part i - vsha.org · and is available to families who are displaced due to ... plus care program...
TRANSCRIPT

PART I
Vermont State Housing Authority Page 1 of 2 March 2018 PLEASE KEEP FOR YOUR RECORDS
Equal Housing Opportunity
Provider Vermont State Housing Authority One Prospect Street Montpelier, VT 05602 Phone: 802-828-1991; Fax: 802-828-2111;
Message Line: 1-800-820-5119; TTY: 1-800-798-3118
Housing Choice Voucher Program: Application for Assistance
Thank you for your interest in the Housing Choice Voucher Program. Please make sure to read the instructions below prior to submitting your application as there is important information of which you should be aware.
PLEASE KEEP THESE INSTURCTIONS FOR YOUR RECORDS ALONG WITH PART III
Only return Part II to VSHA • Vermont State Housing Authority operates the Housing Choice Voucher (HCV) Program primarily through telephone, mail and electronic correspondence. If you have questions feel free to contact the Intake Department directly. If you would like to meet with staff it is best to call for an appointment to insure availability. • If you or anyone in your family is a person with disabilities and you need a reasonable accommodation to complete this application, please refer to the “Notice of Right to Reasonable Accommodation” on page 2. • Vermont State Housing Authority will provide free interpretation services to clients who have limited English Proficiency. • If you move and do not update your address, your file may be inactivated during our update. You will need to re-apply. • Please answer all questions on the application form. Do not leave any questions blank. If a question does not apply to you, please write “none”. All Yes or No questions must be checked (√). • If you need more space to answer a question, please attach one or more pages to the application. • Unless specifically indicated, all questions in this application apply to all members of the household. • All information that you provide on this application must be true and complete. It is a violation of federal and state criminal law to make false statements on an application for housing assistance. Vermont State Housing Authority will verify information through computer matching with other federal agencies through HUD’s Upfront Income Verification (UIV) process. If you do not understand a question, please call the Intake Department. • The legal head of household and all adults 18 and over must sign and date the application. • Criminal background checks and sex offender registration checks on all adult household members (including live-in aides) will be completed before determining final eligibility. To qualify for housing assistance an applicant must: • Have an annual income at the time of admission that does not exceed the income limit established by the Department of Housing and Urban Development (HUD).
• Meet the HUD requirements for citizenship or immigration status. • Provide a copy of Social Security cards for all family members when requested. • Pay any money owed to VSHA or any other housing authority. • Not be subject to lifetime sex offender registration requirements. • Sign authorization forms in order to verify eligibility requirements.

PART I
Vermont State Housing Authority Page 2 of 2 March 2018 PLEASE KEEP FOR YOUR RECORDS
• Not have any household members who have engaged in any criminal activity that threatens the health, safety, or right to peaceful enjoyment of the premises by other residents. • Not have any household members who have engaged in any drug-related or violent criminal activity. RETURN COMPLETED APPLICATION (PART II) TO: Vermont State Housing Authority One Prospect St Montpelier, VT 05602 Notice of Right to Reasonable Accommodation A Reasonable Accommodation is intended to enable a person with a disability to have equal access to and enjoyment of the housing programs administered by the Vermont State Housing Authority (VSHA) through changes to either rules, policies or procedures. VSHA is obligated to make an accommodation that is reasonable, provided that doing so does not present an undue financial and administrative burden and has an identifiable relationship to the individual’s disability. If you have a disability and you need: • an exception, change or adjustment in our rules, policies, practices or services that would make it easier for you to apply for or participate in our programs, • a change in the way we communicate with you or give you information, You may ask for this kind of exception, change or adjustment, which we call a Reasonable Accommodation. If you verify you have a disability, if your request is reasonable and financially and administratively possible, we will try to make the changes you request. If you need assistance in making your Request for a Reasonable Accommodation, VSHA staff will be happy to provide help. We will review your request and give you an answer in 10 working days unless there is a problem getting all the information we need or unless you agree to a longer time. We will let you know if we need more information or verification from you or if we would like to talk to you about other ways to meet your needs. If we turn down your request, we will explain the reasons and you can give us more information if you think that will help. To request a Reasonable Accommodation: • Call 1-802-828-1991 • Call 1-800-798-3118 (TTY line) • Write to Vermont State Housing Authority, One Prospect St, Montpelier, VT 05602 • Email [email protected] • Message Line: 1-800-820-5119 If you need help completing the reasonable accommodation form, or if you would like to submit a request in some other way, please let us know.

PART II: Return This Section to VSHA
Page 1 of 2 Vermont State Housing Authority March 2018
Head of Household name: ________________________________ SS#: XXX-XX-_______
Vermont State Housing Authority offers the following preferences that can affect your place on the waiting list. If you feel you qualify for any of these preferences, please check below. The Disaster Preference is ranked the highest of all preferences. The Transitional Housing Preference and Homeless Families with Case Management Support Preference are ranked equally. If a change in these preferences is proposed in the future, a public hearing would be held since the outcome may affect your placement on the waiting list.
Preferences:
1. [ ] Yes [ ] No Disaster Preference: This preference is ranked the highest of all preferences and is available to families who are displaced due to fire, flood, natural disaster, or condemnation by a local, State, or Federal Agency.
2. [ ] Yes [ ] No Preference for Homeless Families with Case Management Support: This Preference will be provided to families who are homeless (as defined below) and who will be receiving regular on-site case management support from a local homeless services, social services or mental health agency for at least one year after moving into a voucher-assisted unit. Status will be verified through the agency providing case management.
Homeless Definition: An individual or family who lacks a fixed, regular, and adequate nighttime residence, meaning: a. An individual or family with a primary nighttime residence that is a public or private place not designed for or ordinarily used as a regular sleeping accommodation for human beings, including a car, park abandoned building, bus or train station, airport, or camping ground; or b. An individual or family living in a supervised publicly or privately operated shelter designated to provide temporary living arrangements (including congregate shelters, transitional housing, and hotels and motels paid for by charitable organizations or by federal, state, or local government programs for low-income individuals); or c. An individual who is exiting an institution where he or she resided for 90 days or less and who resided in an emergency shelter or place not meant for human habitation immediately before entering that institution”. This Preference is limited to no more than 100 applicants / fiscal year

PART II: Return This Section to VSHA
Page 2 of 2 Vermont State Housing Authority March 2018
3. [ ] Yes [ ] No Transitional Housing Preference: This preference is available to individuals and families who are Transitioning from one of the following programs administered by the Vermont State Housing Authority (check appropriate program below):
[ ] VSHA’s / HUD’s Family Unification program for Youth in Transition;
[ ] The Vermont Rental Subsidy Program (a 12 month rapid rehousing Initiative administered by the Vermont Agency of Human Services, Applications for this preference
will be accepted only after 9 months of participation)
[ ] Individuals/families transitioning from a Domestic Violence Transitional Housing Program (currently on or eligible to be on the Continuum of Care Homeless Inventory Chart for homeless beds), these include:
□ Voices against Violence (scattered Site TH)
□ STEPS VT □ Sophie’s Place □ Scattered Site TH
□ WomenSafe [ ] VSHA’s / HUD’s Continuum of Care Programs
□ Shelter+Care: Applicants transitioning from HUD’s/VSHA’s Shelter Plus Care program MUST provide certification from the (Shelter plus Care) sponsoring organization
that the applicant has participated in the shelter plus care program for no less than 36 months and has met the goals of their case management plan.
□ Rapid Rehousing: Applications for this preference will be accepted only after 9 months of participation in Rapid Rehousing
To be considered for the Transitional Housing Preference, applicants must meet the following additional criteria:
1. Actively participating in a case-management plan – which includes an exit plan with an appropriate organization providing these services; and
2. Be in compliance with any lease agreement (verbal or written). Families must be current in their rent and any other conditions of tenancy. Families cannot be subject to an eviction action. VSHA will require Certification from the applicant’s current landlord stating they are in good standing and in compliance with their lease agreement.
If you are claiming one of these local preferences, you must provide us with the name, address and phone number of the Town Health Officer or Agency (homeless services, social services or mental health agency) that can verify your housing situation. Name of Agency who can verify preference status: ___________________________________ Name of Individual (if known) and title who can verify preference status: _______________________ Address of Agency: _________________________ Phone number of Agency /Individual_____________

Vermont State Housing Authority March 2018 Page 1 of 5
PART II: Tenant Information Form Please complete this form and return to: Vermont State Housing Authority One Prospect Street Montpelier, VT 05602
Part 1: Household Information Starting on the first line for the Head of Household, please supply the following information for all adults and children that will live in the housing unit to be assisted. List adults first, then children.
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
More Space for household information on next page
Name: (head of household)_________________________________Email: _________________________
(Street Address) (City) (State) (Zip)
Mailing Address (if different from above)____________________________________________________ Home Phone:_____________________ Cell:_______________________ Work____________________
I am applying for: □Housing Choice Voucher □Project Based Voucher □Moderate Rehab I am interested in the following properties:_______________________________ __________________________ _____________________________ _____________________________ ________________________________ _____________________________ _____________________________ ________________________________
If more space is needed please attach an additional page (see part III for complete list)
If you need assistance completing This form, contact us at: 802-828-1991
Vermont State Housing Authority March 2018 Page 2 of 5
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
1.Last Name 2.First Name 3.MI 4.DOB 5. Gender 6. Relationship to Head ? 7. Disabled
□ Y □ N 8. Ethnicity (check one box) 9. Race (check all that apply) 10. social sec. #
□Hispanic/ □Non-Hispanic/ Latino Latino
□ White □America Indian/Alaska Native □Native Hawaiian/Pacific Islander/other □ Asian □Black/African American
Part 1: Household (continued)
1 Does your family lack a regular nighttime residence, live in a shelter or other non- residential place?
□Yes □ No
2 Is the Head of Household pregnant?
□Yes □ No
3 Have you or anyone in your household every served in the armed services? If so. Who? _______________________ Which Branch? _________________________________
□Yes □ No
4 Do you give VSHA Permission to share your name with the Veterans Administration Medical Center?
Name:__________________________ Signature:__________________________________ □Yes □ No
5 Do you currently live or have you previously lived in, public housing, housing assisted by the Section 8 program, or any other type of federally subsidized housing? □Yes □ No
6 Have you or any member of your household been evicted from public housing, Indian housing,
section 23 housing or housing assisted by the Section 8 program, for drug related criminal activity during the past three years?
□Yes □ No
7 Do you or any member of your household have a history of controlled substance or alcohol abuse
that has not been abated through rehabilitation?
□Yes □ No
8 Have you or any member of your household been convicted of drug-related criminal activity for
manufacture or production of methamphetamine on the premises of federally assisted housing?
□Yes □ No
9 Are you or any member of your household subject to a lifetime sex offender registration under a
state sex offender registration?
□Yes □ No
10
If any child or foster child under age 6 residing in the assisted unit tested positive for EBL list the first name of each child with EBL (elevated blood level) here: _______________________________
□Yes □ No
Vermont State Housing Authority March 2018 Page 3 of 5
Part 2: unit to be occupied by assisted family (if known) Owner Information: Assisted Unit Information:
Name: Address: Apt #: Address: City: Phone: State:
Part 3: Asset Information: 1. Has any member of the family given away or disposed of assets valued at more than $1000 for
less than fair market value during the past two years? □yes □no List household assets held by any family member (even children), in the space provided below. An asset is any one of the following:
401 (k) Checking account Life insurance policies Pensions Stock Bonds Individual retirement accounts Money Market Account Property (Land) Trust Funds Certificate of Deposits Inheritances Mutual Funds Savings Accounts
Documentation Required: Please provide current statements showing the value and interest rate of each asset and check
the “Documentation Attached” box for each income.
Account Holder Type of Account Account # Current Balance Documentation Attached
$ □yes □no verification Source Name and address
Account Holder Type of Account Account # Current Balance Documentation Attached
$ □yes □no verification Source Name and address
Account Holder Type of Account Account # Current Balance Documentation Attached
$ □yes □no verification Source Name and address
Account Holder Type of Account Account # Current Balance Documentation Attached
$ □yes □no verification Source Name and address
Account Holder Type of Account Account # Current Balance Documentation Attached
$ □yes □no verification Source Name and address

Vermont State Housing Authority March 2018 Page 4 of 5
Part 4: Income Information:
1. Did you file a federal income tax return last year? □yes □no 2. Does anyone living outside your household pay for or provide money for any of your household bills or living
expenses? □yes □no List income information for all family members 18 or older, including income received on behalf of the household members under the age of 18. Income is any one of the following:
Alimony Food Stamps Self-Employment Wages/Salaries Child Support Military pay Social Security Benefits Welfare Benefits Financial Assistance to attend school Periodic gifts SSI Workers Compensation Disability Benefits Retirement Payments Unemployment Benefits
DOCUMENTATION REQUIRED: Provide two current and consecutive original paystubs, payroll summary reports, SSA benefit verification letters, child support payment stubs, welfare benefit letters and /or printouts, self-employment tax statements, or unemployment benefits notices, and check the Documentation Attached box for each income.
Member Name
Income type
Monthly income
Documentation attached
□yes □no verification Source Name and address
Member Name
Income type
Monthly income
Documentation attached
□yes □no verification Source Name and address
Member Name
Income type
Monthly income
Documentation attached
□yes □no verification Source Name and address
Member Name
Income type
Monthly income
Documentation attached
□yes □no verification Source Name and address
If you need more space please attach additional page
Part 5: Household Expenses
1. Does any adult household member (18 or older) attend school full time ?(If yes, provide current enrollment and financial aid information from registrar or admissions officer and enter contact information in the section below) □yes □no 2. Does any adult household member (18 or older) have UNREIMBURSED expenses for
child care so that an adult family member can work?
□yes □no 3. Does any member of your family have UNREIMBURSED EXPENSES for care of a person with
disabilities so that an adult family member can work? □yes □no 4. ONLY complete the following if the head of household, spouse, or co-head is age 62
Or older, or has a disability. Does any member of your family have UNREIMBURSED medical expenses (i.e. medical premiums, medical/dental/optical expenses, prescriptions and OTC medicines)
□yes □no List expense information relating to questions marked as yes on next page

Vermont State Housing Authority March 2018 Page 5 of 5
DOCUMENTATION REQUIRED: Provide documentation from verification source showing the monthly payment for each expense and check the Documentation Attached box for each expense.
Member Name Allowance type
Monthly Payment
$ Documentation attached
□yes □no
verification source Name and Address
Member Name Allowance type
Monthly Payment
$ Documentation attached
□yes □no
verification source Name and Address
Member Name Allowance type
Monthly Payment
$ Documentation attached
□yes □no
verification source Name and Address
Member Name Allowance type
Monthly Payment
$ Documentation attached
□yes □no
verification source Name and Address
Member Name Allowance type
Monthly Payment
$ Documentation attached
□yes □no
verification source Name and Address
Part 6: HEAD OF HOUSEHOLD MUST SIGN THIS FORM CERTIFYING ACCURACY OF INFORMATION PROVIDED I certify that the information on this form is true and complete to the best of my knowledge and belief. I understand that I can be fined up to $10,000 or imprisoned up to five years if I furnish false or incomplete information. Name: ______________________________________________ Signature: ___________________________________________ Date: ________________

PART II: Please Return to VSHA
HUD/FEDERALLY MANDATED EXCLUDED INCOME Although not included for purposed of eligibility or rent calculation, HUD requires that nay income received from the
following categories be documented. Please read the list and fill in any lines that are applicable. If more than one family
member received one category, please list them separately.
Exclusion Family Member Annual Amount
Income from employment of children under 18 Payments received from Foster children or Foster adults Lump sum additions to family assets (deferred payment, inheritance, capital gains insurance payments, etc.) Medical Reimbursements Income of Live-in Aide Student Financial Aid Special Armed Services Pay (when family member is exposed to hostile fire) Resident Services Stipend (not to exceed $200 per month Sporadic Income (gifts, pay of a census taker)
Holocaust reparation payments Earnings for full time students (in excess of $480) Doesn’t include head or spouse Adoption Assistance Payments Development Disability Care Payment Refunds and rebates for property taxes PASS (plan for achieving self-support) Other publicly funded programs (amounts specifically for reimbursement of out of pocket expenses to allow participation in a specific program) HUD Funded training program Americorps Living Allowance Indian Settlements/Trust Title IV of the Higher Education Act of 1965 Spina Bifida-any allowance paid under the provision of 38 U.S.C. 1805 to a child suffering from Spina Bifida who is a child of a Vietnam Veteran Agent Orange Settlements Child Care and Development Block Grant Act of 1990 Earned Income Tax Credit Refunds Crime Victim Compensation Title V of the older Americans Act (Senior community Service in Employment Program)
I hereby certify that the above information is true and correct to the best of my knowledge. ______________________________________________ ____________________ Head of household Date
Vermont State Housing Authority1 Prospect StMontpelier, VT 05602
PART II

PART II

Vermont State Housing Authority1 Prospect StMontpelier, VT 05602
PART II

VERMONT STATE HOUSING AUTHORITYREQUEST FOR CRIMINAL RECORD CHECK
SECTION 8 HOUSING
Applicant:
Maiden Name:
Aliases:
Date of Birth:
SS#:
Gender:
Place of Birth:
Phone Number:
List all states in which you have lived:
RELEASE
I, ______________________________, hereby acknowledge and agree to a check of mycriminal record which may be maintained by either the Vermont Criminal Information Centeror the Federal Bureau of Investigation/National Criminal Information Center. I understandthat the results of that check will be made available to the Vermont State Housing Authorityfor use in reviewing my suitability as a tenant. I further understand that I have the right toappeal the results of the criminal record check to the Vermont Criminal Information Center,Department of Public Safety, 103 South Main Street, Waterbury, Vermont, 05671-2101.
Signature of Applicant: Date:
City/Town State Country
Race:
HAPPY Software, Inc. 10/19/2016 Page 1

VERMONT STATE HOUSING AUTHORITYREQUEST FOR CRIMINAL RECORD CHECK
SECTION 8 HOUSING
Applicant:
Maiden Name:
Aliases:
Date of Birth:
SS#:
Gender:
Place of Birth:
Phone Number:
List all states in which you have lived:
RELEASE
I, ______________________________, hereby acknowledge and agree to a check of mycriminal record which may be maintained by either the Vermont Criminal Information Centeror the Federal Bureau of Investigation/National Criminal Information Center. I understandthat the results of that check will be made available to the Vermont State Housing Authorityfor use in reviewing my suitability as a tenant. I further understand that I have the right toappeal the results of the criminal record check to the Vermont Criminal Information Center,Department of Public Safety, 103 South Main Street, Waterbury, Vermont, 05671-2101.
Signature of Applicant: Date:
City/Town State Country
Race:
HAPPY Software, Inc. 10/19/2016 Page 1
OMB Control # 2502-0581Exp. (11/30/2015)
Optional and Supplemental Contact Information for HUD-Assisted Housing Applicants
SUPPLEMENT TO APPLICATION FOR FEDERALLY ASSISTED HOUSINGThis form is to be provided to each applicant for federally assisted housing
Instructions: Optional Contact Person or Organization: You have the right by law to include as part of your application for housing,the name, address, telephone number, and other relevant information of a family member, friend, or social, health, advocacy, or otherorganization. This contact information is for the purpose of identifying a person or organization that may be able to help in resolving anyissues that may arise during your tenancy or to assist in providing any special care or services you may require. You may update,remove, or change the information you provide on this form at any time. You are not required to provide this contact information,but if you choose to do so, please include the relevant information on this form.
Check this box if you choose not to provide the contact information.
Applicant Name:
Mailing Address:
Telephone No: Cell Phone No:
Name of Additional Contact Person or Organization:
Address:
Telephone No: Cell Phone No:
E-Mail Address (if applicable):
Relationship to Applicant:
Reason for Contact: (Check all that apply)
Emergency
Unable to contact you
Termination of rental assistance
Eviction from unit
Late payment of rent
Assist with Recertification Process
Change in lease terms
Change in house rules
Other: ______________________________
Commitment of Housing Authority or Owner: If you are approved for housing, this information will be kept as part of your tenant file. If issuesarise during your tenancy or if you require any services or special care, we may contact the person or organization you listed to assist in resolving theissues or in providing any services or special care to you.
Confidentiality Statement: The information provided on this form is confidential and will not be disclosed to anyone except as permitted by theapplicant or applicable law.
Legal Notification: Section 644 of the Housing and Community Development Act of 1992 (Public Law 102-550, approved October 28, 1992)requires each applicant for federally assisted housing to be offered the option of providing information regarding an additional contact person ororganization. By accepting the applicant’s application, the housing provider agrees to comply with the non-discrimination and equal opportunityrequirements of 24 CFR section 5.105, including the prohibitions on discrimination in admission to or participation in federally assisted housingprograms on the basis of race, color, religion, national origin, sex, disability, and familial status under the Fair Housing Act, and the prohibition onage discrimination under the Age Discrimination Act of 1975.
Signature of Applicant Date
The information collection requirements contained in this form were submitted to the Office of Management and Budget (OMB) under the Paperwork Reduction Act of 1995 (44 U.S.C. 3501-3520). Thepublic reporting burden is estimated at 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completingand reviewing the collection of information. Section 644 of the Housing and Community Development Act of 1992 (42 U.S.C. 13604) imposed on HUD the obligation to require housing providersparticipating in HUD’s assisted housing programs to provide any individual or family applying for occupancy in HUD-assisted housing with the option to include in the application for occupancy the name,address, telephone number, and other relevant information of a family member, friend, or person associated with a social, health, advocacy, or similar organization. The objective of providing suchinformation is to facilitate contact by the housing provider with the person or organization identified by the tenant to assist in providing any delivery of services or special care to the tenant and assist withresolving any tenancy issues arising during the tenancy of such tenant. This supplemental application information is to be maintained by the housing provider and maintained as confidential information.Providing the information is basic to the operations of the HUD Assisted-Housing Program and is voluntary. It supports statutory requirements and program and management controls that prevent fraud,waste and mismanagement. In accordance with the Paperwork Reduction Act, an agency may not conduct or sponsor, and a person is not required to respond to, a collection of information, unless thecollection displays a currently valid OMB control number.
Privacy Statement: Public Law 102-550, authorizes the Department of Housing and Urban Development (HUD) to collect all the information (except the Social Security Number (SSN)) which will beused by HUD to protect disbursement data from fraudulent actions.
Form HUD- 92006 (05/09)
PART II: RETURN THIS SECTION TO VSHA
Please return to VSHA: 1 Prospect St. Montpelier,VT 05602 3

Paperwork Reduction Notice: Public reporting burden for this collection of information is estimated to average 7 minutesper response. This includes the time for respondents to read the document and certify, and any recordkeeping burden. Thisinformation will be used in the processing of a tenancy. Response to this request for information is required to receivebenefits. The agency may not collect this information, and you are not required to complete this form, unless it displaysa currently valid OMB control number. The OMB Number is 2577‐0266, and expires 08/31/2016.
NOTICE TO APPLICANTS AND PARTICIPANTS OF THE FOLLOWING HUD RENTAL ASSISTANCE PROGRAMS:
Public Housing (24 CFR 960)
Section 8 Housing Choice Voucher, including the Disaster Housing Assistance Program (24 CFR 982)
Section 8 Moderate Rehabilitation (24 CFR 882)
Project-Based Voucher (24 CFR 983)
The U.S. Department of Housing and Urban Development maintains a national repository of debts owed to Public Housing Agencies (PHAs) or Section 8 landlords and adverse information of former participants who have voluntarily or involuntarily terminated participation in one of the above-listed HUD rental assistance programs. This information is maintained within HUD’s Enterprise Income Verification (EIV) system, which is used by Public Housing Agencies (PHAs) and their management agents to verify employment and income information of program participants, as well as, to reduce administrative and rental assistance payment errors. The EIV system is designed to assist PHAs and HUD in ensuring that families are eligible to participate in HUD rental assistance programs and determining the correct amount of rental assistance a family is eligible for. All PHAs are required to use this system in accordance with HUD regulations at 24 CFR 5.233.
HUD requires PHAs, which administers the above-listed rental housing programs, to report certain information at the conclusion of your participation in a HUD rental assistance program. This notice provides you with information on what information the PHA is required to provide HUD, who will have access to this information, how this information is used and your rights. PHAs are required to provide this notice to all applicants and program participants and you are required to acknowledge receipt of this notice by signing page 2. Each adult household member must sign this form.
What information about you and your tenancy does HUD collect from the PHA? The following information is collected about each member of your household (family composition): full name, date of birth, and Social Security Number.
The following adverse information is collected once your participation in the housing program has ended, whether you voluntarily or involuntarily move out of an assisted unit:
1. Amount of any balance you owe the PHA or Section 8 landlord (up to $500,000) and explanation for balance owed(i.e. unpaid rent, retroactive rent (due to unreported income and/ or change in family composition) or other chargessuch as damages, utility charges, etc.); and
2. Whether or not you have entered into a repayment agreement for the amount that you owe the PHA; and3. Whether or not you have defaulted on a repayment agreement; and4. Whether or not the PHA has obtained a judgment against you; and5. Whether or not you have filed for bankruptcy; and6. The negative reason(s) for your end of participation or any negative status (i.e., abandoned unit, fraud, lease
violations, criminal activity, etc.) as of the end of participation date.
U.S. Department of Housing and Urban Development Office of Public and Indian Housing
DEBTS OWED TO PUBLIC HOUSING AGENCIES AND TERMINATIONS
OMB No. 2577-0266 Expires 08/31/2016
08/2013 Form HUD-52675
PART II

2
Who will have access to the information collected? This information will be available to HUD employees, PHA employees, and contractors of HUD and PHAs.
How will this information be used? PHAs will have access to this information during the time of application for rental assistance and reexamination of family income and composition for existing participants. PHAs will be able to access this information to determine a family’s suitability for initial or continued rental assistance, and avoid providing limited Federal housing assistance to families who have previously been unable to comply with HUD program requirements. If the reported information is accurate, a PHA may terminate your current rental assistance and deny your future request for HUD rental assistance,subject to PHA policy.
How long is the debt owed and termination information maintained in EIV? Debt owed and termination information will be maintained in EIV for a period of up to ten (10) years from the end of participation date.
What are my rights? In accordance with the Federal Privacy Act of 1974, as amended (5 USC 552a) and HUD regulations pertaining to its implementation of the Federal Privacy Act of 1974 (24 CFR Part 16), you have the following rights: 1. To have access to your records maintained by HUD, subject to 24 CFR Part 16.2. To have an administrative review of HUD’s initial denial of your request to have access to your records maintained
by HUD.3. To have incorrect information in your record corrected upon written request.4. To file an appeal request of an initial adverse determination on correction or amendment of record request within
30 calendar days after the issuance of the written denial.5. To have your record disclosed to a third party upon receipt of your written and signed request.
What do I do if I dispute the debt or termination information reported about me? If you disagree with the reported information, you should contact in writing the PHA who has reported this information
about you. The PHA’s name, address, and telephone numbers are listed on the Debts Owed and Termination Report.You have a right to request and obtain a copy of this report from the PHA. Inform the PHA why you dispute the
information and provide any documentation that supports your dispute. HUD's record retention policies at 24 CFR Part 908and 24 CFR Part 982 provide that the PHA may destroy your records three years from the date your participation in the program ends. To ensure the availability of your records, disputes of the original debt or termination information must bemade within three years from the end of participation date; otherwise the debt and termination information will be presumed correct. Only the PHA who reported the adverse information about you can delete or correct your record.
Your filing of bankruptcy will not result in the removal of debt owed or termination information from HUD’s EIV system. However, if you have included this debt in your bankruptcy filing and/or this debt has been discharged by the bankruptcy court, your record will be updated to include the bankruptcy indicator, when you provide the PHA with documentation of your bankruptcy status.
The PHA will notify you in writing of its action regarding your dispute within 30 days of receiving your written dispute. If the PHA determines that the disputed information is incorrect, the PHA will update or delete the record. If the PHA determines that the disputed information is correct, the PHA will provide an explanation as to why the information is correct.
This Notice was provided by the below-listed PHA: I hereby acknowledge that the PHA provided me with the Debts Owed to PHAs & Termination Notice:
Signature Date
Printed Name
OMB No. 2577-0266 Expires 08/31/2016
08/2013 Form HUD-52675
PART II
Paperwork Reduction Notice: Public reporting burden for this collection of information is estimated to average 7 minutesper response. This includes the time for respondents to read the document and certify, and any recordkeeping burden. Thisinformation will be used in the processing of a tenancy. Response to this request for information is required to receivebenefits. The agency may not collect this information, and you are not required to complete this form, unless it displaysa currently valid OMB control number. The OMB Number is 2577‐0266, and expires 08/31/2016.
NOTICE TO APPLICANTS AND PARTICIPANTS OF THE FOLLOWING HUD RENTAL ASSISTANCE PROGRAMS:
Public Housing (24 CFR 960)
Section 8 Housing Choice Voucher, including the Disaster Housing Assistance Program (24 CFR 982)
Section 8 Moderate Rehabilitation (24 CFR 882)
Project-Based Voucher (24 CFR 983)
The U.S. Department of Housing and Urban Development maintains a national repository of debts owed to Public Housing Agencies (PHAs) or Section 8 landlords and adverse information of former participants who have voluntarily or involuntarily terminated participation in one of the above-listed HUD rental assistance programs. This information is maintained within HUD’s Enterprise Income Verification (EIV) system, which is used by Public Housing Agencies (PHAs) and their management agents to verify employment and income information of program participants, as well as, to reduce administrative and rental assistance payment errors. The EIV system is designed to assist PHAs and HUD in ensuring that families are eligible to participate in HUD rental assistance programs and determining the correct amount of rental assistance a family is eligible for. All PHAs are required to use this system in accordance with HUD regulations at 24 CFR 5.233.
HUD requires PHAs, which administers the above-listed rental housing programs, to report certain information at the conclusion of your participation in a HUD rental assistance program. This notice provides you with information on what information the PHA is required to provide HUD, who will have access to this information, how this information is used and your rights. PHAs are required to provide this notice to all applicants and program participants and you are required to acknowledge receipt of this notice by signing page 2. Each adult household member must sign this form.
What information about you and your tenancy does HUD collect from the PHA? The following information is collected about each member of your household (family composition): full name, date of birth, and Social Security Number.
The following adverse information is collected once your participation in the housing program has ended, whether you voluntarily or involuntarily move out of an assisted unit:
1. Amount of any balance you owe the PHA or Section 8 landlord (up to $500,000) and explanation for balance owed(i.e. unpaid rent, retroactive rent (due to unreported income and/ or change in family composition) or other chargessuch as damages, utility charges, etc.); and
2. Whether or not you have entered into a repayment agreement for the amount that you owe the PHA; and3. Whether or not you have defaulted on a repayment agreement; and4. Whether or not the PHA has obtained a judgment against you; and5. Whether or not you have filed for bankruptcy; and6. The negative reason(s) for your end of participation or any negative status (i.e., abandoned unit, fraud, lease
violations, criminal activity, etc.) as of the end of participation date.
U.S. Department of Housing and Urban Development Office of Public and Indian Housing
DEBTS OWED TO PUBLIC HOUSING AGENCIES AND TERMINATIONS
OMB No. 2577-0266 Expires 08/31/2016
08/2013 Form HUD-52675
PART II

2
Who will have access to the information collected? This information will be available to HUD employees, PHA employees, and contractors of HUD and PHAs.
How will this information be used? PHAs will have access to this information during the time of application for rental assistance and reexamination of family income and composition for existing participants. PHAs will be able to access this information to determine a family’s suitability for initial or continued rental assistance, and avoid providing limited Federal housing assistance to families who have previously been unable to comply with HUD program requirements. If the reported information is accurate, a PHA may terminate your current rental assistance and deny your future request for HUD rental assistance,subject to PHA policy.
How long is the debt owed and termination information maintained in EIV? Debt owed and termination information will be maintained in EIV for a period of up to ten (10) years from the end of participation date.
What are my rights? In accordance with the Federal Privacy Act of 1974, as amended (5 USC 552a) and HUD regulations pertaining to its implementation of the Federal Privacy Act of 1974 (24 CFR Part 16), you have the following rights: 1. To have access to your records maintained by HUD, subject to 24 CFR Part 16.2. To have an administrative review of HUD’s initial denial of your request to have access to your records maintained
by HUD.3. To have incorrect information in your record corrected upon written request.4. To file an appeal request of an initial adverse determination on correction or amendment of record request within
30 calendar days after the issuance of the written denial.5. To have your record disclosed to a third party upon receipt of your written and signed request.
What do I do if I dispute the debt or termination information reported about me? If you disagree with the reported information, you should contact in writing the PHA who has reported this information
about you. The PHA’s name, address, and telephone numbers are listed on the Debts Owed and Termination Report.You have a right to request and obtain a copy of this report from the PHA. Inform the PHA why you dispute the
information and provide any documentation that supports your dispute. HUD's record retention policies at 24 CFR Part 908and 24 CFR Part 982 provide that the PHA may destroy your records three years from the date your participation in the program ends. To ensure the availability of your records, disputes of the original debt or termination information must bemade within three years from the end of participation date; otherwise the debt and termination information will be presumed correct. Only the PHA who reported the adverse information about you can delete or correct your record.
Your filing of bankruptcy will not result in the removal of debt owed or termination information from HUD’s EIV system. However, if you have included this debt in your bankruptcy filing and/or this debt has been discharged by the bankruptcy court, your record will be updated to include the bankruptcy indicator, when you provide the PHA with documentation of your bankruptcy status.
The PHA will notify you in writing of its action regarding your dispute within 30 days of receiving your written dispute. If the PHA determines that the disputed information is incorrect, the PHA will update or delete the record. If the PHA determines that the disputed information is correct, the PHA will provide an explanation as to why the information is correct.
This Notice was provided by the below-listed PHA: I hereby acknowledge that the PHA provided me with the Debts Owed to PHAs & Termination Notice:
Signature Date
Printed Name
OMB No. 2577-0266 Expires 08/31/2016
08/2013 Form HUD-52675
PART II

PART II
Page 1 of 2
Declaration of Citizenship Please complete this form and return to: Vermont State Housing Authority 1 Prospect Street Montpelier, VT 05602
Part 1: Applies to All Family/Household Members Each person who will benefit under the Section 8 Rental Assistance Program must either be a citizen or national of the United States, or be a noncitizen who has eligible immigration status that qualifies them for rental assistance as determined by the U.S. Department of Housing and Urban Development and the U.S. Immigration and Naturalization Service.
One box on this form must be checked for each family member indicating status as a citizen or a national of the United States, or a noncitizen with eligible immigration status. Family members residing in the unit to be assisted that do not claim to be a citizen or national of the United States, or do not claim to be a noncitizen with eligible immigration status should not check any box.
All adults must sign where indicated. For each child who is not 18 years of age, the form must be signed by an adult member of the family residing in the dwelling unit who is responsible for the child.
Head of Household Certification As head of household I certify, under penalty of perjury, that all members of my household are listed on Part 1 of this form and that members of my household that have not checked either box on Part 1 of this form do not claim to be citizens or nationals of the United States, or noncitizens with eligible immigration status.
Signature Date
First Name Last Name Age
I am a citizen or a national of the U.S
I am a noncitizen with eligible immigration status
Signature of Adult listed to the left, or Signature of Guardian for Minors
□ □ X
□ □ X
□ □ X
□ □ X
□ □ X
□ □ X
□ □ X
□ □ X
□ □ X
Warning- Title 18 US Code Section 1001 states that a person is guilty of a felony for knowingly and willingly making a false or fraudulent statement to any department or agency of the United States. If this form contains false or incomplete information, you may be required to repay all overpaid rental assistance you received; fined up to $10,000; imprisoned for up to 5 years; and/or prohibited from receiving future assistance.

PART II
Page 2 of 2
Part 2: Applies to Noncitizen Family Members Only All family members who have claimed eligible immigration status on Part 1 of this form must provide this office with an original of one of the following documents:
(1) Form I-551, Alien Registration Receipt Cart (2) Form I-94, Arrival-Departure Record with appropriate annotations or documents (3) Form I-688, Temporary Resident Card (4) Form I-688B, Employment Authorization Card (5) A receipt issued by the INS indicating that an application for issuance of a replacement document in
one of the above-listed categories has been made and the applicant’s entitlement to the document has been verified.
Consent to Verify Eligible Immigration Status Each family member required to complete part 2 of this form must sign below granting consent to verify eligible immigration status. For each child who is not 18 years of age, the form must be signed by an adult member of the family residing in the dwelling unit who is responsible for the child.
Office Use
Only
INS VERIF. #
First Name Last Name Age
Signature of Adult listed to the left, or Signature of Guardian for Minors
X
X
X
X
X
X
X
X
X
Evidence supplied with this form may be released by the Housing Agency, without responsibility for its further use or transmission, to the Immigration and Naturalization Service for purposes of verification of the immigration status of the individual or to the U.S Department of Housing and Urban Development, as required. The U. S. Department of Housing and Urban Development is not responsible for the further use or transmission of the evidence or other information.

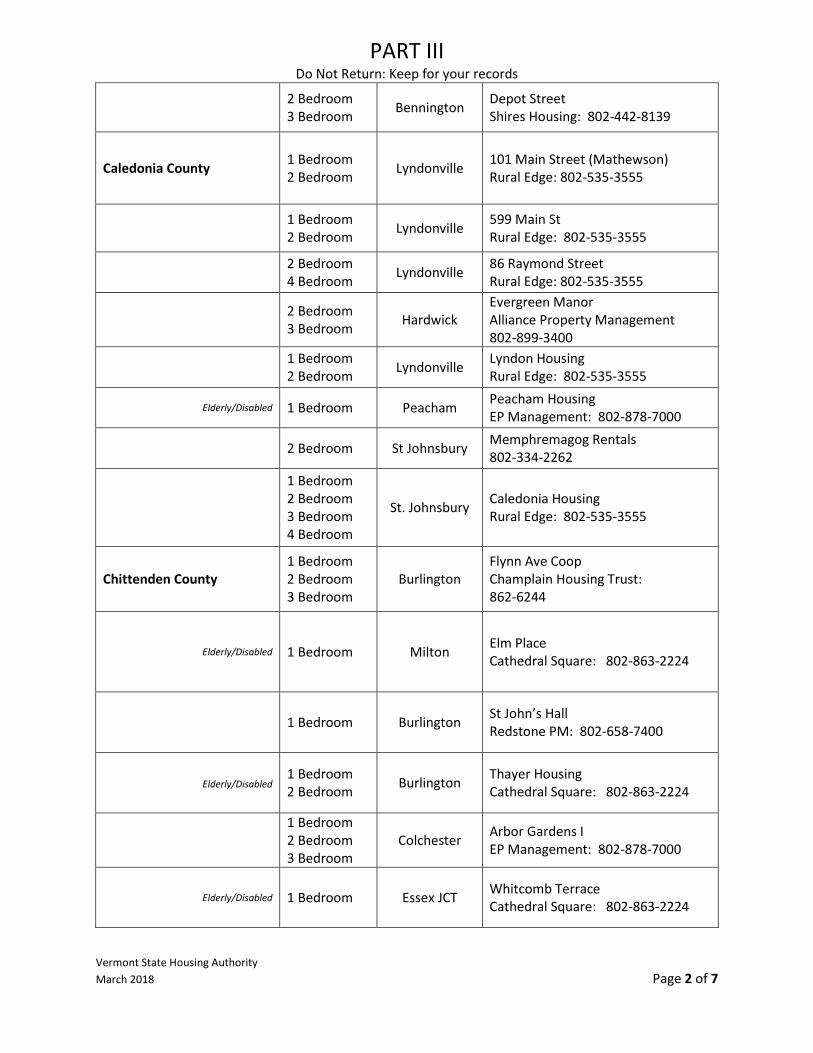
PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 1 of 7
Project Based Voucher Option: The following properties have set number of units with a subsidy attached to them. A tenant living in one of the assisted units will pay 30% of their adjusted monthly income towards rent and utilities.
Choosing to be on the waiting list for a specific property under this project based assistance does not affect your status on the regular Housing Choice Voucher waiting list.
Properties with Elderly/disabled are designated housing for persons over the age of 62 or those who are disabled. Location Property
Addison County 2 Bedroom 3 Bedroom Bristol Bristol Family Housing
ACCT: 802-877-3749
0 Bedroom 1 Bedroom Middlebury Court Street Apartments
ACCT: 802-877-3749
2 Bedroom 3 Bedroom Waltham McKnight Ln
ACCTL 802-877-3749
Elderly/Disabled 1 Bedroom Middlebury Middlebury Commons VSHA: 802-828-1045
2 Bedroom 3 Bedroom 4 Bedroom
Middlebury North Pleasant Street Apts ACCT: 802-877-3749
1 Bedroom 2 Bedroom 3 Bedroom
Middlebury Pine Meadow Apartments Maloney Properties: 802-472-5016
2 bedroom 3 Bedroom Middlebury Seminary Street Apartments
ACCT: 802-877-3749
1 Bedroom 2 Bedroom 3 Bedroom
Middlebury Smith Housing ACCT: 802-877-3749
1 Bedroom 3 Bedroom Middlebury Vergennes Housing
ACCT: 802-877-3749
Elderly/Disabled 1 Bedroom Vergennes Willow Apartments Summit PM: 802-846-5430
Bennington County
1 Bedroom 2 Bedroom 3 Bedroom
Bennington
Applegate Apartments Shires Housing: 802-442-8139
1 Bedroom 2 Bedroom 3 Bedroom
Bennington/ Arlington
Battenkill North Shires Housing: 802-442-8139
PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 2 of 7
2 Bedroom 3 Bedroom Bennington Depot Street
Shires Housing: 802-442-8139
Caledonia County 1 Bedroom 2 Bedroom Lyndonville
101 Main Street (Mathewson) Rural Edge: 802-535-3555
1 Bedroom 2 Bedroom Lyndonville 599 Main St
Rural Edge: 802-535-3555
2 Bedroom 4 Bedroom Lyndonville 86 Raymond Street
Rural Edge: 802-535-3555
2 Bedroom 3 Bedroom Hardwick
Evergreen Manor Alliance Property Management 802-899-3400
1 Bedroom 2 Bedroom Lyndonville Lyndon Housing
Rural Edge: 802-535-3555
Elderly/Disabled 1 Bedroom Peacham Peacham Housing EP Management: 802-878-7000
2 Bedroom St Johnsbury Memphremagog Rentals 802-334-2262
1 Bedroom 2 Bedroom 3 Bedroom 4 Bedroom
St. Johnsbury Caledonia Housing Rural Edge: 802-535-3555
Chittenden County 1 Bedroom 2 Bedroom 3 Bedroom
Burlington Flynn Ave Coop Champlain Housing Trust: 862-6244
Elderly/Disabled 1 Bedroom Milton Elm Place Cathedral Square: 802-863-2224
1 Bedroom Burlington St John’s Hall Redstone PM: 802-658-7400
Elderly/Disabled 1 Bedroom 2 Bedroom Burlington Thayer Housing
Cathedral Square: 802-863-2224
1 Bedroom 2 Bedroom 3 Bedroom
Colchester Arbor Gardens I EP Management: 802-878-7000
Elderly/Disabled 1 Bedroom Essex JCT Whitcomb Terrace Cathedral Square: 802-863-2224

PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 3 of 7
Elderly/Disabled 1 Bedroom 2 Bedroom Milton School Street Manor
Simplicity PM: 802-861-6468
Elderly/Disabled 1 Bedroom 2 Bedroom 3 Bedroom
Shelburne Harrington Village Cathedral Square: 802-863-2224
Elderly/Disabled 0 Bedroom 1 Bedroom Winooski Genest Building
Farrell: 802-863-0224
Essex County 2 Bedroom 3 Bedroom 4 Bedroom
Brighton Brighton Scattered Rural Edge: 802-535-3555
Elderly/Disabled & Family
1 Bedroom 2 Bedroom Island Pond Alder/Mountain
MG Contracting: 802-723-6130
Franklin County 1 Bedroom 2 Bedroom St. Abans Driscoll Block
Americanadian LLC: 802-527-2300
1 Bedroom 2 Bedroom Enosburg Falls
Falls Housing LP Champlain Housing Trust: 862-6244
Elderly/Disabled 1 Bedroom Fairfax Hidden Pines Champlain Housing Trust: 802-862-6244
Elderly/Disabled 0 Bedroom Franklin Franklin Carriage House Franklin Homestead: 802-285-2944
1 Bedroom 2 Bedroom Richford
Main Street Mill Alliance Property Management: 802-899-3400
Elderly/Disabled 1 Bedroom 2 Bedroom St Albans Hawk’s Nest
802 PM: 802-879-6507
Elderly/Disabled 1 Bedroom St. Albans Welden Villa Apartments VSHA: 802-828-1045
Grand Isle County Service Enriched
1 Bedroom 2 Bedroom 3 Bedroom
Grand Isle Isle Lane Champlain Housing Trust: 862-6244
Lamoille County 1 Bedroom 2 Bedroom Morrisville
Arthur’s Main St. Housing Alliance Property Management: 802-899-3400
Orange County
Service Enriched
1 Bedroom 2 Bedroom 3 Bedroom
Bradford Waits River Housing DOWNSTREET: 802-476-4493

PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 4 of 7
Elderly/Disabled 0 Bedroom 1 Bedroom Chelsea The Gardens
TGWS: 802-433-1600
1 Bedroom 2 Bedroom Randolph Hedding Drive
Stewart PM: (603) 641-2163
1 Bedroom 2 Bedroom 3 Bedroom
Randolph Salisbury Square Stewart PM: (603) 641-2163
Orleans County 1 Bedroom 2 Bedroom Derby Derby Housing
Rural Edge: 802-535-3555
Elderly/Disabled 1 Bedroom 2 Bedroom Derby Hotel/ Kidder
Rural Edge: 802-535-3555
2 Bedroom Newport Memphremagog rentals 802-334-2262
1 Bedroom 2 Bedroom 3 Bedroom
Newport Ctr Choquette Scattered Sites 802-334-6304
Rutland County Service enriched/ Elderly/Disabled
1 Bedroom 2 Bedroom 3 Bedroom
Brandon Parkvillage Apartments Summit PM: 802-846-5430
Elderly/Disabled 1 Bedroom Fair Haven Adams House Housing Trust of Rutland County: 802-775-3139
Elderly/Disabled 1 Bedroom Fair Haven Parkview Apartments John Hamel: 802-349-5225
2 Bedroom 3 Bedroom Rutland
Columbian Avenue Housing Trust of Rutland County: 802-775-3139
3 Bedroom Rutland Marble Street Housing Trust of Rutland County: 802-775-3139
1 Bedroom 2 Bedroom 3 Bedroom
Rutland Rutland Rehab Scattered Site Housing Trust of Rutland County: 802-775-3139
2 Bedroom West Rutland Kazon Building
TPM: 802-496-9400
1 Bedroom 2 Bedroom West Rutland
Stanislaus Apartments Housing Trust of Rutland County: 802-775-3139
Washington County
1 Bedroom 2 Bedroom 3 Bedroom
Barre Good Neighbors DOWNSTREET: 802-476-4493
Elderly/Disabled 1 Bedroom 2 Bedroom Cabot Cabot Commons
DOWNSTREET: 802-476-4493

PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 5 of 7
Service Enriched 1 Bedroom 2 Bedroom Northfield Dogwood Glen I
VSHA: 802-828-1045
2 Bedroom 3 Bedroom Plainfield Hollister Hill Apartments
VSHA: 802-828-1045
Elderly/Disabled 1 Bedroom Waitsfield Evergreen Place Senior Housing DOWNSTREET: 802-476-4493
Elderly/Disabled 1 Bedroom Waterbury Stimson & Graves Building
DOWNSTREET: 802-476-4493
1 Bedroom 2 Bedroom Waterbury Ctr. Green Mountain Seminary Apts
DOWNSTREET: 802-476-4493
Windham County 1 Bedroom 2 Bedroom 3 Bedroom
Bellows Falls Bellows Falls Housing Stewart PM: (603) 641-2163
1 Bedroom 2 Bedroom Bellows Falls Howard Block
Stewart PM: (603) 641-2163
1 Bedroom 2 Bedroom 4 Bedroom
Bellows Falls Pine Street Stewart PM: (603) 641-2163
2 Bedroom 3 Bedroom Brattleboro Clark Street
W-WHT-(802) 254-4604
1 Bedroom 2 Bedroom Brattleboro Abbott Block
Stewart PM: (603) 641-2163
2 Bedroom Brattleboro Canal Street Apartments W-WHT-(802) 254-4604
Service Enriched
0 Bedroom 1 Bedroom 2 Bedroom 3 Bedroom 4 Bedroom
Brattleboro Esteyville Housing W-WHT-(802) 254-4604
0 Bedroom 1 Bedroom 2 Bedroom 3 Bedroom
Brattleboro Portfolio Enhancement I W-WHT-(802) 254-4604
0 Bedroom 1 Bedroom 2 Bedroom
Brattleboro Portfolio Enhancement II W-WHT- (802) 254-4604
1 Bedroom Brattleboro The Wilder Building W-WHT-(802) 254-4604
1 Bedroom 2 Bedroom 3 Bedroom
Brattleboro Westgate Allocated Stewart PM: (603) 641-2163

PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 6 of 7
2 Bedroom 3 Bedroom Brattleboro Westgate Bond
Stewart PM: (603) 641-2163
1 Bedroom 2 Bedroom 3 Bedroom
Brattleboro Whetstone W-WHT-(802) 254-4604
Elderly/Disabled 1 Bedroom 2 Bedroom Brattleboro
Red Clover Commons Brattleboro Housing Authority (802) 254-5590
1 Bedroom 2 Bedroom 3 Bedroom
Guilford Algiers W-WHT-(802) 254-4604
Elderly/Disabled 0 Bedroom Putney Noyes House W-WHT-(802) 254-4604
1 Bedroom 2 Bedroom 3 Bedroom
W Brattleboro Western Avenue Housing W-WHT-(802) 254-4604
Elderly/Disabled 1 Bedroom W. Dover Butterfield Elderly Housing Stewart PM: (603) 641-2163
Windsor County 1 Bedroom 2 Bedroom Chester Chester Gage
Stewart PM: (603) 641-2163
Elderly/Disabled 1 Bedroom Hartford Colodny Building VSHA: 802-828-1045
Service Enriched 1 Bedroom 2 Bedroom 3 Bedroom
Ludlow Black River Overlook Stewart PM: (603) 641-2163
Elderly/Disabled 1 Bedroom Proctorsville Freeman House Stewart PM: (603) 641-2163
2 Bedroom Proctorsville Proctorsville Green Stewart PM: (603) 641-2163
1 Bedroom 2 Bedroom 3 Bedroom
Woodstock Safford Commons Twin Pines: (802)291-7000
1 Bedroom 2 Bedroom 3 Bedroom
Springfield Southview Stewart PM: (603) 641-2163
1 Bedroom 2 Bedroom 3 Bedroom
Springfield Westview Terrace Springfield Housing: 802-885-4905
1 Bedroom 2 Bedroom
White River Jct
Hartford Scattered-PBV Twin Pines: (802)291-7000
1 Bedroom 2 Bedroom
White River Jct
Hartford Scattered-VASH Twin Pines: (802)291-7000

PART III
Do Not Return: Keep for your records
Vermont State Housing Authority March 2018 Page 7 of 7
1 Bedroom 2 Bedroom White River Jct Morale House
Twin Pines: 802-291-7000
Service Enriched
1 Bedroom 2 Bedroom 3 Bedroom 4 Bedroom
White River Jct Northwoods VSHA: 802-828-1045
Service Enriched 1 Bedroom 2 Bedroom 3 Bedroom
Windsor Union Square Stewart PM: (603) 641-2163
Moderate Rehabilitation Property Option: The following Mod Rehab Properties have vacancies from time to time. If you choose to live in one of these units, you will pay 30% of your monthly adjusted income towards rent and utilities. The Mod Rehab program is not funded from the same monies as Housing Choice Voucher program, so you cannot take your assistance with you if you move from the property. You may remain on the Housing Choice Voucher waiting list while living in one of these units.
Location Property
Caledonia County 0 Bedroom 1 Bedroom 2 Bedroom
St. Johnsbury
Depot Square Apartments: (802) 748-4330
Chittenden County 0 Bedroom Burlington Sara Cole House: Champlain Housing Trust 802-862-6244
0 Bedroom Burlington
St. John's Hall Redstone PM: 802-658-7400
Orange County 2 Bedroom 3 Bedroom Wells River
Ottati apartments EP Management: 802-775-1100
Washington County 1 Bedroom 2 Bedroom 3 Bedroom
Northfield Alan Ritchie Vine St: 224-6254
Lamoille County 2 Bedroom 3 Bedroom Morrisville
Sunset Apartments Phyllis Houle: 802-888-4021