MCT/LCT patients.
Table 3Inter-group changes in the mean of the difference in variation of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3days with a peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich inmedium-chain triglycerides. Data are expressed as mean ! standard deviation and analyzed by the Wilcoxon test.
Immunological marker Group T1eT0 P value T2eT0 P value T3eT0 P value
Interleukin-6 FO "0.05 ! 0.30 <0.0001* 0.09 ! 0.52 0.029* 0.22 ! 0.60 0.202MCT/LCT 0.15 ! 0.26 1.29 ! 1.18 0.60 ! 0.99
Interleukin-10 FO "0.005 ! 0.05 0.019* 0.76 ! 0.32 <0.0001* "0.07 ! 0.13 <0.0001*MCT/LCT 0.01 ! 0.03 "0.10 ! 0.03 0.20 ! 0.04
Oxidative burst FO "0.08 ! 0.65 0.632 "0.96 ! 0.70 0.028* e e
MCT/LCT 0.11 ! 0.78 "1.16 ! 0.73 e
Percentage HLA-DR (Mf) FO 2.67 ! 15.94 0.464 "2.31 ! 7.83 0.046* e e
MCT/LCT "8.11 ! 31.20 "15.86 ! 18.92 e
Percentage CD32 (Mf) FO 1.17 ! 12.98 0.253 0.19 ! 12.48 0.025* e e
MCT/LCT "4.96 ! 7.84 "15.11 ! 16.72 e
Intensity CD32 (Nf) FO "0.14 ! 99.87 0.200 65.00 ! 138.84 0.010* e e
MCT/LCT "1.23 ! 35.68 20.26 ! 91.61 e
Mf ¼ Monocytes; Nf ¼ Neutrophils.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 507
t0 = start of infusion, t1 = pre-operative post-infusion, t2 = post-operative day 3, t3 = post-operative day 6

Results
immune response.18 The effect of fish oil LE supplementation insurgical patients under PN is often compared to LEs based onsoybean oil as a control. However, soybean oil LEs are rich in n-6PUFA, and therefore they are potentially inflammatory and immu-nosuppressive. In surgical patients, MCT/LCT has been shown toprevent abdominal abscesses and improve or maintain immuneresponse markers compared to soybean oil LE.19e21
Changes in immune response to the surgical trauma are markedby increased production of both pro-inflammatory and anti-inflammatory mediators. Therefore, we evaluated key mediatorsof these effects as well as leukocyte functions and surface mole-cules that may be influenced by their imbalance in order to identifytargets of post-operative immune response that could be modu-lated by fish oil LE.
We found that the post-operative plasma concentration of IL-6 was decreased in patients treated with fish oil LE compared topatients treated with control LE. In agreement with this finding,previous studies have shown that surgical patients under
standard PN also presented decreased post-operative levels ofserum IL-6 after the supplementation with LE containing fish oilcompared to pure soybean oil LE.22,23 However, it was hypothe-sized that the post-operative decrease of IL-6 levels observed inthese studies may be a consequence of the n-6 PUFA infusion,which is present in large amounts in the LE soybean oil used asa control. Omega-6 PUFAs are precursors of the pro-inflammatory leukotriene (LT) B4, which has been experimen-tally associated with a dose-dependent accumulation of IL-6mRNA and cytokine release, while omega-3 PUFAs competewith the same enzymatic pathways for the less inflammatoryLTB5 synthesis.24
The control LE used in our study contains 50% less omega-6PUFA than soybean oil LE, and therefore we suggest that thedecreased post-operative levels of IL-6 found may be due to thehigh content of n-3 PUFA provided by fish oil LE rather than thedecrease of omega-6 PUFAs. In addition, our findings supportrecent studies that have also shown decreased IL-6 levels in surgical
Fig. 2. Intra-group changes (mean ! standard error) of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3 days witha peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chaintriglycerides. Wilcoxon test, Up < 0.05 vs. T0, for FO patients; *p < 0.05 vs. T0, for MCT/LCT patients.
Table 3Inter-group changes in the mean of the difference in variation of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3days with a peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich inmedium-chain triglycerides. Data are expressed as mean ! standard deviation and analyzed by the Wilcoxon test.
Immunological marker Group T1eT0 P value T2eT0 P value T3eT0 P value
Interleukin-6 FO "0.05 ! 0.30 <0.0001* 0.09 ! 0.52 0.029* 0.22 ! 0.60 0.202MCT/LCT 0.15 ! 0.26 1.29 ! 1.18 0.60 ! 0.99
Interleukin-10 FO "0.005 ! 0.05 0.019* 0.76 ! 0.32 <0.0001* "0.07 ! 0.13 <0.0001*MCT/LCT 0.01 ! 0.03 "0.10 ! 0.03 0.20 ! 0.04
Oxidative burst FO "0.08 ! 0.65 0.632 "0.96 ! 0.70 0.028* e e
MCT/LCT 0.11 ! 0.78 "1.16 ! 0.73 e
Percentage HLA-DR (Mf) FO 2.67 ! 15.94 0.464 "2.31 ! 7.83 0.046* e e
MCT/LCT "8.11 ! 31.20 "15.86 ! 18.92 e
Percentage CD32 (Mf) FO 1.17 ! 12.98 0.253 0.19 ! 12.48 0.025* e e
MCT/LCT "4.96 ! 7.84 "15.11 ! 16.72 e
Intensity CD32 (Nf) FO "0.14 ! 99.87 0.200 65.00 ! 138.84 0.010* e e
MCT/LCT "1.23 ! 35.68 20.26 ! 91.61 e
Mf ¼ Monocytes; Nf ¼ Neutrophils.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 507
t0 = start of infusion, t1 = pre-operative post-infusion, t2 = post-operative day 3, t3 = post-operative day 6

Results
immune response.18 The effect of fish oil LE supplementation insurgical patients under PN is often compared to LEs based onsoybean oil as a control. However, soybean oil LEs are rich in n-6PUFA, and therefore they are potentially inflammatory and immu-nosuppressive. In surgical patients, MCT/LCT has been shown toprevent abdominal abscesses and improve or maintain immuneresponse markers compared to soybean oil LE.19e21
Changes in immune response to the surgical trauma are markedby increased production of both pro-inflammatory and anti-inflammatory mediators. Therefore, we evaluated key mediatorsof these effects as well as leukocyte functions and surface mole-cules that may be influenced by their imbalance in order to identifytargets of post-operative immune response that could be modu-lated by fish oil LE.
We found that the post-operative plasma concentration of IL-6 was decreased in patients treated with fish oil LE compared topatients treated with control LE. In agreement with this finding,previous studies have shown that surgical patients under
standard PN also presented decreased post-operative levels ofserum IL-6 after the supplementation with LE containing fish oilcompared to pure soybean oil LE.22,23 However, it was hypothe-sized that the post-operative decrease of IL-6 levels observed inthese studies may be a consequence of the n-6 PUFA infusion,which is present in large amounts in the LE soybean oil used asa control. Omega-6 PUFAs are precursors of the pro-inflammatory leukotriene (LT) B4, which has been experimen-tally associated with a dose-dependent accumulation of IL-6mRNA and cytokine release, while omega-3 PUFAs competewith the same enzymatic pathways for the less inflammatoryLTB5 synthesis.24
The control LE used in our study contains 50% less omega-6PUFA than soybean oil LE, and therefore we suggest that thedecreased post-operative levels of IL-6 found may be due to thehigh content of n-3 PUFA provided by fish oil LE rather than thedecrease of omega-6 PUFAs. In addition, our findings supportrecent studies that have also shown decreased IL-6 levels in surgical
Fig. 2. Intra-group changes (mean ! standard error) of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3 days witha peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chaintriglycerides. Wilcoxon test, Up < 0.05 vs. T0, for FO patients; *p < 0.05 vs. T0, for MCT/LCT patients.
Table 3Inter-group changes in the mean of the difference in variation of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3days with a peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich inmedium-chain triglycerides. Data are expressed as mean ! standard deviation and analyzed by the Wilcoxon test.
Immunological marker Group T1eT0 P value T2eT0 P value T3eT0 P value
Interleukin-6 FO "0.05 ! 0.30 <0.0001* 0.09 ! 0.52 0.029* 0.22 ! 0.60 0.202MCT/LCT 0.15 ! 0.26 1.29 ! 1.18 0.60 ! 0.99
Interleukin-10 FO "0.005 ! 0.05 0.019* 0.76 ! 0.32 <0.0001* "0.07 ! 0.13 <0.0001*MCT/LCT 0.01 ! 0.03 "0.10 ! 0.03 0.20 ! 0.04
Oxidative burst FO "0.08 ! 0.65 0.632 "0.96 ! 0.70 0.028* e e
MCT/LCT 0.11 ! 0.78 "1.16 ! 0.73 e
Percentage HLA-DR (Mf) FO 2.67 ! 15.94 0.464 "2.31 ! 7.83 0.046* e e
MCT/LCT "8.11 ! 31.20 "15.86 ! 18.92 e
Percentage CD32 (Mf) FO 1.17 ! 12.98 0.253 0.19 ! 12.48 0.025* e e
MCT/LCT "4.96 ! 7.84 "15.11 ! 16.72 e
Intensity CD32 (Nf) FO "0.14 ! 99.87 0.200 65.00 ! 138.84 0.010* e e
MCT/LCT "1.23 ! 35.68 20.26 ! 91.61 e
Mf ¼ Monocytes; Nf ¼ Neutrophils.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 507
t0 = start of infusion, t1 = pre-operative post-infusion, t2 = post-operative day 3, t3 = post-operative day 6

Results
immune response.18 The effect of fish oil LE supplementation insurgical patients under PN is often compared to LEs based onsoybean oil as a control. However, soybean oil LEs are rich in n-6PUFA, and therefore they are potentially inflammatory and immu-nosuppressive. In surgical patients, MCT/LCT has been shown toprevent abdominal abscesses and improve or maintain immuneresponse markers compared to soybean oil LE.19e21
Changes in immune response to the surgical trauma are markedby increased production of both pro-inflammatory and anti-inflammatory mediators. Therefore, we evaluated key mediatorsof these effects as well as leukocyte functions and surface mole-cules that may be influenced by their imbalance in order to identifytargets of post-operative immune response that could be modu-lated by fish oil LE.
We found that the post-operative plasma concentration of IL-6 was decreased in patients treated with fish oil LE compared topatients treated with control LE. In agreement with this finding,previous studies have shown that surgical patients under
standard PN also presented decreased post-operative levels ofserum IL-6 after the supplementation with LE containing fish oilcompared to pure soybean oil LE.22,23 However, it was hypothe-sized that the post-operative decrease of IL-6 levels observed inthese studies may be a consequence of the n-6 PUFA infusion,which is present in large amounts in the LE soybean oil used asa control. Omega-6 PUFAs are precursors of the pro-inflammatory leukotriene (LT) B4, which has been experimen-tally associated with a dose-dependent accumulation of IL-6mRNA and cytokine release, while omega-3 PUFAs competewith the same enzymatic pathways for the less inflammatoryLTB5 synthesis.24
The control LE used in our study contains 50% less omega-6PUFA than soybean oil LE, and therefore we suggest that thedecreased post-operative levels of IL-6 found may be due to thehigh content of n-3 PUFA provided by fish oil LE rather than thedecrease of omega-6 PUFAs. In addition, our findings supportrecent studies that have also shown decreased IL-6 levels in surgical
Fig. 2. Intra-group changes (mean ! standard error) of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3 days witha peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chaintriglycerides. Wilcoxon test, Up < 0.05 vs. T0, for FO patients; *p < 0.05 vs. T0, for MCT/LCT patients.
Table 3Inter-group changes in the mean of the difference in variation of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3days with a peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich inmedium-chain triglycerides. Data are expressed as mean ! standard deviation and analyzed by the Wilcoxon test.
Immunological marker Group T1eT0 P value T2eT0 P value T3eT0 P value
Interleukin-6 FO "0.05 ! 0.30 <0.0001* 0.09 ! 0.52 0.029* 0.22 ! 0.60 0.202MCT/LCT 0.15 ! 0.26 1.29 ! 1.18 0.60 ! 0.99
Interleukin-10 FO "0.005 ! 0.05 0.019* 0.76 ! 0.32 <0.0001* "0.07 ! 0.13 <0.0001*MCT/LCT 0.01 ! 0.03 "0.10 ! 0.03 0.20 ! 0.04
Oxidative burst FO "0.08 ! 0.65 0.632 "0.96 ! 0.70 0.028* e e
MCT/LCT 0.11 ! 0.78 "1.16 ! 0.73 e
Percentage HLA-DR (Mf) FO 2.67 ! 15.94 0.464 "2.31 ! 7.83 0.046* e e
MCT/LCT "8.11 ! 31.20 "15.86 ! 18.92 e
Percentage CD32 (Mf) FO 1.17 ! 12.98 0.253 0.19 ! 12.48 0.025* e e
MCT/LCT "4.96 ! 7.84 "15.11 ! 16.72 e
Intensity CD32 (Nf) FO "0.14 ! 99.87 0.200 65.00 ! 138.84 0.010* e e
MCT/LCT "1.23 ! 35.68 20.26 ! 91.61 e
Mf ¼ Monocytes; Nf ¼ Neutrophils.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 507
t0 = start of infusion, t1 = pre-operative post-infusion, t2 = post-operative day 3, t3 = post-operative day 6

Results
immune response.18 The effect of fish oil LE supplementation insurgical patients under PN is often compared to LEs based onsoybean oil as a control. However, soybean oil LEs are rich in n-6PUFA, and therefore they are potentially inflammatory and immu-nosuppressive. In surgical patients, MCT/LCT has been shown toprevent abdominal abscesses and improve or maintain immuneresponse markers compared to soybean oil LE.19e21
Changes in immune response to the surgical trauma are markedby increased production of both pro-inflammatory and anti-inflammatory mediators. Therefore, we evaluated key mediatorsof these effects as well as leukocyte functions and surface mole-cules that may be influenced by their imbalance in order to identifytargets of post-operative immune response that could be modu-lated by fish oil LE.
We found that the post-operative plasma concentration of IL-6 was decreased in patients treated with fish oil LE compared topatients treated with control LE. In agreement with this finding,previous studies have shown that surgical patients under
standard PN also presented decreased post-operative levels ofserum IL-6 after the supplementation with LE containing fish oilcompared to pure soybean oil LE.22,23 However, it was hypothe-sized that the post-operative decrease of IL-6 levels observed inthese studies may be a consequence of the n-6 PUFA infusion,which is present in large amounts in the LE soybean oil used asa control. Omega-6 PUFAs are precursors of the pro-inflammatory leukotriene (LT) B4, which has been experimen-tally associated with a dose-dependent accumulation of IL-6mRNA and cytokine release, while omega-3 PUFAs competewith the same enzymatic pathways for the less inflammatoryLTB5 synthesis.24
The control LE used in our study contains 50% less omega-6PUFA than soybean oil LE, and therefore we suggest that thedecreased post-operative levels of IL-6 found may be due to thehigh content of n-3 PUFA provided by fish oil LE rather than thedecrease of omega-6 PUFAs. In addition, our findings supportrecent studies that have also shown decreased IL-6 levels in surgical
Fig. 2. Intra-group changes (mean ! standard error) of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3 days witha peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chaintriglycerides. Wilcoxon test, Up < 0.05 vs. T0, for FO patients; *p < 0.05 vs. T0, for MCT/LCT patients.
Table 3Inter-group changes in the mean of the difference in variation of immunological markers from patients with gastrointestinal cancer who were pre-operatively treated for 3days with a peripheral infusion of a fish oil parenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich inmedium-chain triglycerides. Data are expressed as mean ! standard deviation and analyzed by the Wilcoxon test.
Immunological marker Group T1eT0 P value T2eT0 P value T3eT0 P value
Interleukin-6 FO "0.05 ! 0.30 <0.0001* 0.09 ! 0.52 0.029* 0.22 ! 0.60 0.202MCT/LCT 0.15 ! 0.26 1.29 ! 1.18 0.60 ! 0.99
Interleukin-10 FO "0.005 ! 0.05 0.019* 0.76 ! 0.32 <0.0001* "0.07 ! 0.13 <0.0001*MCT/LCT 0.01 ! 0.03 "0.10 ! 0.03 0.20 ! 0.04
Oxidative burst FO "0.08 ! 0.65 0.632 "0.96 ! 0.70 0.028* e e
MCT/LCT 0.11 ! 0.78 "1.16 ! 0.73 e
Percentage HLA-DR (Mf) FO 2.67 ! 15.94 0.464 "2.31 ! 7.83 0.046* e e
MCT/LCT "8.11 ! 31.20 "15.86 ! 18.92 e
Percentage CD32 (Mf) FO 1.17 ! 12.98 0.253 0.19 ! 12.48 0.025* e e
MCT/LCT "4.96 ! 7.84 "15.11 ! 16.72 e
Intensity CD32 (Nf) FO "0.14 ! 99.87 0.200 65.00 ! 138.84 0.010* e e
MCT/LCT "1.23 ! 35.68 20.26 ! 91.61 e
Mf ¼ Monocytes; Nf ¼ Neutrophils.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510 507
Results
patients treated post-operatively with fish oil LE compared to MCT/LCT and olive oil-based LEs.25e27
We also assessed the post-operative levels of CRP, which isa hepatic pro-inflammatory component of immune responseregulated by IL-6. Accordingly, post-operative CRP significantlyincreased only in patients treated with the control LE, but no-different post-operative levels of this mediator were observedbetween both studied groups. In agreement with our data, Badía-Tahull et al. did not find between treatment-changes in the post-operative levels of CRP of surgical patients receiving fish oil-supplemented PN compared to a standard olive oil-based LE.28
The post-operative plasma concentration of IL-10 was alsoassessed as an anti-inflammatory marker in this study. Post-oper-ative production of IL-10 is desirable for controlling hyper-inflammation, but the persistence of high levels of this cytokinecan adversely contribute to immune paralysis. Overexpression ofIL-10 has been correlatedwith decreased post-operative expressionof HLA-DR on monocytes, which is considered to be a centralmarker of immune paralysis after surgical trauma.29
Our data suggest that treatment of patients with fish oil LEinduces favorable post-operative physiological modulation of IL-10concentrations, with an increase in the cytokine on the 3rd post-operative day followed by a decreased by the 6th post-operativeday. Previous studies did not detect changes in post-operativelevels of IL-10 after post-operative infusion of fish oil LE comparedto both soybean oil LE and MCT/LCT. These observations suggestthat the period of parenteral infusion of fish oil LE may be impor-tant for detecting changes in post-operative levels of IL-10. Inaddition, while our patients treated with control LE had decreasedpost-operative monocytes expressing HLA-DR, patients treatedwith fish oil LE maintained this immunological marker at baselinelevels. Our data are in agreement with the findings of Weiss et al.who showed that PN with fish oil LE maintained the post-operativeexpression of leukocyte HLA-DR, which was decreased in patientsthat received the infusion of PN with soybean oil LE.23
A decrease in the number of HLA-DR positive monocytes indi-cates the functional deactivation of these leukocytes, which isconsidered to be a centralmarker of immune paralysis after surgicaltrauma.29 In fact, the decrease in the number of monocytesexpressing HLA-DR in our study was accompanied by a decrease inthe number of monocytes expressing CD32 and decreased oxidativeburst in patients treated with control LE, while fish oil LE preservedthese leukocyte phenotype markers and reduced the negativeimpact on oxidative burst function. Decreased leukocyte oxidativeburst as well as HLA-DR and CD32 expression on monocytes arefrequently observed after surgical trauma and are associated withpost-operative infectious and non-infectious complications.Therefore, our immunological data suggest that pre-operativeinfusion of fish oil LE may contribute to improve clinical outcomes.
Our original primary clinical endpoint was to evaluate thefrequency of post-operative infections and the length of ICU and
hospital stay of surgical patients treated with pure fish oil LE.There were not significant differences between treatment andcontrol groups, in contrast to previous studies assessingparenteral regimens supplemented with fish oil LE.6 Helleret al., in surgical patients treated with parenteral regimenssupplemented with fish oil LE, observed a tendency of shorterICU stays only in those patients with sepsis risk after stratifi-cation of total patient population in “higher risk groups”.30
Based on this previous study, we further analyzed (post-hoc)clinical outcome separately for more susceptible elderly (!60years of age) and/or malnourished patients.31,32 A smallervariation of length of ICU stay was observed in this subgroup ofpatients treated with fish oil LE, in relation to control LE. Theseclinical data may support previous evidence by Heller et al.showing the benefit of treating debilitated patients undergoingmajor cancer surgery with fish oil LE in order to improve clinicaloutcomes.29 Therefore, additional studies are needed to explorethis issue.
This study had several limitations. It included only adultsurgical patients with gastrointestinal cancer and similar resultsmay therefore not be achieved in other surgical groups. Patientswere included without consideration of their nutritional status oralimentary habits (even antioxidants consume) because the maincontribution of our study was to assess whether, regardless thesenutritional factors, post-operative immune response couldbenefit from pre-operative infusion of fish oil LE. At baseline our
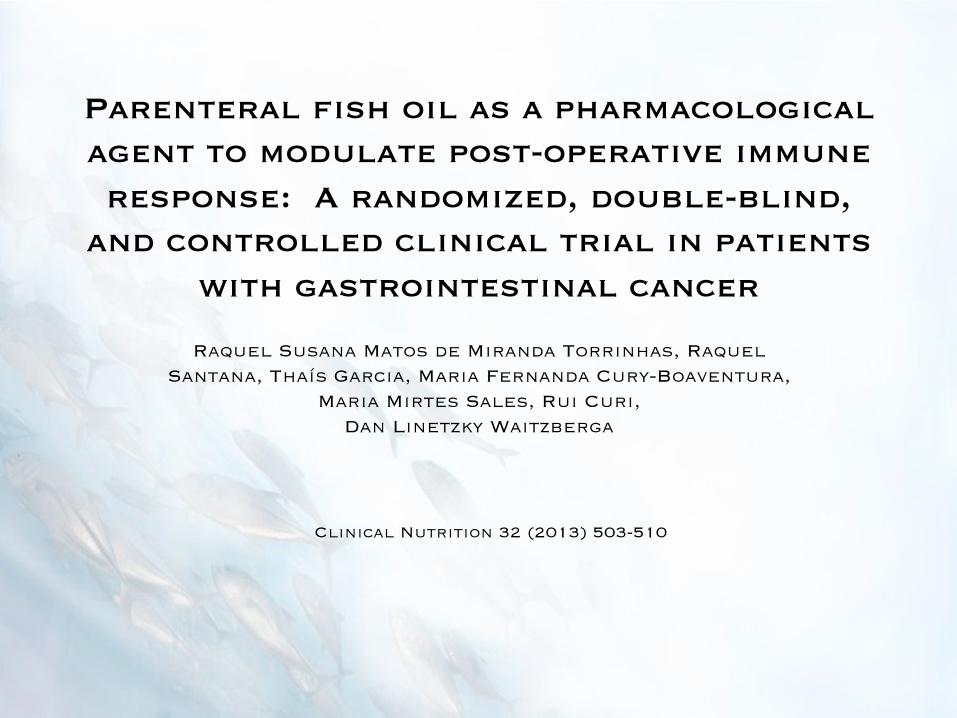
Table 4Immediate post-operative clinical outcomes of patients with gastrointestinal cancer who were pre-operatively treated for 3 days with a peripheral infusion of a fish oilparenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chain triglycerides.
Lipid emulsion Complications (%) Length of stay (mean of days " standard deviation)
Infectious Intensive care unity Hospital
T R T R T R
FO 6.5a 10a 1.1 " 0.23 1 " 0.37 11.29 " 1.14 10.85 " 1.31MCT/LCT 15.6b 27.8b 1.6 " 0.50 2.41 " 1.02 12 " 1.29 13.38 " 1.97p value 0.426 0.222 0.826 0.228 0.844 0.395
T: total patient; R: patient with additional risk (elderly and/or malnourished).a Local surgical wound (n ¼ 1) and pneumonia (n ¼ 1).b Local surgical wound (n ¼ 3) and sepsis (n ¼ 2).
Fig. 3. Variation (95% confidence interval e C.I.) of intensive care unit (ICU) dischargeof elderly and/or malnourished surgical patients with gastrointestinal cancer whowere pre-operatively treated for 3 days with a peripheral infusion of a fish oilparenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a controlparenteral lipid emulsion (MCT/LCT) that was rich in medium-chain triglycerides.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510508
patients treated post-operatively with fish oil LE compared to MCT/LCT and olive oil-based LEs.25e27
We also assessed the post-operative levels of CRP, which isa hepatic pro-inflammatory component of immune responseregulated by IL-6. Accordingly, post-operative CRP significantlyincreased only in patients treated with the control LE, but no-different post-operative levels of this mediator were observedbetween both studied groups. In agreement with our data, Badía-Tahull et al. did not find between treatment-changes in the post-operative levels of CRP of surgical patients receiving fish oil-supplemented PN compared to a standard olive oil-based LE.28
The post-operative plasma concentration of IL-10 was alsoassessed as an anti-inflammatory marker in this study. Post-oper-ative production of IL-10 is desirable for controlling hyper-inflammation, but the persistence of high levels of this cytokinecan adversely contribute to immune paralysis. Overexpression ofIL-10 has been correlatedwith decreased post-operative expressionof HLA-DR on monocytes, which is considered to be a centralmarker of immune paralysis after surgical trauma.29
Our data suggest that treatment of patients with fish oil LEinduces favorable post-operative physiological modulation of IL-10concentrations, with an increase in the cytokine on the 3rd post-operative day followed by a decreased by the 6th post-operativeday. Previous studies did not detect changes in post-operativelevels of IL-10 after post-operative infusion of fish oil LE comparedto both soybean oil LE and MCT/LCT. These observations suggestthat the period of parenteral infusion of fish oil LE may be impor-tant for detecting changes in post-operative levels of IL-10. Inaddition, while our patients treated with control LE had decreasedpost-operative monocytes expressing HLA-DR, patients treatedwith fish oil LE maintained this immunological marker at baselinelevels. Our data are in agreement with the findings of Weiss et al.who showed that PN with fish oil LE maintained the post-operativeexpression of leukocyte HLA-DR, which was decreased in patientsthat received the infusion of PN with soybean oil LE.23
A decrease in the number of HLA-DR positive monocytes indi-cates the functional deactivation of these leukocytes, which isconsidered to be a centralmarker of immune paralysis after surgicaltrauma.29 In fact, the decrease in the number of monocytesexpressing HLA-DR in our study was accompanied by a decrease inthe number of monocytes expressing CD32 and decreased oxidativeburst in patients treated with control LE, while fish oil LE preservedthese leukocyte phenotype markers and reduced the negativeimpact on oxidative burst function. Decreased leukocyte oxidativeburst as well as HLA-DR and CD32 expression on monocytes arefrequently observed after surgical trauma and are associated withpost-operative infectious and non-infectious complications.Therefore, our immunological data suggest that pre-operativeinfusion of fish oil LE may contribute to improve clinical outcomes.
Our original primary clinical endpoint was to evaluate thefrequency of post-operative infections and the length of ICU and
hospital stay of surgical patients treated with pure fish oil LE.There were not significant differences between treatment andcontrol groups, in contrast to previous studies assessingparenteral regimens supplemented with fish oil LE.6 Helleret al., in surgical patients treated with parenteral regimenssupplemented with fish oil LE, observed a tendency of shorterICU stays only in those patients with sepsis risk after stratifi-cation of total patient population in “higher risk groups”.30
Based on this previous study, we further analyzed (post-hoc)clinical outcome separately for more susceptible elderly (!60years of age) and/or malnourished patients.31,32 A smallervariation of length of ICU stay was observed in this subgroup ofpatients treated with fish oil LE, in relation to control LE. Theseclinical data may support previous evidence by Heller et al.showing the benefit of treating debilitated patients undergoingmajor cancer surgery with fish oil LE in order to improve clinicaloutcomes.29 Therefore, additional studies are needed to explorethis issue.
This study had several limitations. It included only adultsurgical patients with gastrointestinal cancer and similar resultsmay therefore not be achieved in other surgical groups. Patientswere included without consideration of their nutritional status oralimentary habits (even antioxidants consume) because the maincontribution of our study was to assess whether, regardless thesenutritional factors, post-operative immune response couldbenefit from pre-operative infusion of fish oil LE. At baseline our
Table 4Immediate post-operative clinical outcomes of patients with gastrointestinal cancer who were pre-operatively treated for 3 days with a peripheral infusion of a fish oilparenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a control parenteral lipid emulsion (MCT/LCT) that was rich in medium-chain triglycerides.
Lipid emulsion Complications (%) Length of stay (mean of days " standard deviation)
Infectious Intensive care unity Hospital
T R T R T R
FO 6.5a 10a 1.1 " 0.23 1 " 0.37 11.29 " 1.14 10.85 " 1.31MCT/LCT 15.6b 27.8b 1.6 " 0.50 2.41 " 1.02 12 " 1.29 13.38 " 1.97p value 0.426 0.222 0.826 0.228 0.844 0.395
T: total patient; R: patient with additional risk (elderly and/or malnourished).a Local surgical wound (n ¼ 1) and pneumonia (n ¼ 1).b Local surgical wound (n ¼ 3) and sepsis (n ¼ 2).
Fig. 3. Variation (95% confidence interval e C.I.) of intensive care unit (ICU) dischargeof elderly and/or malnourished surgical patients with gastrointestinal cancer whowere pre-operatively treated for 3 days with a peripheral infusion of a fish oilparenteral lipid emulsion (FO) that was rich in omega-3 fatty acids, or a controlparenteral lipid emulsion (MCT/LCT) that was rich in medium-chain triglycerides.
R.S.M. de Miranda Torrinhas et al. / Clinical Nutrition 32 (2013) 503e510508

Discussion/Conclusions
! Favorable modulation of post-operative immune mediators ! Preserved or improved leukocyte phenotype
! Rapid immune function modulation with improved clinical outcomes
! Low adverse effects of infusion ! Nausea, vomiting, local phlebitis n = 3 for FOLE, n = 2 for control ! All adverse effects disappeared without interruption of LE
treatment
! MCT/LCT emulsion contains 50% less n-6 than similar studies utilizing soybean oil

Discussion/Conclusions
! Post-operative CRP significantly increased in patients only treated with control LE
! Favorable IL-10 modulation day 3 post-operation followed by a decrease by day 6
! Decreased HLA-DR positive monocytes, Decreased CD32 expressing monocytes, decreased oxidative burst in control group versus FOLE group preserving leukocyte phenotype
! No significant difference between control group and FOLE group for frequency of post-surgical infection or length of ICU or hospital stay
! Pre-operative infusion of FOLE may attenuate immune dysfunction after surgical trauma

Discussion/Conclusions
! Future research focusing on the elderly and malnourished groups are needed due to smaller variation of length of ICU stay
! Future research on patients not requiring PN could verify the post-surgical benefits found aiding in avoiding post-operative immune paralysis and multiple organ failure