patient information - prosites, inc.c1-preview.prosites.com/88749/wy/docs/childpatientbundle.pdf ·...
TRANSCRIPT

Patient's Name:
lf patient is a minor, parent or guardian's name:
Address:
Patient Information
Birthdate:
tr Male tr Female tr Married tr Single tr Child tr Other
Ap.rtm.nt *
How long at this address?GitY
Phone (Home):
Stelc Zip Codc
(Work): Ext _ (Cellular):Email address: May we send email appointment reminders?
Social Security Number. Drive/s License Number
Employer Name:
Address:
Occupation:
Str€ft
Stst€ Zip CodeHow long at this employer?
BirthdateCilY
Spouse's Name
Employer Name:
Address:
Occupation:
Str€.t Pfronc il
How long at this employer?
Insurance Company Name and Address
Subscriber Social Security Number. B irthdate_G rou p Nu m ber
Do you have additional dentaf insurance? Subscriber Name
Subscriber Social Security Number Birthdate Group Nurnber.
Secondary Insurance Company Name and Address
Please let us know how you heard about our otfice:
Nearest relative not residing with you
Address:
Relationdhip
Emergency contact (someone other than responsible party)
Addrcss: Phone
Phone
Conaenl for Setvlce.A| r ordlbrdF, Lrlnrnl bt !ib.{id, nrnd.l.trief. ritt |rid b. ntd h -yrE, n!. t|ctb. dFrrb !to.l r*nf.Ma tm nN p.tl-r.lq ur (ur.Inu.d h iFr 6 rn rL-drr| po.reu, q! tr Fl C adr Furil ,a !a (|.lrfihd ltlb.. !x!t n(
All.lnritit_d.ddr.flicr.o.-td.rrai!..vi*9-ffi$bcrFftb{|fir:ddan-{rnfl|,tn,d!.,atstrhc-lraltrtir..rvb.rrrtp.dbnr$
Pdfna lE riy dria hrrs uil-.t '!t lrl aI rbt l rRtc.. 6rr{.nd r. drrg.d dndly b th pd.nt rd H h. d .h. i. Fr!.dr rrpqdbb lo. p.tirn$l li.lF t|el| ih prha. f||rrE Emr d ... h n||d|.oll.clb trm burrc. coop..Lr d wl crdl my rdr colL.lbn lo lr pda{. @6L tb'xvr. !a rldi f- crrd '.b.
on thc s$rrrnptlqr that otr chergcr will br psid by an intwance cornp.ny.
A ...*r dlf!. d lt{l F rs$ (1!* F II|n) or L uTd i.lr€ l,| !. dlrl.d cr.l6|lr €..lll0 ifF, u\b. f$iorty sim inadd rr||trnnlr .ll ldfu
I uxlr rxl lh.t !r La adnah irLd ta 0lir (|.r||l c'l cal,| olrt ba a mdad ftr a F..bd ot rU ,|E{r fqn L dda of !| ldbl urrldiol.
h dr.ld-.tloo b. Ur Flb.bd tr{cB r|.xbrd b r., d .l my !..t b! h. Doqo.. | .qr to p.y t$o !i. oodrDb v.tr ol rad rraic.r b .rld Ooda, a li. r.Er.. t h. rhr !.id.rvi.- r. rrr.Lr4 a*l$fv. (6}iLyr d blllf |td.4.hdlb. dbnfd. I luttrr trx ru t n n|-b v.lx o, ..U .rv5.r .lr.lr b. .. !{bd h.. otidd b, !r m. b rft. drin rrUr & FF.r! !r.oL lluiraarrtliaardrxotrr!n.lrotr?ltracq{fbnhmnL$.1 I cd.liirb. fltr ol $t irit[ rnn d coi.ildr rxt ltrtr.!rr. ion ro.-b &n!y i... f rt D. l lt hd hrt|f|.h..
llrfinyFrlr.ldlbyoodlt|rrdgr|.,bLl.far|lti|.lhcr.danyrEtb.Lal.rm.n-d.i.dbt.bnn,
I havc lled the lbov€ conditions of trrltmont End pEymenl End .grur to thalr cont6nt.
Signature of patient, parent or guardian
_ Date: Relationship to Patient:
Name
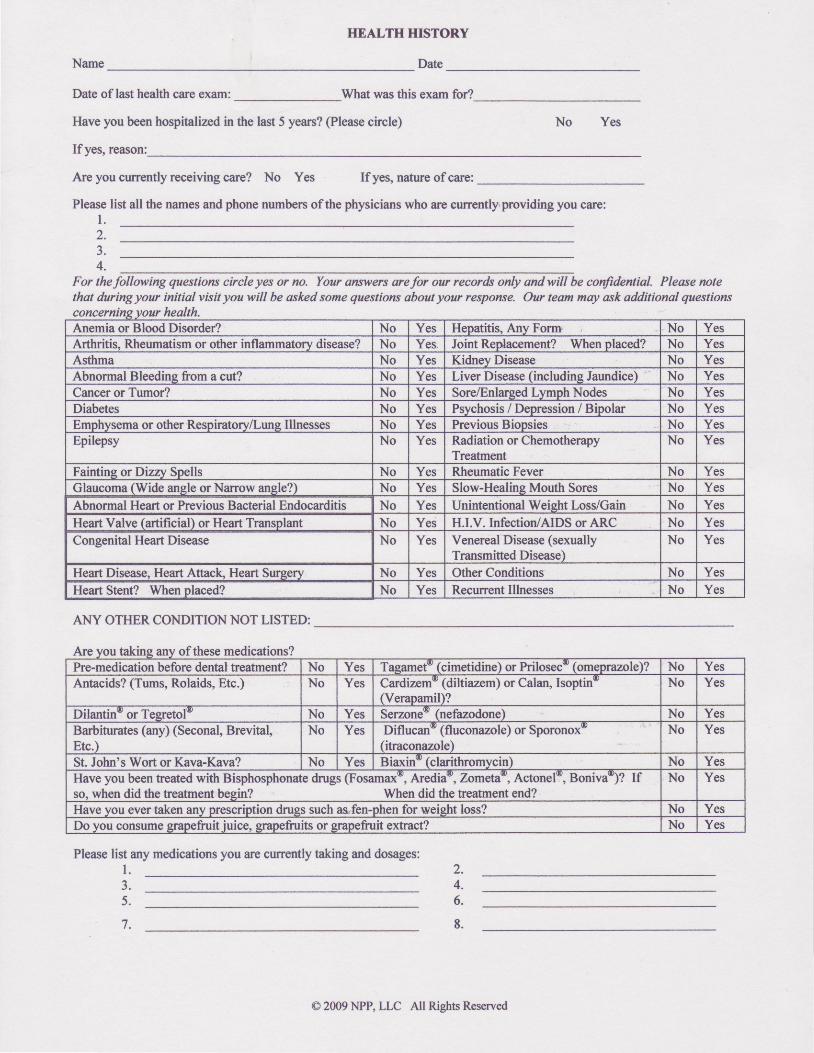
TIEALTH HISTORY
Date
Date of last health cire exam: What was this exam for?
Have you been hospitalized in the last 5 years? (Please circle) No Yes
Ifyes, reason:
Are you currently receiving care? No Yes If yes, nature of care:
Please list all the names and phone numbers of the physicians who are eurrently'providing you care:l .
For thefollowing qtestions circle yes or no, YorE anstrerc oefo our records only andwill be cotfideftial- Please notethat during you initial visit you utill be askcd some questions about yow response. Ow team may ask additional questions
health.
ANY OTHER CONDITION NOT LISTED:
Please list any medications you ile currently taking and dosages:1 . 2.
4.6.
8.
2.3.4.
J .
5.
7.
tAnemia or Blood Disorder? No Yes Henatitis. Any Form. No YesArthritis. Rheumatism or other inflammatonr disease? No Yes. Joint Replacement? When placed? No YesAsthma No Yes Kidnev Disease No YesAbnormal Bleedine from a cut? No Yes Liver Disease (includine Jaundice) No YesCancer or Tumor? No Yes Sore/Enlarged Lymph Nodes No YesDiabetes No Yes Psychosis / Depression / Bipolar No YesEmphvsema or other Respiratorv/Lune Illnesses No Yes Previous Bionsies No YesEpilepsy No Yes Radiation or Chemotherapy
TreatmentNo Yes
Faintine or Diz,w Soells No Yes Rheumatic Fever No YesGlaucoma (Wide anele orNarrow anele?) No Yes Slow-Healine Mouth Sores No YesAbnonnal Heart or Previous Bacterial Endocarditis No Yes Unintentional Weieht Loss/Gain No YesHeart Valve (artificial) or Heart Transplant No Yes H.I.V. lnfectioniAlDS or ARC No YesCongenital Heart Disease No Yes Venereal Disease (sexually
Transmitted Disease)No Yes
Heart Disease, Heart Attack" Heart Surgery No Yes Other Conditions No YesHeart Stent? When placed? No Yes Recurrent Illnesses No Yes
Are you takine any of these medications?Pre-medication before dental treatment? No Yes Tasamet* (cimetidine) or Prilosec- (omeprazole)? No YesAntacids? (Tums, Rolaids, Etc.) No Yes Cardizem- (diltiazem) or Calan, Isoptin
(Verapamil)?No Yes
Dilantin'or Tegretol* No Yes Serzone* (nefazodone) No YesBarbiturates (any) (Seconal, Brevital,Etc.)
No Yes Diflucan- (fluconazole) or Sporonox(itraconazole)
No Yes
St. John's Wort or Kava-Kava? No Yes B ia,rin* (c larithromyc in) No YesHave you been treated with Bisphosphonate drugs (Fosamaxt, Aredia*,7-ometav, Actonela, Boniva)? Ifso, when did the treatment beein? When did the treatment end?
No Yes
Have vou ever taken anv prescription drugs such as..fen-phen for weieht lsss? No YesDo you consume grapefruit-iuice, grapefruits or grapefruit extract? No Yes
O 2009 NPP, LLC All Rights Reserved

Please list any dieary or herbal supplements you are taking, and for what purpose:l . 2 .
4.6.
Women: Are you pregnant?If no, are you planning a pregnancy in the near future?Are you a nwsing mother?Are you taking birth control pills?
Abnormal Blood Pressure? (Please circle)Have you ever received a diagnosis of "high blood pressure"?What is your normal blood pressure? S tD Today:
Are you allergic or have you had a reaction to:a. Local anestheticsb. Penicillin or other antibioticsc. Aspirin, Ibuprofen or Tylenold. Codeine, Valium@ or other sedativese. Latex or Metalsf. Sulfites ( Red wine, PABA in sunscreen, Food in salad bar? )g. Other (please speciff)
obacco, Alcohol
DOCTOR'S USE ONLYComments on patient interview concerning medical history:
J .
5.
No YesNo YesNo YesNo Yes
No Yes
No YesNo YesNo YesNo Yes
,Do you use tobacco? Ifyes, circle type: smoke chew How much per day? For how lond No YesDo you want to quit using tobacco? No YesDo you consume alcohol? If yes. approximately how manv alcoholic beverages per week? No YesDo you use any mood altering drugs other than those previously listed? ( CONFIDENTIAL & MAY BELIFE THREATENING WITH DENTAL ANESTI#TIC, )
No Yes
Weisht and Diet considerationsWeight Meals per Dav Dietarv Restrictions Food Allereies
Sugar in your diet (circle one): none slisht moderate hish
Significant findings from questionnaire or oral interview:
Dental management considerations :
I undentaad the abwe irformotion is necessary to prwide me virt dental care in a safe and fficient maftEr. I haveanswoed all questions to the best ofnty btowledge Shouldftrther irfornaion be needed, yoa have ny permlssion to akthe respective health care prwider or agercy, who malt release such Won ration byou. I utillnotify the doctor {ehotge innn health od medication
Patient (Print Name) Patient Signature Date
Doctor (Print Name) Doctor Signature
@ 2009 NPP, LLC All Rights Reserved
Date
,-
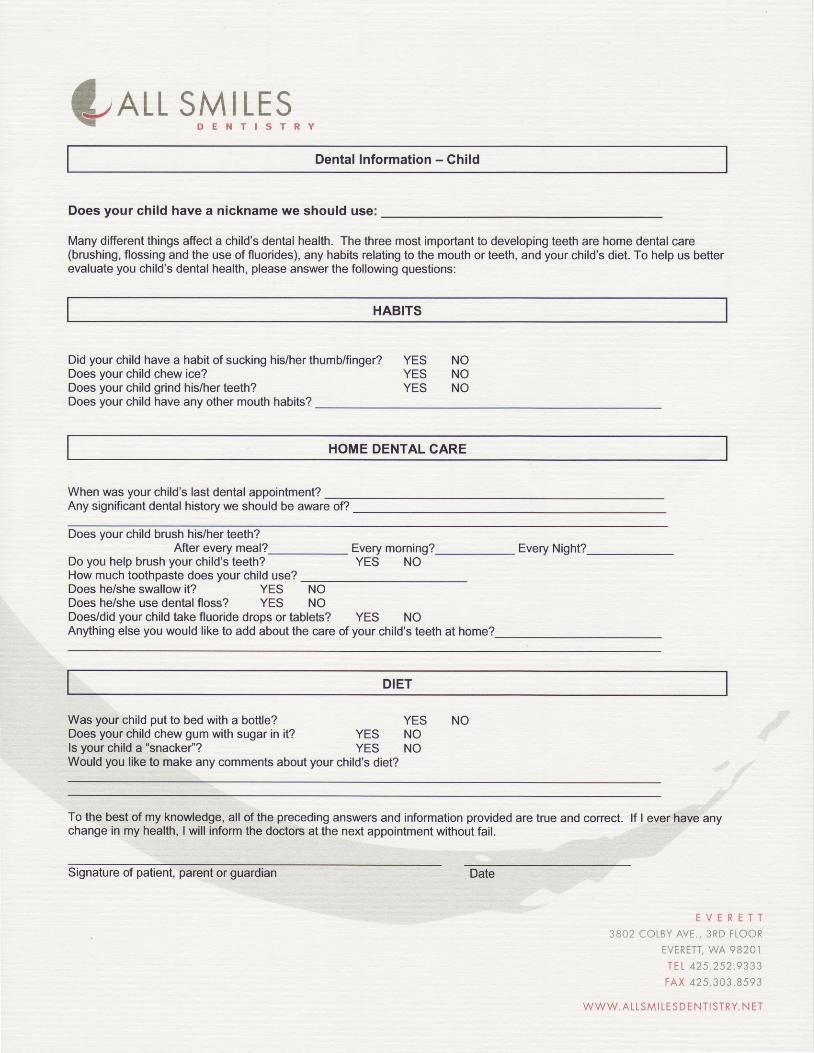
?ALL s|l*r 1,q9."Dental Information - Child
Does your child have a nickname we should use:
Many different things afiect a child's dental health. The three most important to developing teeth are home dental care(brushing, flossing and the use of fluorides), any habits relating to the mouth or teeth, and your child's diet. To help us befterevaluate you child's dental health, please answer the following questions:
HABITS
Did your child have a habit of sucking his/her thumb/finger? YES NODoes your child chew ice?Does your child grind his/her teeth?Does your child have any other mouth habits?
YES NOYES NO
HOME DENTAL CARE
When was your child's last dental appointment?Any significant dental history we should be aware of?
Does your child brush his/her teeth?After every meal? Every morning?
YES NOEvery Night?
Do you help brush your child's teeth?How much toothpaste does your child use?Does he/she swallow it? YES NODoes he/she use dental floss? YES NODoes/did your child take fluoride drops or tablets? YES NOAnything else you would like to add about the care of your child's teeth at home?
DIET
Was your child put to bed with a bottle? YES NODoes your child chew gum with sugar in it? YES NOls your child a "snacke/'? YES NOWould you like to make any comments about your child's diet?
To the best of my knor,ledge, all of the preceding answers and information provided are true and conect. lf I ever have anychange in my health, I will inform the doctors at the next appointment without fail.
E V E R E T T
3BO2 COLBY AVE. , 3RD FLOOR
EVERETT, WA 9B2OI
r E L 4 2 s . 2 s 2 . 9 3 3 3
FA,X 425 .303 .8593
W W W . A L L S M I L E S D E N T I S T R Y . N E T
Signature of patient, parent or guardian Date
E
fuALL SMILES\ E T
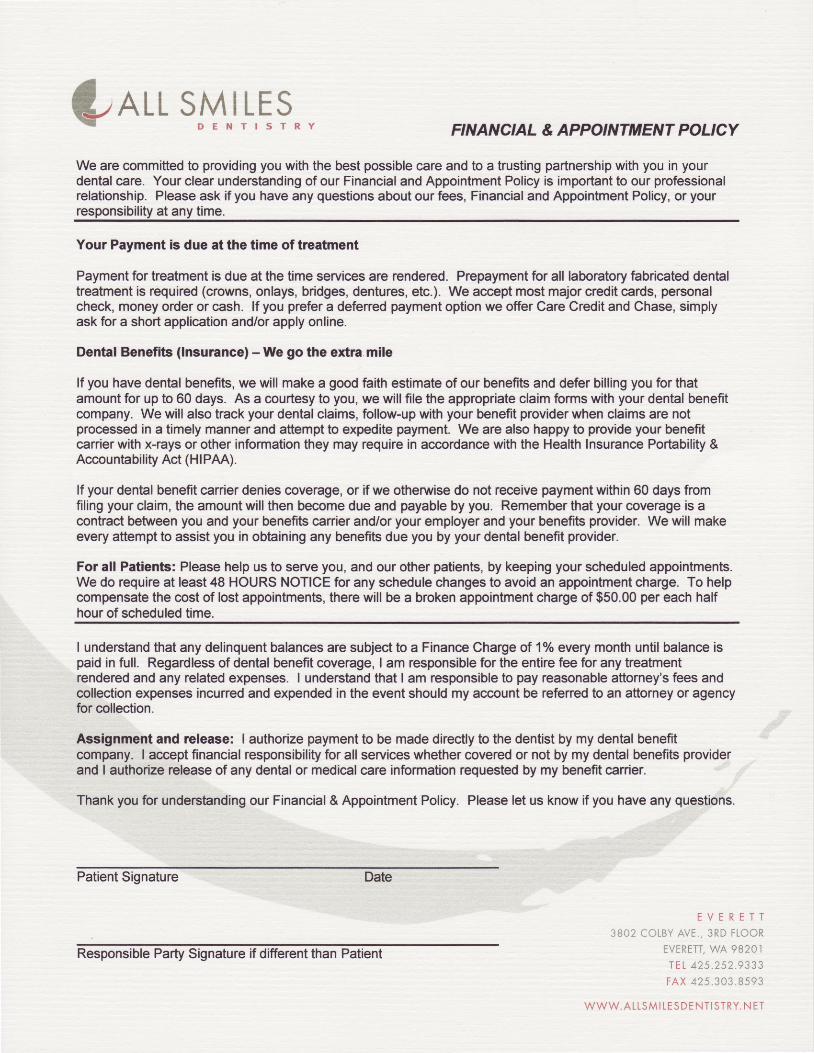
D E N T I s T R Y FINANCIAL & APPOINTMENT POLICY
We are committed to providing you with the best possible care and to a trusting partnership with you in yourdental care. Your clear understianding of our Financial and Appointment Policy is important to our professionalrelationship. Please ask if you have any questions about our fees, Financial and Appointment Policy, or yourresponsibility at any time.
Your P.yment i3 due 8t the time of trcatment
Payment for treatment is due at the time services are rendered. Prepayment for all laboratory fabricated dentaltreatment is required (crowns, onlays, bridges, dentures, eb.). We accept most major credit cads, personalcheck, money order or cash. lf you prefer a defened payment option we offer Care Credit and Chase, simplyask for a short application and/or apply online.
Dental Ben€fit3 (lnsurance) - We go the extra.mile
lf you have dental benefits, we will make a good fuith estimate of our benefits and defer billing you br thatamount for up to 60 days. As a courtesy to you, we will file the appropriate claim brms with your dental benefitcompany. We will also track your dental claims, follow-up with your benefit prcvider when claims are notprocessed in a timely manner and attempt to expedite payment. We are also happy to provide your benefitcanier with x-rays or other information they may require in accodance with the Health Insurance Portiability &Accountability Act (Hl PAA).
lf your dental benefit canier denies coveEge, or if we otheMise do not receive payment within 60 days fromfiling your claim, the amount will then become due and payable by you. Remember that your coverage is acontract between you and your benefib caffier and/or your employer and your benefits provider. We will makeevery attempt to assist you in oblaining any benefits due you by your dental benefit provider.
For all Patlents: Please help us to serve you, and our other patients, by keeping your scheduled appointments.We do require at least 48 HOURS NOTICE for any schedule changes to avoid an appoinEnent charge. To helpcompensate the cost of lost appointments, there will be a broken appointment charge of $50.00 per each halfhour of scheduled time.
I understand that any delinquent balances are subjec{ to a Finance Charge of 1% every month until balance ispaid in full. Regardless of dental beneftt coverage, I am responsible for the entire be for any treatnentrendered and any related expenses. I understand that I am responsible to pay reasonable attomey's fees andcollection expenses incuned and expended in the event should my account be refened to an attomey or agencyfor collection.
Assignment and releasc: I authorize payment to be made directly to the dentist by my dental benefitcompany. I accept financial responsibility for all services whether covered or not by my dental benefits providerand I authorize release of any dental or medical carc information requested by my benefit carier.
Thank you for understanding our Financial & Appointment Policy. Please let us know if you have any questions.
Patient Signature Date
E V E R E T T
3 B C 2 C O L B Y A V E . , 3 R D F L O O R
EVERETT, Y /A 9B2OI
T E L 4 2 5 . 2 5 2 . 9 3 3 3
FAX 425 .303 8593
W W W . A L L S M I L E S D E N T I S T R Y . N E T
Responsible Party Signature if ditferent than Patient
sE,arr,sMll-ESE/^LL " i I t * ' l , t r rRy
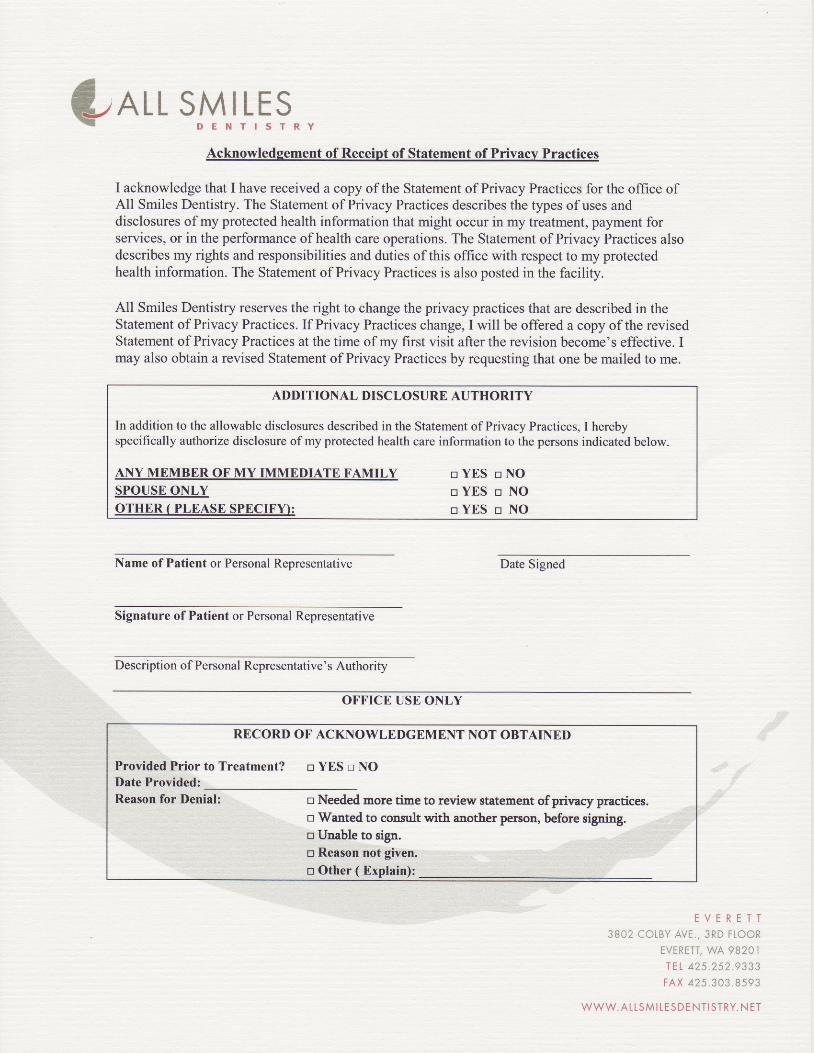
Acknowledgement of Receipt of Statement of Privacv Practices
I acknowledge that I have received a copy of the Statement of Privacy Practices for the office ofAll Smiles Dentistry. The Statement of Privacy Practices describes the types of uses anddisclosures of my protected health information that might occur in my treatment, payment forservices, or in the perfonnance of health care operations. The Statement of Privacy Practices alsodescribes my rights and responsibilities and duties of this office with respect to my protectedhealth information. The Statement of Privacy Practices is also posted in the facility.
All Smiles Dentistry reserves the right to change the privacy practices that are described in theStatement of Privacy Practices. If Privacy Practices change, I will be offered a copy of the revisedStatement of Privacy Practices at the time of my first visit after the revision become's effective. Imay also obtain a revised Statement of Privacy Practices by requestingthat one be mailed to me.
Name of Patient or Personal Representative Date Signed
Signature of Patient or Personal Representative
Description of Personal Representative' s Authority
ADDITIONAL DISCLOSURE AUTHORITY
In addition to the allowable disclosures described in the Statement of Privacy Practices, I herebyspecifically authorize disclosure of my protected health care information to the persons indicated below.
ANY MEMBER OF MY IMMEDIATE FAMILYSPOUSE ONLYOTHER ( PLEASE SPECIFD:
n Y E S n N OnYES n NOnYES n NO
OFFICE USE ONLY
RBCORD OF ACKNOWLEDGEMENT NOT OBTAINED
Provided Prior to Treatment? n YES n NODate Provided:Reason for Denial: n Needed more tine to review statement of privacy practices.
n Wanted to consult with another penlon, before signing.n Unable to sign.n Reason not given.
n Other ( Explain):
E V E R E T T
3 8 0 2 C O L B Y A V E . , 3 R D F L O O R
EVERETT, WA 9B2OI
IEL 425 252 9333
F A X 4 2 5 3 0 3 8 5 9 3
W W W . A L L S M I T E S D E N T I S T R Y . N E T
n
WAI.L SMILES: - D E N T I S T R Y
Statement of Privacy Practices
Our office is dedicated to protect the privacy rights of our patients and the confidential information entrusted to us. Thecommitment of each employee to ensure that your health information is never compromised is a principal concept of ourpractice. We may, from time to time, amend our privacy policies and practices but will always inform you of any changesthat might affect your rights.
Protecting Your PeFooal Healthcarc Information
We use and disclose information we collect from you only as allowed by the Health Insurance Portability andAccountability Act and the state of Washington. This includes issues relating to your treatment, payment and our healthcare operations. Your personal health information will never be otheMise given to anyone - even family members -without your wriften consent. You, of course, may given written authorization for us to disclose your information to anyoneyou choose, for any purpose.
Our offices and electronic systems are secured fofin unauthorized access and our employees are trained to make certainthe contidentiality of your records is always protected. Our privacy policy and ptectices apply to all former, cunent, andfuture patients, so you can be confident that your protected health infiormation will never be improperly disclosed orreleased.
Gollecting Protected Health lnformation
We will only request personal information needed to provide out standard of quality health care, implement paymentactivities, conduct normal health practice operations, and comply with the law. This may include your name, address,telephone numbe(s), Social Security Number, employment data, medical history, health records, etc. While most of theinformation will be collected form you, we may obtain information from third parties if it is deemed necessary. Regardlessof the source, your personal information will always be protected to the full extent of the law.
Discloaurc of Your Perconal Hoalth lnfomation
As stated above, we may disclose information as required by law. We are obligated to provide information to lawenforcement as government officials under certain circumstances. We will not use your information for marketingpurposes without your wriften consent.
We may use and/or disclose your health information to communicate reminders about your appointrnents includingvoicemaiyemail messages, answering machines, and postcards.
Pationt Rights
You have a right to request copies of your he€lthcare information; to request copies in a variety of formats; and to requesta list of instances in which we, or our business associates, have disclosed your protected informat'on for uses other thanstated above. All such requestes must be in writing. WE may charge for your copies in an amount allowed by law. lf youbelieve your rights have been violated, rve urge you to notify us immediately. You can also notiry the U.S. Department ofHealth and Human Services.
Please let us know if you have any questions conceming your privacy rights and the protection of your O"oonl l?1,1 , ,information'
3e02 colBy AvE., 3RD FLooREVERETT, WA 9E2OI
I E L 4 2 5 2 5 2 9 3 3 3
F A X 4 2 5 . 3 0 3 8 5 9 3
W W W . A L L S M I L E S D E N T I S T R Y . N E T
All Smiles Dentistry