patient driven groupings odel special presentation for
TRANSCRIPT

Gina Mazza MBA, BSN, RN, CPHQ
Senior Vice President
Fazzi Associates
PATIENT DRIVEN GROUPINGS MODEL:Special Presentation for Advisory Board
November 2019
Lisa Woolery RN, BSN, COQS, BCHH-C,
AHIMA Certified ICD-10-CM Trainer
Director of Coding Education
Fazzi Associates

Today’s Objectives
Identify the changes and insight related to PDGM from the
2020 final rule.
Discuss service utilization strategies, including LUPA
management.
Discuss key insights on coding guidelines related to PDGM

Payment Impact, 2020
Budget Neutral Approach
Non-routine Supplies paid in standard
payment
RAPs continue – for one year
LUPA category remains – with various
thresholds
Partial Episode Payment Maintained
Outlier Policy Maintained
30-Day Unit of Payment
• 30-day period = days 1-30 of a current 60-day episode where “day
1” is the current 60-day episode’s From Date.
• Second period is days 31 and ongoing.
• CMS has finalized a 2020, national standardized 30-day payment
amount, $1,864.03.
• Going forward will calculate payment amount by updating the
preceding year by the HH payment update percentage.

PDGMCase MixStructure
Admission Sourceand Timing Community Early Community Late Institutional Early Institutional Late
Comorbidity None Low High
Functional Level Low Medium High
= HHRG 432
Clinical Group
Neuro Rehab
Wounds
Complex Nursing Interventions
MS Rehab
Behavioral Health
MMTA - Surgical Aftercare
MMTA - Cardiac/Circulatory
MMTA - Endocrine
MMTA - GI/GU
MMTA - Infectious Disease/ Neoplasms/Blood-Forming Disease
MMTA – Respiratory
MMTA - Other

Admission Source
• Uses a 14 day “look-back” period to each 30 day period.
• Community: No acute or post-acute care in the 14 days prior to the HH admission.
• Institutional: Acute care or post-acute, inpatient psychiatric facility. Skilled nursing facility, inpatient rehab facility, long term care hospital in the 14 days prior to the admission.
• Medicare claims processing system would check for presence of an acute/post-acute Medicare claim occurring prior to 14 days of the HH admission and on an ongoing basis.
• Manual Occurrence Codes will be allowed.

Optional Occurrence Codes
61- Hospital Discharge Date
62- Other Institution Discharge Date
Uses a 14 day “look-back” period to each 30 day period.
Occurrence codes are not reported on RAPs.
Monitor remittance advice for recoding of payment.

Timing
• Only the first 30-day period in a sequence of periods defined as early
and all other subsequent 30-day periods would be considered late.
• First episodes are those where the beneficiary has not had home health
paid for by Medicare in the 60-days prior to the start of the first episode.
• Medicare Secondary Payer functions as if primary Medicare.
• To identify the first 30-day period in a sequence, Medicare claims processing system would verify that the claims “From Date” and “Admission Date” match.

Clinical Groupings
• Each 30-day period of care will be assigned to one of twelve groups based on the reported principal diagnosis.
• Diagnosis code must support the need for HH services.
• Claims will be returned to provider if primary diagnosis is not accepted in PDGM.

“Questionable Encounters”
• Unspecified diagnoses: Location, Laterality and Acuity
• Not appropriate by severity: Rash, contusion, abrasion
• Symptom codes (R codes) Dysphagia R13.1 is back!
• Pain M-codes: Muscle Weakness!
• History codes

Common Diagnoses No Longer Accepted –Under PDGM
• Muscle Weakness
• Other abnormalities of gait and mobility
• Unsteadiness of Gait
• Repeated falls
• Low back pain/Back pain unspecified
• Pain in r/l hip, shoulder, knee
• Retention of urine
• Bacteremia
• Dysphagia
• Dizziness
• Polyneuropathy, unspecified
• Rheumatoid Arthritis, unspecified
Alternatives to Ineligible Diagnoses
• What condition is responsible for the symptom? Code first the condition.
• Is the patient still in recovery from surgery? Code first the Aftercare.
• Is the diagnosis acceptable when further specified? Obtain specifics needed.
• Is the condition an injury? Code the injury with appropriate 7th
character.

Finding an Alternative Diagnosis
Diagnosis not fitting into a clinical grouping How to approach
M62.81 Muscle Weakness Ask for the reason the patient is presenting with muscle weakness. Did the patient have surgery or an injury? If so, the aftercare of the surgery or the injury may be a more appropriate diagnosis. Is there muscle atrophy?
M54.5 Low back pain or M54.9 Back pain, unspecified Ask for the reason patient is presenting with low back pain. For example, does the patient have a chroniccondition like spinal stenosis or a back injury. The chronic condition may be more appropriate reason for referral. Is chronic pain a more appropriate reason for referral?
R13.10 Dysphagia, unspecified Ask for reason patient is now presenting with dysphagia. For example, does the patient have a chronic condition,like a stroke, that has resulted in the dysphagia. If so, the chronic condition may be the more appropriate reason for referral

Finding and Alternative DiagnosisDiagnosis not fitting into a clinical grouping How to approach
Rheumatoid Arthritis, unspecified Ask the referral source to identify the rheumatoid factor or the specified type (juvenile or idiopathic) and ask the referral source to specify single or multiple locations
Polyneuropathy Ask the referral source for the reason the patient is now presenting with polyneuropathy. For example, does the patient have a chronic condition, like diabetes, that has resulted in the polyneuropathy. If so the chronic condition may be the correct diagnosis. Or the referral source may need to specify the exact type of neuropathy (ex idiopathic)
Retention of Urine, unspecified Ask the referral source the reason the patient is presenting with urine retention. For example, does the patient have a chronic condition like BPH that has resulted in urine retention. Use that diagnosis instead

The Challenge
• The primary and secondary diagnoses assigned must be supported by clinician documentation and the F2F
• When the primary diagnosis & the F2F match up – but the clinician documentation does not support the code – you are at risk for denial
• When the primary diagnosis & the clinician documentation match up – but the F2F does not support the code – you are at risk for denial
• Coding guidance must still be followed, which may result in an “unacceptable” primary diagnosis
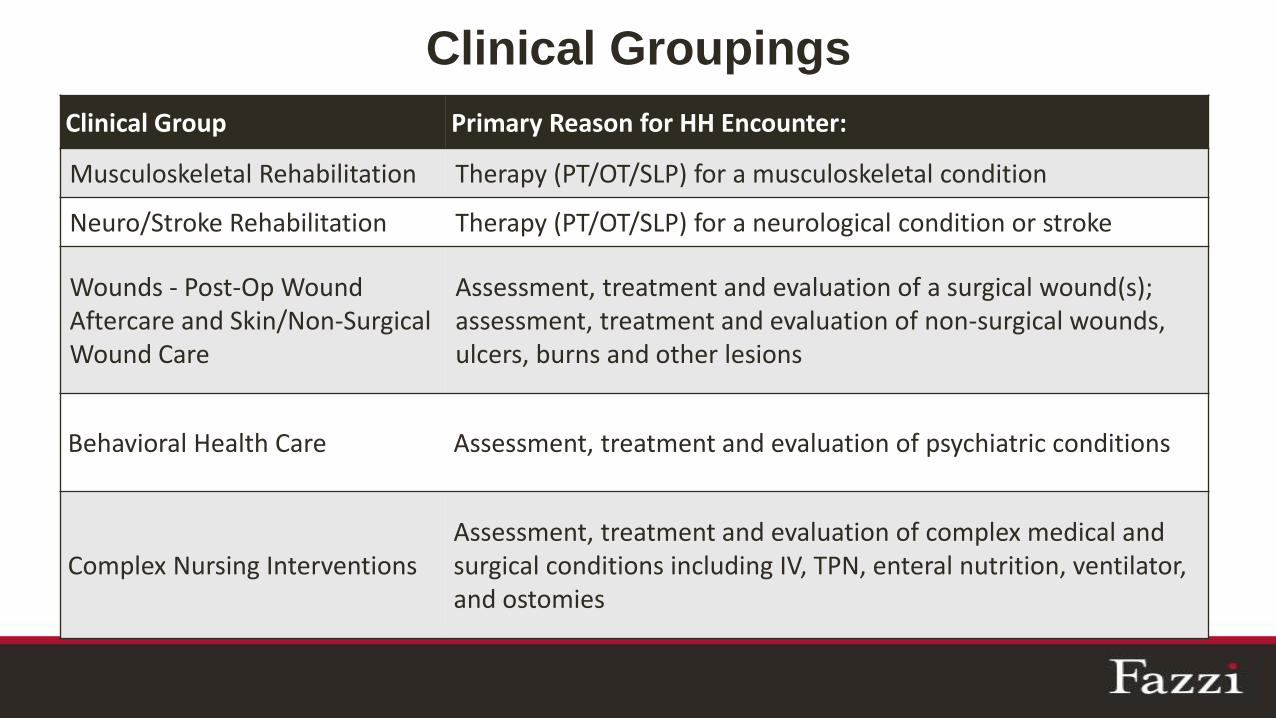
Clinical Groupings
Clinical Group Primary Reason for HH Encounter:
Musculoskeletal Rehabilitation Therapy (PT/OT/SLP) for a musculoskeletal condition
Neuro/Stroke Rehabilitation Therapy (PT/OT/SLP) for a neurological condition or stroke
Wounds - Post-Op Wound Aftercare and Skin/Non-Surgical Wound Care
Assessment, treatment and evaluation of a surgical wound(s); assessment, treatment and evaluation of non-surgical wounds, ulcers, burns and other lesions
Behavioral Health Care Assessment, treatment and evaluation of psychiatric conditions
Complex Nursing InterventionsAssessment, treatment and evaluation of complex medical and surgical conditions including IV, TPN, enteral nutrition, ventilator, and ostomies

12 Clinical Groups, ContinuedClinical Group Primary Reason for HH Encounter:
MMTA – Surgical AftercareAssessment, evaluation, teaching, and medication management for surgical aftercare
MMTA – Cardiac/CirculatoryAssessment, evaluation, teaching, and medication management for cardiac or other circulatory related conditions
MMTA – EndocrineAssessment, evaluation, teaching, and medication management for endocrine related conditions
MMTA – GI/GUAssessment, evaluation, teaching, and medication management for gastrointestinal or genitourinary related conditions
MMTA – Infectious Disease/Neoplasms/Blood-forming Diseases
Assessment, evaluation, teaching and medication management for conditions related to infectious diseases, neoplasms, and blood-forming diseases
MMTA – RespiratoryAssessment, evaluation, teaching and medication management for respiratory related conditions
MMTA – OtherAssessment, evaluation, teaching, and medication management for a variety of medical and surgical conditions not classified in one of the previously listed groups

Clinical Group Frequency of Use %
MS Rehab 17.9
Neuro Rehab 10.1
Wound 8.9
Behavioral
Health3.6
Complex Nursing 3.5
MMTA 56.1
Source: Department of Health and Human Services, Centers for Medicare & Medicaid Services, Federal Register, Vol. 83, No. 219,
November 13, 2018 and Federal Register, Vol. 82, No. 144, July 28, 2017.
MMTA
Aftercare 6.1
Cardiac 31.7
Endocrine 8.5
GI/GU 8.0
Infectious 6.9
Respiratory 14.4
Other 24.4
Distribution of Clinical Groups

Comorbidities
• Secondary diagnosis codes used to case-mix adjust the period further through the comorbidity adjustment.
• No Adjustment: No comorbidity diagnosis that falls into a comorbidity adjustment subgroup.
• Low Comorbidity Adjustment: A comorbidity diagnosis that falls into one comorbidity adjustment subgroup.
• High Comorbidity Adjustment: Two or more diagnosis that fall within the same comorbidity subgroup interaction.

For reporting purposes, “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring:
clinical evaluation; or
therapeutic treatment; or
diagnostic procedures; or
extended length of hospital stay; or
increased nursing care and/or monitoring.
“all conditions that coexist at the time of admission, that develop subsequently, or that affect the treatment received and/or the length of stay. Diagnoses that relate to an
earlier episode which have no bearing on the current hospital stay are to be excluded.”
Comorbidities: Reporting Additional Diagnoses

Diagnoses Comorbidities LOW
https://www.federalregister.gov/documents/2019/11/08/2019-24026/medicare-and-medicaid-programs-cy-2020-home-health-prospective-payment-system-rate-update-home
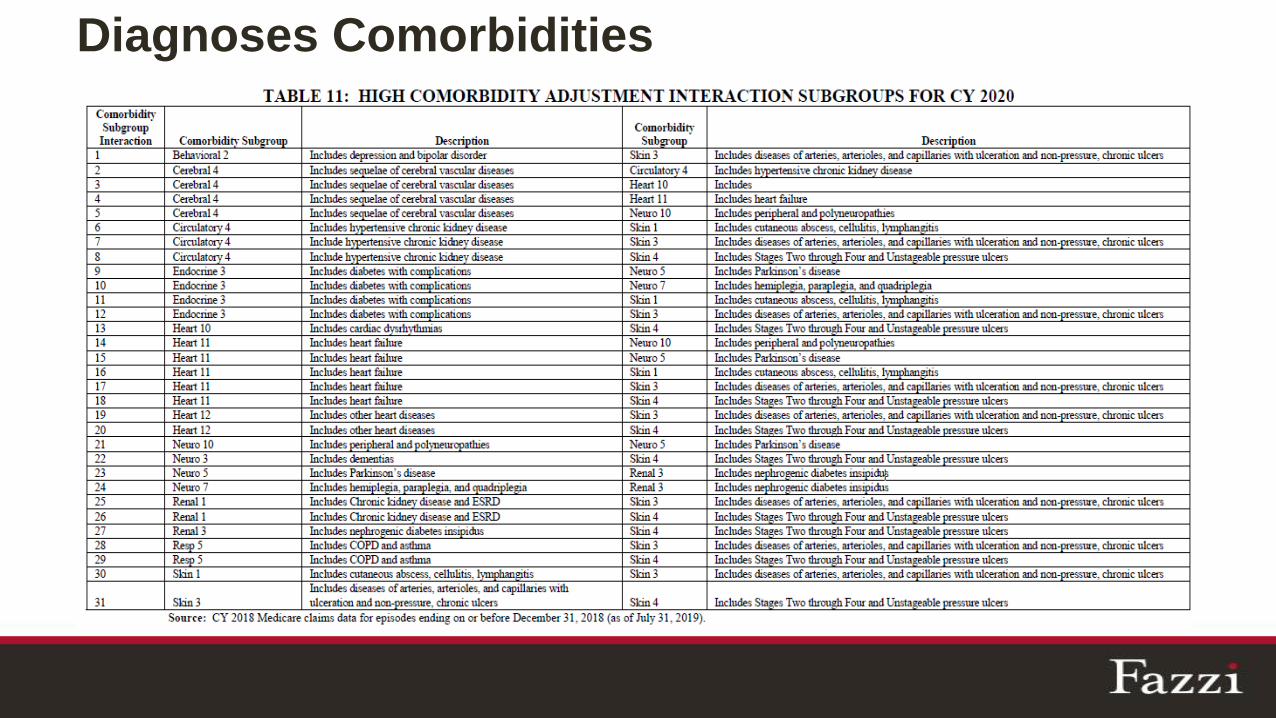
Diagnoses Comorbidities

None to HIGH Comorbidity Comparison
23
Early/Institutional
AFC THR
M1800 Grooming: 1
M1810 Upper body: 2
M1820 Lower body: 2
M1830 Bathing: 5
M1840 Toilet TX: 2
M1850 Transfers: 2
M1860 Ambulation: 3
M1033 Hosp Risk: 4+
Early/Institutional
AFC THR, A-Fib, PU heel US
M1800 Grooming: 1
M1810 Upper body: 2
M1820 Lower body: 2
M1830 Bathing: 5
M1840 Toilet TX: 2
M1850 Transfers: 2
M1860 Ambulation: 3
M1033 Hosp Risk: 4+
$ 342.48
Functional Impairment
• Functional status allows for higher payment for higher service needs.
• Functional scores result in 3 levels: low, medium, high.
• Functional levels per clinical group.
• Functional scores and levels have been updated for 2020.

Functional ItemsM1800: Grooming
M1033: Risk of Hospitalization
Current HH PPS M1810: Dressing upper body
M1860: Ambulation & locomotion
M1820: Dressing lower body
M1830: Bathing
M1840: Toileting
M1850: Transferring
M1810: Dressing upper body
M1860: Ambulation & locomotion
M1820: Dressing lower body
M1830: Bathing
M1840: Toileting
M1850: Transferring
PDGM

Plan for OASIS D1
• Addition of two existing items to the Follow-Up assessment.
• Optional data collection at specific time points for 23 items.
• Effective for M0090 Date Assessment Completed as of January 1, 2020 or later and, recertifications on or after December 27, 2019.
• Recerts on or after December 27, 2019: enter the M0090 date of January 1, 2020 and submit on January 1, 2020.
Source: CMS OASIS- D1 OASIS Updates for CY 2020https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HomeHealthQualityInits/Downloads/OASIS-D1-Update-Memorandum_Revised_May-2019.pdf

Order Management
Workflows of 30-Day Payment Periods
June
S M T W T F S
1
2 3 4 5 6 7 8
9 10 11 12 13 14 15
16 17 18 19 20 21 22
23 24 25 26 27 28 29
30
60-Day Certification
July
S M T W T F S
1
2 3 4 5 6 7 8
9 10 11 12 13 14 15
16 17 18 19 20 21 22
23 24 25 26 27 28 29
30 31
Front-load
services
Tapered
services
OASIS
OASIS RAPClaimRAP
Claim

PDGM and Quality Episode
• Two 30-day payment periods within one 60-day certification period.
• 60-day timing for certification periods remains unchanged.
• Assessment within 5 days of SOC and, no less than last 5 days of every 60 days unchanged.
• Plan of Care corresponds with 60-day certification.
• OASIS time points remain unchanged.
• Significant Change in Condition is required.

§484.55(d) Standard: Update of the comprehensive assessment.
The comprehensive assessment must be updated and revised (including
the administration of the OASIS) as frequently as the patient’s condition
warrants due to a major decline or improvement in the patient’s health
status, but not less frequently than-
Interpretive Guidelines §484.55(d)
A marked improvement or worsening of a patient’s condition, which changes, and was not anticipated in, the patient’s plan of care would be considered a “major decline or improvement in the patient’s health status” that would warrant update and revision of the comprehensive assessment.

LUPAs
• LUPA thresholds will vary for a 30 day period depending
on the payment group to which it is assigned.
• LUPA thresholds range from 2-6 visits.
• LUPA add-on factors will remain the same as current
system.
• LUPA thresholds for each PDGM payment group will be
reevaluated every year.

LUPA Management
• Build OASIS Competence to more accurately capture acuity.
• OASIS and risk-profile drive plan of care using evidence based
practice and data.
• Reduce LUPAs created by subpar behaviors (e.g. planned recert
LUPAs, missed visits)
• Audit for trends of LUPAs and identify the cause.
• Learn what you can and cannot control. Focus on best practice
care planning.
• For what is left with LUPAs, lower your cost.

Request for Anticipated Payment (RAP)January 1, 2020:
• Agencies certified on/after January 1, 2019 submit a “No Pay” RAP at beginning of care and every 30 days in PDGM.
• Agencies certified before January 1, 2019, submit RAP and receive split payment of 20% RAP and 80% final claim.
January 1, 2021:
• All certified providers submit a no-pay RAP within 5 calendar days at the beginning of each 30 day period. RAP payment is eliminated.
• RAPs for first and second payment period can be submitted together.
January 1 2022:
• All certified providers submit a one-time Notice of Admission (NOA) within 5 days from the start of care date.
• Covers all contiguous 30 day periods.
Non-timely Submission Penalty
• Applies to No-Pay RAPS and Notice of Admission (NOA).
• Penalty for not submitting a timely NOA: 1/30th of payment each day RAP or NOA is not received.

Agency Behavior Change Assumptions Adjustment
-4.36% Adjustment to Payment
1. Clinical Group Coding: Coding to maximize payments.
2. Comorbidity Coding: More 30 day periods will receive comorbidity adjustment.
3. LUPA Threshold: 1-2 extra visits will be made to receive the full 30 day payment.
As You Initiate Strategic Change Efforts, Remember the J Curve of Change
• Whenever you initiate change, it never goes exactly how you expect.
• There is often resistance and the belief by some that the change won’t work.
• Like the letter J, the path may go down but it will go up.
• Having a clear vision and an unwavering commitment to your mission and core values will absolutely lead to success.


Additional Support Available for Post-Acute Care Collaborative Members

References
• Fazzi Business Intelligence Analysis
• Department of Health and Human Services, Centers for Medicare & Medicaid Services, Federal Register, Vol. 83, No. 219, November 13, 2018
• HHS. CMS. Medicare and Medicaid Programs: CY 2020 Home Health Prospective Payment System Rate Update; Home health Value-Based Purchasing Model; and Home Health Quality Reporting Requirements and Home Infusion Therapy Requirements. Final Rule.