part 1: ocular allergy - mededicus llcmededicus.com/downloads/ocular_surface_wellness_prt1.pdfpart...
TRANSCRIPT
Proceedings From an Expert Roundtable Discussion
Mile Brujic, OD, FAAO—Program Chair and ModeratorAlan Kabat, OD, FAAO
David Kading, OD, FAAOChristine Sindt, OD, FAAO
Loretta Szczotka-Flynn, OD, PhD, FAAO
Original Release: March 1, 2014
Expiration: January 7, 2017
faculty
Updates in Oc
ular Surface Wellness
A supplement to
This course is COPE approved for 2 hours
of CE credit for optometrists.
COPE Course ID: 40008-AS
This continuing education activity is supportedthrough an unrestricted educational grant from
Administrator
Sponsored by
CE Monograph
Part 1: Ocular Allergy
Online Testing and Instant Certificate Processing
http://tinyurl.com/OcularSurface1

2
Learning Method and MediumThis educational activity consists of a case reportand ten (10) study questions. The participantshould, in order, read the Learning Objectivescontained at the beginning of this activity, read thematerial, answer all questions in the post test, andcomplete the Activity Evaluation/Credit Requestform. To receive credit for this activity, please followthe instructions provided below in the section titledTo Obtain CE Credit. This educational activity shouldtake a maximum of 2.0 hours to complete.
Content SourceThis continuing education (CE) activity capturescontent from a roundtable discussion.
Activity DescriptionEye care providers face multiple challenges inmanaging ocular surface disorders including ocularallergy and dry eye. Studies show that ocularallergies are often underdiagnosed and often nottreated optimally. Recently, a group of expertsconvened to discuss their insights and approachesfor managing patients with ocular allergy includingspecial considerations for patients wearing contactlenses. This CE activity brings you highlights fromthese discussions in a 2-part series: Part 1 focuseson Ocular Allergy, Part 2 on Dry Eye.
Target AudienceThis educational activity is intended foroptometrists.
Learning Objectives Upon completion of this activity, participants willbe better able to:
• Make a differential diagnosis in patients withocular allergy• Select the therapy that is most appropriate for the patient’s diagnosis and phase of ocular allergy• Incorporate current approaches to successfullymanage contact lens wearing patients whoalso have ocular allergy• Counsel patients on proactive measures formanaging ocular allergy
Accreditation Designation StatementThis course is COPE approved for 2 hours of CEcredit for optometrists.COPE Course ID: 40008-AS
DisclosuresMile Brujic, OD, FAAO, had a financial agreementor affiliation during the past year with the followingcommercial interests in the form of Consultant/Advisory Board: Alcon, Inc; Allergan, Inc; Bio-Tissue,Inc; NicOx SA; TelScreen; Transitions Optical, Inc;Valeant Pharmaceuticals International, Inc; andVmax Vision, Inc; Contracted Research: Alcon, Inc;Honoraria from promotional, advertising or non-CME services received directly fromcommercial interests or their Agents (eg, SpeakersBureaus): Alcon, Inc; Allergan, Inc; Optovue, Inc;Paragon, Valley Contax; and Vmax Vision, Inc.
Alan G. Kabat, OD, FAAO, had a financialagreement or affiliation during the past year withthe following commercial interests in the form ofConsultant/Advisory Board: Alcon, Inc; Allergan,Inc; Bio-Tissue, Inc; NicOx SA; TearScience; andValeant Pharmaceuticals Inc; Honoraria frompromotional, advertising or non-CME servicesreceived directly from commercial interests or theirAgents (eg, Speakers Bureaus): Alcon, Inc; andValeant Pharmaceuticals Inc.
David L. Kading, OD, FAAO, has had a financialagreement or affiliation with the followingcommercial interests in the form ofConsultant/Advisory Board/SpeakerBureau/Contracted Writing: Alcon, Inc; Allergan,Inc; Aton Pharma, Inc; Bausch + LombIncorporated; Bio-Tissue, Inc; Contamac; CibaVision; CooperVision; Essilor Laboratories ofAmerica; Inspire Pharmaceuticals, Inc; NicOx;Valeant Pharmaceuticals Inc; and Valley Contax;Contracted Research: Alcon, Inc; Bausch + LombIncorporated; Ciba Vision; CooperVision;SynergEyes; and Valley Contax.
Christine Sindt, OD, FAAO, had a financialagreement or affiliation during the past year withthe following commercial interests in the form ofConsultant/Advisory Board: Alcon Vision Care;Contracted Research: Alcon Vision Care;Ownership Interest: EyePrint Prosthetics.
Loretta Szczotka-Flynn, OD, PhD, FAAO, had afinancial agreement or affiliation during the pastyear with the following commercial interests in theform of Consultant/Advisory Board: Alcon, Inc;Contracted Research: Alcon, Inc; and Johnson &Johnson Vision Care, Inc.
Disclosure AttestationEach of the contributing physicians listed abovehas attested to the following:1. that the relationships/affiliations noted will notbias or otherwise influence his or herinvolvement in this activity;
2. that practice recommendations given relevant tothe companies with whom he or she hasrelationships/affiliations will be supported bythe best available evidence or, absent evidence,will be consistent with generally acceptedmedical practice; and
3. that all reasonable clinical alternatives will bediscussed when making practicerecommendations.
Product Usage in Accordance with Labeling Please refer to the official prescribing informationfor each product for discussion of approvedindications, contraindications, and warnings.
Grantor StatementThis CE activity is supported through anunrestricted educational grant from Alcon, Inc.
To Obtain CE CreditWe offer instant certificate processing and supportGreen CE. Please take this post test and evaluationonline by going to http://tinyurl.com/OcularSurface1.Upon passing, you will receive your certificateimmediately. You must answer 7 out of 10questions correctly in order to pass, and may takethe test up to 2 times. Upon registering andsuccessfully completing the post test, yourcertificate will be made available online and youcan print it or file it. Please make sure you take the online post test and evaluation on a devicethat has printing capabilities. There are no fees for participating in and receiving CE credit for this activity.
DisclaimerThe views and opinions expressed in thiseducational activity are those of the faculty and donot necessarily represent the views of the StateUniversity of New York College of Optometry,MedEdicus LLC, Alcon, Inc, or Review of Optometry.
This CE activity is copyrighted to MedEdicus LLC ©2014. All right reserved.
Mile Brujic, OD, FAAO (Program Chair and Moderator)Premier Vision GroupBowling Green, Ohio
Alan Kabat, OD, FAAOProfessorSouthern College of OptometryMemphis, Tennessee
David Kading, OD, FAAOSpecialty Eyecare GroupSeattle, Washington
Christine Sindt, OD, FAAODirector, Contact Lens ServiceClinical Associate Professor ofOphthalmology and Visual Sciences
University of IowaCarver College of MedicineIowa City, Iowa
Loretta Szczotka-Flynn, OD, PhD, FAAO
Director, Contact Lens ServiceUniversity Hospitals Case Medical Center
Professor of OphthalmologyCase Western Reserve University School of Medicine
Cleveland, Ohio
faculty

3
introductionOcular allergy is a common condition associated withsignificant morbidity and economic burden from both directand indirect costs.1-5 It encompasses a group of type I andtype IV hypersensitivity-mediated ocular surface diseasesthat include seasonal allergic conjunctivitis (SAC), perennialallergic conjunctivitis (PAC), atopic keratoconjunctivitis (AKC),vernal keratoconjunctivitis (VKC), and contact lens–inducedpapillary conjunctivitis (CLPC; previously known as giantpapillary conjunctivitis). According to various studies, theoverall prevalence of ocular allergy ranges between 15%and 40%.1 However, SAC and PAC are the most commonforms, accounting for up to 95% of allergic eye disease inthe United States.2
While SAC and PAC are not generally considered sight-threatening diseases, they can adversely affect visualfunction, contact lens wear comfort, work productivity, sleep,and quality of life.3-5 Numerous studies have also shown theassociation between excessive ocular itching and thedevelopment of keratoconus.6,7 In addition, ocular allergyhas cosmetic sequelae associated with having red, irritatedeyes and the potential for frequent, long-term scratching tocause progressive collagenous stress along the eyelid skin.Despite its many consequences, allergic conjunctivitis isunderdiagnosed and undertreated.1 Optometrists, asprimary eye care providers, are positioned to address these problems.
Several factors can contribute to the suboptimalmanagement of patients with allergic conjunctivitis. Manypatients self-treat their condition with over-the-counter (OTC)medications and do not even present for care to health careproviders. Some patients with allergic conjunctivitis may seekattention for concomitant atopic diseases (ie, asthma,allergic rhinitis, urticaria, or eczema),8 and the primary careclinician or dermatologist who is managing those comorbidconditions may overlook the patient’s ocular manifestations.Due to the periodic nature of reactions in patients with SACand PAC, it is likely that even those patients who regularlysee an eye care provider for other reasons may not haveactive allergic symptoms at the time of their visit. Amongpatients who present for care because of signs andsymptoms of allergic eye disease, the diagnosis may still bemissed because other common ocular surface conditionswith overlapping manifestations—such as dry eye,meibomian gland dysfunction (MGD), and contact lens–related discomfort—may coexist.
The aim of this continuing education activity is to improvecare for patients with allergic conjunctivitis by raisingawareness of its prevalence and burden, presentingstrategies to increase its recognition, and reviewingapproaches for safe and effective treatment.
DiagnosisAllergic conjunctivitis is usually a clinical diagnosis based onthe findings from the patient’s history and physicalexamination.
HistoryObtaining an accurate medical history from each patient isimportant to elicit the characteristic signs and symptoms ofallergic conjunctivitis, the causative allergens, the presence ofother allergic disorders, and the use of medications forcontrolling allergy signs and symptoms. Considering the highprevalence of SAC and PAC and the opportunity to providepreemptive care, clinicians should probe for these conditionsas part of the history in all patients.
Itching is the hallmark symptom of allergic conjunctivitis, andin patients who present with red, irritated eyes, a chiefcomplaint of itching should direct the diagnostic evaluationtoward allergy. However, absence of a report of itching doesnot necessarily rule out allergic conjunctivitis since somepatients experiencing itchy eyes may describe it using otherterms (eg, burning, stinging, or irritated eyes). Other commoncomplaints of patients with allergic conjunctivitis are tearing,redness, and eyelid swelling, while chemosis is seen in severecases. Most patients will also have nasal symptoms, includingnasal itching, congestion, or a runny nose.
The patient’s medical history should also elicit whether ornot the patient is using any anti-allergy medications at anytime throughout the year. This information can explain anincomplete clinical picture of allergy in a patient with activedisease and identify an underlying cause for problems withdry eye or contact lens discomfort. For example, patientswho are using an oral antihistamine medication may nothave prominent itch, but may be suffering from the oculardrying effects of those medications. In addition, the patient’smedication history can trigger the clinician to inquire aboutSAC or PAC in patients who are seen when their allergiesmay not be active.
Electronic medical records can help in obtaining themedication history, although the patient’s record may notinclude a full list of medications and in particular may bemissing information about OTC products. Asking specificallyabout agents purchased without a prescription is importantconsidering that anti-allergy agents are top-selling OTCmedications and because some patients do not consider OTCproducts as “medications.”
Recognizing that patients may have poor recall of medicationsthey used several months earlier, it is also helpful to routinelyask patients to bring in bottles of any medications they haveused since their last visit. Patients who do not bring in theirmedications or are unable to provide product names shouldbe asked about the reason why they were using themedication. This may help the clinician in determining theclass of medication that was taken.
If the medication history shows a patient is self-treating forallergy with an oral antihistamine and does not have activedisease, further questioning is needed to determine whetheror not allergic conjunctivitis is a problem. Although mostpatients with seasonal and perennial allergies suffer withboth nasal and ocular manifestations, it is possible that onlythe nose or only the eyes are affected.9 Even if the patientdenies ocular allergy symptoms, the optometrist must still
4
consider whether or not the use of an oral antihistamine forallergic rhinitis may be causing dry eye.
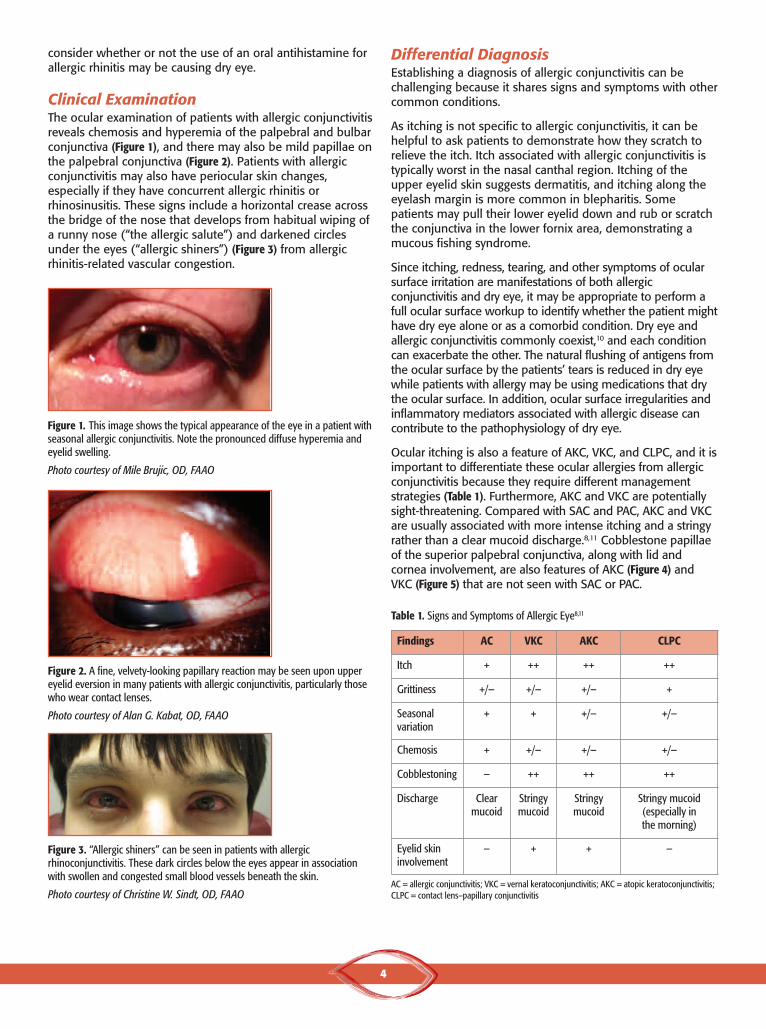
Clinical ExaminationThe ocular examination of patients with allergic conjunctivitisreveals chemosis and hyperemia of the palpebral and bulbarconjunctiva (Figure 1), and there may also be mild papillae onthe palpebral conjunctiva (Figure 2). Patients with allergicconjunctivitis may also have periocular skin changes,especially if they have concurrent allergic rhinitis orrhinosinusitis. These signs include a horizontal crease acrossthe bridge of the nose that develops from habitual wiping ofa runny nose (“the allergic salute”) and darkened circlesunder the eyes (“allergic shiners”) (Figure 3) from allergicrhinitis-related vascular congestion.
Differential Diagnosis Establishing a diagnosis of allergic conjunctivitis can bechallenging because it shares signs and symptoms with othercommon conditions.
As itching is not specific to allergic conjunctivitis, it can behelpful to ask patients to demonstrate how they scratch torelieve the itch. Itch associated with allergic conjunctivitis istypically worst in the nasal canthal region. Itching of theupper eyelid skin suggests dermatitis, and itching along theeyelash margin is more common in blepharitis. Somepatients may pull their lower eyelid down and rub or scratchthe conjunctiva in the lower fornix area, demonstrating amucous fishing syndrome.
Since itching, redness, tearing, and other symptoms of ocularsurface irritation are manifestations of both allergicconjunctivitis and dry eye, it may be appropriate to perform afull ocular surface workup to identify whether the patient mighthave dry eye alone or as a comorbid condition. Dry eye andallergic conjunctivitis commonly coexist,10 and each conditioncan exacerbate the other. The natural flushing of antigens fromthe ocular surface by the patients’ tears is reduced in dry eyewhile patients with allergy may be using medications that drythe ocular surface. In addition, ocular surface irregularities andinflammatory mediators associated with allergic disease cancontribute to the pathophysiology of dry eye.
Ocular itching is also a feature of AKC, VKC, and CLPC, and it isimportant to differentiate these ocular allergies from allergicconjunctivitis because they require different managementstrategies (Table 1). Furthermore, AKC and VKC are potentiallysight-threatening. Compared with SAC and PAC, AKC and VKCare usually associated with more intense itching and a stringyrather than a clear mucoid discharge.8,11 Cobblestone papillaeof the superior palpebral conjunctiva, along with lid andcornea involvement, are also features of AKC (Figure 4) andVKC (Figure 5) that are not seen with SAC or PAC.
Figure 1. This image shows the typical appearance of the eye in a patient withseasonal allergic conjunctivitis. Note the pronounced diffuse hyperemia andeyelid swelling.
Photo courtesy of Mile Brujic, OD, FAAO
Table 1. Signs and Symptoms of Allergic Eye8,11
Figure 2. A fine, velvety-looking papillary reaction may be seen upon uppereyelid eversion in many patients with allergic conjunctivitis, particularly thosewho wear contact lenses.
Photo courtesy of Alan G. Kabat, OD, FAAO
Figure 3. “Allergic shiners” can be seen in patients with allergicrhinoconjunctivitis. These dark circles below the eyes appear in associationwith swollen and congested small blood vessels beneath the skin.
Photo courtesy of Christine W. Sindt, OD, FAAO
Findings AC VKC AKC CLPC
Itch + ++ ++ ++
Grittiness +/− +/− +/− +
Seasonalvariation
+ + +/− +/−
Chemosis + +/− +/− +/−
Cobblestoning − ++ ++ ++
Discharge Clear mucoid
Stringy mucoid
Stringy mucoid
Stringy mucoid(especially in the morning)
Eyelid skininvolvement
− + + −
AC = allergic conjunctivitis; VKC = vernal keratoconjunctivitis; AKC = atopic keratoconjunctivitis;CLPC = contact lens–papillary conjunctivitis

5
CLPC is also associated with more severe pruritus than allergicconjunctivitis. Eversion of the upper eyelid allows the clinicianto examine for papillary changes in the upper tarsal plate thatare pathognomonic of CLPC (Figures 6 and 7) and should beperformed in all contact lens wearers, whether or not they aresymptomatic. The presence of a velvety appearing tarsal platein asymptomatic patients is an early sign of CLPC. Detection ofthis change allows for timely intervention that can preventprogression to the development of frank giant papillae andthe unfortunate sequelae of contact lens intolerance.
Patients who are contact lens wearers may also develop red,irritated eyes for a variety of other reasons that are related tolens fit, lens material and/or design, hygiene, wearingschedule, or a lens-care solution interaction. These problemsmay occur in isolation or coexist and exacerbate allergicconjunctivitis. Patients with allergy who also wear contactlenses will often experience greater symptoms of redness,itching, and discomfort than those patients who do not wearcontact lenses. Having patients temporarily discontinue contactlens wear can help to rule out a contact lens–related cause, butthis idea is often rejected by some patients, especially if theyare not highly symptomatic. Determining if the patient’s signsand symptoms of itching and redness worsen after the lensesare inserted in the morning can direct the evaluation towardidentifying possible sources of contact lens–related ocularredness and irritation. Infectious causes of conjunctivitis(bacterial, viral, chlamydial) should also be considered.
Treatment of Allergic ConjunctivitisEffective treatment of allergic conjunctivitis incorporatesnonpharmacologic and pharmacologic interventions.Nonpharmacologic strategies focus primarily onenvironmental measures to reduce allergen exposure. Thesestrategies include limiting time spent outdoors duringperiods when allergen levels are high and wearingsunglasses to protect the eyes from additional allergen loadswhile outside. Showering and washing or rinsing the hair atnight before going to bed minimizes the allergen load thatmay be in the hair. Furthermore, although difficult, avoidingeye rubbing is important as it can mechanically induce mastcell release and also introduce allergens from the skin.Since many patients are allergic to dust mites and becausemites accumulate in pillows and bedding, patients may beadvised about using hypoallergenic bedding, changing theirsheets frequently and washing them in hot water, andputting their pillow into a hot dryer for 20 minutes to killdust mites. Keeping the windows and doors closed at home,taking shoes and outerwear off at the door, removing carpetsfrom floors, and using a high-efficiency particulate absorptionfilter to remove allergens from the circulating air are allstrategies to reduce the indoor allergen burden.
In addition to strategies for allergen avoidance, patients can beadvised about topical nonpharmacologic measures to controlallergic conjunctivitis. The use of artificial tears, isotonic saline,or rewetting drops by contact lens wearers can be a helpfulstrategy to dilute and flush away allergens and inflammatorymediators. In general, preservative-free formulations arepreferred to avoid any potential for preservative-inducedhypersensitivity, and refrigeration of these topical products is
Figure 4. Large, irregular macropapillae on the upper tarsus are a commonfinding in atopic keratoconjunctivis. With chronic disease, inflammation maylead to scarring.
Photo courtesy of Al Kabat, OD, FAAO
Figure 5. Giant “cobblestone” papillae, seen here upon eversion of the upperlid, are a hallmark of vernal keratoconjunctivitis. Note the polygonal shape andlack of uniformity.
Photo courtesy of Al Kabat, OD, FAAO
Figure 6. View of the everted upper eyelid in a patient who developed contactlens–induced papillary conjunctivitis due to contact lens overwear.
Photo courtesy of Mile Brujic, OD, FAAO
Figure 7. Contact lens–induced papillary conjunctivitis with large papillaenoted in Zones 2 and 3 of the upper tarsal plate.
Photo courtesy of Loretta Szczotka-Flynn OD, PhD, FAAO

6
Table 2. Over-the-Counter and Prescription Medications for Ocular Allergy12
Generic (brand) name Indication Pediatric use Dosing
OTC PRODUCTS
H1-antagonist/mast cell stabilizer
Ketotifen fumaratea, 0.025%, (Alaway, Claritin Eye, Eye Itch Relief, Zaditor,Zyrtec Itchy Eye, generic)
Temporary relief of itchy eyes due to ragweed, pollen,grass, animal hair, and dander
≥3 years twice a day, every 8 to 12 hours
Decongestant/antihistamine
Naphazoline/pheniramine (Naphcon-A, Opcon-A, Visine-A)
Temporary relief of minor eye symptoms of itching and redness caused by ragweed, pollen grass, animaldander, and hair
≥6 years 1 or 2 drops up to 4 times daily
PRESCRIPTION PRODUCTS
Antihistamines
Emedastine difumarate, 0.05%, (Emadine) Temporary relief of the signs and symptoms of AC ≥3 years up to 4 times a day
Dual acting antihistamine/mast cell stabilizers
Alcaftadine, 0.25%, (Lastacaft) Prevention of itching associated with AC ≥2 years once a day
Azelastine, 0.05%, (Optivar + generic) Treatment of itching of the eye associated with AC ≥ 3 years twice a day
Bepotastine besilate, 1.5%, (Bepreve) Treatment of itching associated with AC ≥2 years twice a day
Epinastine HCl, 0.05%, (Elestat + generic) Prevention of itching associated with AC ≥2 years twice a day
Olopatadine HCl, 0.1%, (Patanol) Treatment of the signs and symptoms of AC ≥3 years twice a day (at an interval of6 to 8 hours)
Olopatadine HCl, 0.2%, (Pataday) Treatment of ocular itching associated with AC ≥2 years once a day
Mast cell stabilizers
Cromolyn sodium, 4%, (Crolom, generic) Treatment of VKC, vernal conjunctivitis, and vernal keratitis
≥4 years 1 to 2 drops 4 to 6 timesdaily
Lodoxamide tromethamine, 0.1%, (Alomide) Treatment of VKC, vernal conjunctivitis, and vernal keratitis
≥2 years 1 to 2 drops 4 times a day forup to 3 months
Nedocromil sodium, 2%, (Alocril + generic) Treatment of itching associated with AC ≥3 years 1 to 2 drops up to twicea day
Pemirolast potassium, 0.1%, (Alamast) Prevention of itching of the eye due to AC ≥3 years 1 to 2 drops4 times a day
Other
Ketorolac tromethamine, 0.5%, (Acular +generic) (NSAID)
Temporary relief of ocular itching due to SAC ≥2 years 4 times a day
Loteprednol etabonate, 0.2%, (Alrex)(Ester corticosteroid)
Temporary relief of the signs and symptoms of SAC Safety and effectivenessnot established inpediatric patients
4 times a day
aThe www.pdr.net drug summary for ketotifen fumarate lists antihistamine for mechanism of action. However, in addition to being a noncompetitive H1-antagonist,ketotifen also has mast cell stabilizing activity.11
AC = allergic conjunctivitis; H1 = histamine1; NSAID = nonsteroidal anti-inflammatory drug; SAC = seasonal allergic conjunctivitis; VKC = vernal keratoconjunctivitis
Antigen binds to IgE
Mast celldegranulates
Preformed mediators
Histamine Proteases Heparin
Newly formed mediators Chemokines & cytokines
Eicosanoids(prostaglandins,
leukotrienes,thromboxanes)
ItchingChemosisRedness
Mucus secretion ItchingRednessTearing
Mucus secretionNerve stimulation
Leukocyte infiltration
RednessChemosis
IgE expressionUpregulation of
adhesion molecules
Leukocyte activation& migration
Platelet-activatingfactor
7
helpful as the cold solution is both soothing and acts tocounteract the elevated tissue temperature associated with inflammation.
Medical TherapyThe feasibility of nonpharmacologic approaches for ocularallergy management varies depending on lifestyle issues andthe causative allergen. While they may be sufficient forpatients who are only mildly symptomatic, they are oftenunsatisfactory as a stand-alone measure. Therefore, medicaltherapy is the cornerstone for effective management of mostpatients with allergic conjunctivitis.
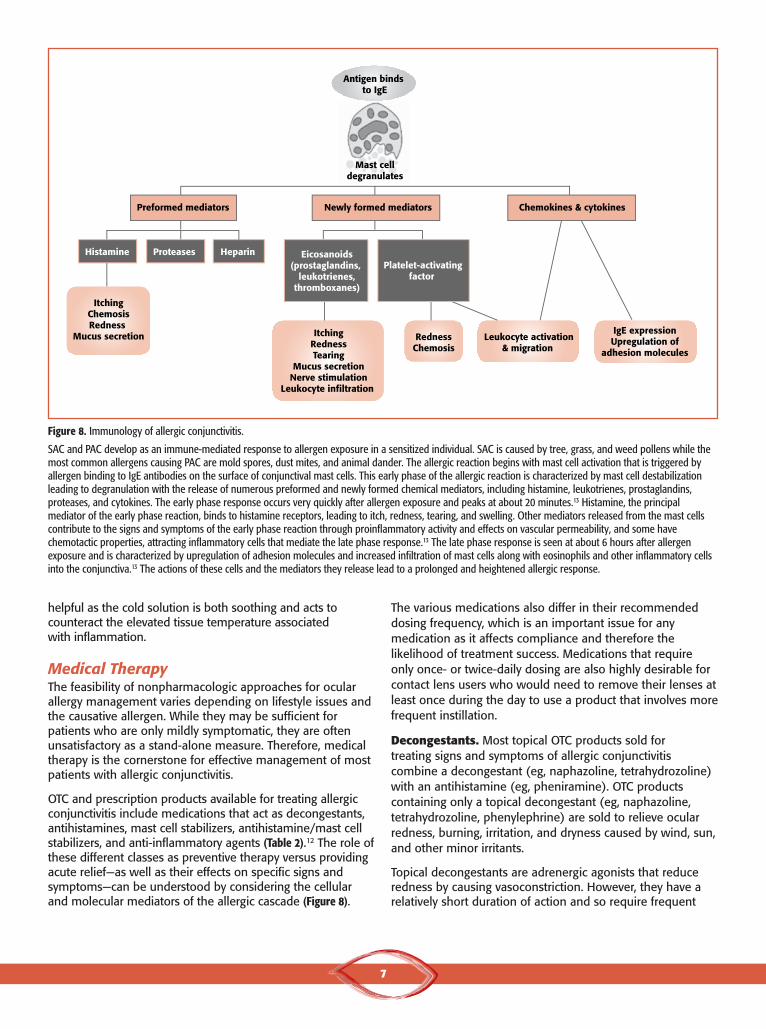
OTC and prescription products available for treating allergicconjunctivitis include medications that act as decongestants,antihistamines, mast cell stabilizers, antihistamine/mast cellstabilizers, and anti-inflammatory agents (Table 2).12 The role ofthese different classes as preventive therapy versus providingacute relief—as well as their effects on specific signs andsymptoms—can be understood by considering the cellularand molecular mediators of the allergic cascade (Figure 8).
The various medications also differ in their recommendeddosing frequency, which is an important issue for anymedication as it affects compliance and therefore thelikelihood of treatment success. Medications that requireonly once- or twice-daily dosing are also highly desirable forcontact lens users who would need to remove their lenses atleast once during the day to use a product that involves morefrequent instillation.
Decongestants. Most topical OTC products sold for treating signs and symptoms of allergic conjunctivitiscombine a decongestant (eg, naphazoline, tetrahydrozoline)with an antihistamine (eg, pheniramine). OTC productscontaining only a topical decongestant (eg, naphazoline,tetrahydrozoline, phenylephrine) are sold to relieve ocularredness, burning, irritation, and dryness caused by wind, sun,and other minor irritants.
Topical decongestants are adrenergic agonists that reduceredness by causing vasoconstriction. However, they have arelatively short duration of action and so require frequent
Figure 8. Immunology of allergic conjunctivitis.
SAC and PAC develop as an immune-mediated response to allergen exposure in a sensitized individual. SAC is caused by tree, grass, and weed pollens while themost common allergens causing PAC are mold spores, dust mites, and animal dander. The allergic reaction begins with mast cell activation that is triggered byallergen binding to IgE antibodies on the surface of conjunctival mast cells. This early phase of the allergic reaction is characterized by mast cell destabilizationleading to degranulation with the release of numerous preformed and newly formed chemical mediators, including histamine, leukotrienes, prostaglandins,proteases, and cytokines. The early phase response occurs very quickly after allergen exposure and peaks at about 20 minutes.13 Histamine, the principalmediator of the early phase reaction, binds to histamine receptors, leading to itch, redness, tearing, and swelling. Other mediators released from the mast cellscontribute to the signs and symptoms of the early phase reaction through proinflammatory activity and effects on vascular permeability, and some havechemotactic properties, attracting inflammatory cells that mediate the late phase response.13 The late phase response is seen at about 6 hours after allergenexposure and is characterized by upregulation of adhesion molecules and increased infiltration of mast cells along with eosinophils and other inflammatory cellsinto the conjunctiva.13 The actions of these cells and the mediators they release lead to a prolonged and heightened allergic response.
8
dosing, 1 to 2 drops up to 4 times daily.14 Furthermore, thesemedications often cause burning and stinging.14 In addition,the chronic use of a topical decongestant can lead toconjunctival inflammation that can exacerbate the allergicreaction and be associated with rebound hyperemia whentreatment is stopped.15 Other adverse reactions reported withthe chronic use of topical decongestants include pupillarydilation, corneal opacities, and dry eye.16-18 In addition,topical decongestants are contraindicated in patients withangle-closure glaucoma and associated with potential safetyconcerns in patients with cardiovascular disease,hyperthyroidism, and diabetes.
Antihistamines. Antihistamines provide rapid relief of itchingby blocking histamine binding to its receptors. However, theydo not prevent initiation of the allergic cascade or inhibit theactivity of any other allergy mediators. Oral antihistaminesmay be helpful for patients with allergic nasal symptoms, butcan lead to dry mouth, ocular surface dryness, and sedation.These adverse reactions particularly occur with oldergeneration antihistamines.19 However, sedation can also occurwith cetirizine,19 and both cetirizine and loratadine have beenassociated with ocular drying effects.20
Mast cell stabilizers. Mast cell stabilizers act to prevent thedegranulation of mast cells; they are useful to preventsequelae from future allergen exposure. They do not inhibitthe action of any mediators that are already released.Therefore, mast cell stabilizers do not provide acute relieffrom existing signs and symptoms.
Dual-acting antihistamine/mast cell stabilizers.Medications that provide both antihistamine and mast cellstabilizing properties are the current mainstay for themanagement of allergic conjunctivitis, and many of thesemedications offer activity against the inflammatory cells andcytokines involved in the delayed allergic response. Withtheir multimodal mechanisms, these agents can prevent theonset of the allergic response if started prior to allergenexposure as well as provide immediate and ongoing relief inpatients who have experienced a flare-up.
Available antihistamine/mast cell stabilizers include 1 agentavailable in OTC products and several prescriptionmedications. The antihistamine/mast cell stabilizers offerconvenient dosing schedules of only once or twice a day andare safe. In clinical practice, they have been used on a long-term basis without any serious adverse reactions. The onlyprecaution to their use is to avoid in patients withhypersensitivity to any ingredient in the formulation.
Anti-inflammatory agents. Corticosteroid treatment has acritical role for managing inflammation associated with thesevere forms of ocular allergy, VKC, AKC, and CLPC, and isuseful as a short-term intervention for controlling a severepresentation of acute SAC or PAC. In addition, corticosteroidtreatment can be useful on a short-term basis for dry eyedisease, which may be comorbid with allergy.
Corticosteroids act on both the early and late phases of theallergic reaction by suppressing mast cell proliferation, inhibitingthe production of multiple inflammatory mediators, andreducing the influx of inflammatory cells.21 There is conflictinginformation about the relative efficacy of corticosteroids versusantihistamine/mast cell stabilizers for relieving itching,22,23
although an agent with antihistamine activity would beexpected to provide faster onset of relief. Intraocular pressure(IOP) monitoring at follow-up visits is important for all patientsbeing treated with a topical corticosteroid.
Nonsteroidal anti-inflammatory drugs act to preventprostaglandin synthesis and desensitize pain receptors sothat they decrease inflammation and itching. However,ketorolac tromethamine, 0.5%, is the only topical NSAIDapproved by the US Food and Drug Administration (FDA) forthe management of allergic conjunctivitis, and it is not widelyused because of the availability of more effective options andits high potential to cause burning and stinging withinstillation. According to the prescribing information, up to40% of the patients using ketorolac tromethamine, 0.5%,experienced burning and stinging.24
Patient Counseling Reviewing the available options with patients helps them tounderstand the rationale for their clinician’s therapeuticrecommendations and engages them as partners in care,which can help to improve compliance. The discussion withpatients on medications should include information aboutrelative costs, dosing frequency, efficacy, and possible adversereactions. It should conclude with a definitive recommendationand prescription for what the optometrist considers as thebest option, although still making sure that patientsunderstand other modalities can be tried if the first isunsatisfactory. Consider, for example, the situation in which apatient picks up a prescription and finds it is prohibitivelyexpensive. Patients who have not been informed about viablealternatives may be displeased with their doctor and chooseto self-treat with an OTC product and/or see another provider.
Although it is important to be sensitive to cost issues, OTCproducts may offer less value than prescription products, atleast, in part, because the OTC medications may requiremore frequent dosing. Providing patients with somesuggestions about OTC products to try also puts the onus onthem to go to the store, decide among a host of agents, andmake the purchase. Handing patients a written prescriptionreduces reliance on patient follow-through, but still assumesthe patient will bring the prescription to the pharmacy.Sending a prescription directly to the pharmacy goes 1 stepfurther and also reinforces the optometrist’s authoritativeposition. Follow-up visits will verify that patients are usingtheir treatment and determine its success.
It is better to have patients schedule the visit before theyleave the office than to suggest they call for an appointment.

9
Treatment SelectionDecisions on medical treatment for SAC or PAC depend onwhether the patient needs relief from an acute flare-up or isbeing treated to prevent an allergic reaction.
An antihistamine/mast cell stabilizer is usually sufficient byitself for treating active disease in patients who have mild tomoderate signs and symptoms of SAC or PAC.
An ophthalmic antihistamine/mast cell stabilizer can alsoimprove nasal rhinitis,25-27 although patients with more thanmild allergic rhinitis may need additional therapy. The use ofa systemic antihistamine that will produce some oculardrying effects is generally best avoided in patients withallergic conjunctivitis. Alternatives include intranasalantihistamines and corticosteroids.
Patients with a moderate-to-severe flare of AC or PAC may bestarted simultaneously on a topical corticosteroid that is thentapered off when signs of inflammation improve. Anecdotally,most patients achieve an adequate response after only 1 or 2 weeks of corticosteroid treatment. Scheduling a follow-upvisit 5 to 7 days after corticosteroid initiation will allow theclinician to evaluate its benefit and safety. Although allcorticosteroids can be used to control ocular inflammation,loteprednol etabonate, 0.2%, is indicated specifically for reliefof the signs and symptoms of SAC, and has a good safetyprofile with respect to risk of IOP elevation.28,29
Patients with SAC may begin using an antihistamine/mastcell stabilizer prior to the start of allergy season and continueusing the medication while allergen levels remain elevated.Although a mast cell stabilizer could also theoretically beprescribed for this purpose, it rarely is because it usuallyrequires more frequent dosing and does not provideantihistamine activity that will help patients when challengedwith allergens. A similar preventive approach using anantihistamine/mast cell stabilizer can be recommended topatients with PAC who are able to anticipate allergenexposure (eg, a patient who is allergic to horse dander andwill encounter the animals on vacation). Patients with PAC
who have year-round exposure to triggering allergens may bemaintained on an antihistamine/mast cell stabilizerindefinitely. Again, medications with mast cell stabilizingactivity alone might be considered instead for maintenance,but their more frequent dosing schedule can present acompliance issue, and they would not control symptoms ifmast cell degranulation occurs.
Patients with comorbid allergic disorders may be referred toan allergist for further evaluation and optimal management oftheir nonocular symptoms.
Allergic Conjunctivitis in Patients Wearing Contact LensesLens Selection and CareAllergic conjunctivitis is an important contributor to contactlens intolerance as demonstrated by the results of a studyshowing that 75% of the patients with allergicrhinoconjunctivitis reported partial or absolute intolerance oftheir lenses.30 Although contact lenses can act as a barrier toairborne allergens, they can also serve as a vehicle forincreasing allergen exposure by trapping environmentalallergens and binding antigens from the tear film, ocularsurface, lids, and lens care solutions. Considering thatbacteria and bacterial products are well-recognized to beantigenic in patients with atopic dermatitis and allergicairway disease,31 it is plausible that microbial bioburden onthe lens surface may also be a trigger for allergic reactions.This potential relationship is important considering theubiquitous opportunities for microorganisms to accumulateon the lens surface.
Ideally, patients might be furloughed from contact lens wearwhen they are experiencing significant problems with allergicconjunctivitis. However, most patients will resist this idea, andit is impractical for others, such as patients with keratoconuswhose visual function depends on gas permeable (GP)contact lens wear. Concern about the buildup of antigens on the contact lens surface provides a rationale forrecommending daily disposable lenses to soft contact lenswearers who are suffering with allergic conjunctivitis, andthere is clinical trial evidence showing the efficacy of thisstrategy for improving patient comfort.32 Daily disposablelenses provide the benefits of placing a new, clean lens onthe eye at the beginning of every day. Thus, any depositionthat may have occurred on the lens the prior day is not anexacerbating issue. Furthermore, the use of daily disposablelenses eliminates exposing the eye to lens care solutioningredients that can themselves precipitate allergic reactions.
As technologies have advanced with 2-week and monthlydisposable lenses, there has also been a significant evolutionin the daily disposable lens modality. Several product optionsare currently available in the daily disposable lens categorythat represent 3 different material types: hydrogel, siliconehydrogel, and water gradient technology. In addition, newwetting agents are being added to lenses in an attempt toimprove the lens wearing experience.
Why Samples Are Not Always a Good ThingSometimes optometrists think they are doing patientsa service by handing out medication samples.However, similar to seeing a mint left on a hotel pillowat night, patients may consider the sample a nicegesture, but assign little value to it because it is free.The end result is that they may be unlikely to use theproduct or even to remember its name.
In contrast, when patients are given a prescription fora medication along with an explanation of why thatspecific product was chosen, they are more likely toregard it as important and be compliant with theinstructions for use.

10
There are no conclusive clinical trial data or other evidenceon which to base recommendations for choosing anyparticular daily disposable product or material class. Differentlenses within the same class may have unique chemicalcharacteristics.
A new category of water gradient technology lenses made ofdeleficon A is the latest addition to the daily disposablemarket. This lens has a high dK silicone hydrogel core withan outer layer (~10% of the lens thickness) made of anonsilicone hydrophilic polymer. The water content of thelens varies from 33% for the silicone hydrogel core to >80%on average for the outer layer in which the water contenttransitions to reach almost 100% at the surface. The lenssurface is also unique in its level of lubricity33; it was shownto have less impact on the prelens tear film surface qualitythan a daily disposable hydrogel lens made of nelficon A.34
With its moisture rich surface characteristics, the watergradient technology lens is a logical consideration in thechallenging population of patients with ocular allergy.
When a daily disposable contact lens is not a viable optionfor a patient with ocular allergies who wears soft contactlenses, other strategies need to be put into place to optimizecontact lens wear. This process begins with patient educationand reinforcing the importance of thorough cleaning andother aspects of good lens hygiene practices. Making surepatients are rubbing and rinsing their lenses is critical in thispopulation. In addition, clinicians should ascertain thatpatients have not strayed from using the lens care systemsrecommended to them.
For soft lenses, surfactant cleaners may be needed in rareinstances, in addition to the multipurpose disinfecting solutionthat a patient may be using, as the surfactant cleaner assists inremoving additional antigens from the lens surface of heavilydepositing ocular allergy sufferers. The use of a peroxide-based system for cleaning and disinfection should also beconsidered for these patients as it will minimize chemicalexposure on the eye while effectively cleaning the lenses.
An alcohol-based surfactant cleaner is also effective forcleaning GP lenses. To help reduce allergen exposure, patientswith GP lenses should be instructed to rinse the lens well withpreservative-free saline before lens insertion. A peroxide-basedcleaning and disinfection system is approved for use by theFDA with both soft and GP contact lenses, and should beconsidered in GP lens wearers with significant ocular allergies.
Among contact lens wearers, the prevalence of allergy isparticularly high in patients with keratoconus.35 Patients withkeratoconus require aggressive management of allergicconjunctivitis to limit eye rubbing that can contribute to theirdisease progression as well as allow them to maintaincontact lens wear. Although small diameter GP lenses work
well for patients with keratoconus, the challenge of ocularallergies can make lens wear much more difficult for thispopulation. Edge awareness is especially problematic inallergic patients because they have a compromised andinflamed ocular surface. Large diameter GP lenses, such asscleral lenses, minimizes the lens edge interaction andprovides an alternative for those patients experiencingsignificant comfort issues wearing small diameter lenses.
Medication Use With Contact Lens WearEffective treatment of allergic conjunctivitis using topicalantihistamine/mast cell stabilizing agents can improvecomfort in contact lens wearing patients.36,37 However,because soft contact lenses can absorb medications and actas a platform for sustained drug delivery,38 patients wearingsoft contact lenses must be counseled not to use theseallergy medications while wearing their lenses and to wait 10 to 15 minutes after instilling drops before inserting theirlenses. Considering the risks associated with corticosteroidtreatment (ie, IOP elevation, cataract formation, andsecondary infection), it is best to discontinue wearing contactlens while patients are being treated with a corticosteroid.
Gas permeable lens materials do not absorb medications,and medication that adheres to the lens surface can beeffectively removed with proper cleaning. Patients withkeratoconus and others dependent on their GP lens may beallowed to continue wearing their contact lenses while beingtreated with a topical corticosteroid. However, theimportance of meticulous lens cleaning, as well asinstructions about not dosing the medication with the lens inthe eye and waiting after medication dosing to insert thelens, must be reinforced.
conclusionAllergic conjunctivitis can have a significant impact on thequality of life for all individuals and poses particularproblems for contact lens wearers. Establishing the diagnosisof allergic conjunctivitis by conducting an appropriatemedical history and a thorough clinical examination of thepatient is the first step to providing effective care.Optometrists must recognize the importance of beingproactive in their efforts to identify allergy sufferers. Medicaltherapy can effectively relieve distress from the signs andsymptoms of allergic conjunctivitis and, combined withallergen avoidance strategies, can limit allergic episodes inmost patients. For optimal care, some patients may be bestreferred to an allergist, and for those who wear contactlenses, modern contact lens technology, good lens hygiene,and careful selection of care systems can facilitate continuedcomfortable wear.
1. Rosario N. Bielory L. Epidemiology of allergic conjunctivitis. Curr OpinAllergy Clin Immunol. 2011;11(5):471-476.
2. Butrus S, Portela R. Ocular allergy: diagnosis and treatment. OphthalmolClin North Am. 2005;18(4):485-492.
3. Kumar P, Elston R, Black D, et al. Allergic rhinoconjunctivitis and contactlens intolerance. CLAO J. 2009;17:31-34.
4. Pitt AD, Smith AF, Lindsell L, et al. Economic and quality-of-life impact ofseasonal allergic conjunctivitis in Oxfordshire. Ophthalmic Epidemiol.2004;11:17-33.
5. Smith AF, Pitt AD, Rodriguez AE, et al. The economic and quality of lifeimpact of seasonal allergic conjunctivitis in a Spanish setting. OphthalmicEpidemiol. 2005;12:233-242.
6. McMonnies CW, Boneham GC. Keratoconus, allergy, itch, eye-rubbing andhand-dominance. Clin Exp Optom. 2003;86(6):376-384.
7. Bawazeer AM, Hodge WG, Lorimer B. Atopy and keratoconus: a multivariateanalysis. Br J Ophthalmol. 2000;84(8):834-836.
8. Bielory L. Allergic diseases of the eye. Med Clin N Am. 2006;90:129-148.
9. Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergyin the United States, 1988-1994. J Allergy Clin Immunol. 2010;126(4):778-783.
10. Hom MMM, Nguyen AL, Bielory L. Allergic conjunctivitis and dry eyesyndrome. Ann Allergy Asthma Immunol. 2012;108(3):163-166.
11. Bielory L, Meltzer EO, Nichols KK, et al. An algorithm for the managementof allergic conjunctivitis. Allergy Asthma Proc. 2013;34:408-420.
12. Physicians’ desk reference [e-Book]. Montvale, NJ: PDR Network, LLC;2014. http://www.nxtbook.com/nxtbooks/pdr/physiciansdeskreference2014/. Accessed February 5, 2014.
13. Bacon AS, Ahluwalia P, Irani AM, et al. Tear and conjunctival changes duringthe allergen-induced early- and late-phase responses. J Allergy ClinImmunol. 2000;106(5):948-954.
14. Bielory L, Katelaris CH, Lightman S, Maclerio RM. Treating the ocularcomponent of allergic rhinoconjunctivitis and related eye disorders.MedGen Med. 2007;9(3):35.
15. Soparkar CN, Wilhelmus KR, Koch DD, Wallace GW, Jones DB. Acute andchronic conjunctivitis due to over-the-counter ophthalmic decongestants.Arch Ophthalmol. 1997;115(1):34-38.
16. Williams TL, Williams AJ, Enzenauer RW. Case report: unilateral mydriasisfrom topical Opcon-A and soft contact lens. Aviat Space Environ Med.1997;68(11):1035-1037.
17. Herman DC, Bartley GB. Corneal opacities secondary to topical naphazolineand antazoline (Albalon-A). Am J Ophth. 1987;103(1):110-111.
18. Göbbels MJ, Achten C, Spitznas M. Effect of topically applied oxymetazolineon tear volume and tear flow in humans. Graefes Arch Clin ExpOphthalmol. 1991;229(2):147-149.
19. Wallace DV, Dykewicz, Bernstein DI, et al. The diagnosis and managementof rhinitis: an updated practice parameter. J Allergy Clin Immunol. 2008;122:S1-S84.
20. Ousler GW, Wilcox KA, Gupta G, Abelson MB. An evaluation of the oculardrying effects of 2 systemic antihistamines: loratadine and cetirizinehydrochloride. Ann Allergy Asthma Immunol. 2004;93(5):460-464.
21. McGill JI, Holgate ST, Church MK, Anderson DF, Bacon A. Allergic eyediseases mechanisms. Br J Ophthalmol. 1998;82:1203-1214.
22. Borazan M, Karalezli A, Akova YA, Akman A, Kiyici H, Erbek SS. Efficacy ofolopatadine HCl 0.1%, ketotifen fumarate 0.025%, epinastine HCl 0.05%,emedastine 0.05% and fluorometholone acetate 0.1% ophthalmic solutionfor seasonal allergic conjunctivitis: a placebo-controlled environmental trial.Acta Ophthalmol. 2009;87(5):549-554.
23. Gong L, Sun X, Qu J, et al. Loteprednol etabonate suspension 0.2%administered QID compared with olopatadine solution 0.1% administeredBID in the treatment of seasonal allergic conjunctivitis: a multicenter,randomized, investigator-masked, parallel group study in Chinese patients.Clin Ther. 2012;34(6):1259-1272.
24. Acular [package insert]. Irvine, CA; Allergan; 2012.
25. Abelson MB, Gomes PJ, Vogelson CT, et al. Effects of a new formulation ofolopatadine ophthalmic solution on nasal symptoms relative to placebo intwo studies involving subjects with allergic conjunctivitis orrhinoconjunctivitis. Curr Med Res Opin. 2005;21(5):683-691.
26. Torkildsen GL, Williams JI, Gow JA, Gomes PJ, Abelson MB, McNamara TR;Bepotastine Besilate Ophthalmic Solutions Clinical Study Group.Bepotastine besilate ophthalmic solution for the relief of nonocularsymptoms provoked by conjunctival allergen challenge. Ann AllergyAsthma Immunol. 2010;105(1):57-64.
27. Greiner JV, Edwards-Swanson K, Ingerman A. Evaluation of alcaftadine0.25% ophthalmic solution in acute allergic conjunctivitis at 15 minutesand 16 hours after instillation versus placebo and olopatadine 0.1%. ClinOphthalmol. 2011;5:87-93
28. Comstock TL, Decory HH. Advances in corticosteroid therapy for ocularinflammation: loteprednol etabonate. Int J Inflam. 2012;2012:789623.[Epub 2012 Mar 28]
29. Ilyas H, Slonim CB, Braswell GR, Favetta JR, Schulman M. Long-term safetyof loteprednol etabonate 0.2% in the treatment of seasonal and perennialallergic conjunctivitis. Eye Contact Lens. 2004;30(1):10-13.
30. Kumar P, Elston R, Black D, Gilhotra S, DeGuzman N, Cambre K. Allergicrhinoconjunctivitis and contact lens intolerance. CLAO J. 1991;17(1):31-34.
31. Renz H. Herz U. The bidirectional capacity of bacterial antigens to modulateallergy and asthma. Eur Respir J. 2002;19(1):158-171.
32. Hayes VY, Schnider CM, Veys J. An evaluation of 1-day disposable contactlens wear in a population of allergy sufferers. Cont Lens Anterior Eye.2003;26(2):85-93.
33. Rudy A, Huo Y, Perry SS, Ketelson H. Surface mechanical and tribologicalproperties of silicone hydrogels measured by atomic force microscopy.Invest Ophth Vis Sci. 2012;53, E-Abstract 6114.
34. Szczesna-Iskander DH. Comparison of tear film surface quality measured invivo on water gradient silicone hydrogel and hydrogel contact lenses. EyeContact Lens. 2014;40(1):23-27.
35. Shneor E, Millodot M, Blumberg S, Ortenberg I, Behrman S, Gordon-ShaagA. Characteristics of 244 patients with keratoconus seen in an optometriccontact lens practice. Clin Exp Optom. 2013;96(2):219-224.
36. Nichols KK, Morris S, Gaddie IB, Evans D. Epinastine 0.05% ophthalmicsolution in contact lens-wearing subjects with a history of allergicconjunctivitis. Eye Contact Lens. 2009;35(1):26-31.
37. Brodsky M, Berger WE, Butrus S, Epstein AB, Irkec M. Evaluation of comfortusing olopatadine hydrochloride 0.1% ophthalmic solution in the treatmentof allergic conjunctivitis in contact lens wearers compared to placebo usingthe conjunctival allergen-challenge model. Eye Contact Lens.2003;29(2):113-116.
38. Lesher GA, Gunderson GG. Continuous drug delivery through the use ofdisposable contact lenses. Optom Vis Sci. 1993;70(12):1012-1018.
To Obtain COPE Credit Online and Instant CertificateTo obtain COPE CE Credit for this activity, read the material in its entirety and consult referenced sources as necessary. We offer instant certificate processing and support Green CE. Please take this post test and evaluation online by going tohttp://tinyurl.com/OcularSurface1. Upon passing, you will receive your certificate immediately. You must score 70% orhigher to receive credit for this activity, and may take the test up to 2 times.
References
Look for the second CE module of Ocular Surface Wellness—Dry Eye in a coming issue.

Updates in Oc
ular Surface Wellness
Part 1: Ocular Allergy