patellar tendiopathy, lumbar spine herniation, serratus anterior dysfunction, neck injury
TRANSCRIPT

Patellar tendinopathy (PT) affects an athlete’s performance ability to jump, land, change direction and run. It can lead to a reduction in tolerance of training and competition load, and eventually a decline in performance, resulting in missed training and competition.
Managing PT during the competition phase of a season can be frustrating. High loads are continually placed on the tendon, and the condition can be frequently slow to respond to treatment interventions. It is important to be realistic and not expect a full recovery of the tendon during this in-season phase.
Subjective historyWhen diagnosing athletes with suspected
PT, a thorough subjective history must be taken before a clinical examination takes place. This helps with not only an accurate diagnosis, but also gives an understanding of the potential causes and the severity of the tendinopathy. Critical questions to ask are shown in Table 1 below.
Once a thorough subjective history has been completed, a clinician should have a primary diagnosis, understand how irritable the tendon is, what phase the tendon is in and reasons as to why the PT is present. This will help guide a physical assessment.
Physical assessment A therapist assessing the athlete should already have a strong primary diagnosis
based on the subjective history. The priority of the physical examination is to confirm the primary hypothesis, exclude other potential hypothesis and to determine the irritability of the tendon, which will ascertain the functionality of the athlete. Table 2 outlines the best current thinking on examination procedures.
Further investigationsImaging using MRI and ultrasound can identify the presence of pathology in the t e n d o n . U l t r a s o u n d ( U S ) t i s s u e characterisation shows the amount of disorganisation within a tendon and can help characterise the extent of structural pathology(2). However the presence of a PT on
Patellar tendinopathy
Jumpers knee: an in-season management approachPatellar tendinopathy is a common injury in jumping sports, especially when loads are high or suddenly increase. With this in mind, Luke Heath guides the practitioner through the problem-solving steps required to formulate a rehabilitation program for restoring the load absorption capacity of a grumbling patella tendon…
diagnosis • treatment • rehabilitation • prevention
ISSN: 2397-6640 Issue 154 MAY 2016
From the editorIt’s at this time of year when the athletic season gets into full swing, which means that sportsmen and women up and down the country will be entering the hardest phase of their training. And with increased training load and volume comes increased injury risk, which is reflected in the content of this issue.
In our lead article, Luke Heath considers the issue of patellar tendinopathy, a common injury in sports involving jumping, especially when loads are high or suddenly increase. With this in mind, Luke provides advice on history taking and diagnosis, and guides the practitioner through the problem-solving steps required to formulate a rehabilitation program for restoring full the load absorption capacity.
Following on, Chris Mallac discusses the lengthy rehab period following a micro-discectomy procedure, which is a relatively common procedure in elite athletes needing a rapid return to sport - for example so as not to miss out on the peak season of competition. In addition, goes on
to provide a host of strength-based exercises aimed at restoring function as quickly as possible.
Chris is obviously a very busy man as he is also the author of our third article! In it, he looks at serratus anterior. Dysfunction in this muscle can lead to shoulder injuries such as impingement, rotator cuff breakdown and performance decrements during overhead tasks, all of which are more likely to reveal themselves at times of increased training load. Chris Mallac looks at its anatomy and biomechanics, and highlights some clinically relevant exercises designed to retrain serratus anterior function.
Rounding up the issue, Kay Robinson continues with her discussion of sporting injuries to the neck. In the previous issue, Kay provided a detailed guide to neck injury assessment. In this article she focuses on the best approaches to neck injury management and rehabilitation, with the goal of a safe and speedy return to full performance.
We take an early summer break in June,
but we’ll see you again in early July with more cutting-edge guidance and advice on the diagnosis, treatment, rehab and prevention of sports injuries!
Andrew Hamilton BSc Hons MRSC ACSM (commissioning editor)
In this issuePatellar tendinopathy in jumpers: restoration of load-bearing capacity 1
Lumbar spine disc herniation: post-surgery rehab and strength-training programme 5
Serratus anterior dysfunction: anatomy, biomechanics and how to restore optimum function 10
Neck injuries: management and rehab for a safe and speedy return to sport 15
2 SPORTS INJURY BULLETIN No 154
completely, a de-training effect will occur. Isometric single leg knee extensions
and/or single leg decline squats should be prescribed for pain reduction: 5 repetitions x 10-60 second holds performed four-times per day. In reactive tendons, isometric contractions with moderate-heavy loads has been reported to be effective in reducing pain for hours(2,3,6). It is important that these exercises do
not further aggravate the tendon, so prescribe the correct time and appropriate
management of a PT is favourable. The initial treatments goals are aimed at pain management, education and planning.
Pain management Relative rest is the first priority to unload
the reactive tendon. However, there should not be complete cessation of activities because this will decrease the overall capacity of the tendon(5). The overall capacity refers to the amount of load a tendon can withstand and by resting
imaging does not always mean it is the source of pain, and clinical confirmation is necessary(3). MRI and US imaging are the two modalities used in my practice; an acute strain to a tendon should be excluded and the US can help confirm worsening tendon pathology. Management of a tendon differs according to what phase a tendinopathy is in.
Acute Management Whilst the pathology of the tendon may never completely resolve, conservative
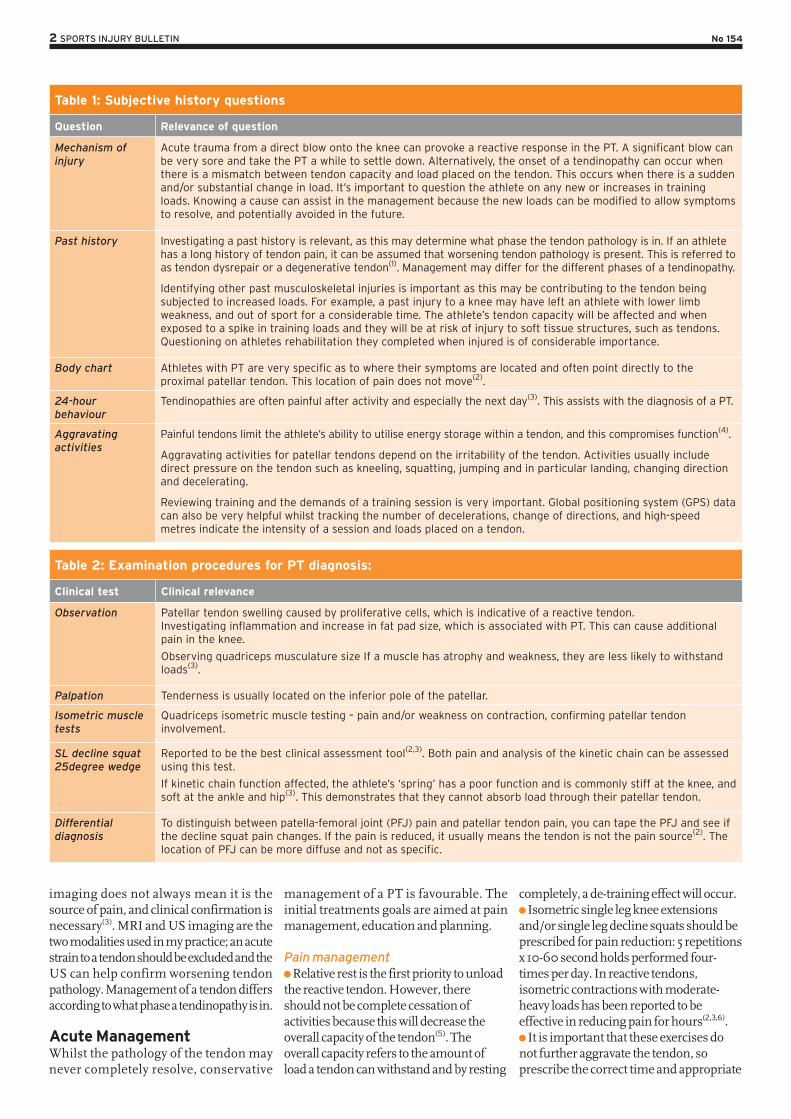
Table 1: Subjective history questions
Question Relevance of question
Mechanism of injury
Acute trauma from a direct blow onto the knee can provoke a reactive response in the PT. A significant blow can be very sore and take the PT a while to settle down. Alternatively, the onset of a tendinopathy can occur when there is a mismatch between tendon capacity and load placed on the tendon. This occurs when there is a sudden and/or substantial change in load. It’s important to question the athlete on any new or increases in training loads. Knowing a cause can assist in the management because the new loads can be modified to allow symptoms to resolve, and potentially avoided in the future.
Past history Investigating a past history is relevant, as this may determine what phase the tendon pathology is in. If an athlete has a long history of tendon pain, it can be assumed that worsening tendon pathology is present. This is referred to as tendon dysrepair or a degenerative tendon(1). Management may differ for the different phases of a tendinopathy.
Identifying other past musculoskeletal injuries is important as this may be contributing to the tendon being subjected to increased loads. For example, a past injury to a knee may have left an athlete with lower limb weakness, and out of sport for a considerable time. The athlete’s tendon capacity will be affected and when exposed to a spike in training loads and they will be at risk of injury to soft tissue structures, such as tendons. Questioning on athletes rehabilitation they completed when injured is of considerable importance.
Body chart Athletes with PT are very specific as to where their symptoms are located and often point directly to the proximal patellar tendon. This location of pain does not move(2).
24-hour behaviour
Tendinopathies are often painful after activity and especially the next day(3). This assists with the diagnosis of a PT.
Aggravating activities
Painful tendons limit the athlete’s ability to utilise energy storage within a tendon, and this compromises function(4).
Aggravating activities for patellar tendons depend on the irritability of the tendon. Activities usually include direct pressure on the tendon such as kneeling, squatting, jumping and in particular landing, changing direction and decelerating.
Reviewing training and the demands of a training session is very important. Global positioning system (GPS) data can also be very helpful whilst tracking the number of decelerations, change of directions, and high-speed metres indicate the intensity of a session and loads placed on a tendon.
Table 2: Examination procedures for PT diagnosis:
Clinical test Clinical relevance
Observation Patellar tendon swelling caused by proliferative cells, which is indicative of a reactive tendon.Investigating inflammation and increase in fat pad size, which is associated with PT. This can cause additional pain in the knee.
Observing quadriceps musculature size If a muscle has atrophy and weakness, they are less likely to withstand loads(3).
Palpation Tenderness is usually located on the inferior pole of the patellar.
Isometric muscle tests
Quadriceps isometric muscle testing – pain and/or weakness on contraction, confirming patellar tendon involvement.
SL decline squat 25degree wedge
Reported to be the best clinical assessment tool(2,3). Both pain and analysis of the kinetic chain can be assessed using this test.
If kinetic chain function affected, the athlete’s ‘spring’ has a poor function and is commonly stiff at the knee, and soft at the ankle and hip(3). This demonstrates that they cannot absorb load through their patellar tendon.
Differential diagnosis
To distinguish between patella-femoral joint (PFJ) pain and patellar tendon pain, you can tape the PFJ and see if the decline squat pain changes. If the pain is reduced, it usually means the tendon is not the pain source(2). The location of PFJ can be more diffuse and not as specific.

3 SPORTS INJURY BULLETIN No 154
resistance as tolerated by the athlete. In reactive tendons, avoiding any pain is essential to avoid any further aggravation. In tendons in the dysrepair or degenerative phases, exercising into pain of a less than 3-4 out of 10 on the visual analogue scale (VAS) is appropriate. Morning pain, single leg decline squat on a wedge and 3x vertical hops should be used to monitor pain and response to load on a daily basis every morning.
Icing after activity for 20 minutes for an analgesic effect may help reactive tissue around the patellar tendon (such as a fat pad) settle down.
Education Athletes must be educated on the
importance of resting the tendon and not pushing past 3/10 pain on VAS whilst in the reactive phase of a tendinopathy, because symptoms will worsen. The athlete should be educated about how tendons may feel okay during training but may sore the next day. Progressions in loads should be calculated, not to be aggressive and risk a flare up of symptoms – eg planning and measuring the amount of decelerations in a running program.
Avoid stretching the tendon, through doing quadriceps stretches. Compressive loads can further aggravate a tendon(1). Soft tissue massage and/or acupuncture through the quadriceps and hip flexors can be utilised alternatively to maintain knee and hip ROM.
Interdisciplinary management: management of tendon pain should be seen as an issue for an interdisciplinary team to solve. As such, it is helpful to discuss the situation with a physician and dietician as they can administer some ibuprofen, high dose of fish oil and
Table 3: Typical in-season programming
Mon Tues Wed Thurs Fri Sat Sun
Description LOAD-BEARING WEIGHTS (Optional depending on irritability of tendon)
TRAIN (Optional depending on irritability of tendon)
TRAIN / LOAD-BEARING WEIGHTS
OFF TRAIN PLAY OFF
Specifics Medium tendon loading
Lighter training session
Main training session / Key load-bearing lift – high tendon loading
Isometrics only Very light team run pre-game
Recovery Focus / Isometrics only
Tendon Load Med Med High Low Med/Low High Low
Specific activities that load patellar tendons are high-end sprinting and eccentric loading regimes. Compressive loads also load tendons, which are activities done in outer joint ranges, such as split squats.
green tea. This may help decrease tendon pain(7).
Ongoing management Managing tendinopathies in-season is
about trying to explore the correct balance of unloading the tendon without causing a detraining effect on the tendon. Daily pain monitoring as discussed provides useful information about tendon responses to load. Use of the VISA-P (Victorian Institute of Sport questionnaire) may also be useful.
ProgrammingReactive tendon response is the main cause of in-season pain, so the key intervention should be aimed at reducing loads. Load modificat ion can be programmed specifically to relieve tendon pain: Programming should periodise an
athlete’s week into high, low and medium-load days, to respect the tissue adaptation from demanding sessions where increased elastic loading is present.
High-load days include increased amounts of stretch shortening cycle (SSC), such as field sessions including training where there may be a lot of running, jumping and mechanical load.
Medium-load days include specific tendon strength program and/or a less demanding field/running session.
Low days-load include isometric holds only.
Programming an athlete’s week with PT during the in-season phase can be challenging not only because you’re managing the athletes symptoms but also because of other factors such as recovery from a game and external factors such as match schedules. A typical week is outlined above in Table 3.
Strengthening the tendon and kinetic chainDuring the competition phase of the season it is hard for symptomatic PT to become completely symptom free and to achieve strength gains. The following program in Table 4 takes time and depends on the irritability of the tendon. A less than 3/10 pain level should be the threshold and exercises should not progressed if this level of pain or higher is present.
Exit criteriaBefore being able to jog, the athlete must be pain-free walking, on stairs and be able to perform the following programme AND have a pain score of less than 4 out of 10 pain post session/next morning when performing a SL decline squat:
Decline SL squats on wedge to parallel (x 4 reps each side) with a pain score of less than 3/10;
SL calf raises – x25 reps each side; DL skips (30 secs on/off x 5reps); Alternate skips (40 secs on/20 secs off x
10reps); DL hopping/landing progressing to SL
hopping/landing sequences (including forward, lateral and multi-directional hopping);
Running progressions on an Alter-G treadmill (if available) progressing from an entry level of 70-100% weight bearing;
The introduction of running must be calculated, progressive and programmed to include high, low and medium days as discussed;
Tendon daily monitoring must be completed and be a guide for progressing the athlete through the above exit criteria, running progressions and training.
4 SPORTS INJURY BULLETIN No 154
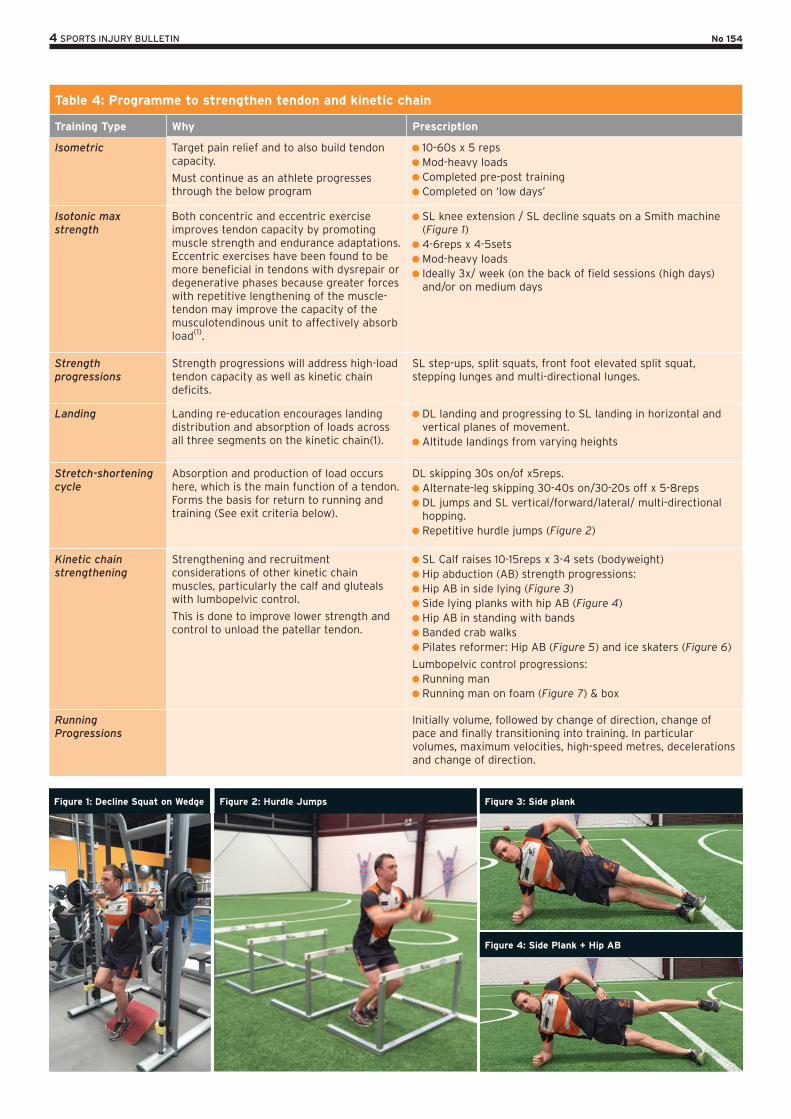
Table 4: Programme to strengthen tendon and kinetic chain
Training Type Why Prescription
Isometric Target pain relief and to also build tendon capacity.
Must continue as an athlete progresses through the below program
10-60s x 5 reps Mod-heavy loads Completed pre-post training Completed on ‘low days’
Isotonic max strength
Both concentric and eccentric exercise improves tendon capacity by promoting muscle strength and endurance adaptations. Eccentric exercises have been found to be more beneficial in tendons with dysrepair or degenerative phases because greater forces with repetitive lengthening of the muscle-tendon may improve the capacity of the musculotendinous unit to affectively absorb load(1).
SL knee extension / SL decline squats on a Smith machine (Figure 1)
4-6reps x 4-5sets Mod-heavy loads Ideally 3x/ week (on the back of field sessions (high days) and/or on medium days
Strength progressions
Strength progressions will address high-load tendon capacity as well as kinetic chain deficits.
SL step-ups, split squats, front foot elevated split squat, stepping lunges and multi-directional lunges.
Landing Landing re-education encourages landing distribution and absorption of loads across all three segments on the kinetic chain(1).
DL landing and progressing to SL landing in horizontal and vertical planes of movement.
Altitude landings from varying heights
Stretch-shortening cycle
Absorption and production of load occurs here, which is the main function of a tendon. Forms the basis for return to running and training (See exit criteria below).
DL skipping 30s on/of x5reps. Alternate-leg skipping 30-40s on/30-20s off x 5-8reps DL jumps and SL vertical/forward/lateral/ multi-directional hopping.
Repetitive hurdle jumps (Figure 2)
Kinetic chain strengthening
Strengthening and recruitment considerations of other kinetic chain muscles, particularly the calf and gluteals with lumbopelvic control.
This is done to improve lower strength and control to unload the patellar tendon.
SL Calf raises 10-15reps x 3-4 sets (bodyweight) Hip abduction (AB) strength progressions: Hip AB in side lying (Figure 3) Side lying planks with hip AB (Figure 4) Hip AB in standing with bands Banded crab walks Pilates reformer: Hip AB (Figure 5) and ice skaters (Figure 6)
Lumbopelvic control progressions: Running man Running man on foam (Figure 7) & box
Running Progressions
Initially volume, followed by change of direction, change of pace and finally transitioning into training. In particular volumes, maximum velocities, high-speed metres, decelerations and change of direction.
Figure 1: Decline Squat on Wedge Figure 2: Hurdle Jumps Figure 3: Side plank
Figure 4: Side Plank + Hip AB

5 SPORTS INJURY BULLETIN No 154
approach to managing PT will hopefully keep athletes competing for their season.
References1. British Journal of Sports Medicine 2009; 43(6),
409-16
2. Sport Health 2014; 32(1), 17-20
3. Journal of Physiotherapy 2014; ,60, 122–129
4. British Journal of Sports Medicine 2014; 48,
506–509
5. Best Practice & Research Clinical
Rheumatology 2007; 21(2), 295–316
6. British Journal of Sports Medicine 2009;
43(6), 409-16
7. Journal of Science and Medicine in Sport
2008; 11, 235—238
decelerations, and change of directions.
SummaryPTs during the competition phase of a season can be challenging to manage. It is important that a thorough history is taken to understand why the athlete has a mismatch between tendon capacity and load. Once this has been established, relative rest (not complete rest) and programming of high, low, medium training days must be done to unload the tendon. Acute management aiming to decrease pain is of utmost importance. A focus on isometric exercises for pain relief will help achieve this. If symptoms are respected and monitored daily, this
Outcome measuresThe best outcome measure is the athlete’s pain provocation (VAS) during competition – more specifically VAS whilst performing specific activities such as decline squatting, hopping, jumping, running, changing direction and decelerating. Outcome measures specific to strength gains are increases in thigh circumference measured by DEXA scan or tape measure and by an increase in weight lifted, reps and sets. Quantifying lower limb power is achieved by measuring a single-leg hop for distance, vertical jump (single/double leg) and a cross-over hop test. Running sessions should be also be measured, quantifying volume, high speed metres, number of
Disc herniation
Lumbar spine micro-discectomy – Part 2In the first part of this 2-part series, Chris Mallac looked at the likely signs and symptoms of disc herniation, as well as the selection criteria for micro-discectomy surgery in athletes. In this article, he discusses the lengthy rehab period following a micro-discectomy procedure, and provides a host of strength based exercises
Surgeries to alleviate the symptoms of disc herniation, with or without nerve root compromise, include conventional open d i s c e c t o m y , m i c r o - d i s c e c t o m y , percu taneous l aser d i scec tomy , percutaneous discectomy and micro-endoscopic discectomy (MED).
Other surgical terms have been used in the literature such as herniotomy which is synonymous with fragmentectomy or sequestrectomy. The term ‘herniotomy’ is defined as removal of the herniated disc fragment only, and the ‘conventional
discectomy’ as removal of the herniated disc and its degenerative nucleus from the intervertebral disc space.
When surgery is required, minimising tissue disruption and strict adherence to an aggressive rehabilitation regimen may expedite an athlete’s return to play(1), which explains why micro discectomy is a favoured surgical procedure for athletes.
Micro discectomy procedures involves removing a small part of the vertebral bone over a nerve root, or removing the f r a g m e n t e d d i s c m a t e r i a l f r o m
underneath the compressed nerve root. The procedure is performed through a small 1 to 2 inch incision in the midline of the spine. The erector spinae muscles are retracted off the bony lamina of the spine.
The surgeon is then able to enter the spine by removing the ligamentum flavum that covers the nerve roots. The nerve roots can be visualised with operating glasses or with an operating microscope. The surgeon will then move the nerve root to the side and to then remove the disc material from under the nerve root.
Figure 5: Reformer Figure 6: Reformer – Ice skaters Figures 7: Running man on foam
Figure 5: Reformer – Hip AB

6 SPORTS INJURY BULLETIN No 154
cross-sectional area is the smallest (therefore has a greater potential for nerve compromise) at the most upper lumbar segment and the cross-sectional area increases further down towards the lower lumbar spine(14).
The location of the disc herniation (foraminal, posterolateral or central) may also contribute to these differences. In this study, upper lumbar herniations were more likely to occur in the far lateral and foraminal positions than were those at the lower two intervertebral levels(13).
Post-surgical rehab Following micro-discectomy surgery, the small incision and limited soft tissue trauma allows the patient to be ambulatory reasonably quickly, and they are usually encouraged to start rehabilitation at some point in the 2-6 weeks following surgery.
In a review on the efficacy of active rehabilitation in patients following lumbar spine discectomy, it can be concluded that individuals can safely engage in high or low-intensity supervised or home-based exercises initiated at 4 to 6 weeks following first-time lumbar discectomy(15).
Herbert et al (2010) found that with effective post-surgical rehabilitation programs, there was a primary emphasis on lumbar stabilisation exercises(16). Secondly, positive trials tended to initiate rehabilitation earlier in the postoperative period when compared to negative trials (approximately 4 versus 7 weeks). In their case study, they successfully initiated a lumbar stabilisation program 1 week post-surgery in a 29 year old lady, and this focused heavily on lumbar multifidus (LM) and transverse abdominus (TrA) activation exercises that improved function as measured on an Oswestry scale (see below). This approach also improved pain response and TrA and LM function, measured as muscle function under ultrasound and muscle morphology measured under MRI(16).
Outcome measuresThe most universally used outcome measure following back injury and/or disc surgery is the Oswestry Disability Questionnaire(17). The Oswestry Disability Questionnaire provides a quantitative assessment of low-back pain related disability. Individuals rate the difficulty of 10 functional activities (eg walking, standing, lifting) on a scale from 0 to 5, with higher scores indicating greater disability. This questionnaire is reported to have good l e v e l s o f t e s t - r e t e s t r e l i a b i l i t y ,
longer career and higher return to play rate than those treated non-operatively(8). 5. Schroeder et al (2013) reported 85% RTP rates in 87 hockey players, with no significant difference in rates or outcomes between the surgical and nonsurgical cohorts(9). 6. A study by Watkins et al (2003) dealing with professional and Olympic athletes showed the satisfactory outcomes of micro-discectomy in terms of return to play, because elite athletes in general were highly motivated to return to play(10). Also, athletes who had single-level micro-discectomy were more likely to return to their original levels of sports activities than were those who had two-level micro-discectomies.7. A study by Anakwenze et al (2010) investigating open discectomy in National Basketball Association players demonstrated that 75% of patients returned to play again compared with 88% in control subjects who did not undergo the surgery(11). Furthermore, for those players who returned, overall athletic performance was slightly improved or no worse than control subjects.8. A recent review found that conservative treatment, or micro-discectomy, in athletes with lumbar disc herniation seemed to be satisfactory in terms of returning the injured athletes to their original levels of sports activities(12).
These studies conclude that although a diagnosis of lumbar disc herniation has career-ending potential, most players are able to return to play and generate excellent performance-based outcomes, even if surgery is required.
What is also apparent from research studies is that the level of the disc herniation can also determine prognosis following surgery. Athletes shower a greater difference in improvement between operative and non-operative treatment for upper level herniations (L2-L3 and L3-L4) than for herniations at the L4-L5 and L5-S1 levels. Patients with the upper leve l hernia t ions had less improvement with non-operat ive treatment and slightly better operative outcomes than those with lower level herniations(13).
There are several possible explanations for these findings. A number of studies have shown that reduced spinal canal cross-sectional area is associated with an increased probability of symptomatic disc herniation, and greater intensity of herniat ion symptoms. The spinal
It is also sometimes necessary to remove a small portion of the associated facet joint to allow access to the nerve root, and to also relieve pressure on the nerve root stemming from the facet joint. This procedure is minimally invasive as the joints, ligaments and muscles are left intact, and the procedure does not interfere with the mechanical structure of the spine.
Surgical outcomesOverall , athletes with lumbar disc herniation have a favourable prognosis with conservative treatment; more than 90% of athletes with a disc herniation improve with non-operative treatment. Many show a response to conservative therapy with improved pain and sciatica within 6 weeks of the initial onset(2). This suggests that the need to operate immediately may be considered hasty.
However, in the event of fai led conservative treatment, or with the pressure of an important upcoming competition, surgery may be required in some cases. Even though it involves surgical treatment, micro-discectomy is reported to have a high success rate – more than 90% in some studies(3,4). Patients generally have very little pain, are able to return to preinjury activity levels, and are subjectively satisfied with their results.
The success rate of micro-discectomy is comparable between athletes and non-athletes. The following studies are summarised to highlight the success rate of micro-discectomy procedures:1. In a study on 342 professional athletes diagnosed with lumbar disc herniation in sports such as hockey, football, baseball and basketball, it was found that successful return to play occurred 82% of the time, and 81% of surgically treated athletes returned for an additional average of 3.3 years(5).2. Patients have a 75% chance of recovery from a limb paresis that may be associated with a disc herniation after surgical treatment. If the preoperative paresis was mild then they can expect an 84% chance of full recovery. Patients with more severe paresis have less chance of recovery (55%)(6).3. Wang et al (1999) in a study on 14 athletes requiring discectomy procedures found that in single level disc procedures, the return to sport was 90%. However when the procedure involved 2 levels enjoyed much less favourable results(7). 4. In a study of 137 National Football League players with lumbar disc herniation, surgical treatment of lumbar disc herniation led to a significantly
7 SPORTS INJURY BULLETIN No 154
points. The athlete can initiate very gentle nerve mobilisation techniques and he/she is taught how to engage the TrA and LM muscles (see Figures 2a and 2b). If the physiotherapist has access to a muscle stimulator (Compex), this can be used in atrophy mode on the lumbar spine multifidus and erector spinae. The key criteria to exit this early stage are pain-free walking and an Oswestry Disability Score of 41-60%.
Early loading and foundationThe primary feature of this stage is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive range of motion program to improve lumbar spine flexion, extension and rotation. In this stage the physiotherapist will guide the athlete through safe and gentle stretches for the hip quadrant muscles such as the hip flexors, gluteals, hamstrings and adductors. The athlete also continues gentle neuro-mobilisation exercises to progress the mobility of the sciatic nerve – a concern in this condition as neural tethering is a possibility due to the scar tissue formation caused by the surgical procedure.
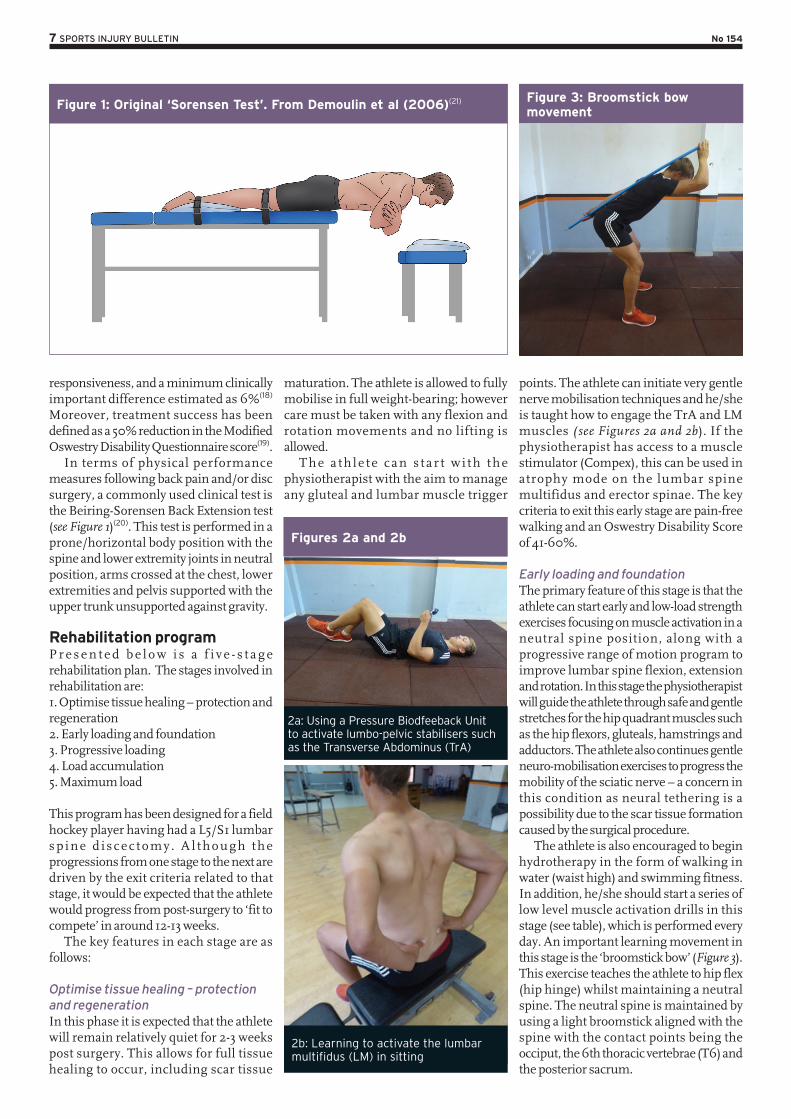
The athlete is also encouraged to begin hydrotherapy in the form of walking in water (waist high) and swimming fitness. In addition, he/she should start a series of low level muscle activation drills in this stage (see table), which is performed every day. An important learning movement in this stage is the ‘broomstick bow’ (Figure 3). This exercise teaches the athlete to hip flex (hip hinge) whilst maintaining a neutral spine. The neutral spine is maintained by using a light broomstick aligned with the spine with the contact points being the occiput, the 6th thoracic vertebrae (T6) and the posterior sacrum.
maturation. The athlete is allowed to fully mobilise in full weight-bearing; however care must be taken with any flexion and rotation movements and no lifting is allowed.
The a th le te can s t a r t w i th the physiotherapist with the aim to manage any gluteal and lumbar muscle trigger
responsiveness, and a minimum clinically important difference estimated as 6%(18) Moreover, treatment success has been defined as a 50% reduction in the Modified Oswestry Disability Questionnaire score(19).
In terms of physical performance measures following back pain and/or disc surgery, a commonly used clinical test is the Beiring-Sorensen Back Extension test (see Figure 1)(20). This test is performed in a prone/horizontal body position with the spine and lower extremity joints in neutral position, arms crossed at the chest, lower extremities and pelvis supported with the upper trunk unsupported against gravity.
Rehabilitation program P r e s e n t e d b e l o w i s a f i v e - s t a g e rehabilitation plan. The stages involved in rehabilitation are:1. Optimise tissue healing – protection and regeneration2. Early loading and foundation3. Progressive loading4. Load accumulation5. Maximum load
This program has been designed for a field hockey player having had a L5/S1 lumbar sp ine d i scec tomy . A l though the progressions from one stage to the next are driven by the exit criteria related to that stage, it would be expected that the athlete would progress from post-surgery to ‘fit to compete’ in around 12-13 weeks.
The key features in each stage are as follows:
Optimise tissue healing – protection and regenerationIn this phase it is expected that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue healing to occur, including scar tissue
Figure 1: Original ‘Sorensen Test’. From Demoulin et al (2006)(21)
Figures 2a and 2b
Figure 3: Broomstick bow movement
2a: Using a Pressure Biodfeeback Unit to activate lumbo-pelvic stabilisers such as the Transverse Abdominus (TrA)
2b: Learning to activate the lumbar multifidus (LM) in sitting
8 SPORTS INJURY BULLETIN No 154
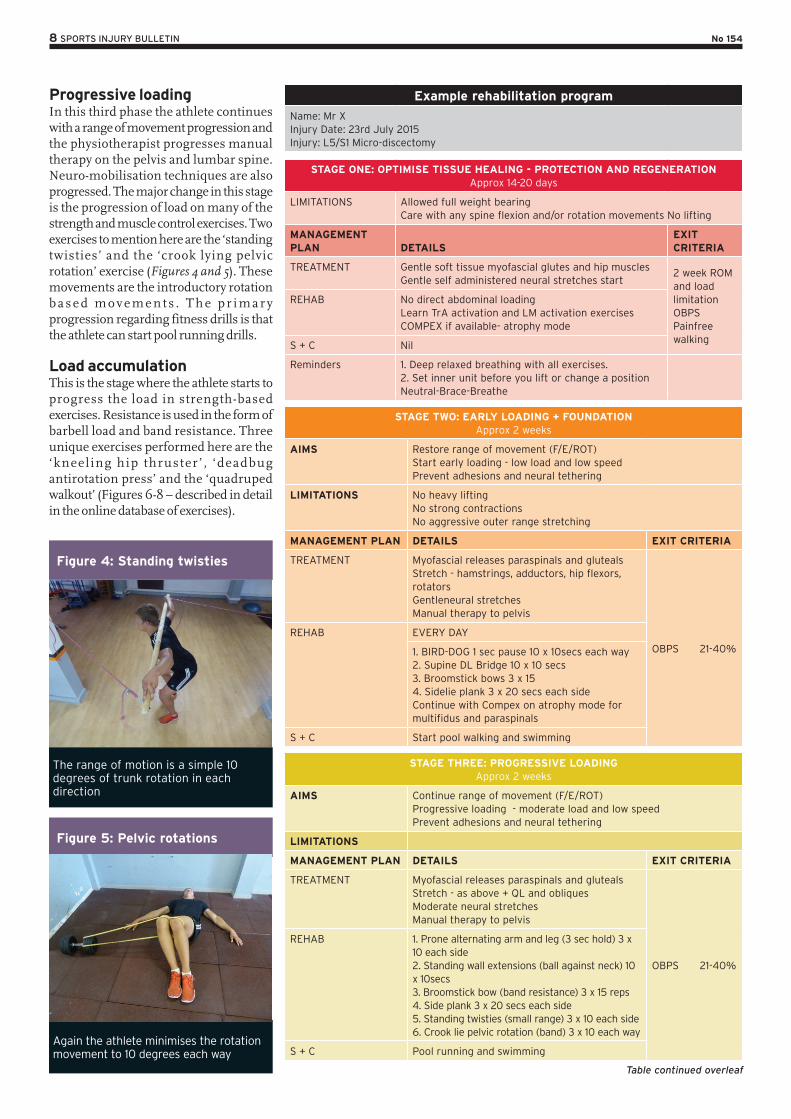
Progressive loadingIn this third phase the athlete continues with a range of movement progression and the physiotherapist progresses manual therapy on the pelvis and lumbar spine. Neuro-mobilisation techniques are also progressed. The major change in this stage is the progression of load on many of the strength and muscle control exercises. Two exercises to mention here are the ‘standing twisties’ and the ‘crook lying pelvic rotation’ exercise (Figures 4 and 5). These movements are the introductory rotation b a s e d m o v e m e n t s . T h e p r i m a r y progression regarding fitness drills is that the athlete can start pool running drills.
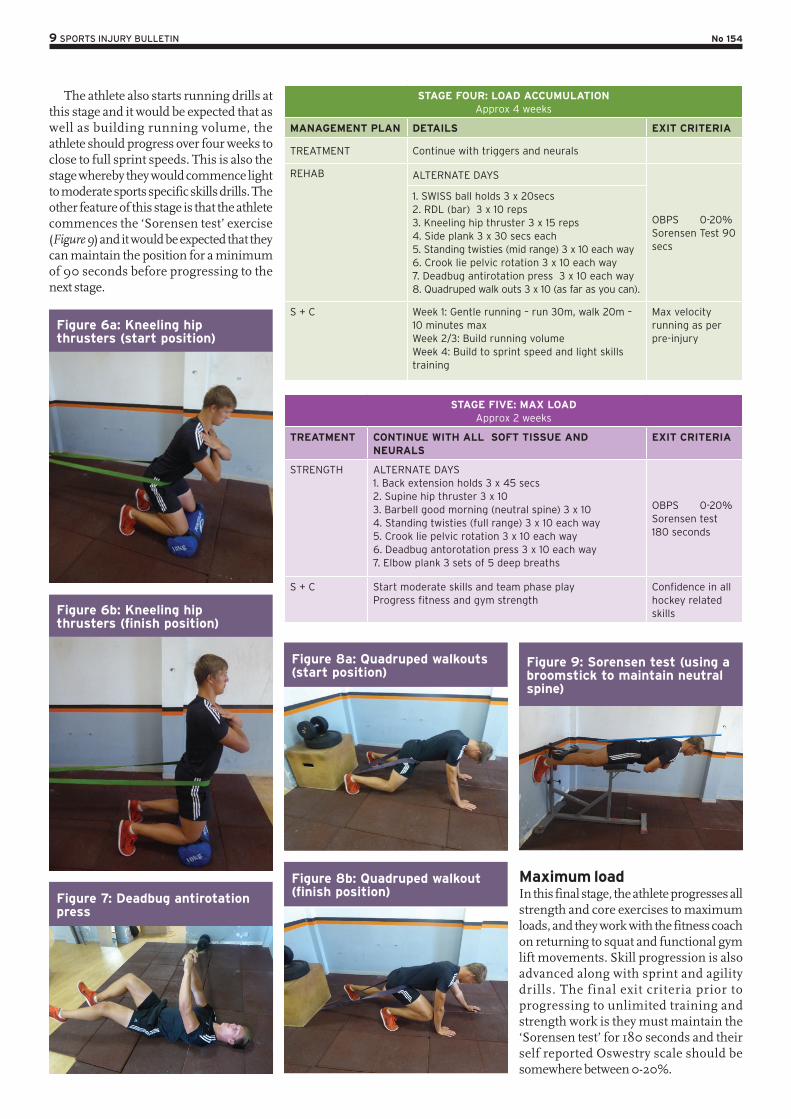
Load accumulationThis is the stage where the athlete starts to progress the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three unique exercises performed here are the ‘kneel ing hip thruster ’ , ‘deadbug antirotation press’ and the ‘quadruped walkout’ (Figures 6-8 – described in detail in the online database of exercises).
Example rehabilitation program
Name: Mr XInjury Date: 23rd July 2015Injury: L5/S1 Micro-discectomy
STAGE ONE: OPTIMISE TISSUE HEALING - PROTECTION AND REGENERATION Approx 14-20 days
LIMITATIONS Allowed full weight bearingCare with any spine flexion and/or rotation movements No lifting
MANAGEMENT PLAN DETAILS
EXIT CRITERIA
TREATMENT Gentle soft tissue myofascial glutes and hip musclesGentle self administered neural stretches start
2 week ROM and load limitationOBPSPainfree walking
REHAB No direct abdominal loadingLearn TrA activation and LM activation exercisesCOMPEX if available- atrophy mode
S + C Nil
Reminders 1. Deep relaxed breathing with all exercises.2. Set inner unit before you lift or change a positionNeutral-Brace-Breathe
STAGE TWO: EARLY LOADING + FOUNDATION Approx 2 weeks
AIMS Restore range of movement (F/E/ROT) Start early loading - low load and low speed Prevent adhesions and neural tethering
LIMITATIONS No heavy lifting No strong contractions No aggressive outer range stretching
MANAGEMENT PLAN DETAILS EXIT CRITERIA
TREATMENT Myofascial releases paraspinals and glutealsStretch - hamstrings, adductors, hip flexors, rotatorsGentleneural stretchesManual therapy to pelvis
OBPS 21-40%
REHAB EVERY DAY
1. BIRD-DOG 1 sec pause 10 x 10secs each way 2. Supine DL Bridge 10 x 10 secs3. Broomstick bows 3 x 154. Sidelie plank 3 x 20 secs each sideContinue with Compex on atrophy mode for multifidus and paraspinals
S + C Start pool walking and swimming
STAGE THREE: PROGRESSIVE LOADING Approx 2 weeks
AIMS Continue range of movement (F/E/ROT) Progressive loading - moderate load and low speedPrevent adhesions and neural tethering
LIMITATIONS
MANAGEMENT PLAN DETAILS EXIT CRITERIA
TREATMENT Myofascial releases paraspinals and glutealsStretch - as above + QL and obliquesModerate neural stretchesManual therapy to pelvis
OBPS 21-40%
REHAB 1. Prone alternating arm and leg (3 sec hold) 3 x 10 each side2. Standing wall extensions (ball against neck) 10 x 10secs3. Broomstick bow (band resistance) 3 x 15 reps4. Side plank 3 x 20 secs each side5. Standing twisties (small range) 3 x 10 each side6. Crook lie pelvic rotation (band) 3 x 10 each way
S + C Pool running and swimming
Figure 4: Standing twisties
Figure 5: Pelvic rotations
The range of motion is a simple 10 degrees of trunk rotation in each direction
Again the athlete minimises the rotation movement to 10 degrees each way
Table continued overleaf
9 SPORTS INJURY BULLETIN No 154
Maximum loadIn this final stage, the athlete progresses all strength and core exercises to maximum loads, and they work with the fitness coach on returning to squat and functional gym lift movements. Skill progression is also advanced along with sprint and agility drills. The final exit criteria prior to progressing to unlimited training and strength work is they must maintain the ‘Sorensen test’ for 180 seconds and their self reported Oswestry scale should be somewhere between 0-20%.
The athlete also starts running drills at this stage and it would be expected that as well as building running volume, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would commence light to moderate sports specific skills drills. The other feature of this stage is that the athlete commences the ‘Sorensen test’ exercise (Figure 9) and it would be expected that they can maintain the position for a minimum of 90 seconds before progressing to the next stage.
STAGE FOUR: LOAD ACCUMULATION Approx 4 weeks
MANAGEMENT PLAN DETAILS EXIT CRITERIA
TREATMENT Continue with triggers and neurals
REHAB ALTERNATE DAYS
OBPS 0-20%Sorensen Test 90 secs
1. SWISS ball holds 3 x 20secs 2. RDL (bar) 3 x 10 reps 3. Kneeling hip thruster 3 x 15 reps 4. Side plank 3 x 30 secs each 5. Standing twisties (mid range) 3 x 10 each way6. Crook lie pelvic rotation 3 x 10 each way7. Deadbug antirotation press 3 x 10 each way8. Quadruped walk outs 3 x 10 (as far as you can).
S + C Week 1: Gentle running – run 30m, walk 20m – 10 minutes maxWeek 2/3: Build running volumeWeek 4: Build to sprint speed and light skills training
Max velocity running as per pre-injury
STAGE FIVE: MAX LOAD Approx 2 weeks
TREATMENT CONTINUE WITH ALL SOFT TISSUE AND NEURALS
EXIT CRITERIA
STRENGTH ALTERNATE DAYS 1. Back extension holds 3 x 45 secs2. Supine hip thruster 3 x 103. Barbell good morning (neutral spine) 3 x 104. Standing twisties (full range) 3 x 10 each way5. Crook lie pelvic rotation 3 x 10 each way6. Deadbug antorotation press 3 x 10 each way7. Elbow plank 3 sets of 5 deep breaths
OBPS 0-20%Sorensen test 180 seconds
S + C Start moderate skills and team phase playProgress fitness and gym strength
Confidence in all hockey related skills
Figure 6a: Kneeling hip thrusters (start position)
Figure 6b: Kneeling hip thrusters (finish position)
Figure 7: Deadbug antirotation press
Figure 9: Sorensen test (using a broomstick to maintain neutral spine)
Figure 8b: Quadruped walkout (finish position)
Figure 8a: Quadruped walkouts (start position)
10 SPORTS INJURY BULLETIN No 154
15. Physical Therapy. 2013. 93: 591-596
16. Journal of orthopaedic & sports physical
therapy. 2010. 40(7). 402-412
17. Physiotherapy. 1980;66:271-273
18. Spine (Phila Pa 1976). 2009;34:2803-2809
19. Phys Ther. 2001;81:776-788
20. Spine 1984, 9:106-119
21. Joint Bone Spine 73 (2006) 43–50
8. Spine (Phila Pa 1976). 2010;35(12):1247–51
9. Am J Sports Med. 2013;41(11):2604–8
10. Spine J. 2003;3:100–105
11. Spine. Apr 1 2010;35(7):825-8
12. Open Access Journal of Sports Medicine.
2011:2 25–31
13. J Bone Joint Surg Am. 2008;90:1811-9
14. Eur Spine J. 2002;11:575-81
References1. Neurosurgical Focus. 2006;21:E4
2. Phys Sportsmed. 2005;33(4):21–7
3. Spine. 1996;21:1777-86
4. Neurosurgery 1992;30:861-7
5. Spine J. 2011;11(3):180–6
6. European Spine Journal. 2012. 21: 655-659
7. SPINE 1999;24:570-573
Shoulder pain
Serratus anterior and overhead athletes: don’t underestimate its importance!Serratus anterior is an important muscle for the overhead athlete. Dysfunction in this muscle can lead to shoulder injuries such as impingement, rotator cuff breakdown and performance decrements during overhead tasks. Chris Mallac looks at its anatomy and biomechanics, and highlights some clinically relevant exercises designed to retrain serratus anterior function
Shoulder pain is a common complaint in overhead athletes involved in sports such as swimming, tennis and the throwing sports. Overhead upper extremity movements place incredibly high demands on the shoulder complex, requiring high muscular activation around both the scapula-thoracic joint and glenohumeral joint. Researchers have reported that abnormal biomechanics of the shoulder girdle and repeated overhead movements can lead to injuries in overhead throwing athletes(1).
In particular, muscular imbalances around the shoulder complex in the form of altered activation patterns and inherent myofascial restrictions, may lead to diminished scapular control and dyskinesis resulting in glenohumeral joint in jur ies , such as ins tabi l i t y and impingement(2).
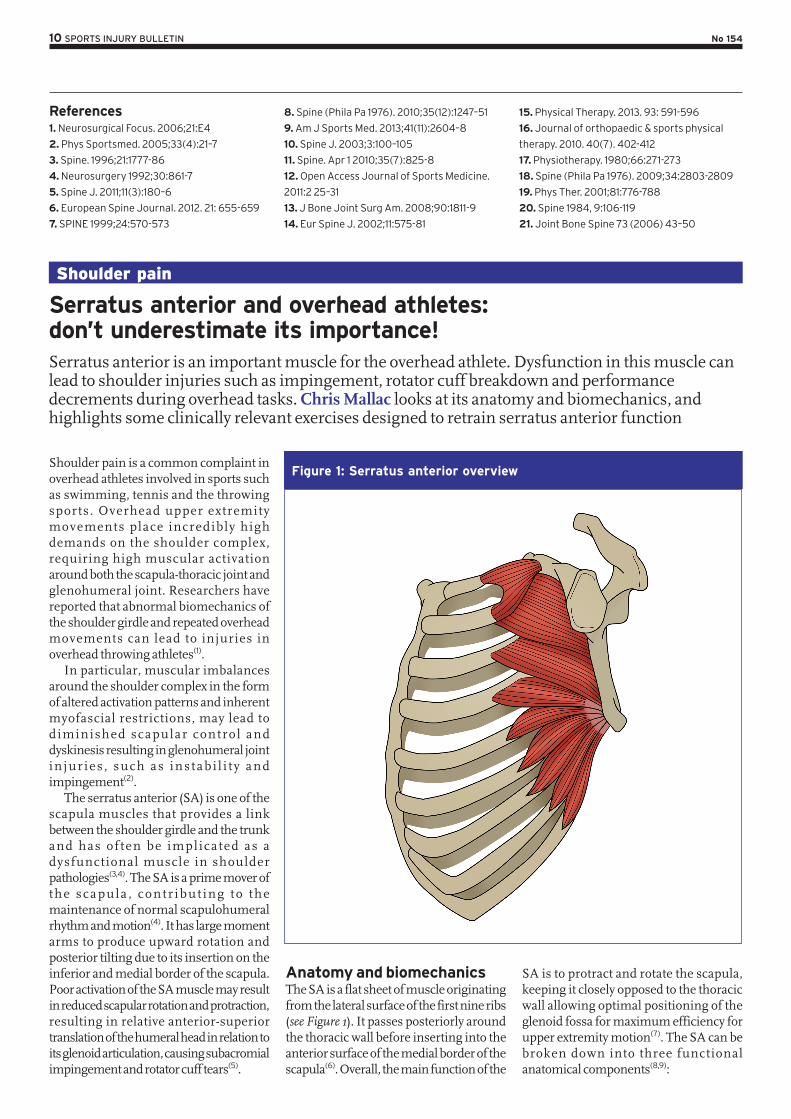
The serratus anterior (SA) is one of the scapula muscles that provides a link between the shoulder girdle and the trunk and has of ten be implicated as a dysfunctional muscle in shoulder pathologies(3,4). The SA is a prime mover of the scapula , contr ibut ing to the maintenance of normal scapulohumeral rhythm and motion(4). It has large moment arms to produce upward rotation and posterior tilting due to its insertion on the inferior and medial border of the scapula. Poor activation of the SA muscle may result in reduced scapular rotation and protraction, resulting in relative anterior-superior translation of the humeral head in relation to its glenoid articulation, causing subacromial impingement and rotator cuff tears(5).
Anatomy and biomechanicsThe SA is a flat sheet of muscle originating from the lateral surface of the first nine ribs (see Figure 1). It passes posteriorly around the thoracic wall before inserting into the anterior surface of the medial border of the scapula(6). Overall, the main function of the
SA is to protract and rotate the scapula, keeping it closely opposed to the thoracic wall allowing optimal positioning of the glenoid fossa for maximum efficiency for upper extremity motion(7). The SA can be broken down into three functional anatomical components(8,9):
Figure 1: Serratus anterior overview
11 SPORTS INJURY BULLETIN No 154
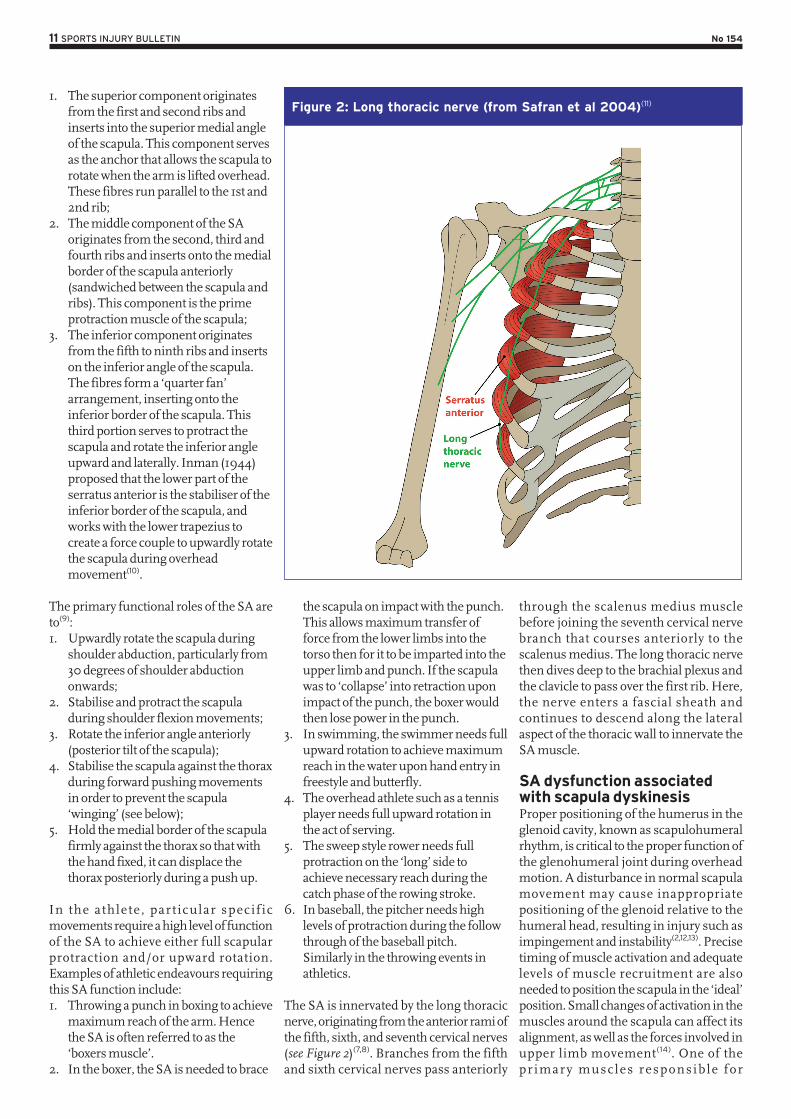
through the scalenus medius muscle before joining the seventh cervical nerve branch that courses anteriorly to the scalenus medius. The long thoracic nerve then dives deep to the brachial plexus and the clavicle to pass over the first rib. Here, the nerve enters a fascial sheath and continues to descend along the lateral aspect of the thoracic wall to innervate the SA muscle.
SA dysfunction associated with scapula dyskinesisProper positioning of the humerus in the glenoid cavity, known as scapulohumeral rhythm, is critical to the proper function of the glenohumeral joint during overhead motion. A disturbance in normal scapula movement may cause inappropriate positioning of the glenoid relative to the humeral head, resulting in injury such as impingement and instability(2,12,13). Precise timing of muscle activation and adequate levels of muscle recruitment are also needed to position the scapula in the ‘ideal’ position. Small changes of activation in the muscles around the scapula can affect its alignment, as well as the forces involved in upper limb movement(14). One of the pr imary muscles responsib le for
the scapula on impact with the punch. This allows maximum transfer of force from the lower limbs into the torso then for it to be imparted into the upper limb and punch. If the scapula was to ‘collapse’ into retraction upon impact of the punch, the boxer would then lose power in the punch.
3. In swimming, the swimmer needs full upward rotation to achieve maximum reach in the water upon hand entry in freestyle and butterfly.
4. The overhead athlete such as a tennis player needs full upward rotation in the act of serving.
5. The sweep style rower needs full protraction on the ‘long’ side to achieve necessary reach during the catch phase of the rowing stroke.
6. In baseball, the pitcher needs high levels of protraction during the follow through of the baseball pitch. Similarly in the throwing events in athletics.
The SA is innervated by the long thoracic nerve, originating from the anterior rami of the fifth, sixth, and seventh cervical nerves (see Figure 2)(7,8). Branches from the fifth and sixth cervical nerves pass anteriorly
1. The superior component originates from the first and second ribs and inserts into the superior medial angle of the scapula. This component serves as the anchor that allows the scapula to rotate when the arm is lifted overhead. These fibres run parallel to the 1st and 2nd rib;
2. The middle component of the SA originates from the second, third and fourth ribs and inserts onto the medial border of the scapula anteriorly (sandwiched between the scapula and ribs). This component is the prime protraction muscle of the scapula;
3. The inferior component originates from the fifth to ninth ribs and inserts on the inferior angle of the scapula. The fibres form a ‘quarter fan’ arrangement, inserting onto the inferior border of the scapula. This third portion serves to protract the scapula and rotate the inferior angle upward and laterally. Inman (1944) proposed that the lower part of the serratus anterior is the stabiliser of the inferior border of the scapula, and works with the lower trapezius to create a force couple to upwardly rotate the scapula during overhead movement(10).
The primary functional roles of the SA are to(9):1. Upwardly rotate the scapula during
shoulder abduction, particularly from 30 degrees of shoulder abduction onwards;
2. Stabilise and protract the scapula during shoulder flexion movements;
3. Rotate the inferior angle anteriorly (posterior tilt of the scapula);
4. Stabilise the scapula against the thorax during forward pushing movements in order to prevent the scapula ‘winging’ (see below);
5. Hold the medial border of the scapula firmly against the thorax so that with the hand fixed, it can displace the thorax posteriorly during a push up.
In the athlete, part icular specif ic movements require a high level of function of the SA to achieve either full scapular protraction and/or upward rotation. Examples of athletic endeavours requiring this SA function include:1. Throwing a punch in boxing to achieve
maximum reach of the arm. Hence the SA is often referred to as the ‘boxers muscle’.
2. In the boxer, the SA is needed to brace
Figure 2: Long thoracic nerve (from Safran et al 2004)(11)

12 SPORTS INJURY BULLETIN No 154
The gross examples of scapular winging can also be due to a pathological lesion to the long thoracic nerve that innervates the SA muscle. For the purposes of this discussion, direct nerve insults to the long thoracic nerve will not be discussed as often these injuries will seriously curtail athletic participation in an athlete. The reader is directed to references 19-23 for a more detailed discussion on these pathological nerve lesions.
SA importance The importance of a conditioned serratus anterior muscle has been highlighted in E M G s t u d i e s o f s p o r t s s u c h a s swimming(24), throwing(25), and tennis(26). A fatigued serratus anterior muscle will reduce scapular rotation and protraction and allow the humeral head to translate anteriorly and superiorly, possibly leading to secondary impingement and rotator cuff tears(27). More direct studies on the role that SA plays in shoulder pathologies has been studied by other researchers. The pertinent points of some of these studies can be summarised below;
1. When the trapezius and SA EMG is investigated in people suffering from shoulder pathology is compared with those without pathology, it has been found that upper trapezius can show an increased activity during arm elevation and lowering, and that SA shows decreased activation at some elevation angles (usually 70-100 degrees)(28).
2. When the muscle activation patterns of swimmers with shoulder pain is compared to those without, it has been found that middle and lower SA show decreased activity in all phases of swimming motion. This can be a possible cause of the shoulder pain or a consequence of a painful shoulder whereby the swimmer uses compensatory muscle activation patterns(29).
3. Similarly, other researchers have found a ‘latency’ or activation delay in the SA in the shoulders of painful swimmers as they raise their arms in the scapular plane(30).
4. Ludewig and Cook (2000) hypothesised that patients with decreased SA activation are associated with more shoulder pain and/or instability, and that an increase in lower trapezius activity was an attempt to compensate for decreased serratus anterior activation(2).
maintaining normal rhythm and shoulder motion is the SA(15).
Clinically, it has been shown that if a therapist actively repositions a patient’s scapula into an ‘ideal’ posture by reducing the anterior tilt, then it is noticed that impingement pain is reduced, and strength increases in the shoulder during overhead activities(16). The SA is a muscle that will actively work to position the scapula into posterior tilt during overhead activities.
Lack of strength or endurance in the SA allows the scapula to rest in a downwardly rotated and anterior tilted position, causing the inferior border to become more p r o m i n e n t . F u r t h e r m o r e , g r o s s pathological inhibition of the SA or an imbalance between the SA and the other protracting muscle, the pectoralis minor, may result in a ‘winging scapula’. Scapular winging may precipitate or contribute to persistent symptoms in patients with orthopaedic shoulder abnormalities(17,18).
Th i s s capu la r w ing ing i s bes t appreciated on watching the scapula posture during a push up exercise. Often if the winging is due to a muscle imbalance and the primary scapula stabiliser is the pectoralis minor, this will usually correct if the patient is asked to ‘plus’ and protract the scapula. If the wing disappears then the cause is most likely muscle imbalance, if it remains then it may be a pathological inhibition of the SA. Examples of this are shown below in figures 3-6.
Figure 3: Scapular winging on push up bilaterally
Figure 4: Winging corrects on execution of a ‘plus’
Figure 5: Scapular winging on push up bilaterally (right greater than left)
Figure 6: Left scapula corrects with ‘plus’ however note the right is still winged

13 SPORTS INJURY BULLETIN No 154
effective strategy for the selective mobilisation of this component of the SA.
5. Seo et al (2013) also found that the performance of a push up and knee push up on an unstable surface (Swiss ball) increased activation of the SA(37).
Below are some examples of clinically used SA activation exercises that anecdotally seem to recruit SA to high levels of function:
and lower parts of the SA, while performing variations of the push-up exercise (push up and push up plus(36). The results indicated that the different parts of SA have distinct functions in the stabilisation process and therefore are recruited differently. The authors concluded that the main role of the lower SA is the fixation of the scapula onto the thoracic wall and therefore recommend performing the push-up plus on an unstable surface as a more
5. Lin et al (2005) studied subjects with various types of shoulder dysfunction and found decreased serratus anterior activity and increased upper trapezius activity, without a change in lower trapezius activity in injured shoulders when compared to normal subjects(31).
Scapula position has also been associated with the ability of the rotator cuff to function. Excessive anterior tilt of the scapula, internal rotation, or excessive elevation of the acromion are factors that decrease the rotator cuff activation and cause an inadequate distribution of tension along the tendons. Such situations impair the optimum length-to-tension ratio of these muscles, leading to a loss of stabilisation and increasing the chance of muscular disruption or degeneration(32). It has been shown that the rotator cuff function improves in the presence of functioning scapula muscles such as the SA and lower trapezius.
Exercises for SAA significant amount of research has been c o n d u c t e d o n f i n d i n g t h e b e s t rehabilitation exercises for the SA. The major i ty o f these s tudies look a t movements such as push ups, push up-plus exercises, cable and dumbbell ‘punch’ type movements. These exercises essentially emulate the function of the SA in its protraction role. Some of the findings of the more noted studies are;
1. Decker et al (1999) looked at the EMG activity and applied resistance associated with eight scapulohumeral exercises performed below shoulder height that target the SA muscle and how to design a continuum of SA muscle exercises for progressive rehabilitation or training(33). The best exercises according to these researchers are the push ups, dynamic hug, scaption and SA punch exercises.
2. Barreto et al (2012) found high levels of activation of the SA in scaption exercises and adequate levels of activation of SA in MMP (modified military press)(34).
3. Kim et al (2014) studied the interesting effect of vibration on SA activation and found that the push-up plus exercise performed using the Redcord system with mechanical vibration at 50 Hz increases SA muscle activity(35).
4. Park and Yoo (2011) evaluated the effect of unstable surface on the upper
1. The wall slider (figures 7a and 7b)a. Using a foam roller or pool noodle on
the wall, place the wrists against the
roller so that the forearm commences in
a neutral pronation/supination position.
The hands are approximately six inches
apart and the elbows are about twelve
inches apart.
b. Protract the scapula so that the space
between the shoulder blades is filled in
with an increase in thoracic kyphosis.
c. Slowly flex the shoulder so that the
roller moves up the wall. This creates
scapula upward rotation.
d. As the shoulder is flexing, slowly
supinate the forearms. This then creates
obligatory shoulder external rotation.
e. Reach as high as possible into
shoulder flexion.
f. Although the feet do not move, the
trunk will gently lean into the wall as the
arms are raised in shoulder flexion.
g. The finish point is when the little
fingers touch and the forearm is in
maximum supination.
h. This should be felt as a strong serratus
anterior contraction on the ribcage wall.
i. Slowly descend and return to the
starting point with the forearms in
neutral pronation/supination.
j. Perform three sets of ten repetitions.
2. Swiss ball rotations (Figure 8)a. Hold a Swiss ball (55cm) between the
arms with the ball gently resting on the
chest and the forearms in neutral
pronation/supination.
b. Slowly rotate the trunk to the left. As
this is done, the right arm is made longer
by actively protracting the scapula and
the left arm is made shorter by actively
retracting and depressing the scapula.
The arms ‘glide’ around the Swiss ball.
c. As the arm is made longer
Figure 7a: Wall slider (start position)
Figure 7b: Wall slider (finish position
(notice the forearm is supinated and shoulder externally rotated)

14 SPORTS INJURY BULLETIN No 154
(protraction) slowly rotate the palm
upwards to encourage supination of the
forearm and external rotation of the
shoulder.
d. Return to the start position and
commence again.
e. This can be progressed by holding
Theratubing in the hands, which wraps
around the upper trunk. This provides
resistance to the scapula protraction.
3. TrX Serratus rollouts (Figures 9a and 9b)a. Place the forearms through the loops
of a Trx or other suspension device.
b. The straps are placed at wrist level for
a high-load exercise or just below the
elbows for a shorter lever low-load
exercise.
c. The commencing hand position is
similar to the wall slider above. The hands
are approximately six inches apart and
the elbows are about twelve inches apart.
d. Slowly flex the shoulder so that the
arms elevate above the head and at the
same time start to slowly externally rotate
the shoulder by supinating the forearms.
e. The finish point is when maximum
flexion/elevation is achieved and the little
fingers touch.
f. Although the feet do not move, the
trunk will start to lean forward as the
arms are raised.
g. This finish position involves maximum
scapula upward rotation.
h. Return to the start and perform three
sets of fifteen repetitions.
i. This is a progression on the wall slider as
the suspension device is inherently
unstable and requires more muscular effort
throughout the kinetic chain to control.
4. TrX push up plus (Figures 10a and 10b)a. On a TrX, position the handles two to
three feet off the ground. The lower the
handles, the more difficult the exercise.
b. Holding the handles in a push up
position, slowly perform a push up and
slowly ‘screw’ the hands into supination
and shoulder external rotation.
c. At the top of the movement, protract
the scapula and fill in the space between
the shoulder blades with a slight thoracic
kyphosis.
d. This is a progression from a push up
plus as the Trx is unstable and requires
more kinetic chain muscular effort.
e. Return to the bottom position and
perform three sets of ten repetitions.
Figure 8: Swiss ball rotations
Figure 9a: TrX Serratus rollout (start position)
Figure 10a: TrX push up plus(start position)
Figure 10b: TrX push up plus (finish position)
Figure 9b: TrX Serratus rollout (finish position)
(notice the hand is turning into supination)

15 SPORTS INJURY BULLETIN No 154
17. Contemp Orthop 1991. 22: 525–532
18. Physiol Ther. 2007;30(1):69-75
19. J Shoulder Elbow Surg 2000;9:31–5
20. J Shoudler Elbow Surg 1998;7:458–61
21. Curr Rev Musculoskelet Med 2008. 1:1–11
22. Chirurgie de la main 30 2011. 90–96
23. J. Bone & Joint Surg 1955. 37-A:567-574
24. Am J Sports Med 1991. 19: 569–576
25. J Bone Joint Surg 1988. 70A: 220–226
26. Am J Sports Med 1988. 16: 481–485
27. J Orthop Sports Phys Ther 1994. 20: 307–318
28. Am J Phys Med 1977;56(5):223–40
29. Am J Sports Med1991;19(6):577–82
30. Int J Sports Med 1997;18(8):618–24
31. J Electromyogr Kinesiol. 2005;15(6):576–
586
32. Arch Phys Med Rehabil. 2002;83(1):60-9
33. Am J Sports Med 1999. Vol. 27, No. 6. 784-791
34. ConScientiae Saúde 2012. 11 (4) 660-667
35. J. Phys. Ther 2014. Sci. 26: 1275–1276
36. J Electromyogr Kinesiol. 2011 Oct;21(5):861-7
37. J Phys Ther Sci. 2013 Jul;25(7):833-7
3. J OrthopSports Phys Ther 1999. 29: 574–586
4. J Orthop Sports Phys Ther 1996. 24: 57–65
5. J. Orthop. Sports Phys. Ther. 1994;20(6):307-
318.
6. Drake RL, Vogl W, Mitchell AWM. Gray’s
anatomy for students. Philadelphia: Elsevier Inc;
2005. p. 633–47.
7. Clin Orthop Relat Res 1999. 368:17–27.
8. J BoneJoint Surg 1979;61:825–32
9. Simons et al (1999) Travell and Simons’
Myofascial Pain and Dysfunction. Volume 1
Upper Half of the Body (2nd edition). Williams
and Wilkins. Baltimore.
10. J Bone Joint Surgery. 1944. 26(1); 1-30.
11. Am J Sports Med 2004; 32:1063–76.
12. J Orthop Sports Phys Ther 1993. 18: 427–432
13. Kibler WB: Normal shoulder mechanics and
function. Instr Course Lect 46: 39–42, 1997
14. Am J Sports Med. 2003;31(4):542-9
15. Phys Ther 1994. 75: 194–202
16. Journal of orthopaedic & sports physical
therapy. 2008. 38(1). 4-11
SummaryThe serratus anterior (SA) is a muscle that plays an important role in the dynamic movement and control of the scapula during pushing movements and overhead elevation. Specifically it is a protractor, upward rotator, posterior tilt muscle of the scapula and additionally it fixes the scapula against the rib cage during movement. It is an important muscle for the overhead athlete as dysfunction in this muscle can lead to shoulder injuries such as impingement, rotator cuff breakdown and performance decrements during overhead tasks. This article has highlighted some clinically relevant exercises designed to retrain SA function in the athlete with SA dysfunction.
References1. J.Athl. Train. 2007; 42(2):311-319.
2. Phys Ther. 2000;80(3):276–291.
Neck injury
Neck injury in sport: management and rehab
In her previous article, Kay Robinson looked at neck injury assessment. In this article she focuses on injury management and rehabilitation, with the goal of a return to full performance
Having read part one in this series, clinicians can hopefully see the merit in assessing the cervical spine’s competency when screening and monitoring – particularly in sports where athletes are at risk of neck injuries due to axial loading, prolonged position exposure, whiplash and external forces such as vibrations and G force.
This article looks at treatment strategies that can be applied to all neck dysfunctions from acute injuries, right through to getting athletes back to their performance environment in peak condition. As with all injury management processes, there needs to be a clear understanding of the injury and planned rehabilitation, by both the athlete and high performance team/coaches etc. For the sake of simplicity, we will break down this rehabilitation into four stages:
Early management Initial rehabilitation Rehabilitation progression Return to performance.
Early managementThis stage of rehabilitation should begin as soon as any serious cervical or head injury has been excluded following thorough
medica l assessment and fur ther investigation if appropriate. The key goals in early management following neck injury are reduction of pain, reduction of muscle spasm and restoration of normal range of motion.
High qua l i t y e v idence on the management of acute cervical pain is lacking. However empirical evidence supports a combination of therapeutic modalities including, massage, electrical stimulation, heat, analgesics and range of motion exercises (1). This should be combined with postural education and ensuring there aren’t compensatory dysfunctions throughout the rest of the kinetic chain, especially the shoulder girdle, thoracic and lumbar spine.
Initial treatment should be carried out with the neck in neutral alignment and a ‘gravity-eliminated’ position to reduce any nerve root, disc or facet joint irritation and limit involvement of over active superficial muscles.
Gentle range of movement has good analgesic qualities and should begin as soon as possible taking care not to commence aggressive stretching of the muscles in spasm, which may reduce the
stability of the neck(2). Research shows that in patients with neck pain, the key stabilisers (deep neck flexors) become inhibited therefore must be retrained prior to further rehabilitation or loading(3).
Deep neck flexor training can begin immediately and is carried out using the stages as described by Jull et al. (2008) in the ‘Cranio-Cervical Flexion Test’ (see article part I) using a pressure cuff for feedback and working through progressive pressure increases and holds(4). Once the athlete can achieve this, avoiding compensation strategies, the routine should be done independently regularly throughout the day, and can be progressed to more gravity challenging and sport specific positions.
Following the reduction of acute symptoms, the restoration of cervical motion in all planes required for the athlete’s specific sport, and the ability to activate and maintain deep neck flexors, the athlete can progress to ‘initial rehabilitation’
Initial rehabilitationThis stage of rehabilitation is paramount in building neck mobiliser strength

16 SPORTS INJURY BULLETIN No 154
regained, sport specific neck training can begin. In contact sports, tackle bags can be used to replicate controlled contact. Divers may return to low board dives and drivers to simulation work. If athletes are exposed to external forces such as G force and vibration, this too should be replicated as rehabilitation and injury prevention.
If the athlete remains pain free, has strength comparable to baseline measures, has no change in shoulder or trunk kinematics, and has participated in controlled normal training situations (including additional external forces) then the athlete can progress to ‘return to performance’.
Return to performanceThe final phase of rehabilitation from neck injury combines the strength training that the athlete has honed, with an emphasis on the restoration of specific skills required to return to their particular sport, along with regaining confidence in being exposed to forces on the cervical spine.
I n c o r p o r a t i n g t h e a s p e c t o f unanticipated load is crucial at this stage. Eckner et al’s (2004) study showed that training pre-activation of cervical muscles to brace against impacts had the potential to decrease neck and head injuries in sport(5). This training mode should be practiced in rugby prior to going into a contested scrum situation, prior to heading a football, and also when tumbling in gymnastics. By combining training approaches such as isometric, isokinetic strengthening, exposure to vibration and impacts in and out of the sport specific setting, there is an increased chance of adapting neural elements resulting in optimal motor skill, muscular control and co-ordination.
As wi th any in jury , r e turn - to -performance programming is injury and athlete specific. As such, the decisions leading to return to play should be centered on the individual athlete but involve the entire interdisciplinary team. The athlete
Rehabilitation progressionOnce asymptomatic, and when isometric contraction of 100% MVC and full range of motion has been achieved, the focus should progress to eccentric and concentric neck strengthening through range. This is commonly an area that is identified as a weakness through screening and therefore can be used in athlete development as well as return from injury.
The athlete’s background should be considered carefully when programming. For instance, rugby players will likely to have considerable more exposure to neck strength training previously than a young gymnast returning from injury.
Through-range strengthening should be higher volume and medium intensity, and should be carried out using manual or dynamometry resistance. Initially cable machines may lead to overload but they can be used as a progression. Movements should begin in the sagittal plane and then incorporate coronal and transverse plane strength.
Principles of overload should be maintained with neck strengthening; small gains should be expected to occur gradually rather than seeing sudden spikes in training. This is particularly important when understanding the anatomy and the need for the stability across many small joints.
Once baseline strength has been
without exposing the musculature to excessive forces. Monitoring and screening data should be used where available to aid programming. Full range of motion and DNF strengthening should continue throughout this stage.
Commonly, when managing peripheral joint injuries, isometric strengthening is prescribed and yet it is often over looked following cervical injury. Again, this begins in a neutral, gravity-eliminated position, and progresses to standing followed by sport-specific positions.
For example, in the sport of Skeleton, the athlete needs to maintain neck position in prone on the sled. Motorcyclists must maintain neck position while on a bike, therefore need to have their balance challenged alongside strengthening. It is also important to consider any helmets or headgear that is worn as this can also be introduced at this stage.
Initial strength training should begin at a medium volume and low intensity and be gradually increased in terms of repetition, length of contraction and sets. Throughout this stage athletes should be monitored for any reproduction of symptoms, loss of range and any change in shoulder kinematics. As during assessment, considerations should be made to stabilise the torso and minimise lower limb involvement in order to ensure true neck strengthening.
Handheld dynamometer – Athletes should begin by carrying out 30% of their maximum voluntary contraction (MVC) to learn the technique. Over sessions they should incrementally increase to performing 100% MVC.
Cable/pulley system – Using a head harness, the mass on the pulley system should be set to avoid any overload.
Manual isometric strengthening – Manual contraction is performed against a static surface or body part. Can be easily done in all environments but unable to measure/limit loads.
Examples of strengthening exercises (following sessions to familiarise athletes with technique)
Movement Reps Rest Sets RestIntensity
(% of one rep max)
Cervical flexion x8 1 min 3 2 mins 60-70%
Cervical extension x8 1 min 3 2 mins 60-70%
Cervical side flexion x8 1 min 3 2 mins 60-70%
Cervical rotation x8 1 min 3 2 mins 60-70%
Methods of isometric neck strengthening
17 SPORTS INJURY BULLETIN No 154
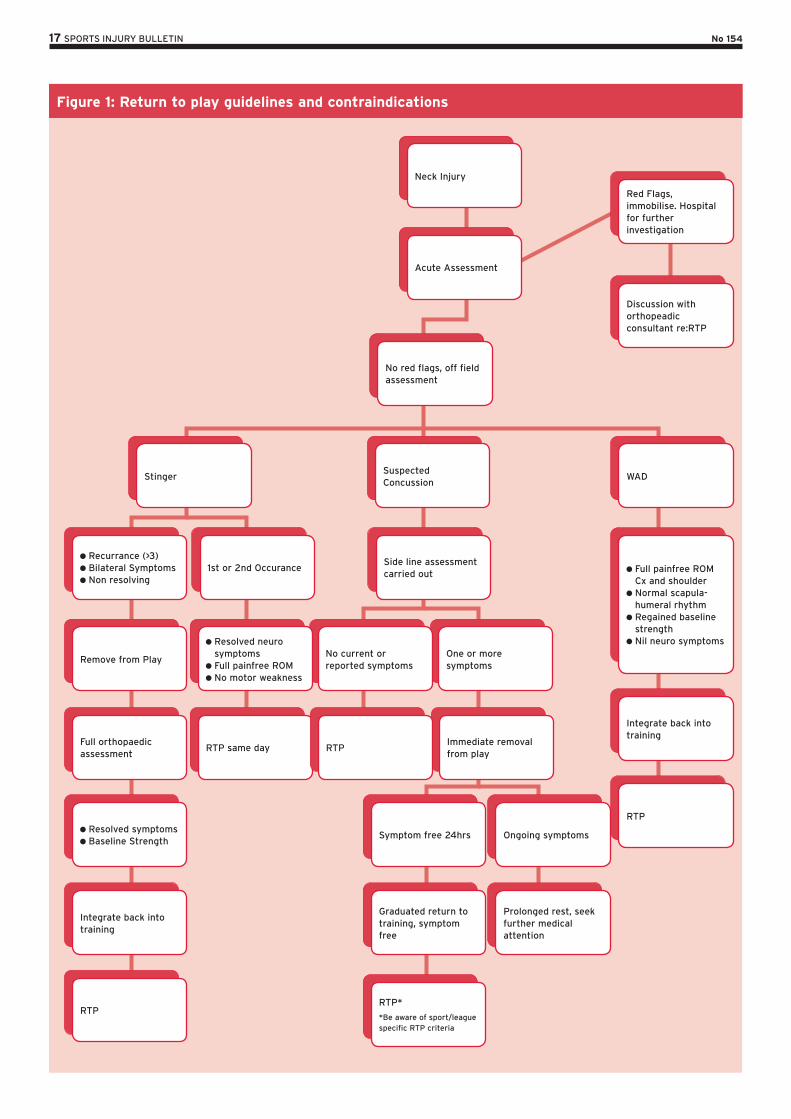
Figure 1: Return to play guidelines and contraindications
Neck Injury
Acute Assessment
Recurrance (>3) Bilateral Symptoms Non resolving
Remove from Play
Full orthopaedic assessment
Resolved symptoms Baseline Strength
Integrate back into training
RTP
RTP same day
1st or 2nd Occurance
Symptom free 24hrs
Graduated return to training, symptom free
RTP*
*Be aware of sport/league specific RTP criteria
WAD
Integrate back into training
RTP
Full painfree ROM Cx and shoulder
Normal scapula-humeral rhythm
Regained baseline strength
Nil neuro symptoms
Ongoing symptoms
Prolonged rest, seek further medical attention
Immediate removal from play
One or more symptoms
RTP
No current or reported symptoms
Suspected Concussion
Side line assessment carried out
No red flags, off field assessment
Stinger
Red Flags, immobilise. Hospital for further investigation
Discussion with orthopeadic consultant re:RTP
Resolved neuro symptoms
Full painfree ROM No motor weakness

18 SPORTS INJURY BULLETIN No 154
should be physically and psychologically ready to return with all strength, skill and confidence deficits addressed in order to reduce risk of further injury and maximise the individual’s performance on return.
Return to performance (RTP) protocols will vary depending on injury, sport and position the athlete is returning to. Figure 1 summarises the available evidence as a guide to key contraindications when returning to play following common neck injuries.
The timing of post-injury neck training should be carefully considered when programming as part of a strengthening regime; neck strengthening is known to be fatiguing and strength is initially reduced for up to a day post loading (likely longer in females)(6). Therefore, heavy neck-strength training followed by return to performance in quick succession should be avoided to minimise the risk of further injury.
Sports with heavier schedules and less recovery days should consider focusing on heavier neck strengthening in pre or mid-season breaks to allow for optimal gains. This should also be an important reason to test the athlete performing under varying levels of tiredness, and ensure they are robust enough to withstand the forces they are exposed to while competing.
SummaryAll neck weakness and movement dysfunctions found through assessment and screening should be addressed immediately in order to prevent further injury. Rehabilitation should progress from regaining range of motion, strengthening the neck and surrounding structures, to sport specific training. Deep understanding of sport specific demands and loads that the neck is subjected to is crucial for practitioners to deliver optimal
rehabilitation. This can be aided by the use of baseline data and ongoing research into the area. By following a clear assessment and rehabilitation protocol specific to individuals, we can minimise further injury and ensure athletes are returning to optimal performance with the specific strength and movement attributes required.
References1. Conservative treatments for whiplash.
Cochrane Database of Systematic Reviews
2007
2. Advances in Physiotherapy 2006; 8(98-105)
3. Sports Medicine 2009. 39(9): 697-7
4. Journal of Manipulative and Physiological
Therapeutics 2008. 31:525-533
5. American Journal of Sports Medicine 2004.
42:566
6. Physical Therapy in Sport 2010. 11(3):75-80
Contributors to this issue
Luke Heath currently works with the Greater Western Sydney Giants football team as their rehabilitation physiotherapist. Luke has also worked with the Australian Academy of sport, Australian Rugby Union, and the Australian rugby sevens team
Chris Mallac has worked as Head of Performance at London Irish Rugby, Head of Sports Med at Bath Rugby and Head Physio at Queensland Reds Super 14. He is currently teaching globally on Rehab Trainer Courses
Kay Robinson is a physiotherapist specialising in young athlete development, the sporting neck and return to performance. She is also physiotherapist to the gold medal winning GB Skeleton team at Sochi2014
Sports Injury Bulletin is published by Green Star Media Ltd, Meadow View, Tannery Lane, Bramley, Guildford GU5 0AB, UK. Telephone +44 (0)1483 892894
Commissioning Editor Andrew Hamilton
Technical Editor Chris Mallac
Managing Director Andrew Griffiths
Customer Services Duncan Heard [email protected]
Marketing Gina Edwards [email protected]
© Green Star Media Ltd. All rights reserved.
To subscribe to Sports Injury Bulletin call Duncan Heard on +44 (0)1483 892894