pathogenesis of mooren's ulcer: some new...
TRANSCRIPT
British Journal ofOphthalmology, 1984, 68, 182-187
Pathogenesis of Mooren's ulcer:some new conceptsP. I. MURRAY AND A. H. S. RAHI
From the Department of Pathology, Institute ofOphthalmology, University ofLondon, andMoorfields Eye Hospital, London
SUMMARY Mooren's ulcer is a chronic, painful corneal ulceration of unknown aetiology. Recenthistological and immunological studies suggest an autoimmune basis. It is now becoming clear thatthe immune system plays an intricate role in maintaining homoeostasis in health and disease.Regulation of the immune response appears to involve a subset of peripheral blood T lymphocytesknown as suppressor cells. A qualitative or quantitative deficiency ofsuppressor cells may thereforebe responsible for chronic inflammation, autoimmune disease, and immunodeficiency states. Toexplain the reported immunological aberrations the number of suppressor T cells in addition toother immunological parameters were studied in a patient with bilateral Mooren's ulcers. Adeficiency of suppressor T cells was found in the peripheral blood. This deficit in the immuno-regulatory mechanism explains some of the immunological abnormalities reported in previousstudies. Furthermore this study provides additional evidence for an autoimmune aetiology. In thelight of these findings the possibility of a new line of treatment has been raised.
Mooren's ulcer' is a chronic, painful ulceration of thecornea that begins in the periphery with a steep,undermined, leading edge. The ulcer spreads firstcircumferentially and then centrally to involve thewhole cornea. It is bilateral in approximately 25% ofcases but does not necessarily develop simultaneouslyin both eyes. An unequivocal cause has not beenestablished for this progressive and relentless con-dition, but an autoimmune aetiology is stronglysuspected.
Inflammation is essentially a protective response tominimise the effect of injuries-microbiological,immunological, or otherwise. In certain individualsthe inflammatory response may, however, outlive itsuseful purpose. Failure to 'switch-off' certaininflammatory responses beyond their purposefulexistence represents a weakness in the regulatorymechanism in the immune response involving a subsetof peripheral blood lymphocytes, known assuppressor cells. It has been suggested that patientshaving a qualitative or quantitative deficiency of thissuppressor machinery are more prone to chronic in-flammation2 and autoimmune disease.3Correspondence to Dr P. I. Murray, Department of Pathology,Institute of Ophthalmology, 17-25 Cayton Street, London, EC1V9AT.
Developments in the field of cellular immunologyare now constantly illuminating the complex functionsof lymphocytes in humoral and cell-mediatedimmunity. With the advent ofmonoclonal antibodies4the role of T-cell subsets,5 especially helper andsuppressorT-cells, has been made clearer. Imbalancesof the helper/suppressor ratio have increased ourunderstanding of immune regulation in variousdisease processes.
Peripheral blood lymphocytes consist of 3 distinctcell populations:
(1) B lymphocytes number about 20% of humanperipheral blood mononuclear cells. They originateand differentiate in the bone marrow and haveimmunoglobulins on their surface membrane. Theselymphocytes become antibody secreting plasma cellsin lymphoid organs and inflamed tissues.
(2) T lymphocytes number 65-70% of humanperipheral blood mononuclear cells. Their precursorsare in the bone marrow, but differentiation andmaturation takes place in the thymus, where itsmicroenvironment and the hormones produced byepithelial cells play an important role. They do notexpress surface immunoglobulin but spontaneouslyform rosettes with sheep red blood cells-known as Erosettes.
182
on 24 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.3.182 on 1 March 1984. D
ownloaded from
Pathogenesis ofMooren's ulcer: some new concepts
T lymphocytes can be subdivided into at least 4subsets: (a) Helper T-cells (TH)-number 60% of Tcells. They produce chemical messengers such asinterleukin which allow B lymphocytes to transforminto plasma cells and influence other T cell subsets.They can be identified by monoclonal antibody, forexample, OKT4 (Ortho Diagnostics).
(b) Suppressor T cells (Ts), number 30% ofT cells.They have a modulatory role and check overstimula-tion or prolonged stimulation of the immune system.They can similarly be identified by monoclonal anti-body, for example, OKT8.
(c) Cytotoxic T cells (Tc). These cells on antigenicchallenge become cytotoxic for virus-infected cellsand grafted tissues. They have some features incommon with suppressor T-cells.
(d) Delayed hypersensitivity T cells (TDH). Thesecells share some membrane characteristics with helperT cells, and produce inflammatory lymphokines(soluble, low molecular weight proteins) includingvarious chemotactic and permeability factors.
(3) Null lymphocytes (non-B, non-T) number 10%of human peripheral blood mononuclear cells andrepresent a heterogenous group. Natural killet (NK)cells can kill target cells in the absence of antibody,but the killer (K) cells always require the presence ofIgG. The group probably contains undifferentiated Tlymphocytes and monocytes. The NK cells are nowbelieved to play an important role in immunesurveillance and control of tumour growth.
Decreased numbers ofT lymphocytes (as measuredby the number of lymphocytes forming E rosetteswith sheep red blood cells) have been observed inpatients with various immunodeficiency diseases,sarcoidosis, leprosy, systemic virus infections,collagen vascular disease, and some types of cancer.It has also been shown that there is an abnormality inT cell subsets (either qualitative or quantitative) insuch diseases as systemic lupus erythematosus7(SLE), multiple sclerosis,8 myasthenia gravis,9 atopiceczema,'° and chronic active hepatitis.2
Abnormalities in T cells and their subsets have alsobeen reported in various ophthalmological con-ditions. Char et al. " found a significant decrease in Erosettes in patients with Vogt-Koyanagi-Haradasyndrome, and Heredia et al.'2 detected reducedsuppressor cell activity in retinitis pigmentosa.Grabner et al. 13 stated that during the active stage ofacute anterior uveitis the function of the suppressorcells was abnormal. Nussenblatt etal. 4 have reportedan increase in suppressor cell activity in 'activeposterior uveitis, and in the same conditionNussenblatt et al. showed an increased number ofsuppressor cells. We ourselves have found a reductionin suppressor cells in a case of lepromatous uveitis(unpublished observation). Abnormalities of the
helper/suppressor ratio have also been found inpatients with Graves' ophthalmopathy,'6 andrecurrent herpes simplex keratitis.'7As previous studies'8-26 have suggested an
autoimmune basis for Mooren's ulcer, it was decidedtherefore to investigate subsets of peripheral Tlymphocytes and other immunological parameters ina 67-year-old man suffering from bilateral Mooren'sulcers.
Case report
A 67-year-old man developed soreness and irritationof his left eye in June 1981. There was no history ofinjury. On examination his visual acuities were 6/5right, 6/6 left, and he had a left corneal ulcer involvingthe inferotemporal periphery. He was initially treatedwith a topical steroid and antibiotic combination,which had little effect. Over the next few months theulcer became more painful and progressed relent-lessly despite the addition of systemic indomethacinto the above medication. In May 1982 he underwent aleft conjunctival resection combined with cryo-therapy, but the ulcer advanced progressively, and inDecember 1982 a left total tarsorrhaphy wasperformed.
In January 1982 he developed a painful ulcer in theinferotemporal periphery of his right cornea. Thisinitially responded well to a right conjunctivalresection and cryotherapy performed in March 1982.Unfortunately his right eye flared up 4 months later,and a further conjunctival resection and cryotherapywere undertaken. In December 1982, after anotherflare-up, a right conjunctival flap was fashioned in theinferotemporal quadrant. In February 1983 he wasadmitted for investigation. On admission his rightvisual acuity was 6/5, his left visual acuity wasperception of light only. His medication was guttaePredsol-N (prednisolone and neomycin) 4 times dailyto the right eye, indomethacin slow release 75 mgonce daily, and propranolol 40 mg twice daily. Thelast drug was for hypertension, which had beendiagnosed 5 years earlier. During his stay in hospitalhe was found to have diabetes mellitus and wasstarted on glibenclamide 2-5 mg twice daily.
Materials and methods
MEASUREMENT OF T CELLS (E ROSETTES)AND THEIR SUBSETS15 ml of venous blood collected in a preservative-freeheparinised container was mixed with equalquantities of Roswell Park Memorial Institute(RPMI) 1640 tissue-culture medium (Flowlaboratories) containing 2 g/l sodium bicarbonate.Lymphocytes were isolated by a standard density
183
on 24 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.3.182 on 1 March 1984. D
ownloaded from

P. 1. Murray and A. H. S. Rahi
gradient technique by Ficoll-Paque. The lympho-cytes obtained were washed 3 times and the numberadjusted to 3 x 109/l. (Mean viability of lymphocytes>98% as assessed by 041% trypan blue exclusion.)Two drops of neuraminidase-treated sheep red bloodcells, which had been stored in fetal calf serumcontaining antibiotics, were then added to 200 ,l ofthe lymphocyte suspension, and after spinning for 5minutes at 300 g this was then incubated at 4°C forone hour. The cells were then gently resuspended,and at least 200 E rosettes (lymphocyte with at least 3red cells attached to it) were counted in a haemo-cytometer. A total lymphocyte count was alsoperformed.
Subpopulations of T cells were estimated byindirect fluorescence. Monoclonal antiserarecognising helper (OKT4, Ortho Diagnostics) andsuppressor (OKT8) subpopulations were used. 5 ,ul ofthe monoclonal reagents or phosphate buffered saline(PBS) was added to 200 ,u1 aliquots of lymphocytesuspension. The cells were incubated at 4°C for 20minutes, after which excess antibody was removed bywashing twice with cold PBS and sodium azide (toprevent capping). 100 ,ul of a second layer offluorescein labelled rabbit antimouse Ig was thenadded to each aliquot and left to incubate for a further20 minutes at 4°C. After 2 washes wet slide prepara-tions were made. Positively stained cells were countedunder a Zeiss epifluorescence microscope (at least200 cells were counted per slide), and the results wereexpressed as a percentage after subtraction for non-specific staining.Serum IgG, A, M, rheumatoid factor, and C-
reactive protein were all measured by ratenephelometry with the Beckman ImmunochemistryAnalyser II and commercially available humanantisera.
Circulating immune complexes (CIC) were precipi-tated by a polyethylene glycol (PEG) technique. Thecomplexes were then redissolved and analysed forprecipitable IgG with the Beckman ImmunochemistryAnalyser II. The level ofIgG in the CIC was expressedas a percentage of the total serum concentration ofIgG by the following equation:
Concentration of IgG in CIC (mg/I) x 100Serum concentration of IgG (mg/I)
Circulating antibodies to cornea, conjunctiva, andnonocular tissues were detected by a standard indirectimmunofluorescence technique. Examination wasperformed as before with a Zeiss epifluorescencemicroscope equiped with the appropriate inter-ference filters.The results thus achieved were compared with
normal values obtained in this laboratory.
Results
Table 1 Immunological parameters in a patient withMooren's ulcer
Immunological parameter Result Normal values
Total T cells (E rosettes) 65% 65-75%Helper T cells (OKT4+) 45 40-45Suppressor T cells (OKT8+) 13 23-27Helper/suppressor ratio 3 5 1-6-1-9Serum immunoglobulinsIgG 11-6 g/l 6-0-15-0 g/lIgA 5-84 g/l 0 9-4O0 g/IIgM 1-20 g/l 0-6-3-0 g/lCirculating autoantibodies to:Cornea Both positive -
1:10 dilutionConjunctiva (rat substrate) -
both notdetected onhuman substrate
Antibodies to nonocular tissues:Antinuclear antibodies Not detected 15%Gastric parietal cells Not detected 3%Smooth muscle Not detected 16%Circulating immune complexes 0-13% IgG <0 7% IgGRheumatoid factor <60 0 IU/mI <60-0 IU/mlC-reactive protein <6-0 mg/l <6-0 mg/l
Table 2 Immunopathological abnormalities in Mooren'sulcer
I Infiltration of tissue by lymphocytes/plasma cells/neutrophilseosinophils/mast cells
2 Raised serum IgA3 Tissue fixed immunoglobulins and complement4 Circulating auto antibodies to cornea and conjunctiva5 Raised circulating immune complex6 Cellular immunity to corneal antigen7 Reduced suppressor T cells
Discussion
Recent studies indicate that Mooren's ulcer may havean immunological basis. The relevant findings (Table2) can be discussed under 3 headings:
HISTOLOGICAL EVIDENCE OF AN IMMUNEREACTIONBrown'8 found lymphocytes and plasma cells in con-junctiva adjacent to the ulcer. This was confirmed byFoster et al. '9 who also noted the presence ofneutrophils. Tabbara and Ostler,20 as well as findingthe above 3 cell types, showed that 15-20% of theinfiltrating cells in the conjunctiva were eosinophils.Review of cases on the registry of this departmentshowed in addition the presence of degenerate mastcells.
NON-SPECIFIC IMMUNOLOGICAL PARAMETERSMondino et al.21 revealed that 56% of patients withMooren's ulcer had elevations of serum IgA which
184
on 24 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.3.182 on 1 March 1984. D
ownloaded from

Pathogenesis ofMooren's ulcer: some new concepts
were 2 standard deviations above the mean fornormal persons. (Mondino22 reported that bycontinuing this study the figure had risen to 63%.)High levels of serum IgA was also an importantfeature in this case. The reason for this immunologicalabnormality is obscure. It is of interest that raisedserum IgA levels have also been reported in patientswith acute anterior uveitis associated with activeankylosing spondylitis.2" They also found depositionof immunoglobulins G and M and complement inconjunctiva adjacent to the ulcer. This finding hassince been confirmed by Foster et al.19 and Tabbaraand Ostler.20 Berkowitz et al.23 found circulatingimmune complexes at higher levels in patients withMooren's ulcer than in the normal population. Usinga PEG precipitation technique, however, we failed toconfirm this finding.
SPECIFIC (CORNEAL AND CONJUNCTIVAL) IMMUNE
PARAMETERSSchaap et al.24 found circulating autoantibody tocornea in one patient with Mooren's ulcer, andMondino eral.2' showed that8out of9 patients studiedhad autoantibodies to cornea and conjunctiva.Mondino et al.25 demonstrated positive macrophagemigration inhibition test in response to salineextract of whole human cornea, and Foster et al.19were unable to demonstrate autoantibody to corneaor conjunctiva but noted blastogenic transformationand proliferation of lymphocytes by extracts ofnormal corneal stroma. Although they used bothhuman and xenogeneic tissues in their studies, it is notclear whether both types of extract were used.Wood and Kaufman28 and later Tabbara and
Ostler20 described 2 clinical types of Mooren's ulcer:(a) Old patients with males predominant (3:2), andhaving no predilection for race; 25% of cases arebilateral, with moderate to severe pain, and pursue aslow and relentless course. Their prognosis is fair andthey rarely perforate. (b) Young patients with malespredominant (3:1); blacks are frequently affected.The cases are usually bilateral (75%), with variableamounts of pain, and have a rapid progression. Theprognosis is poor; one-third perforate, and trauma isa predisposing factor.From our case history our patient fits into category
(a), and our findings in this patient are similar tothose in previous studies-namely, raised serum IgA,and the detection of autoantibody to cornea andconjunctiva. It must be stated, however, that auto-antibody to cornea and conjunctiva was detectedonly on xenogeneic substrate (Fig. 1); we were unableto confirm this on human substrate. The 4 possibilitiesfor this inconsistency are: (1) Rat cornea and con-junctiva as compared with human substrate may havea higher concentration of tissue-specific antigens
Fig. 1 Indirect immunofluorescence test snowingfluorescence of rat comeal epithelium with serum frompatient with Mooren's ulcer. (x272).
which are located at more accessible positions. (2)The human substrate used was not fresh but oneweek old, and although it was refrigerated the possi-bility exists that some of the antigens might have beenlost. (3) The reaction involved nonspecific antibodiescross-reacting with transplantation and otherxenogeneic antigens. (4) The antibodies in thepatient's serum were specific but of low affinity andtherefore possibly reacted only with xenogeneicsubstrate.The most significant finding (in our study) was a
decrease in suppressor T cells, causing an increase inthe helper/suppressor ratio. This has not beenreported before. The total number of E-rosetting Tcells, however, were within normal limits. One of therecent advances in immunology is the elucidation of avery important although complex core regulatorycircuit (Fig. 2) which modulates the immuneresponses and regulates the biological outcome.Applying this concept to chronic inflammatorydisorders of the eye we can explain most of theimmunological aberrations found in Mooren's ulceron the basis of a reduction of suppressor T cells asseen in the present case.The immune system29 is an intricate network
homoeostatically balanced by positive and negativeinternal signals or messages passing between thedifferent subsets of lymphocytes. These subsets differin their surface membrane characterstics as well astheir roles; some induce, others regulate, or may actas effector cells in the immune response. The currentmodel of induction and modulation of the immuneresponse requires recognition of antigen on thesurface of the macrophage by precursors of thymus-derived helper T cells. The next event is the release ofa soluble factor, interleukin 1, from the macrophage,which acts on the precursor helper T cell causingrelease of a second factor, interleukin 2. The pre-
185
on 24 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.3.182 on 1 March 1984. D
ownloaded from
P. 1. Murray and A. H. S. Rahi
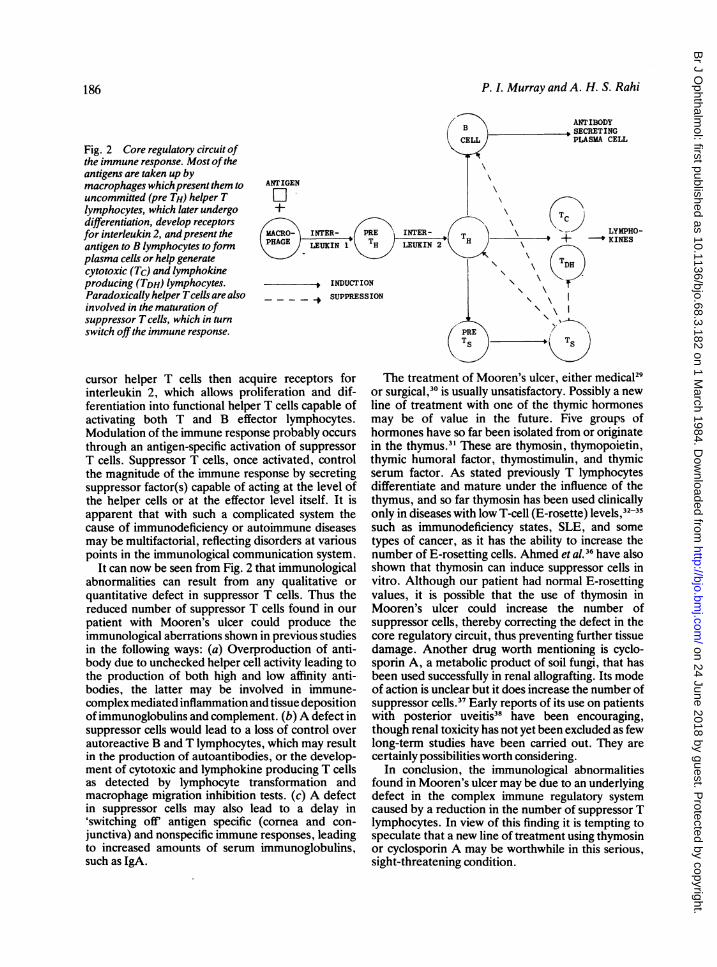
Fig. 2 Core regulatory circuit ofthe immune response. Most oftheantigens are taken up bymacrophages which present them to ANTIGENuncommitted (pre TH) helper T OIlymphocytes, which later undergo +differentiation, develop receptorsfor interleukin 2, and present the MACRO-
antigen to B lymphocytes toform PHAGE LEUKIN 1plasma cells or help generatecytotoxic (Tc) and lymphokineproducing (TDH) lymphocytes. INDUCT]Paradoxically helper Tcells are also _ _ SUPPRE'involved in the maturation ofsuppressor T cells, which in turn
switch off the immune response.
cursor helper T cells then acquire receptors forinterleukin 2, which allows proliferation and dif-ferentiation into functional helper T cells capable ofactivating both T and B effector lymphocytes.Modulation of the immune response probably occursthrough an antigen-specific activation of suppressorT cells. Suppressor T cells, once activated, controlthe magnitude of the immune response by secretingsuppressor factor(s) capable of acting at the level ofthe helper cells or at the effector level itself. It isapparent that with such a complicated system thecause of immunodeficiency or autoimmune diseasesmay be multifactorial, reflecting disorders at variouspoints in the immunological communication system.
It can now be seen from Fig. 2 that immunologicalabnormalities can result from any qualitative orquantitative defect in suppressor T cells. Thus thereduced number of suppressor T cells found in ourpatient with Mooren's ulcer could produce theimmunological aberrations shown in previous studiesin the following ways: (a) Overproduction of anti-body due to unchecked helper cell activity leading tothe production of both high and low affinity anti-bodies, the latter may be involved in immune-complex mediated inflammation and tissue depositionofimmunoglobulins and complement. (b) A defect insuppressor cells would lead to a loss of control overautoreactive B and T lymphocytes, which may resultin the production of autoantibodies, or the develop-ment of cytotoxic and lymphokine producing T cellsas detected by lymphocyte transformation andmacrophage migration inhibition tests. (c) A defectin suppressor cells may also lead to a delay in'switching off' antigen specific (cornea and con-junctiva) and nonspecific immune responses, leadingto increased amounts of serum immunoglobulins,such as IgA.
IO
ss
/B > ANTIBODYSECRETING
CEL PLASMA CELL
T
RE INTER- \ -- LYMPHO-N LEUKIN 2 H
W~~~~~~~~~~~
;ION \ \IIONS \ \, '
The treatment of Mooren's ulcer, either medical29or surgical,30 is usually unsatisfactory. Possibly a newline of treatment with one of the thymic hormonesmay be of value in the future. Five groups ofhormones have so far been isolated from or originatein the thymus.31 These are thymosin, thymopoietin,thymic humoral factor, thymostimulin, and thymicserum factor. As stated previously T lymphocytesdifferentiate and mature under the influence of thethymus, and so far thymosin has been used clinicallyonly in diseases with low T-cell (E-rosette) levels,32-35such as immunodeficiency states, SLE, and sometypes of cancer, as it has the ability to increase thenumber of E-rosetting cells. Ahmed et al.36 have alsoshown that thymosin can induce suppressor cells invitro. Although our patient had normal E-rosettingvalues, it is possible that the use of thymosin inMooren's ulcer could increase the number ofsuppressor cells, thereby correcting the defect in thecore regulatory circuit, thus preventing further tissuedamage. Another drug worth mentioning is cyclo-sporin A, a metabolic product of soil fungi, that hasbeen used successfully in renal allografting. Its modeof action is unclear but it does increase the number ofsuppressor cells.3" Early reports of its use on patientswith posterior uveitis38 have been encouraging,though renal toxicity has not yet been excluded as fewlong-term studies have been carried out. They arecertainly possibilities worth considering.
In conclusion, the immunological abnormalitiesfound in Mooren's ulcer may be due to an underlyingdefect in the complex immune regulatory systemcaused by a reduction in the number of suppressor Tlymphocytes. In view of this finding it is tempting tospeculate that a new line of treatment using thymosinor cyclosporin A may be worthwhile in this serious,sight-threatening condition.
186
on 24 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.3.182 on 1 March 1984. D
ownloaded from

Pathogenesis ofMooren's ulcer: some new concepts
Our thanks are due to Mr Noel Rice for allowing us to publish detailsof this case, to Mr J. Prasad for technical assistance, and to Miss K.Betts for secretarial help. P. I. Murray is at present the recipient ofthe Friends of Moorfields Research Fellowship Grant.
References
I Duke-Elder S, Leigh AG. Diseases of the outer eye: In: Duke-Elder S, ed. System of Ophthalmology. London: Kimpton, 1965:8 (2): 916.
2 Frazer IH, Mackay IR. T-Lymphocyte sub-populations definedby two sets of monoclonal antibodies in chronic active hepatitisand systemic lupus erythematosus. Clin Exp Immunol 1982; 50:107-14.
3 Strelkauskas AJ, Callery RT, McDowell J, et al. Direct evidencefor loss of human suppressor cells during active autoimmunedisease. Proc NadAcad Sci USA 1978; 75: 5150-4.
4 Reinherz EL, Kung PC, Goldstein G, Schlossman SF. Separationof functional subsets of human T-cells by a monoclonal antibody.Proc NadAcad Sci USA 1979; 76: 4061-5.
5 Reinherz EL, Schlossman SF. Regulation of the immuneresponse-inducer and suppressor T-lymphocyte subsets in humanbeings. N Engl J Med 1980; 303: 370-3.
6 Wybran J, Fudenberg HH. Thymus-derived rosette forming cellsin various disease states: cancer, lymphoma, bacterial and viralinfections and other diseases. J Clin Invest 1973; 52: 1026-32.
7 Abdou NI, Sagawa A, Pascual E, Herbert J, Sadeghee S.Suppressor T-cell abnormality in idiopathic systemic lupuserythematosus. Clin Immunol Immunopathol 1976; 6: 192-9.
8 Reinherz EL, Weiner HL, Hauser SL, Cohen JA, Distaso JA,Schlossman SF. Loss of suppressor T-cells in active multiplesclerosis-analysis with monoclonal antibodies. N Engl J Med1980; 303: 125-9.
9 Miller AE, Hudson J, Tindall RSA. Immune regulation inmyasthenia gravis: evidence for an increased suppressor T-cellpopulation. Ann Neurol 1982; 12:341-7.
10 Butler M, Atherton D, Levinsky RJ. Quantitative and functionaldeficit of suppressor T-cells in children with atopic eczema. ClinExp Immunol 1982; 50:92-8.
11 Char DH, Brunn J, West W. Thymus-derived lymphocytes in theVogt-Koyanagi syndrome. Invest Ophthalmol Visual Sci 1977; 16:179-81.
12 Heredia CD, Vich JM, Huguet J, Garcia-Calderon JV, andGarcia-Calderon PA. Altered cellular immunity and suppressorcell activity in patients with primary retinitis pigmentosa. Br JOphthalmol 1981; 65:850-4.
13 Grabner G, Berger R, and Knapp W. Concanavalin A inducedsuppressor cell activity in inflammatory uveal disease. In: Trevor-Roper P, ed. Proceedings of the 6th Congress of European Oph-thalmology London: Academic Press and Royal Society ofMedicine, 1980:487-91.
14 Nussenblatt RB, Cevario SJ, and Gery 1. Altered suppressor-cellactivities in uveitis. Lancet 1979; u: 601-3.
15 Nussenblatt RB, Salinas-Carmona M, Leake W, Scher 1. T-lymphocyte subsets in uveitis. Am J Ophthalmol 1983; 95:614-21.
16 Felberg N, Sergott R, Savino P, Blizzard J, Schatz N.Lymphocyte subpopulations in Graves' ophthalmopathy. ArvoAbstracts. Supplement to Invest Ophthalmol Visual Sci. St Louis:Mosby, 1983: 192.
17 Stelzer GT, Eiferman RA, Watson S. Alterations in T-cellsubsets in patients with recurrent herpes simplex keratitis. ArvoAbstracts. Supplement to Invest Ophthalmol Visual Sci. St Louis:Mosby, 1983: 192.
18 Brown SI. Mooren's ulcer. Histopathology and proteolyticenzymes of adjacent conjunctiva. Br J Ophthalmol 1975; 59:670-4.
19 Foster CS, Kenyon KR, Greiner J, Greineder DK, Friedland B,Allansmith MR. The immunopathology of Mooren's ulcer. Am JOphthalmol 1979; 88:149-58.
20 Tabbara KF, Ostler HB. Mooren's ulcer. In: Trevor-Roper P, ed.Proceedings of the 6th Congress of European Ophthalmology.London: Academic Press and Royal Society of Medicine, 1980:269-73.
21 Mondino BJ, Brown SI, and Rabin BS. Autoimmune phenomenaof the external eye. Ophthalmology 1978; 85: 801-17.
22 Mondino BJ. Autoimmune phenomena in ocular cicatricialpemphigoid, Mooren's ulcer and Sjogren's syndrome. In:Helmsen RJ, Suran A, Gery I, eds. Proceedings ofImmunologyof the Eye: Workshop: II Special Suppl Immunology Abstracts1981: 77-89.
23 Berkowitz PJ, Arentsen JJ, Felberg NT, Laibson PR. Presence ofcirculating immune complexes in patients with peripheral cornealdisease. Arch Ophthalmol 1983; 101: 242-5.
24 Schaap OL, Feltkamp TEW, and Breebaart AC. Circulatingantibodies to comeal tissue in a patient suffering from Mooren'sulcer (ulcus rodens corneae). Clin Exp Immunol 1969; 5:365-70.
25 Mondino -BJ, Brown SI, Rabin BS. Cellular immunity inMooren's ulcer. Am J Ophthalmol 1978; 85: 788-91.
26 Brown SI. What is Mooren's ulcer? Trans Ophthalmol Soc UK1978; 98: 390-2.
27 Cowling P, Ebringer R, Ebringer A. Association of inflammationwith raised serum IgA in anklyosing spondylitis. Ann Rheum Dis1980; 39: 545-9.
28 Wood TO, Kaufman HE. Mooren's ulcer. Am J Ophthalmol1971; 71: 417-22.
29 Waterfield JD. New approaches to immunodeficiency in man. J RSoc Med 1982; 75: 825-7.
30 Stilma JS. Conjunctival excision or lamellar scleral autograft in 38Mooren's ulcers from Sierra Leone. Br J Ophthalmol 1983; 67:475-8.
31 Trainin M, Pecht M. Handzel ZT. Thymic hormones: inducersand regulators of the T-cell system. Immunology Today 1983; 4:16-21.
32 Goldstein AL, Low TLK, Thurman GB, et al. Current status ofthymosin and other hormones of the thymus gland. Recent ProgHorm Res 1981; 37: 369-412.
33 Costanzi J, Daniels J, Thurman G, Goldstein A, and HokansonJ. Clinical trials with thymosin. Ann NY Acad Sci 1979; 332:148-59.
34 Goldstein AL, Cohen GH, Rossio JL, Thurman GB. Brown CN,Ulrich JT. Use of thymosin in the treatment of primary immuno-deficiency diseases and cancer. Med Clin N Am 1976; 60:591-607.
35 Chretien PB, Lipson SD, Makuch RW, Kenady DE. Effects ofthymosin in vitro in cancer patients and correlation with clinicalcourse after thymosin immunotherapy. Ann NY Acad Sci 1979;332:135-47.
36 Ahmed A, Wong DM, Thurman GB, et al. T-lymphocytematuration: cell surface markers and immune function inducedby T-lymphocyte cell-free products and thymosin polypeptides.Ann NYAcad Sci 1979; 332: 81-94.
37 Routhier G, Epstein 0, Janossy G, et al. Effects of cyclosporin Aon suppressor and inducer T lymphocytes in primary biliarycirrhosis. Lancet 1980; ii: 1223-6.
38 Nussenblatt RB, Palestine AG, Rook AH, Scher I, Wacker WB,Gery I. Treatment of intraocular inflammatory disease with cyclo-sporin A. Lancet 1983; ii: 235-8.
187
on 24 June 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.3.182 on 1 March 1984. D
ownloaded from