patient participation and shared decision making in ... · patient participation and shared...
TRANSCRIPT

Available online at www.sciencedirect.com
Z. Evid. Fortbild. Qual. Gesundh. wesen (ZEFQ) 105 (2011) 263–270
Patient participation and shareddecision making in Germany –history, agents and current transfer topracticeMartin Härter1,∗, Hardy Müller2, Jörg Dirmaier1, Norbert Donner-Banzhoff3, Christiane Bieber4, Wolfgang Eich4
1University Medical Center Hamburg-Eppendorf, Department of Medical Psychology2Techniker Krankenkasse (TK), Scientific Institute of TK for Benefit and Efficiency in Health Care, Hamburg3University Hospital Marburg, Department of General Practice4University Medical Center Heidelberg, Department of General Internal Medicine and Psychosomatics
SummaryThe main focus of the present paper is to describe 1) the healthcare sys-tem specific influences on patient participation in medical decision makingand 2) the current state of research and implementation of shared decisionmaking (SDM) after ten years of substantial advances in health policy andresearch in this field.What about policy regarding SDM?The ‘‘Medical Patients Rights Act’’ is to standardise all the rights and respon-sibilities within the scope of medical treatment. This also comprises the rightto informed decisions, comprehensive and comprehensible information forpatients, and decisions based on the partnership of clinicians and patients.What about tools – decision support for patients?SDM training programmes for healthcare professionals have been devel-oped and partly implemented. Several decision support interventions – pri-marily with support from health insurance funds – have been developedand evaluated.
What about professional interest and implementation?Against the background of the German health policy’s endorsement ofpatient participation, the German government and other public institu-tions are currently funding different research programmes in which shareddecision making is playing a substantial role. The development and im-plementation of decision support tools for patients and professionals aswell as the implementation of trainings for healthcare professionals requirestronger efforts.What does the future look like?With the support of health policy and with the utilisation of scien-tific evidence, the transfer of shared decision making into practice isconsidered to be meaningful in the German healthcare system. Thetranslation into routine care will remain an important task for thefuture.
K(
ey words: patient participation, shared decision mAs supplied by publisher)
∗Corresponding author. Prof. Dr. Martin Härter, UniversityTel.: +49 40-7410-52978; fax: +49 40-7410-58170.E-Mail:[email protected] (M. Härter).
Z. Evid. Fortbild. Qual. Gesundh. wesen (doi:10.1016/j.zefq.2011.04.002
aking, health policy, patient orientation, Germany
Medical Center Hamburg-Eppendorf, Department of Medi
ZEFQ)
cal Psychology, Martinistraße 52, D-22391 Hamburg.
263

Patientenbeteiligung und Partizipative Entscheidungsfindung in Deutschland: HistorischeEntwicklung, Träger und Praxistransfer
ZusammenfassungZiel dieses Beitrags ist einerseits die Beschreibung, wie das deutscheGesundheitssystem spezifischen Einfluss auf die Patientenbeteiligung beimedizinischen Entscheidungen nimmt. Andererseits werden der gegen-wärtige Stand der Forschung und die Implementierung der PartizipativenEntscheidungsfindung (PEF; Shared Decision Making) 10 Jahre nach sub-stanziellen Fortschritten in der Gesundheitspolitik und Forschung in diesemFeld ausgewertet.Wie steht es mit gesetzlichen Regelungen zur PEF?Das geplante Gesetz über Patientenrechte soll die Rechte und Verant-wortlichkeiten bezüglich medizinischer Behandlungsmaßnahmen regeln.Es umfasst sowohl das Recht auf informierte Entscheidungen sowie um-fassende und verständliche Informationen für Patienten als auch medi-zinische Entscheidungen, die partnerschaftlich von Ärzten (und anderenGesundheitsberufen) und Patienten getroffen werden.Wie steht es mit PEF-Instrumenten – Entscheidungshilfen für Patien-ten?Spezifische Trainingsprogramme zur Partizipativen Entscheidungsfin-dung für medizinische Fachkräfte wurden entwickelt und teilweise
implementiert. Medizinische Entscheidungshilfen wurden – haupt-sächlich mit Unterstützung von Krankenkassen – entwickelt undevaluiert.Wie steht es mit dem Interesse der Profession und der Implemen-tierung?Vor dem Hintergrund der Unterstützung der Patientenbeteiligung durchdie deutsche Gesundheitspolitik fördern die Bundesregierung und andereöffentliche Träger Forschungsprogramme, in denen Patientenorientierungund PEF einen Schwerpunkt bilden. Es sind jedoch noch verstärkte Anstren-gungen im Bereich der Entwicklung und Implementierung von Entschei-dungshilfen für Patienten sowie der Implementierung von Trainingspro-grammen für Gesundheitsberufe notwendig.Wie sieht die Zukunft aus?Mit der Unterstützung der Gesundheitspolitik und gestärkt durch wis-senschaftliche Belege zur Wirksamkeit wird die Übertragung der PEFin das deutsche Versorgungssystem als bedeutsam eingeschätzt. Trans-lation in die Routineversorgung ist eine wichtige Aufgabe für dieZukunft.
S ative iente(
I
TocaoattsaaTpceipvaalrTifltpis
pis
Ppc(FC
TswutImhtwcalmhave advisory and proposal rights. Ad- diagnostics, and advantages and risks
2
chlüsselwörter: Patientenbeteiligung, PartizipWie vom Gastherausgeber eingereicht)
ntroduction
he German health care system is basedn solidarity and self-government and isontribution-financed. The health insur-nce system is composed of a mixturef statutory and private health insur-nce programs covering almost the en-ire population. For all insured persons,he health care benefits of the compul-ory insurance are fundamentally equalnd defined by law. This applies topproximately 89% of the population.he remaining 11% are insured throughrivate insurance, in which the healthare benefits are determined by differ-nt rates according to the needs of thensured person. Unlike many other Euro-ean countries, Germany does not pro-ide its citizens with health care throughcentralised state-run system, but viacomplex network of public bodies at
aw and a large number of independentegional and local bodies.he goal of this article is 1) to clar-fy the specific health care system in-uences upon which patient participa-ion, patient information, and the im-
lementation of shared decision makingn Germany are based. 2) The currenttatus of milestones concerning training
vpa
64
Entscheidungsfindung, Gesundheitspolitik, Pat
rograms, research, development andmplementation of SDM will be de-cribed.
atient participation inolitical decisionsoncerning health caremacro level)ederal Joint Committee andommissioner for Patients
he Federal Joint Committee (Gemein-amer Bundesausschuss, www.g-ba.de)as institutionalised as a legal entitynder public law formed by the Na-ional Association of Statutory Healthnsurance Physicians (KBV), the Ger-an Hospital Society (DKG) and theealth insurance funds in 2004. Theask of the board is to substantiatehich outpatient or inpatient medi-
al benefits are adequate, practicablend cost-effective, and therefore be-ong to health services. Within the com-ittee, patients, as official members,
isory rights include the sharing of ex-eriences and of interests of patientsnd the self-help of chronically ill and
Z. Evid. Fortbild. Qual.
norientierung
disabled persons. The proposal rightsrefer, for instance, to the acceptabil-ity of new research and treatmentmethods. Around 100 experts are in-volved as permanent patient represen-tatives, who represent and counsel theFederal Joint Committee. Furthermore,in 2004, the Federal Government ap-pointed the ‘‘Commissioner for Patientsof the Federal Government’’ (rank ofa state secretary) to represent patientinterests. His foremost contribution isto strengthen patient rights and to ad-vance these within the health care sys-tem (www.patientenbeauftragte.de).
Patient laws and juristicperspectives on shareddecision making
In 1999, the Conference of GermanHealth Ministers adopted the document‘‘Patient rights in Germany today’’. It isexplicitly laid down that patients havethe right to clear, expert and satisfac-tory education and counselling in or-der to explain the usage and risks of
of the treatment or non-treatment op-tions. Physicians must be sure that pa-tients have understood the information.
Gesundh. wesen 105 (2011) 263–270www.elsevier.de/zefq

IiirFtaPwsacmipcsthfAfatlsmthtop
NsmlIE
Tciatpmiet
rsb
gcG
A
Agit(giAacoeoattlpsaNdpelptbaapmlmwG
GE
Fw
t is pre-assigned that patients must benformed about the type and possibil-ty of different risks and their relation toecovery chances.urther legal regulations that influencehe diffusion of shared decision makingre the German Social Code (SGB V,aragraph 1 and SGB IX, Paragraph 9),hich concerns patients’ solidarity, re-
ponsibility and active participation incute care as well as rehabilitation (in-luding a ‘‘personal budget’’ for treat-ent decisions). In addition, the health
nsurance funds are assigned to sup-ort these goals through education andounselling. This law allows health in-urance funds to implement contribu-ions to the collective of the insured in-abitants in order to diffuse informationor patients or develop decision aids.t the end of 2010, the Commissioner
or Patients of the Federal Governmentnnounced a ‘‘Law on Patients’ Rights’’o come into force in 2011/2012. Thisaw is to standardize all rights and re-ponsibilities within the framework ofedical treatment. This also comprises
he right to informed decisions, compre-ensive and comprehensible informa-ion for patients, and decisions basedn the partnership of the clinician andatient.1
ational institutionsupporting patients’edical decisions (meso
evel)nstitute for Quality andfficiency in Health Care (IQWiG)
he Institute for Quality and Effi-iency in Health Care (www.iqwig.de)s an independent, non-governmentalnd non-profit foundation that is in-ended to establish evidence-based re-orts on drugs, non-drug interventions,ethods for diagnosis and screen-
ng, treatment guidelines and dis-ase management programs. In addi-ion, as an independent publisher of
1 (Submission for a modern law on patients’ights (‘‘Für ein modernes Patientenrechtege-etz’’, Bundestag-Drucksache 17/907, http://dip21.undestag.de/dip21/btd/17/009/1700907.pdf)
(scientific association that, within oneof its departments (‘‘patient informationand involvement‘‘), expressly accepts
Z. Evid. Fortbild. Qual. Gesundh. wesen (www.elsevier.de/zefq
evidence-based consumer health andpatient information, IQWiG has beenproviding evidence-based health infor-mation for patients and the generalcommunity since 2004. This informa-tion supports evidence-based decisionmaking in the German health care ser-vices. Informed Health Online went on-line in 2006, and has covered morethan 150 important medical topics sofar (www.informedhealthonline.de).
Health insurance, self-helporganizations and independentcounselling services
It is in the responsibility of social healthinsurance funds to preserve or cure thehealth of their members or improvetheir medical condition (Social SecurityCode, Art. 1). Scientifically sound andefficient measures have to be applied(Art. 70). Patients’ information andshared decision making are program-matically embedded. Within the frame-work of the Social Legislation Code (§65b, Volume Five), it is stated that in-dependent organizations for patientcounselling are funded by contributionsfrom the mandatory health insurance.These organizations pursue the goalof securing independent, neutral andhigh-quality counselling for patients inGermany, in order to strengthen theirautonomy and individual responsibil-ity. These counselling facilities informpatients of their rights as patients, en-able access to quality-assured patientinformation, and prepare the patientfor the medical consultation (www.unabhaengige-patientenberatung.de).This service has been legally establishedsince the beginning of 2011 followinga lengthy pilot phase.The Social Legislation Code (§ 20c, Vol-ume Five) also determines that self-helpgroups, organizations and contact of-fices are to be aided by the manda-tory health insurance. Self-help groupsshould receive a contribution from thehealth insurance funds of D 0.57 peryear (2011) and per insured person.
With this assistance, basic support forthe existing organizations can be carriedout, as well as the support of individuallyselected self-help projects. Self-help or-bCi
ZEFQ) 105 (2011) 263–270
anizations are actively supporting theoncept of shared decision making inermany.
gency for Quality in Medicine
nother non-governmental medical or-anization that strengthens patient
nfluence on medical decisions ishe Agency for Quality in Medicinewww.aezq.de), which is a non-profit or-anization owned by the German Med-
cal Association (BÄK) and the Nationalssociation of Statutory Health Insur-nce Physicians (KBV). The Agency hasreated a website, where informationn health is reviewed by patients andxperts regarding its quality and auton-my (www.patienten-information.de),nd which links to reliable informa-ion sources for consumers and pa-ients. Since medical treatment guide-ines are difficult to understand for mostatients, patient guidelines and deci-ion support tools (mostly print materi-ls) have been developed for the currentational Clinical Practice Guidelines (in-ications: asthma, chronic obstructiveulmonary disease, coronary heart dis-ase, diabetes, depression) and guide-ines in oncology (breast, prostate, andancreatic cancer)2 in order to makehe medical guidelines comprehensi-le and offer extensive informationnd support. Shared decision making,s the most valid clinician-patient ap-roach for guideline-oriented recom-endations, has recently been estab-
ished as a therapeutic strategy (recom-endation level B) for the first timeithin the National Clinical Practiceuideline on ‘‘Depression’’ [1]
erman Network forvidence-Based Medicine
ounded in 2000, the German Net-ork for Evidence-Based Medicine
www.ebm-netzwerk.de/english) is a
2 Guideline program and decision tools supportedy the German Cancer Association (DKG), the Germanancer Aid (DKH) and the Scientific Medical Societies
n Germany (AWMF)
265

sftahtsdoaaitfP
P
Tti(tThkttttctrktecgo
HC
HsFtatsahht
2
zswufoatds
-
-
-
Pm(Tmc1iptmig(McciiPto(cittcourses. The current dissemination ofSDM in medical education, and the im-
2
hared decision making. The area of in-ormation for patients and patient par-icipation within this network consists ofn aggregation of health professionals,ealth care researchers and representa-ives of the patient organizations andelf-help groups. The functions of thisepartment lie especially in the domainf educating people about the meaningnd issues of evidence-based medicine,s well as in developing and dispers-ng evidence-based treatment informa-ion for laypersons, recently guidelinesor health information (=Good Clinicalractice for Health Information, 2009)3.
atient Universities
he first university for pa-ients in Germany was foundedn Hannover in October 2006www.patientenuniversitaet.de), andhe second in Jena in October 2009.he universities’ goals are to offerealth education, empowerment,nowledge about healthcare struc-ures and methodological principleso citizens and patients. The universi-ies aim to address both experts andhe general population. Specific edu-ational provisions, which are orientedoward citizens, patients and their rep-esentatives, are designed to impartnowledge about responsibilities whenreating illnesses, as well as knowl-dge of the structures of the healthare system and methodological back-round for the assessment of studyutcomes.
ealth Targets and Nationalancer Plan
ealth targets.de (www.gesundheitziele.de) is a co-operation between theederal Ministry of Health (BMG) andhe Association for Social Security Policynd Research (GVG) and is funded byhe Ministry. Health targets.de aims totrengthen the idea of target setting atll levels of the health care system and
as so far been developing six specificealth targets, one explicitly concerninghe improvement of patients’ and citi-3 www.ebm-netzwerk.de/grundlagen/images/gpgi009 11.pdf
pw
hk
66
ens’ competence in health-related is-ues. In 2008, the National Cancer Planas started in Germany. This program,nder the direction the Federal Ministryor Health, describes the main tasks toptimize oncologic care in four areas ofction. In the area ‘‘Strengthening Pa-ient Orientation’’, the aim of sharedecision making has explicitly been de-cribed as follows:
Patients have to be actively involved inmaking decisions regarding their careEvidence-based information shouldbe provided to patients during therapyand care to support them in makingdecisionsShared decision making should beimplemented4.
atient participation inedical decision making
micro level)he approach of patient participation inedical decision making has been dis-
ussed openly in Germany since the late990 s. However, the first publications
n German [2–4] only discussed the ap-roach conceptually. Clinical trials forhe evaluation of patient participation inedical decision making were primar-
ly initiated through the research pro-ram of the Federal Ministry of Healthwww.shared-decision-making.org) [5].edical education at the universities
oncerning the topics physician-patientommunication and decision makings executed at Institutes of Med-cal Psychology, Medical Sociology,sychosomatics, and General Prac-ice. In an older survey, 12 outf 23 Medical Psychology institutes52%) disclosed that they have in-orporated shared decision makingnto medical education [6], and thatraining efforts had been undertakeno prepare academic teachers for these
lementation and importance of SDM,as again assessed in February 2011
4 National Cancer Plan, Background Paper:ttp://www.bmg.bund.de/glossarbegriffe/nationaler-rebsplan.html.)
Z. Evid. Fortbild. Qual.
via telephone interviews. Results canbe reported from 24 of 32 MedicalPsychology departments (Germany has32 medical schools). 67% (N = 16) ofthose interviewed stated that SDM ispart of their curriculum. On average, in-stitutes spend 3-4 hours per semesteron teaching SDM (lectures / seminars).The relevance of SDM within the cur-riculum has been rated with a meanof 5.3 (in 2006: mean 4.4, range: 0to 10). Nine of the institutes indicatedthat they use SDM-specific teaching ma-terials, of which five refer to a partic-ular SDM training manual [30]. Thus,this update shows a moderate increasein the dissemination and importance ofSDM in medical education in Germanycompared to 2007.
Current state of nationalresearch on shareddecision makingSince the funding of the research pro-gram ‘‘Patient as partner in medicaldecision making’’ (2001-2005), fundedby the German Ministry of Health(GMH), research in this subject hasbecome measurably consistent. In atheory-guided consensus process, theGerman-language definition of patientparticipation in medical decision making(Shared Decision Making = PartizipativeEntscheidungsfindung - PEF) was es-tablished [3]. Prior to the funding, in-dividual work groups at different uni-versities had researched this subject(www.evidence.de; www.gesundheit.uni-hamburg.de). Controlled studieshave been made possible in large partby this research program [5].Studies were implemented within fiveareas of internal medicine (hyperten-sion [7], respiratory illnesses, arterial ob-structive disease, breast cancer [8–10]and palliative care [11,12]) as wellas five areas in the fields of neu-rology and psychiatry (multiple sclero-sis [13–16], chronic pain [17–19], al-cohol abuse [20], depression [21–24]
and schizophrenia [25–27]). Further-more, many questionnaires for themeasurement of processes and out-come of shared decision making wereGesundh. wesen 105 (2011) 263–270www.elsevier.de/zefq
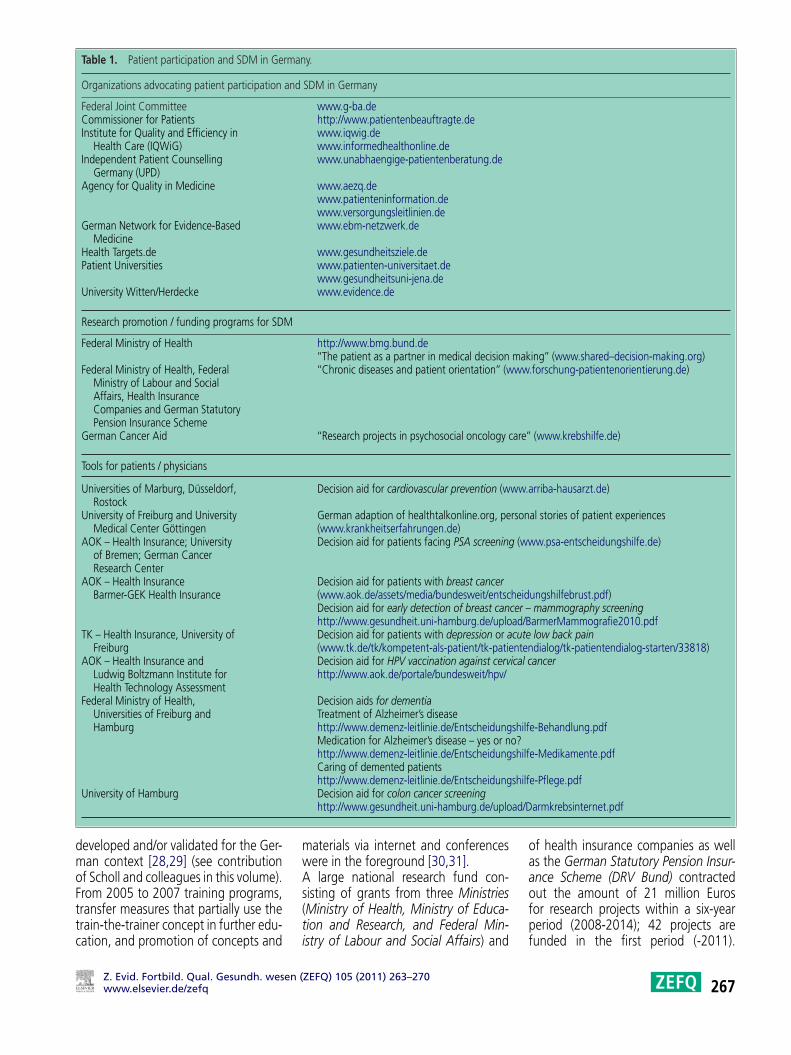
Table 1. Patient participation and SDM in Germany.
Organizations advocating patient participation and SDM in Germany
Federal Joint Committee www.g-ba.deCommissioner for Patients http://www.patientenbeauftragte.deInstitute for Quality and Efficiency in
Health Care (IQWiG)www.iqwig.dewww.informedhealthonline.de
Independent Patient CounsellingGermany (UPD)
www.unabhaengige-patientenberatung.de
Agency for Quality in Medicine www.aezq.dewww.patienteninformation.dewww.versorgungsleitlinien.de
German Network for Evidence-BasedMedicine
www.ebm-netzwerk.de
Health Targets.de www.gesundheitsziele.dePatient Universities www.patienten-universitaet.de
www.gesundheitsuni-jena.deUniversity Witten/Herdecke www.evidence.de
Research promotion / funding programs for SDM
Federal Ministry of Health http://www.bmg.bund.de‘‘The patient as a partner in medical decision making’’ (www.shared–decision-making.org)
Federal Ministry of Health, FederalMinistry of Labour and SocialAffairs, Health InsuranceCompanies and German StatutoryPension Insurance Scheme
‘‘Chronic diseases and patient orientation’’ (www.forschung-patientenorientierung.de)
German Cancer Aid ‘‘Research projects in psychosocial oncology care’’ (www.krebshilfe.de)
Tools for patients / physicians
Universities of Marburg, Düsseldorf,Rostock
Decision aid for cardiovascular prevention (www.arriba-hausarzt.de)
University of Freiburg and UniversityMedical Center Göttingen
German adaption of healthtalkonline.org, personal stories of patient experiences(www.krankheitserfahrungen.de)
AOK – Health Insurance; Universityof Bremen; German CancerResearch Center
Decision aid for patients facing PSA screening (www.psa-entscheidungshilfe.de)
AOK – Health InsuranceBarmer-GEK Health Insurance
Decision aid for patients with breast cancer(www.aok.de/assets/media/bundesweit/entscheidungshilfebrust.pdf)Decision aid for early detection of breast cancer – mammography screeninghttp://www.gesundheit.uni-hamburg.de/upload/BarmerMammografie2010.pdf
TK – Health Insurance, University ofFreiburg
Decision aid for patients with depression or acute low back pain(www.tk.de/tk/kompetent-als-patient/tk-patientendialog/tk-patientendialog-starten/33818)
AOK – Health Insurance andLudwig Boltzmann Institute forHealth Technology Assessment
Decision aid for HPV vaccination against cervical cancerhttp://www.aok.de/portale/bundesweit/hpv/
Federal Ministry of Health,Universities of Freiburg andHamburg
Decision aids for dementiaTreatment of Alzheimer’s diseasehttp://www.demenz-leitlinie.de/Entscheidungshilfe-Behandlung.pdfMedication for Alzheimer’s disease – yes or no?http://www.demenz-leitlinie.de/Entscheidungshilfe-Medikamente.pdfCaring of demented patientshttp://www.demenz-leitlinie.de/Entscheidungshilfe-Pflege.pdf
ad/D
dmoFttc
oaao
University of Hamburg
eveloped and/or validated for the Ger-an context [28,29] (see contributionf Scholl and colleagues in this volume).rom 2005 to 2007 training programs,
ransfer measures that partially use therain-the-trainer concept in further edu-ation, and promotion of concepts andZ. Evid. Fortbild. Qual. Gesundh. wesen (www.elsevier.de/zefq
Decision aid for colon cancer screeninghttp://www.gesundheit.uni-hamburg.de/uplo
materials via internet and conferenceswere in the foreground [30,31].A large national research fund con-sisting of grants from three Ministries
(Ministry of Health, Ministry of Educa-tion and Research, and Federal Min-istry of Labour and Social Affairs) andfpf
ZEFQ) 105 (2011) 263–270
armkrebsinternet.pdf
f health insurance companies as wells the German Statutory Pension Insur-nce Scheme (DRV Bund) contractedut the amount of 21 million Euros
or research projects within a six-yeareriod (2008-2014); 42 projects areunded in the first period (-2011).267

StmgasfTdamdtitGdsdhcIagnsgwooapmOptfatabiassB(tio(
PA
w
FhiFsegw‘cclcttmccpaetgsm
IadGTmthpiifSNbpgift
2
tudies are proposed within the threehemes ‘‘Need-specific patient infor-ation’’ (1), ‘‘Patient education pro-rams for chronically ill patients’’ (2)nd ‘‘Organisation of participatorytructure of health care’’ (3) (www.orschung-patientenorientierung.de).en projects are further investigatingiverse SDM-related research questionsnd interventions (e.g. the develop-ent of shared goals in coronary heartisease or in vocational rehabilitation,he development of decision supportnterventions in chronic diseases, theransfer of ‘‘healthtalkonline.org’’ intoerman, the development and/or vali-ation of SDM-related assessment in-truments, or the evaluation of inter-isciplinary SDM training programs forealth professionals in rehabilitationlinics).n addition, the German Cancer Aid,
non-profit organization with theoal of improving prevention, diag-osis, therapy, psychological care andelf-help, is funding different researchrants (two periods from 2008-2014,ww.krebshilfe.de) for psychosocialncology with an emphasis on patientrientation (background, developmentnd implementation of the concepts ofatient orientation and shared decisionaking in health care)5.ther cooperation partners that sup-ort specific research and implemen-ation projects are health insuranceunds. Web-based patient decision aidsnd interactive health information sys-ems, which include decision makingids for prostate cancer screening, acuteack pain, and depression are be-
ng worked on and evaluated and re-lised via the websites of health in-urance companies6. The Scientific In-titute of Techniker Krankenkasse forenefit and Efficiency in Health CareWINEG) has defined patients’ informa-ion as one issue of three fields of activ-ty. In this field of activity, diverse areas
f evidence-based patient informationEBPI) have been developed [32,33].5 www.krebshilfe.de/fileadmin/Inhalte/Downloads/DFs/Foerderung/2010 Psychosoz Onkol 2/PSOusschreibunstext final homepage.pdf6 www.tk-online.de;ww.psa-entscheidungshilfe.de
tDpdAtpm
Medical Center Hamburg-Eppendorffor their support in conducting the tele-
68
inally, decision support technologiesave been developed and implemented
n routine care through funding of theederal Ministry of Education and Re-earch (www.arriba-hausarzt.de). Thelectronic library of decision aids foreneral practitioners, ‘‘arriba-libTM’’,ith ‘‘lib’’ being an acronym for
‘library’’, has a modular structure andurrently contains evidence-based de-ision aids for the topics cardiovascu-ar prevention [34–36], atrial fibrillation,oronary heart disease, oral antidiabe-ics, conventional and intensified insulinherapy, and unipolar depression. Theodules are structured to assist physi-
ians in counselling their patients ac-ording to the shared decision makinghilosophy. These steps can be regardeds a framework to help the clinician toffectively structure the encounter. Theools are, however, only available foreneral practitioners, organized withinpecific integrated care contracts at theoment.
mplementation strategiesnd perspectives of sharedecision making inermany
he dissemination of shared decisionaking is possible through different in-
ervention strategies: Interventions forealth care providers are mostly accom-lished through publications, continu-
ng education and training. The follow-ng table offers an overview of agencies,unding programs and tools advocatingDM in Germany (see Table 1).ationwide training interventions hadeen administered [30,31], and the im-lementation in communication pro-rams in many of the German Med-
cal schools has been rather success-ul [6]. However, the transfer to rou-ine medical care still has a long wayo go.espite promising individual researchrojects [14,15,34] as well as projects ofifferent health insurance funds and the
gency for Quality in Medicine initia-ives, the development of decision sup-ort materials and technologies in Ger-any is, in comparison to important
Z. Evid. Fortbild. Qual.
English-speaking countries, still laggingbehind. This is an area in which theneed for development and evaluationis very high. International and/or Euro-pean efforts to adapt and transfer es-tablished decision tools may representrational ways to proceed faster [37].A clear indication for increasing im-plementation is the linking of shareddecision making with the actions of se-cure quality management, self-help ini-tiatives [38] and the patient safety ini-tiative within the German health care.Patient participation in medical decisionmaking is increasingly seen as a qual-ity indicator for medical care and musttherefore be addressed within the qual-ity reports of hospitals and practices (pa-tient orientation is already defined as acriterion within the certification processfor quality management systems in hos-pitals and practices, see: www.ktq.de).Altogether, there are many differentfacets that have enabled the imple-mentation of shared decision mak-ing in Germany. Shared decision mak-ing has been successfully initiatedand paths for implementation evalu-ated. However, many steps still haveto be taken to further develop andimplement the approach of shareddecision making in daily medicalcare.Research was, and is, a strong driverin this field in Germany. At the end of2010, the Federal Government passedthe framework program ‘‘Health Re-search’’, in which the Federal Ministryof Education and Research is support-ing research with more than five billionEuros between 2011 and 2014. It hasexplicitly been stated that one of the sixaction areas will focus on patient orien-tation, patient safety and processes formutual decision making7.
AcknowledgementWe are grateful to Sarah Dwinger, LisaTlach, and Ivo Engert at the University
phone survey (status of implementation
7 http://www.bmbf.de/pub/gesundheitsforschung.pdf
Gesundh. wesen 105 (2011) 263–270www.elsevier.de/zefq

osSt
R
f shared decision making in medicalchools’ curricula). The authors thankarah Mannion (Berlin) for her transla-ion and copyediting support.
eferences[1] Härter M, Klesse C, Bermejo I, Schneider F,
Berger M. Unipolar depression: diagnosticand therapeutic recommendations from thecurrent S3/National Clinical Practice Guide-line. Dtsch Arztebl Int 2010;107(40):700–8.
[2] Isfort J, Floer B, Koneczny N, Vollmar HC,Butzlaff M. Shared Decision-making: Arztoder Patient: Wer entscheidet? Dtsch medWochenschr 2002;127(39):2021–4.
[3] Härter M. Partizipative Entscheidungsfind-ung (Shared Decision-Making) – ein von Pa-tienten, Ärzten und der Gesundheitspolitikgeforderter Ansatz setzt sich durch. Z ArztlFortbild Qualitatssich 2004;98:89–92.
[4] Dierks ML, Seidel G. GleichberechtigteBeziehungsgestaltung zwischen Ärztenund Patienten – wollen Patienten wirklichPartner sein? In: Härter M, Loh A, SpiesC, editors. Gemeinsam entscheiden – er-folgreich behandeln. Neue Wege für Ärzteund Patienten im Gesundheitswesen. Köln:Deutscher Ärzteverlag; 2005. p. 35–44.
[5] Loh A, Simon D, Bieber C, Eich W, HärterM. Patient and citizen participation in Ger-man health care-current state and futureperspectives. Z Arztl Fortbild Qualitatssich2007;101(4):229–35.
[6] Loh A, Simon D, Rockenbauch K, HärterM. Partizipative Entscheidungsfindung -Stellenwert und Verbreitung in der medi-zinischen Ausbildung. Z Med Psychol2006;15(2):87–92.
[7] Deinzer A, Veelken R, Kohnen R, SchmiederRE. Is a shared decision-making ap-proach effective in improving hyper-tension management? J Clin Hypertens2009;11(5):266–70.
[8] Vodermaier A, Caspari C, Bauerfeind I,Kahlert S, Straub J, Untch M. Decisionaids für Partizipative Entscheidungsfindungbeim primären Mammakarzinom [Decisionaids for shared decision-making in primarybreast cancer]. Z Arztl Fortbild Qualitatssich2004;98(2):127–34.
[9] Vodermaier A, Caspari C, Koehm J, KahlertS, Ditsch N, Untch M. Contextual factorsin shared decision making: a randomisedcontrolled trial in women with a strongsuspicion of breast cancer. Br J Cancer2009;24;100(4):590–7, 24.
[10] Vodermaier A, Caspari C, Wang L, Koehm J,Ditsch N, Untch M. How and for whom aredecision aids effective? Long-term psycho-logical outcome of a randomized controlledtrial in women with newly diagnosed breast
cancer. Health Psychol 2011;30(1):12–9.[11] Schweitzer S, van Oorschot B, Köhler N,Leppert K, Steinbach K, Hausmann C,et al. Der Patient und seine Familie – Ein-
Z. Evid. Fortbild. Qual. Gesundh. wesen (www.elsevier.de/zefq
stellungen und Mitsprachemöglichkeitenvon Angehörigen palliativ behandelterTumorpatienten. Psychother Psych Med2005;55:298–304.
[12] Van Oorschot B, Sayer B, Schaefer I. Pallia-tivberatung im Modellvorhaben ‘‘Patientenals Partner – Tumorpatienten und ihrMitwirken bei medizinischen Entscheidun-gen’’. Z Palliativmed 2005;6:90–4.
[13] Kasper J, Köpke S, Mühlhauser I, HeesenC. Evidence-based patient informationabout treatment of multiple sclerosis-Aphase one study on comprehension andemotional responses. Patient Educ Couns2006;62:56–63.
[14] Kasper J, Köpke S, Mühlhauser I, NüblingM, Heesen C. Informed shared decisionmaking about immunotherapy for pa-tients with multiple sclerosis (ISDIMS): arandomized controlled trial. Eur J Neurol2008;15(12):1345–52.
[15] Köpke S, Kasper J, Mühlhauser I, NüblingM, Heesen C. Patient education pro-gram to enhance decision autonomy inmultiple sclerosis relapse management:a randomized-controlled trial. Mult Scler2009;15(1):96–104.
[16] Heesen C, Kasper J, Segal J, Koepke S,Mühlhauser I. Decisional role preferences,knowledge and information interests in pa-tients with multiple sclerosis. Mult Scler2004;10:643–50.
[17] Bieber C, Müller KG, Blumenstiel K, Schnei-der A, Richter A, Wilke S, et al. Long-termeffects of a shared decision-making in-tervention on physician-patient interactionand outcome in fibromyalgia. A qualitativeand quantitative one year follow-up of arandomized controlled trial. Patient EducCouns 2006;63:357–66.
[18] Hochlehnert A, Richter A, Bludau HB,Bieber C, Blumenstiel K, Mueller K,et al. A computer-based information-toolfor chronic pain patients. Computer-ized information to support the processof shared decision-making. Patient EducCouns 2006;61:92–8.
[19] Bieber C, Müller KG, Blumenstiel K, RichterA, Hochlehnert A, Wilke S, et al. Ashared decision making communicationtraining programme for physicians treat-ing fibromyalgia patients - effects of a ran-domized controlled trial. J Psychosom Res2008;64(1):13–20.
[20] Neumann T, Neuner B, Weiss-Gerlach E,Tonnesen H, Gentilello L, Wernecke KD,et al. The effect of computerized tailoredbrief advice on at-risk drinking in subcrit-ically injured trauma patients. J Trauma2006;61:805–14.
[21] Loh A, Kremer N, Giersdorf N, Jahn H,Hänselmann S, Bermejo I, et al. Informa-tion and participation interests of patientswith depression in clinical decision-making
in primary care. Z Arztl Fortbild Qualitatssich2004;98:101–7.[22] Loh A, Simon D, Hennig K, Hennig B, HärterM, Elwyn G. The assessment of depressive
ZEFQ) 105 (2011) 263–270
patients’ involvement in decision-making inaudio taped primary care consultations. PatEduc Couns 2006;63:314–8.
[23] Loh A, Leonhart R, Wills CE, Simon D,Härter M. The impact of patient participa-tion on adherence and clinical outcome inprimary care of depression. Pat Educ Couns2007;65:69–78.
[24] Loh A, Simon D, Wills CE, KristonL, Niebling W, Härter M. The effectsof a shared decision-making interven-tion in primary care of depression: acluster-randomized controlled trial. PatEduc Couns 2007;67(3):324–32.
[25] Hamann J, Langer B, Winkler V, BuschR, Cohen R, Leucht S, et al. Shareddecision-making for in-patients withschizophrenia. Acta Psychiatr Scand2006;14:265–73.
[26] Hamann J, Cohen C, Leucht S, BuschR, Kissling W. Shared decision-makingand long-term outcome in schizophreniatreatment. J Clin Psychiatry 2007;68(7):992–7.
[27] Reichhart T, Kissling W, Scheuring E,Hamann J. Patient participation in Germanpsychiatry - a critical review. Psychiatr Prax2008;35(3):111–21.
[28] Simon D, Kriston L, Loh A, Spies C, ScheiblerF, Wills C, et al. Confirmatory factor analy-sis and recommendations for improvementof the Autonomy-Preference-Index (API).Health Expect 2010;13(3):234–43.
[29] Kriston L, Scholl I, Hölzel L, Simon D, LohA, Härter M. The 9-item Shared DecisionMaking Questionnaire (SDM-Q-9). Devel-opment and psychometric properties in aprimary care sample. Patient Educ Couns2010;80(1):94–9.
[30] Bieber C, Loh A, Ringel N, EichW, Härter M. Patientenbeteiligung beimedizinischen Entscheidungen. Manualzur Partizipativen Entscheidungsfindung(Shared Decision Making). Publisher: Uni-versitätsklinika Heidelberg und Freiburg;2007.
[31] Bieber C, Nicolai J, Ringel N, BlumenstielK, Schneider A, Hartmann M, et al. Train-ing physicians in Shared Decision-Making(SDM) - who can be reached andwhat is achieved? Patient Educ Couns2009;77:48–54.
[32] Genz J, Haastert B, Mayer G, SteckelbergA, Müller H, Cole D, et al. Blood glucosetesting and primary prevention of diabetesmellitus type 2 – evaluation of the effect ofevidence based patient information. BMCPublic Health 2010;14(10):15.
[33] Straub C, Nebling T, Müller H. Translatingresearch into practice: A German sicknessfund supporting patient participation. Pa-tient Educ Couns 2008;73:544–50.
[34] Krones T, Keller H, Sonnichsen A, SadowskiEM, Baum E, Wegscheider K, et al. Abso-
lute cardiovascular disease risk and shareddecision making in primary care: A ran-domized controlled trial. Ann Fam Med2008;6(3):218–27.269

decision-making and the contribution of
2
[35] Hirsch O, Keller H, Albohn-Kühne C,Krones T, Donner-Banzhoff N. Satis-faction of patients and primary carephysicians with shared decision mak-
ing. Eval Health Prof 2010;33(3):321–42.[36] Krones T, Keller H, Becker A, SönnichsenA, Baum E, Donner-Banzhoff N. The the-
70
ory of planned behaviour in a random-ized trial of a decision aid on cardiovas-cular risk prevention. Patient Educ Couns2010;78(2):169–76.
[37] Albrecht K, Simon D, Buchholz A, ReuterK, Frosch D, Seebauer L, et al. How doesa German audience appraise an Americandecision aid on early stage breast cancer?
Z. Evid. Fortbild. Qual.
Patient Educ Couns 2010 Jun 3 [Epub aheadof print].
[38] Simon D, Härter M. The principles of shared
self-help institutions. Bundesgesundheits-blatt Gesundheitsforschung Gesundheits-schutz 2009;52(1):86–91.
Gesundh. wesen 105 (2011) 263–270www.elsevier.de/zefq